🩺 Station 12 — Complete Neurological Examination of Limbs
AIM OSPE/OSCE Lab — Practical Station | KMU Style | MBBS Practical + Viva
📋 Complete OSPE Station Content
OSPE Station Name
Station 12 — Complete Neurological Examination of Limbs
Learning Target
By the end of this station, the student should be able to:
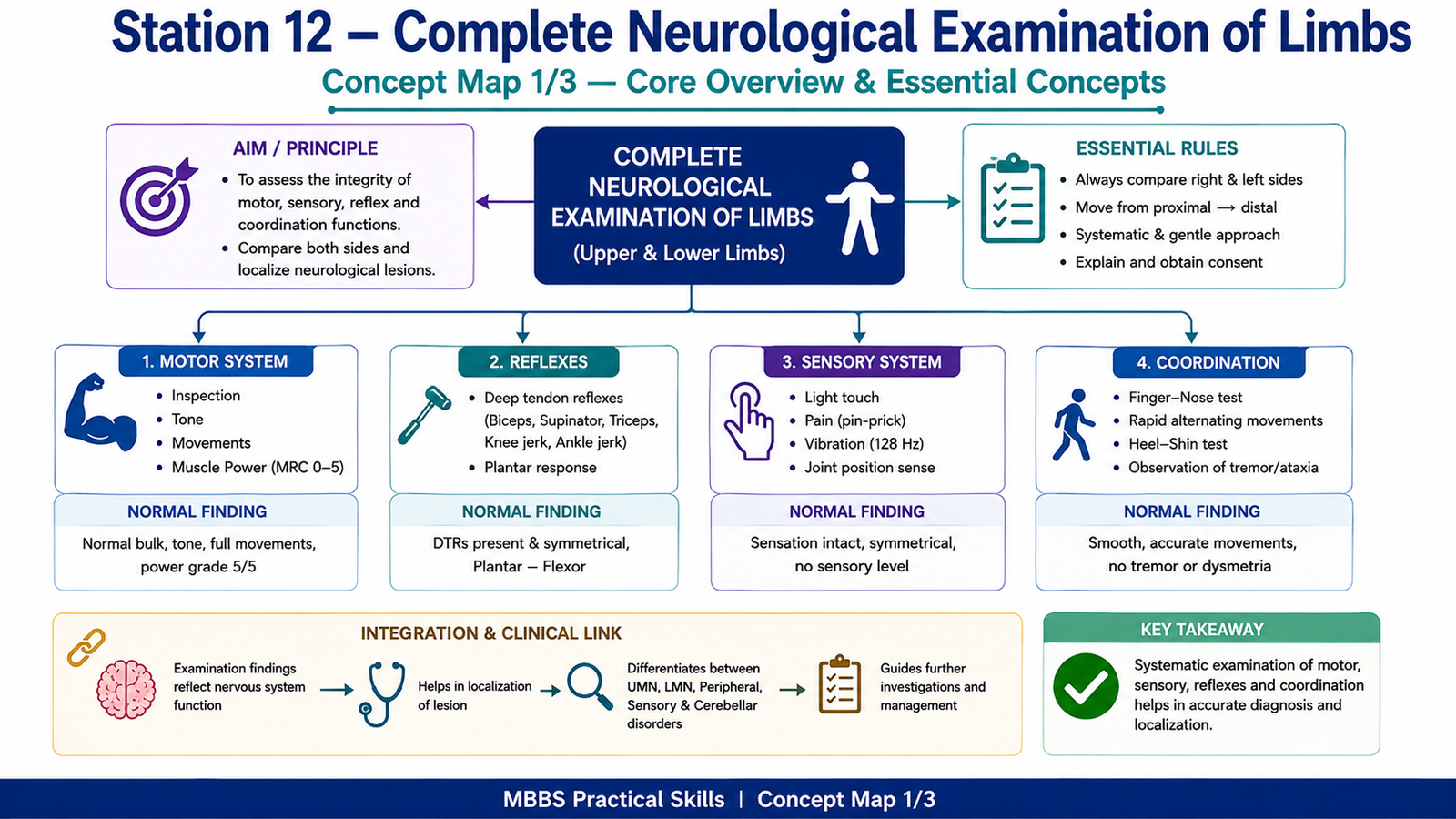
- Perform a systematic neurological examination of upper and lower limbs, including motor, sensory, reflexes, and coordination.
- Interpret common neurological findings to differentiate normal limb examination from upper motor neuron, lower motor neuron, sensory pathway, or cerebellar involvement.
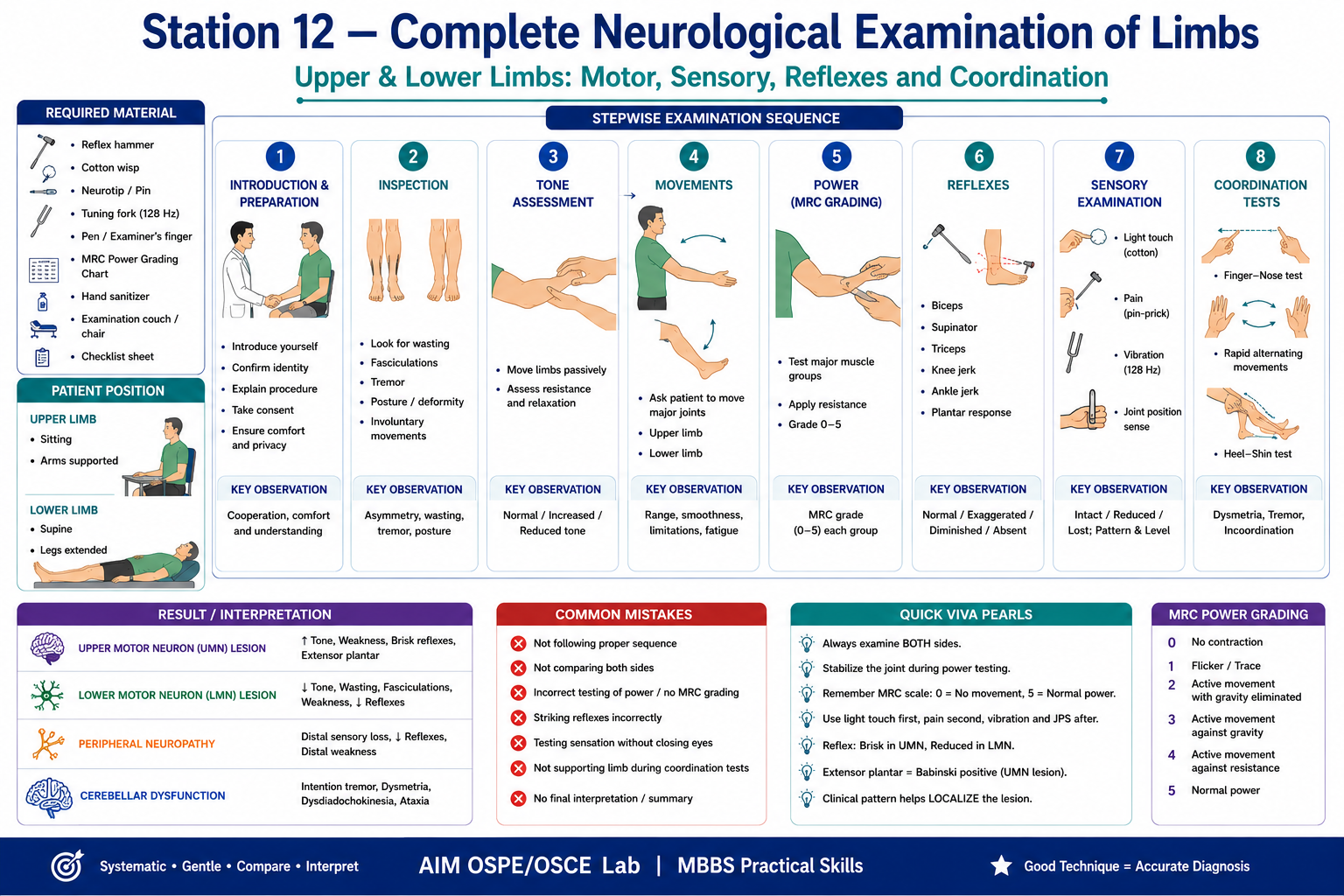
Required Material
- Examination couch or chair
- Standardized patient / volunteer
- Hand sanitizer
- Reflex hammer
- Cotton wisp
- Neurotip / disposable pin-prick stimulator
- Tuning fork, preferably 128 Hz
- Pen or examiner’s finger as target
- MRC power grading chart
- Examiner checklist
- Open space for gait/coordination if required
Student Task / Procedure
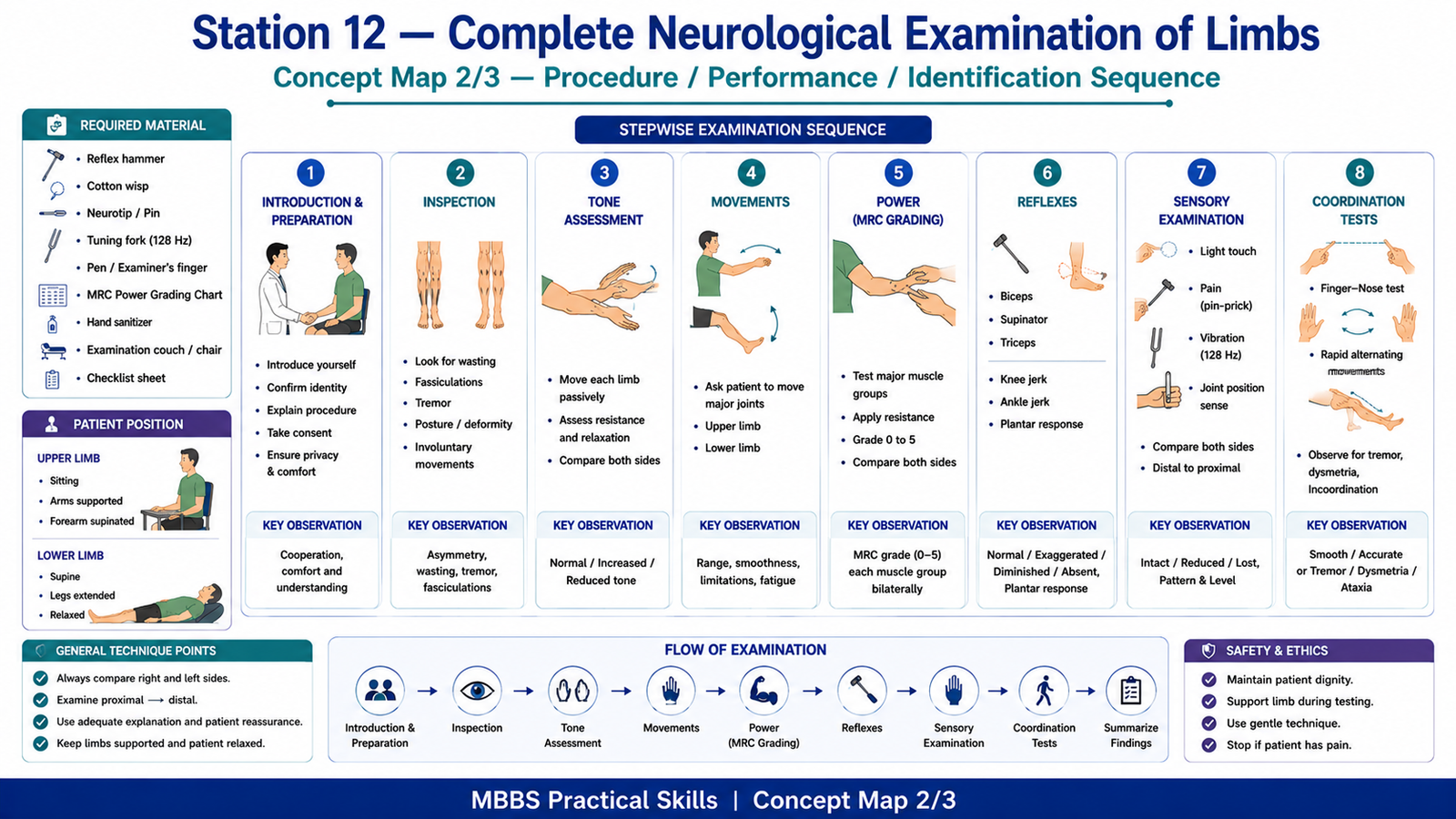
Perform the neurological examination of limbs in the following steps:
- Introduce yourself, confirm patient identity, explain the procedure, and take consent.
- Position the patient comfortably and expose upper and lower limbs appropriately.
- Inspect both upper and lower limbs for wasting, fasciculations, tremor, abnormal posture, deformity, or involuntary movements.
- Assess tone in upper and lower limbs by passive movements.
- Assess active movements of major joints of upper and lower limbs.
- Assess muscle power of major muscle groups using MRC grading from 0–5.
- Test deep tendon reflexes in upper and lower limbs.
- Test plantar response in lower limbs if required.
- Assess sensory function using light touch, pain, vibration, and joint position sense where appropriate.
- Test coordination using finger-nose test, rapid alternating movements, and heel-shin test.
- Compare right and left sides throughout the examination.
- Summarize the findings and state the likely clinical significance.
Observation / Identification Points
The student should observe, perform, or identify:
- Correct communication, consent, exposure, and patient comfort
- Inspection findings:
- Muscle wasting
- Fasciculations
- Tremor
- Abnormal posture
- Involuntary movements
- Asymmetry between limbs
- Motor assessment:
- Tone: normal, increased, reduced, spasticity, rigidity
- Active movements of shoulder, elbow, wrist, fingers, hip, knee, ankle, and toes
- Power grading using MRC scale
- Side-to-side comparison
- Reflex assessment:
- Biceps reflex
- Supinator reflex
- Triceps reflex
- Knee jerk
- Ankle jerk
- Plantar response if required
- Sensory assessment:
- Light touch
- Pain/pin-prick
- Vibration sense
- Joint position sense
- Comparison of both sides and distal-to-proximal pattern
- Coordination assessment:
- Finger-nose test
- Rapid alternating movements
- Heel-shin test
- Intention tremor
- Dysmetria
- Dysdiadochokinesia
- Clinical interpretation:
- UMN pattern
- LMN pattern
- Peripheral neuropathy pattern
- Cerebellar involvement
Result / Interpretation
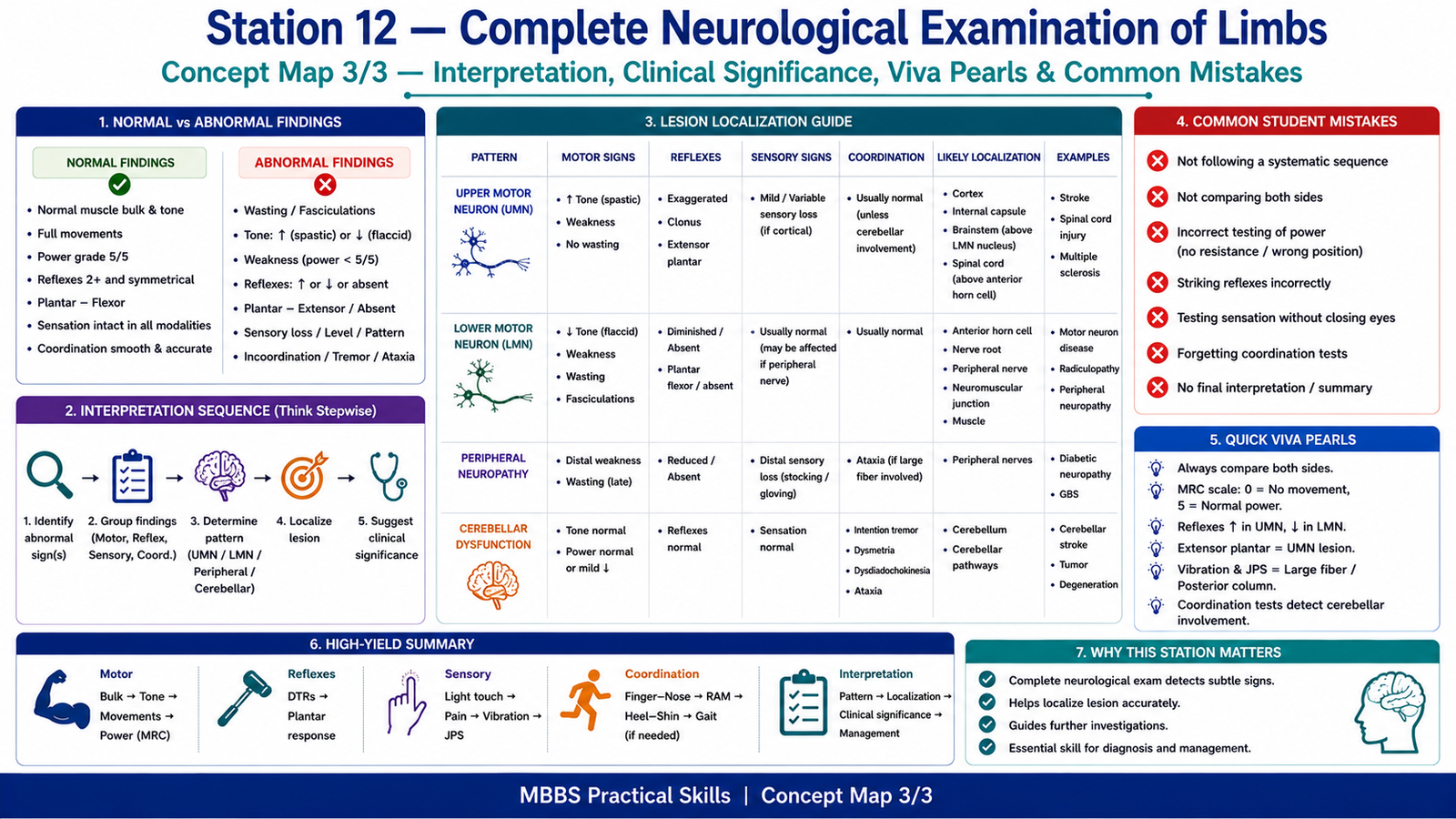
A normal neurological examination of limbs shows normal muscle bulk, no fasciculations, normal tone, full active movements, power grade 5/5 in all major muscle groups, normal reflexes, flexor plantar response, intact sensation, and normal coordination.
Abnormal findings should be interpreted according to pattern:
- Upper motor neuron lesion: increased tone, spasticity, weakness, exaggerated reflexes, and extensor plantar response
- Lower motor neuron lesion: wasting, fasciculations, reduced tone, reduced power, and diminished reflexes
- Peripheral neuropathy: distal sensory loss, reduced reflexes, and distal weakness
- Cerebellar dysfunction: intention tremor, dysmetria, dysdiadochokinesia, heel-shin incoordination, and ataxia
The aim of complete limb neurological examination is not only to detect abnormality but also to localize the lesion and identify the likely neurological system involved.
Viva Questions
1. What are the main components of limb neurological examination?
Motor examination, sensory examination, reflexes, and coordination.
2. What is the difference between an upper motor neuron and lower motor neuron lesion?
UMN lesions usually cause increased tone, exaggerated reflexes, and extensor plantar response. LMN lesions cause wasting, fasciculations, reduced tone, and reduced reflexes.
3. What is the MRC grading system used for?
It is used to grade muscle power from 0 to 5.
4. Why should both sides be compared during neurological examination?
Comparison helps detect asymmetry and localize neurological lesions.
5. What does loss of vibration sense suggest?
It may suggest posterior column involvement or peripheral neuropathy.
Common Student Mistakes
- Performing the examination in a random order
- Forgetting to compare right and left sides
- Testing power without stabilizing the joint
- Striking reflexes incorrectly or too forcefully
- Testing sensation without asking the patient to close their eyes
- Forgetting to summarize findings clinically
AIM Feedback
A complete neurological examination of limbs must be systematic. Start with inspection, then proceed to tone, movements, power, reflexes, sensation, and coordination. Always compare both sides and report findings clearly. Do not simply say “normal” or “abnormal”; explain the pattern. Increased tone with brisk reflexes suggests UMN involvement, while wasting with reduced reflexes suggests LMN involvement. Sensory loss helps identify pathway or peripheral nerve involvement, and coordination testing helps detect cerebellar dysfunction.
🖼️ Visual / Image Support
🧩 Concept Map / Interpretation Support