
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The heart is a continuously active muscular pump that requires a constant supply of oxygen and nutrients to maintain effective contraction. This supply is provided by the coronary circulation, which consists of specialized arteries and veins supplying the myocardium. Because cardiac muscle has very high metabolic demands, interruption of coronary blood flow rapidly leads to ischemia and myocardial infarction.
The heart is also enclosed within a fibroserous sac called the pericardium, which stabilizes the heart, prevents excessive movement, and reduces friction during cardiac activity. Disorders involving the pericardium or coronary vessels are among the most important causes of morbidity and mortality worldwide.
Understanding coronary circulation and pericardial anatomy is essential for interpreting ischemic heart disease, coronary thrombosis, pericarditis, cardiac tamponade, angiography, ECG changes, and emergency cardiac conditions.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Coronary circulation: Blood supply of the heart muscle through coronary arteries and veins.
- Coronary arteries: Arteries arising from ascending aorta supplying myocardium.
- Coronary sinus: Main venous channel draining the heart into the right atrium.
- Pericardium: Fibroserous sac surrounding the heart and roots of great vessels.
- Pericardial cavity: Potential space between parietal and visceral pericardium containing serous fluid.
- Coronary thrombosis: Formation of thrombus within a coronary artery causing obstruction.
- Pericarditis: Inflammation of the pericardium.
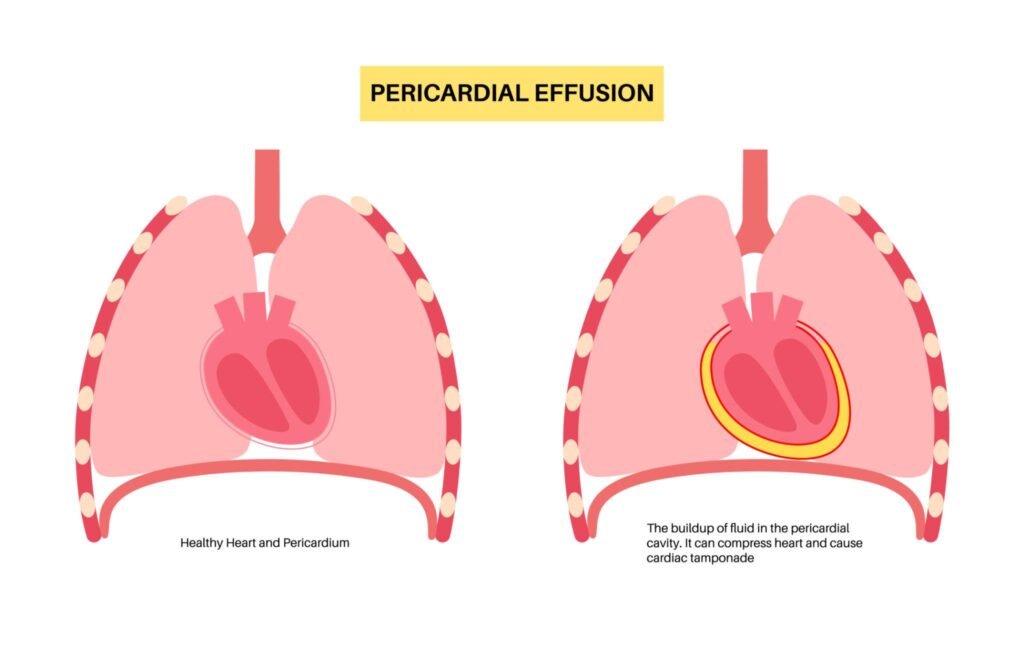
- Pericardial effusion: Abnormal accumulation of fluid in the pericardial cavity.
- Cardiac tamponade: Compression of heart due to rapid fluid accumulation in pericardial cavity.
Essential Terminology
- Right coronary artery (RCA)
- Left coronary artery (LCA)
- Anterior interventricular artery (LAD)
- Circumflex artery
- Marginal arteries
- Coronary dominance
- Anastomosis
- Myocardial ischemia
- Fibrous pericardium
- Serous pericardium
- Transverse sinus
- Oblique sinus
Basic Overview
- Coronary arteries arise from ascending aorta just above aortic valve.
- Blood flow to myocardium mainly occurs during diastole.
- Coronary veins drain mainly into coronary sinus.
- Pericardium has fibrous and serous layers.
- Reflections of serous pericardium form pericardial sinuses.
- Coronary artery obstruction causes ischemic heart disease.
- Rapid pericardial fluid accumulation may cause cardiac tamponade.
🔹 3️⃣ Core Learning — Curriculum Coverage
Coronary Arteries of the Heart
🧠 CORE
- Coronary arteries are functional end arteries supplying myocardium.
- Arise from ascending aorta above aortic valve cusps.
- Two main arteries:
- Right coronary artery (RCA)
- Left coronary artery (LCA)
- Coronary arteries travel within coronary sulcus and interventricular grooves.
- Myocardial oxygen extraction is very high at rest.
- Coronary circulation increases during increased cardiac work.
- Blood flow mainly occurs during ventricular relaxation (diastole).
🔬 CONCEPT EXPLAINED
The myocardium is thick, continuously contracting muscle tissue with extremely high oxygen demand. Diffusion from heart chambers alone is insufficient; therefore, a specialized arterial supply is necessary.
The coronary arteries originate from the ascending aorta immediately above the aortic valve within the aortic sinuses. During ventricular systole, contraction of myocardium compresses coronary vessels, reducing blood flow. During diastole, ventricular relaxation allows coronary perfusion. This explains why adequate diastolic pressure is critical for myocardial oxygenation.
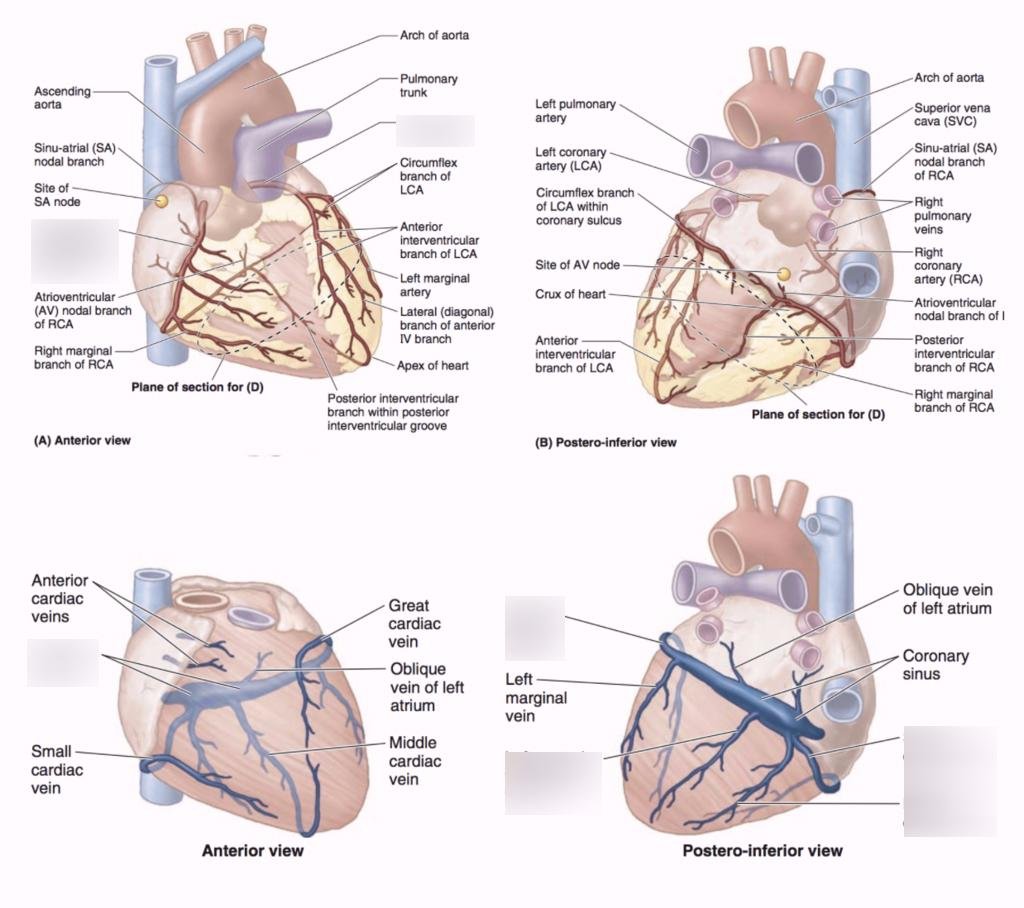
Right Coronary Artery (RCA)
Course
- Arises from anterior aortic sinus.
- Passes between right auricle and pulmonary trunk.
- Runs in coronary sulcus.
Major Branches
- Right marginal artery
- SA nodal branch
- AV nodal branch
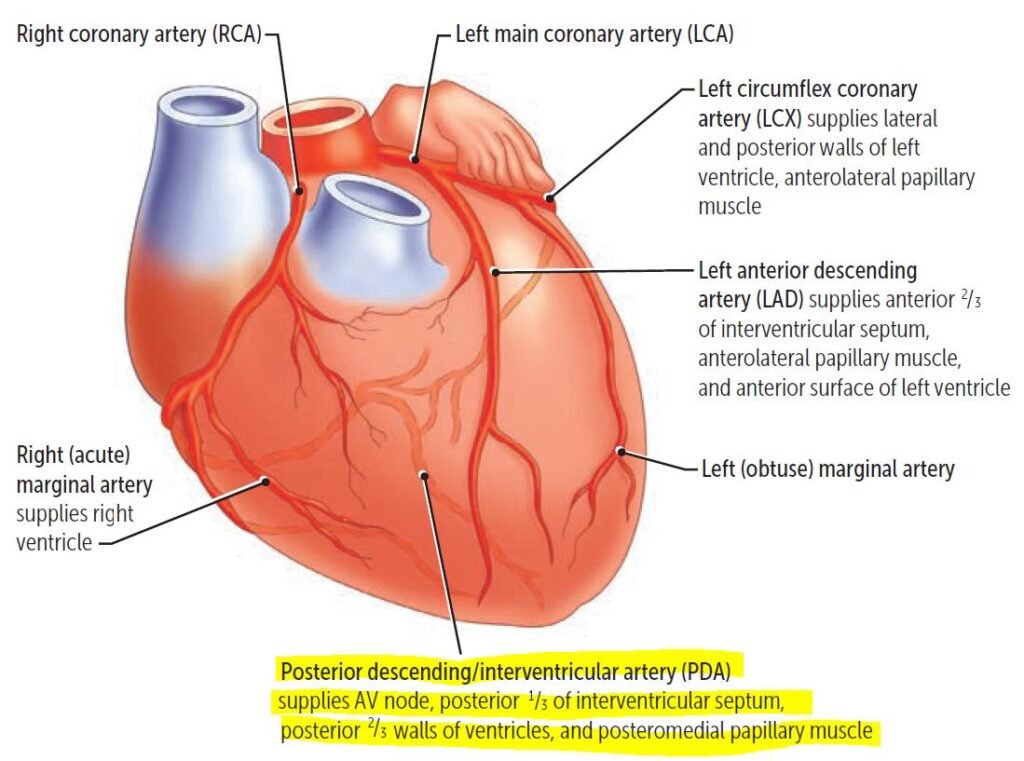
- Posterior interventricular artery
Areas Supplied
- Right atrium
- Most of right ventricle
- Part of left ventricle
- SA node (commonly)
- AV node
- Posterior one-third of interventricular septum
Left Coronary Artery (LCA)
Course
- Arises from left posterior aortic sinus.
- Passes behind pulmonary trunk.
- Divides into major branches.
Major Branches
- Anterior interventricular artery (LAD)
- Circumflex artery
- Left marginal artery
Areas Supplied
- Left atrium
- Most of left ventricle
- Part of right ventricle
- Anterior two-thirds of interventricular septum
- AV bundle and bundle branches
Coronary Anastomosis
Small arterial connections exist between branches of coronary arteries, especially near apex and interventricular septum. However, these are usually insufficient during sudden arterial blockage, making coronary arteries functionally end arteries.
Coronary Dominance
- Determined by artery giving posterior interventricular branch.
- RCA dominance is most common.
⚠️ CLINICAL IMPORTANCE
- Occlusion of LAD commonly causes anterior wall myocardial infarction.
- RCA blockage may produce arrhythmias due to SA or AV nodal ischemia.
- Reduced coronary perfusion causes angina pectoris.
- Severe prolonged ischemia causes myocardial infarction.
- Coronary angiography visualizes arterial obstruction.
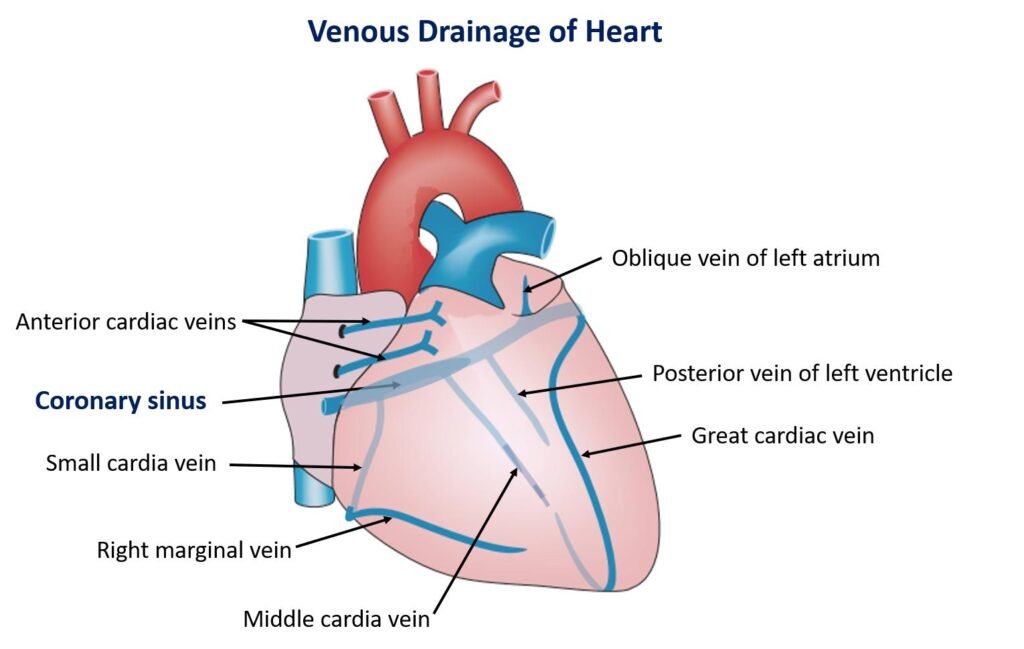
Venous and Lymphatic Drainage of the Heart
🧠 CORE
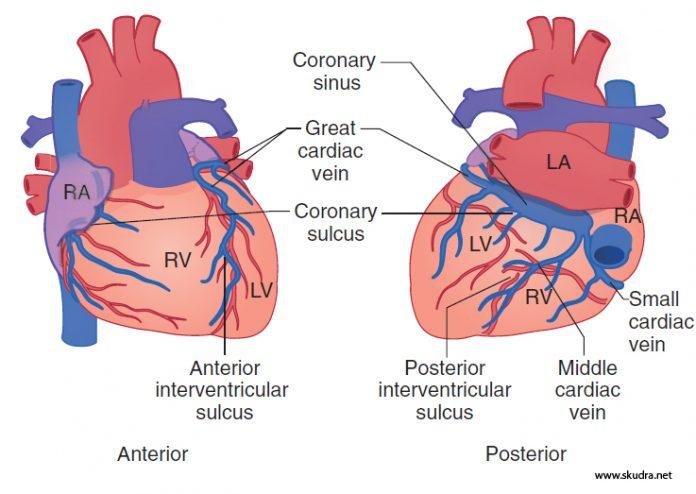
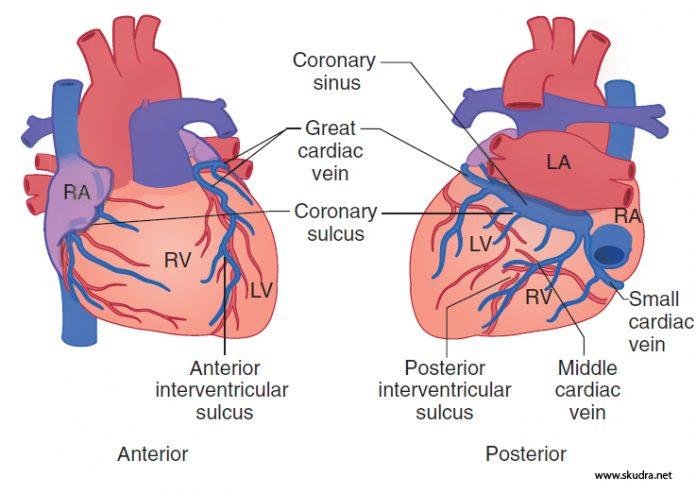
- Venous drainage mainly occurs through coronary sinus.
- Coronary sinus opens into right atrium.
- Great, middle, and small cardiac veins drain into coronary sinus.
- Anterior cardiac veins drain directly into right atrium.
- Lymphatics accompany coronary arteries.
- Cardiac lymph drains into tracheobronchial lymph nodes.
🔬 CONCEPT EXPLAINED
The myocardium continuously produces metabolic waste products requiring efficient venous drainage. Most venous blood enters the coronary sinus, which lies in posterior coronary sulcus.
Major Veins
- Great cardiac vein: accompanies LAD.
- Middle cardiac vein: accompanies posterior interventricular artery.
- Small cardiac vein: accompanies right marginal artery.
Some veins bypass coronary sinus and open directly into right atrium.
Cardiac lymphatics remove excess interstitial fluid and cellular debris. Lymphatic obstruction may worsen myocardial edema and inflammation.
⚠️ CLINICAL IMPORTANCE
- Coronary sinus catheterization is used in cardiac procedures.
- Venous obstruction may impair myocardial drainage.
- Lymphatic spread may contribute to inflammatory cardiac diseases.
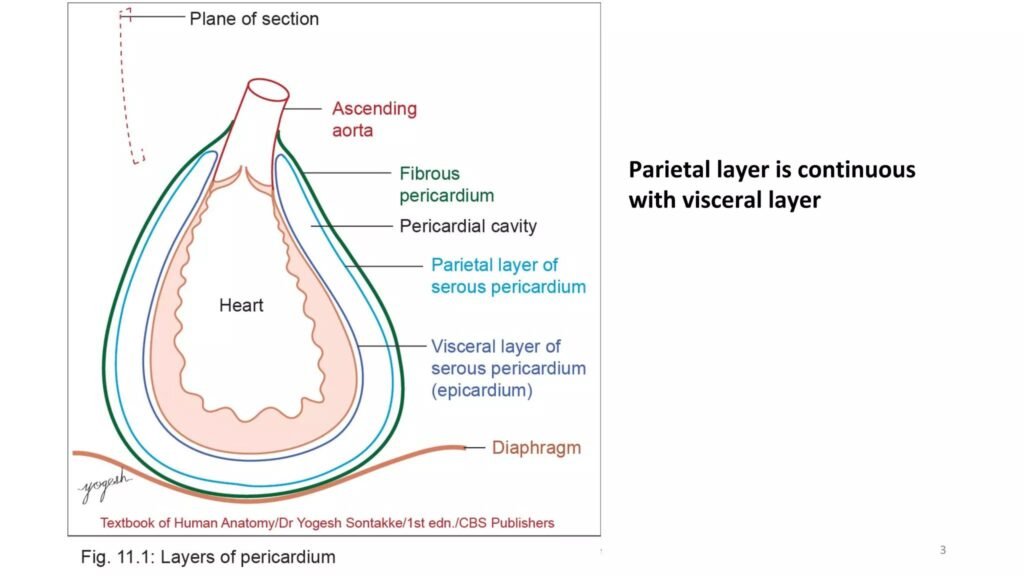
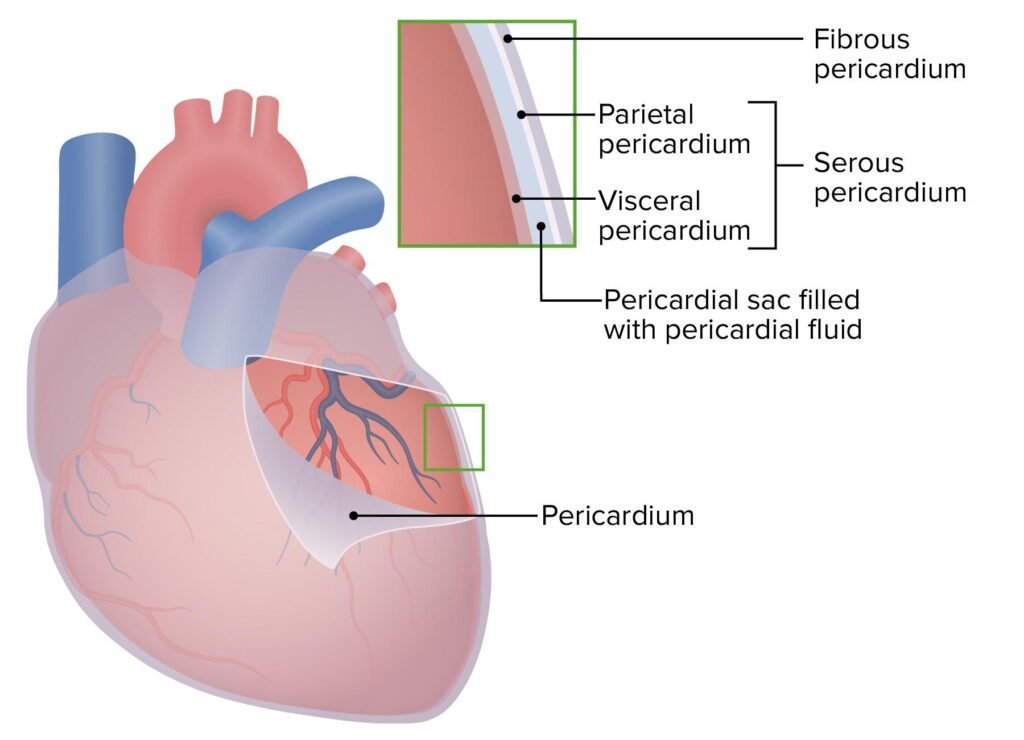
Pericardium
🧠 CORE
- Pericardium is fibroserous sac surrounding heart.
- Has two major parts:
- Fibrous pericardium
- Serous pericardium
- Serous pericardium has:
- Parietal layer
- Visceral layer (epicardium)
- Pericardial cavity contains lubricating fluid.
- Fibrous pericardium limits excessive cardiac dilation.
- Reflections form transverse and oblique sinuses.
🔬 CONCEPT EXPLAINED
The heart moves continuously within thoracic cavity. The pericardium stabilizes cardiac position and minimizes friction during movement.
Fibrous Pericardium
- Tough outer connective tissue layer.
- Attached inferiorly to diaphragm.
- Blends superiorly with great vessels.
Serous Pericardium
Parietal Layer
- Lines inner fibrous pericardium.
Visceral Layer (Epicardium)
- Closely adherent to heart surface.
Between these layers lies the pericardial cavity containing serous fluid reducing friction.
Pericardial Reflections and Sinuses
Reflection of serous pericardium around great vessels creates sinuses.
Transverse Pericardial Sinus
Located between:
- Aorta and pulmonary trunk anteriorly
- Superior vena cava posteriorly
Oblique Pericardial Sinus
Blind recess behind left atrium.
Entry and Exit of Great Vessels
Entering Vessels
- Superior vena cava
- Inferior vena cava
- Pulmonary veins
Exiting Vessels
- Aorta
- Pulmonary trunk
These vessels pass through reflections of pericardium.
⚠️ CLINICAL IMPORTANCE
- Pericarditis causes chest pain aggravated by movement.
- Pericardial effusion compresses heart.
- Cardiac tamponade severely restricts ventricular filling.
- Pericardiocentesis removes excess fluid.
- Surgeons use transverse sinus during cardiac surgery.
Physiology of Coronary Circulation
🧠 CORE
- Coronary blood flow depends mainly on diastolic pressure.
- Myocardium extracts large amount of oxygen at rest.
- Coronary flow increases during exercise.
- Local metabolic factors regulate coronary circulation.
- Adenosine is important vasodilator.
- Sympathetic stimulation indirectly increases coronary flow.
🔬 CONCEPT EXPLAINED
Cardiac muscle requires continuous ATP production through aerobic metabolism. Increased myocardial activity increases oxygen demand, producing vasodilator metabolites such as adenosine, carbon dioxide, hydrogen ions, and potassium.
These metabolites dilate coronary arterioles and increase blood supply according to metabolic needs.
During systole, ventricular contraction compresses coronary vessels, especially in left ventricle. Therefore, most left coronary perfusion occurs during diastole.
⚠️ CLINICAL IMPORTANCE
- Hypotension reduces coronary perfusion.
- Tachycardia shortens diastole and decreases coronary flow.
- Severe coronary narrowing produces ischemia during exertion.
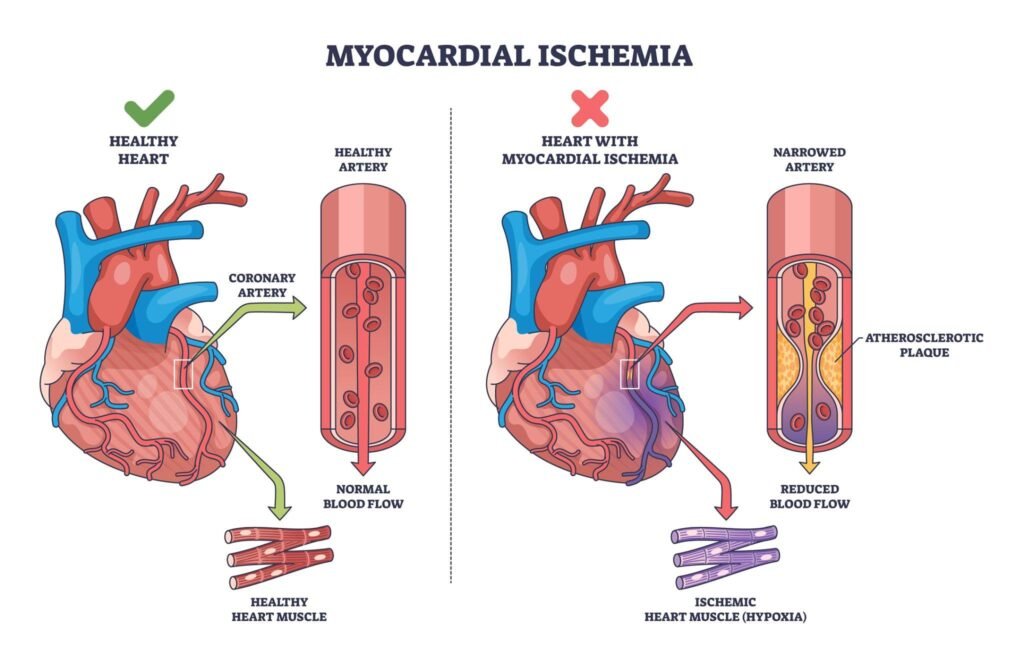
Coronary Thrombosis and Ischemic Heart Disease
🧠 CORE
- Coronary thrombosis is thrombus formation inside coronary artery.
- Usually occurs over ruptured atherosclerotic plaque.
- Leads to myocardial ischemia and infarction.
- Major risk factors include:
- Hypertension
- Diabetes mellitus
- Smoking
- Hyperlipidemia
- Obesity
🔬 CONCEPT EXPLAINED
Atherosclerosis damages vascular endothelium and forms lipid plaques inside coronary arteries. Plaque rupture exposes thrombogenic material causing platelet aggregation and clot formation.
The thrombus obstructs coronary blood flow leading to oxygen deprivation of myocardium.
If ischemia persists:
- Reversible injury → angina
- Irreversible injury → myocardial infarction
⚠️ CLINICAL IMPORTANCE
- Sudden coronary occlusion causes myocardial infarction.
- Infarction may produce arrhythmias or heart failure.
- Early reperfusion therapy reduces myocardial damage.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Coronary Arteries
- Narrow arterial branches → precise myocardial supply → effective oxygen delivery
Diastolic Coronary Flow
- Ventricular relaxation → vessel decompression → adequate myocardial perfusion
Fibrous Pericardium
- Tough outer layer → prevents excessive expansion → maintains cardiac stability
Serous Pericardium
- Smooth lubricated surfaces → friction reduction → efficient cardiac movement
Coronary Anastomosis
- Limited collateral circulation → poor compensation during sudden occlusion → myocardial infarction risk
🩺 5️⃣ Clinical Correlation
Angina Pectoris
- Temporary myocardial ischemia
- Causes chest pain during exertion
- Relieved by rest or nitrates
Myocardial Infarction
- Irreversible myocardial necrosis
- Usually due to coronary thrombosis
- Commonly affects left ventricle
Pericarditis
- Inflammation of pericardium
- Causes sharp chest pain
- Pericardial friction rub may be heard
Pericardial Effusion
- Fluid accumulation within pericardial cavity
- May compress heart chambers
Cardiac Tamponade
- Life-threatening emergency
- Rapid fluid accumulation restricts ventricular filling
- Causes hypotension and shock
📌 6️⃣ Summary Points
- Coronary arteries arise from ascending aorta above aortic valve.
- Left coronary artery mainly supplies left ventricle.
- LAD is most commonly occluded coronary artery.
- Coronary blood flow mainly occurs during diastole.
- Coronary arteries are functional end arteries.
- Coronary sinus drains most venous blood of heart.
- Fibrous pericardium prevents excessive cardiac dilation.
- Pericardial cavity normally contains lubricating fluid.
- Transverse sinus lies between arterial and venous ends of heart.
- Coronary thrombosis usually follows plaque rupture.
- Pericardial effusion may cause cardiac tamponade.
- Cardiac tamponade decreases ventricular filling and cardiac output.