🩺 Station 10 — Cerebellar Examination
AIM OSPE/OSCE Lab — Practical Station | KMU Style | MBBS Practical + Viva
📋 Complete OSPE Station Content
OSPE Station Name
Station 10 — Cerebellar Examination
Learning Target
By the end of this station, the student should be able to:
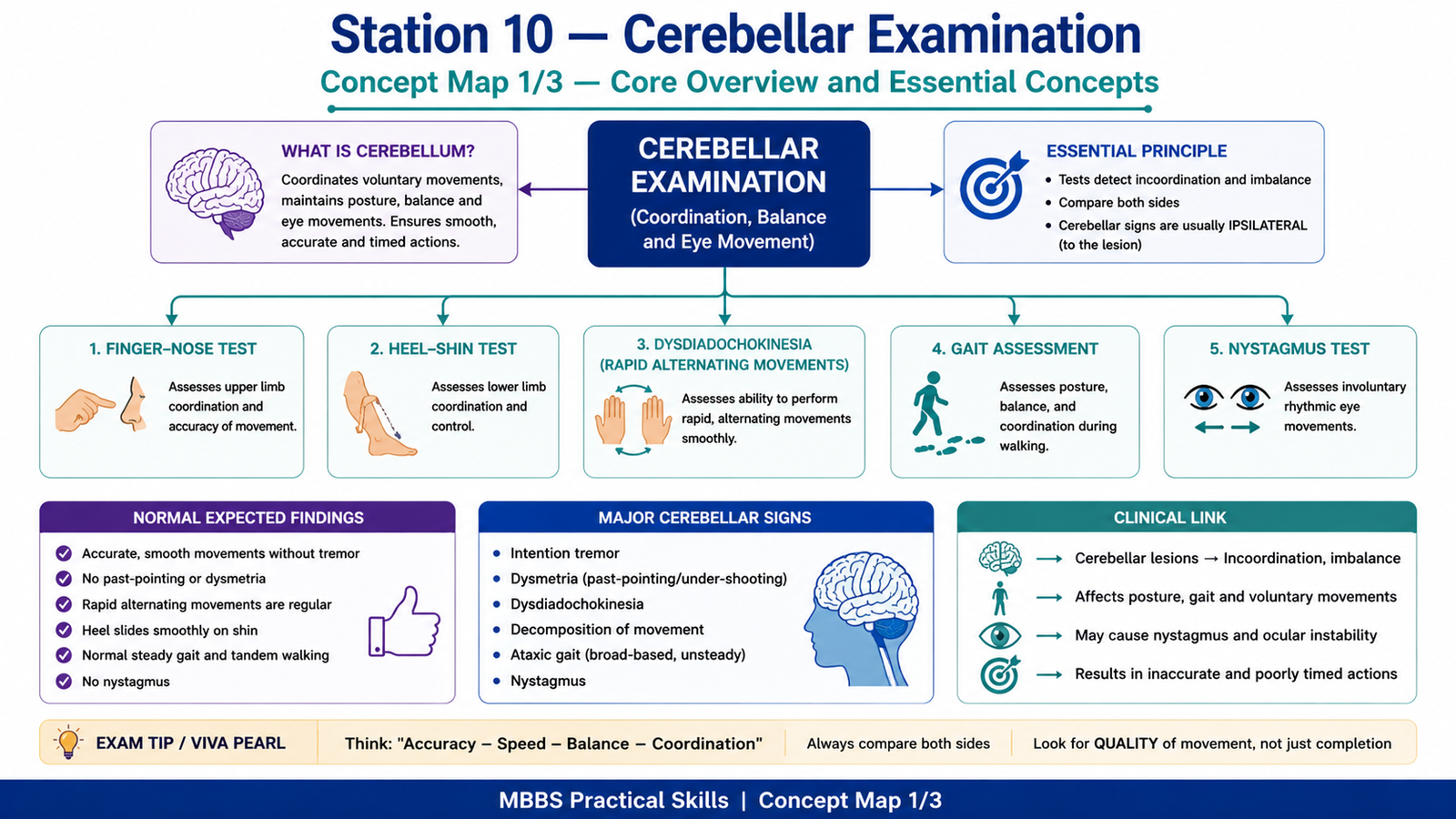
- Perform basic cerebellar examination, including finger-nose test, heel-shin test, dysdiadochokinesia, gait assessment, and nystagmus testing.
- Identify common cerebellar signs and interpret their clinical significance at MBBS level.
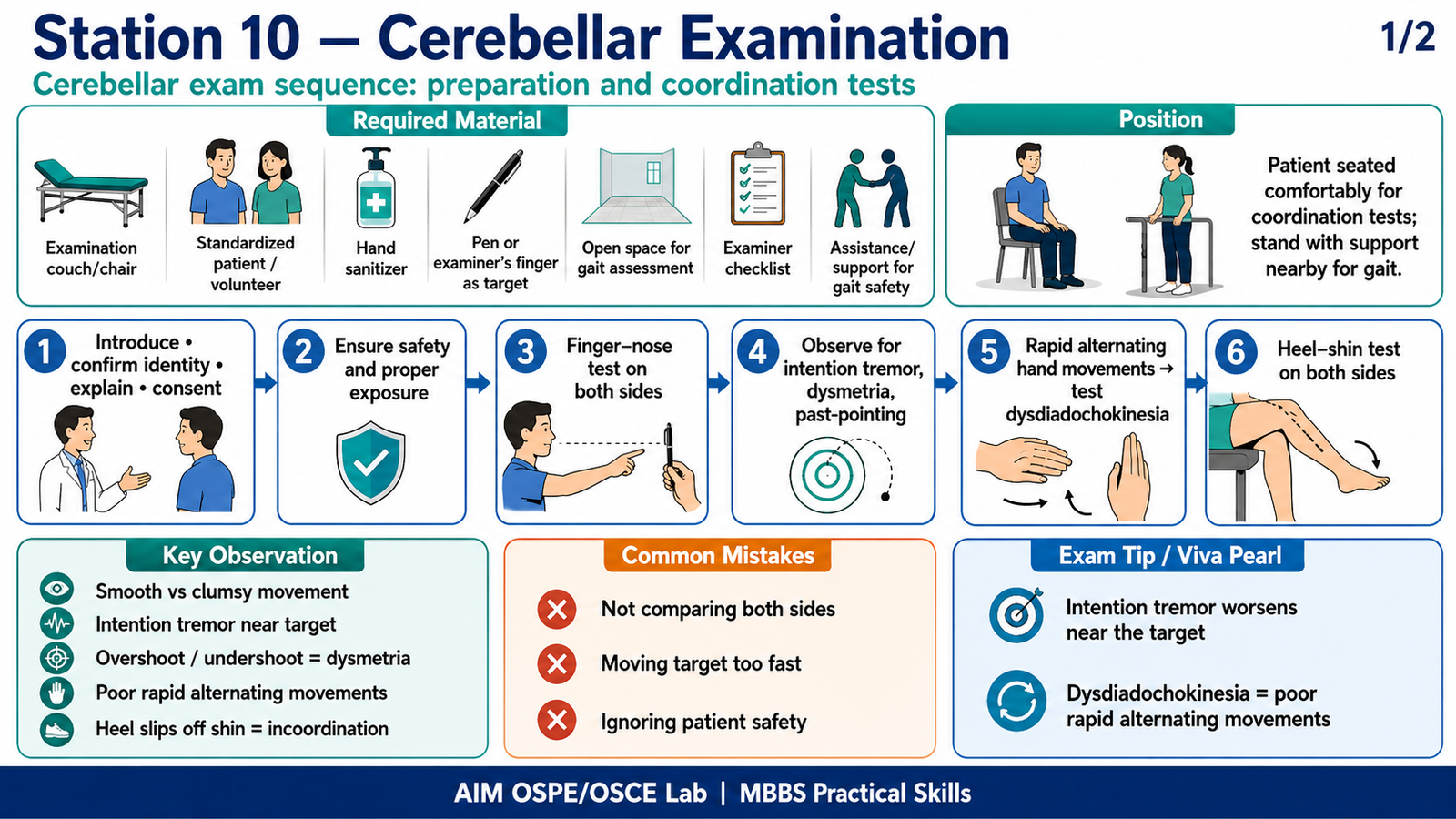
Required Material
- Examination couch or chair
- Standardized patient / volunteer
- Hand sanitizer
- Pen or examiner’s finger as target
- Open space for gait assessment
- Examiner checklist
- Assistance/support nearby for gait safety
Student Task / Procedure
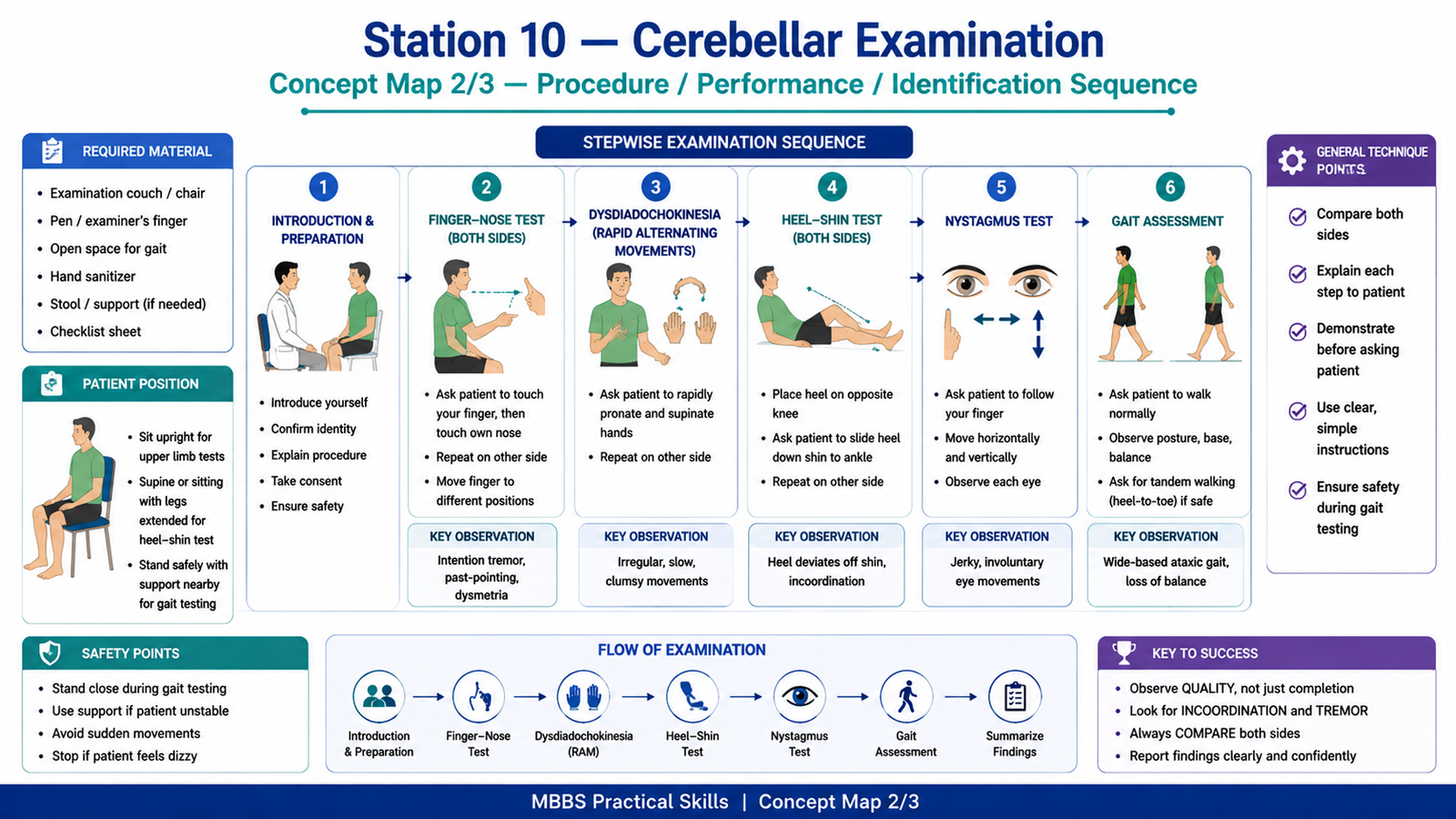
Perform the cerebellar examination in the following steps:
- Introduce yourself, confirm patient identity, explain the procedure, and take consent.
- Ensure the patient is comfortable and safe, especially before gait testing.
- Ask the patient to sit upright with upper limbs exposed.
- Perform the finger-nose test on both sides.
- Observe for intention tremor, past-pointing, and dysmetria.
- Ask the patient to perform rapid alternating movements of the hands to test dysdiadochokinesia.
- Ask the patient to lie down or sit safely and perform the heel-shin test on both sides.
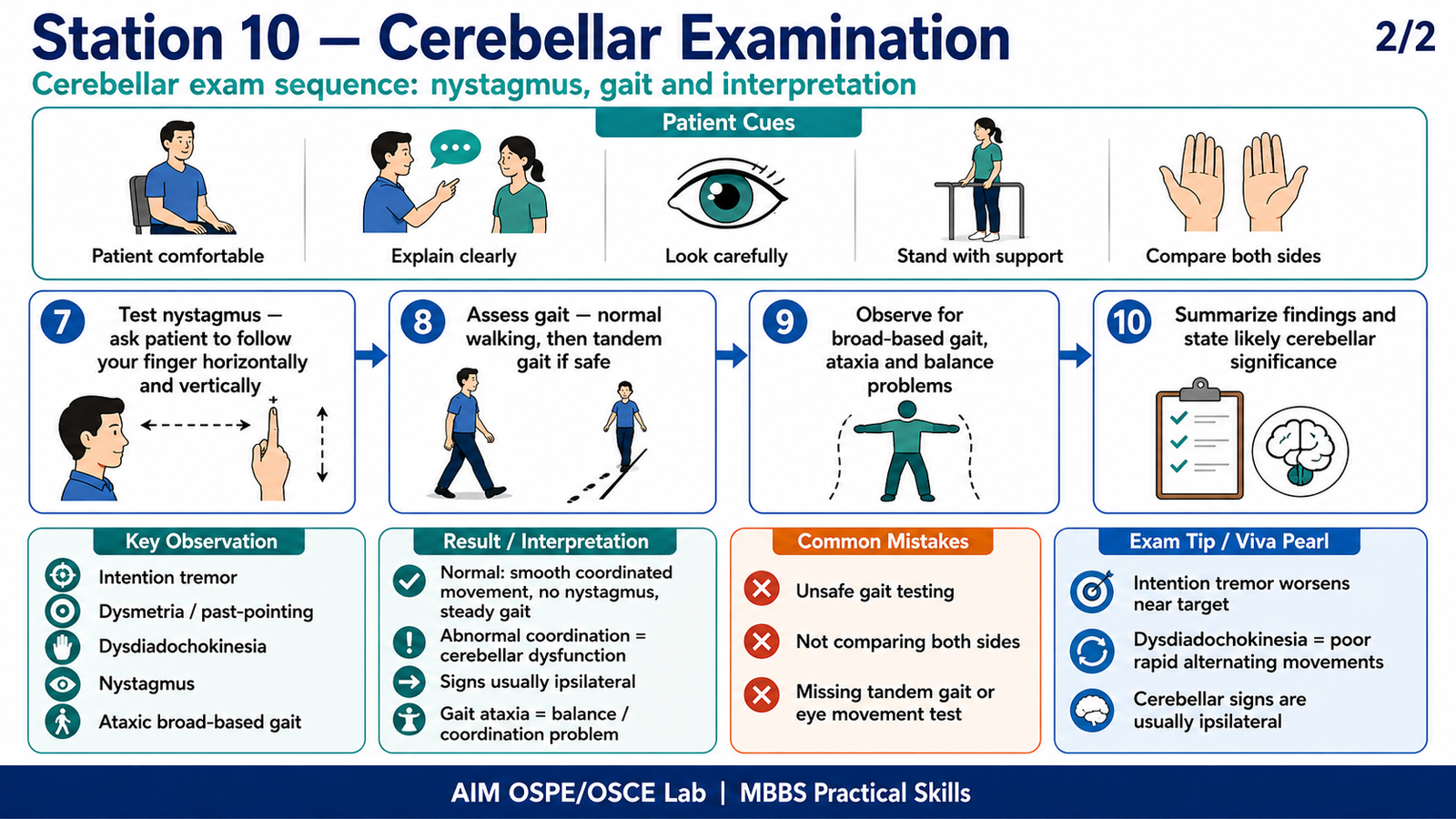
- Test for nystagmus by asking the patient to follow your finger horizontally and vertically.
- Assess gait by asking the patient to walk normally, then perform tandem walking if safe.
- Summarize the findings and mention the likely cerebellar significance.
Observation / Identification Points
The student should observe or demonstrate:
- Proper introduction, consent, and patient safety
- Correct performance of finger-nose test
- Correct performance of rapid alternating movements
- Correct performance of heel-shin test
- Correct method for checking nystagmus
- Safe gait assessment
- Important cerebellar signs:
- Intention tremor
- Dysmetria
- Past-pointing
- Dysdiadochokinesia
- Ataxic gait
- Nystagmus
- Impaired coordination
- Side-to-side comparison
- Clear summary of findings
Result / Interpretation
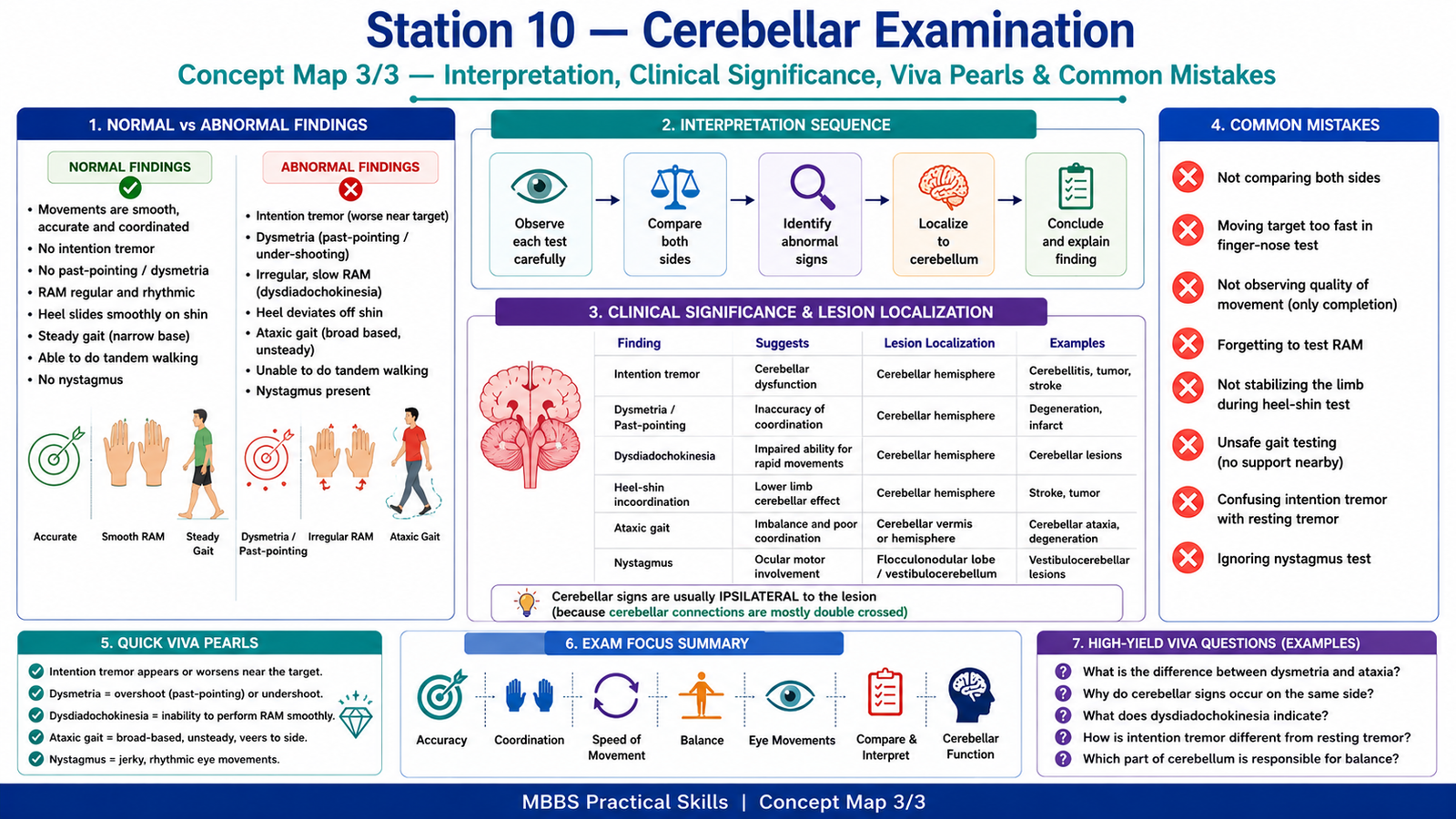
Normal cerebellar examination shows smooth, accurate, coordinated movements without tremor, past-pointing, dysdiadochokinesia, nystagmus, or ataxic gait.
Abnormal findings suggest cerebellar dysfunction. Intention tremor and dysmetria indicate impaired coordination. Dysdiadochokinesia suggests inability to perform rapid alternating movements smoothly. Heel-shin incoordination suggests lower limb cerebellar dysfunction. Nystagmus may occur due to cerebellar or vestibulocerebellar involvement. Ataxic gait suggests impaired balance and coordination.
Cerebellar lesions usually produce signs on the same side of the body as the lesion because cerebellar control is predominantly ipsilateral.
Viva Questions
1. What is dysmetria?
Dysmetria is inaccurate movement in which the patient overshoots or undershoots the target.
2. What is intention tremor?
Intention tremor is a tremor that appears or worsens as the patient approaches a target during voluntary movement.
3. What is dysdiadochokinesia?
It is the inability to perform rapid alternating movements smoothly.
4. Why is gait tested in cerebellar examination?
Gait is tested because cerebellar dysfunction commonly causes ataxic, broad-based, unsteady gait.
5. Cerebellar signs occur on which side of the lesion?
Usually on the same side as the cerebellar lesion.
Common Student Mistakes
- Performing finger-nose test too quickly without observing accuracy
- Forgetting to compare both sides
- Testing gait without ensuring patient safety
- Confusing cerebellar tremor with resting tremor
- Not asking the patient to perform rapid alternating movements properly
AIM Feedback
Cerebellar examination is mainly a test of coordination, balance, accuracy, and smoothness of movement. Always compare both sides and observe the quality of movement, not just whether the patient can complete the task. During finger-nose and heel-shin tests, look for intention tremor, dysmetria, and incoordination. During rapid alternating movements, look for irregular rhythm and poor coordination. Gait testing must always be done safely. A strong OSPE answer includes both correct performance and clear interpretation of cerebellar signs.
🖼️ Visual / Image Support
🧩 Concept Map / Interpretation Support