
This topic uses the AIM Learning Cycle to help MBBS students understand the structural organization of the anterior abdominal wall and inguinal canal by integrating Anatomy and Clinical concepts.
1. Curriculum Coverage
Anatomy
• Origin, insertion, nerve supply and actions of anterolateral abdominal wall muscles
• Formation of rectus sheath
• Contents of rectus sheath
• Surface anatomy of anterior abdominal wall
• Structures related to transpyloric plane
• Types of abdominal hernias
• Boundaries of inguinal canal
• Contents of inguinal canal in males and females
• Direct and indirect inguinal hernia
📚Standard Reference Framework
Primary Anatomy Reference:
BD Chaurasia — Standard Undergraduate Depth
Concept Support:
Gray’s Anatomy for Students
Spatial Atlas:
Netter Atlas
Physiology:
Guyton & Hall
Histology:
DiFiore Atlas
Biochemistry:
Lippincott Illustrated Reviews
🎯Depth Policy
All content is restricted to Undergraduate MBBS Level.
Depth will not exceed BD Chaurasia standard.
2. Learning Material
1️⃣ Introduction
The anterior abdominal wall forms the front boundary of the abdominal cavity and plays a vital role in supporting abdominal organs, maintaining posture, and assisting respiration and movements. It extends from the thoracic margin above to the pelvis below, and from the vertebral column posteriorly to the skin anteriorly.
A key specialized structure within this wall is the inguinal canal, an oblique passage in the lower abdomen that allows structures such as the spermatic cord in males and round ligament in females to pass through.
Clinically, this region is extremely important because it is a common site of hernias, especially inguinal hernias, which are among the most frequent surgical conditions encountered worldwide. Understanding the layered structure, muscle arrangement, and canal boundaries is essential for diagnosis and safe clinical practice.
2️⃣ Foundation Basics
Key Definitions
• Anterior Abdominal Wall — The multilayered muscular and fascial structure forming the front of the abdomen.
• Anterolateral Abdominal Muscles — Muscles forming the lateral abdominal wall responsible for movement and support.
• Rectus Sheath — A fibrous covering formed by abdominal muscle aponeuroses enclosing the rectus abdominis muscle.
• Inguinal Canal — An oblique passage in the lower abdominal wall transmitting reproductive structures.
• Hernia — Protrusion of an organ or tissue through a weakened body wall.
• Transpyloric Plane — A horizontal anatomical plane passing through important abdominal structures.
Essential Terminology
• Aponeurosis — Flat tendon-like sheet of connective tissue.
• Linea Alba — Midline fibrous structure formed by fusion of aponeuroses.
• Semilunar Line — Curved lateral border of rectus abdominis.
• Deep Inguinal Ring — Entrance of inguinal canal.
• Superficial Inguinal Ring — Exit of inguinal canal.
• Hesselbach’s Triangle — Weak area in lower abdominal wall associated with hernias.
3️⃣ Core Learning — Curriculum Coverage
Muscles Included:
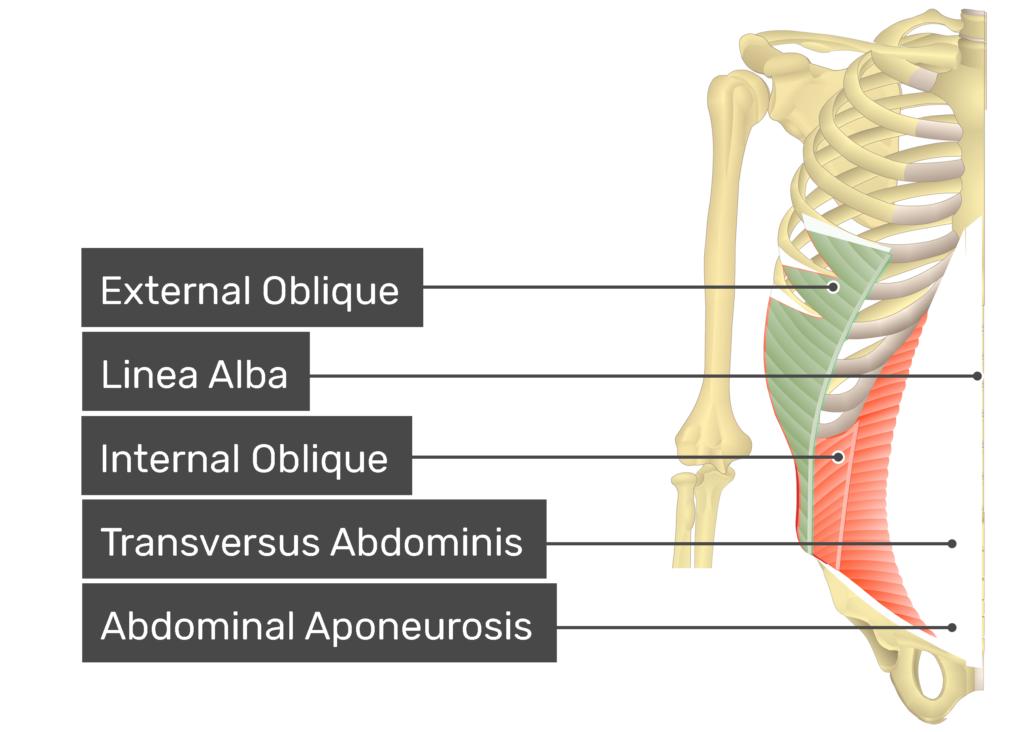
- External Oblique
- Internal Oblique
- Transversus Abdominis
- Rectus Abdominis
- Pyramidalis (minor muscle)
🧠 CORE
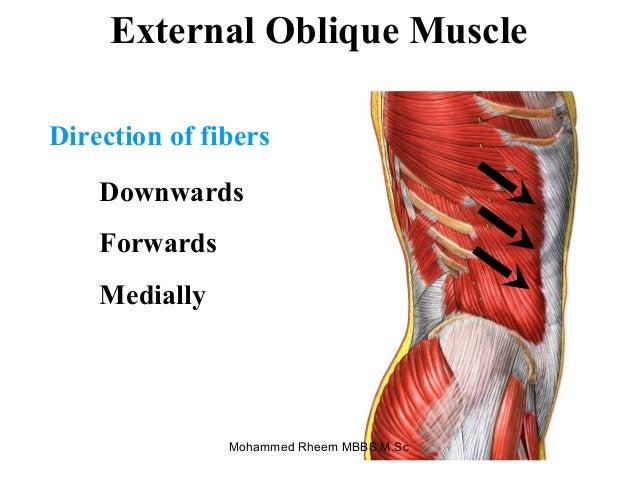
- Definition: Most superficial abdominal muscle forming lateral abdominal wall
- Location: Superficial layer, lateral abdomen
- Origin: Lower 8 ribs (5th–12th ribs)
- Insertion: Linea alba, pubic tubercle, anterior iliac crest
- Nerve Supply: Thoracoabdominal nerves (T7–T11), Subcostal nerve (T12)
- Action:
• Compress abdominal contents
• Flex trunk
• Rotate trunk to opposite side - Functional Role: Provides abdominal wall strength and trunk movement
🔬 CONCEPT EXPLAINED
Structure:
Fibers run downward and medially, similar to direction of hands in pockets.
Mechanism:
- Bilateral contraction → trunk flexion
- Unilateral contraction → rotation to opposite side
- Compression supports abdominal organs
Structure → Function:
Oblique fiber direction allows twisting movements and provides broad muscular support.
⚠️ IF DAMAGED
Cause: Nerve injury (T7–T12)
Effect:
- Weak abdominal wall
- Reduced trunk rotation
- Increased risk of hernia
🧠 CORE
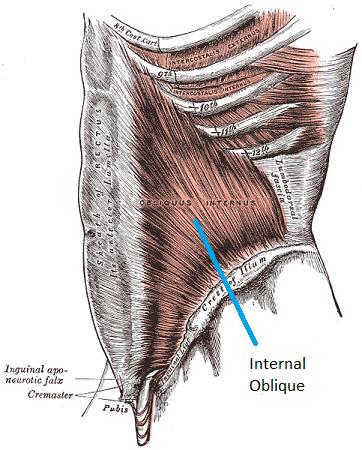
- Definition: Intermediate muscle of lateral abdominal wall
- Location: Between external oblique and transversus abdominis
- Origin: Thoracolumbar fascia, iliac crest, inguinal ligament
- Insertion: Lower ribs (10–12), linea alba
- Nerve Supply: Thoracoabdominal nerves (T7–T11), T12, L1
- Action:
Compress abdominal contents
Flex trunk
Rotate trunk to same side
🔬 CONCEPT EXPLAINED
Structure:
Fibers run upward and medially, opposite to external oblique.
Mechanism:
- Bilateral contraction → trunk flexion
- Unilateral contraction → rotation to same side
Structure → Function:
Opposite fiber orientation to external oblique allows balanced trunk rotation.
⚠️ IF DAMAGED
- Weak trunk rotation
- Reduced abdominal compression
- Risk of hernia formation
🧠 CORE
- Definition: Deepest abdominal muscle
- Location: Deep layer of abdominal wall
- Origin: Lower ribs, thoracolumbar fascia, iliac crest
- Insertion: Linea alba
- Nerve Supply: T7–T12, L1
- Action: Compress abdominal contents
- Functional Role: Provides major abdominal wall support
🔬 CONCEPT EXPLAINED
Structure:
Fibers run horizontally across abdomen.
Mechanism:
Contraction pulls abdominal wall inward → compresses organs.
Structure → Function:
Horizontal fibers act like a corset, stabilizing abdominal contents.
⚠️ IF DAMAGED
- Loss of abdominal support
- Increased intra-abdominal pressure complications
- Risk of abdominal wall weakness
🧠 CORE
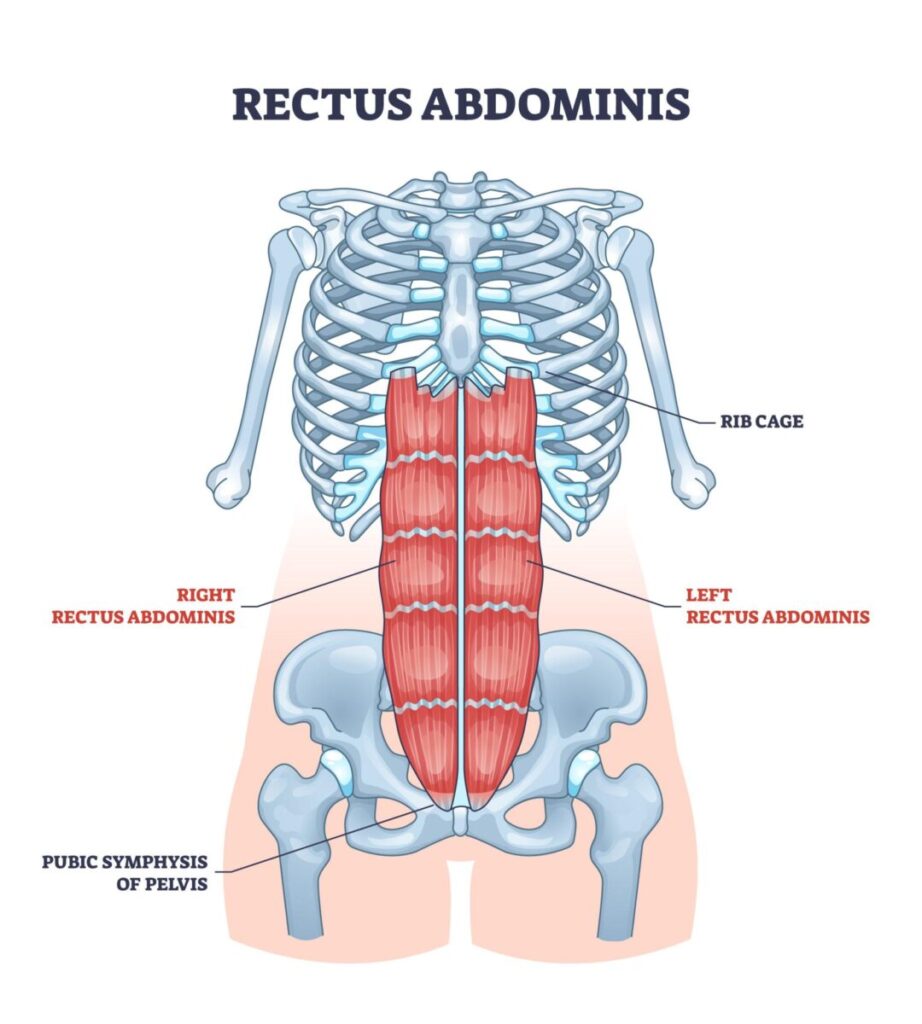
- Definition: Long vertical muscle in anterior abdominal wall
- Location: On either side of linea alba
- Origin: Pubic crest
- Insertion: 5th–7th costal cartilages
- Nerve Supply: T7–T12
- Action:
• Flex trunk
• Stabilize pelvis
• Compress abdomen
🔬 CONCEPT EXPLAINED
Structure:
Contains tendinous intersections, dividing muscle into segments.
Mechanism:
Shortening pulls rib cage downward → trunk flexion.
Structure → Function:
Segmented design increases strength and flexibility.
⚠️ IF DAMAGED
- Weak trunk flexion
- Reduced abdominal support
- Postural instability
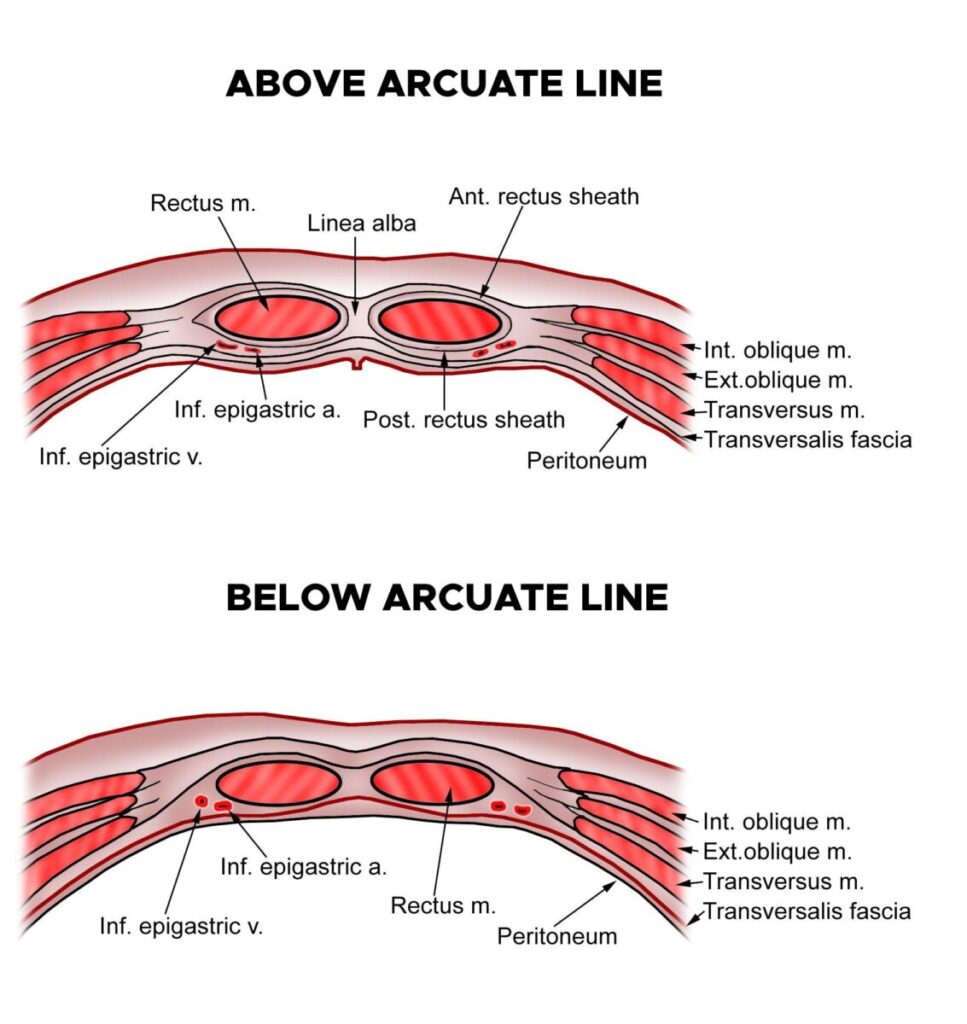
🧠 CORE
- Definition: Fibrous sheath enclosing rectus abdominis
- Formed By: Aponeuroses of three abdominal muscles
• External oblique
• Internal oblique
• Transversus abdominis - Has anterior and posterior layers
- Changes structure at arcuate line
🔬 CONCEPT EXPLAINED
Above Arcuate Line:
- External oblique → anterior
- Internal oblique → splits
- Transversus → posterior
Below Arcuate Line:
All aponeuroses pass anteriorly.
Structure → Function:
Provides strength and protection to rectus muscle.
⚠️ IF DAMAGED
- Weak abdominal wall
- Hernia formation risk
- Loss of abdominal wall integrity
Contents of Rectus Sheath
🧠 CORE
Contains:
- Rectus abdominis muscle
- Pyramidalis muscle
- Superior epigastric vessels
- Inferior epigastric vessels
- Thoracoabdominal nerves
🔬 CONCEPT EXPLAINED
Rectus sheath protects muscles and vessels while allowing movement.
Structure → Function:
Strong fibrous covering prevents injury to internal vessels.
⚠️ IF DAMAGED
- Bleeding (epigastric vessel injury)
- Muscle dysfunction
- Hematoma formation
🧠 CORE
- Definition: Surface anatomy refers to visible and palpable landmarks on the abdominal wall used to identify internal structures.
- 3D Location:
• Anterior aspect of abdomen
• Extends from costal margin above to pubic symphysis below
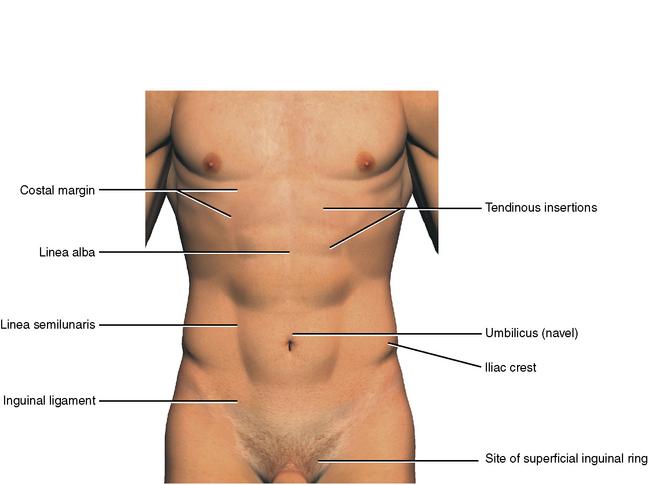
• From midline (linea alba) to flanks laterally - Major Surface Landmarks:
• Linea alba
• Linea semilunaris
• Umbilicus
• Costal margin
• Iliac crest
• Inguinal ligament - Functional Role:
• Helps clinicians locate organs
• Guides physical examination
• Used in surgical incisions
🔬 CONCEPT EXPLAINED
Structure
The anterior abdominal wall contains several important visible landmarks used to divide the abdomen into regions.
Key Surface Structures
- Linea Alba
- Midline fibrous structure
- Extends from xiphoid process to pubic symphysis
- Formed by fusion of abdominal muscle aponeuroses
- Linea Semilunaris
- Curved line marking lateral border of rectus abdominis
- Important surgical landmark
- Umbilicus
- Located at L3–L4 vertebral level
- Important reference point
- Marks center of abdomen
- Inguinal Ligament
- Runs from anterior superior iliac spine (ASIS) to pubic tubercle
- Forms lower boundary of abdomen
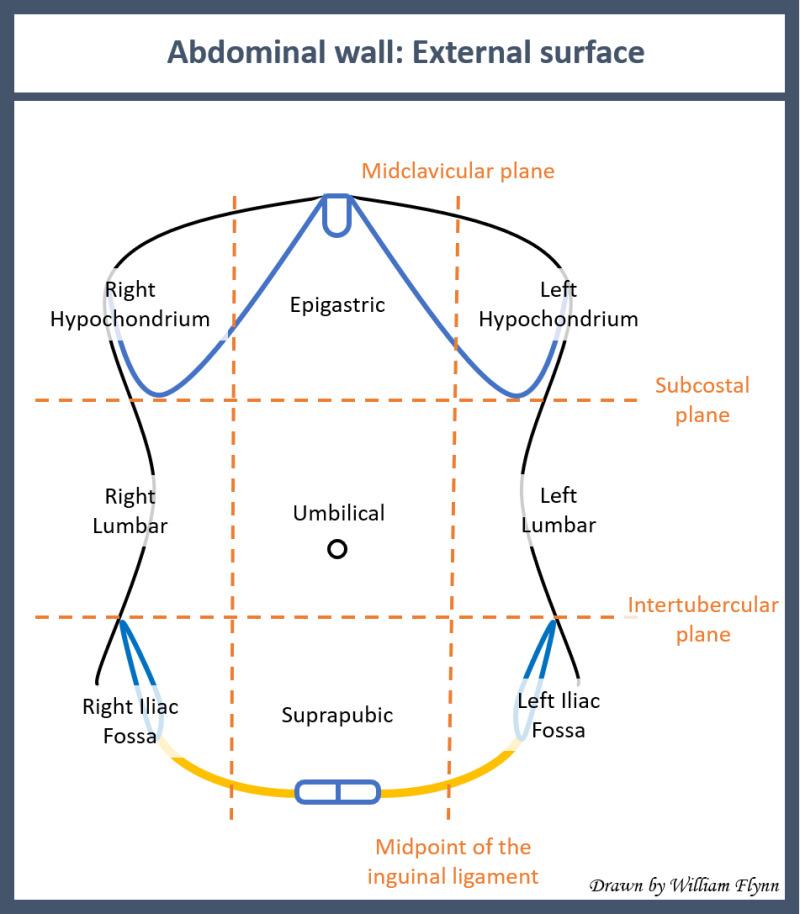
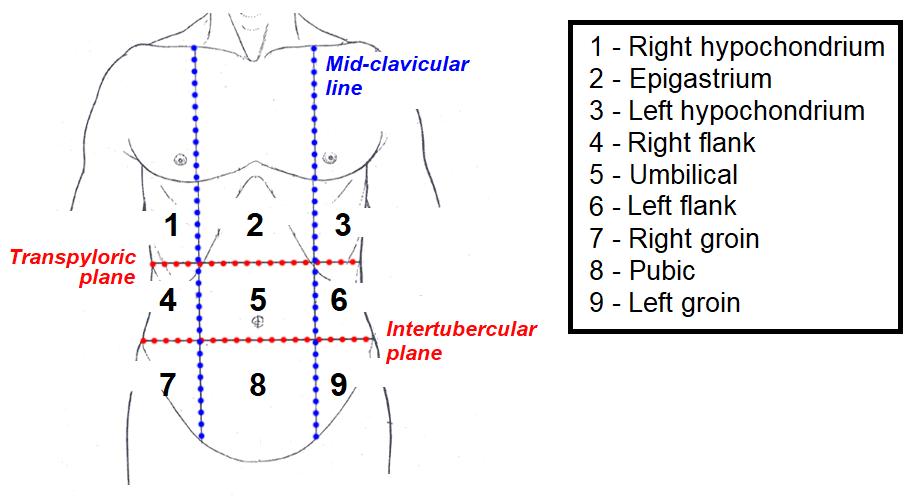
Abdominal Regions Division
9-Region Division
Formed by:
- Two vertical midclavicular lines
- Two horizontal planes
Regions:
Upper Row - Right hypochondrium
- Epigastric
- Left hypochondrium
Middle Row - Right lumbar
- Umbilical
- Left lumbar
Lower Row - Right iliac
- Hypogastric
- Left iliac
4-Quadrant Division
Formed by:
- Median plane
- Transumbilical plane
Quadrants: - Right Upper Quadrant (RUQ)
- Left Upper Quadrant (LUQ)
- Right Lower Quadrant (RLQ)
- Left Lower Quadrant (LLQ)
Structure → Function
Surface landmarks allow:
Surface landmark
→ Organ localization
→ Accurate clinical diagnosis
Example:
McBurney’s Point
→ Location of appendix
→ Helps diagnose appendicitis
⚠️ IF DAMAGED
Cause: Loss of anatomical knowledge or incorrect localization
Effect:
- Incorrect diagnosis
- Surgical injury to organs
- Misplaced incisions
Additional High-Yield Surface Landmarks
McBurney’s Point
Location:
- Junction of lateral 1/3 and medial 2/3 of line from umbilicus to ASIS
Clinical Importance: - Site of maximum tenderness in appendicitis
Midclavicular Line
Location:
- Vertical line passing through midpoint of clavicle
Clinical Importance: - Divides abdomen into regions
Inguinal Ligament Surface Marking
Location:
- Between ASIS and pubic tubercle
Clinical Importance: - Important boundary of inguinal canal
🧠 CORE
- Definition:
A horizontal anatomical plane passing through the abdomen at the level of L1 vertebra, used as an important surface landmark to locate abdominal organs. - 3D Location:
• Lies midway between:
o Suprasternal notch
o Pubic symphysis
• Approximately halfway between xiphisternum and umbilicus - Alternate Name:
Addison’s Plane - Major Structures Related to Transpyloric Plane:
• Pylorus of stomach
• Neck of pancreas
• Fundus of gallbladder
• Origin of superior mesenteric artery
• Hila of kidneys
• Duodenojejunal flexure - Functional Role:
Helps clinicians locate major abdominal organs during examination and imaging.
🔬 CONCEPT EXPLAINED
Structure
The transpyloric plane is a key horizontal reference line used in anatomy and clinical medicine.
It crosses the vertebral column at L1 level, making it one of the most reliable anatomical reference planes.
Major Structures Located at Transpyloric Plane
1️⃣ Pylorus of Stomach
- Junction between stomach and duodenum
- Lies at L1 level
- Important in gastric emptying
Structure → Function:
Pyloric sphincter regulates passage of food into duodenum.
2️⃣ Neck of Pancreas
- Lies anterior to portal vein formation
- Divides head and body of pancreas
Structure → Function:
Important landmark in pancreatic anatomy and surgery.
3️⃣ Fundus of Gallbladder
- Lies at tip of right 9th costal cartilage
- Located at level of transpyloric plane
Structure → Function:
Stores bile produced by liver.
4️⃣ Superior Mesenteric Artery (SMA) Origin
- Arises from abdominal aorta at L1
Structure → Function:
Supplies midgut structures.
5️⃣ Hilum of Kidneys
- Both kidneys lie at this level
- Left kidney slightly higher than right
Structure → Function:
Allows entry and exit of renal vessels and ureter.
6️⃣ Duodenojejunal Flexure
- Junction between duodenum and jejunum
- Suspended by ligament of Treitz
Structure → Function:
Important for transition of digestion and absorption.
Structure → Function → Outcome
Transpyloric Plane
→ Identifies central abdominal organs
→ Helps in diagnosis and safe surgical access
Example:
Pain at transpyloric level
→ May involve pylorus or pancreas
→ Helps narrow diagnosis
⚠️ IF DAMAGED / MISINTERPRETED
Cause: Incorrect anatomical identification
Effect:
- Misdiagnosis of abdominal pathology
- Injury to vital structures during surgery
- Difficulty locating organs clinically
Clinical Importance of Transpyloric Plane
Used In:
- Abdominal examination
- Ultrasound localization
- CT scan interpretation
- Surgical planning
- Organ surface marking
High-Yield Memory Aid
Structures at Transpyloric Plane — Remember:
“PPP KFD”
P → Pylorus
P → Pancreas (neck)
P → Portal vein formation
K → Kidneys (hilum)
F → Fundus of gallbladder
D → Duodenojejunal flexure
🧠 CORE
- Definition:
A hernia is the protrusion of a viscus (usually intestine) through a weakness in the abdominal wall. - 3D Location:
Occurs at weak areas of anterior abdominal wall, especially in the lower abdomen. - Major Components of Hernia:
- Hernial sac (peritoneum)
- Hernial contents (usually intestine)
- Hernial coverings (abdominal wall layers)
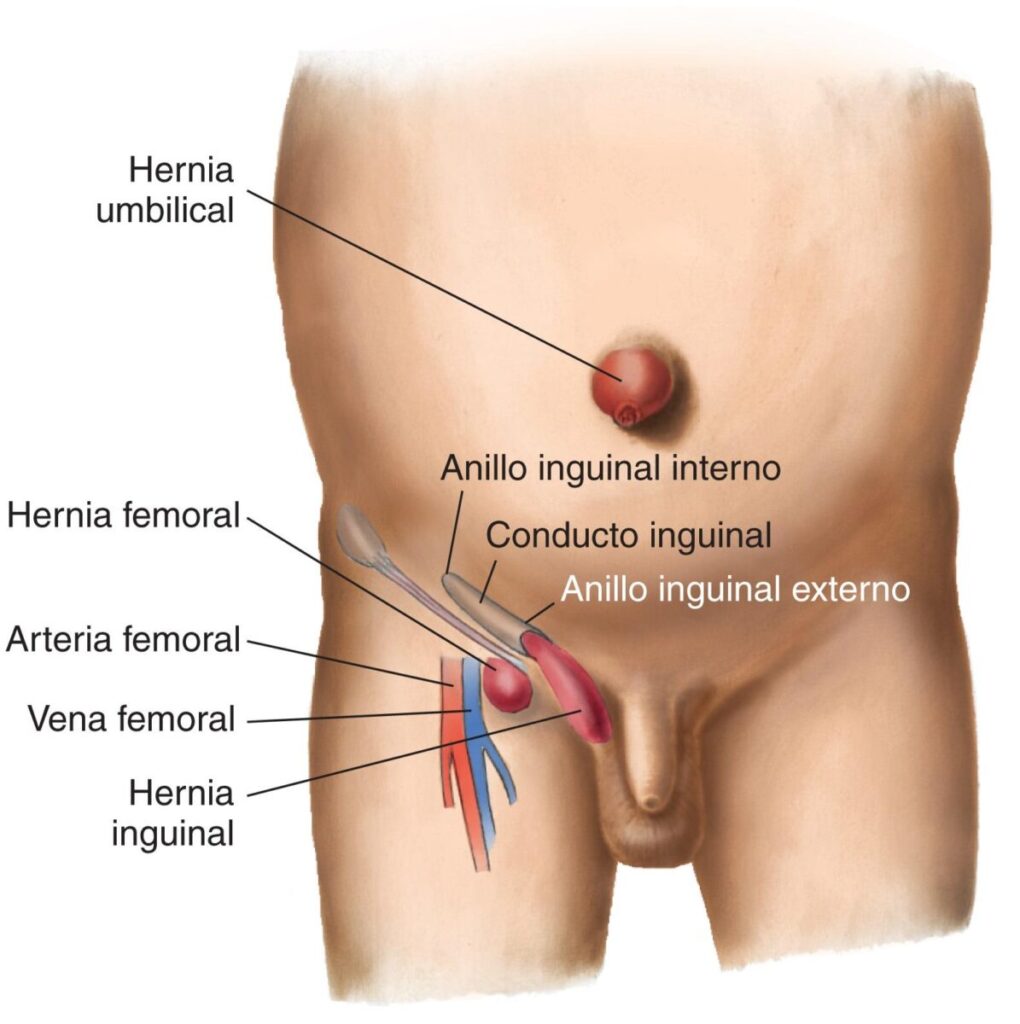
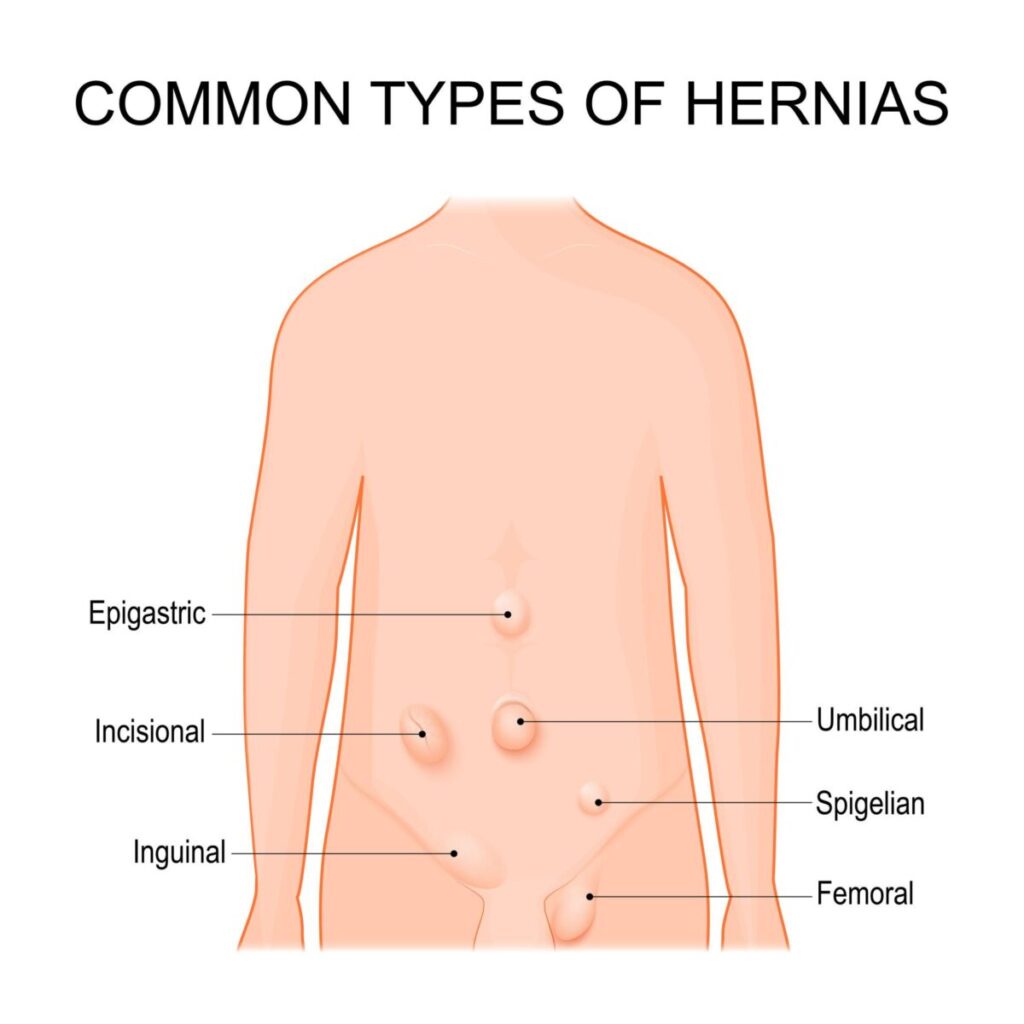
- Common Types of Abdominal Hernias (BD Chaurasia level):
• Inguinal hernia (most common)
• Femoral hernia
• Umbilical hernia
• Incisional hernia
• Epigastric hernia - Primary Function (Why it exists):
Weak areas exist naturally to allow passage of structures such as spermatic cord and vessels.
🔬 CONCEPT EXPLAINED
What is a Hernia?
Normally, abdominal muscles and fascia hold abdominal organs inside.
If there is:
- Weak muscle wall
OR - Increased intra-abdominal pressure
→ Abdominal contents push outward
→ Hernia develops.
Major Types of Abdominal Hernias
1️⃣ Inguinal Hernia
🧠 CORE
- Most common abdominal hernia
- Occurs in inguinal region above inguinal ligament
- More common in males
- Two types:
• Direct inguinal hernia
• Indirect inguinal hernia
🔬 Structure → Function
The inguinal canal is a natural weak point allowing passage of spermatic cord.
Weak abdominal wall
→ Intestine pushes through
→ Inguinal hernia develops
⚠️ IF DAMAGED
Cause → Weak posterior wall
Effect → Hernia formation
2️⃣ Femoral Hernia
🧠 CORE
- Occurs below inguinal ligament
- Passes through femoral canal
- More common in females
- Higher risk of strangulation
🔬 Structure → Function
Femoral canal normally contains lymphatics.
Weak femoral ring
→ Abdominal contents pass into thigh region
→ Femoral hernia forms
⚠️ IF DAMAGED
Cause → Weak femoral canal
Effect → Painful swelling below inguinal ligament
3️⃣ Umbilical Hernia
🧠 CORE
- Occurs at umbilicus
- Common in infants
- Due to incomplete closure of umbilical ring
🔬 Structure → Function
Umbilical ring normally closes after birth.
Failure of closure
→ Weak area persists
→ Umbilical hernia forms
⚠️ IF DAMAGED
Cause → Weak umbilical scar
Effect → Bulging at umbilicus
4️⃣ Incisional Hernia
🧠 CORE
- Occurs at site of previous surgical incision
- Due to poor healing of abdominal wall
🔬 Structure → Function
Scar tissue weaker than muscle.
Weak scar
→ Organ protrusion
→ Incisional hernia develops
⚠️ IF DAMAGED
Cause → Poor wound healing
Effect → Hernia at surgical site
5️⃣ Epigastric Hernia
🧠 CORE
- Occurs through linea alba
- Located between umbilicus and xiphisternum
- Contains preperitoneal fat
🔬 Structure → Function
Linea alba contains small defects.
Fat pushes through defect
→ Epigastric swelling forms
⚠️ IF DAMAGED
Cause → Weak linea alba
Effect → Midline swelling
Why Hernias Occur (High-Yield Mechanism)
Weak abdominal wall
+
Increased pressure (coughing, lifting, pregnancy)
↓
Protrusion of abdominal contents
↓
Hernia formation
Structure → Function → Outcome
Weak area in abdominal wall
→ Allows passage of structures
→ Predisposes to hernia formation
Clinical Correlation (BD Chaurasia Level)
Reducible Hernia
- Swelling disappears on pressure
- Contents return into abdomen
Irreducible Hernia
- Cannot be pushed back
- Risk of obstruction
Strangulated Hernia
- Blood supply cut off
- Medical emergency
Concept Map: Boundaries of Inguinal Canal
ROOF
Internal Oblique + TransversusANTERIOR POSTERIOR
External Oblique Transversalis Fascia
(+ Internal Oblique) (+ Conjoint Tendon) FLOOR
Inguinal Ligament
🧠 CORE
- Definition:
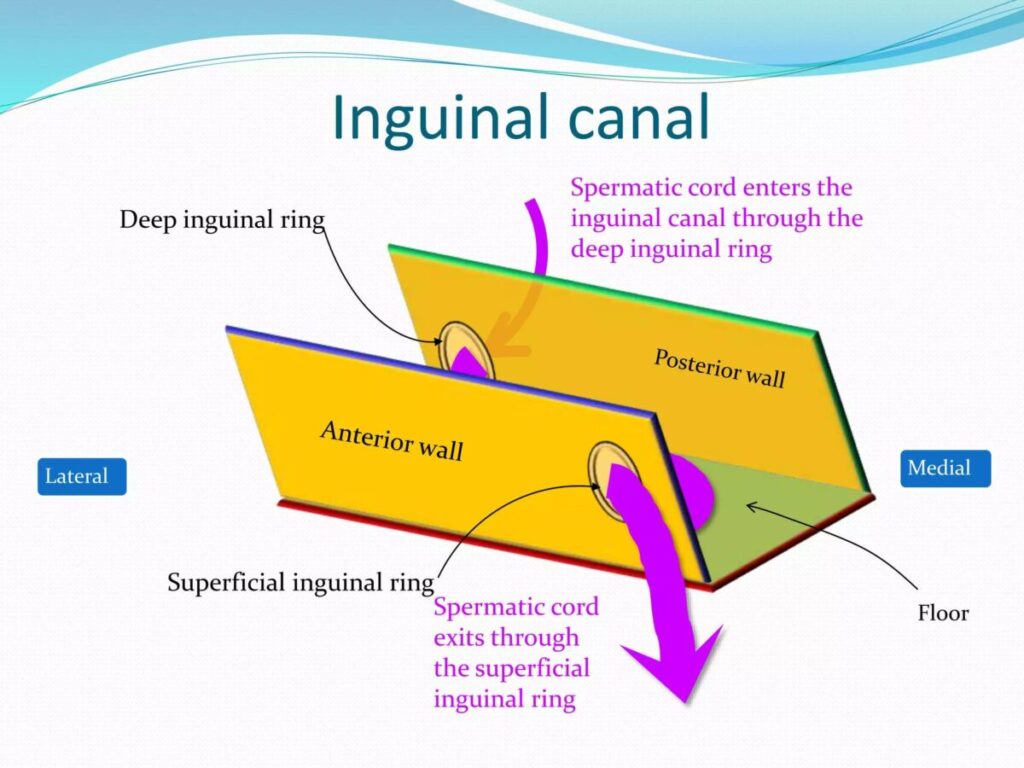
The inguinal canal is an oblique passage in the lower anterior abdominal wall, transmitting structures between abdomen and external genitalia. - 3D Location:
Located above medial half of inguinal ligament
Extends from deep inguinal ring (posterolateral)
Ends at superficial inguinal ring (anteromedial)
- Length:
Approximately 4 cm - Openings:
Deep inguinal ring (entrance)
Superficial inguinal ring (exit)
- Major Boundaries:
Anterior wall
Posterior wall
Roof
Floor
- Primary Function:
Allows passage of spermatic cord (male) and round ligament (female).
🔬 CONCEPT EXPLAINED
What is the Inguinal Canal?
The inguinal canal is a slanting tunnel running downward, forward, and medially in the lower abdomen.
It exists because during development, the testis descends from abdomen into scrotum, leaving behind this passage.
Boundaries of Inguinal Canal
(VERY HIGH-YIELD — Frequently asked in exams)
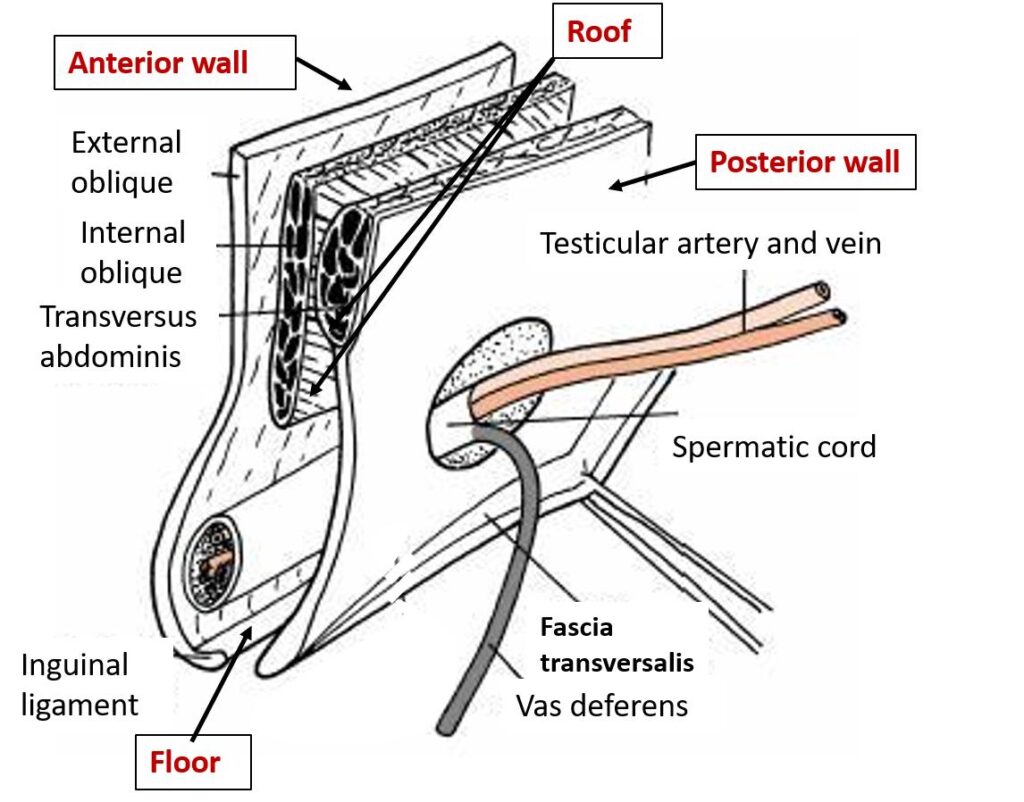
1️⃣ Anterior Wall
🧠 CORE
Formed by:
- Aponeurosis of external oblique muscle (throughout)
- Internal oblique muscle fibers (laterally)
3D Position:
- Lies in front of inguinal canal
Functional Role:
Provides front protection to canal contents.
🔬 Structure → Function
External oblique aponeurosis forms a strong fibrous sheet.
Extra reinforcement laterally by internal oblique
→ Prevents bulging at deep ring
→ Supports inguinal canal.
⚠️ IF DAMAGED
Weak anterior wall
→ Increased risk of inguinal hernia
2️⃣ Posterior Wall
🧠 CORE
Formed by:
- Transversalis fascia (throughout)
- Conjoint tendon (medially)
3D Position:
- Lies behind inguinal canal
Functional Role:
Provides main structural strength.
🔬 Structure → Function
Transversalis fascia is thin but reinforced medially by conjoint tendon.
This reinforcement protects Hesselbach’s triangle — a weak area.
⚠️ IF DAMAGED
Weak posterior wall
→ Direct inguinal hernia
(Very important clinical relation)
3️⃣ Roof
🧠 CORE
Formed by:
- Arching fibers of:
Internal oblique
Transversus abdominis
3D Position:
- Upper boundary of canal
Functional Role:
Acts as muscular cover.
🔬 Structure → Function
Arching fibers contract
→ Compress canal
→ Prevent hernia formation.
⚠️ IF DAMAGED
Weak roof
→ Loss of muscular support
→ Hernia risk increases.
4️⃣ Floor
🧠 CORE
Formed by:
- Inguinal ligament
- Lacunar ligament (medially)
3D Position:
- Lower boundary of canal
Functional Role:
Supports contents of inguinal canal.
🔬 Structure → Function
Inguinal ligament acts like a floor support beam.
Lacunar ligament strengthens medial part.
⚠️ IF DAMAGED
Weak floor
→ Hernial protrusion downward
→ Femoral hernia risk.
Deep and Superficial Inguinal Rings
(Exam favorite topic)
Deep Inguinal Ring
🧠 CORE
- Opening in transversalis fascia
- Located above midpoint of inguinal ligament
- Entrance of canal
Superficial Inguinal Ring
🧠 CORE
- Opening in external oblique aponeurosis
- Located above pubic tubercle
- Exit of canal
Structure → Function → Outcome
Oblique canal
+
Strong muscular walls
↓
Protects abdominal contents
↓
Reduces hernia risk
High-Yield Memory Aid
Boundaries of Inguinal Canal
Mnemonic:
“MALT”
M → Muscle (roof)
A → Aponeurosis (anterior wall)
L → Ligament (floor)
T → Transversalis fascia (posterior wall)
Clinical Integration (BD Chaurasia Focus)
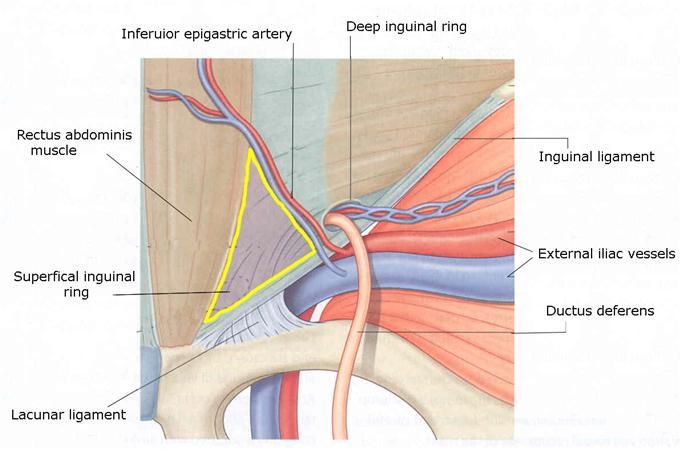
Hesselbach’s Triangle
(Important weak area)
Boundaries:
- Medial — Rectus abdominis
- Lateral — Inferior epigastric vessels
- Inferior — Inguinal ligament
Clinical relevance:
Site of direct inguinal hernia.
Concept Map — Contents of Inguinal Canal
INGUINAL CANAL
↓
┌─────────────────────┐
│ │
MALE FEMALE
│ │
Spermatic Cord Round Ligament
│ │
└──────┬──────────────┘
↓
Ilioinguinal Nerve
(Both Sexes)
🧠 CORE
- Definition:
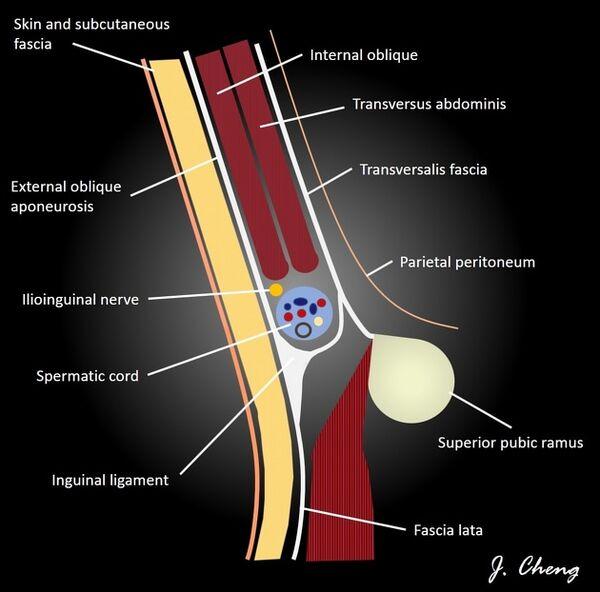
The inguinal canal contents are structures that pass through the canal from abdomen to external genitalia. - 3D Location:
Within the inguinal canal, running from deep inguinal ring (lateral) to superficial inguinal ring (medial). - Main Difference:
• Male: Spermatic cord
• Female: Round ligament of uterus - Structures Present in Both Sexes:
• Ilioinguinal nerve - Primary Function:
Allows passage of reproductive structures while maintaining abdominal wall integrity.
🔬 CONCEPT EXPLAINED
The inguinal canal acts as a protected passageway that transmits structures from the abdomen to external genitalia.
It exists mainly because of testicular descent in males and persistence of a similar but smaller passage in females.
Contents of Inguinal Canal in MALE
(VERY HIGH-YIELD — Frequently asked)
🧠 CORE
Main Content:
Spermatic Cord
Additional Structure:
- Ilioinguinal nerve
Spermatic Cord — Major Components
🧠 CORE
Contains:
- Vas deferens
→ Transports sperm - Testicular artery
→ Branch of abdominal aorta - Pampiniform plexus of veins
→ Venous drainage of testis - Cremasteric artery
→ From inferior epigastric artery - Artery to vas deferens
→ From superior vesical artery - Genital branch of genitofemoral nerve
→ Supplies cremaster muscle - Lymphatics
→ Drain testis - Remnant of processus vaginalis
Structure → Function
Spermatic cord components allow:
Testicular artery
→ Blood supply to testis
Vas deferens
→ Sperm transport
Pampiniform plexus
→ Temperature regulation of testis
(Ilioinguinal nerve supplies sensation to upper medial thigh and scrotum)
⚠️ IF DAMAGED
Cause → Injury to spermatic cord
Effect →
- Loss of blood supply
- Infertility risk
- Pain and swelling
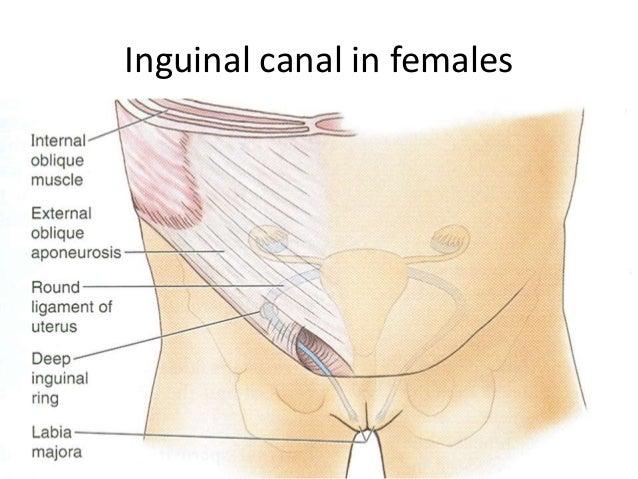
Contents of Inguinal Canal in FEMALE
🧠 CORE
Contains:
- Round ligament of uterus
- Ilioinguinal nerve
Round Ligament of Uterus
🧠 CORE
- Fibrous band extending from uterus to labia majora
- Maintains anteverted position of uterus
Structure → Function
Round ligament
→ Supports uterus
→ Maintains correct uterine position
⚠️ IF DAMAGED
Cause → Ligament weakness
Effect →
- Loss of uterine support
- Predisposition to uterine displacement
Structure → Function → Outcome
Inguinal canal
→ Transmits reproductive structures
→ Maintains reproductive function
Comparison — Male vs Female Contents
(High-Yield Table — BD Chaurasia Style)
Feature Male Female
Main Content Spermatic cord Round ligament
Additional Nerve Ilioinguinal nerve Ilioinguinal nerve
Canal Size Larger Smaller
Hernia Risk Higher Lower
Developmental Basis (Why Canal Exists)
(High-Yield Understanding)
During fetal life:
Testis descends
↓
Passes through abdominal wall
↓
Forms inguinal canal
In females:
Similar pathway persists as smaller canal.
Clinical Correlation
Ilioinguinal Nerve Injury
Cause → Surgical damage
Effect →
- Loss of sensation
- Groin numbness
Varicocele
Cause → Dilated pampiniform plexus
Effect →
- Scrotal swelling
- Fertility issues
Direct vs Indirect Inguinal Hernia (Single Integrated Map)
INGUINAL HERNIA
│
┌──────────────────┴──────────────────┐
│ │
INDIRECT HERNIA DIRECT HERNIA
(Most Common Type) (Posterior Wall Weakness)
│ │
│ │
Entry Point Entry Point
Deep Inguinal Ring Posterior Wall
│ │
│ │
Relation to Inferior Relation to Inferior
Epigastric Vessels Epigastric Vessels
│ │
LATERAL MEDIAL
│ │
│ │
Pathway Pathway
Deep Ring → Canal Through Hesselbach Triangle
→ Superficial Ring │
│ │
│ │
May Reach Scrotum Rarely Reaches Scrotum
│ │
│ │
Cause Cause
Patent Processus Vaginalis Weak Posterior Wall
(Congenital) (Acquired)
│ │
│ │
Common In Common In
Young Males Elderly Males
🧠 CORE
• Definition:
An inguinal hernia is the protrusion of abdominal contents through the inguinal region due to weakness in the abdominal wall.
• Types:
- Indirect Inguinal Hernia
- Direct Inguinal Hernia
• Key Distinguishing Landmark:
Inferior epigastric vessels
• Primary Functional Importance:
Understanding the difference helps in clinical diagnosis and surgical management.
🔬 CONCEPT EXPLAINED
The inguinal region contains natural weak areas where abdominal contents may protrude.
The route taken by the hernia sac determines whether it is direct or indirect.
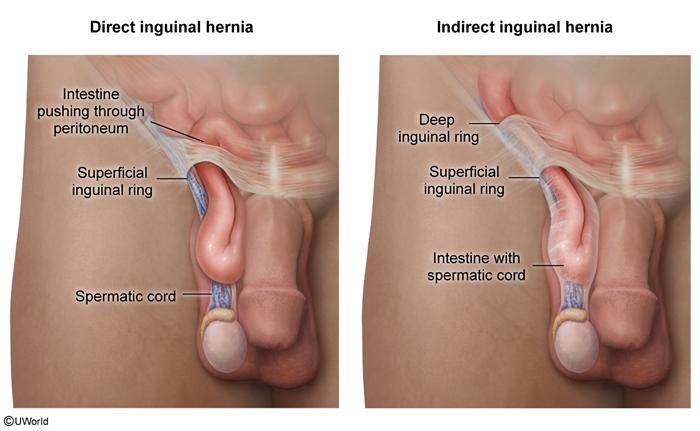
1️⃣ Indirect Inguinal Hernia
(Most Common Type — Very High Yield)
🧠 CORE
• Definition:
Hernia that passes through the deep inguinal ring and follows the inguinal canal pathway.
• Location:
Lateral to inferior epigastric vessels
• Pathway:
Deep ring
→ Inguinal canal
→ Superficial ring
→ May reach scrotum
• Common In:
Young males
• Cause:
Persistence of processus vaginalis (congenital cause)
🔬 Structure → Function
Normally:
Processus vaginalis closes
↓
Prevents abdominal contents from entering canal
If remains open:
↓
Intestine follows spermatic cord pathway
↓
Indirect hernia forms
⚠️ IF DAMAGED / OCCURS
Cause → Patent processus vaginalis
Effect →
• Hernia extends into scrotum
• Scrotal swelling
• Risk of strangulation
2️⃣ Direct Inguinal Hernia
🧠 CORE
• Definition:
Hernia that protrudes directly through posterior wall of inguinal canal.
• Location:
Medial to inferior epigastric vessels
• Site:
Hesselbach’s Triangle
• Common In:
Older males
• Cause:
Weak posterior wall of inguinal canal.
🔬 Structure → Function
Posterior wall becomes weak
↓
Abdominal contents push forward
↓
Direct hernia develops
Unlike indirect hernia:
Usually does not enter scrotum.
⚠️ IF DAMAGED / OCCURS
Cause → Weak abdominal muscles
Effect →
• Bulging in groin
• Usually reducible
• Lower risk of reaching scrotum
Hesselbach’s Triangle
(Very Important Exam Landmark)
🧠 CORE
Boundaries:
• Medial — Rectus abdominis
• Lateral — Inferior epigastric vessels
• Inferior — Inguinal ligament
Clinical Role:
Site of direct inguinal hernia.
Key Difference — Direct vs Indirect Hernia
(Extremely High-Yield Table — BD Chaurasia Standard)
| Feature | Indirect Hernia | Direct Hernia |
| Relation to inferior epigastric vessels | Lateral | Medial |
| Entry point | Deep inguinal ring | Posterior wall |
| Pathway | Through canal | Direct protrusion |
| Reaches scrotum | Common | Rare |
| Cause | Congenital | Acquired |
| Age group | Young | Elderly |
| Site | Outside Hesselbach triangle | Inside Hesselbach triangle |
Structure → Function → Outcome
Weak abdominal wall
↓
Increased intra-abdominal pressure
↓
Hernial protrusion occurs
Type depends on route of protrusion.
Clinical Correlation
Expansile Cough Impulse
Finding:
Swelling increases on coughing.
Indicates:
Presence of inguinal hernia.
Strangulated Hernia
Cause → Blood supply cut off
Effect →
• Severe pain
• Intestinal obstruction
• Surgical emergency
4️⃣ Mechanism Flow
Mechanism 1 — Formation of Rectus Sheath
Above Arcuate Line
1️⃣ External oblique → passes anterior to rectus muscle
2️⃣ Internal oblique → splits into two layers
3️⃣ Transversus abdominis → passes posterior
4️⃣ Layers meet in midline → form linea alba
✅ Result:
Rectus muscle enclosed in strong anterior & posterior walls
Below Arcuate Line
1️⃣ All aponeuroses pass anterior to rectus muscle
2️⃣ Posterior wall contains only transversalis fascia
⚠️ Result:
Posterior wall becomes weak area
Mechanism 2 — Formation of Inguinal Canal
1️⃣ Testis develops in abdomen
2️⃣ Descends toward scrotum
3️⃣ Processus vaginalis forms pathway
4️⃣ Testis passes through this pathway
5️⃣ Remaining pathway becomes inguinal canal
✅ Result:
Permanent passage formed in abdominal wall.
Mechanism 3 — Indirect Inguinal Hernia
1️⃣ Processus vaginalis remains open
2️⃣ Abdominal pressure increases
3️⃣ Contents enter deep ring
4️⃣ Pass through inguinal canal
5️⃣ May reach scrotum
⚠️ Result:
Indirect inguinal hernia develops
Mechanism 4 — Direct Inguinal Hernia
1️⃣ Posterior wall becomes weak
2️⃣ Pressure pushes abdominal contents
3️⃣ Hernia protrudes through Hesselbach triangle
⚠️ Result:
Direct inguinal hernia develops
Mechanism 5 — Protective (Shutter) Mechanism
1️⃣ Internal oblique & transversus arch over canal
2️⃣ During contraction → fibers descend
3️⃣ Canal becomes compressed
✅ Result:
Helps prevent hernia formation
Mechanism 6 — Abdominal Muscle Pressure Action
1️⃣ Abdominal muscles contract
2️⃣ Abdominal volume decreases
3️⃣ Pressure increases
✅ Used in:
- Defecation
- Micturition
- Vomiting
- Childbirth
5️⃣ Functional Integration
Structure → Function → Outcome
1️⃣ Layered Abdominal Muscles
External oblique + Internal oblique + Transversus
→ Compress abdomen
→ Support abdominal organs
→ Maintain intra-abdominal pressure
2️⃣ Rectus Sheath Formation
Aponeurotic layers surround rectus muscle
→ Provide protection and strength
→ Prevent bulging of abdominal contents
3️⃣ Inguinal Canal Design
Oblique pathway with muscular roof
→ Allows passage of reproductive structures
→ Reduces risk of herniation
4️⃣ Posterior Wall Strength
Transversalis fascia + Conjoint tendon
→ Supports weak medial area
→ Prevents direct hernia
5️⃣ Weak Areas in Abdominal Wall
Natural openings exist
→ Allow passage of structures
→ Predispose to hernia formation
6️⃣ Clinical Correlation
(Exam-Relevant & Common Conditions Only)
1️⃣ Inguinal Hernia
Most common abdominal wall hernia.
Types:
- Indirect → Congenital (patent processus vaginalis)
- Direct → Acquired (posterior wall weakness)
Clinical Finding:
Groin swelling with expansile cough impulse
2️⃣ Femoral Hernia
- Occurs below inguinal ligament
- More common in females
- High risk of strangulation
Clinical Sign:
Swelling below inguinal ligament.
3️⃣ Umbilical Hernia
- Occurs at umbilicus
- Common in infants
- Due to incomplete closure of umbilical ring.
4️⃣ Strangulated Hernia
Blood supply to herniated contents stops.
Features:
- Severe pain
- Swelling
- Surgical emergency.
5️⃣ Rectus Sheath Hematoma
Bleeding into rectus sheath due to vessel injury.
Clinical Features:
- Painful abdominal swelling
- Local tenderness.
6️⃣ Varicocele (Related to Spermatic Cord)
Dilated pampiniform plexus.
Common Side:
Left side
Effect:
- Scrotal swelling
- Possible infertility.
⭐ 7️⃣ Points to Remember
(High-Yield Revision Points)
1️⃣ External oblique fibers run downward & medially (“hands in pockets”).
2️⃣ Internal oblique fibers run upward & medially.
3️⃣ Transversus abdominis fibers run horizontally.
4️⃣ Rectus sheath posterior wall weak below arcuate line.
5️⃣ Inguinal canal length ≈ 4 cm.
6️⃣ Deep ring lies lateral to inferior epigastric vessels.
7️⃣ Direct hernia → medial to inferior epigastric vessels.
8️⃣ Indirect hernia → lateral to inferior epigastric vessels.
9️⃣ Hesselbach triangle → site of direct inguinal hernia.
🔟 Indirect hernia may reach scrotum, direct usually does not.
3. Pre Test
Results




#1. Which muscle forms the most superficial layer of the anterolateral abdominal wall?
#2. Fibers of the internal oblique muscle are primarily directed in which orientation?
#3. The main action of transversus abdominis muscle is:
#4. Rectus abdominis muscle is enclosed within which anatomical structure?
#5. Below the arcuate line, the posterior wall of rectus sheath is mainly formed by:
#6. Which vessel runs within the rectus sheath and supplies the rectus abdominis muscle?
#7. The linea alba is formed by fusion of:
#8. The transpyloric plane lies at the level of which vertebra?
#9. Which structure is located at the level of the transpyloric plane?
#10. The superficial inguinal ring is an opening in which structure?
#11. Which structure forms the posterior wall of the inguinal canal?
#12. The floor of the inguinal canal is mainly formed by:
#13. Which structure passes through the inguinal canal in males?
#14. Which nerve is present in the inguinal canal in both males and females?
#15. Indirect inguinal hernia occurs lateral to which structure?
#16. Direct inguinal hernia protrudes through which anatomical region?
#17. Which type of hernia commonly reaches the scrotum?
#18. The conjoint tendon is formed by fusion of aponeuroses of:
#19. Which abdominal wall region is commonly associated with direct inguinal hernia?
#20. Which structure forms the roof of the inguinal canal?
4. Diagnostic Feedback
Your score in this pre-test reflects your current level of understanding of the topic.
Score 0–7 → Foundational Level
You may not yet be familiar with the basic concepts of connective tissue structure and biochemistry.
Focus on understanding the components of extracellular matrix, collagen structure, glycosaminoglycans, and proteoglycans before attempting more advanced questions.
Score 8–14 → Developing Understanding
You have a partial understanding of connective tissue components and their functions.
Review the relationships between collagen fibers, extracellular matrix proteins, and ground substance, and how these components contribute to tissue strength and elasticity.
Score 15–20 → Strong Conceptual Base
You already have a solid understanding of connective tissue biochemistry and structure.
As you proceed through the learning material, focus on integrating histological structure with biochemical mechanisms and physiological functions.
5. Guided Reasoning
Ask AIM Tutor
I answered this MCQ incorrectly in my MBBS learning module.
Please help me understand:
1. What concept is being tested in this question?
2. Why is the correct option correct?
3. Why are the other options incorrect?
4. What is the key concept I should remember for exams?
Here is the MCQ:
6. Concept Integration
1️⃣ MASTER INTEGRATION CHAIN
Whole Topic Core Flow
(Normal Function → Failure → Drug Action)
Layered Abdominal Wall Muscles
(External → Internal → Transversus → Rectus)
↓
Rectus Sheath Formation
(Strong muscular support)
↓
Inguinal Canal Formation
(Controlled passage for reproductive structures)
↓
Maintains:
- Abdominal pressure
- Organ support
- Safe anatomical passage
↓
WEAKNESS OR DEFECT
(Muscle failure / fascia weakness)
↓
Hernial Protrusion Occurs
(Indirect or Direct Hernia)
↓
Clinical Features: - Groin swelling
- Pain on coughing
- Risk of obstruction
↓
Drug & Treatment Action: - Analgesics → Pain control
- Muscle relaxation → Reduce strain
- Surgical mesh repair → Strengthens wall
↓
Restored Wall Strength
↓
Normal abdominal function resumes
3️⃣ CORE MECHANISM INTEGRATION
Primary Failure Mechanism — Hernia Formation
(Main Functional Breakdown of Topic)
Normal Abdominal Wall
(Muscles + Fascia + Canal)
↓
Weak Area Develops
(Hesselbach triangle / Deep ring)
↓
Increase in Intra-Abdominal Pressure
(Coughing / Lifting / Straining)
↓
Abdominal Contents Push Outward
↓
Hernial Sac Forms
↓
Type Depends on Pathway:
Lateral to Inferior Epigastric
→ Indirect Hernia
Medial to Inferior Epigastric
→ Direct Hernia
↓
Possible Complication:
Strangulation → Ischemia → Emergency
4️⃣ CLINICAL INTEGRATION SNAPSHOT
Clinical Flow 1 — Indirect Inguinal Hernia
Patent Processus Vaginalis
(Congenital defect)
↓
Open Deep Inguinal Ring
↓
Intestinal Loop Enters Canal
↓
Scrotal Swelling Develops
↓
Symptoms:
- Groin swelling
- Cough impulse
↓
Treatment:
Herniotomy / Herniorrhaphy
↓
Canal Closed → Hernia Prevented
Clinical Flow 2 — Direct Inguinal Hernia
Weak Posterior Wall
(Aging / Muscle weakness)
↓
Pressure from Abdomen
↓
Hesselbach Triangle Bulges
↓
Groin Swelling Appears
↓
Symptoms:
- Reducible swelling
- Discomfort on exertion
↓
Treatment:
Mesh Repair Surgery
↓
Wall Strength Restored
5️⃣ ULTRA-HIGH-YIELD MASTER SUMMARY
Final System Integration Model
(Last-Day Revision Tool)
NORMAL FUNCTION
Layered Muscles
- Rectus Sheath
- Inguinal Canal
↓
Provide: - Strength
- Protection
- Controlled passage
DISEASE MECHANISM
Weak Fascia or Muscle
↓
Raised Intra-Abdominal Pressure
↓
Hernia Formation
(Direct / Indirect
DRUG / TREATMENT ACTION
Analgesics → Pain Relief
Support Devices → Reduce strain
Surgical Mesh → Reinforce wa
FINAL OUTCOME
Wall Strength Restored
↓
Normal abdominal support maintained
7. KMU Past Papers
MCQ 1
Question:
A 52-year-old laborer presents with a swelling in the right groin that becomes prominent while lifting heavy objects and reduces on lying down. On examination, the swelling appears medial to the inferior epigastric vessels. Weakness of which anatomical structure most likely contributed to this condition?
Options:
A. Transversalis fascia in posterior canal wall
B. Aponeurosis of external oblique
C. Fibers of internal oblique muscle
D. Deep inguinal ring margins
E. Inguinal ligament attachments
Correct Answer:
A. Transversalis fascia in posterior canal wall
Explanation:
Direct hernia occurs medial to inferior epigastric vessels due to weakness of posterior wall formed mainly by transversalis fascia.
MCQ 2
Question:
During abdominal surgery, a surgeon incises the anterior wall of the rectus sheath above the arcuate line. Which structure will be encountered immediately posterior to the rectus abdominis muscle at this level?
Options:
A. External oblique aponeurosis
B. Internal oblique anterior lamina
C. Transversalis fascia
D. Posterior lamina of internal oblique
E. Skin and superficial fascia
Correct Answer:
D. Posterior lamina of internal oblique
Explanation:
Above arcuate line, internal oblique splits into anterior and posterior laminae.
MCQ 3
Question:
A patient develops a painful swelling within the rectus sheath after blunt abdominal trauma. The swelling expands due to rupture of a vessel running within the sheath. Which vessel is most likely responsible?
Options:
A. Deep circumflex iliac artery
B. Superficial epigastric artery
C. Inferior epigastric artery
D. Lumbar artery branch
E. External iliac artery
Correct Answer:
C. Inferior epigastric artery
Explanation:
Inferior epigastric vessels lie within rectus sheath and are commonly injured.
MCQ 4
Question:
A surgeon repairing an inguinal hernia notes that contraction of muscles forming the roof of the canal compresses its lumen. Which physiological mechanism best explains this protective function?
Options:
A. Increased blood flow through epigastric vessels
B. Contraction of arching muscle fibers
C. Elastic recoil of superficial fascia
D. Movement of spermatic cord coverings
E. Inward displacement of skin layers
Correct Answer:
B. Contraction of arching muscle fibers
Explanation:
Internal oblique and transversus arching fibers compress canal (shutter mechanism).
MCQ 5
Question:
A 6-month-old infant presents with intermittent swelling in the scrotum since birth. The swelling increases during crying. Persistence of which embryological structure is most likely responsible?
Options:
A. Tunica albuginea
B. Processus vaginalis
C. Round ligament remnant
D. Umbilical vein
E. Mesonephric duct
Correct Answer:
B. Processus vaginalis
Explanation:
Patent processus vaginalis leads to congenital indirect hernia.
MCQ 6
Question:
A radiologist identifies a structure at the level of the transpyloric plane during abdominal imaging. Which structure is most likely visualized at this level?
Options:
A. Body of pancreas
B. Fundus of stomach
C. Neck of pancreas
D. Ascending colon
E. Urinary bladder
Correct Answer:
C. Neck of pancreas
Explanation:
Neck of pancreas lies at transpyloric plane (L1).
MCQ 7
Question:
A patient with chronic cough develops an inguinal hernia. Increased intra-abdominal pressure repeatedly acts on weak areas of the abdominal wall. Which muscle contributes most to maintaining abdominal pressure during forceful expiration?
Options:
A. Rectus femoris
B. Transversus abdominis
C. External intercostal
D. Latissimus dorsi
E. Quadratus lumborum
Correct Answer:
B. Transversus abdominis
Explanation:
Transversus abdominis compresses abdominal contents effectively.
MCQ 8
Question:
During dissection, a student observes that the posterior wall of the inguinal canal is reinforced medially by fusion of two aponeuroses. Which structure is being observed?
Options:
A. Inguinal ligament
B. Rectus sheath
C. Conjoint tendon
D. Semilunar line
E. Lacunar ligament
Correct Answer:
C. Conjoint tendon
Explanation:
Conjoint tendon strengthens posterior wall medially.
MCQ 9
Question:
A surgeon plans an incision along the linea alba to minimize bleeding. Which anatomical property of this structure makes it suitable for midline incision?
Options:
A. Contains numerous arteries
B. Consists mainly of muscle fibers
C. Formed by dense fibrous tissue
D. Contains lymphatic channels
E. Contains sensory nerves
Correct Answer:
C. Formed by dense fibrous tissue
Explanation:
Linea alba is fibrous and relatively avascular.
MCQ 10
Question:
A swelling appears below the inguinal ligament and lateral to the pubic tubercle in an elderly female. Which anatomical passage is most likely involved?
Options:
A. Deep inguinal ring
B. Superficial inguinal ring
C. Umbilical ring
D. Femoral canal
E. Obturator canal
Correct Answer:
D. Femoral canal
Explanation:
Femoral hernia occurs through femoral canal below inguinal ligament.
MCQ 11
Question:
A 45-year-old man presents with a reducible swelling in the groin that becomes tense during coughing. The swelling does not descend into the scrotum. Weakness in which anatomical region is most likely responsible?
Options:
A. Deep inguinal ring
B. Femoral canal
C. Hesselbach triangle
D. Umbilical ring
E. Linea semilunaris
Correct Answer:
C. Hesselbach triangle
Explanation:
Direct inguinal hernia occurs through Hesselbach triangle and usually does not reach the scrotum.
MCQ 12
Question:
During surgical repair of an inguinal hernia, the surgeon identifies the floor of the inguinal canal. Which structure forms the primary support of this region?
Options:
A. Lacunar ligament
B. Inguinal ligament
C. External oblique muscle
D. Internal oblique muscle
E. Rectus abdominis
Correct Answer:
B. Inguinal ligament
Explanation:
The inguinal ligament forms the main structural floor of the inguinal canal.
MCQ 13
Question:
A medical student palpates the lateral border of the rectus abdominis muscle during abdominal examination. Which anatomical landmark corresponds to this structure?
Options:
A. Linea alba
B. Linea semilunaris
C. Transumbilical plane
D. Midclavicular line
E. Costal margin
Correct Answer:
B. Linea semilunaris
Explanation:
Linea semilunaris marks the lateral border of rectus abdominis.
MCQ 14
Question:
During abdominal imaging, a surgeon identifies the hilum of the kidney at the same level as several other abdominal structures. This level corresponds to which anatomical plane?
Options:
A. Transumbilical plane
B. Subcostal plane
C. Intertubercular plane
D. Transpyloric plane
E. Median plane
Correct Answer:
D. Transpyloric plane
Explanation:
Kidney hilum lies approximately at the transpyloric plane (L1 level).
MCQ 15
Question:
A 60-year-old patient develops an abdominal wall bulge after previous surgery. The swelling occurs at the site of the surgical scar. Which structural property of healing tissue contributes to this condition?
Options:
A. Increased muscle elasticity
B. Dense vascular supply
C. Reduced tensile strength of scar tissue
D. Increased collagen cross-linking
E. Enhanced muscle contraction
Correct Answer:
C. Reduced tensile strength of scar tissue
Explanation:
Incisional hernia occurs due to weak scar tissue with reduced tensile strength.
MCQ 16
Question:
During dissection, a structure passing through the inguinal canal is found to regulate temperature of the testes by countercurrent heat exchange. Which structure performs this function?
Options:
A. Testicular artery
B. Vas deferens
C. Pampiniform plexus
D. Cremaster muscle
E. Genital branch of nerve
Correct Answer:
C. Pampiniform plexus
Explanation:
Pampiniform plexus cools arterial blood through countercurrent heat exchange.
MCQ 17
Question:
A patient experiences loss of sensation over the upper medial thigh following inguinal hernia repair. Injury to which nerve is most likely responsible?
Options:
A. Femoral nerve
B. Obturator nerve
C. Sciatic nerve
D. Ilioinguinal nerve
E. Pudendal nerve
Correct Answer:
D. Ilioinguinal nerve
Explanation:
Ilioinguinal nerve passes through inguinal canal and supplies upper medial thigh.
MCQ 18
Question:
During anatomical demonstration, a student notes that the anterior wall of the inguinal canal is strengthened laterally by fibers from which muscle?
Options:
A. Rectus abdominis
B. Transversus abdominis
C. Internal oblique
D. External intercostal
E. Pyramidalis
Correct Answer:
C. Internal oblique
Explanation:
Internal oblique fibers reinforce anterior wall laterally.
MCQ 19
Question:
A surgeon performs a midline incision through the abdomen to access internal organs. Minimal bleeding occurs due to the avascular nature of which structure?
Options:
A. Linea semilunaris
B. Umbilical ring
C. Inguinal ligament
D. Linea alba
E. Rectus sheath
Correct Answer:
D. Linea alba
Explanation:
Linea alba is relatively avascular, making it ideal for midline incisions.
MCQ 20
Question:
A patient with long-standing abdominal weakness develops protrusion of fat through a small defect in the linea alba above the umbilicus. Which type of hernia is most likely present?
Options:
A. Umbilical hernia
B. Femoral hernia
C. Epigastric hernia
D. Indirect inguinal hernia
E. Direct inguinal hernia
Correct Answer:
C. Epigastric hernia
Explanation:
Epigastric hernia occurs through defects in the linea alba above the umbilicus.
8. Post Test
Attempt Your Post Test Here
9. Explanation of Incorrect Answers
Incorrect answers are valuable learning opportunities. When reviewing MCQs, focus on understanding the concept behind the question, not just memorizing the correct option.
If you answered a question incorrectly:
• Identify the concept being tested.
• Determine why the correct option is correct.
• Understand why the other options are incorrect.
You can paste the MCQ into the AIM Tutor and ask for a step-by-step explanation. This helps strengthen conceptual understanding and improves reasoning for future questions.
Learning Tip
If your Post-Test score is below 80%, review the key concepts and attempt the Post-Test again to reinforce your understanding.
10. Student Memory Support
1️⃣ High-Yield Flashcards
Flashcard 1
Q: Which muscle has fibers running downward and medially (“hands in pockets”)?
A: External oblique
Flashcard 2
Q: Which abdominal muscle fibers run horizontally and act like a corset?
A: Transversus abdominis
Flashcard 3
Q: What structure encloses rectus abdominis muscle?
A: Rectus sheath
Flashcard 4
Q: What lies posterior to rectus abdominis below arcuate line?
A: Transversalis fascia
Flashcard 5
Q: At what vertebral level is the transpyloric plane located?
A: L1 vertebral level
Flashcard 6
Q: Which structure forms the posterior wall of inguinal canal?
A: Transversalis fascia
Flashcard 7
Q: Which structure forms the roof of inguinal canal?
A: Internal oblique and transversus abdominis
Flashcard 8
Q: Which nerve is found in the inguinal canal in both sexes?
A: Ilioinguinal nerve
Flashcard 9
Q: Indirect inguinal hernia occurs lateral to which vessels?
A: Inferior epigastric vessels
Flashcard 10
Q: Direct inguinal hernia occurs through which anatomical region?
A: Hesselbach triangle
Flashcard 11
Q: Which structure forms the floor of inguinal canal?
A: Inguinal ligament
Flashcard 12
Q: What forms the linea alba?
A: Fusion of abdominal muscle aponeuroses
2️⃣ Mnemonics
Mnemonic Title: Boundaries of Inguinal Canal
Mnemonic Word:
MALT
Meaning:
M → Muscle (Roof — Internal oblique & Transversus)
A → Aponeurosis (Anterior — External oblique)
L → Ligament (Floor — Inguinal ligament)
T → Transversalis fascia (Posterior wall)
Mnemonic Title: Transpyloric Plane Structures
Mnemonic Word:
“PPP KFD”
Meaning:
P → Pylorus
P → Pancreas (neck)
P → Portal vein formation
K → Kidney hilum
F → Fundus of gallbladder
D → Duodenojejunal flexure
Mnemonic Title: Hesselbach Triangle Boundaries
Mnemonic Word:
“RIP”
Meaning:
R → Rectus abdominis (Medial)
I → Inferior epigastric vessels (Lateral)
P → Poupart’s ligament (Inguinal ligament — Inferior)
3️⃣ Memory Tables
Table 1 — Direct vs Indirect Inguinal Hernia
| Feature | Indirect Hernia | Direct Hernia |
| Relation to inferior epigastric vessels | Lateral | Medial |
| Entry point | Deep inguinal ring | Posterior wall |
| Pathway | Through canal | Through Hesselbach triangle |
| Reaches scrotum | Common | Rare |
| Cause | Congenital | Acquired |
Table 2 — Rectus Sheath Above vs Below Arcuate Line
| Feature | Above Arcuate Line | Below Arcuate Line |
| Posterior wall | Present | Absent |
| Internal oblique | Splits | Does not split |
| Posterior layer | Strong | Weak |
| Hernia risk | Lower | Higher |
4️⃣ Rapid Revision Points
Must Remember:
• External oblique fibers run downward & medially
• Internal oblique fibers run upward & medially
• Transversus fibers run horizontally
• Rectus sheath posterior wall weak below arcuate line
• Inguinal canal length ≈ 4 cm
• Deep ring lies lateral to inferior epigastric vessels
• Direct hernia → medial to inferior epigastric vessels
• Indirect hernia → lateral to inferior epigastric vessels
• Hesselbach triangle → site of direct hernia
• Ilioinguinal nerve present in both sexes
5️⃣ Clinical Memory Hooks
Clinical Hook 1:
Indirect Inguinal Hernia → Patent processus vaginalis
Clinical Hook 2:
Direct Inguinal Hernia → Weak posterior wall (Hesselbach triangle)
Clinical Hook 3:
Femoral Hernia → Swelling below inguinal ligament
Clinical Hook 4:
Rectus Sheath Hematoma → Injury to inferior epigastric vessels
Clinical Hook 5:
Midline Surgical Incision → Made through linea alba (avascular)
✔ Topic Completion
📊 Your Performance
Pre-Test: Not Attempted
Post-Test: Not Attempted
Improvement: --