
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Cardiac output is the amount of blood pumped by the heart per minute. It is one of the most important indicators of cardiovascular function because it determines tissue perfusion and oxygen delivery. Venous return is closely linked with cardiac output because the heart can pump only the blood that returns to it. This topic mainly involves the heart, veins, skeletal muscle pump, autonomic nervous system, and peripheral circulation. Understanding cardiac output also explains exercise physiology, shock, edema, breathlessness, and heart failure. Clinically, reduced cardiac output can cause fatigue, hypotension, renal hypoperfusion, pulmonary congestion, and systemic venous congestion.
🔹 2️⃣ Foundation Concepts
Key Definitions
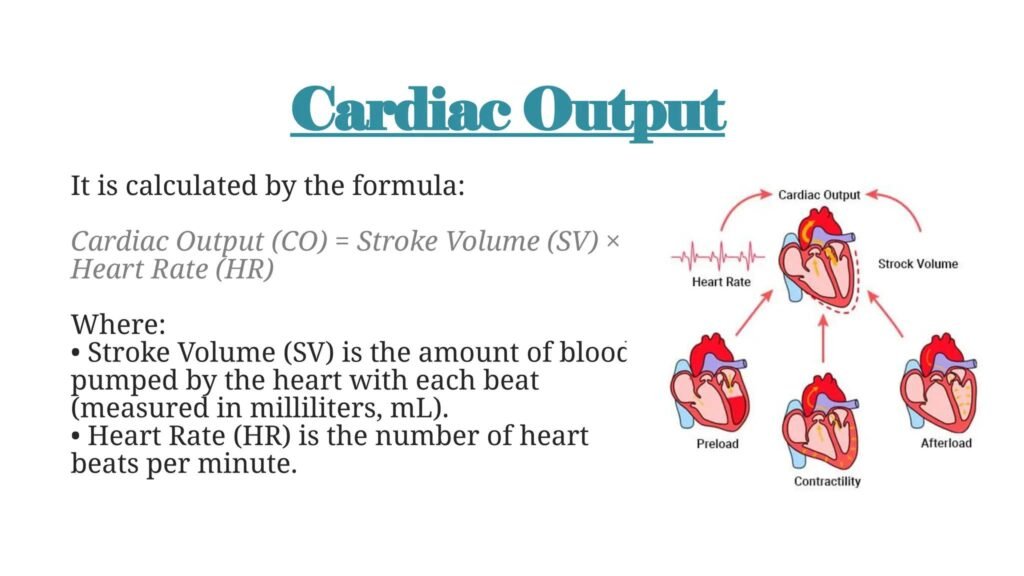
- Cardiac Output (CO): Amount of blood pumped by each ventricle per minute.
CO = Stroke Volume × Heart Rate - Stroke Volume (SV): Amount of blood ejected by ventricle per beat.
- Heart Rate (HR): Number of heart beats per minute.
- End-Diastolic Volume (EDV): Volume of blood in ventricle at the end of diastole.
- End-Systolic Volume (ESV): Volume of blood remaining in ventricle after systole.
- Ejection Fraction (EF): Percentage of EDV ejected during systole.
- Venous Return: Amount of blood returning to the right atrium per minute.
- Preload: Initial stretch of ventricular muscle before contraction; mainly related to EDV.
- Afterload: Resistance against which the ventricle must pump.
- Contractility: Intrinsic force of cardiac muscle contraction independent of preload.
- Peripheral Resistance: Resistance offered by systemic blood vessels, mainly arterioles.
🔹 3️⃣ Core Learning — Curriculum Coverage
A. Cardiac Output: Basic Concept and Regulation
🧠 CORE
- Cardiac output is the volume of blood pumped by the heart per minute.
- Normal resting cardiac output is about 5 L/min in adults.
- It increases greatly during exercise.
- Cardiac output depends mainly on:
- Heart rate
- Stroke volume
- Venous return
- Myocardial contractility
- Peripheral resistance
- The right and left ventricular outputs are normally equal.
- Cardiac output maintains blood pressure and tissue perfusion.
🔬 CONCEPT EXPLAINED
Cardiac output exists to match tissue blood flow with metabolic demand. At rest, organs require a moderate supply of oxygen and nutrients. During activity, skeletal muscles need more oxygen, so cardiac output increases.
The heart does not work alone. It is controlled by venous return, autonomic nervous system, blood volume, vascular tone, and myocardial contractility.
Cause → Effect:
- Increased venous return → increased EDV
- Increased EDV → increased myocardial stretch
- Increased stretch → stronger contraction
- Stronger contraction → increased stroke volume
- Increased stroke volume → increased cardiac output
This is the basis of the Frank-Starling mechanism.
⚠️ CLINICAL IMPORTANCE
If cardiac output falls, organs receive less blood. The brain may show dizziness, kidneys reduce urine output, muscles become fatigued, and lungs may develop congestion if the left heart fails.
B. Pressure-Volume Loop of the Left Ventricle
🧠 CORE
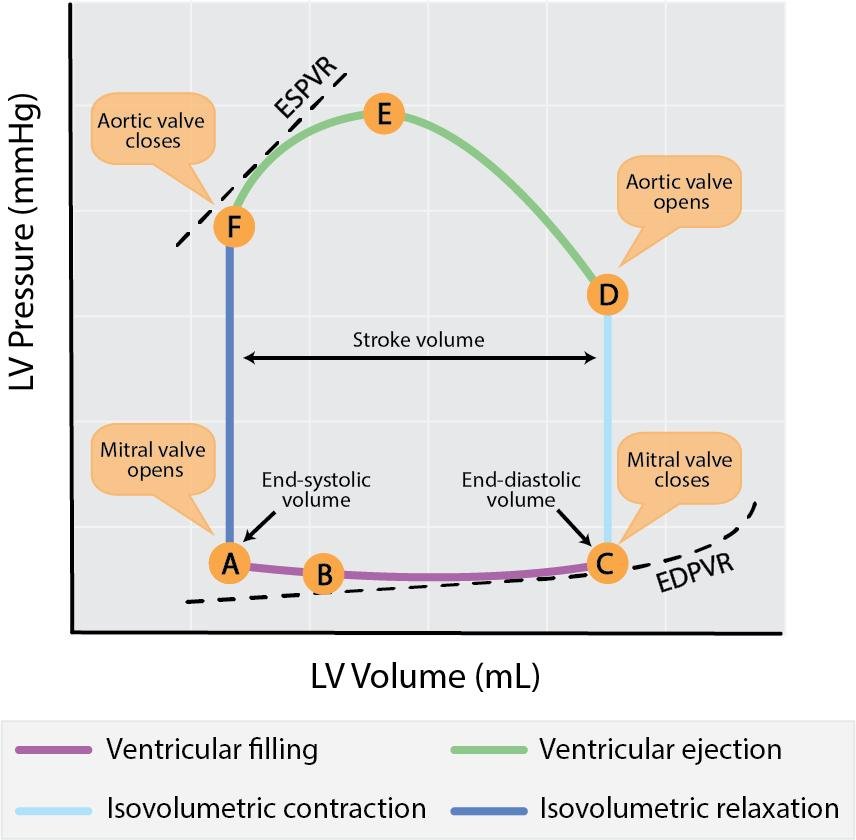
- The pressure-volume loop shows changes in ventricular pressure and volume during one cardiac cycle.
- It includes:
- Ventricular filling
- Isovolumetric contraction
- Ventricular ejection
- Isovolumetric relaxation
- EDV is the maximum ventricular volume before contraction.
- ESV is the blood left after contraction.
- Stroke volume = EDV − ESV.
- Ejection fraction = SV / EDV × 100.
- Systolic work output is represented by the area inside the loop.
🔬 CONCEPT EXPLAINED
The pressure-volume loop helps students understand how the ventricle fills, contracts, ejects blood, and relaxes.
Stepwise logic:
- Ventricular filling:
Mitral valve opens and blood enters the left ventricle. Ventricular volume increases. - End-diastolic volume reached:
At the end of filling, the ventricle contains maximum blood. - Isovolumetric contraction:
Mitral valve closes. The ventricle contracts but volume does not change because both valves are closed. - Ventricular ejection:
When ventricular pressure exceeds aortic pressure, the aortic valve opens and blood is ejected. - End-systolic volume remains:
After ejection, some blood remains in the ventricle. - Isovolumetric relaxation:
Aortic valve closes. The ventricle relaxes with no change in volume until mitral valve opens again.
⚠️ CLINICAL IMPORTANCE
- Increased preload shifts the loop to the right because EDV increases.
- Increased afterload increases ventricular pressure and may reduce stroke volume.
- Reduced contractility increases ESV and decreases ejection fraction.
- In heart failure, pressure-volume loop changes show poor ventricular pumping.
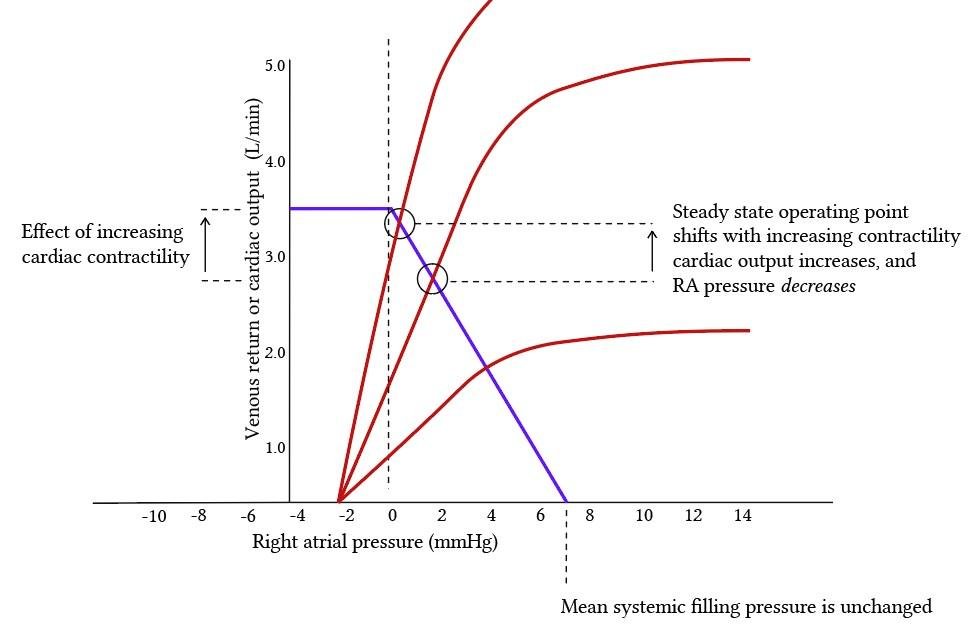
C. Frank-Starling Mechanism: Control of Cardiac Output by Venous Return
🧠 CORE
- Frank-Starling law states that the heart pumps all blood returned to it within physiological limits.
- Increased venous return increases EDV.
- Increased EDV stretches cardiac muscle fibers.
- Moderate stretch improves actin-myosin interaction.
- This increases force of contraction.
- Stroke volume rises.
- Cardiac output increases.
- It balances right and left ventricular output.
🔬 CONCEPT EXPLAINED
The Frank-Starling mechanism is an intrinsic cardiac control mechanism. It does not require nervous stimulation.
Cause → Effect:
- More venous return → more ventricular filling
- More filling → increased myocardial fiber length
- Increased fiber length → stronger contraction
- Stronger contraction → greater stroke volume
- Greater stroke volume → increased cardiac output
Why it exists:
This mechanism prevents blood from accumulating in veins or lungs. If the right ventricle pumps more blood to the lungs, the left ventricle receives more blood and automatically pumps more. This keeps both sides of the heart balanced.
⚠️ CLINICAL IMPORTANCE
In heart failure, excessive stretch does not improve contraction. The ventricle becomes weak and dilated. Blood backs up, causing pulmonary congestion in left-sided failure and peripheral edema in right-sided failure.
D. Venous Return and Its Regulation
🧠 CORE
- Venous return is blood returning to the right atrium.
- It normally equals cardiac output.
- It depends on:
- Blood volume
- Venous tone
- Skeletal muscle pump
- Respiratory pump
- Right atrial pressure
- Peripheral resistance
- Veins act as capacitance vessels.
- Sympathetic stimulation increases venous return by venoconstriction.
🔬 CONCEPT EXPLAINED
Venous return is the main determinant of cardiac output in normal physiology. The heart cannot pump more blood than it receives.
Control mechanisms:
- Blood volume: More blood volume increases venous return.
- Venous tone: Sympathetic stimulation constricts veins and pushes blood toward the heart.
- Skeletal muscle pump: Contracting muscles compress veins and move blood upward.
- Venous valves: Prevent backflow of blood.
- Respiratory pump: Inspiration lowers thoracic pressure and increases venous return.
- Right atrial pressure: High right atrial pressure reduces venous return.
Movement coordination sequence:
- Initiation: Physical activity begins.
- Muscle activation: Skeletal muscles contract rhythmically.
- Joint movement: Limb movement compresses deep veins.
- Functional outcome: Blood is pushed toward the heart, increasing venous return and cardiac output.
⚠️ CLINICAL IMPORTANCE
Prolonged standing reduces venous return because blood pools in lower limbs. This may cause dizziness or fainting. Immobility can reduce muscle pump activity and increase risk of venous stasis.
E. Cardiac Contractility: Calcium, ATP, and Myocardial Force
🧠 CORE
- Contractility is the force of contraction at a given fiber length.
- Calcium is essential for cardiac muscle contraction.
- ATP is required for contraction and relaxation.
- Calcium enters through L-type calcium channels.
- Calcium triggers release of more calcium from sarcoplasmic reticulum.
- Actin-myosin interaction produces contraction.
- SERCA pumps calcium back into sarcoplasmic reticulum.
- Na⁺/Ca²⁺ exchanger removes calcium from the cell.
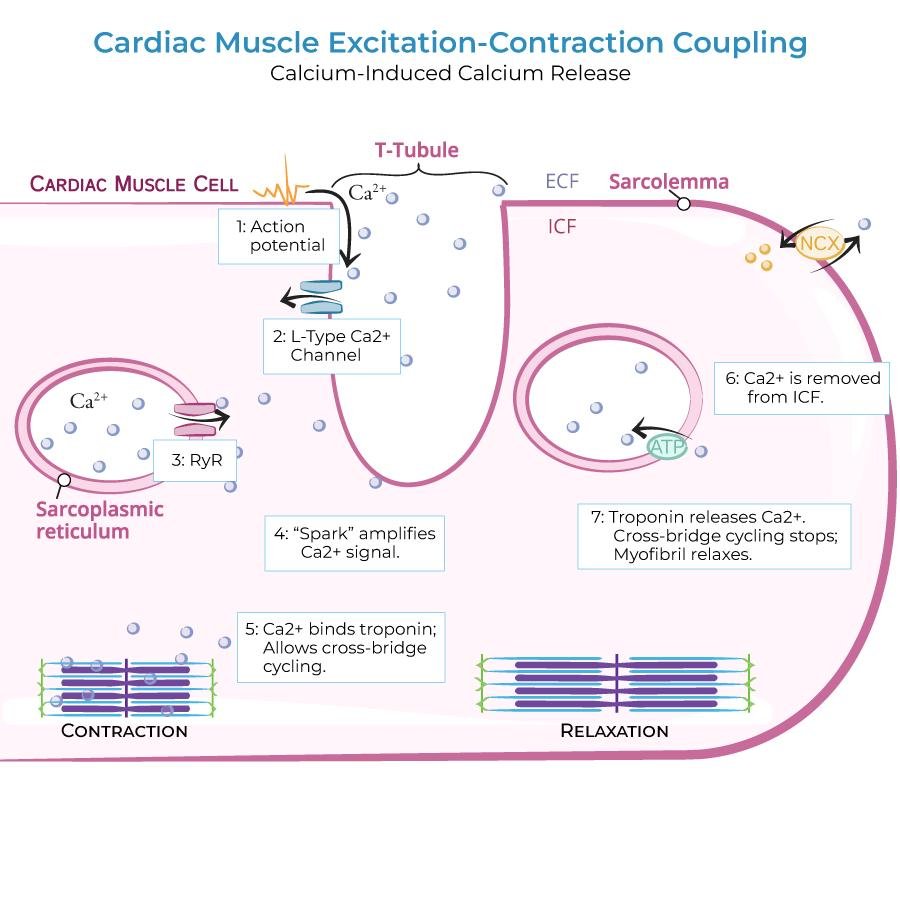
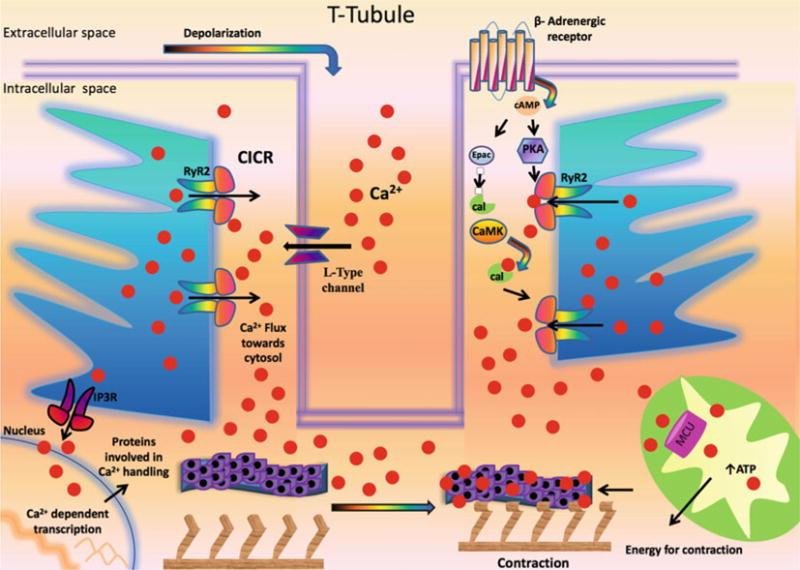
🔬 CONCEPT EXPLAINED
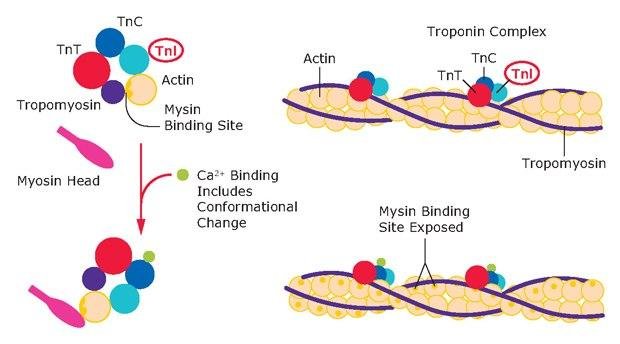
Cardiac contraction depends on calcium-induced calcium release.
Sequential activation:
- Action potential reaches cardiac muscle cell.
- Calcium enters through L-type calcium channels.
- This calcium stimulates sarcoplasmic reticulum to release more calcium.
- Calcium binds to troponin C.
- Tropomyosin moves away from actin-binding sites.
- Actin and myosin interact.
- Cross-bridge cycling occurs using ATP.
- Muscle contracts and blood is ejected.
- Calcium is removed from cytoplasm by SERCA and Na⁺/Ca²⁺ exchange.
- Muscle relaxes.
Functional outcome:
- More intracellular calcium → stronger contraction
- Less calcium availability → weaker contraction
- ATP deficiency → impaired contraction and relaxation
⚠️ CLINICAL IMPORTANCE
In myocardial ischemia, ATP production falls. This weakens contraction and reduces cardiac output. Calcium handling also becomes abnormal, contributing to arrhythmias and contractile failure.
F. Peripheral Resistance and Its Regulation
🧠 CORE
- Peripheral resistance is mainly controlled by arterioles.
- Increased resistance increases afterload.
- Decreased resistance reduces afterload.
- Arteriolar diameter is controlled by:
- Sympathetic nervous system
- Local metabolites
- Hormones
- Endothelial factors
- Peripheral resistance helps regulate arterial blood pressure.
- Excessive resistance can reduce stroke volume.
🔬 CONCEPT EXPLAINED
Peripheral resistance determines how difficult it is for the left ventricle to eject blood. If arterioles constrict, resistance rises. The ventricle must generate more pressure to open the aortic valve and eject blood.
Cause → Effect:
- Arteriolar constriction → increased peripheral resistance
- Increased resistance → increased afterload
- Increased afterload → reduced stroke volume
- Reduced stroke volume → reduced cardiac output
During exercise, arterioles in active muscles dilate. This reduces local resistance and allows increased blood flow to working muscles.
⚠️ CLINICAL IMPORTANCE
Hypertension increases afterload. Over time, the left ventricle works harder, leading to hypertrophy and eventually possible heart failure.
G. Normal Cardiac Output and Venous Return at Rest and During Activity
🧠 CORE
- Resting cardiac output is about 5 L/min.
- During exercise, cardiac output increases.
- Increase occurs due to:
- Increased heart rate
- Increased stroke volume
- Increased venous return
- Increased sympathetic stimulation
- Skeletal muscle pump improves venous return.
- Blood flow is redistributed to active muscles.
- Venous return must increase to sustain increased cardiac output.
🔬 CONCEPT EXPLAINED
At rest, tissue oxygen demand is moderate. During exercise, skeletal muscle metabolism increases. The cardiovascular system responds by increasing cardiac output.
Movement coordination sequence:
- Initiation: Exercise begins.
- Muscle activation: Skeletal muscles contract repeatedly.
- Joint movement: Limb movement compresses veins.
- Functional outcome: Venous return increases, EDV rises, stroke volume increases, and cardiac output rises.
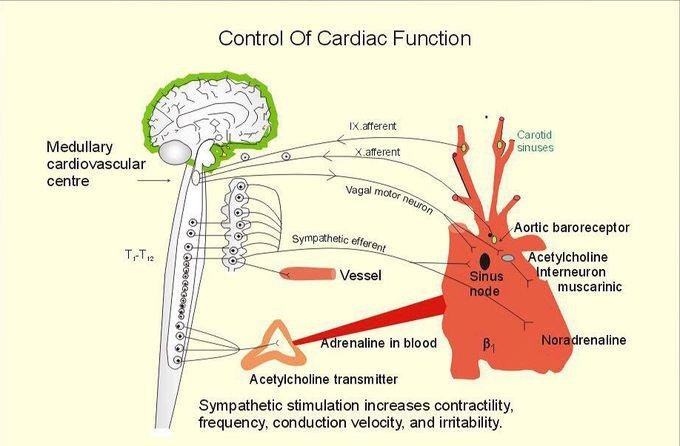
Control mechanisms:
- Sympathetic stimulation increases heart rate and contractility.
- Venoconstriction increases venous return.
- Local vasodilation increases blood flow to active muscles.
- Respiratory movements increase venous return.
⚠️ CLINICAL IMPORTANCE
Patients with heart failure cannot increase cardiac output adequately during exertion. Therefore, they develop fatigue and breathlessness on activity.
H. Measurement of Cardiac Output
🧠 CORE
- Cardiac output can be measured by:
- Fick principle
- Indicator dilution method
- Thermodilution method
- Echocardiography
- Fick principle is based on oxygen consumption.
- Indicator dilution uses concentration of injected indicator.
- Thermodilution uses temperature change.
- Echocardiography estimates stroke volume and cardiac output non-invasively.
🔬 CONCEPT EXPLAINED
The Fick principle states that cardiac output can be calculated if oxygen consumption and arterial-venous oxygen difference are known.
Basic logic:
- If tissues consume a known amount of oxygen
- And the difference between arterial and venous oxygen content is known
- Then blood flow required to deliver that oxygen can be calculated
Thermodilution is commonly used in clinical settings through a pulmonary artery catheter. Echocardiography is safer and commonly used to assess ventricular function and ejection fraction.
⚠️ CLINICAL IMPORTANCE
Measurement of cardiac output is important in shock, heart failure, ICU monitoring, and assessment of severe cardiac disease.
I. Causes of Abnormally High and Low Cardiac Output
🧠 CORE
High Cardiac Output Causes
- Exercise
- Fever
- Anemia
- Hyperthyroidism
- Arteriovenous fistula
- Pregnancy
- Beriberi
Low Cardiac Output Causes
- Myocardial infarction
- Heart failure
- Severe hemorrhage
- Shock
- Severe dehydration
- Cardiac tamponade
- Severe valve disease
- Arrhythmias
🔬 CONCEPT EXPLAINED
High cardiac output usually occurs when tissue demand is increased or peripheral resistance is reduced. For example, in anemia, oxygen-carrying capacity is low, so the heart pumps more blood to deliver adequate oxygen.
Low cardiac output occurs when the heart cannot pump effectively or venous return is reduced.
Cause → Effect:
- Myocardial infarction → damaged myocardium
- Damaged myocardium → reduced contractility
- Reduced contractility → reduced stroke volume
- Reduced stroke volume → reduced cardiac output
⚠️ CLINICAL IMPORTANCE
Low cardiac output is clinically more dangerous because it can lead to organ hypoperfusion, hypotension, renal failure, and shock.
J. Heart Failure: Definition and Types
🧠 CORE
- Heart failure is inability of the heart to pump sufficient blood for body needs.
- It may occur due to reduced pumping ability or excessive workload.
- It may be:
- Left-sided heart failure
- Right-sided heart failure
- Congestive heart failure
- Left-sided failure mainly causes pulmonary congestion.
- Right-sided failure mainly causes systemic venous congestion.
- Reduced cardiac output causes fatigue and poor tissue perfusion.
🔬 CONCEPT EXPLAINED
Heart failure does not mean the heart has stopped. It means the heart is unable to pump effectively according to body requirements.
In left-sided failure:
- Left ventricle fails to pump blood into aorta.
- Blood backs up into left atrium.
- Pressure rises in pulmonary veins.
- Fluid enters lung tissue.
- Patient develops breathlessness.
In right-sided failure:
- Right ventricle fails to pump blood into lungs.
- Blood backs up into systemic veins.
- Venous pressure rises.
- Fluid accumulates in tissues.
- Patient develops peripheral edema.
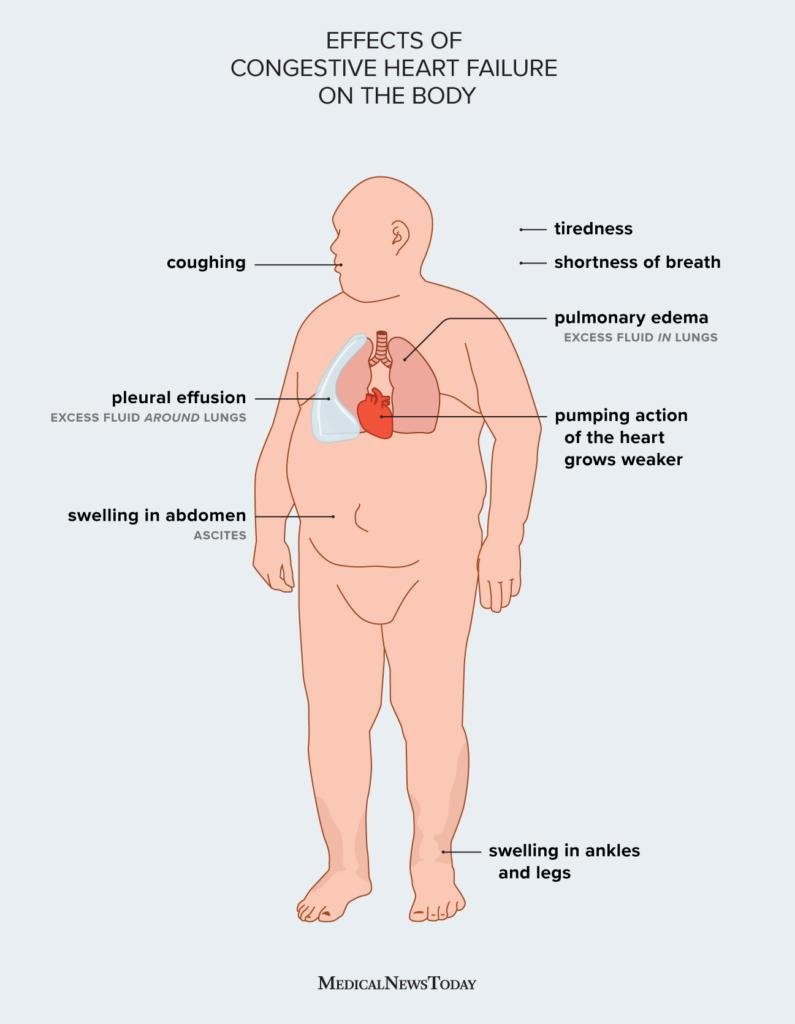
⚠️ CLINICAL IMPORTANCE
Heart failure explains three major clinical features:
- Breathlessness: Due to pulmonary congestion.
- Edema: Due to systemic venous congestion.
- Fatigue: Due to reduced cardiac output and poor tissue perfusion.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Function | Outcome |
|---|---|---|
| Left ventricle | Pumps blood into systemic circulation | Maintains tissue perfusion |
| Right ventricle | Pumps blood into pulmonary circulation | Enables blood oxygenation |
| Veins | Store and return blood to heart | Maintain venous return |
| Venous valves | Prevent backflow | Support upward blood flow |
| Skeletal muscles | Compress veins during movement | Increase venous return |
| Arterioles | Regulate peripheral resistance | Control blood pressure and afterload |
| Myocardial cells | Contract using calcium and ATP | Generate stroke volume |
| Autonomic nervous system | Controls HR, contractility, vascular tone | Matches CO with body demand |
🩺 5️⃣ Clinical Correlation
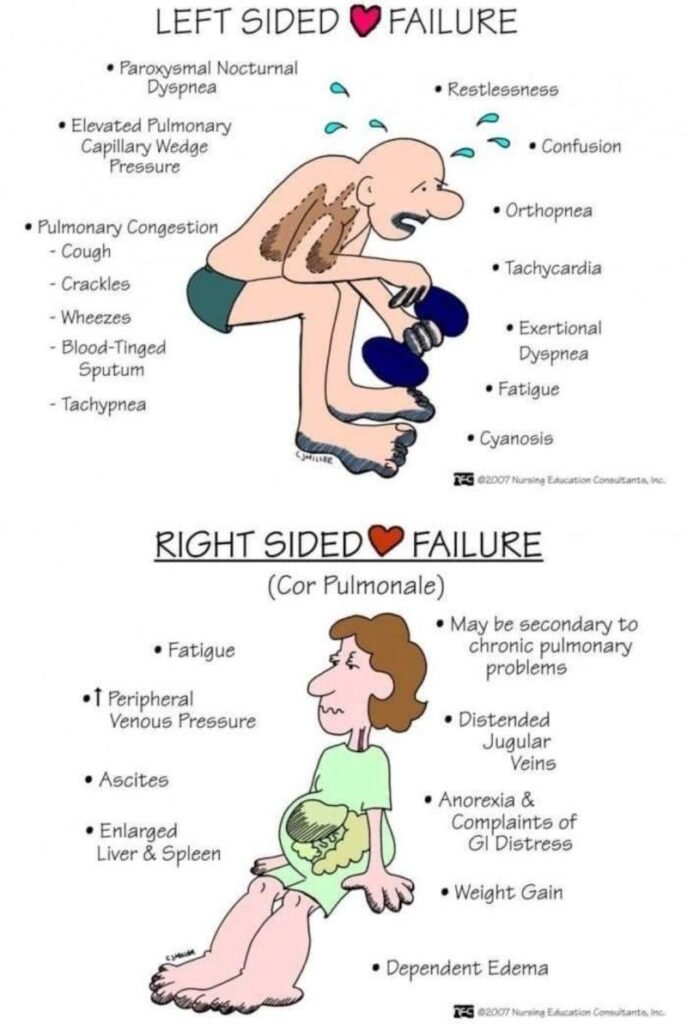
1. Left-Sided Heart Failure
- Main problem: left ventricle fails to pump blood forward.
- Blood backs up into lungs.
- Clinical features:
- Breathlessness
- Orthopnea
- Pulmonary congestion
- Fatigue
- Cause → Effect:
- Weak LV → increased pulmonary venous pressure → lung congestion → dyspnea
2. Right-Sided Heart Failure
- Main problem: right ventricle fails to pump blood to lungs.
- Blood backs up into systemic veins.
- Clinical features:
- Peripheral edema
- Raised JVP
- Hepatic congestion
- Ascites in severe cases
- Cause → Effect:
- Weak RV → systemic venous congestion → increased capillary pressure → edema
3. Myocardial Infarction and Low Cardiac Output
- Myocardial infarction damages cardiac muscle.
- Contractility decreases.
- Stroke volume falls.
- Cardiac output decreases.
- Patient may develop hypotension, shock, or heart failure.
4. Hypertension and Heart Failure
- Hypertension increases afterload.
- Left ventricle works harder.
- Initially, ventricular hypertrophy develops.
- Later, the ventricle may fail.
- Cardiac output decreases.
5. Anemia and High Cardiac Output
- Hemoglobin is reduced.
- Oxygen delivery falls.
- Body compensates by increasing cardiac output.
- Long-standing severe anemia may cause high-output heart failure.
📌 6️⃣ Summary Points
- Cardiac output = stroke volume × heart rate.
- Normal resting cardiac output is about 5 L/min.
- Venous return normally equals cardiac output.
- Frank-Starling mechanism matches cardiac output with venous return.
- Increased EDV increases myocardial stretch and stroke volume.
- Stroke volume = EDV − ESV.
- Ejection fraction = SV / EDV × 100.
- Calcium is essential for cardiac contraction.
- ATP is required for both contraction and relaxation.
- Increased peripheral resistance increases afterload.
- Left-sided heart failure causes pulmonary congestion and breathlessness.
- Right-sided heart failure causes systemic venous congestion and edema.