
This topic uses the AIM Learning Cycle to help MBBS students understand the anatomical structure and development of the esophagus by integrating Anatomy, Embryology and Histology.
1. Curriculum Coverage
Anatomy
• Extent of esophagus
• Course of esophagus
• Relations of esophagus
• Gross structure of esophagus
Embryology
• Development of esophagus
Histology
• Epithelium of esophagus
• Esophageal glands
• Musculature differences in esophagus
Pathology
• Histological types of esophageal carcinoma
• Presentation of esophageal carcinoma
2. Learning Material
1️⃣ INTRODUCTION
The esophagus is a muscular tube that transports food from the pharynx to the stomach, forming an essential part of the gastrointestinal tract. It lies in the neck, thorax, and abdomen, passing through the posterior mediastinum before entering the stomach. Proper functioning of the esophagus ensures safe swallowing and prevents reflux of gastric contents. Understanding its structure, development, and histology helps explain swallowing disorders, congenital defects, and cancers. Clinically, the esophagus is important because it is involved in conditions such as dysphagia, gastroesophageal reflux disease (GERD), and esophageal carcinoma, which are frequently tested in exams and encountered in clinical practice.
2️⃣ FOUNDATION BASICS
Key Definitions
• Esophagus: A muscular tube connecting the pharynx to the stomach.
• Deglutition: The process of swallowing.
• Upper Esophageal Sphincter (UES): Muscular opening at the junction of pharynx and esophagus.
• Lower Esophageal Sphincter (LES): Functional sphincter preventing gastric reflux.
• Peristalsis: Wave-like muscular contraction moving food downward.
Essential Terminology
• Posterior mediastinum: Space in thoracic cavity where most of esophagus lies.
• Constrictions of esophagus: Narrow areas clinically important.
• Stratified squamous epithelium: Protective epithelial lining of esophagus.
• Adventitia: Outer connective tissue covering most of esophagus.
• Carcinoma: Malignant tumor arising from epithelial tissue.
Basic Overview
• Length: ~25 cm
• Extends from C6 vertebra to T11 vertebra
• Divided into:
o Cervical part
o Thoracic part
o Abdominal part
• Functions mainly in transport of food
• Lined by protective mucosa
• Supported by coordinated muscular contractions
3️⃣ CORE LEARNING — CURRICULUM COVERAGE
ANATOMY
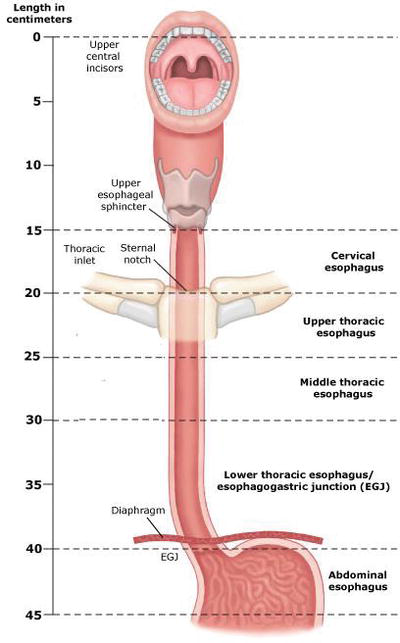
Extent of Esophagus
🧠 CORE
• Begins at lower border of cricoid cartilage (C6)
• Ends at cardiac orifice of stomach (T11)
• Length: ~25 cm
• Lies posterior to trachea
• Passes through esophageal hiatus at T10
• Divided into:
o Cervical part (5 cm)
o Thoracic part (18 cm)
o Abdominal part (2 cm)
• Connects pharynx to stomach
• Crosses diaphragm before entering stomach
🔬 CONCEPT EXPLAINED
Structure:
The esophagus begins at the level of C6 vertebra, where the pharynx ends. It descends vertically through the thorax and passes through the diaphragm at T10, ending at T11.
Mechanism:
This pathway allows swallowed food to travel from mouth to stomach efficiently.
Structure → Function:
Its vertical alignment ensures gravity assists swallowing.
⚠️ IF DAMAGED
• Injury → disruption of swallowing
• Result → dysphagia
• Severe trauma → leakage of contents → mediastinitis
Course of Esophagus
🧠 CORE
• Begins at C6
• Passes behind trachea
• Enters thorax through superior thoracic aperture
• Lies in posterior mediastinum
• Deviates slightly to left near lower thorax
• Passes through diaphragm at T10
• Ends at T11
• Crossed anteriorly by left bronchus
• Lies anterior to vertebral column
🔬 CONCEPT EXPLAINED
Structure:
The esophagus descends behind the trachea and heart before entering the stomach.
Mechanism:
Its position allows smooth transition of food through thorax.
Structure → Function:
Posterior location protects it from compression during breathing.
⚠️ IF DAMAGED
Compression → swallowing difficulty
Example:
• Enlarged left atrium → compresses esophagus
• Result → dysphagia
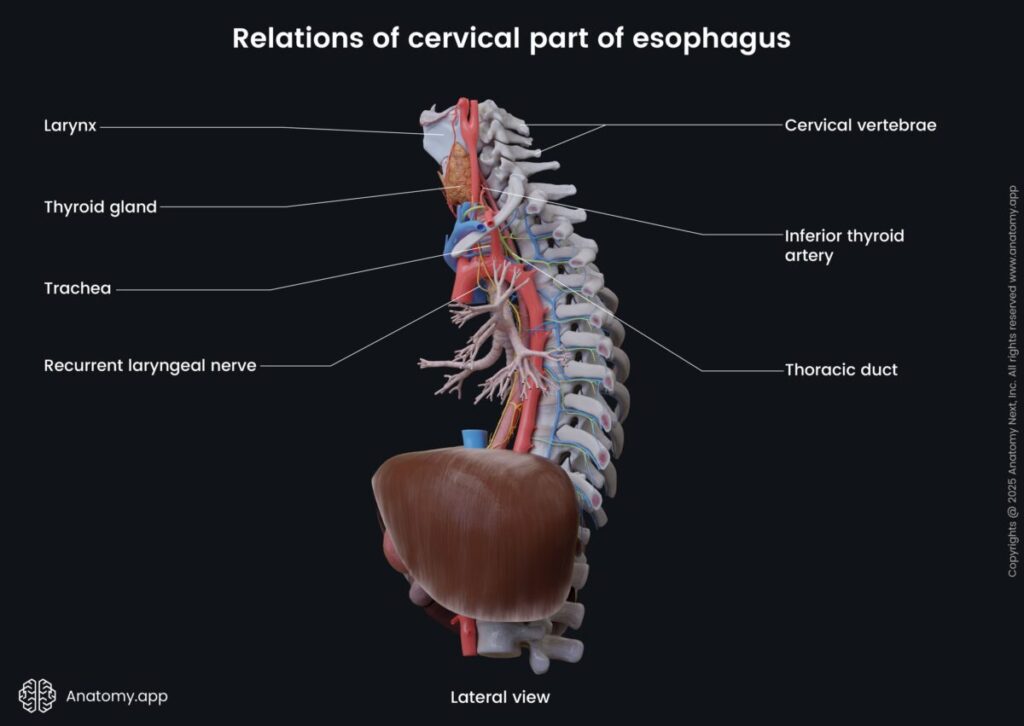
Relations of Esophagus
🧠 CORE
Cervical Part Relations
Anterior:
• Trachea
Posterior:
• Vertebral column
Lateral:
• Thyroid gland
• Carotid sheath
Thoracic Part Relations
Anterior:
• Trachea
• Left bronchus
• Left atrium
Posterior:
• Vertebral column
• Thoracic duct
Lateral:
• Lungs and pleura
Abdominal Part Relations
Anterior:
• Left lobe of liver
Posterior:
• Left crus of diaphragm
🔬 CONCEPT EXPLAINED
Structure:
Relations change as esophagus moves from neck to abdomen.
Mechanism:
These relations influence symptoms in diseases affecting nearby organs.
Structure → Function:
Close relation to heart explains cardiac effects on swallowing.
⚠️ IF DAMAGED
• Tumor growth → compress adjacent structures
• Example:
Esophageal tumor → tracheal compression → breathing difficulty
Gross Structure of Esophagus
🧠 CORE
• Muscular tube
• Four layers:
- Mucosa
- Submucosa
- Muscularis externa
- Adventitia
• Contains four constrictions
• Upper and lower sphincters present
• Lumen normally collapsed
• Rich nerve supply from vagus nerve
• Blood supply from multiple arteries - 🔬 CONCEPT EXPLAINED
Structure:
The esophagus wall consists of muscular layers allowing contraction.
Mechanism:
Muscle contraction produces peristalsis, pushing food downward.
Structure → Function:
Circular and longitudinal muscle layers enable directional movement.
⚠️ IF DAMAGED
Muscle damage → ineffective peristalsis
Result → food stagnation → dysphagia
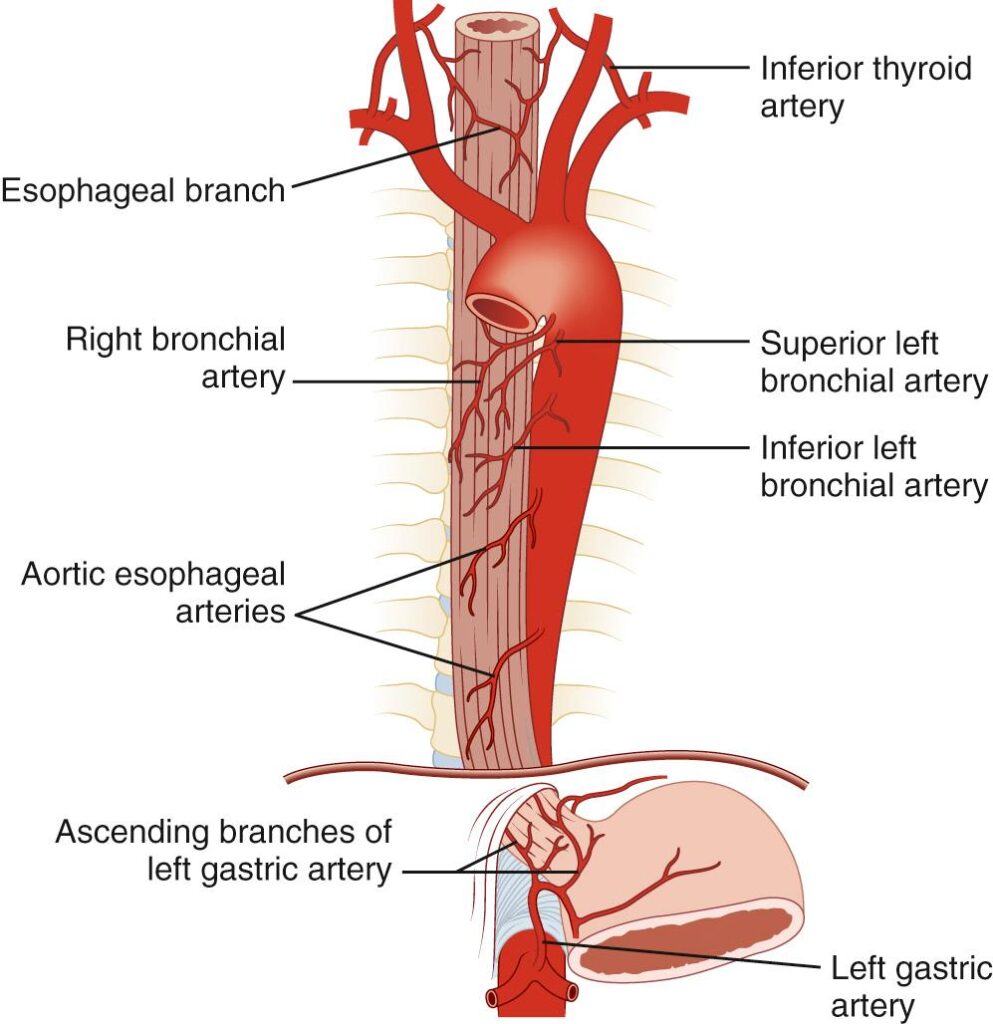
Blood Supply of Esophagus
Include:
Arterial:
• Inferior thyroid artery
• Thoracic aorta
• Left gastric artery
Venous:
• Portal-systemic anastomosis
• Varices concept
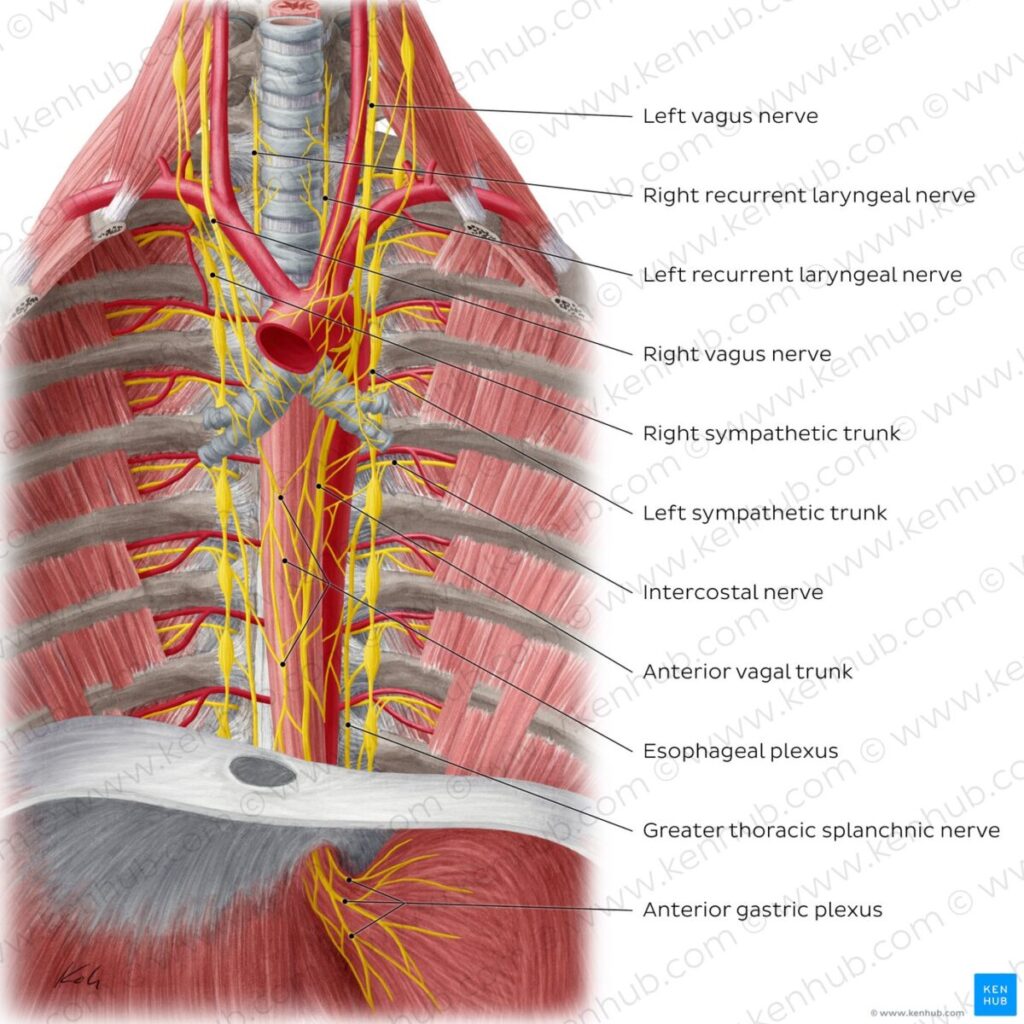
Nerve Supply
Include:
• Vagus nerve
• Sympathetic trunk
• Esophageal plexus
EMBRYOLOGY
Development of Esophagus
🧠 CORE
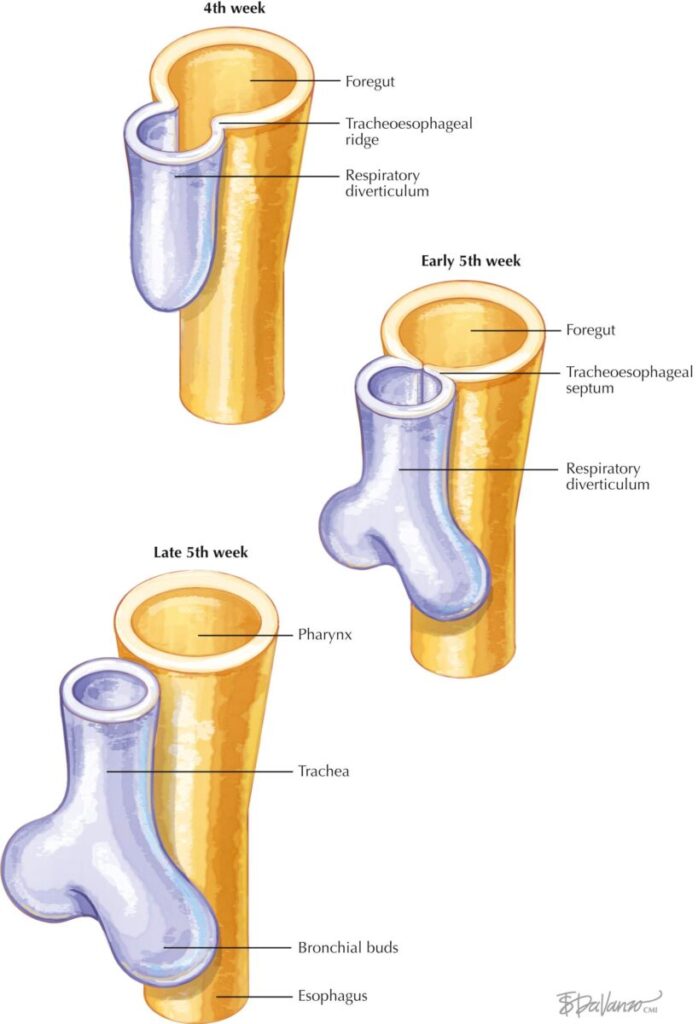
• Develops from foregut
• Begins in 4th week
• Tracheoesophageal septum divides foregut
• Upper part forms esophagus
• Lining initially stratified columnar
• Later becomes stratified squamous
• Muscles differentiate from mesenchyme
• Length increases as heart descends
🔬 CONCEPT EXPLAINED
Structure:
Foregut divides into respiratory and digestive tubes.
Mechanism:
Septum formation separates trachea and esophagus.
Structure → Function:
Separation prevents aspiration of food into lungs.
⚠️ IF DAMAGED
Failure of separation →
→ Tracheoesophageal fistula
Effects:
• Choking during feeding
• Milk enters lungs
• Respiratory distress
HISTOLOGY
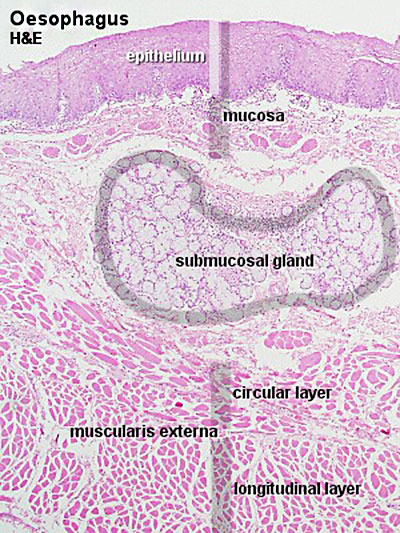
Epithelium of Esophagus
🧠 CORE
• Stratified squamous epithelium
• Non-keratinized
• Protective function
• Resists mechanical injury
• Thick mucosal lining
• Contains basal cells
• Rapid cell turnover
• Protects against friction
🔬 CONCEPT EXPLAINED
Structure:
Multiple layers of cells provide mechanical strength.
Mechanism:
Food bolus causes friction → epithelium resists damage.
Structure → Function:
Stratification prevents ulcer formation.
⚠️ IF DAMAGED
Chronic irritation →
→ Metaplasia (Barrett esophagus)
Risk:
→ Esophageal carcinoma
Esophageal Glands
Types of Esophageal Glands
• Proper glands
• Cardiac glands
🧠 CORE
• Located in submucosa
• Mucus-secreting glands
• Lubricate lumen
• Facilitate swallowing
• Protect mucosa
• Numerous along length
• Produce alkaline mucus
Structure:
Glands open into esophageal lumen.
Mechanism:
Mucus reduces friction.
Structure → Function:
Smooth passage of food.
⚠️ IF DAMAGED
Reduced mucus →
→ Painful swallowing
Musculature Differences in Esophagus
🧠 CORE
Upper third:
• Skeletal muscle
Middle third:
• Mixed muscle
Lower third:
• Smooth muscle
Function:
• Produces peristalsis
Controlled by:
• Vagus nerve
🔬 CONCEPT EXPLAINED
Structure:
Gradual transition from voluntary to involuntary muscle.
Mechanism:
Allows voluntary swallowing initially and involuntary continuation.
Structure → Function:
Ensures coordinated movement.
⚠️ IF DAMAGED
Nerve injury →
→ Loss of peristalsis
→ Dysphagia
PATHOLOGY
Histological Types of Esophageal Carcinoma
🧠 CORE
Two main types:
- Squamous cell carcinoma
- Adenocarcinoma
Locations:
• Squamous: upper and middle
• Adenocarcinoma: lower esophagus
Risk factors:
• Smoking
• Alcohol
• GERD
• Barrett esophagus
🔬 CONCEPT EXPLAINED
Structure:
Carcinoma arises from epithelial lining.
Mechanism:
Chronic irritation causes mutation.
Structure → Function:
Tumor narrows lumen.
⚠️ IF DAMAGED
Tumor growth →
→ Obstruction → Dysphagia
Presentation of Esophageal Carcinoma
🧠 CORE
• Progressive dysphagia
• Weight loss
• Painful swallowing
• Regurgitation
• Hoarseness
• Chronic cough
• Hematemesis (late)
• Anemia
🔬 CONCEPT EXPLAINED
Structure:
Tumor compresses lumen.
Mechanism:
Food passage becomes difficult.
Structure → Function:
Swallowing failure leads to malnutrition.
⚠️ IF DAMAGED
Late detection →
→ Poor prognosis
4️⃣ MECHANISM FLOW — SWALLOWING THROUGH ESOPHAGUS
- Food enters pharynx
- Upper esophageal sphincter relaxes
- Food enters esophagus
- Circular muscles contract
- Longitudinal muscles shorten tube
- Peristaltic wave pushes food downward
- Lower sphincter relaxes
- Food enters stomach
5️⃣ FUNCTIONAL INTEGRATION
Structure → Function → Outcome
• Stratified epithelium → Protection → Safe food passage
• Muscular layers → Peristalsis → Food transport
• Submucosal glands → Lubrication → Smooth swallowing
• Sphincters → Direction control → Prevent reflux
6️⃣ CLINICAL CORRELATION
Common exam-relevant conditions:
Dysphagia
Cause:
• Tumor
• Nerve damage
• Stricture
Effect:
• Difficulty swallowing
Gastroesophageal Reflux Disease (GERD)
Cause:
• Weak lower esophageal sphincter
Effect:
• Acid reflux
• Heartburn
Tracheoesophageal Fistula
Cause:
• Developmental defect
Effect:
• Food enters airway
Esophageal Carcinoma
Key signs:
• Progressive dysphagia
• Weight loss
⭐ 7️⃣ POINTS TO REMEMBER
- Esophagus extends from C6 to T11
- Passes through diaphragm at T10
- Length approximately 25 cm
- Lined by stratified squamous epithelium
- Upper third contains skeletal muscle
- Lower third contains smooth muscle
- Develops from foregut
- Failure of septum formation → tracheoesophageal fistula
- Two major carcinoma types exist
- Progressive dysphagia is key warning symptom
- Submucosal glands produce lubricating mucus
- Lower esophageal sphincter prevents reflux
MASTER CONCEPT MAP — ESOPHAGUS
ESOPHAGUS
│
─────────────────────────────────────────────────────
│ │ │
ANATOMY HISTOLOGY EMBRYOLOGY
│ │ │
│ │ │
Extent Epithelium Foregut origin
Course Glands Tracheoesophageal septum
Relations Muscle layers Lengthening process
Gross structure Wall layers Congenital defects
│ │ │
│ │ │
Blood Supply Mucosal protection TE Fistula
Nerve Supply Lubrication Esophageal atresia
Constrictions Peristalsis Separation failure
│ │ │
─────────────────────────────────────────────────────
│
FUNCTION
│
Food Transport
│
Peristalsis
│
─────────────────────────────────────────────────────
│
CLINICAL
│
Dysphagia ─ GERD ─ Carcinoma ─ VaricesSUBMAP 1 — Anatomy Overview Map
ESOPHAGUS — ANATOMY
│
─────────────────────────────────────
│ │ │
EXTENT COURSE RELATIONS
│ │ │
C6 start Neck Anterior
T11 end Thorax Posterior
T10 hiatus Abdomen Lateral
25 cm length Left deviation Organs
│
─────────────────────────────────────
│
GROSS STRUCTURE
│
Layers → Mucosa
Submucosa
Muscle
Adventitia
│
Constrictions (4)
│
Blood Supply
│
Nerve SupplySUBMAP 3 — Histology Map
ESOPHAGUS HISTOLOGY
│
─────────────────────────────────
│ │ │ │
Mucosa Submucosa Muscle Outer layer
│ │ │ │
Epithelium Glands Upper 1/3 Adventitia
Squamous Proper Skeletal
Non-keratin Cardiac Middle Mixed
Lower Smooth
│
Function
│
Protection
Lubrication
PeristalsisSUBMAP 4 — Development Map
DEVELOPMENT OF ESOPHAGUS
│
─────────────────────────────────
│ │ │
Foregut Septum Growth
Origin Formation Lengthening
│ │ │
Separation of trachea and esophagus
│
─────────────────────────────────
│
DEFECTS
│
TE Fistula
Esophageal Atresia
Feeding difficulty
AspirationSUBMAP 5 — Clinical Integration Map
CLINICAL CONDITIONS
│
─────────────────────────────────
│ │ │ │
Dysphagia GERD Carcinoma Varices
│ │ │ │
Obstruction LES failure Tumor Portal HTN
│ │ │ │
Swallow difficulty Acid reflux Weight loss Bleeding3. PRE-TEST MCQs
Results




#1. At which vertebral level does the esophagus begin?
#2. The esophagus passes through the diaphragm at which vertebral level?
#3. Which structure lies directly anterior to the cervical part of the esophagus?
#4. Which part of the esophagus is crossed anteriorly by the left bronchus?
#5. Which of the following structures is posterior to the thoracic esophagus?
#6. The physiological constriction of the esophagus produced by the arch of aorta occurs at which vertebral level?
#7. Which arterial source supplies the cervical part of the esophagus?
#8. Which artery mainly supplies the abdominal part of the esophagus?
#9. The main parasympathetic nerve supply to the esophagus is provided by which structure?
#10. From which embryological structure does the esophagus develop?
#11. Failure of separation between respiratory and digestive tubes results in which congenital anomaly?
#12. Which epithelial type lines the esophagus?
#13. Where are the esophageal glands proper located?
#14. Which type of muscle is found in the upper third of the esophagus?
#15. Which muscle type predominates in the lower third of the esophagus?
#16. Which of the following represents the most common histological type of esophageal carcinoma in the upper esophagus?
#17. Which histological type of carcinoma most commonly occurs in the lower esophagus?
#18. Which symptom is typically the earliest clinical presentation of esophageal carcinoma?
#19. Which outermost covering is present around most of the esophagus?
#20. Which structure forms the lower physiological constriction of the esophagus?
4. Diagnostic Feedback
Your score in this pre-test reflects your current level of understanding of the topic.
Score 0–7 → Foundational Level
You may not yet be familiar with the basic concepts of connective tissue structure and biochemistry.
Focus on understanding the components of extracellular matrix, collagen structure, glycosaminoglycans, and proteoglycans before attempting more advanced questions.
Score 8–14 → Developing Understanding
You have a partial understanding of connective tissue components and their functions.
Review the relationships between collagen fibers, extracellular matrix proteins, and ground substance, and how these components contribute to tissue strength and elasticity.
Score 15–20 → Strong Conceptual Base
You already have a solid understanding of connective tissue biochemistry and structure.
As you proceed through the learning material, focus on integrating histological structure with biochemical mechanisms and physiological functions.
5. Guided Reasoning
Ask AIM Tutor
I answered this MCQ incorrectly in my MBBS learning module.
Please help me understand:
1. What concept is being tested in this question?
2. Why is the correct option correct?
3. Why are the other options incorrect?
4. What is the key concept I should remember for exams?
Here is the MCQ:
6. Concept Integration
1️⃣ MASTER INTEGRATION CHAIN
Whole Topic Core Flow
Foregut Development
↓
Proper Separation of Trachea & Esophagus
↓
Formation of Muscular Tube (C6 → T11)
↓
Histological Specialization
• Stratified squamous epithelium → Protection
• Submucosal glands → Lubrication
• Muscle layers → Peristalsis
↓
Functional Swallowing (Deglutition)
↓
Safe Transport of Food to Stomach
Failure → Disease → Drug Action
Development Failure
→ Tracheoesophageal fistula
→ Feeding difficulty & aspiration
→ Surgical correction required
Muscle / Nerve Dysfunction
→ Weak peristalsis
→ Dysphagia
→ Prokinetic drugs improve movement
Lower Sphincter Weakness
→ Acid reflux (GERD)
→ Mucosal damage
→ Proton pump inhibitors reduce acid
Chronic Irritation
→ Cellular mutation
→ Esophageal carcinoma
→ Surgical ± chemoradiotherapy
3️⃣ CORE MECHANISM INTEGRATION
Primary Functional Failure — Dysphagia Mechanism
This is the central failure pathway of the esophagus.
Stepwise Mechanism
- Structural narrowing OR muscle dysfunction occurs
Causes:
• Tumor growth
• Stricture formation
• Nerve damage
• Developmental defect
↓ - Peristaltic wave becomes ineffective
Because:
• Muscle contraction weakens
• Lumen narrows
↓ - Food movement becomes delayed
↓ - Bolus accumulates in esophagus
↓ - Clinical Symptoms appear:
• Difficulty swallowing
• Regurgitation
• Weight loss
↓ - Severe cases lead to:
• Malnutrition
• Aspiration
• Dehydration
4️⃣ CLINICAL INTEGRATION SNAPSHOT
These connect:
Disease → Mechanism → Symptom → Treatment
Clinical Flow 1 — GERD Integration
Weak Lower Esophageal Sphincter
↓
Gastric acid reflux into esophagus
↓
Stratified squamous epithelium damaged
↓
Inflammation develops
↓
Symptoms:
• Heartburn
• Chest discomfort
↓
Treatment:
• Proton pump inhibitors
• Lifestyle modification
Clinical Flow 2 — Esophageal Carcinoma Integration
Chronic irritation
(smoking, alcohol, reflux)
↓
Cellular mutation in epithelium
↓
Tumor formation
↓
Lumen narrowing
↓
Symptoms:
• Progressive dysphagia
• Weight loss
↓
Treatment:
• Surgery
• Radiotherapy
Clinical Flow 3 — Tracheoesophageal Fistula Integration
Failure of tracheoesophageal septum
↓
Abnormal connection between trachea and esophagus
↓
Milk enters airway during feeding
↓
Symptoms:
• Choking
• Cyanosis
• Recurrent pneumonia
↓
Treatment:
• Early surgical correction
5️⃣ ULTRA-HIGH-YIELD MASTER SUMMARY
Last-Day Revision Model
This is the final integration memory anchor.
NORMAL FUNCTION
Foregut Development
→ Muscular Tube Formation
→ Protective Epithelium
→ Peristalsis
→ Food Transport
DISEASE MECHANISM
Development Failure
→ TE Fistula
Muscle Failure
→ Dysphagia
Sphincter Failure
→ GERD
Chronic Irritation
→ Carcinoma
DRUG ACTION
Prokinetics
→ Improve peristalsis
Proton Pump Inhibitors
→ Reduce acid injury
Chemotherapy
→ Destroy tumor cells
TREATMENT EFFECT
Restored swallowing
Reduced reflux injury
Tumor control
Improved nutrition
7. KMU Past Papers
MCQ 1
Question:
A foreign body becomes lodged at the level where the esophagus is crossed by the arch of the aorta. This constriction corresponds to which vertebral level?
Options:
A. T2
B. T3
C. T4
D. T5
E. T6
Correct Answer:
C. T4
Explanation:
The second physiological constriction occurs where the aortic arch crosses the esophagus at T4 level.
MCQ 2
Question:
During endoscopy, resistance is felt approximately 15 cm from the incisor teeth. This corresponds to which anatomical structure?
Options:
A. Left bronchial crossing
B. Cricopharyngeal junction
C. Esophageal hiatus
D. Aortic arch crossing
E. Cardiac orifice of stomach
Correct Answer:
B. Cricopharyngeal junction
Explanation:
The first physiological constriction occurs at the cricopharyngeal junction, about 15 cm from incisors.
MCQ 3
Question:
A patient with left atrial enlargement presents with progressive difficulty in swallowing. Which anatomical relationship explains this symptom?
Options:
A. Esophagus lies anterior to left atrium
B. Esophagus lies posterior to left atrium
C. Esophagus lies lateral to left atrium
D. Esophagus lies superior to left atrium
E. Esophagus lies inferior to left atrium
Correct Answer:
B. Esophagus lies posterior to left atrium
Explanation:
The esophagus lies posterior to the left atrium, so atrial enlargement compresses it.
MCQ 4
Question:
Failure of elongation of the esophagus during development may result in which anatomical outcome?
Options:
A. Stomach remaining in thoracic cavity
B. Duodenal atresia formation
C. Meckel diverticulum formation
D. Rotation of stomach failure
E. Formation of accessory spleen
Correct Answer:
A. Stomach remaining in thoracic cavity
Explanation:
Shortening or failure of elongation may cause the stomach to remain partially in the thorax.
MCQ 5
Question:
A carcinoma affecting the lower esophagus is most likely to metastasize through which venous pathway?
Options:
A. Superior vena cava only
B. Portal venous circulation
C. Pulmonary venous system
D. Renal venous drainage
E. Coronary sinus pathway
Correct Answer:
B. Portal venous circulation
Explanation:
Lower esophagus drains into left gastric vein, which connects to portal circulation.
MCQ 6
Question:
Damage to the vagus nerve supplying the esophagus will most directly affect which function?
Options:
A. Mucus production in glands
B. Peristaltic movement of bolus
C. Epithelial cell renewal
D. Blood supply to mucosa
E. Lymphatic drainage
Correct Answer:
B. Peristaltic movement of bolus
Explanation:
Vagus nerve controls motor activity, essential for peristalsis.
MCQ 7
Question:
Which histological feature provides protection against mechanical injury during swallowing?
Options:
A. Simple columnar epithelium
B. Stratified squamous epithelium
C. Transitional epithelium
D. Pseudostratified epithelium
E. Simple cuboidal epithelium
Correct Answer:
B. Stratified squamous epithelium
Explanation:
Multiple layers resist friction from food bolus.
MCQ 8
Question:
Which portion of the esophagus is most likely affected first by disorders involving voluntary swallowing?
Options:
A. Upper third
B. Middle third
C. Lower third
D. Abdominal segment
E. Terminal sphincter region
Correct Answer:
A. Upper third
Explanation:
Upper third contains skeletal muscle, involved in voluntary control.
MCQ 9
Question:
A biopsy from the distal esophagus reveals glandular epithelium replacing squamous lining. This indicates which pathological change?
Options:
A. Dysplasia
B. Metaplasia
C. Hyperplasia
D. Necrosis
E. Hypertrophy
Correct Answer:
B. Metaplasia
Explanation:
Replacement of squamous epithelium by columnar epithelium indicates metaplasia.
MCQ 10
Question:
A tumor compressing the thoracic duct near the esophagus would most likely affect which function?
Options:
A. Oxygen transport
B. Lymph drainage from abdomen
C. Cardiac contraction
D. Pulmonary ventilation
E. Renal filtration
Correct Answer:
B. Lymph drainage from abdomen
Explanation:
Thoracic duct carries lymph from abdomen to venous circulation.
MCQ 11
Question:
Which region of the esophagus contains a mixture of skeletal and smooth muscle fibers?
Options:
A. Cervical region
B. Upper third
C. Middle third
D. Lower third
E. Terminal segment
Correct Answer:
C. Middle third
Explanation:
Middle third contains mixed skeletal and smooth muscle.
MCQ 12
Question:
Which structural feature prevents reflux of gastric contents into the esophagus?
Options:
A. Cricopharyngeus muscle
B. Lower esophageal sphincter
C. Submucosal glands
D. Thoracic duct
E. Longitudinal muscle fibers
Correct Answer:
B. Lower esophageal sphincter
Explanation:
LES maintains pressure preventing reflux.
MCQ 13
Question:
Which congenital defect results from persistence of communication between foregut and respiratory diverticulum?
Options:
A. Esophageal varices
B. Tracheoesophageal fistula
C. Pyloric stenosis
D. Umbilical hernia
E. Intestinal malrotation
Correct Answer:
B. Tracheoesophageal fistula
Explanation:
Failure of separation leads to abnormal communication.
MCQ 14
Question:
Which artery is most responsible for supplying the thoracic portion of the esophagus?
Options:
A. Inferior thyroid artery
B. Internal thoracic artery
C. Thoracic aorta branches
D. Common carotid artery
E. Superior mesenteric artery
Correct Answer:
C. Thoracic aorta branches
Explanation:
Thoracic esophagus receives esophageal branches from thoracic aorta.
MCQ 15
Question:
Which structural change most directly explains dysphagia in esophageal carcinoma?
Options:
A. Increased gland secretion
B. Narrowing of lumen
C. Increased muscle contraction
D. Reduced vascular supply
E. Enhanced epithelial renewal
Correct Answer:
B. Narrowing of lumen
Explanation:
Tumor growth narrows lumen, obstructing food passage.
MCQ 16
Question:
Which histological structure facilitates lubrication during swallowing?
Options:
A. Muscularis externa
B. Lamina propria
C. Submucosal glands
D. Adventitial tissue
E. Serosal covering
Correct Answer:
C. Submucosal glands
Explanation:
These glands secrete mucus that lubricates lumen.
MCQ 17
Question:
Which physiological mechanism moves the food bolus through the esophagus?
Options:
A. Diffusion
B. Osmosis
C. Filtration
D. Peristalsis
E. Passive flow
Correct Answer:
D. Peristalsis
Explanation:
Sequential muscle contractions propel bolus.
MCQ 18
Question:
Which anatomical feature contributes most to the structural rigidity of the esophageal wall?
Options:
A. Mucosal folds
B. Circular muscle fibers
C. Stratified epithelium
D. Adventitial tissue
E. Submucosal connective tissue
Correct Answer:
E. Submucosal connective tissue
Explanation:
Dense connective tissue supports wall integrity.
MCQ 19
Question:
Which factor most strongly predisposes to adenocarcinoma of the distal esophagus?
Options:
A. Chronic tobacco use
B. Persistent alcohol intake
C. Long-standing acid reflux
D. Vitamin deficiency
E. Chronic dehydration
Correct Answer:
C. Long-standing acid reflux
Explanation:
Chronic reflux leads to Barrett esophagus and adenocarcinoma.
MCQ 20
Question:
Which anatomical change explains regurgitation in patients with lower esophageal sphincter dysfunction?
Options:
A. Increased peristaltic pressure
B. Failure of sphincter closure
C. Reduced gland secretion
D. Thickening of mucosa
E. Compression by diaphragm
Correct Answer:
B. Failure of sphincter closure
Explanation:
LES incompetence allows backward flow of gastric contents.
8. Post-Test
Post Test MCQs
9. Explanation of Incorrect Answers
Incorrect answers are valuable learning opportunities. When reviewing MCQs, focus on understanding the concept behind the question, not just memorizing the correct option.
If you answered a question incorrectly:
• Identify the concept being tested.
• Determine why the correct option is correct.
• Understand why the other options are incorrect.
You can paste the MCQ into the AIM Tutor and ask for a step-by-step explanation. This helps strengthen conceptual understanding and improves reasoning for future questions.
Learning Tip
If your Post-Test score is below 80%, review the key concepts and attempt the Post-Test again to reinforce your understanding.
10. Student Memory Support
1️⃣High-Yield Flashcards
Flashcard 1
Q: At which vertebral level does the esophagus begin?
A: Lower border of C6 vertebra.
Flashcard 2
Q: At which vertebral level does the esophagus pass through the diaphragm?
A: T10 vertebral level.
Flashcard 3
Q: At which vertebral level does the esophagus end?
A: T11 vertebral level.
Flashcard 4
Q: What type of epithelium lines the esophagus?
A: Stratified squamous non-keratinized epithelium.
Flashcard 5
Q: Which muscle type is present in the upper third of the esophagus?
A: Skeletal muscle.
Flashcard 6
Q: Which muscle type predominates in the lower third of the esophagus?
A: Smooth muscle.
Flashcard 7
Q: From which embryological structure does the esophagus develop?
A: Foregut.
Flashcard 8
Q: What congenital defect results from failure of tracheoesophageal separation?
A: Tracheoesophageal fistula.
Flashcard 9
Q: Where are esophageal glands proper located?
A: Submucosal layer.
Flashcard 10
Q: What is the most common early symptom of esophageal carcinoma?
A: Progressive dysphagia.
Flashcard 11
Q: What is the outer covering of most of the esophagus?
A: Adventitia.
Flashcard 12
Q: Which artery mainly supplies the cervical part of the esophagus?
A: Inferior thyroid artery.
Flashcard 13
Q: Which histological type of carcinoma commonly occurs in upper esophagus?
A: Squamous cell carcinoma.
Flashcard 14
Q: Which histological type commonly affects the lower esophagus?
A: Adenocarcinoma.
2️⃣Mnemonics
Mnemonic Title: Esophageal Constrictions
Mnemonic Word:
“CABD”
Meaning:
C → Cricoid cartilage (C6)
A → Aortic arch (T4)
B → Bronchus (T5)
D → Diaphragm (T10)
Mnemonic Title: Muscle Type Distribution
Mnemonic Word:
“SSM”
Meaning:
S → Skeletal (Upper third)
S → Skeletal + Smooth (Middle third)
M → Smooth (Lower third)
Mnemonic Title: Arterial Supply Segments
Mnemonic Word:
“ITL”
Meaning:
I → Inferior thyroid artery (Cervical)
T → Thoracic aorta branches (Thoracic)
L → Left gastric artery (Abdominal)
3️⃣Memory Tables
Table 1 — Muscle Distribution in Esophagus
| Region | Muscle Type | Functional Control |
| Upper third | Skeletal muscle | Voluntary |
| Middle third | Mixed muscle | Mixed control |
| Lower third | Smooth muscle | Involuntary |
Table 2 — Types of Esophageal Carcinoma
| Type | Common Location | Key Risk |
| Squamous cell carcinoma | Upper & middle | Smoking, alcohol |
| Adenocarcinoma | Lower esophagus | GERD, Barrett esophagus |
4️⃣Rapid Revision Points (Last-Minute)
Must Remember:
• Esophagus extends from C6 to T11
• Passes diaphragm at T10
• Length approximately 25 cm
• Four physiological constrictions present
• Lined by stratified squamous epithelium
• Submucosal glands secrete mucus
• Upper third contains skeletal muscle
• Lower third contains smooth muscle
• Develops from foregut
• Failure of septum → TE fistula
• Progressive dysphagia → warning sign of carcinoma
• Most of esophagus covered by adventitia
5️⃣Clinical Memory Hooks
Clinical Hook 1:
Foreign body lodgment → Physiological constrictions
Clinical Hook 2:
Left atrial enlargement → Compression of esophagus → Dysphagia
Clinical Hook 3:
GERD → Lower esophageal damage → Adenocarcinoma risk
Clinical Hook 4:
Newborn choking during feeding → Tracheoesophageal fistula
Clinical Hook 5:
Progressive dysphagia + weight loss → Esophageal carcinoma
✔ Topic Completion
📊 Your Performance
Pre-Test: Not Attempted
Post-Test: Not Attempted
Improvement: --