
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The heart is a specialized muscular organ responsible for pumping blood throughout the body. It is located in the middle mediastinum of the thoracic cavity between the lungs, slightly toward the left side. Structurally, the heart consists of four chambers, specialized cardiac muscle, valves, and conducting pathways that ensure efficient circulation. Histologically, cardiac muscle possesses unique junctional complexes and contractile properties that allow synchronized rhythmic contractions. Physiologically, the heart acts as a self-exciting muscular pump capable of automatic contraction without nervous stimulation. Understanding the gross anatomy and microscopic organization of the heart is essential for interpreting cardiovascular diseases, ECG changes, valvular disorders, heart failure, and ischemic conditions. This topic forms the foundation for future understanding of cardiac physiology and clinical cardiology.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Heart: Hollow muscular organ that pumps blood through systemic and pulmonary circulation.
- Cardiac muscle: Specialized involuntary striated muscle found only in the heart.
- Intercalated disc: Specialized junction connecting adjacent cardiac muscle cells.
- Automaticity: Ability of cardiac muscle to generate impulses spontaneously.
- Rhythmicity: Ability to contract regularly at constant intervals.
- Conductivity: Ability to transmit impulses from one cell to another.
- Myocardium: Muscular middle layer of the heart wall.
- Endocardium: Inner endothelial lining of the heart chambers.
- Epicardium: Outer visceral layer of serous pericardium.
Essential Terminology
- Apex of heart
- Base of heart
- Coronary sulcus
- Interventricular groove
- Pericardium
- Cardiac skeleton
- Sarcomere
- Gap junction
- Desmosome
- Syncytium
Basic Overview
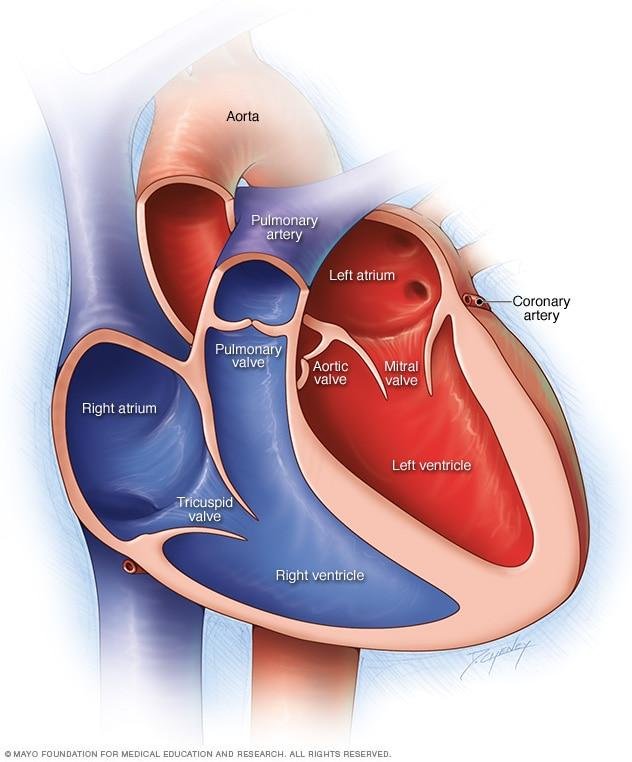
- The heart has four chambers:
- Right atrium
- Right ventricle
- Left atrium
- Left ventricle
- The heart wall has three layers:
- Endocardium
- Myocardium
- Epicardium
- Cardiac muscle is:
- Striated
- Branched
- Involuntary
- Richly vascular
- The heart functions through:
- Electrical impulse generation
- Impulse conduction
- Coordinated contraction
🔹 3️⃣ Core Learning — Curriculum Coverage
Gross Anatomy and Surface Marking of the Heart
🧠 CORE
- Heart lies in middle mediastinum.
- Approximately two-thirds lies left of midline.
- Apex formed mainly by left ventricle.
- Base formed mainly by left atrium.
- Heart has:
- Apex
- Base
- Sternocostal surface
- Diaphragmatic surface
- Right pulmonary surface
- Left pulmonary surface
- Major grooves:
- Coronary sulcus
- Anterior interventricular groove
- Posterior interventricular groove
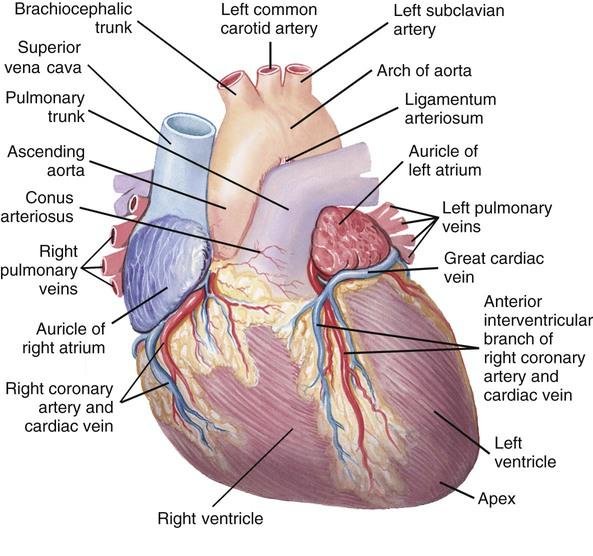
- Great vessels attached superiorly:
- Aorta
- Pulmonary trunk
- SVC
- IVC
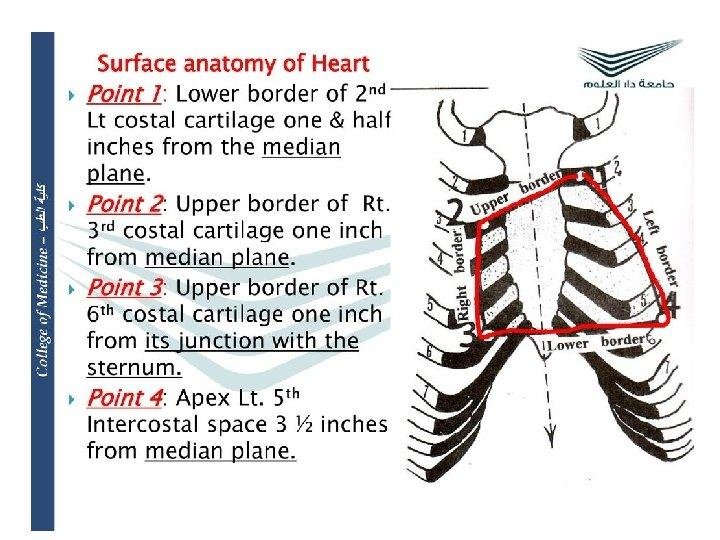
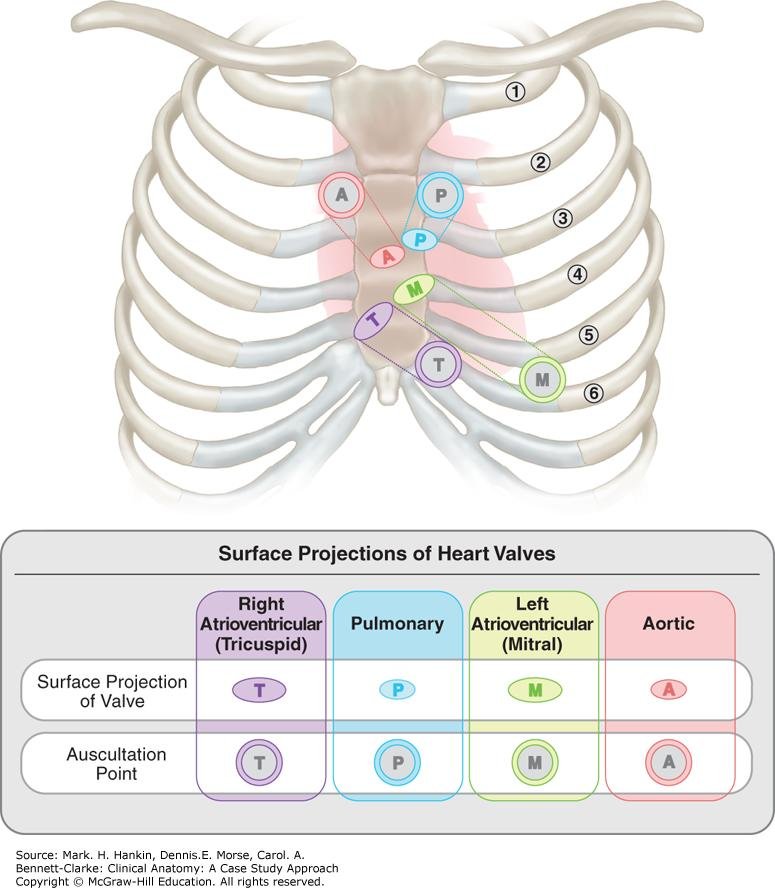
- Surface markings are clinically important for auscultation and imaging.
🔬 CONCEPT EXPLAINED
The heart is positioned obliquely in the thoracic cavity with the apex directed downward, forward, and to the left. This orientation allows efficient distribution of blood to both pulmonary and systemic circulation. The thick muscular left ventricle forms the apex because it must generate high pressure for systemic circulation.
Surface markings help clinicians identify cardiac structures on the chest wall during physical examination, imaging, and procedures. The aorta arises posterior to the sternum and ascends upward before arching backward. The superior vena cava descends vertically into the right atrium, while the inferior vena cava enters inferiorly through the diaphragm.
The coronary sulcus separates atria from ventricles externally, while interventricular grooves indicate the position of the septum internally. These grooves also contain coronary vessels supplying the myocardium.
⚠️ CLINICAL IMPORTANCE
- Cardiomegaly alters normal surface markings.
- Pericardial effusion may obscure heart borders on X-ray.
- Valve auscultation areas are based on surface anatomy.
- Incorrect interpretation of mediastinal widening may indicate aortic disease.
- Apex beat displacement suggests ventricular enlargement.
Chambers and Gross Structure of the Heart
🧠 CORE
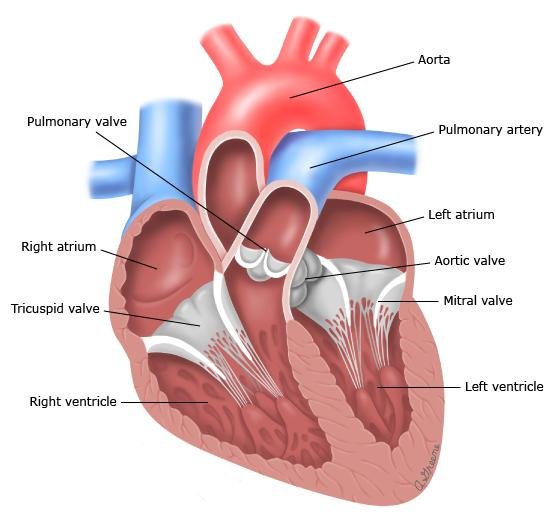
- Heart consists of four chambers.
- Right side handles deoxygenated blood.
- Left side handles oxygenated blood.
- Right ventricle pumps to lungs.
- Left ventricle pumps to systemic circulation.
- Left ventricular wall is thickest.
- Septa separate right and left sides.
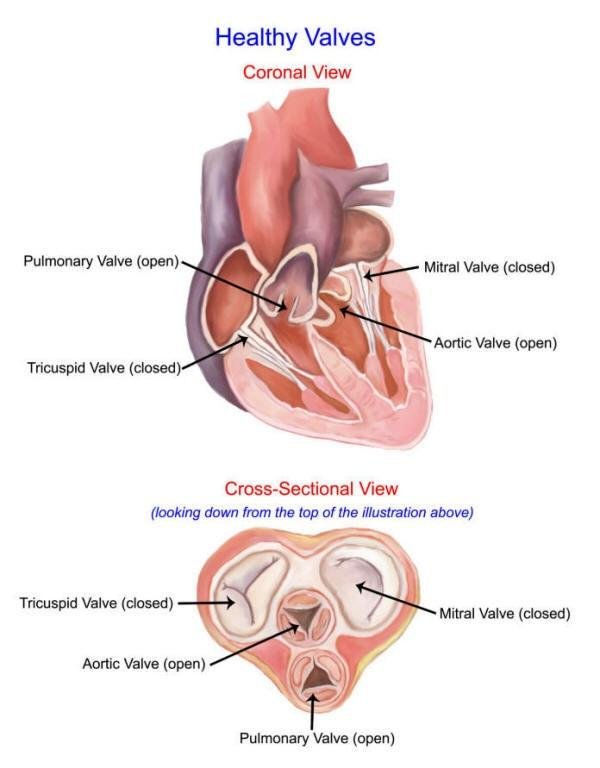
- Valves maintain unidirectional blood flow.
🔬 CONCEPT EXPLAINED
The atria act mainly as receiving chambers, while ventricles function as pumping chambers. The left ventricle has a thicker myocardium because systemic circulation requires much higher pressure than pulmonary circulation.
Valves prevent backflow of blood during contraction. The atrioventricular valves open during ventricular filling and close during ventricular contraction. Semilunar valves prevent reverse flow from arteries into ventricles.
Trabeculae carneae and papillary muscles strengthen ventricular walls and assist valve function. Chordae tendineae anchor valve cusps and prevent prolapse during systole.
The anatomical arrangement ensures efficient oxygen delivery and maintenance of blood pressure.
⚠️ CLINICAL IMPORTANCE
- Ventricular hypertrophy occurs due to pressure overload.
- Valve stenosis impairs forward blood flow.
- Valve incompetence causes regurgitation.
- Septal defects allow abnormal blood mixing.
- Myocardial infarction commonly affects ventricular walls.
Histological Organization of Cardiac Muscle
🧠 CORE
- Cardiac muscle cells are:
- Branched
- Striated
- Short cylindrical cells
- Nucleus usually central.
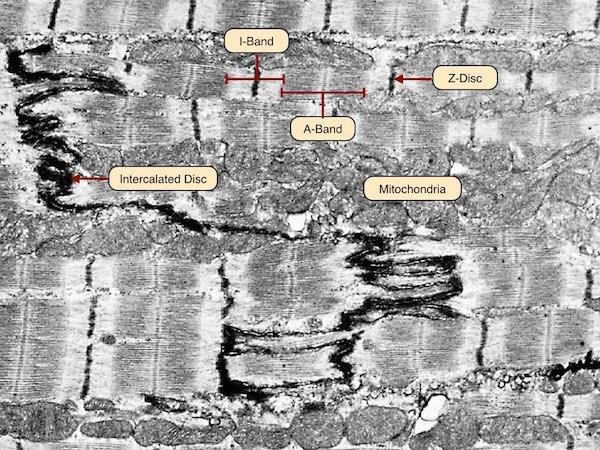
- Rich in mitochondria.
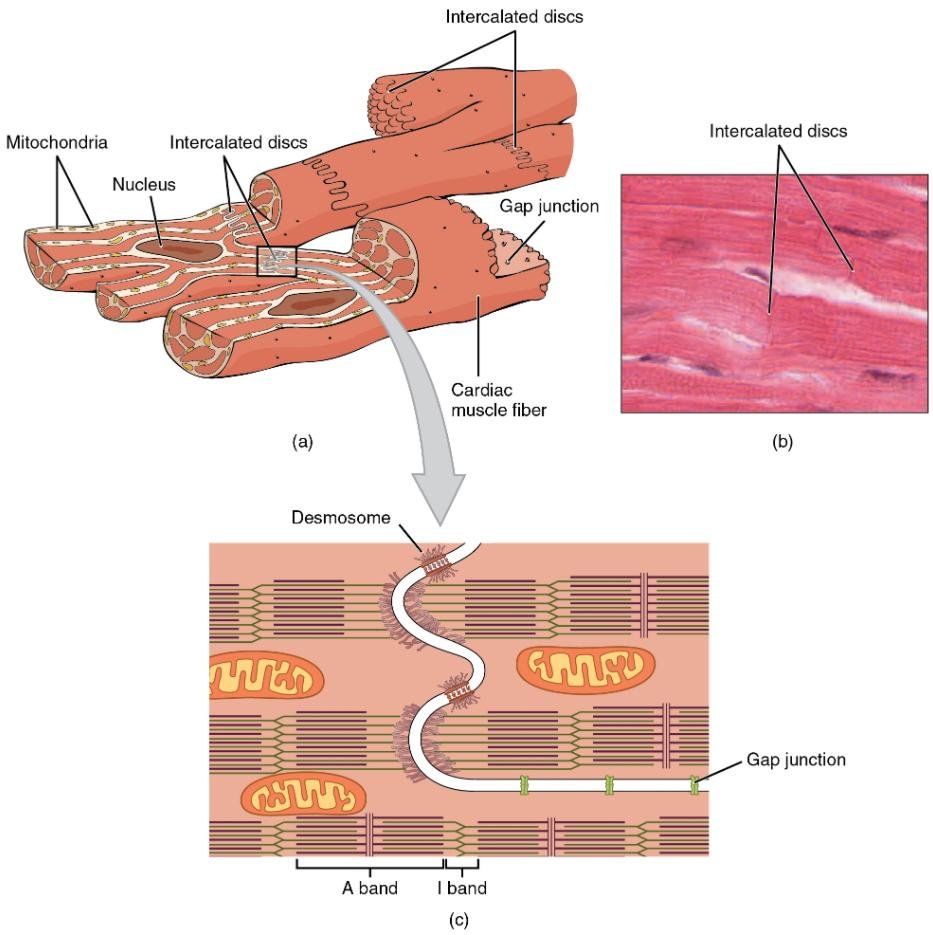
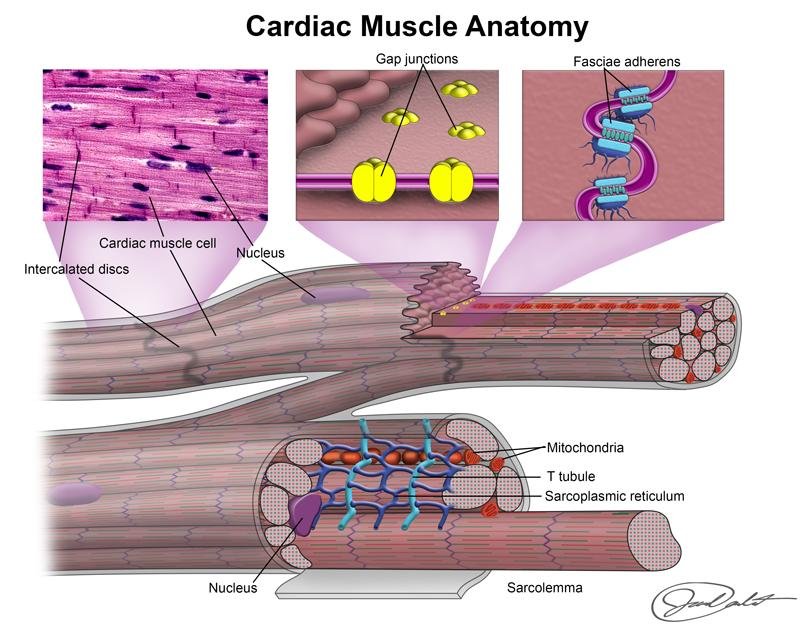
- Connected by intercalated discs.
- Myocardium highly vascular.
- Heart wall has:
- Endocardium
- Myocardium
- Epicardium
🔬 CONCEPT EXPLAINED
Cardiac muscle combines features of skeletal and smooth muscle. Striations result from organized actin and myosin filaments, while involuntary control resembles smooth muscle.
Cardiac muscle cells branch and interconnect, forming a functional syncytium. This design allows electrical impulses to spread rapidly so that the myocardium contracts as a coordinated unit.
The myocardium contains abundant mitochondria because continuous contraction requires large ATP production. Rich blood supply supports high metabolic demand.
The endocardium provides a smooth endothelial lining minimizing friction and clot formation. The epicardium contains connective tissue, fat, nerves, and coronary vessels that nourish the heart.
⚠️ CLINICAL IMPORTANCE
- Ischemia damages high-energy cardiac muscle rapidly.
- Myocarditis affects myocardial function.
- Fibrosis disrupts coordinated contraction.
- Endocardial damage predisposes to thrombus formation.
- Hypertrophy increases myocardial oxygen demand.
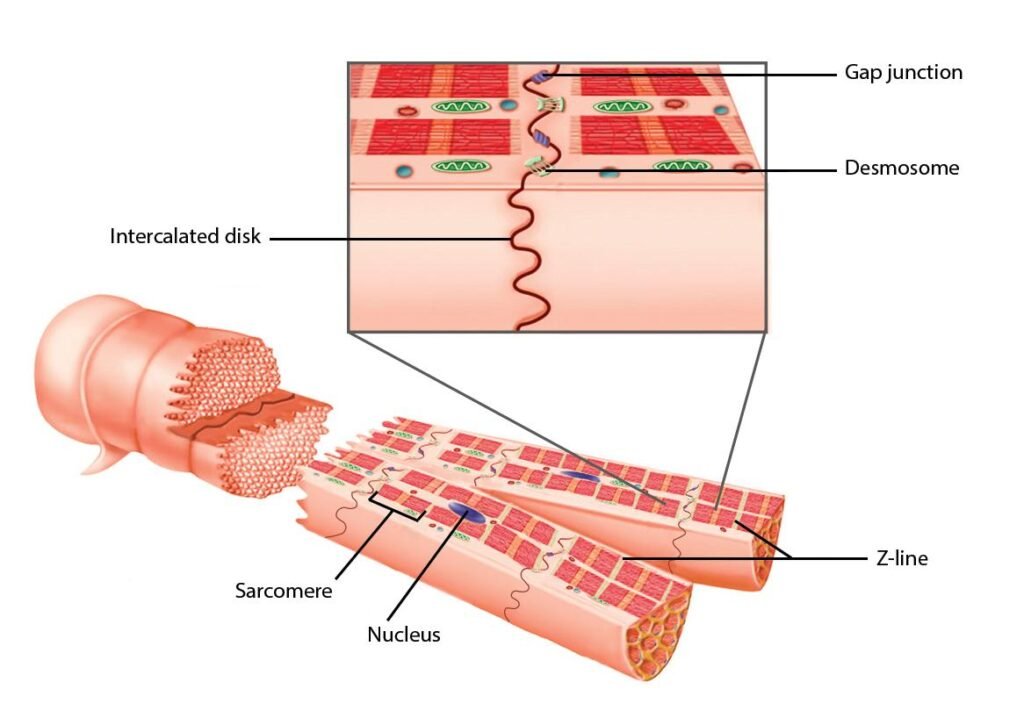
Intercalated Discs and Junctional Specializations
🧠 CORE
- Intercalated discs connect cardiac muscle cells.
- Main junctions include:
- Fascia adherens
- Desmosomes
- Gap junctions
- Gap junctions allow impulse transmission.
- Desmosomes provide mechanical strength.
- Fascia adherens anchors actin filaments.
🔬 CONCEPT EXPLAINED
Intercalated discs are specialized cell junctions essential for synchronized cardiac contraction. Gap junctions allow rapid movement of ions between cells, enabling electrical coupling. Because of this arrangement, the myocardium behaves as a functional syncytium.
Desmosomes prevent cells from separating during powerful contractions. Fascia adherens transmit contractile force from one cell to another.
This structural arrangement allows the heart to contract efficiently without tearing apart despite continuous activity throughout life.
⚠️ CLINICAL IMPORTANCE
- Defective gap junctions may cause arrhythmias.
- Damage to intercalated discs impairs impulse conduction.
- Cardiomyopathies may involve junctional protein abnormalities.
- Conduction abnormalities disturb coordinated pumping.
Microscopic Identification of Cardiac Muscle
🧠 CORE
Cardiac Muscle Features
- Branched fibers
- Central nucleus
- Striations present
- Intercalated discs visible
Skeletal Muscle Features
- Long cylindrical fibers
- Peripheral nuclei
- No branching
- Voluntary
Smooth Muscle Features
- Spindle-shaped cells
- No striations
- Single central nucleus
- Involuntary
🔬 CONCEPT EXPLAINED
Histological differentiation depends on cellular organization and contractile specialization. Cardiac muscle resembles skeletal muscle due to striations but differs because of branching fibers and intercalated discs.
Smooth muscle lacks organized sarcomeres, so striations are absent. Its spindle-shaped appearance reflects adaptation for slow sustained contraction.
Recognition of these features is essential during microscopic examination and pathology interpretation.
⚠️ CLINICAL IMPORTANCE
- Histological changes help diagnose myocarditis and cardiomyopathy.
- Degeneration patterns differ among muscle types.
- Myocardial necrosis is identified microscopically after infarction.
Physiologic Anatomy and Functional Properties of Cardiac Muscle
🧠 CORE
Properties of Cardiac Muscle
- Automaticity
- Rhythmicity
- Conductivity
- Excitability
- Contractility
Functional Features
- Acts as syncytium
- Long refractory period
- Self-excitable tissue
- Continuous rhythmic contraction
🔬 CONCEPT EXPLAINED
Cardiac muscle is designed for lifelong rhythmic contraction. Specialized pacemaker cells generate spontaneous impulses without external stimulation. These impulses spread through conducting pathways and gap junctions.
The myocardium behaves as two syncytia:
- Atrial syncytium
- Ventricular syncytium
Fibrous cardiac skeleton electrically separates atria from ventricles except through the AV bundle. This ensures coordinated sequential contraction.
The long refractory period prevents tetanic contraction. Unlike skeletal muscle, the heart must relax between contractions to allow ventricular filling.
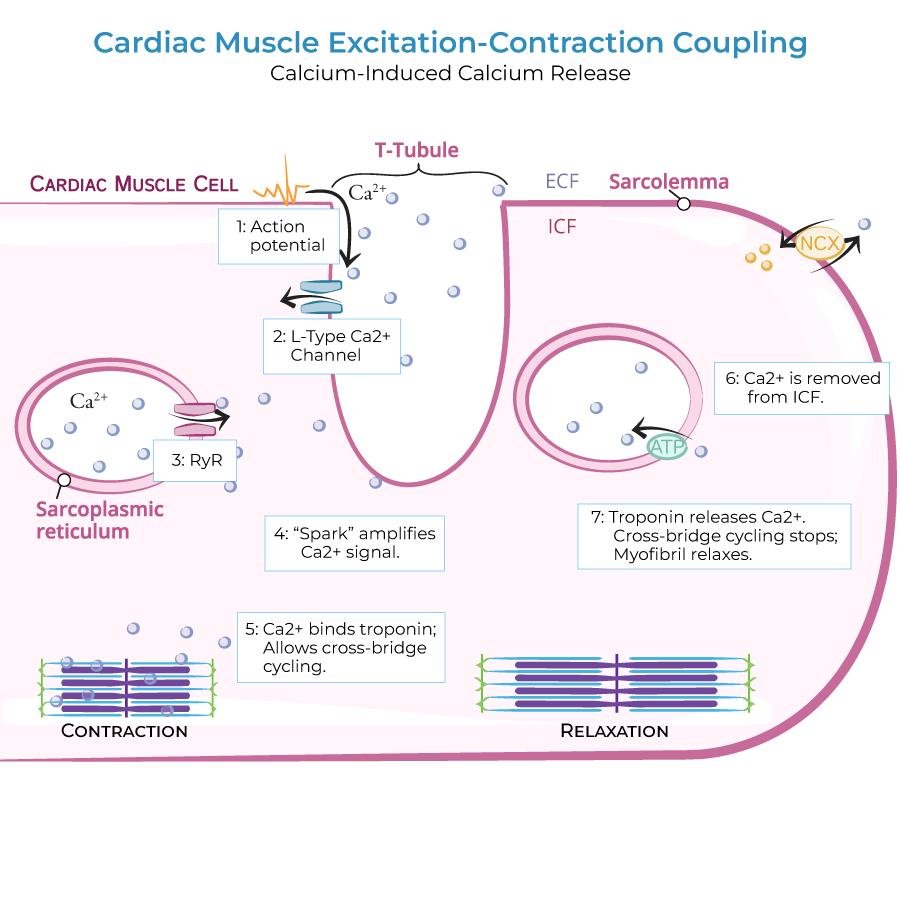
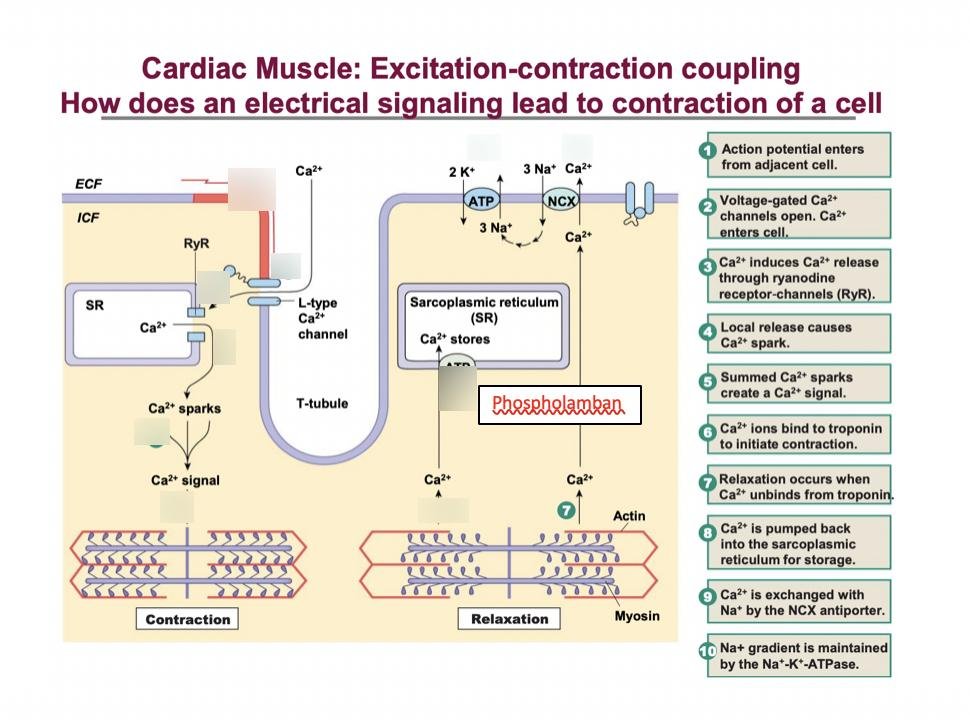
Cardiac muscle contraction depends heavily on calcium influx. Electrical excitation triggers calcium release, resulting in actin-myosin interaction and contraction.
⚠️ CLINICAL IMPORTANCE
- Loss of automaticity causes arrhythmias.
- Impaired conductivity produces heart block.
- Reduced contractility causes heart failure.
- Abnormal excitability predisposes to ectopic beats.
- Calcium channel abnormalities alter cardiac function.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Function | Functional Outcome |
|---|---|---|
| Thick left ventricular wall | Generates high pressure | Systemic circulation maintained |
| Intercalated discs | Electrical and mechanical coupling | Synchronized contraction |
| Gap junctions | Rapid impulse transmission | Efficient pumping |
| Valves | Prevent backflow | Unidirectional blood flow |
| Branched cardiac fibers | Coordinated contraction | Functional syncytium |
| Rich mitochondria | ATP production | Continuous contraction |
| Coronary circulation | Oxygen delivery | Myocardial survival |
🩺 5️⃣ Clinical Correlation
Common Clinical Conditions
Valvular Heart Disease
- Stenosis narrows valve opening.
- Regurgitation causes backflow.
- Leads to chamber hypertrophy and heart failure.
Myocardial Infarction
- Coronary artery obstruction causes ischemia.
- Cardiac muscle undergoes necrosis.
- Pumping ability decreases.
Arrhythmias
- Result from abnormal impulse generation or conduction.
- May cause palpitations or sudden death.
Cardiomyopathy
- Structural myocardial disease.
- Causes impaired contraction and heart failure.
Heart Failure
- Inadequate cardiac pumping.
- Results in tissue hypoperfusion and edema.
📌 6️⃣ Summary Points
- Left ventricle forms apex of heart.
- Left ventricular wall is thickest due to systemic pressure.
- Cardiac muscle is branched and involuntary.
- Intercalated discs connect adjacent cardiac cells.
- Gap junctions allow rapid impulse spread.
- Desmosomes provide mechanical attachment.
- Heart wall consists of endocardium, myocardium, and epicardium.
- Cardiac muscle has abundant mitochondria for continuous activity.
- Long refractory period prevents tetany.
- Cardiac muscle functions as a syncytium.
- Valves ensure one-way blood flow.
- Automaticity allows spontaneous contraction.