
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
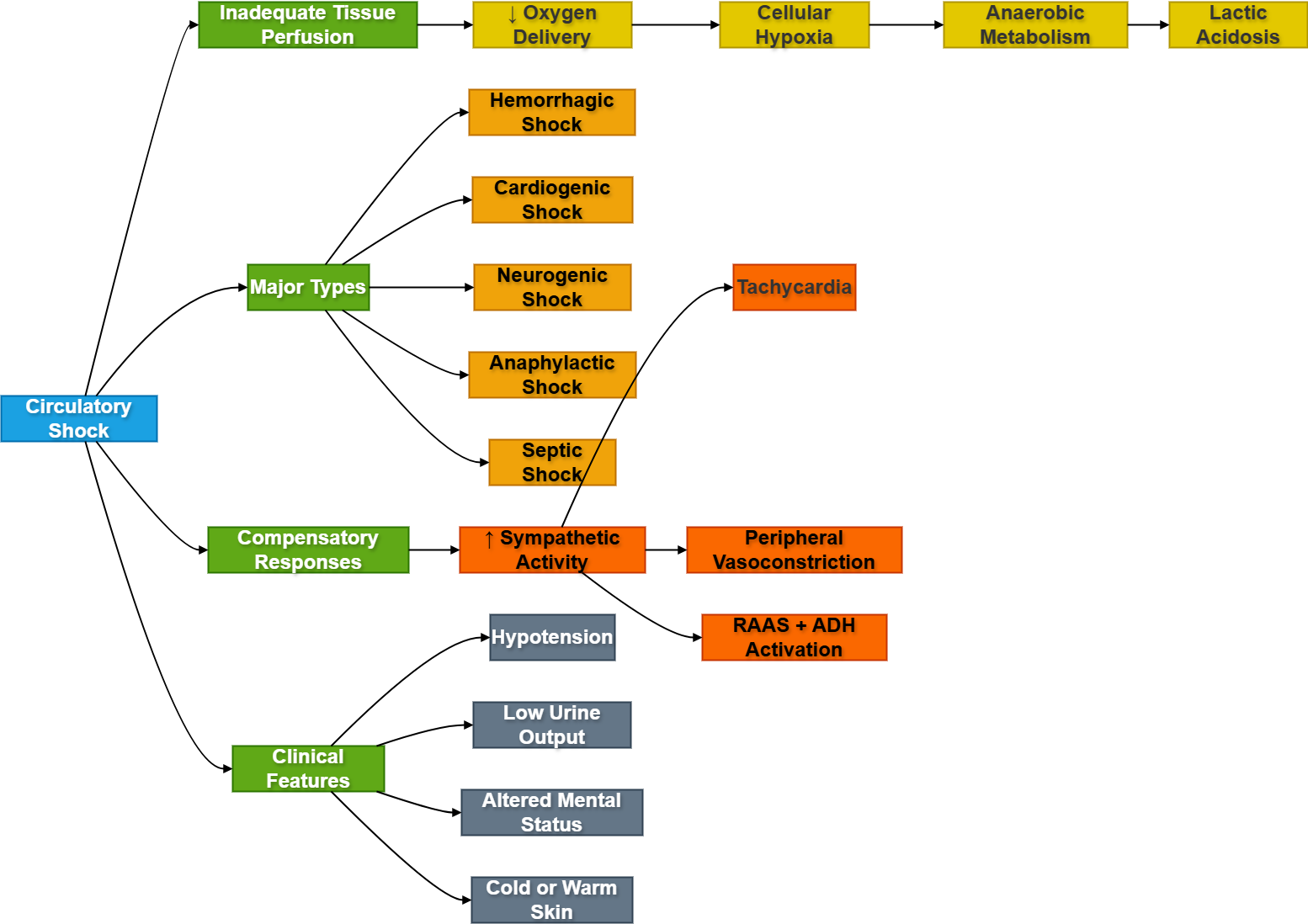
Circulatory shock is a life-threatening condition in which the circulatory system fails to provide adequate blood flow and oxygen delivery to tissues. It represents a state of severe tissue hypoperfusion leading to cellular dysfunction and organ failure. Shock primarily affects the cardiovascular system, but prolonged shock ultimately damages all organs including the brain, kidneys, lungs, and heart.
The body normally maintains tissue perfusion through cardiac output and vascular resistance. In shock, this balance is disturbed due to loss of blood volume, pump failure, vasodilation, or impaired vascular tone. Early recognition of shock is clinically critical because delayed treatment can progress to irreversible organ damage and death.
Understanding the physiological basis of shock helps explain hypotension, tachycardia, cold extremities, metabolic acidosis, and compensatory cardiovascular responses commonly seen in emergency medicine and intensive care settings.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Circulatory Shock: A state of inadequate tissue perfusion resulting in insufficient oxygen and nutrient delivery to cells.
- Hypoperfusion: Reduced blood flow to tissues.
- Hypotension: Abnormally low arterial blood pressure.
- Cardiac Output (CO): Amount of blood pumped by the heart per minute.
- Mean Arterial Pressure (MAP): Average arterial pressure driving tissue perfusion.
- Compensatory Mechanisms: Physiological responses activated to maintain blood pressure and organ perfusion.
- Multiple Organ Dysfunction Syndrome (MODS): Failure of multiple organs due to prolonged shock.
Essential Terminology
- Preload: Ventricular filling before contraction.
- Afterload: Resistance against ventricular ejection.
- Peripheral Resistance: Resistance offered by blood vessels to blood flow.
- Vasoconstriction: Narrowing of blood vessels.
- Vasodilation: Widening of blood vessels.
- Tissue Hypoxia: Inadequate oxygen supply to tissues.
Basic Overview
- Shock causes inadequate oxygen delivery to tissues.
- Major causes include:
- Loss of blood volume
- Cardiac pump failure
- Severe vasodilation
- Allergic reactions
- Infection
- Shock progresses through:
- Non-progressive stage
- Progressive stage
- Irreversible stage
- Early treatment aims to restore circulation and oxygen delivery.
https://ailearningcycle.com/wp-content/uploads/2026/05/ghg.drawio.png
🔹 3️⃣ Core Learning — Curriculum Coverage
Circulatory Shock: General Concepts and Pathophysiology
🧠 CORE
- Shock results from failure of adequate tissue perfusion.
- Oxygen delivery becomes lower than tissue demand.
- Reduced perfusion causes cellular hypoxia.
- ATP production decreases due to impaired oxidative metabolism.
- Anaerobic glycolysis increases lactic acid production.
- Blood pressure may initially be maintained by compensatory mechanisms.
- Vital organs affected:
- Brain
- Heart
- Kidneys
- Lungs
- Persistent shock causes organ failure and death.
🔬 CONCEPT EXPLAINED
Normal tissue perfusion depends upon adequate cardiac output and vascular resistance. When blood flow becomes insufficient, tissues fail to receive enough oxygen and nutrients. Cells shift from aerobic metabolism to anaerobic glycolysis, producing less ATP and generating lactic acid.
The body initially attempts compensation through sympathetic activation. Heart rate increases, arterioles constrict, and venous return improves to maintain blood pressure and blood flow to essential organs such as the brain and heart.
If the underlying cause persists, cellular injury worsens. Capillary permeability increases, inflammatory mediators are released, and microcirculatory failure develops. Eventually organ dysfunction becomes irreversible.
⚠️ CLINICAL IMPORTANCE
- Common manifestations:
- Hypotension
- Tachycardia
- Cold clammy skin
- Reduced urine output
- Altered mental status
- Lactic acidosis is an important indicator of tissue hypoxia.
- Untreated shock can rapidly progress to multiorgan failure.
Classification of Shock
🧠 CORE
Major types of circulatory shock:
- Hypovolemic shock
- Cardiogenic shock
- Neurogenic shock
- Anaphylactic shock
- Septic shock
Primary physiological disturbances include:
- Reduced blood volume
- Impaired cardiac pumping
- Loss of vascular tone
- Excessive vasodilation
- Abnormal capillary permeability
🔬 CONCEPT EXPLAINED
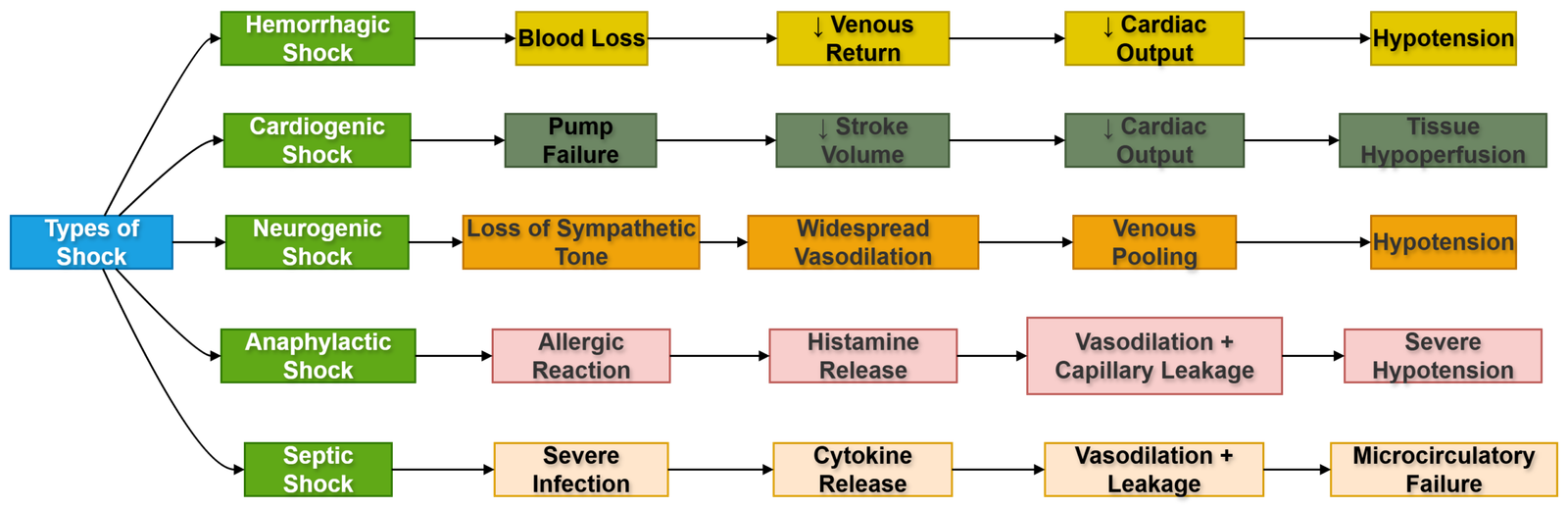
Different types of shock share the common endpoint of tissue hypoperfusion, but mechanisms differ.
Hypovolemic Shock
Occurs due to reduced circulating blood volume from hemorrhage, dehydration, burns, or plasma loss.
Cardiogenic Shock
Results from failure of the heart to pump effectively, commonly after myocardial infarction.
Neurogenic Shock
Caused by loss of sympathetic vascular tone due to spinal cord injury or anesthesia.
Anaphylactic Shock
Results from severe allergic reactions causing histamine-mediated vasodilation and increased capillary permeability.
Septic Shock
Develops due to severe infection causing inflammatory mediator release, vasodilation, and circulatory collapse.
⚠️ CLINICAL IMPORTANCE
- Different types of shock require different treatments.
- Rapid identification of the underlying cause is essential.
- Shock type influences:
- Skin temperature
- Pulse pressure
- Venous pressure
- Cardiac output
Stages of Shock
🧠 CORE
Three major stages:
- Non-progressive (Compensated) stage
- Progressive (Decompensated) stage
- Irreversible stage
Major compensatory mechanisms:
- Sympathetic activation
- RAAS activation
- ADH secretion
- Fluid shift from interstitium to plasma
🔬 CONCEPT EXPLAINED
1. Non-Progressive (Compensated) Stage
The body activates reflex compensatory mechanisms to maintain circulation.
Key responses include:
- Tachycardia
- Vasoconstriction
- Increased cardiac contractility
- Fluid conservation by kidneys
Blood flow to vital organs is preserved despite reduced perfusion elsewhere.
2. Progressive Stage
Compensation becomes inadequate.
- Tissue hypoxia worsens
- Lactic acidosis develops
- Vasomotor center depression occurs
- Capillary permeability increases
- Cardiac output further declines
Positive feedback cycles worsen circulatory failure.
3. Irreversible Stage
Severe cellular injury and organ damage occur.
- Myocardial depression develops
- Lysosomal enzymes leak
- Extensive tissue necrosis occurs
- Renal failure develops
- Brain damage becomes permanent
Even correction of blood pressure may not reverse damage at this stage.
⚠️ CLINICAL IMPORTANCE
- Early shock is reversible with prompt treatment.
- Progressive shock requires aggressive resuscitation.
- Irreversible shock has very high mortality.
Hemorrhagic Shock
🧠 CORE
- Most common form of hypovolemic shock.
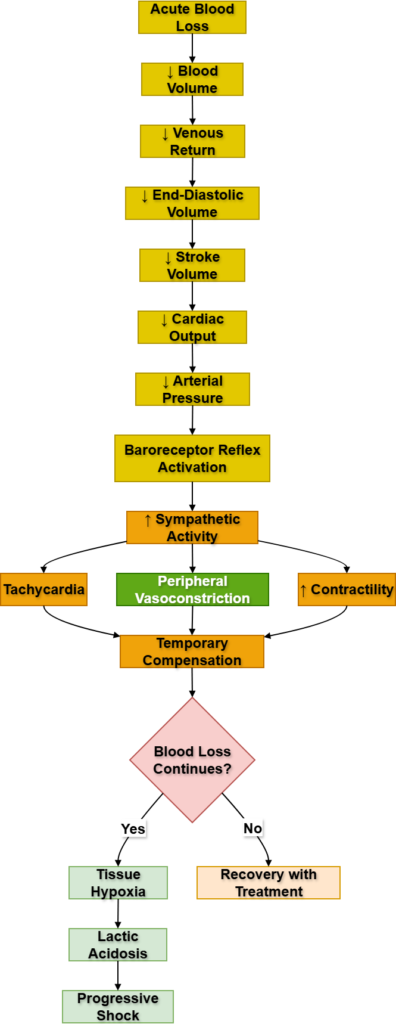
- Caused by acute blood loss.
- Reduced venous return lowers cardiac output.
- Arterial pressure falls.
- Sympathetic reflexes activate compensation.
- Severe blood loss causes circulatory collapse.
🔬 CONCEPT EXPLAINED
Loss of blood volume decreases venous return to the heart. Reduced ventricular filling lowers stroke volume and cardiac output.
Baroreceptors detect falling arterial pressure and stimulate sympathetic activation:
- Heart rate increases
- Peripheral vasoconstriction occurs
- Blood flow shifts toward vital organs
If blood loss exceeds compensatory capacity, tissue hypoxia worsens and shock progresses rapidly.
The kidneys conserve sodium and water through RAAS and ADH activation to restore plasma volume.
⚠️ CLINICAL IMPORTANCE
- Common causes:
- Trauma
- Gastrointestinal bleeding
- Obstetric hemorrhage
- Clinical signs:
- Cold pale skin
- Weak pulse
- Tachycardia
- Hypotension
- Severe hemorrhage can rapidly become fatal.
Cardiogenic Shock
🧠 CORE
- Caused by severe cardiac pump failure.
- Cardiac output becomes critically low.
- Commonly follows myocardial infarction.
- Pulmonary congestion often develops.
- Tissue perfusion decreases despite adequate blood volume.
🔬 CONCEPT EXPLAINED
In cardiogenic shock, the heart cannot generate sufficient force to maintain circulation. Reduced stroke volume lowers arterial pressure and organ perfusion.
The sympathetic nervous system increases heart rate and vasoconstriction, but excessive afterload may further burden the failing heart.
Blood backs up into pulmonary circulation causing pulmonary edema and impaired oxygenation.
Because cardiac pumping ability is impaired, simple fluid replacement alone cannot correct the problem.
⚠️ CLINICAL IMPORTANCE
- Major cause:
- Acute myocardial infarction
- Findings:
- Severe hypotension
- Pulmonary edema
- Cyanosis
- Cold extremities
- High mortality if untreated.
Neurogenic Shock
🧠 CORE
- Caused by loss of sympathetic vascular tone.
- Leads to widespread vasodilation.
- Venous pooling decreases venous return.
- Cardiac output falls.
- Often associated with spinal cord injury.
🔬 CONCEPT EXPLAINED
Sympathetic nerves normally maintain vascular tone. In spinal cord injury or severe anesthesia, sympathetic outflow is interrupted.
Arterioles dilate and veins become highly compliant. Blood pools in peripheral vessels, reducing venous return and cardiac output.
Unlike other forms of shock, tachycardia may be absent because sympathetic cardiac stimulation is impaired.
⚠️ CLINICAL IMPORTANCE
- Seen in:
- Cervical spinal trauma
- Deep spinal anesthesia
- Patients may have:
- Warm skin
- Hypotension
- Bradycardia
- Vasopressors are often required.
Anaphylactic Shock
🧠 CORE
- Severe allergic hypersensitivity reaction.
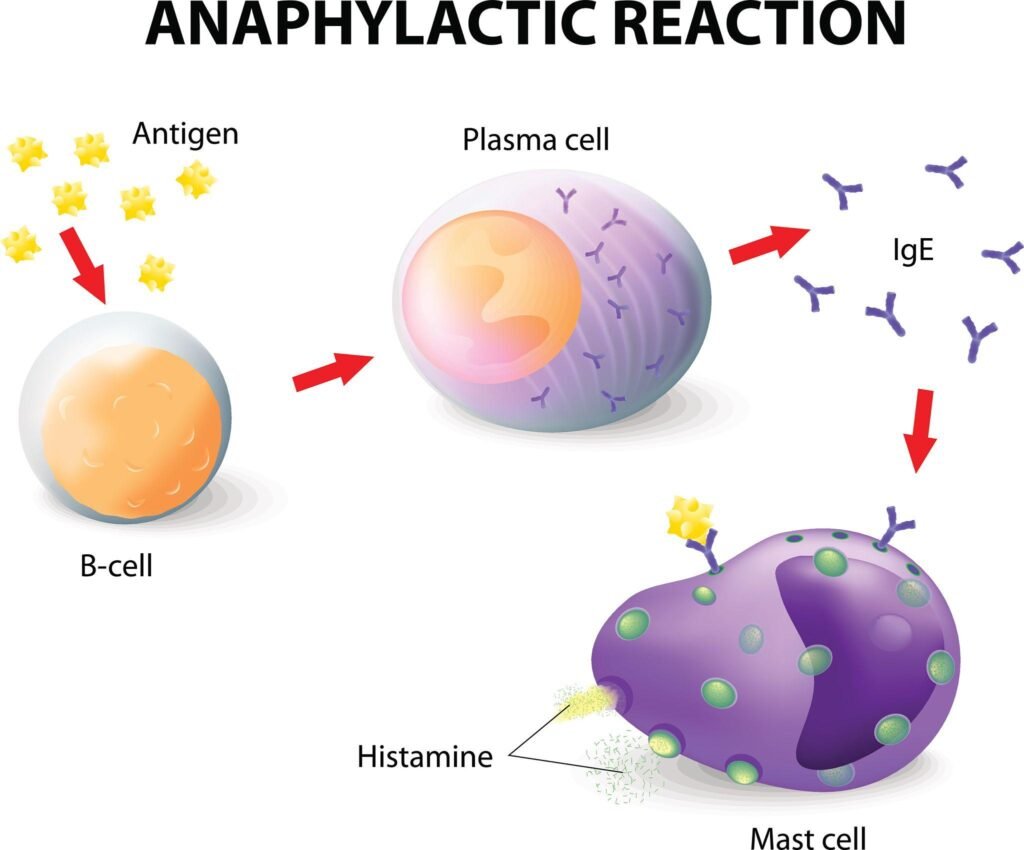
- Mediated by IgE and mast cell activation.
- Histamine release causes vasodilation.
- Capillary permeability increases markedly.
- Bronchoconstriction may occur.
🔬 CONCEPT EXPLAINED
Exposure to allergens triggers IgE-mediated mast cell degranulation. Histamine and inflammatory mediators produce:
- Widespread vasodilation
- Plasma leakage
- Reduced venous return
- Airway narrowing
Rapid reduction in arterial pressure and impaired oxygenation can become life-threatening within minutes.
⚠️ CLINICAL IMPORTANCE
- Common triggers:
- Drugs
- Insect stings
- Foods
- Clinical findings:
- Hypotension
- Wheezing
- Facial swelling
- Urticaria
- Epinephrine is life-saving.
Septic Shock
🧠 CORE
- Caused by severe systemic infection.
- Bacterial endotoxins activate inflammatory pathways.
- Massive vasodilation occurs.
- Capillary leakage develops.
- Microcirculatory dysfunction impairs oxygen delivery.
🔬 CONCEPT EXPLAINED
Bacterial toxins stimulate cytokine release including TNF-α and interleukins. These mediators produce systemic vasodilation and increased capillary permeability.
Initially cardiac output may rise due to vasodilation (“warm shock”), but later myocardial depression and severe hypotension develop.
Disseminated intravascular coagulation (DIC) and multiple organ dysfunction may occur due to inflammatory injury.
⚠️ CLINICAL IMPORTANCE
- Common in severe bacterial infections.
- Features:
- Fever
- Hypotension
- Warm flushed skin initially
- Altered mental status
- Major cause of ICU mortality.
Physiology of Treatment in Shock
🧠 CORE
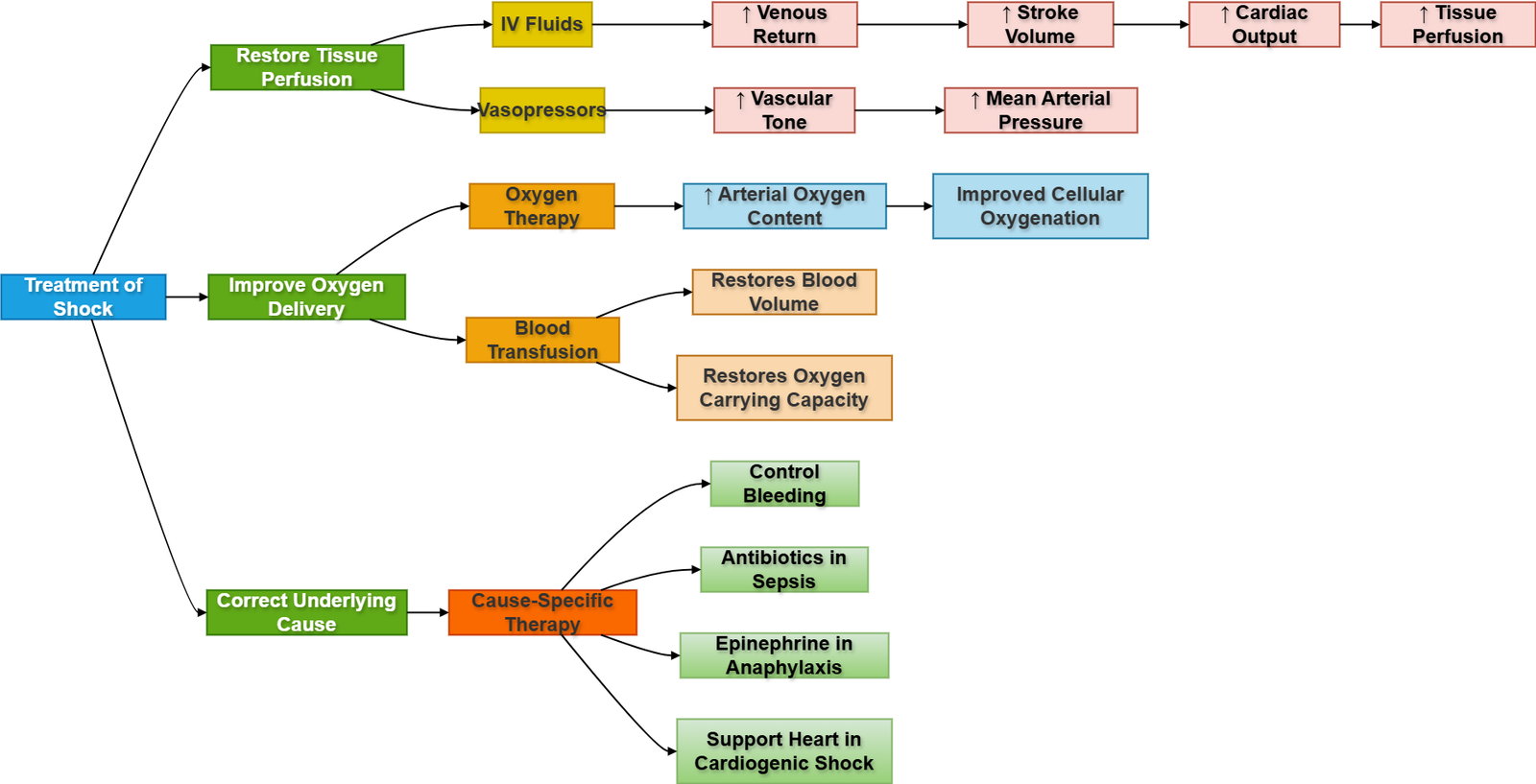
Treatment aims to:
- Restore tissue perfusion
- Improve oxygen delivery
- Correct underlying cause
- Maintain blood pressure
- Prevent organ damage
Major treatment approaches:
- Fluid replacement
- Blood transfusion
- Vasopressors
- Oxygen therapy
- Treatment of underlying cause
🔬 CONCEPT EXPLAINED
Fluid Resuscitation
In hypovolemic states, intravenous fluids restore venous return and cardiac output.
Blood Transfusion
Needed in hemorrhagic shock to restore oxygen-carrying capacity.
Vasopressors
Drugs like norepinephrine increase vascular tone and arterial pressure.
Oxygen Therapy
Improves tissue oxygen delivery during hypoperfusion.
Treatment of Underlying Cause
- Antibiotics for septic shock
- Epinephrine for anaphylaxis
- Revascularization in cardiogenic shock
Early restoration of microcirculation prevents irreversible organ damage.
⚠️ CLINICAL IMPORTANCE
- Delayed treatment worsens mortality.
- Monitoring urine output is important for renal perfusion assessment.
- Excessive fluid administration in cardiogenic shock may worsen pulmonary edema.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure/Component | Function | Outcome in Shock |
|---|---|---|
| Heart | Maintains cardiac output | Failure causes cardiogenic shock |
| Blood vessels | Maintain vascular tone | Vasodilation causes hypotension |
| Blood volume | Maintains venous return | Loss causes hypovolemic shock |
| Sympathetic nervous system | Compensatory vasoconstriction | Maintains BP initially |
| Kidneys | Fluid conservation | Maintains circulating volume |
| Capillaries | Exchange of oxygen/nutrients | Leakage worsens hypoperfusion |
| Cellular mitochondria | ATP production | Failure causes cellular injury |
🩺 5️⃣ Clinical Correlation
Hemorrhagic Shock
- Seen after trauma or severe bleeding.
- Causes cold clammy skin and weak pulse.
Cardiogenic Shock
- Common after myocardial infarction.
- Pulmonary edema is a major complication.
Septic Shock
- Common in ICU patients with severe infection.
- Warm flushed skin may occur initially.
Anaphylactic Shock
- Rapid onset after allergen exposure.
- Airway obstruction may become fatal.
Neurogenic Shock
- Associated with spinal cord injury.
- Bradycardia differentiates it from other forms of shock.
📌 6️⃣ Summary Points
- Shock is failure of adequate tissue perfusion.
- Tissue hypoxia leads to anaerobic metabolism and lactic acidosis.
- Major types:
- Hypovolemic
- Cardiogenic
- Neurogenic
- Septic
- Anaphylactic
- Sympathetic activation is the major early compensatory mechanism.
- Hemorrhagic shock is the commonest hypovolemic shock.
- Cardiogenic shock occurs due to pump failure.
- Septic shock initially causes warm vasodilated skin.
- Anaphylactic shock is mediated by histamine release.
- Irreversible shock causes permanent organ damage.
- Early treatment significantly improves survival.
- Urine output is an important indicator of organ perfusion.
- Excessive fluids may worsen cardiogenic shock.