
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Coronary artery disease is one of the most important cardiovascular disorders and is strongly linked with abnormal lipid metabolism. The coronary arteries supply oxygen-rich blood to cardiac muscle, and narrowing of these arteries reduces myocardial oxygen supply. Biochemistry is central to this topic because cholesterol, lipoproteins, cardiac biomarkers, electrolytes, and vitamins all directly affect heart function. Atherosclerosis develops when lipids accumulate in arterial walls, leading to plaque formation and possible myocardial infarction. Laboratory tests such as lipid profile, troponins, CK-MB, and electrolytes help in diagnosis and monitoring. Understanding this topic helps students connect lipid metabolism with clinical heart disease and prevention strategies.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Lipids: Organic molecules that are insoluble in water but soluble in organic solvents.
- Cholesterol: A sterol lipid present in cell membranes and used to synthesize steroid hormones, bile acids, and vitamin D.
- Lipoproteins: Protein-lipid complexes that transport lipids in blood.
- Atherosclerosis: Progressive disease of arteries caused by lipid deposition, inflammation, and fibrous plaque formation.
- Coronary artery disease: Narrowing or blockage of coronary arteries, usually due to atherosclerosis.
- Myocardial infarction: Death of cardiac muscle due to prolonged ischemia.
- Cardiac biomarkers: Blood substances released after myocardial injury, used for diagnosis of MI.
- Troponin: Highly specific cardiac biomarker for myocardial damage.
- Dyslipidemia: Abnormal blood lipid levels, especially high LDL or low HDL.
🔹 3️⃣ Core Learning — Curriculum Coverage
A. Lipids: Definition, Classification and Functions
🧠 CORE
- Lipids are hydrophobic or amphipathic biomolecules.
- Major classes include fatty acids, triglycerides, phospholipids, cholesterol, glycolipids, and lipoproteins.
- Triglycerides are the major storage form of energy.
- Phospholipids are major structural components of cell membranes.
- Cholesterol stabilizes cell membranes and forms steroid hormones, bile acids, and vitamin D.
- Lipids act as energy stores, membrane components, signaling molecules, and thermal insulators.
- Essential fatty acids are required for normal cell function and must be obtained from diet.
🔬 CONCEPT EXPLAINED
Lipids are important because they perform both structural and metabolic roles. In the heart and blood vessels, lipids are especially important because they influence membrane stability, energy supply, inflammation, and vascular health. Triglycerides store large amounts of energy, while phospholipids and cholesterol help maintain the structure of cell membranes.
Cholesterol is not always harmful. It is essential for normal body function, but excess cholesterol, especially in the form of LDL, contributes to atherosclerosis. Therefore, lipid function depends on balance, transport, and proper metabolism.
⚠️ CLINICAL IMPORTANCE
Abnormal lipid levels increase the risk of coronary artery disease. High LDL cholesterol promotes plaque formation, while HDL helps remove cholesterol from tissues. Persistent dyslipidemia is one of the major modifiable risk factors for ischemic heart disease.
B. Cholesterol: Chemical Structure, Function and Fate in the Body
🧠 CORE
- Cholesterol is a sterol lipid with four fused hydrocarbon rings.
- It has a hydroxyl group, making it weakly amphipathic.
- It is present in animal cell membranes.
- It maintains membrane fluidity and stability.
- It is a precursor of steroid hormones, bile acids, and vitamin D.
- Cholesterol is transported in blood by lipoproteins.
- Excess cholesterol may deposit in arterial walls.
- Cholesterol is eliminated mainly after conversion into bile acids.
🔬 CONCEPT EXPLAINED
Chemically, cholesterol has a rigid ring structure. This structure allows it to fit between phospholipids in cell membranes and regulate membrane fluidity. In warm conditions, cholesterol prevents excessive membrane movement; in cold conditions, it prevents membranes from becoming too rigid.
The body obtains cholesterol from diet and also synthesizes it mainly in the liver. After synthesis or absorption, cholesterol is transported through blood by lipoproteins because it is not water-soluble. It may be used for membrane formation, converted into steroid hormones, converted into bile acids, or stored as cholesterol esters.
The liver plays a central role in cholesterol balance. It takes up cholesterol, packages it into lipoproteins, converts it into bile acids, and excretes it through bile.
⚠️ CLINICAL IMPORTANCE
When cholesterol transport becomes abnormal, especially when LDL is high, cholesterol enters the arterial wall. Oxidized LDL triggers inflammation and foam cell formation, leading to atherosclerotic plaque. This is the biochemical basis of coronary artery disease.
C. Lipoproteins and Their Functions
🧠 CORE
- Lipoproteins transport lipids in blood.
- They contain triglycerides, cholesterol, phospholipids, and apoproteins.
- Major lipoproteins are chylomicrons, VLDL, IDL, LDL, and HDL.
- Chylomicrons transport dietary triglycerides.
- VLDL transports endogenous triglycerides from the liver.
- LDL delivers cholesterol to tissues.
- HDL removes excess cholesterol from tissues and returns it to the liver.
- LDL is commonly called “bad cholesterol”; HDL is commonly called “good cholesterol.”
🔬 CONCEPT EXPLAINED
Because lipids are insoluble in plasma, they need carriers. Lipoproteins solve this problem by forming particles with a lipid core and a protein-phospholipid outer layer. The outer layer allows them to move in blood.
Each lipoprotein has a specific role. Chylomicrons carry dietary fat from the intestine. VLDL carries triglycerides made in the liver. LDL is formed from VLDL metabolism and carries cholesterol to tissues. HDL works in the opposite direction by collecting excess cholesterol from tissues and blood vessels and returning it to the liver.
This balance between LDL delivery and HDL removal is very important in coronary artery disease.
⚠️ CLINICAL IMPORTANCE
High LDL increases cholesterol delivery to arterial walls, promoting plaque formation. Low HDL reduces cholesterol removal, increasing cardiovascular risk. Therefore, lipid profile interpretation is essential in assessing CAD risk.
![]()
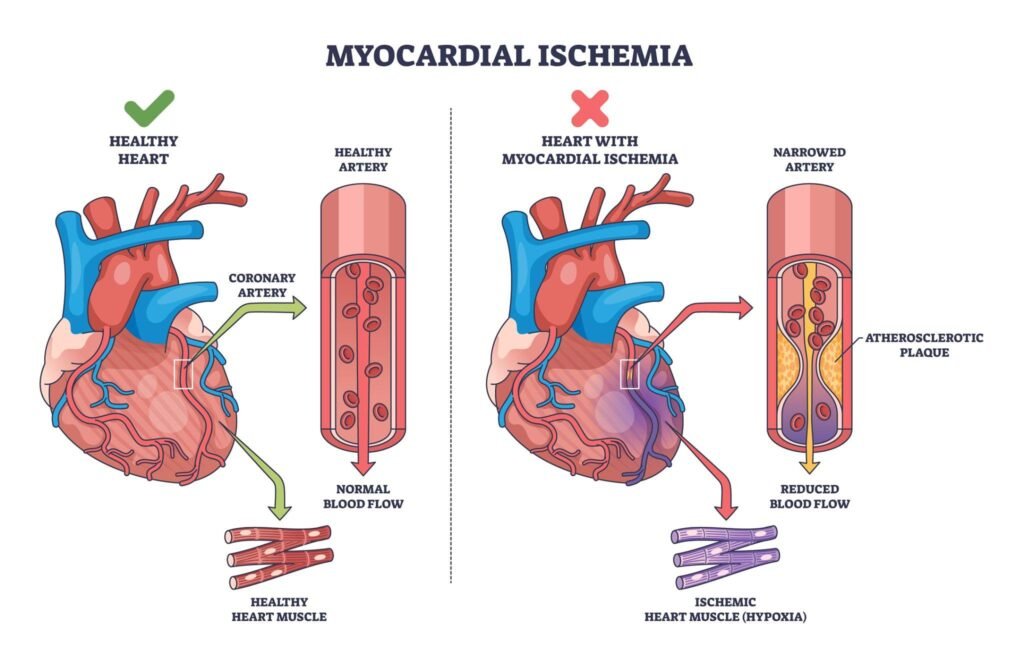
D. Atherosclerosis and Coronary Artery Disease
🧠 CORE
- CAD usually results from atherosclerosis of coronary arteries.
- Major risk factors include dyslipidemia, hypertension, diabetes, smoking, obesity, family history, and sedentary lifestyle.
- Atherosclerosis begins with endothelial injury.
- LDL enters the arterial wall and becomes oxidized.
- Macrophages engulf oxidized LDL and become foam cells.
- Fatty streak is the earliest visible lesion.
- Fibrous plaque narrows the artery.
- Plaque rupture may cause thrombosis and myocardial infarction.
🔬 CONCEPT EXPLAINED
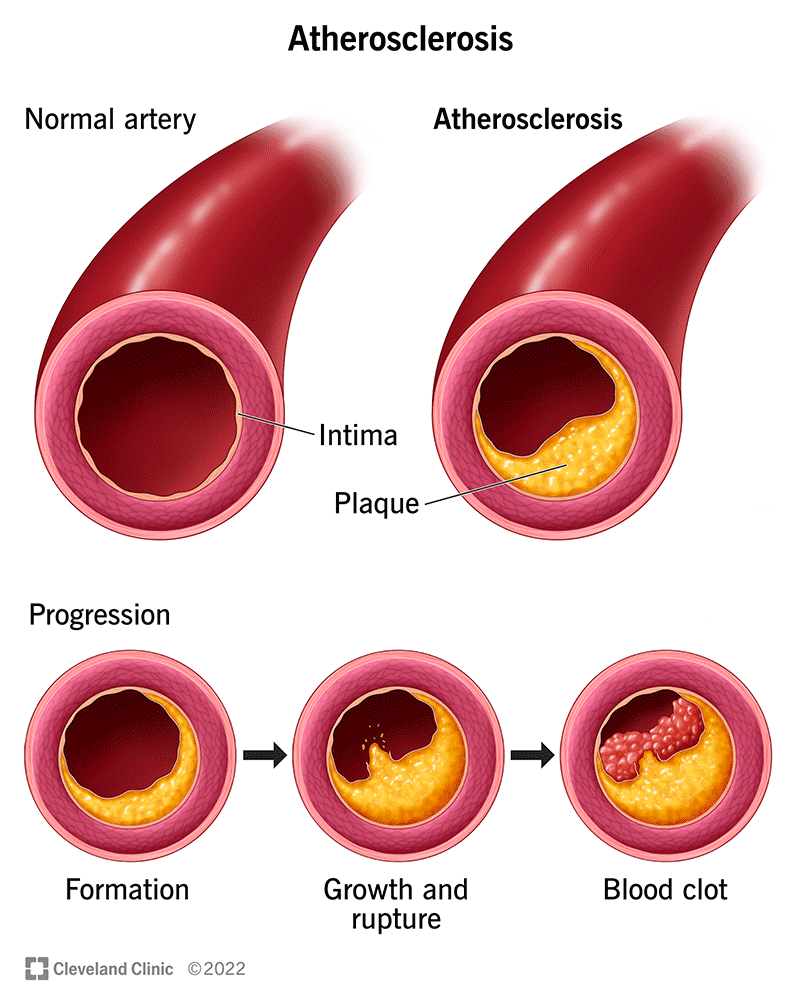
Atherosclerosis is not simply fat deposition; it is a chronic inflammatory process. The inner lining of the artery, called endothelium, becomes damaged due to factors like high LDL, hypertension, smoking, or diabetes. Once the endothelium is injured, LDL particles enter the arterial wall.
Inside the wall, LDL becomes oxidized. Macrophages take up oxidized LDL and become foam cells. These foam cells form fatty streaks. Over time, smooth muscle cells migrate and produce collagen, forming a fibrous cap. This creates an atherosclerotic plaque.
If the plaque gradually enlarges, it narrows the coronary artery and causes angina. If the plaque ruptures suddenly, a blood clot may form and block the artery, causing myocardial infarction.
⚠️ CLINICAL IMPORTANCE
Stable plaque usually causes exertional angina. Unstable plaque may rupture and cause acute coronary syndrome. Laboratory diagnosis includes lipid profile, cardiac biomarkers, glucose/HbA1c, renal function, and inflammatory markers when clinically required.
E. Stages of Atherosclerosis
🧠 CORE
- Endothelial injury begins the process.
- LDL entry and oxidation occur in the arterial wall.
- Foam cell formation produces fatty streaks.
- Smooth muscle migration forms plaque structure.
- Fibrous plaque formation narrows the lumen.
- Complicated plaque may rupture, bleed, calcify, or thrombose.
🔬 CONCEPT EXPLAINED
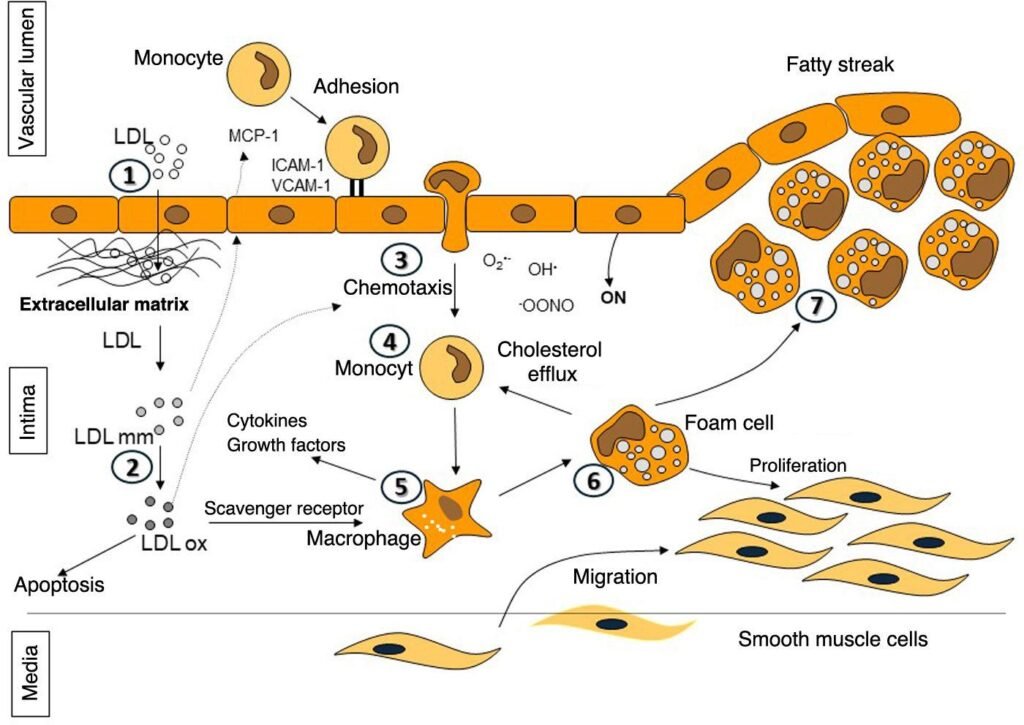
The earliest stage is endothelial dysfunction. This allows LDL to enter the intima. Oxidized LDL attracts monocytes, which enter the wall and become macrophages. These macrophages consume oxidized LDL and become foam cells.
As the process continues, smooth muscle cells move from the media to the intima. They produce extracellular matrix and collagen, forming a fibrous cap. The plaque may remain stable or become unstable. An unstable plaque has a thin cap and is more likely to rupture.
⚠️ CLINICAL IMPORTANCE
Plaque rupture is clinically more dangerous than gradual narrowing because it can suddenly produce coronary thrombosis and acute myocardial infarction.
F. Cardiac Biomarkers in Myocardial Infarction
🧠 CORE
- Cardiac biomarkers are released into blood after myocardial cell injury.
- Troponin I and T are most specific for myocardial infarction.
- CK-MB is useful for detecting reinfarction.
- Myoglobin rises early but is not specific.
- LDH rises late and remains elevated longer.
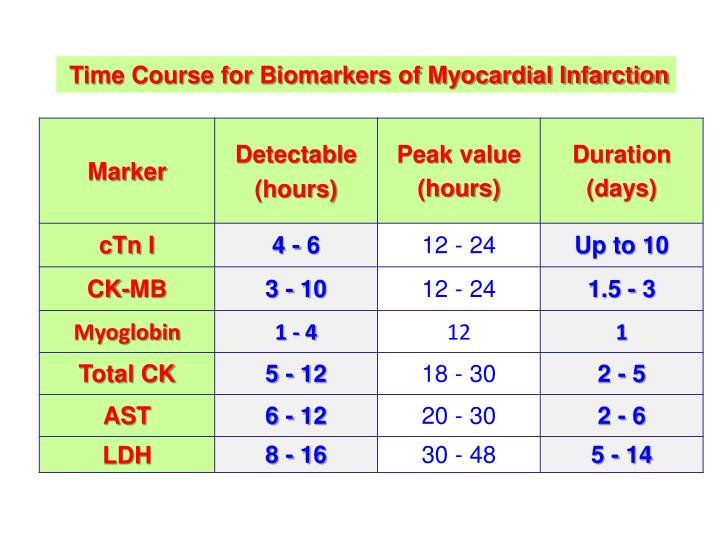
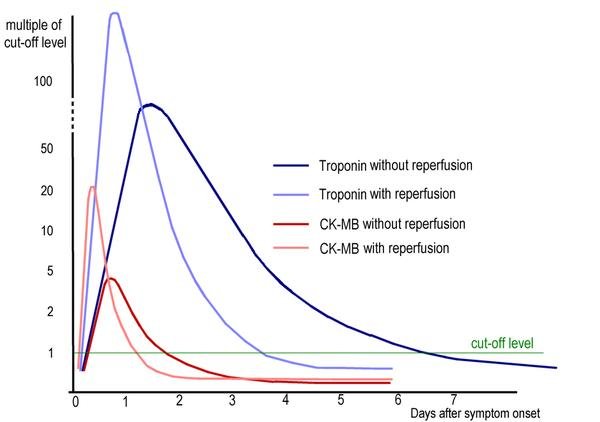
- Troponins rise within hours and remain elevated for several days.
- Biomarker pattern helps confirm timing and diagnosis of MI.
🔬 CONCEPT EXPLAINED
Cardiac muscle cells contain structural and enzymatic proteins. When myocardial cells are injured due to ischemia, their membranes lose integrity and intracellular proteins leak into the blood. This is the biochemical basis of cardiac biomarker testing.
Troponins are part of the contractile apparatus of cardiac muscle. Because cardiac troponin I and T are highly specific to heart muscle, their elevation strongly supports myocardial injury. CK-MB is also found in cardiac muscle and rises earlier than LDH. Myoglobin rises very early but is also present in skeletal muscle, so it is less specific.
⚠️ CLINICAL IMPORTANCE
Troponin is the most important biomarker for myocardial infarction. CK-MB may help detect reinfarction because it returns to normal earlier than troponin. A single value is less useful than serial testing because rise and fall patterns are important.
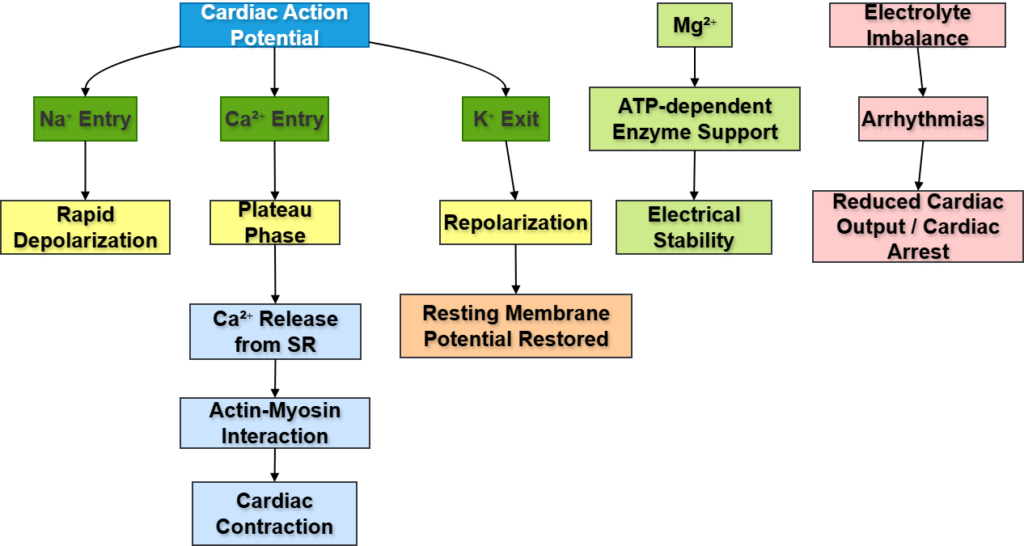
G. Electrolytes and Cardiac Muscle Contractility
🧠 CORE
- Na⁺, K⁺, Ca²⁺, and Mg²⁺ are essential for cardiac electrical and mechanical activity.
- Na⁺ is important for depolarization.
- K⁺ is important for repolarization and resting membrane potential.
- Ca²⁺ triggers cardiac muscle contraction.
- Mg²⁺ supports ATP-related enzyme activity and stabilizes electrical function.
- Electrolyte imbalance can cause arrhythmias.
- Severe abnormalities may lead to cardiac arrest.
🔬 CONCEPT EXPLAINED
Cardiac contraction depends on electrical activity followed by mechanical contraction. Sodium entry helps initiate depolarization. Potassium movement helps restore the resting membrane potential. Calcium entry during the plateau phase triggers calcium release from the sarcoplasmic reticulum, leading to actin-myosin interaction and contraction.
Magnesium is important because many ATP-dependent processes require Mg²⁺. It also helps regulate ion channels and prevents excessive excitability.
⚠️ CLINICAL IMPORTANCE
Hypokalemia and hyperkalemia can both cause dangerous arrhythmias. Hypocalcemia may reduce contractility, while hypercalcemia may increase contraction and disturb rhythm. Magnesium deficiency may predispose to arrhythmias.
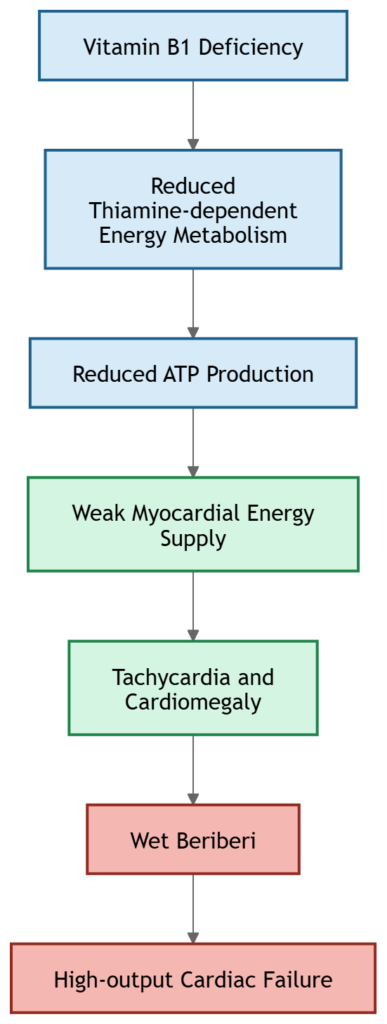
H. Vitamin B1 Deficiency and Cardiac Manifestations
🧠 CORE
- Vitamin B1 is also called thiamine.
- It is important for carbohydrate metabolism and energy production.
- The heart depends heavily on ATP.
- Severe thiamine deficiency can cause beriberi.
- Wet beriberi mainly affects the cardiovascular system.
- It may cause tachycardia, cardiomegaly, high-output cardiac failure, and edema.
🔬 CONCEPT EXPLAINED
Thiamine acts as a coenzyme in energy-producing pathways. When thiamine is deficient, cells cannot efficiently produce ATP from carbohydrates. The heart has a high energy demand, so impaired ATP production affects cardiac pumping.
In wet beriberi, peripheral vasodilation and fluid retention increase the workload on the heart. Over time, this may lead to high-output heart failure.
⚠️ CLINICAL IMPORTANCE
In a malnourished patient or chronic alcohol user with cardiac failure symptoms, thiamine deficiency should be considered. It is a biochemical deficiency with major cardiovascular consequences.
I. Drugs Used in CAD and Lipid Lowering
🧠 CORE
- CAD treatment includes anti-anginal, antiplatelet, anticoagulant, thrombolytic, and lipid-lowering drugs.
- Nitrates relieve angina by reducing cardiac workload.
- Beta-blockers reduce heart rate and oxygen demand.
- Calcium channel blockers reduce vascular tone and workload.
- Antiplatelet drugs reduce thrombus formation.
- Statins are the main lipid-lowering drugs.
- Other lipid-lowering drugs include fibrates, bile acid sequestrants, ezetimibe, and PCSK9 inhibitors.
🔬 CONCEPT EXPLAINED
The biochemical goal in CAD is to reduce myocardial oxygen demand, improve blood flow, prevent clot formation, and correct lipid abnormalities. Statins lower cholesterol mainly by reducing hepatic cholesterol synthesis and increasing LDL receptor expression, which removes LDL from blood.
Antiplatelet drugs are important because plaque rupture leads to platelet activation and thrombus formation. Lipid-lowering therapy reduces future plaque progression and cardiovascular risk.
⚠️ CLINICAL IMPORTANCE
In CAD, treatment is not only for symptom relief. It also prevents myocardial infarction, recurrent ischemia, and sudden cardiac death.
J. Prevention and Community Health Approach
🧠 CORE
- Cardiovascular disease prevention occurs at different levels.
- Primordial prevention: Prevent risk factors from developing.
- Primary prevention: Control risk factors before disease occurs.
- Secondary prevention: Detect and treat early disease.
- Tertiary prevention: Reduce complications and disability.
- Lifestyle modification is central at all levels.
- Community awareness, screening, and follow-up reduce disease burden.
🔬 CONCEPT EXPLAINED
CAD is strongly influenced by lifestyle and metabolic risk factors. Community medicine focuses on preventing disease before it becomes clinically severe. Healthy diet, exercise, tobacco control, blood pressure control, diabetes control, and lipid screening all reduce CAD risk.
Prevention is not limited to hospitals. Schools, workplaces, families, and communities play important roles in reducing cardiovascular risk.
⚠️ CLINICAL IMPORTANCE
For a population, prevention is more effective than treating advanced MI. For an individual patient, controlling LDL, blood pressure, diabetes, smoking, and obesity can significantly reduce future cardiovascular events.
K. Medicolegal Aspects of Sudden Death Due to Cardiovascular Disease
🧠 CORE
- Sudden cardiovascular death may occur due to myocardial infarction, arrhythmia, or severe coronary artery disease.
- It may occur unexpectedly in apparently healthy individuals.
- Proper documentation is important.
- Autopsy may reveal coronary artery narrowing, thrombosis, or myocardial infarction.
- Medicolegal evaluation helps distinguish natural death from suspicious death.
🔬 CONCEPT EXPLAINED
Sudden death due to cardiovascular disease is often natural, but because it may occur unexpectedly, medicolegal assessment may be required. Coronary artery disease is one of the common causes. Severe coronary narrowing, plaque rupture, or arrhythmia may lead to sudden collapse.
⚠️ CLINICAL IMPORTANCE
Doctors must carefully document clinical history, examination findings, investigations, and circumstances of death. This is important for both medical and legal purposes.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
- Cholesterol structure → stabilizes cell membranes → supports normal cell function.
- Lipoprotein structure → transports insoluble lipids in plasma → maintains lipid delivery and removal.
- LDL function → delivers cholesterol to tissues → excess LDL promotes atherosclerosis.
- HDL function → removes cholesterol from tissues → protects against plaque formation.
- Coronary arteries → supply myocardium → narrowing causes ischemia.
- Cardiac biomarkers → released after myocardial injury → help diagnose MI.
- Electrolytes → regulate cardiac electrical activity → imbalance causes arrhythmias.
- Vitamin B1 → supports ATP production → deficiency weakens cardiac energy metabolism.
🩺 5️⃣ Clinical Correlation
1. Stable Angina
Occurs when coronary narrowing limits blood supply during exertion. Pain improves with rest or nitrates.
2. Myocardial Infarction
Occurs when coronary blood flow is suddenly blocked, usually by thrombus over ruptured plaque. Troponins are highly important for diagnosis.
3. Dyslipidemia
High LDL, high triglycerides, or low HDL increases CAD risk.
4. Arrhythmias Due to Electrolyte Imbalance
Potassium, calcium, and magnesium abnormalities may disturb cardiac rhythm.
5. Wet Beriberi
Vitamin B1 deficiency may cause high-output cardiac failure, edema, and tachycardia.
6. Sudden Cardiac Death
May result from severe CAD, acute MI, or fatal arrhythmia.
📌 6️⃣ Summary Points
- LDL delivers cholesterol to tissues and promotes atherosclerosis when elevated.
- HDL removes cholesterol from tissues and is protective.
- Cholesterol is essential for membranes, steroid hormones, bile acids, and vitamin D.
- Atherosclerosis is an inflammatory lipid-related arterial disease.
- Foam cells are macrophages filled with oxidized LDL.
- Fatty streak is the earliest visible lesion of atherosclerosis.
- Plaque rupture can cause thrombosis and myocardial infarction.
- Troponin I and T are the most specific biomarkers of MI.
- CK-MB is useful for detecting reinfarction.
- Calcium is essential for cardiac muscle contraction.
- Potassium imbalance can cause dangerous arrhythmias.
- Vitamin B1 deficiency may cause wet beriberi and heart failure.