
This topic uses the AIM Learning Cycle to help MBBS students understand clinical disorders affecting swallowing and esophageal function by integrating Physiology, Pathology and Clinical Medicine.
1. Curriculum Coverage
Clinical / Pathology
• Clinical abnormalities of swallowing
• Achalasia
• Megaesophagus
• Esophageal candidiasis
• Drugs used in esophageal candidiasis
2. Learning Material
1️⃣ Introduction
Swallowing is a coordinated neuromuscular process that allows safe movement of food from the mouth to the stomach. The esophagus plays a central role in transporting food through rhythmic contractions known as peristalsis. Disorders of swallowing and esophageal function can lead to difficulty eating, malnutrition, aspiration, and infection. These conditions are clinically important because they often present as dysphagia (difficulty swallowing) or odynophagia (painful swallowing). Understanding these disorders helps students recognize early symptoms and manage common clinical problems such as achalasia and esophageal candidiasis.
2️⃣Foundation Basics
Key Definitions
- Swallowing (Deglutition): Movement of food from mouth → pharynx → esophagus → stomach
- Dysphagia: Difficulty in swallowing
- Odynophagia: Painful swallowing
- Peristalsis: Coordinated contraction pushing food forward
- Lower Esophageal Sphincter (LES): Circular muscle controlling entry into stomach
- Achalasia: Failure of LES relaxation
- Megaesophagus: Dilated esophagus due to chronic obstruction
- Esophageal Candidiasis: Fungal infection of esophageal mucosa
- Primary peristalsis: Swallow-induced wave
- Secondary peristalsis: Response to retained food
- LES tone: Resting contraction of lower esophagus
- Myenteric plexus: Controls esophageal motility
- Candida albicans: Most common fungal pathogen
3. Basic Review
Swallowing disorders arise when:
- Neural control fails
- Muscular contraction weakens
- Sphincter relaxation is impaired
- Infection damages mucosa
Result:
➡ Impaired food transport
➡ Pain
➡ Risk of aspiration
3️⃣ Core Learning — Curriculum Coverage
🧠 CORE (High-Yield Essentials)
- Dysphagia = difficulty in swallowing
- May affect oropharyngeal or esophageal phase
- Caused by neuromuscular dysfunction
- Can be structural or functional
- Leads to food retention
- Increases risk of aspiration pneumonia
- Often associated with neurological disease
- Important presenting symptom in esophageal disease
🔬 CONCEPT EXPLAINED
Structure
Swallowing involves:
- Mouth
- Pharynx
- Esophagus
- Lower esophageal sphincter
Mechanism
Swallowing occurs in phases:
- Oral phase (voluntary)
- Pharyngeal phase (reflex)
- Esophageal phase (peristalsis)
Failure at any stage causes dysphagia.
Structure → Function
Normal peristalsis:
- Moves food downward
- Prevents reflux
- Protects airway
⚠️ IF DAMAGED
Cause → Effect
- Nerve damage → weak muscle contraction
- Weak peristalsis → food retention
- Retained food → aspiration risk
- Aspiration → pneumonia
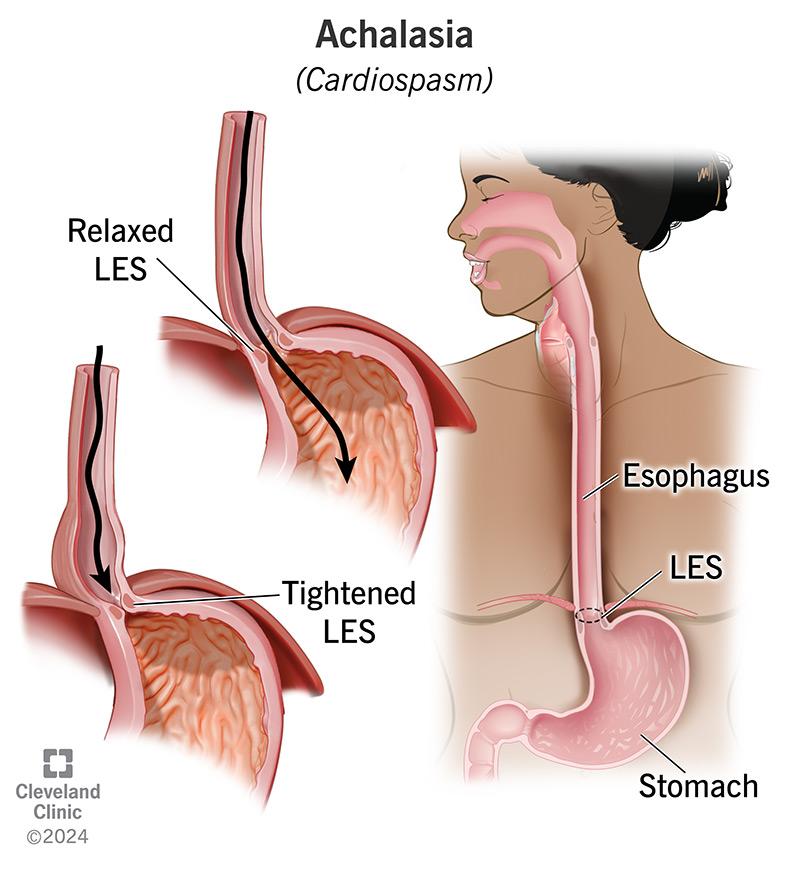
• Achalasia = failure of LES relaxation
• Caused by degeneration of myenteric plexus
• Leads to impaired peristalsis
• Food accumulates in esophagus
• Causes progressive dysphagia
• Both solids and liquids affected
• Produces regurgitation
• Diagnosed by manometry
🔬 CONCEPT EXPLAINED
Structure
Affected structures:
• Myenteric plexus
• LES muscle
• Esophageal body
Mechanism
Stepwise:
- Neural degeneration occurs
- LES fails to relax
- Food cannot enter stomach
- Esophagus dilates
- Peristalsis weakens
Structure → Function
LES normally:
• Relaxes during swallowing
• Allows food entry
In achalasia:
➡ LES remains contracted
➡ Food accumulates
⚠️ IF DAMAGED
Cause → Effect
Myenteric damage → LES failure →
Food retention → dilation → dysphagia
Concept Map 1 — Achalasia
ACHALASIA
│
├── WHAT IS IT
│ • Failure of Lower Esophageal Sphincter (LES) relaxation
│ • Loss of normal peristalsis
│
├── CAUSE
│ • Degeneration of Myenteric Plexus
│ • Loss of inhibitory neurons (NO, VIP)
│
├── MECHANISM
│ Myenteric damage
│ ↓
│ LES fails to relax
│ ↓
│ Food accumulates
│ ↓
│ Esophageal dilation
│ ↓
│ Dysphagia develops
│
├── IMPORTANT FEATURES
│ • Dysphagia for solids AND liquids
│ • Regurgitation of undigested food
│ • Chest discomfort
│ • Weight loss
│
├── DIAGNOSIS
│ • Manometry → gold standard
│ • Barium swallow → Bird-beak appearance
│
├── COMPLICATION
│ • Megaesophagus
│ • Aspiration pneumonia
│
└── TREATMENT
• Pneumatic dilation
• Myotomy surgery
• Nitrates / Calcium channel blockers
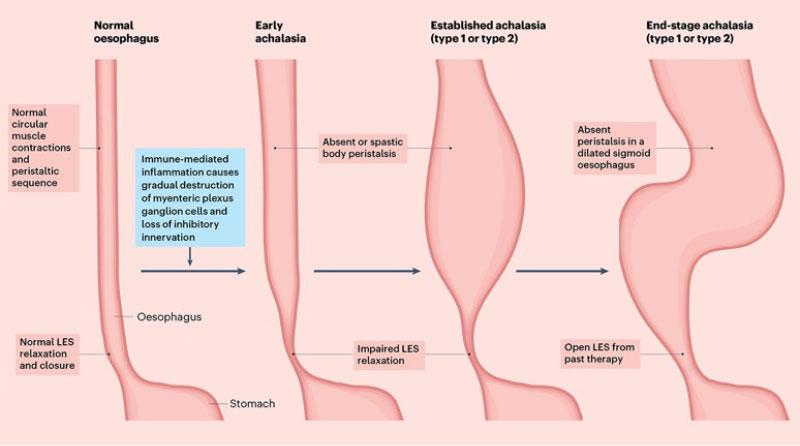
- Mega esophagus = enlarged esophagus
- Usually develops after chronic achalasia
- Caused by prolonged obstruction
- Leads to muscle stretching
- Weakens esophageal wall
- Food retention worsens
- Risk of aspiration increases
- May cause weight loss
🔬 CONCEPT EXPLAINED
Structure
Affected:
- Entire esophageal tube
- Muscular wall
Mechanism
- LES obstruction persists
- Food accumulates
- Pressure increases
- Wall stretches
- Esophagus enlarges
Structure → Function
Dilated esophagus:
- Loses peristaltic power
- Cannot push food effectively
⚠️ IF DAMAGED
Cause → Effect
Chronic obstruction → dilation →
Loss of motility → severe dysphagia
Concept Map 2 — Megaesophagus
MEGAESOPHAGUS
│
├── WHAT IS IT
│ • Marked dilation of esophagus
│ • Due to chronic obstruction
│
├── CAUSE
│ • Long-standing achalasia
│ • Persistent food retention
│
├── MECHANISM
│ LES obstruction persists
│ ↓
│ Food accumulates
│ ↓
│ Pressure increases
│ ↓
│ Esophageal wall stretches
│ ↓
│ Esophagus dilates
│
├── IMPORTANT FEATURES
│ • Severe dysphagia
│ • Food retention
│ • Regurgitation
│ • Weight loss
│
├── COMPLICATION
│ • Aspiration pneumonia
│ • Malnutrition
│
└── MANAGEMENT
• Treat underlying cause
• Surgical correction (if severe)
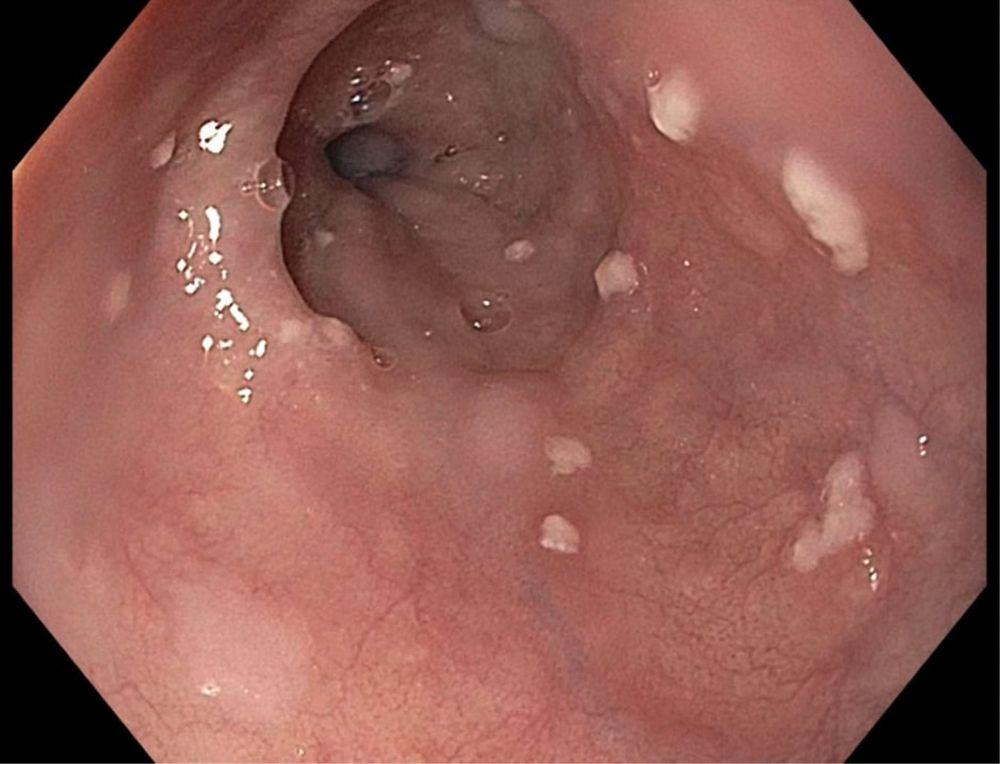
- Esophageal candidiasis = fungal infection
- Caused mainly by Candida albicans
- Occurs in immunocompromised patients
- Produces painful swallowing
- White plaques seen on mucosa
- Leads to inflammation
- Common in diabetes and HIV
- Diagnosed by endoscopy
🔬 CONCEPT EXPLAINED
Structure
Affected:
- Esophageal mucosal lining
Mechanism
- Immune system weakens
- Candida multiplies
- Fungal invasion occurs
- Inflammation develops
- Pain during swallowing occurs
Structure → Function
Damaged mucosa:
➡ Pain
➡ Difficulty swallowing
⚠️ IF DAMAGED
Cause → Effect
Fungal infection → mucosal injury →
Pain → reduced food intake
Concept Map 3 — Esophageal Candidiasis
ESOPHAGEAL CANDIDIASIS
│
├── WHAT IS IT
│ • Fungal infection of esophageal mucosa
│ • Caused mainly by Candida albicans
│
├── RISK FACTORS
│ • Diabetes mellitus
│ • HIV/AIDS
│ • Steroid therapy
│ • Chemotherapy
│ • Immunosuppression
│
├── MECHANISM
│ Immunity decreases
│ ↓
│ Candida multiplies
│ ↓
│ Mucosal invasion
│ ↓
│ Inflammation develops
│ ↓
│ Painful swallowing
│
├── IMPORTANT FEATURES
│ • Odynophagia (painful swallowing)
│ • Dysphagia
│ • White plaques in esophagus
│
├── DIAGNOSIS
│ • Endoscopy → white plaques
│
└── TREATMENT
• Fluconazole (first-line)
• Itraconazole
• Amphotericin B (severe cases)
CORE
- Antifungal drugs are primary treatment
- Fluconazole is first-line drug
- Itraconazole used if resistance occurs
- Amphotericin B used in severe infection
- Nystatin used for mild infection
- Therapy usually lasts 14–21 days
- Oral therapy preferred
- IV therapy used in severe cases
🔬 CONCEPT EXPLAINED
Structure
Drug targets:
➡ Fungal cell membrane
Mechanism
Antifungals:
- Inhibit ergosterol synthesis
- Damage fungal membrane
- Cause fungal death
Structure → Function
Healthy mucosa restored →
Normal swallowing resumes
⚠️ IF DAMAGED
Cause → Effect
Untreated infection → severe inflammation →
Ulceration → bleeding risk
4️⃣Mechanism Flow
Achalasia Mechanism
- Myenteric plexus degenerates
- LES fails to relax
- Food accumulates
- Esophagus dilates
- Dysphagia develops
Esophageal Candidiasis Mechanism
- Immunity decreases
- Candida multiplies
- Mucosa inflames
- Pain occurs
- Swallowing becomes difficult
5️⃣Functional Integration
Structure → Function → Outcome
Myenteric plexus → controls LES → allows swallowing
If damaged:
Myenteric loss → LES contraction → dysphagia
6️⃣Clinical Correlation
Common exam-relevant conditions:
- Achalasia
- Megaesophagus
- Esophageal candidiasis
- Dysphagia
- Odynophagia
Important Signs:
- Progressive dysphagia
- Regurgitation
- Weight loss
- Painful swallowing
⭐7️⃣Points to Remember
- Dysphagia is the most common symptom of esophageal disease
- Achalasia = failure of LES relaxation
- Myenteric plexus damage causes achalasia
- Chronic achalasia leads to megaesophagus
- Esophageal candidiasis occurs in immunocompromised patients
- Candida produces white mucosal plaques
- Fluconazole is first-line treatment
- Dilated esophagus loses peristalsis
- Painful swallowing suggests infection
- Untreated dysphagia may cause aspiration pneumonia
3. PRE-TEST MCQs
Results




#1. Difficulty in swallowing is medically termed as:
#2. Pain experienced during swallowing is best described as:
#3. Failure of relaxation of the lower esophageal sphincter is characteristic of:
#4. Degeneration of which neural structure is primarily responsible for achalasia?
#5. The most typical radiological feature of achalasia seen on barium study is:
#6. Progressive dilation of the esophagus due to long-standing obstruction is termed:
#7. A patient presents with dysphagia affecting both solids and liquids from the early stage. The most likely diagnosis is:
#8. Which organism is most commonly responsible for fungal infection of the esophagus?
#9. Painful swallowing associated with white plaques in the esophagus is most suggestive of:
#10. Which group of patients is at greatest risk of developing esophageal candidiasis?
#11. The primary function of the lower esophageal sphincter is to:
#12. Which investigation is considered the gold standard for confirming achalasia?
#13. Loss of peristaltic activity in the esophagus mainly leads to:
#14. The most common first-line drug used in treating esophageal candidiasis is:
#15. Which complication is most likely to occur due to chronic megaesophagus?
#16. Weakening of the esophageal wall due to prolonged stretching results in:
#17. Which symptom is most characteristic of esophageal candidiasis?
#18. Failure of inhibitory neurotransmission in the esophagus most directly affects:
#19. In untreated esophageal candidiasis, persistent inflammation may lead to:
#20. Which clinical feature best suggests advanced esophageal obstruction?
4. Diagnostic Feedback
Your score in this pre-test reflects your current level of understanding of the topic.
Score 0–7 → Foundational Level
You may not yet be familiar with the basic concepts of connective tissue structure and biochemistry.
Focus on understanding the components of extracellular matrix, collagen structure, glycosaminoglycans, and proteoglycans before attempting more advanced questions.
Score 8–14 → Developing Understanding
You have a partial understanding of connective tissue components and their functions.
Review the relationships between collagen fibers, extracellular matrix proteins, and ground substance, and how these components contribute to tissue strength and elasticity.
Score 15–20 → Strong Conceptual Base
You already have a solid understanding of connective tissue biochemistry and structure.
As you proceed through the learning material, focus on integrating histological structure with biochemical mechanisms and physiological functions.
5. Guided Reasoning
Ask AIM Tutor
I answered this MCQ incorrectly in my MBBS learning module.
Please help me understand:
1. What concept is being tested in this question?
2. Why is the correct option correct?
3. Why are the other options incorrect?
4. What is the key concept I should remember for exams?
Here is the MCQ:
6. Concept Integration
- 1️⃣ MASTER INTEGRATION CHAIN
- Whole Topic Core Flow
- Normal Swallowing
(Coordinated peristalsis + LES relaxation via myenteric plexus)
⬇
Neural or Mucosal Failure Occurs
(Myenteric degeneration OR mucosal infection)
⬇
Functional Obstruction or Inflammation
- LES fails to relax → Achalasia
- Chronic obstruction → Megaesophagus
- Fungal invasion → Esophageal candidiasis
⬇
Food Movement Becomes Impaired - Retention of food
- Painful swallowing
- Progressive dysphagia
⬇
Clinical Symptoms Appear - Dysphagia
- Odynophagia
- Regurgitation
- Weight loss
⬇
Drug or Mechanical Treatment Acts - Antifungals → destroy Candida
- Myotomy / dilation → relieve obstruction
⬇
Restored Function
Improved swallowing + reduced complications
- 3️⃣ CORE MECHANISM INTEGRATION
- Primary Functional Failure — Loss of Esophageal Propulsion
- Normal Myenteric Plexus Function
Maintains coordinated peristalsis + LES relaxation
⬇
Neuronal Degeneration Occurs
Loss of inhibitory neurons (NO, VIP)
⬇
LES Remains Contracted
Food cannot enter stomach
⬇
Food Accumulates in Esophagus
Pressure increases inside lumen
⬇
Progressive Esophageal Dilation
Megaesophagus develops
⬇
Clinical Dysphagia + Regurgitation - Clinical Meaning:
This explains why achalasia leads to megaesophagus and progressive symptoms. - 4️⃣ CLINICAL INTEGRATION SNAPSHOT
- Flow 1 — Achalasia
- Myenteric plexus degeneration
⬇
LES fails to relax
⬇
Food retention in esophagus
⬇
Dysphagia (solids + liquids)
⬇
Treatment:
Pneumatic dilation / Myotomy
⬇
Improved passage of food - Flow 2 — Megaesophagus
- Chronic LES obstruction
⬇
Persistent food retention
⬇
Esophageal wall stretching
⬇
Severe dilation
⬇
Regurgitation + aspiration risk
⬇
Treatment:
Correction of underlying obstruction - Flow 3 — Esophageal Candidiasis
- Immunosuppression
⬇
Candida albicans proliferation
⬇
Mucosal inflammation
⬇
Painful swallowing (Odynophagia)
⬇
Treatment:
Fluconazole therapy
⬇
Fungal destruction + mucosal healing - 5️⃣ ULTRA-HIGH-YIELD MASTER SUMMARY
- Final Revision Integration Model
- Normal Function
Myenteric plexus → coordinated peristalsis → LES relaxation → food enters stomach - ⬇
- Disease Mechanism
- • Neural loss → Achalasia
- Chronic obstruction → Megaesophagus
- Fungal infection → Esophageal candidiasis
- ⬇
- Drug Action
- • Antifungals → destroy fungal membrane
- Mechanical therapy → reduce LES obstruction
- ⬇
- Treatment Effect
- Restored swallowing
Reduced dysphagia
Prevention of complications
7. KMU Past Papers
MCQ 1
Question:
A 38-year-old male complains of progressive difficulty in swallowing both liquids and solids for the past 6 months. Barium swallow shows tapering of the distal esophagus. The primary physiological defect responsible for this condition involves failure of which process?
Options:
Sequential activation of circular muscle fibers
Inhibition of upper esophageal sphincter tone
Relaxation of the lower esophageal sphincter
Opening of pharyngoesophageal junction
Coordination of swallowing center activity
Correct Answer:
Relaxation of the lower esophageal sphincter
Explanation:
Achalasia results from failure of LES relaxation due to loss of inhibitory neuronal function.
MCQ 2
Question:
A patient with long-standing swallowing difficulty develops marked dilatation of the esophagus visible on imaging. The dilation occurs primarily due to which mechanical factor?
Options:
Reduced gastric acid secretion
Repeated mucosal ulceration
Persistent intraluminal pressure elevation
Impaired intestinal absorption
Reduced hepatic metabolism
Correct Answer:
Persistent intraluminal pressure elevation
Explanation:
Food retention increases intraluminal pressure, gradually stretching the esophageal wall leading to megaesophagus.
MCQ 3
Question:
A 45-year-old immunocompromised patient presents with painful swallowing. Endoscopy reveals multiple white plaques over the esophageal lining. Which pathological change best explains the symptom?
Options:
Formation of muscular hypertrophy
Reduction of mucosal blood supply
Fungal invasion causing mucosal inflammation
Accumulation of lipid deposits
Degeneration of smooth muscle
Correct Answer:
Fungal invasion causing mucosal inflammation
Explanation:
Candida infection leads to mucosal inflammation causing odynophagia.
MCQ 4
Question:
A patient with esophageal motility disorder shows absence of normal peristaltic waves. Loss of which neural signaling substance is most responsible for impaired relaxation of smooth muscle?
Options:
Acetylcholine
Histamine
Nitric oxide
Serotonin
Dopamine
Correct Answer:
Nitric oxide
Explanation:
Nitric oxide mediates inhibitory relaxation of LES; its loss contributes to achalasia.
MCQ 5
Question:
A patient complains of frequent regurgitation of undigested food several hours after meals. The symptom most directly results from which functional abnormality?
Options:
Reduced gastric emptying rate
Impaired esophageal clearance
Increased pancreatic secretion
Enhanced intestinal motility
Accelerated hepatic metabolism
Correct Answer:
Impaired esophageal clearance
Explanation:
Failure of esophageal propulsion leads to retention and regurgitation of food.
MCQ 6
Question:
During histological examination of an esophageal biopsy from a patient with chronic swallowing disorder, degeneration of ganglion cells is observed between muscle layers. Which structure is involved?
Options:
Submucosal plexus
Myenteric plexus
Celiac ganglion
Sympathetic trunk
Vagal nucleus
Correct Answer:
Myenteric plexus
Explanation:
Myenteric plexus lies between muscle layers and controls motility.
MCQ 7
Question:
A patient presents with painful swallowing and retrosternal discomfort. Examination reveals fungal infection of esophageal mucosa. Which pharmacological action is most useful in treating this condition?
Options:
Enhancement of mucosal bicarbonate secretion
Inhibition of fungal membrane synthesis
Reduction of gastric acid secretion
Stimulation of gastric emptying
Increase in intestinal enzyme release
Correct Answer:
Inhibition of fungal membrane synthesis
Explanation:
Antifungals like fluconazole inhibit ergosterol synthesis in fungal membranes.
MCQ 8
Question:
A patient develops progressive enlargement of the esophagus due to long-standing motility disorder. Loss of muscular tone in the esophageal wall primarily results from:
Options:
Repeated neural inhibition
Chronic mechanical stretching
Reduced oxygen delivery
Excessive mucosal secretion
Enhanced lymphatic drainage
Correct Answer:
Chronic mechanical stretching
Explanation:
Continuous distension weakens smooth muscle leading to dilation.
MCQ 9
Question:
A patient treated for esophageal fungal infection shows clinical improvement after receiving antifungal therapy. Which cellular component was most likely targeted by the drug?
Options:
DNA polymerase
Ribosomal subunit
Cell membrane sterol
Mitochondrial enzyme
Nuclear protein
Correct Answer:
Cell membrane sterol
Explanation:
Fluconazole targets ergosterol in fungal membranes.
MCQ 10
Question:
An individual with impaired swallowing develops recurrent respiratory infections. Which mechanism best explains this complication?
Options:
Increased gastric motility
Aspiration of retained food
Reduced salivary secretion
Excessive intestinal movement
Altered bile production
Correct Answer:
Aspiration of retained food
Explanation:
Food retained in esophagus can be aspirated into respiratory tract.
MCQ 11
Question:
A patient with esophageal motility disorder shows decreased passage of food despite normal swallowing initiation. The defect most likely occurs in which phase?
Options:
Oral phase
Pharyngeal phase
Esophageal phase
Gastric phase
Intestinal phase
Correct Answer:
Esophageal phase
Explanation:
Achalasia affects esophageal peristalsis.
MCQ 12
Question:
A patient receiving prolonged corticosteroid therapy develops painful swallowing. Which factor most likely predisposed this patient to infection?
Options:
Increased mucosal secretion
Reduced immune response
Enhanced epithelial turnover
Improved vascular supply
Increased enzyme production
Correct Answer:
Reduced immune response
Explanation:
Steroids suppress immunity increasing fungal infection risk.
MCQ 13
Question:
A patient develops progressive dilation of the esophagus. Which structural component primarily loses its contractile efficiency?
Options:
Mucosal epithelium
Smooth muscle layer
Submucosal gland
Adventitial tissue
Serosal membrane
Correct Answer:
Smooth muscle layer
Explanation:
Smooth muscle contraction maintains esophageal tone.
MCQ 14
Question:
A patient reports sensation of food sticking in the chest region after swallowing. Which functional disturbance best explains this symptom?
Options:
Delayed salivary secretion
Impaired esophageal propulsion
Reduced bile secretion
Accelerated gastric motility
Increased pancreatic activity
Correct Answer:
Impaired esophageal propulsion
Explanation:
Failure of coordinated peristalsis causes food retention sensation.
MCQ 15
Question:
An immunocompromised patient develops esophageal infection with mucosal damage. Which biochemical change primarily contributes to fungal survival?
Options:
Altered glucose metabolism
Presence of ergosterol in membrane
Decreased protein synthesis
Enhanced lipid breakdown
Reduced nucleic acid production
Correct Answer:
Presence of ergosterol in membrane
Explanation:
Ergosterol stabilizes fungal membranes and is targeted by antifungal drugs.
MCQ 16
Question:
A patient with advanced esophageal dilation develops significant weight loss. Which physiological change best explains this outcome?
Options:
Reduced intestinal enzyme activity
Failure of nutrient propulsion
Increased metabolic rate
Enhanced gastric emptying
Reduced bile secretion
Correct Answer:
Failure of nutrient propulsion
Explanation:
Food cannot reach stomach efficiently leading to malnutrition.
MCQ 17
Question:
During evaluation of esophageal motility disorder, loss of inhibitory neural control is detected. Which functional imbalance results from this loss?
Options:
Persistent sphincter contraction
Enhanced mucosal secretion
Reduced gastric enzyme activity
Increased intestinal motility
Accelerated hepatic metabolism
Correct Answer:
Persistent sphincter contraction
Explanation:
Loss of inhibitory neurons keeps LES contracted.
MCQ 18
Question:
A patient presents with painful swallowing and mucosal ulceration. Which physiological function of mucosa is primarily compromised?
Options:
Mechanical propulsion
Barrier protection
Muscle contraction
Hormone secretion
Blood filtration
Correct Answer:
Barrier protection
Explanation:
Mucosal damage reduces protective barrier function.
MCQ 19
Question:
A patient with swallowing disorder shows progressive esophageal enlargement visible on imaging. Which factor most strongly determines severity of dilation?
Options:
Rate of salivary secretion
Duration of obstruction
Level of gastric acidity
Presence of intestinal enzymes
Frequency of bile release
Correct Answer:
Duration of obstruction
Explanation:
Long-standing obstruction produces progressive dilation.
MCQ 20
Question:
A patient treated with antifungal therapy shows healing of esophageal mucosa. Restoration of which function best explains clinical improvement?
Options:
Reduced hepatic metabolism
Recovery of mucosal integrity
Increased pancreatic secretion
Accelerated intestinal movement
Decreased bile formation
Correct Answer:
Recovery of mucosal integrity
Explanation:
Healing mucosa restores swallowing function and reduces pain.
8. Post-Test
Attempt Your Post Test Here
9. Explanation of Incorrect Answers
Incorrect answers are valuable learning opportunities. When reviewing MCQs, focus on understanding the concept behind the question, not just memorizing the correct option.
If you answered a question incorrectly:
• Identify the concept being tested.
• Determine why the correct option is correct.
• Understand why the other options are incorrect.
You can paste the MCQ into the AIM Tutor and ask for a step-by-step explanation. This helps strengthen conceptual understanding and improves reasoning for future questions.
Learning Tip
If your Post-Test score is below 80%, review the key concepts and attempt the Post-Test again to reinforce your understanding.
10. Student Memory Support
- 1️⃣ High-Yield Flashcards
- Flashcard 1
Q: What is dysphagia?
A: Difficulty in swallowing. - Flashcard 2
Q: What is odynophagia?
A: Pain during swallowing. - Flashcard 3
Q: What is the primary defect in achalasia?
A: Failure of lower esophageal sphincter (LES) relaxation. - Flashcard 4
Q: Which neural structure degenerates in achalasia?
A: Myenteric plexus. - Flashcard 5
Q: What radiological sign is characteristic of achalasia?
A: Bird-beak appearance. - Flashcard 6
Q: What is megaesophagus?
A: Dilated esophagus due to chronic obstruction. - Flashcard 7
Q: Which organism commonly causes esophageal candidiasis?
A: Candida albicans. - Flashcard 8
Q: What symptom strongly suggests esophageal infection?
A: Painful swallowing (odynophagia). - Flashcard 9
Q: What is the first-line drug for esophageal candidiasis?
A: Fluconazole. - Flashcard 10
Q: What complication may occur due to long-standing dysphagia?
A: Aspiration pneumonia. - Flashcard 11
Q: Why does megaesophagus develop in achalasia?
A: Persistent food retention increases pressure and dilates esophagus. - Flashcard 12
Q: Which neurotransmitters are lost in achalasia inhibitory neurons?
A: Nitric oxide (NO) and VIP.
- 2️⃣ Mnemonics
- Mnemonic Title: Achalasia Key Mechanism
- Mnemonic Word:
“NO RELAX” - Meaning:
N → Nitric oxide loss
O → Obstruction at LES
R → Retention of food
E → Esophageal dilation
L → Loss of peristalsis
A → Achalasia symptoms
X → eXpansion (Megaesophagus)
- Mnemonic Title: Risk Factors for Esophageal Candidiasis
- Mnemonic Word:
“DISH” - Meaning:
D → Diabetes
I → Immunocompromised state
S → Steroid therapy
H → HIV infection
- Mnemonic Title: Features of Achalasia
- Mnemonic Word:
“DRIB” - Meaning:
D → Dysphagia
R → Regurgitation
I → Incomplete LES relaxation
B → Bird-beak sign
- 3️⃣ Memory Tables
- Table 1 — Achalasia vs Megaesophagus
| Feature | Achalasia | Megaesophagus |
| Primary problem | LES fails to relax | Esophageal dilation |
| Cause | Myenteric plexus damage | Long-standing obstruction |
| Function affected | Peristalsis failure | Mechanical dilation |
| Main symptom | Dysphagia | Severe regurgitation |
| Complication | Food retention | Aspiration risk |
- Table 2 — Dysphagia vs Odynophagia
| Feature | Dysphagia | Odynophagia |
| Meaning | Difficulty swallowing | Pain during swallowing |
| Main cause | Motility disorder | Infection or inflammation |
| Common condition | Achalasia | Candidiasis |
| Key clinical clue | Food sticking | Pain with swallowing |
- 4️⃣ Rapid Revision Points
- Must Remember
- • Achalasia occurs due to loss of inhibitory neurons.
• LES fails to relax in achalasia.
• Bird-beak sign is classic for achalasia.
• Chronic achalasia leads to megaesophagus.
• Megaesophagus increases aspiration risk.
• Candida infection causes painful swallowing.
• Immunocompromised patients are prone to candidiasis.
• Fluconazole is first-line treatment.
• Food retention causes esophageal dilation.
• Nitric oxide loss contributes to LES dysfunction. - 5️⃣ Clinical Memory Hooks
- Clinical Hook 1:
Achalasia → Failure of LES relaxation → Dysphagia for solids and liquids - Clinical Hook 2:
Long-standing Achalasia → Esophageal dilation → Megaesophagus - Clinical Hook 3:
HIV or steroid therapy → Candida infection → Painful swallowing - Clinical Hook 4:
Food retention in the esophagus → Aspiration → Recurrent chest infections - Clinical Hook 5:
White plaques on endoscopy → Candida infection → Treat with fluconazole
✔ Topic Completion
📊 Your Performance
Pre-Test: Not Attempted
Post-Test: Not Attempted
Improvement: --