
This topic uses the AIM Learning Cycle to help MBBS students understand the structural organization of the peritoneum and its spaces by integrating Anatomy and Clinical concepts.
1. Curriculum Coverage
Anatomy
• Greater omentum
• Lesser omentum
• Nerve supply of peritoneum
• Lesser sac
• Boundaries of epiploic foramen
• Peritoneal pouches
• Peritoneal recesses
• Peritoneal ligaments
📚 Standard Reference Framework
Primary Anatomy Reference:
BD Chaurasia — Standard Undergraduate Depth
Concept Support:
Gray’s Anatomy for Students
Spatial Atlas:
Netter Atlas
Physiology:
Guyton & Hall
Histology:
DiFiore Atlas
Biochemistry:
Lippincott Illustrated Reviews
🎯 Depth Policy
All content is restricted to Undergraduate MBBS Level.
Depth will not exceed BD Chaurasia standard.
1️⃣ Introduction
The peritoneum is the largest serous membrane of the body and plays a crucial role in supporting abdominal organs and allowing their smooth movement during digestion. It is located within the abdominal and pelvic cavities, lining the walls and covering the viscera. The peritoneum forms folds, sacs, ligaments, and recesses that organize the abdominal organs and provide pathways for blood vessels and nerves.
Clinically, understanding the peritoneum is essential because infections, fluid collections, internal hernias, and abdominal surgeries involve these spaces. Conditions such as peritonitis, ascites, and internal hernias directly relate to peritoneal anatomy.
2️⃣ Foundation Basics
Key Definitions
- Peritoneum → A continuous serous membrane lining the abdominal cavity and covering abdominal organs.
- Parietal peritoneum → Lines abdominal wall.
- Visceral peritoneum → Covers abdominal organs.
- Peritoneal cavity → Potential space between parietal and visceral layers containing small amount of fluid.
- Mesentery → Double layer of peritoneum attaching organs to posterior abdominal wall.
- Omentum → Peritoneal fold connecting stomach to other organs.
- Peritoneal ligament → Double-layered peritoneal fold connecting organ to organ or wall.
- Sac → Large peritoneal compartment (greater sac or lesser sac).
- Recess → Small pocket formed by peritoneal folds.
- Pouch → Dependent space where fluid accumulates.
3️⃣ Core Learning — Curriculum Coverage
🧠 CORE
• A large apron-like fold of peritoneum hanging from the greater curvature of stomach.
• Located anterior to intestines, covering abdominal organs.
• Extends downward from stomach, then folds upward to attach to transverse colon.
• Made of four layers of peritoneum.
• Contains:
o Fat deposits
o Blood vessels
o Lymphatics
o Immune cells
• Major Blood Supply:
o Right gastroepiploic artery (from gastroduodenal artery)
o Left gastroepiploic artery (from splenic artery)
• Function:
o Protection
o Fat storage
o Infection control
o Insulation
🔬 CONCEPT EXPLAINED
The greater omentum develops from the dorsal mesogastrium. It hangs like an apron in front of the intestines, forming a protective barrier. Because it contains fat and immune cells, it can move toward inflamed areas, such as an infected appendix.
Structure → Function Logic:
• Large surface area → Covers intestines
• Fat content → Cushions organs
• Mobility → Helps isolate infection
It acts like the “policeman of the abdomen”, limiting spread of infection.
⚠️ IF DAMAGED
Cause: Injury or infection
Effect:
• Reduced infection containment
• Spread of peritonitis
• Increased risk of abscess formation
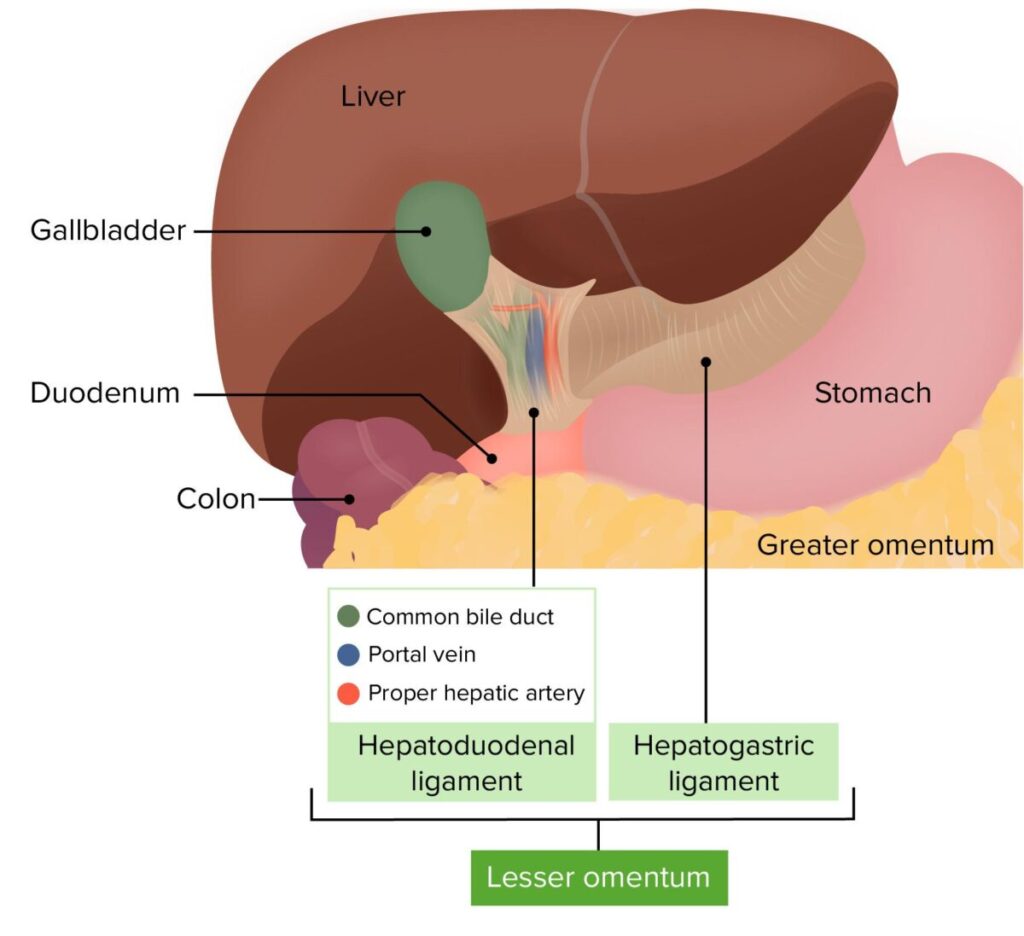
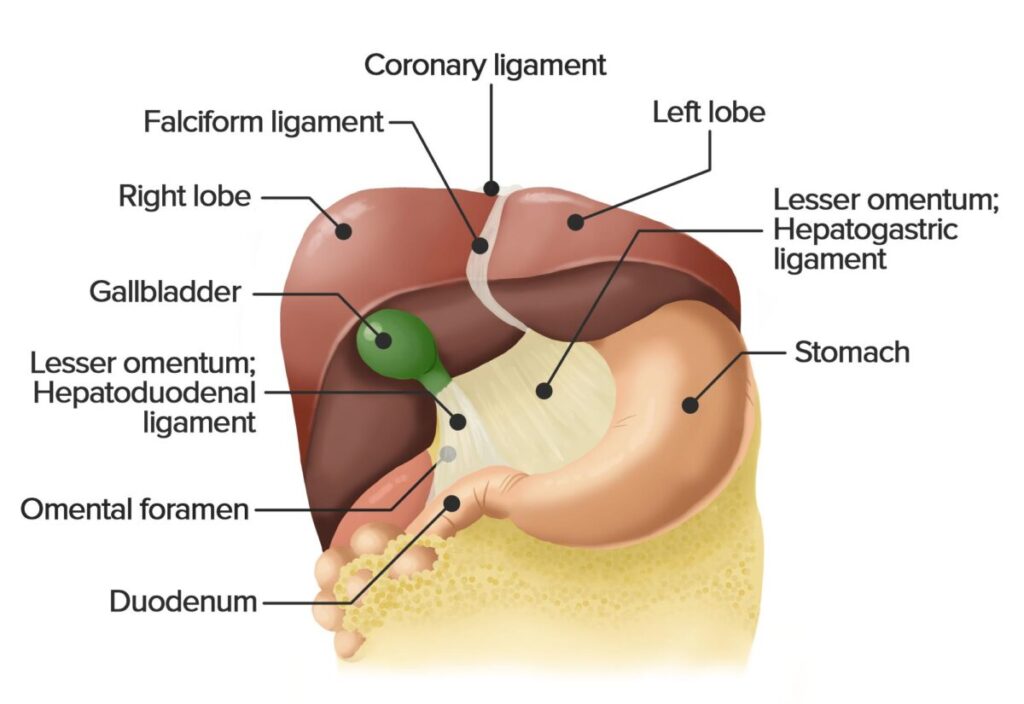
🧠 CORE
• Thin double-layered peritoneal fold.
• Connects:
o Liver → Lesser curvature of stomach
o Liver → First part of duodenum
• Located between liver and stomach.
• Parts:
o Hepatogastric ligament
o Hepatoduodenal ligament
• Contents of hepatoduodenal ligament:
o Portal vein
o Hepatic artery proper
o Common bile duct
• Blood Supply:
o Hepatic arterial branches
Primary Function:
• Provides pathway for major vessels entering liver.
🔬 CONCEPT EXPLAINED
The lesser omentum develops from the ventral mesogastrium. It acts as a support structure holding the liver in position while allowing passage of vessels.
Structure → Function Logic:
Thin membrane → Flexible movement
Strong attachments → Stable vascular pathway
⚠️ IF DAMAGED
Cause: Trauma or surgery
Effect:
• Portal triad injury
• Severe bleeding
• Bile leakage
🧠 CORE
Two types of innervation:
Parietal Peritoneum
• Somatic nerve supply
• Highly sensitive to:
o Pain
o Pressure
o Temperature
Nerves:
• Lower intercostal nerves
• Lumbar nerves
• Phrenic nerve (central diaphragm)
Visceral Peritoneum
• Autonomic nerve supply
• Sensitive to:
o Stretch
o Chemical irritation
Nerves:
• Sympathetic nerves
• Parasympathetic nerves
🔬 CONCEPT EXPLAINED
Parietal peritoneum has somatic nerves similar to skin, so pain is sharp and localized.
Visceral peritoneum has autonomic nerves, so pain is dull and poorly localized.
Structure → Function Logic:
Somatic nerves → Precise localization
Autonomic nerves → Diffuse visceral pain
⚠️ IF DAMAGED
Cause: Inflammation (peritonitis)
Effect:
• Sharp localized pain when parietal peritoneum involved
• Guarding of abdominal wall
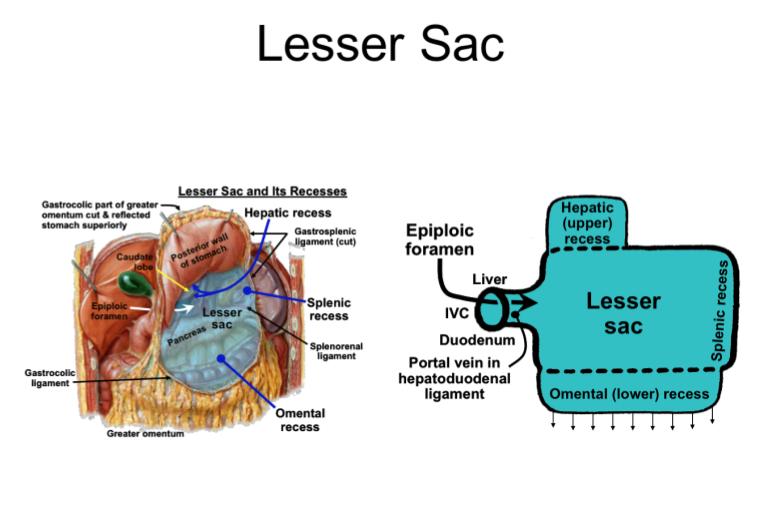
🧠 CORE
• A peritoneal cavity space located posterior to stomach.
• Lies between stomach and pancreas.
• Communicates with greater sac through epiploic foramen.
• Boundaries:
Anterior:
• Stomach
• Lesser omentum
Posterior:
• Pancreas
Superior:
• Liver
Inferior:
• Transverse colon
Function:
• Allows free movement of stomach.
🔬 CONCEPT EXPLAINED
The lesser sac forms due to rotation of the stomach during development. It creates a space behind the stomach, allowing stomach expansion during digestion.
Structure → Function Logic:
Posterior cavity → Allows stomach mobility
⚠️ IF DAMAGED
Cause: Pancreatitis
Effect:
• Fluid accumulation in lesser sac
• Abscess formation
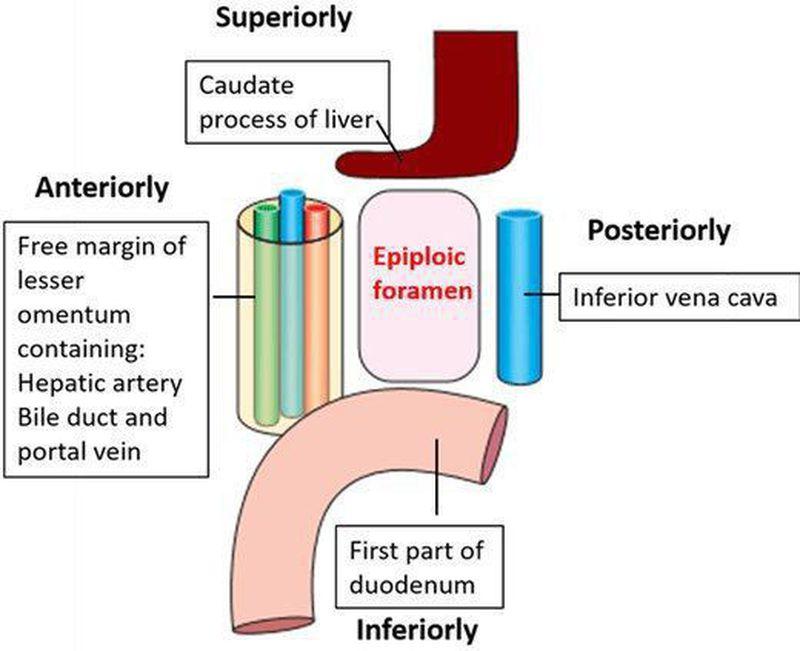
🧠 CORE
Also called Foramen of Winslow.
Connects:
• Lesser sac ↔ Greater sac
Boundaries:
Anterior:
• Hepatoduodenal ligament
Posterior:
• Inferior vena cava
Superior:
• Caudate lobe of liver
Inferior:
• First part of duodenum
Contents:
• Passage between sacs
🔬 CONCEPT EXPLAINED
The epiploic foramen acts as a gateway between peritoneal compartments.
Structure → Function Logic:
Small opening → Controls communication between sacs
⚠️ IF DAMAGED
Cause: Internal hernia
Effect:
• Intestinal obstruction
• Compromised blood supply
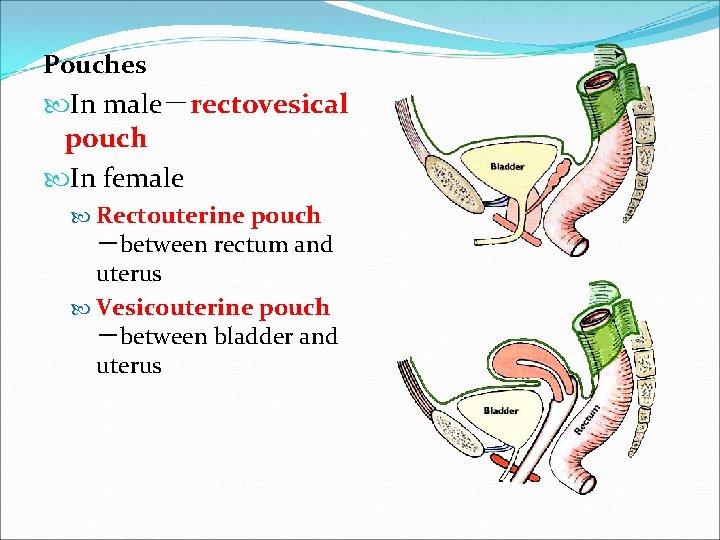
🧠 CORE
Spaces where fluid accumulates.
Male
• Rectovesical pouch
o Between rectum and bladder
Female
• Uterovesical pouch
• Rectouterine pouch (Pouch of Douglas)
Function:
• Lowest point of peritoneal cavity
• Fluid collection site
🔬 CONCEPT EXPLAINED
Gravity causes fluid (blood, pus, ascites) to collect in dependent regions.
Structure → Function Logic:
Dependent location → Fluid accumulation
⚠️ IF DAMAGED
Cause: Infection
Effect:
• Abscess formation
• Pelvic pain
🧠 CORE
Small pockets formed by folds of peritoneum.
Examples:
• Duodenal recess
• Cecal recess
• Intersigmoid recess
Function:
• Allows organ movement
🔬 CONCEPT EXPLAINED
These recesses are spaces formed during gut rotation.
Structure → Function Logic:
Folds → Space formation → Organ flexibility
⚠️ IF DAMAGED
Cause: Herniation
Effect:
• Internal hernia
• Intestinal obstruction
🧠 CORE
Double-layered folds connecting organs.
Examples:
• Falciform ligament
• Gastrosplenic ligament
• Splenorenal ligament
Function:
• Organ stabilization
• Vessel support
🔬 CONCEPT EXPLAINED
Ligaments act as structural supports carrying vessels.
Structure → Function Logic:
Double layer → Strength + vessel passage
⚠️ IF DAMAGED
Cause: Trauma
Effect:
• Organ displacement
• Bleeding
Recommended video
3. PRE-TEST MCQs
Results




#1. A large apron-like fold hanging from the greater curvature of the stomach is known as:
#2. The lesser omentum connects the liver to which of the following structures?
#3. Pain from parietal peritoneum is typically:
#4. Which structure forms the posterior boundary of the epiploic foramen?
#5. The lesser sac is located primarily:
#6. Which of the following structures forms the anterior boundary of the epiploic foramen?
#7. The rectouterine pouch in females is also known as:
#8. Which of the following peritoneal ligaments connects the spleen to the kidney?
#9. The nerve supply to the visceral peritoneum is mainly:
#10. Which structure forms the superior boundary of the epiploic foramen?
#11. The peritoneal pouch present in males between bladder and rectum is:
#12. The greater omentum develops from which embryological structure?
#13. Which of the following structures forms the inferior boundary of the epiploic foramen?
#14. Which peritoneal ligament attaches the liver to the anterior abdominal wall?
#15. Which of the following is most likely to accumulate fluid in the female pelvis?
#16. Which structure forms the communication between the greater and lesser sacs?
#17. Which peritoneal structure is primarily responsible for limiting spread of infection in the abdomen?
#18. Pain arising from visceral peritoneum is typically:
#19. Which of the following is an example of a peritoneal recess?
#20. Which ligament contains the portal triad?
4. Diagnostic Feedback
Your score in this pre-test reflects your current level of understanding of the topic.
Score 0–7 → Foundational Level
You may not yet be familiar with the basic concepts of connective tissue structure and biochemistry.
Focus on understanding the components of extracellular matrix, collagen structure, glycosaminoglycans, and proteoglycans before attempting more advanced questions.
Score 8–14 → Developing Understanding
You have a partial understanding of connective tissue components and their functions.
Review the relationships between collagen fibers, extracellular matrix proteins, and ground substance, and how these components contribute to tissue strength and elasticity.
Score 15–20 → Strong Conceptual Base
You already have a solid understanding of connective tissue biochemistry and structure.
As you proceed through the learning material, focus on integrating histological structure with biochemical mechanisms and physiological functions.
5. Guided Reasoning
Ask AIM Tutor
I answered this MCQ incorrectly in my MBBS learning module.
Please help me understand:
1. What concept is being tested in this question?
2. Why is the correct option correct?
3. Why are the other options incorrect?
4. What is the key concept I should remember for exams?
Here is the MCQ:
6. Concept Integration
1️⃣ MASTER INTEGRATION CHAIN
Whole Topic Core Flow
Peritoneum Structure Organization
(Parietal layer + Visceral layer + Omenta + Ligaments + Sacs + Pouches)
⬇
Normal Functional Roles
Peritoneal Fluid
→ Reduces friction between organs
Omenta & Ligaments
→ Support organs
→ Carry vessels (portal triad in hepatoduodenal ligament)
Peritoneal Spaces
→ Allow organ movement
→ Provide pathways for fluid movement
Peritoneal Nerve Supply
→ Parietal → Sharp localized pain
→ Visceral → Dull poorly localized pain
⬇
Failure / Disease Development
Infection or injury
→ Peritonitis
→ Fluid/pus spreads through sacs & recesses
Portal triad compression
→ Impaired hepatic blood flow
Internal herniation through recesses
→ Intestinal obstruction
Fluid accumulation in dependent pouches
→ Ascites or pelvic abscess
⬇
Drug / Treatment Action
Antibiotics
→ Control infection in peritoneal cavity
Diuretics
→ Reduce ascitic fluid
Surgical drainage
→ Remove pus from pouches (e.g., Douglas pouch)
Supportive fluid therapy
→ Maintain circulation during peritonitis
3️⃣ CORE MECHANISM INTEGRATION
Main Functional Breakdown Mechanism — Peritonitis
Infection enters peritoneal cavity
(e.g., ruptured appendix)
⬇
Inflammation of Peritoneum
Mesothelial irritation
→ Increased vascular permeability
⬇
Fluid & Pus Accumulation
Fluid spreads through:
→ Greater sac
→ Lesser sac
→ Peritoneal recesses
→ Pelvic pouches
⬇
Peritoneal Nerve Stimulation
Parietal peritoneum irritation
→ Sharp localized abdominal pain
Visceral peritoneum irritation
→ Dull diffuse pain
⬇
Functional Consequences
Abdominal guarding
↓
Reduced intestinal movement
↓
Risk of obstruction or sepsis
4️⃣ CLINICAL INTEGRATION SNAPSHOT
Clinical Flow 1 — Peritonitis
Pathology:
Appendix rupture
⬇
Mechanism:
Bacteria enter peritoneal cavity
→ Inflammation spreads via peritoneal spaces
⬇
Symptoms:
Severe abdominal pain
Guarding
Fever
⬇
Treatment:
Antibiotics
Surgical removal of source
Drainage of infected pouches
Clinical Flow 2 — Ascites
Pathology:
Liver disease (portal hypertension)
⬇
Mechanism:
Increased portal pressure
→ Fluid leaks into peritoneal cavity
⬇
Fluid Distribution:
Collects in:
→ Hepatorenal pouch
→ Rectouterine pouch
→ Rectovesical pouch
⬇
Symptoms:
Abdominal distension
Fluid wave
⬇
Treatment:
Diuretics
Paracentesis
5️⃣ ULTRA-HIGH-YIELD MASTER SUMMARY
Last-Day Revision Model
Normal Function
Peritoneum
→ Supports organs
→ Allows friction-free movement
→ Provides fluid pathways
→ Forms sacs, ligaments, pouches
⬇
Disease Mechanism
Infection or fluid leakage
→ Spreads through sacs & recesses
→ Accumulates in dependent pouches
→ Causes peritonitis or ascites
⬇
Drug Action
Antibiotics
→ Control infection
Diuretics
→ Reduce fluid
⬇
Treatment Effect
Drainage + Surgery
→ Removes infection
→ Restores abdominal function
MCQ 1
Question:
A 45-year-old male presents with acute pancreatitis. Imaging shows fluid accumulation confined posterior to the stomach and anterior to the pancreas. Which peritoneal compartment is most likely involved?
Options:
A. Right subphrenic space
B. Lesser sac
C. Greater sac
D. Hepatorenal pouch
E. Left paracolic gutter
Correct Answer:
B. Lesser sac
Explanation:
The lesser sac lies posterior to the stomach and is commonly involved in pancreatitis-related fluid collection.
MCQ 2
Question:
During surgical control of hepatic bleeding, the surgeon compresses structures within the hepatoduodenal ligament. Which anatomical structure lies posterior to this ligament and forms the posterior boundary of the epiploic foramen?
Options:
A. Abdominal aorta
B. Portal vein
C. Inferior vena cava
D. Common hepatic artery
E. Right renal vein
Correct Answer:
C. Inferior vena cava
Explanation:
The inferior vena cava forms the posterior boundary of the epiploic foramen.
MCQ 3
Question:
A patient with generalized peritonitis complains of sharp localized pain when pressure is applied to the abdominal wall. Which feature of the involved structure explains this clinical finding?
Options:
A. Autonomic nerve supply
B. Visceral afferent fibers
C. Somatic sensory innervation
D. Lack of pain receptors
E. Sympathetic nerve predominance
Correct Answer:
C. Somatic sensory innervation
Explanation:
Parietal peritoneum receives somatic nerves, producing sharp localized pain.
MCQ 4
Question:
During laparoscopic examination of a female patient, purulent fluid is found collecting in the most dependent pelvic region while the patient is lying supine. Which anatomical space is most likely involved?
Options:
A. Rectouterine pouch
B. Uterovesical pouch
C. Intersigmoid recess
D. Right paracolic gutter
E. Subhepatic pouch
Correct Answer:
A. Rectouterine pouch
Explanation:
The rectouterine pouch is the lowest point in the female pelvis, making it the most common site for fluid collection.
MCQ 5
Question:
A patient develops intestinal obstruction due to internal herniation of bowel loops into a peritoneal fold near the duodenum. Which structure is most likely responsible?
Options:
A. Lesser omentum
B. Duodenal recess
C. Greater omentum
D. Splenorenal ligament
E. Falciform ligament
Correct Answer:
B. Duodenal recess
Explanation:
Duodenal recesses are common sites for internal hernias causing obstruction.
MCQ 6
Question:
During splenectomy, a surgeon ligates vessels within a peritoneal fold connecting the stomach to the spleen. Which ligament is being divided?
Options:
A. Falciform ligament
B. Gastrosplenic ligament
C. Hepatoduodenal ligament
D. Splenorenal ligament
E. Lesser omentum
Correct Answer:
B. Gastrosplenic ligament
Explanation:
The gastrosplenic ligament connects the stomach to the spleen and contains short gastric vessels.
MCQ 7
Question:
In a patient with severe abdominal infection, inflammatory spread is limited to a localized region due to the protective function of a fatty peritoneal structure. Which anatomical feature is responsible for this protective effect?
Options:
A. High vascular resistance
B. Dense fibrous tissue
C. Aggregates of immune cells
D. Thick muscular layers
E. Reduced lymphatic drainage
Correct Answer:
C. Aggregates of immune cells
Explanation:
The greater omentum contains lymphoid tissue that helps contain infection.
MCQ 8
Question:
Fluid from an upper abdominal infection spreads inferiorly along the lateral abdominal wall into the pelvic cavity. Through which anatomical pathway does this movement most likely occur?
Options:
A. Left paracolic gutter
B. Right paracolic gutter
C. Lesser sac
D. Falciform ligament
E. Hepatogastric ligament
Correct Answer:
B. Right paracolic gutter
Explanation:
The right paracolic gutter allows fluid movement from upper abdomen to pelvis.
MCQ 9
Question:
A traumatic injury damages the ligament connecting the liver to the anterior abdominal wall. Which functional consequence is most likely?
Options:
A. Impaired portal circulation
B. Reduced hepatic venous drainage
C. Loss of structural support to liver
D. Obstruction of bile flow
E. Compression of hepatic artery
Correct Answer:
C. Loss of structural support to liver
Explanation:
The falciform ligament provides support to the liver by attaching it to the anterior abdominal wall.
MCQ 10
Question:
Radiological contrast introduced into the greater sac is later detected within another peritoneal compartment posterior to the stomach. Through which structure did this communication most likely occur?
Options:
A. Epiploic foramen
B. Duodenal recess
C. Transverse mesocolon
D. Hepatogastric ligament
E. Splenorenal ligament
Correct Answer:
A. Epiploic foramen
Explanation:
The epiploic foramen connects the greater sac to the lesser sac.
MCQ 11
Question:
A 50-year-old patient develops a perforated gastric ulcer along the posterior wall of the stomach. Leakage of gastric contents is initially confined to a specific peritoneal compartment before spreading elsewhere. Which space is most likely to first receive the leaked contents?
Options:
A. Right subphrenic space
B. Greater sac
C. Lesser sac
D. Hepatorenal pouch
E. Left paracolic gutter
Correct Answer:
C. Lesser sac
Explanation:
Posterior gastric perforations typically leak into the lesser sac, located behind the stomach.
MCQ 12
Question:
During liver surgery, a surgeon passes a finger through the epiploic foramen to temporarily control hemorrhage from hepatic vessels. Which structure lies immediately anterior to the surgeon’s finger during this maneuver?
Options:
A. Inferior vena cava
B. Hepatoduodenal ligament
C. Pancreatic head
D. First part of duodenum
E. Caudate lobe of liver
Correct Answer:
B. Hepatoduodenal ligament
Explanation:
The hepatoduodenal ligament forms the anterior boundary of the epiploic foramen.
MCQ 13
Question:
A patient presents with dull poorly localized abdominal pain during early appendicitis. This pain characteristic is primarily due to involvement of which anatomical component?
Options:
A. Parietal peritoneum
B. Visceral peritoneum
C. Falciform ligament
D. Greater omentum
E. Mesenteric root
Correct Answer:
B. Visceral peritoneum
Explanation:
Visceral peritoneum has autonomic innervation producing dull poorly localized pain.
MCQ 14
Question:
During splenic trauma, bleeding spreads into a peritoneal fold that connects the spleen to the posterior abdominal wall and contains splenic vessels. Which structure is involved?
Options:
A. Gastrosplenic ligament
B. Splenorenal ligament
C. Hepatogastric ligament
D. Falciform ligament
E. Lesser omentum
Correct Answer:
B. Splenorenal ligament
Explanation:
The splenorenal ligament connects the spleen to the posterior abdominal wall and carries splenic vessels.
MCQ 15
Question:
A patient with advanced liver cirrhosis develops significant ascites. While lying supine, fluid preferentially accumulates in the hepatorenal pouch. Which anatomical relationship explains this phenomenon?
Options:
A. Most anterior abdominal recess
B. Highest abdominal cavity region
C. Most dependent posterior abdominal space
D. Closest space to diaphragm
E. Region with highest lymphatic drainage
Correct Answer:
C. Most dependent posterior abdominal space
Explanation:
Morison pouch (hepatorenal pouch) is the lowest posterior space when supine.
MCQ 16
Question:
A surgical trainee mistakenly injures the structure carrying the portal triad during a cholecystectomy. Which ligament has most likely been damaged?
Options:
A. Hepatogastric ligament
B. Gastrosplenic ligament
C. Splenorenal ligament
D. Hepatoduodenal ligament
E. Falciform ligament
Correct Answer:
D. Hepatoduodenal ligament
Explanation:
The portal triad lies within the hepatoduodenal ligament.
MCQ 17
Question:
A loop of intestine becomes trapped within a peritoneal recess near the sigmoid colon, resulting in bowel obstruction. Which recess is most likely responsible?
Options:
A. Duodenal recess
B. Retrocecal recess
C. Intersigmoid recess
D. Subhepatic recess
E. Right paracolic gutter
Correct Answer:
C. Intersigmoid recess
Explanation:
The intersigmoid recess near the sigmoid colon is a known site for internal herniation.
MCQ 18
Question:
A patient undergoing abdominal surgery experiences irritation of the central part of the diaphragmatic peritoneum. Pain from this region is most likely referred to which area?
Options:
A. Lower back
B. Umbilical region
C. Shoulder region
D. Inguinal region
E. Epigastric region
Correct Answer:
C. Shoulder region
Explanation:
Central diaphragmatic peritoneum is supplied by the phrenic nerve, causing referred shoulder pain.
MCQ 19
Question:
A localized intra-abdominal infection is observed to be surrounded and isolated by a fatty peritoneal structure. Which structural property of this tissue allows this protective role?
Options:
A. High collagen density
B. Smooth muscle contraction
C. Presence of mesothelial folds
D. Mobility within abdominal cavity
E. Fixed attachment to diaphragm
Correct Answer:
D. Mobility within abdominal cavity
Explanation:
The greater omentum can migrate to sites of inflammation, limiting spread.
MCQ 20
Question:
During abdominal imaging, a congenital abnormality is found in which a peritoneal fold fails to properly form, leading to increased intestinal mobility and risk of twisting. Which functional role of normal peritoneal folds has been lost?
Options:
A. Regulation of digestive enzymes
B. Storage of abdominal fat
C. Stabilization of visceral organs
D. Production of peritoneal fluid
E. Absorption of bile salts
Correct Answer:
C. Stabilization of visceral organs
Explanation:
Peritoneal folds normally stabilize organs and limit excessive mobility.
8. Post-Test
Attempt Your Post Test Here
9. Explanation of Incorrect Answers
Incorrect answers are valuable learning opportunities. When reviewing MCQs, focus on understanding the concept behind the question, not just memorizing the correct option.
If you answered a question incorrectly:
• Identify the concept being tested.
• Determine why the correct option is correct.
• Understand why the other options are incorrect.
You can paste the MCQ into the AIM Tutor and ask for a step-by-step explanation. This helps strengthen conceptual understanding and improves reasoning for future questions.
Learning Tip
If your Post-Test score is below 80%, review the key concepts and attempt the Post-Test again to reinforce your understanding.
10. Student Memory Support
1️⃣High-Yield Flashcards
Flashcard 1
Q: What is the greater omentum commonly called due to its protective function?
A: Policeman of the abdomen
Flashcard 2
Q: From which structure does the greater omentum hang?
A: Greater curvature of stomach
Flashcard 3
Q: Which ligament contains the portal triad?
A: Hepatoduodenal ligament
Flashcard 4
Q: What are the contents of the portal triad?
A: Portal vein, hepatic artery, bile duct
Flashcard 5
Q: Where is the lesser sac located?
A: Behind stomach and in front of pancreas
Flashcard 6
Q: Which structure connects the greater and lesser sacs?
A: Epiploic foramen
Flashcard 7
Q: Which nerve type supplies parietal peritoneum?
A: Somatic nerves
Flashcard 8
Q: How is visceral peritoneal pain typically described?
A: Dull and poorly localized
Flashcard 9
Q: What is the lowest peritoneal pouch in females?
A: Rectouterine pouch (Douglas pouch)
Flashcard 10
Q: What is the lowest peritoneal pouch in males?
A: Rectovesical pouch
Flashcard 11
Q: Which ligament connects stomach to spleen?
A: Gastrosplenic ligament
Flashcard 12
Q: Which ligament connects spleen to kidney?
A: Splenorenal ligament
2️⃣Mnemonics
Mnemonic Title: Epiploic Foramen Boundaries
Mnemonic Word:
DIP C
Meaning:
D → Duodenum (Inferior)
I → Inferior vena cava (Posterior)
P → Portal triad (Anterior)
C → Caudate lobe (Superior)
Mnemonic Title: Portal Triad Contents
Mnemonic Word:
DVA
Meaning:
D → Duct (Bile duct)
V → Vein (Portal vein)
A → Artery (Hepatic artery)
Mnemonic Title: Female Pelvic Pouches
Mnemonic Word:
UR
Meaning:
U → Uterovesical pouch
R → Rectouterine pouch
3️⃣Memory Tables
Table 1 — Greater vs Lesser Omentum
| Feature | Greater Omentum | Lesser Omentum |
| Origin | Greater curvature | Lesser curvature |
| Direction | Hangs over intestines | Connects liver to stomach |
| Layers | Four layers | Two layers |
| Main Role | Protection & infection control | Carries portal triad |
Table 2 — Parietal vs Visceral Peritoneum
| Feature | Parietal Peritoneum | Visceral Peritoneum |
| Nerve Supply | Somatic | Autonomic |
| Pain Type | Sharp & localized | Dull & poorly localized |
| Sensitivity | Pressure & temperature | Stretch & distension |
| Clinical Significance | Causes guarding | Causes vague abdominal pain |
4️⃣Rapid Revision Points (Last-Minute Revision)
Must Remember:
• Greater omentum = policeman of abdomen
• Lesser sac lies behind stomach
• Epiploic foramen connects two sacs
• Portal triad lies in hepatoduodenal ligament
• Inferior vena cava forms posterior boundary of epiploic foramen
• Parietal peritoneum pain is sharp and localized
• Visceral peritoneum pain is dull and poorly localized
• Rectouterine pouch is lowest pelvic space in females
• Rectovesical pouch is lowest pelvic space in males
• Peritoneal recesses are sites of internal hernia
• Peritoneal ligaments carry vessels between organs
5️⃣Clinical Memory Hooks
Clinical Hook 1:
Pancreatitis → Fluid collects in lesser sac
Clinical Hook 2:
Pelvic abscess → Fluid collects in rectouterine pouch
Clinical Hook 3:
Peritonitis → Sharp pain occurs when parietal peritoneum is irritated
Clinical Hook 4:
Internal hernia → Commonly occurs in peritoneal recesses
Clinical Hook 5:
Severe liver bleeding → Portal triad compressed in hepatoduodenal ligament