
This topic uses the AIM Learning Cycle to help MBBS students understand gastrointestinal motility and swallowing mechanisms by integrating Physiology and Clinical concepts.
1. Curriculum Coverage
Physiology
• Electrical activity of gastrointestinal smooth muscle
• Mechanism of excitation of smooth muscle
• Slow waves and spike potentials
• Mesenteric plexus
• Submucosal plexus
• Enteric neurotransmitters
• Autonomic nervous system regulation
• Sympathetic and parasympathetic modulation
• Gastrointestinal reflexes
• Gastrointestinal hormones
• Functional types of gastrointestinal movements
• Law of gut
• Blood flow through villus
• Splanchnic circulation
• Effect of metabolic activity on blood flow
• Nervous control of gastrointestinal blood flow
Swallowing Physiology
• Mechanics of ingestion
• Chewing and mastication
• Stages of swallowing
• Effects of pharyngeal stage on respiration
- Basic mechanisms of stimulation of alimentary tract glands
- Dual effect of sympathetic stimulation on alimentary gland secretion
- Anatomy of gastrointestinal blood supply
📚 Standard Reference Framework
Primary Anatomy Reference:
BD Chaurasia — Standard Undergraduate Depth
Concept Support:
Gray’s Anatomy for Students
Spatial Atlas:
Netter Atlas
Physiology:
Guyton & Hall
Histology:
DiFiore Atlas
Biochemistry:
Lippincott Illustrated Reviews
🎯 Depth Policy
All content is restricted to Undergraduate MBBS Level.
Depth will not exceed BD Chaurasia standard
2. Learning Material
Gastrointestinal (GI) smooth muscle shows spontaneous rhythmic electrical activity, which is essential for motility.
Types of Electrical Activity
A. Slow Waves (Basic Electrical Rhythm — BER)
Definition:
Slow waves are rhythmic oscillations in membrane potential that determine the basic rhythm of GI motility.
Key Features
- Not true action potentials
- Generated by Interstitial Cells of Cajal (pacemaker cells)
- Determine frequency of contractions
- Do not cause contraction alone
Frequency of Slow Waves
Organ Frequency
Stomach 3/min
Duodenum 12/min
Ileum 8–9/min
Clinical Correlation
Damage to pacemaker cells results in: - Gastroparesis
- Motility disorders
- Functional dyspepsia
B. Spike Potentials
Spike potentials are true action potentials that occur when slow waves reach threshold.
Features
- Responsible for muscle contraction
- Associated with calcium entry
- Increased by stretch and parasympathetic activity
Clinical Correlation
Excess spike activity → - Diarrhea
- Intestinal spasm
Reduced spike activity → - Ileus
- Constipation
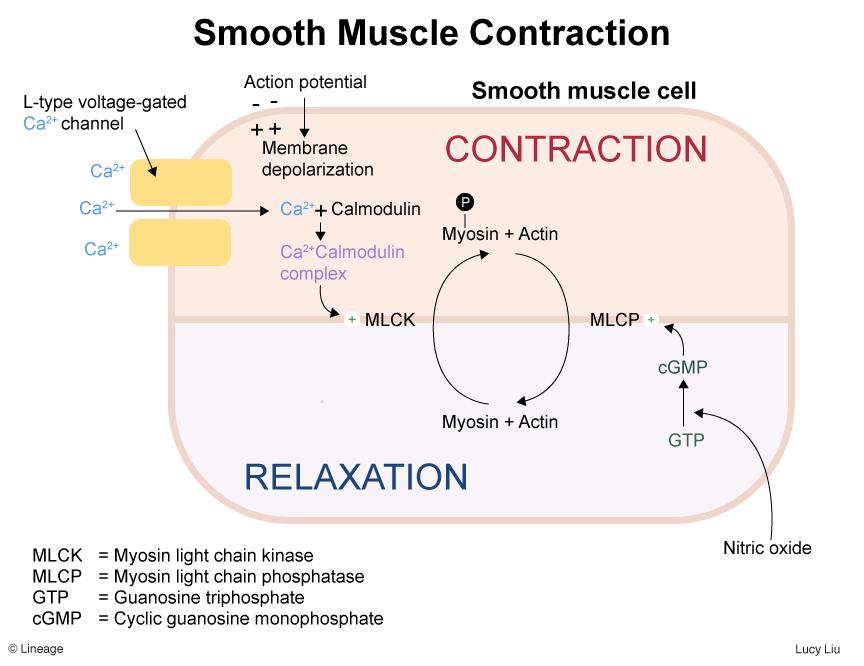
Smooth muscle contraction depends mainly on calcium ion entry.
Mechanism
- Membrane depolarization
- Calcium channels open
- Calcium enters cell
- Calcium binds calmodulin
- Activates myosin light chain kinase (MLCK)
- Contraction occurs
Clinical Correlation
Calcium channel blockers may reduce:
- GI motility
- Smooth muscle tone
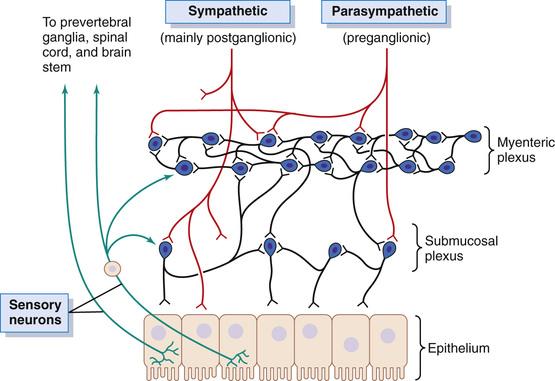
The ENS is known as the “brain of the gut.”
It operates independently but is modified by the autonomic nervous system.
Two Major Plexuses
A. Myenteric Plexus (Auerbach’s Plexus)
Location:
Between longitudinal and circular muscle layers.
Functions
- Controls motility
- Regulates tone
- Coordinates peristalsis
- Controls rate of contraction
Clinical Correlation
Damage leads to: - Achalasia
- Hirschsprung disease
B. Submucosal Plexus (Meissner’s Plexus)
Location:
Within submucosa.
Functions
- Controls secretion
- Regulates absorption
- Local blood flow control
Important neurotransmitters regulate contraction and relaxation.
Excitatory Neurotransmitters
- Acetylcholine
- Substance P
Cause: - Muscle contraction
- Increased secretion
Inhibitory Neurotransmitters - Nitric oxide (NO)
- Vasoactive intestinal peptide (VIP)
Cause: - Muscle relaxation
- Reduced motility
Clinical Correlation
Loss of inhibitory neurons → - Achalasia
- Autonomic Nervous System Regulation
The ENS is influenced by sympathetic and parasympathetic systems.
Parasympathetic System
Origin
- Vagus nerve
- Pelvic nerves
Effects - Increases motility
- Increases secretion
- Relaxes sphincters
Sympathetic System
Origin
- Thoracolumbar spinal cord
Effects - Decreases motility
- Decreases secretion
- Contracts sphincters
GI reflexes regulate coordinated digestion.
Types of Reflexes
Short Reflexes
- Within enteric system
- Local control
Example: - Peristaltic reflex
Long Reflexes
- Involve CNS
Examples: - Gastrocolic reflex
- Enterogastric reflex
Hormones regulate digestion and motility.
Major Hormones
Gastrin
Source:
- G cells (stomach)
Functions: - Increases gastric secretion
- Increases motility
Secretin
Source:
- Duodenum
Functions: - Inhibits gastric motility
- Stimulates pancreatic secretion
Cholecystokinin (CCK)
Source:
- Duodenum
Functions: - Gallbladder contraction
- Pancreatic enzyme secretion
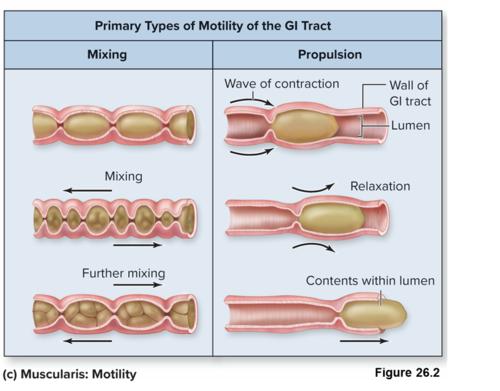
A. Propulsive Movements (Peristalsis)
Move contents forward.
Mechanism
- Contraction behind bolus
- Relaxation ahead of bolus
This mechanism follows:
Law of the Gut
Definition:
“Contraction above and relaxation below the bolus ensures forward movement.”
Clinical Correlation
Failure causes: - Intestinal obstruction symptoms
- Severe constipation
B. Mixing Movements
Help digestion and absorption.
Examples:
- Segmentation contractions
- Pendular movements
GI blood flow increases during digestion.
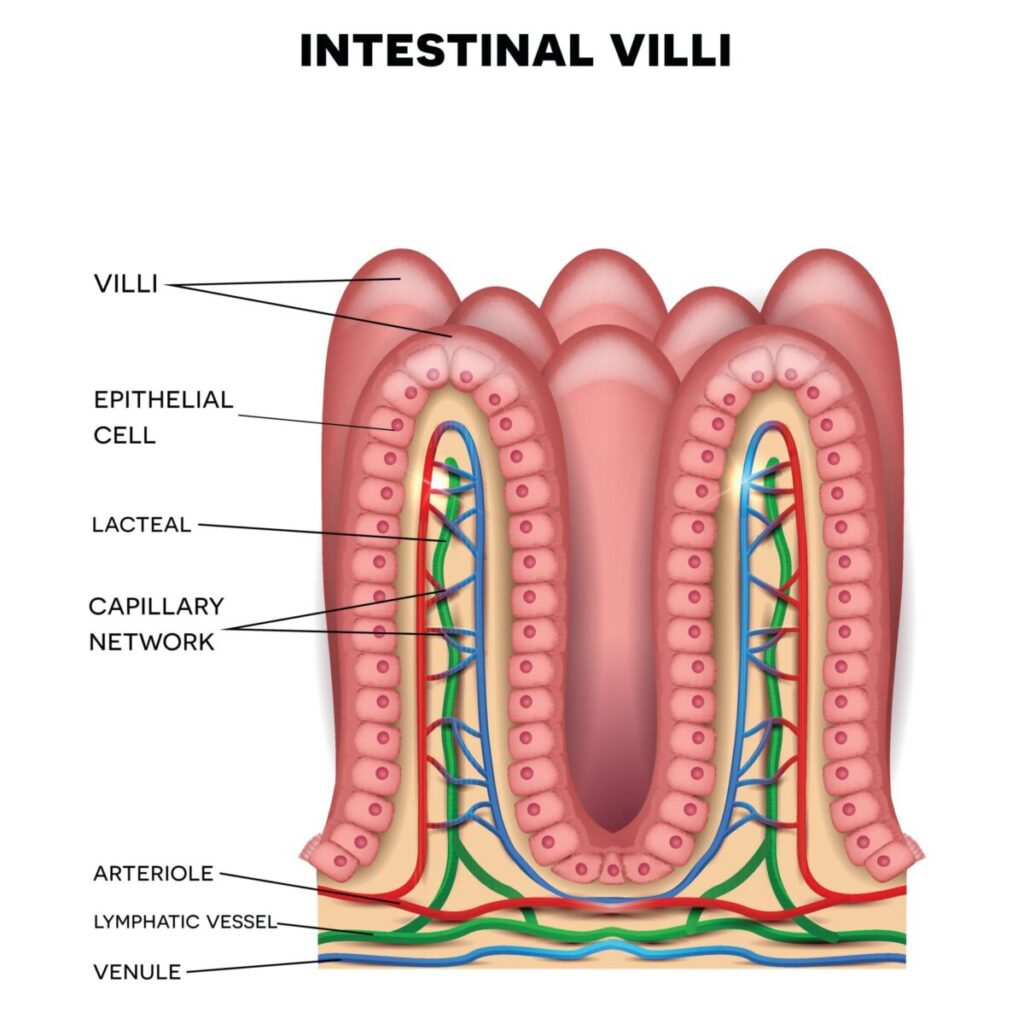
Blood Flow Through Villus
Villus contains:
- Arteriole
- Capillary network
- Venule
Special Feature
Countercurrent exchange occurs between arteriole and venule.
Clinical Correlation
Reduced blood flow → - Ischemic bowel
Splanchnic Circulation
Includes blood supply to:
- Stomach
- Intestines
- Liver
- Pancreas
- Spleen
Major Arteries - Celiac trunk
- Superior mesenteric artery
- Inferior mesenteric artery
Effect of Metabolic Activity on Blood Flow
Increased digestion →
- Increased metabolic activity
- Vasodilation
- Increased blood supply
Nervous Control of GI Blood Flow
Parasympathetic:
- Increases blood flow
Sympathetic: - Causes vasoconstriction
Swallowing is a coordinated reflex involving voluntary and involuntary phases.
Mechanics of Ingestion
Includes:
- Chewing
- Mastication
- Formation of bolus
Chewing and Mastication
Functions
- Break food into small particles
- Increase surface area
- Mix with saliva
Control - Controlled by reflex and voluntary action
Stages of Swallowing
There are three stages:
- Oral Stage (Voluntary)
Food is pushed to pharynx.
Muscles:
- Tongue
- Buccal muscles
- Pharyngeal Stage (Involuntary)
Important protective stage.
Events:
- Soft palate closes nasal cavity
- Epiglottis closes airway
- Vocal cords close
- Respiration temporarily stops
Clinical Correlation
Failure leads to: - Aspiration pneumonia
- Esophageal Stage (Involuntary)
Bolus moves to stomach by peristalsis.
Effect of Pharyngeal Stage on Respiration
During swallowing:
- Respiration stops briefly
- Known as deglutition apnea
Prevents: - Aspiration
Secretion depends on:
- Neural stimulation
- Hormonal stimulation
- Mechanical stimulation
Dual Effect of Sympathetic Stimulation
Sympathetic stimulation:
Short-term:
- Slight secretion
Long-term: - Reduced secretion due to vasoconstriction
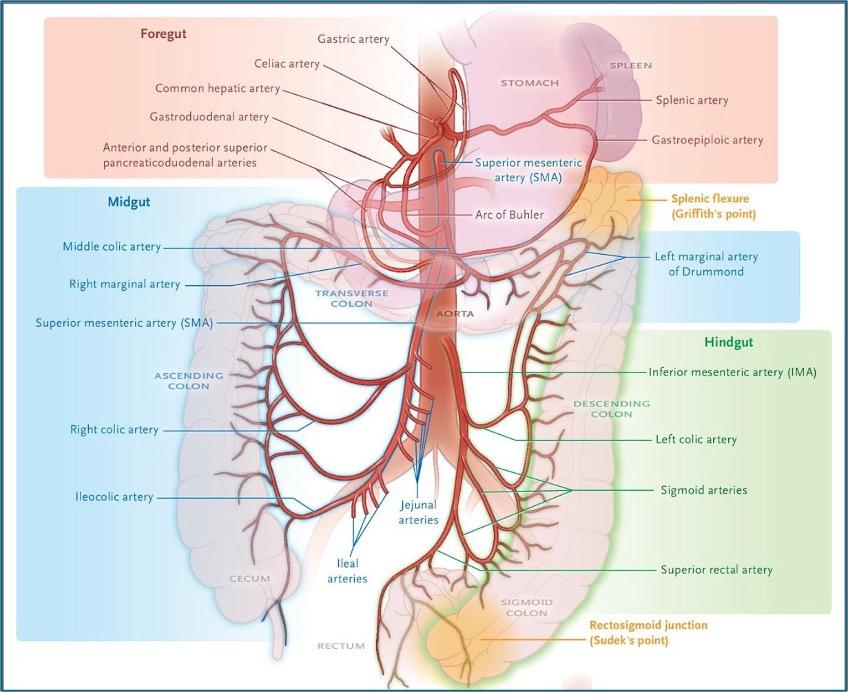
Foregut Blood Supply
Supplied by:
Celiac Trunk
Major Branches
- Left gastric artery
- Common hepatic artery
- Splenic artery
Foregut Organs - Lower esophagus
- Stomach
- Proximal duodenum
- Liver
- Pancreas
- Spleen
Midgut Blood Supply
Supplied by:
Superior Mesenteric Artery (SMA)
Midgut Organs
- Distal duodenum
- Jejunum
- Ileum
- Cecum
- Ascending colon
- Proximal two-thirds of transverse colon
Hindgut Blood Supply
Supplied by:
Inferior Mesenteric Artery (IMA)
Hindgut Organs
- Distal one-third of transverse colon
- Descending colon
- Sigmoid colon
- Rectum (upper part)
Clinical Correlation — Mesenteric Ischemia
Occurs due to:
- Reduced blood supply
- Arterial blockage
Common symptoms: - Severe abdominal pain
- Postprandial pain
- Weight loss
Important clinical connections include:
- Achalasia → Loss of inhibitory neurons
- Hirschsprung disease → Absence of enteric ganglia
- Ileus → Reduced motility
- Dysphagia → Swallowing dysfunction
- Aspiration pneumonia → Failure of airway protection
- Mesenteric ischemia → Reduced splanchnic circulation
MASTER CONCEPT MAP:Topic 4 — Gastrointestinal Motility, Swallowing & Neural Regulation
GASTROINTESTINAL FUNCTION
│
────────────────────┼────────────────────
│
GASTROINTESTINAL MOTILITY
│
───────────────┬─────────┬─────────┬─────────
│ │ │
Electrical Neural Blood Flow
Activity Regulation & Circulation
│ │ │
Slow Waves Enteric NS Splanchnic
Spike Pot. Autonomic NS Villus Flow
│ │
└─────────┴─────────
│
PERISTALSIS
(Law of Gut)
│
SWALLOWING
│
────────────┬────────────┬────────────
│ │
Oral Stage Pharyngeal Esophageal
Stage Stage🧩 SUBMAP 1 — Electrical Activity of GI Smooth Muscle
ELECTRICAL ACTIVITY
│
─────────┼─────────
│
Slow Waves
│
Generated by:
Interstitial Cells of Cajal
│
Set rhythm of contractions
│
↓
Spike Potentials
│
True Action Potentials
│
Calcium Entry → Contraction🧩 SUBMAP 2 — Enteric Nervous System Regulation
ENTERIC NERVOUS SYSTEM
│
───────────────┼──────────────
│
Myenteric Plexus
(Auerbach)
│
Controls Motility
Controls Peristalsis
│
Submucosal Plexus
(Meissner)
│
Controls Secretion
Controls Blood Flow
│
Autonomic Control
───────────┬───────────
│
Parasympathetic
↑ Motility
↑ Secretion
Sympathetic
↓ Motility
Vasoconstriction🧩 SUBMAP 4 — Swallowing Mechanism
SWALLOWING
│
─────────────┼─────────────
│
ORAL STAGE
(Voluntary)
│
↓
PHARYNGEAL STAGE
(Involuntary)
│
Airway Protection Occurs
Respiration Stops Briefly
(Deglutition Apnea)
│
↓
ESOPHAGEAL STAGE
(Peristalsis)
│
Bolus → StomachRecommended Video
3. PRE-TEST MCQs
Results




#1. The rhythmic electrical activity that determines the maximum frequency of gastrointestinal contractions is known as:
#2. Which cells act as pacemaker cells in the gastrointestinal tract?
#3. Smooth muscle contraction in the gastrointestinal tract is mainly triggered by entry of which ion?
#4. The plexus primarily responsible for coordinating gastrointestinal motility is located between muscle layers known as:
#5. Which plexus mainly regulates secretion and local blood flow in the intestinal wall?
#6. Nitric oxide released in the gastrointestinal tract primarily produces:
#7. Activation of the parasympathetic nervous system generally results in which effect on gastrointestinal activity?
#8. Which nervous system division causes contraction of gastrointestinal sphincters?
#9. The reflex that moves intestinal contents forward through coordinated contraction and relaxation is called:
#10. The principle stating contraction above and relaxation below a bolus is known as:
#11. Mixing movements in the small intestine mainly serve to:
#12. Which gastrointestinal hormone stimulates contraction of the gallbladder?
#13. Blood flow through intestinal villi is characterized by which structural arrangement?
#14. An increase in digestive activity produces which effect on intestinal blood flow?
#15. The stage of swallowing during which breathing temporarily stops is:
#16. Which structure prevents food from entering the airway during swallowing?
#17. Chewing facilitates digestion primarily by:
#18. The artery supplying most midgut structures is the:
#19. Sympathetic stimulation of alimentary glands over prolonged periods leads to:
#20. Which factor most directly increases gastrointestinal blood flow during digestion?
4. Diagnostic Feedback
Your score in this pre-test reflects your current level of understanding of the topic.
Score 0–7 → Foundational Level
You may not yet be familiar with the basic concepts of connective tissue structure and biochemistry.
Focus on understanding the components of extracellular matrix, collagen structure, glycosaminoglycans, and proteoglycans before attempting more advanced questions.
Score 8–14 → Developing Understanding
You have a partial understanding of connective tissue components and their functions.
Review the relationships between collagen fibers, extracellular matrix proteins, and ground substance, and how these components contribute to tissue strength and elasticity.
Score 15–20 → Strong Conceptual Base
You already have a solid understanding of connective tissue biochemistry and structure.
As you proceed through the learning material, focus on integrating histological structure with biochemical mechanisms and physiological functions.
6. Concept Integration
1️⃣ MASTER INTEGRATION CHAIN
Whole Topic Core Flow (Normal Function → Failure → Drug Action)
Food Intake
→ Chewing (Mechanical Breakdown — Cranial Nerves, Muscles)
→ Swallowing Reflex Activation (Pharyngeal Coordination + Temporary Respiratory Inhibition)
→ Esophageal Peristalsis Initiated (Law of Gut — ENS Driven)
→ Slow Waves Generated (Interstitial Cells of Cajal — Electrical Rhythm)
→ Spike Potentials Trigger Contraction (Calcium Entry into Smooth Muscle)
→ Enteric Nervous System Coordinates Motility (Myenteric Plexus)
→ Submucosal Plexus Controls Secretion & Blood Flow
→ Autonomic Nervous System Modulates Activity
(Parasympathetic ↑ Motility | Sympathetic ↓ Motility)
→ Gastrointestinal Hormones Modify Activity
(Gastrin ↑ Motility | Secretin ↓ Motility | CCK Supports Digestion)
→ Peristalsis Moves Bolus Forward (Law of Gut)
→ Metabolic Activity Increases Blood Flow (Splanchnic Vasodilation)
→ Villus Perfusion Supports Absorption
Failure Points
- Loss of inhibitory neurons → Achalasia
- Absence of ganglion cells → Hirschsprung disease
- Reduced neural activity → Paralytic ileus
- Failed airway protection → Aspiration pneumonia
- Reduced blood flow → Mesenteric ischemia
Drug Action Sites
- Calcium channel blockers → Reduce smooth muscle contraction
- Anticholinergic drugs → Reduce motility & secretion
- Prokinetic drugs → Enhance peristalsis
- Vasodilators → Improve splanchnic circulation
3️⃣ CORE MECHANISM INTEGRATION
Primary Functional Breakdown Mechanism
Motility Failure Mechanism
Reduced Neural or Electrical Activity
→ Reduced Slow Wave Effectiveness
→ Fewer Spike Potentials
→ Reduced Calcium Entry
→ Weak Smooth Muscle Contraction
→ Ineffective Peristalsis
→ Delayed Movement of Intestinal Contents
→ Accumulation of Contents
→ Functional Obstruction Symptoms
→ Abdominal Distension & Constipation
Integrated Subjects
Physiology → Electrical activity & contraction
Anatomy → Plexus integrity
Clinical Medicine → Ileus symptoms
Pharmacology → Prokinetic drug targets
4️⃣ CLINICAL INTEGRATION SNAPSHOT
Clinical Flow 1 — Achalasia
Loss of Inhibitory Neurons (Nitric Oxide Deficiency)
→ Failure of Esophageal Relaxation
→ Impaired Bolus Passage
→ Dysphagia & Food Retention
→ Treatment: Drugs Enhancing Relaxation or Mechanical Dilation
Clinical Flow 2 — Hirschsprung Disease
Congenital Absence of Enteric Ganglia
→ No Peristalsis in Affected Segment
→ Functional Obstruction
→ Severe Constipation & Abdominal Distension
→ Treatment: Surgical Removal of Affected Segment
Clinical Flow 3 — Mesenteric Ischemia
Reduced Blood Flow in Splanchnic Circulation
→ Reduced Oxygen Delivery to Intestinal Tissue
→ Tissue Injury
→ Severe Abdominal Pain After Meals
→ Treatment: Restoration of Blood Flow
5️⃣ ULTRA-HIGH-YIELD MASTER SUMMARY
Last-Day Rapid Integration Model
NORMAL FUNCTION
Slow Waves
→ Spike Potentials
→ Calcium Entry
→ Smooth Muscle Contraction
→ Coordinated Peristalsis
→ Adequate Blood Flow
→ Efficient Digestion & Absorption
DISEASE MECHANISM
Neural Damage / Reduced Blood Flow
→ Weak or Absent Peristalsis
→ Delayed Movement
→ Accumulation of Contents
→ Clinical Symptoms
Examples:
- Dysphagia
- Constipation
- Abdominal Pain
- Aspiration
DRUG ACTION
Prokinetics → Increase Motility
Anticholinergics → Reduce Excess Motility
Vasodilators → Improve Blood Flow
TREATMENT EFFECT
Restored Neural Activity
→ Improved Motility
→ Normal Bolus Movement
→ Symptom Relief
MCQ 1
Question:
A patient presents with failure of relaxation of the lower esophageal sphincter due to loss of inhibitory neurons. Which neurotransmitter deficiency is most likely responsible?
Options:
A. Acetylcholine
B. Substance P
C. Nitric oxide
D. Serotonin
E. Histamine
Correct Answer:
C. Nitric oxide
Explanation:
Nitric oxide mediates smooth muscle relaxation; its deficiency leads to failure of sphincter relaxation in achalasia.
MCQ 2
Question:
An increase in intracellular calcium in gastrointestinal smooth muscle primarily activates which enzyme responsible for contraction?
Options:
A. Myosin light chain kinase
B. Adenylate cyclase
C. Protein kinase A
D. Sodium-potassium ATPase
E. Phosphodiesterase
Correct Answer:
A. Myosin light chain kinase
Explanation:
Calcium binds calmodulin, activating MLCK, which initiates actin–myosin interaction.
MCQ 3
Question:
A neonate presents with severe constipation and abdominal distension. Histology reveals absence of ganglion cells in distal colon. Which plexus is primarily affected?
Options:
A. Celiac plexus
B. Submucosal plexus
C. Myenteric plexus
D. Cardiac plexus
E. Solar plexus
Correct Answer:
C. Myenteric plexus
Explanation:
Hirschsprung disease involves absence of enteric ganglia, especially affecting the myenteric plexus responsible for peristalsis.
MCQ 4
Question:
A rise in digestive activity increases intestinal blood flow primarily due to which local factor?
Options:
A. Reduced metabolic demand
B. Increased tissue oxygen availability
C. Accumulation of vasodilator metabolites
D. Activation of sympathetic nerves
E. Decreased nutrient absorption
Correct Answer:
C. Accumulation of vasodilator metabolites
Explanation:
Local metabolic products cause vasodilation, increasing blood flow during digestion.
MCQ 5
Question:
A lesion affecting the vagus nerve would most likely result in which change in gastrointestinal function?
Options:
A. Increased peristaltic activity
B. Decreased gastric secretion
C. Reduced sphincter tone
D. Increased digestive hormone release
E. Enhanced intestinal mixing
Correct Answer:
B. Decreased gastric secretion
Explanation:
Parasympathetic vagal stimulation enhances secretion; its loss reduces gastric activity.
MCQ 6
Question:
Failure of coordinated contraction above and relaxation below intestinal contents would impair which physiological principle?
Options:
A. Segmentation
B. Mass movement
C. Migrating motor complex
D. Peristaltic reflex
E. Haustral contraction
Correct Answer:
D. Peristaltic reflex
Explanation:
The peristaltic reflex follows the law of the gut to move contents forward.
MCQ 7
Question:
During swallowing, temporary cessation of breathing occurs primarily to prevent entry of food into which structure?
Options:
A. Nasopharynx
B. Larynx
C. Trachea
D. Esophagus
E. Bronchi
Correct Answer:
C. Trachea
Explanation:
Deglutition apnea protects the airway from aspiration.
MCQ 8
Question:
Which structure is primarily responsible for initiating the rhythmic electrical activity in gastrointestinal smooth muscle?
Options:
A. Enterochromaffin cells
B. Goblet cells
C. Interstitial cells of Cajal
D. Paneth cells
E. Kupffer cells
Correct Answer:
C. Interstitial cells of Cajal
Explanation:
These pacemaker cells generate slow waves controlling contraction rhythm.
MCQ 9
Question:
An increase in sympathetic discharge to gastrointestinal glands over prolonged duration results in which outcome?
Options:
A. Enhanced enzyme release
B. Increased mucosal hydration
C. Reduced secretion due to vasoconstriction
D. Increased mucus formation
E. Enhanced nutrient absorption
Correct Answer:
C. Reduced secretion due to vasoconstriction
Explanation:
Sympathetic vasoconstriction reduces glandular blood supply and secretion.
MCQ 10
Question:
Which arterial supply is primarily responsible for perfusion of the jejunum?
Options:
A. Inferior mesenteric artery
B. Celiac trunk
C. Internal iliac artery
D. Superior mesenteric artery
E. Renal artery
Correct Answer:
D. Superior mesenteric artery
Explanation:
The jejunum is a midgut structure supplied by the superior mesenteric artery.
MCQ 11
Question:
Increased segmentation movements in the intestine would most likely enhance which physiological process?
Options:
A. Rapid propulsion of contents
B. Mechanical mixing with enzymes
C. Rapid gastric emptying
D. Expulsion of fecal matter
E. Closure of intestinal sphincters
Correct Answer:
B. Mechanical mixing with enzymes
Explanation:
Segmentation promotes mixing and improves digestion and absorption.
MCQ 12
Question:
A decrease in inhibitory neurotransmission in the esophagus would most likely produce which functional change?
Options:
A. Increased relaxation of smooth muscle
B. Reduced muscular tone
C. Persistent sphincter contraction
D. Reduced peristaltic activity
E. Increased gastric secretion
Correct Answer:
C. Persistent sphincter contraction
Explanation:
Loss of inhibitory signals prevents relaxation of sphincters.
MCQ 13
Question:
Which physiological mechanism primarily explains oxygen exchange between vessels within intestinal villi?
Options:
A. Turbulent circulation
B. Portal shunting
C. Countercurrent exchange
D. Diffusion limitation
E. Laminar perfusion
Correct Answer:
C. Countercurrent exchange
Explanation:
Close proximity of arteriole and venule allows countercurrent oxygen exchange.
MCQ 14
Question:
Damage to the submucosal plexus would most significantly impair which function?
Options:
A. Coordination of peristalsis
B. Regulation of glandular secretion
C. Initiation of slow waves
D. Activation of skeletal muscles
E. Closure of pyloric sphincter
Correct Answer:
B. Regulation of glandular secretion
Explanation:
The submucosal plexus regulates secretion and local blood flow.
MCQ 15
Question:
During swallowing, closure of the nasopharynx occurs due to elevation of which structure?
Options:
A. Tongue
B. Epiglottis
C. Soft palate
D. Vocal cords
E. Larynx
Correct Answer:
C. Soft palate
Explanation:
Elevation of the soft palate prevents food entering nasal passages.
MCQ 16
Question:
Which mechanism explains the increase in gastrointestinal blood flow following food intake?
Options:
A. Reduced neural stimulation
B. Activation of local vasodilator metabolites
C. Decreased smooth muscle tone
D. Increased venous resistance
E. Closure of precapillary sphincters
Correct Answer:
B. Activation of local vasodilator metabolites
Explanation:
Metabolic products cause vasodilation during digestion.
MCQ 17
Question:
A patient develops aspiration pneumonia following neurological injury. Failure of which stage of swallowing is most likely responsible?
Options:
A. Oral stage
B. Preparatory stage
C. Gastric stage
D. Pharyngeal stage
E. Intestinal stage
Correct Answer:
D. Pharyngeal stage
Explanation:
The pharyngeal stage protects the airway; its failure leads to aspiration.
MCQ 18
Question:
Which hormone primarily stimulates pancreatic enzyme secretion in response to fatty meals?
Options:
A. Secretin
B. Gastrin
C. Cholecystokinin
D. Motilin
E. Somatostatin
Correct Answer:
C. Cholecystokinin
Explanation:
CCK stimulates pancreatic enzyme release and gallbladder contraction.
MCQ 19
Question:
Which physiological property allows intestinal smooth muscle to maintain tone without continuous neural input?
Options:
A. Refractory activity
B. Intrinsic rhythmicity
C. Passive elasticity
D. Synaptic fatigue
E. Ion diffusion
Correct Answer:
B. Intrinsic rhythmicity
Explanation:
Slow waves provide intrinsic rhythmic contraction ability.
MCQ 20
Question:
Loss of enteric ganglia affecting distal colon would most likely produce which functional abnormality?
Options:
A. Increased intestinal motility
B. Reduced sphincter tone
C. Enhanced nutrient absorption
D. Failure of propulsive movement
E. Increased mucus secretion
Correct Answer:
D. Failure of propulsive movement
Explanation:
Absence of ganglia prevents coordinated peristalsis, causing functional obstruction.
8. Post-Test
Post Test
9. Explanation of Incorrect Answers
Incorrect answers are valuable learning opportunities. When reviewing MCQs, focus on understanding the concept behind the question, not just memorizing the correct option.
If you answered a question incorrectly:
• Identify the concept being tested.
• Determine why the correct option is correct.
• Understand why the other options are incorrect.
You can paste the MCQ into the AIM Tutor and ask for a step-by-step explanation. This helps strengthen conceptual understanding and improves reasoning for future questions.
Learning Tip
If your Post-Test score is below 80%, review the key concepts and attempt the Post-Test again to reinforce your understanding.
10. Student Memory Support
1️⃣High-Yield Flashcards
Flashcard 1
Q: What cells generate slow waves in the gastrointestinal tract?
A: Interstitial cells of Cajal
Flashcard 2
Q: Which ion is most important for gastrointestinal smooth muscle contraction?
A: Calcium (Ca²⁺)
Flashcard 3
Q: Which plexus controls gastrointestinal motility?
A: Myenteric (Auerbach’s) plexus
Flashcard 4
Q: Which plexus regulates secretion and local blood flow?
A: Submucosal (Meissner’s) plexus
Flashcard 5
Q: What is the Law of the Gut?
A: Contraction above and relaxation below the bolus
Flashcard 6
Q: Which neurotransmitter causes smooth muscle relaxation in the gut?
A: Nitric oxide (NO)
Flashcard 7
Q: Which stage of swallowing stops respiration temporarily?
A: Pharyngeal stage
Flashcard 8
Q: What movement primarily mixes intestinal contents?
A: Segmentation contractions
Flashcard 9
Q: Which artery supplies midgut structures?
A: Superior mesenteric artery
Flashcard 10
Q: What happens to gland secretion during prolonged sympathetic stimulation?
A: Decreases due to vasoconstriction
Flashcard 11
Q: What structure prevents food entry into airway during swallowing?
A: Epiglottis
Flashcard 12
Q: What mechanism increases blood flow during digestion?
A: Local metabolic vasodilation
2️⃣Mnemonics
Mnemonic Title: GI Plexus Functions
Mnemonic Word:
“MOTOR Moves, SUB Secretes”
Meaning:
Myenteric → Motility
Submucosal → Secretion
Mnemonic Title: Swallowing Stages
Mnemonic Word:
“OPE”
Meaning:
O → Oral
P → Pharyngeal
E → Esophageal
Mnemonic Title: Major GI Arteries
Mnemonic Word:
“CFM”
Meaning:
C → Celiac trunk (Foregut)
F → SMA (Food pipe mid-section — Midgut)
M → IMA (Most distal — Hindgut)
3️⃣Memory Tables
Table 1 — Myenteric vs Submucosal Plexus
| Feature | Myenteric Plexus | Submucosal Plexus |
| Location | Between muscle layers | In submucosa |
| Main Function | Controls motility | Controls secretion |
| Movement Role | Peristalsis | Glandular regulation |
| Clinical Link | Hirschsprung disease | Secretory disorders |
Table 2 — Parasympathetic vs Sympathetic Effects
| Feature | Parasympathetic | Sympathetic |
| Motility | Increases | Decreases |
| Secretion | Increases | Decreases |
| Sphincters | Relaxes | Contracts |
| Blood Flow | Increases | Decreases |
4️⃣Rapid Revision Points (Last-Minute Review)
Must Remember:
• Slow waves set rhythm, spike potentials cause contraction
• Calcium entry is essential for smooth muscle contraction
• Myenteric plexus controls peristalsis
• Submucosal plexus controls secretion
• Law of the gut moves contents forward
• Pharyngeal stage protects airway
• Sympathetic stimulation reduces gland secretion
• Blood flow increases during digestion
• Segmentation mixes food; peristalsis propels food
• Midgut supplied by superior mesenteric artery
• Nitric oxide relaxes smooth muscle
5️⃣Clinical Memory Hooks
Clinical Hook 1:
Achalasia → Loss of nitric oxide → Failure of esophageal relaxation
Clinical Hook 2:
Hirschsprung disease → Absence of myenteric plexus → Severe constipation
Clinical Hook 3:
Paralytic ileus → Reduced neural activity → Absent peristalsis
Clinical Hook 4:
Aspiration pneumonia → Failure of pharyngeal stage protection
Clinical Hook 5:
Mesenteric ischemia → Reduced splanchnic blood flow → Severe abdominal pain