
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The heart functions as a continuously active muscular pump that depends on precise electrical activity for effective contraction and blood circulation. Cardiac muscle cells generate specialized action potentials that differ significantly from skeletal muscle due to the presence of prolonged depolarization and unique calcium handling mechanisms. Excitation–contraction coupling links electrical stimulation with mechanical contraction, ensuring coordinated pumping of the atria and ventricles.
This topic is fundamental for understanding cardiac rhythm, heart sounds, cardiac output, and the physiological basis of arrhythmias. Abnormalities in cardiac electrophysiology may produce dangerous clinical conditions such as tachycardia, fibrillation, heart block, and heart failure. Understanding cardiac action potentials also explains the mechanisms of many cardiovascular drugs including calcium channel blockers and antiarrhythmic agents.
The topic integrates physiology, membrane biophysics, ion channel function, and clinically important electrophysiological disturbances.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Action potential: Rapid electrical change across the cell membrane caused by ion movement.
- Depolarization: Reduction of membrane negativity due to sodium or calcium influx.
- Repolarization: Restoration of resting membrane potential mainly due to potassium efflux.
- Excitation–contraction coupling: Process linking electrical excitation to muscle contraction.
- Chronotropic effect: Effect on heart rate.
- Inotropic effect: Effect on force of contraction.
- Dromotropic effect: Effect on conduction velocity.
- Refractory period: Time during which cardiac muscle cannot be re-excited normally.
- Plateau phase: Prolonged depolarized phase of cardiac action potential caused mainly by calcium influx.
- Slow calcium channels: Voltage-gated L-type calcium channels responsible for prolonged calcium entry.
Essential Terminology
- Fast-response action potential
- Slow-response action potential
- L-type calcium channels
- Sarcoplasmic reticulum
- Troponin complex
- Absolute refractory period
- Relative refractory period
- Effective refractory period
- Membrane excitability
- Automaticity
Basic Overview
- Cardiac muscle contracts after electrical stimulation.
- Action potentials initiate calcium entry into cardiac cells.
- Calcium triggers interaction between actin and myosin.
- Cardiac muscle has a prolonged refractory period preventing tetany.
- Pacemaker tissues generate spontaneous rhythmic activity.
- Electrical disturbances may lead to arrhythmias.
🔹 3️⃣ Core Learning — Curriculum Coverage
Cardiac Muscle and Excitation–Contraction Coupling
🧠 CORE
- Cardiac muscle is striated and involuntary.
- Cells are connected by intercalated discs and gap junctions.
- Depolarization spreads rapidly between cells.
- Calcium plays a central role in contraction.
- Cardiac contraction depends on extracellular calcium entry.
- Sarcoplasmic reticulum is less developed than in skeletal muscle.
- Contraction occurs through sliding filament mechanism.
- Cardiac muscle cannot undergo sustained tetanic contraction.
🔬 CONCEPT EXPLAINED
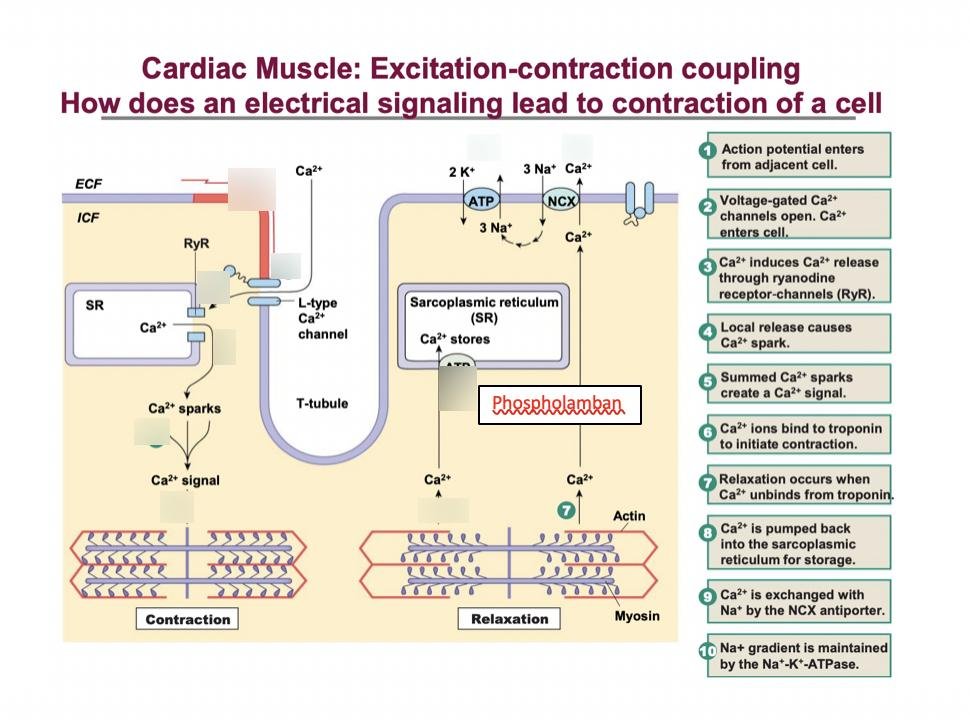
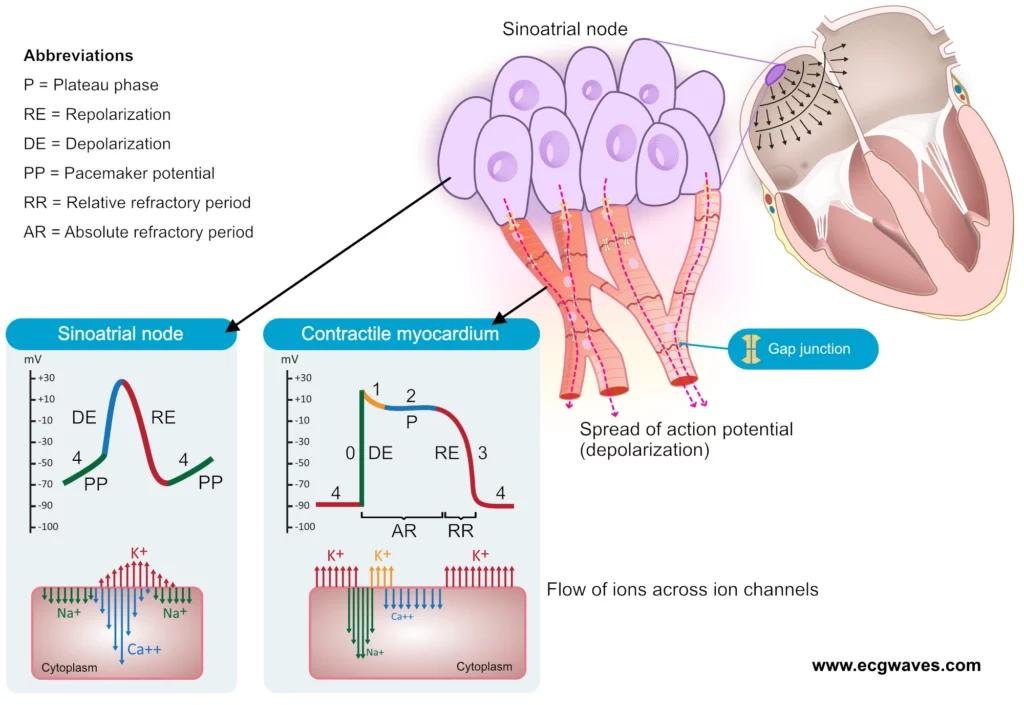
Cardiac muscle fibers are structurally similar to skeletal muscle because both contain actin, myosin, troponin, and tropomyosin arranged in sarcomeres. However, cardiac cells are shorter, branched, and interconnected by intercalated discs containing gap junctions. These gap junctions allow rapid spread of ions, enabling the myocardium to function as a functional syncytium.
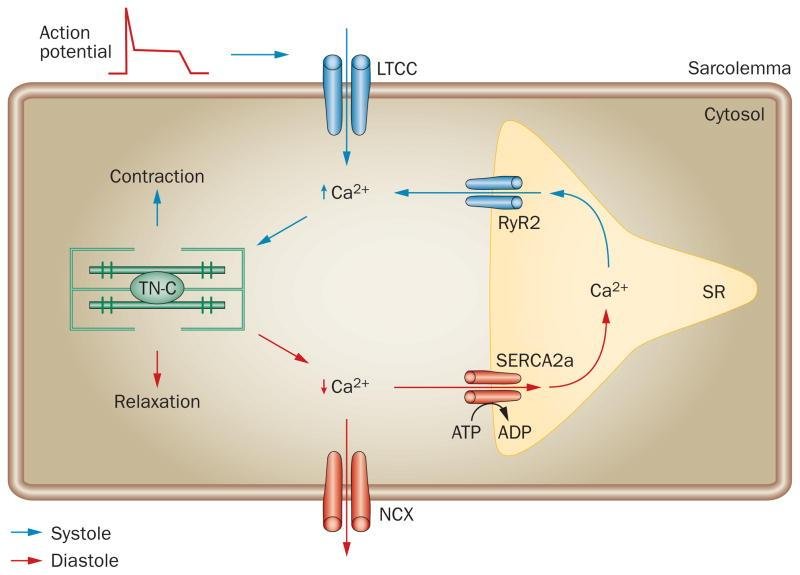
Excitation–contraction coupling begins when an action potential travels along the sarcolemma and T-tubules. Depolarization opens slow L-type calcium channels allowing extracellular calcium to enter the cell. This incoming calcium stimulates additional calcium release from the sarcoplasmic reticulum through calcium-induced calcium release.
The increased intracellular calcium binds to troponin C, causing displacement of tropomyosin and exposing active sites on actin. Myosin heads bind actin and produce contraction using ATP energy.
Relaxation occurs when calcium is removed from the cytoplasm by:
- SERCA pump into sarcoplasmic reticulum
- Sodium-calcium exchanger
- Calcium ATPase pumps
Cardiac muscle requires extracellular calcium for contraction, unlike skeletal muscle where intracellular calcium stores are usually sufficient.
⚠️ CLINICAL IMPORTANCE
- Reduced calcium entry decreases cardiac contractility and may cause heart failure.
- Excess intracellular calcium may contribute to arrhythmias.
- Calcium channel blockers reduce myocardial contraction and heart rate.
- Ischemia impairs ATP production causing defective calcium handling and weak contraction.
Phases of Cardiac Action Potential
🧠 CORE
- Ventricular muscle shows fast-response action potential.
- Five phases are recognized: 0–4.
- Sodium influx causes rapid depolarization.
- Calcium influx causes plateau phase.
- Potassium efflux causes repolarization.
- Plateau prolongs contraction duration.
- Resting membrane potential is about −90 mV.
- Plateau prevents tetanic contraction.
🔬 CONCEPT EXPLAINED
Cardiac ventricular muscle action potential differs from skeletal muscle because of its prolonged plateau phase.
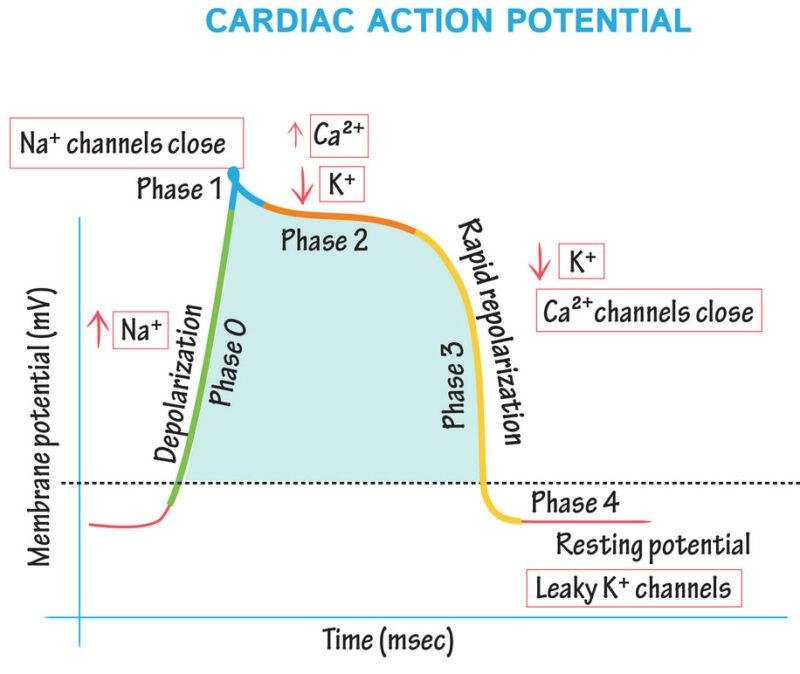
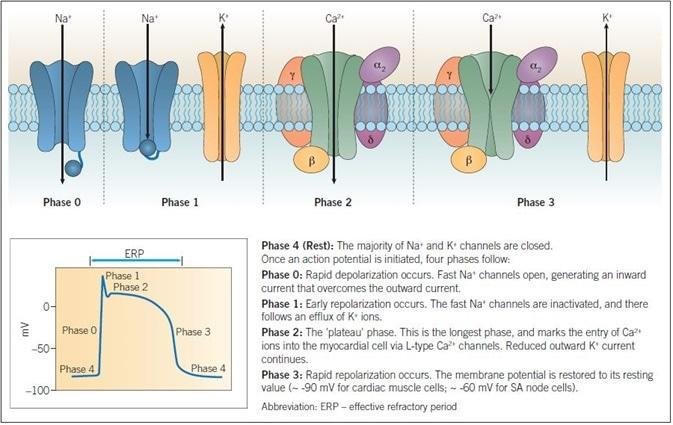
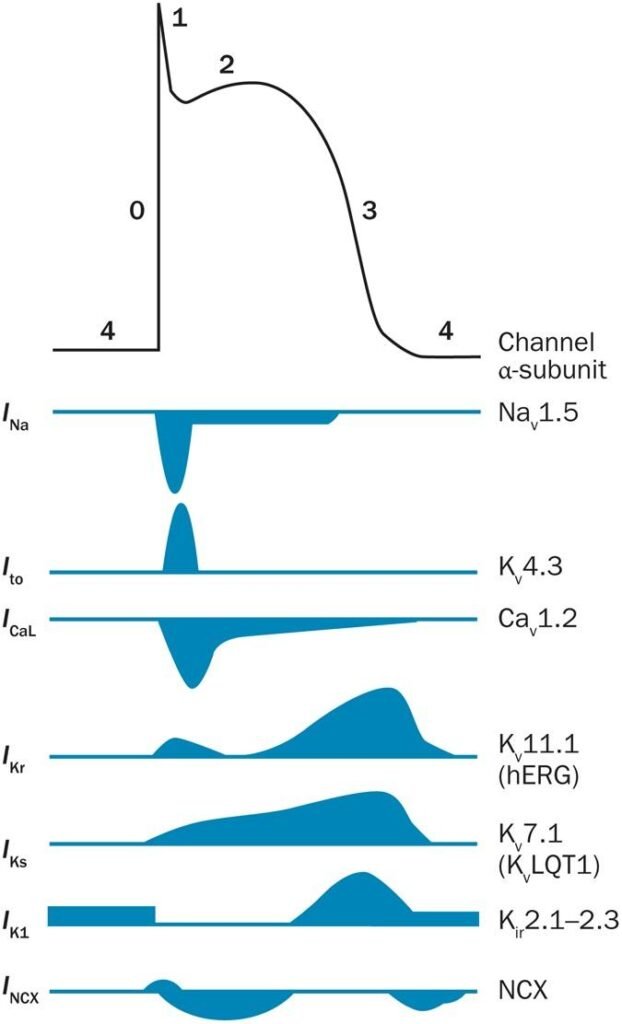
Phase 0 — Rapid Depolarization
Fast voltage-gated sodium channels open causing sudden sodium influx. Membrane potential rapidly becomes positive.
Phase 1 — Initial Repolarization
Transient potassium outward movement produces slight repolarization.
Phase 2 — Plateau Phase
Slow L-type calcium channels open allowing calcium influx while potassium exits simultaneously. Balance between calcium entry and potassium loss creates prolonged plateau.
Phase 3 — Rapid Repolarization
Calcium channels close while potassium efflux increases, restoring resting membrane potential.
Phase 4 — Resting Membrane Potential
High potassium permeability maintains stable resting potential.
The plateau phase is physiologically essential because it prolongs contraction and ensures sufficient ventricular emptying before relaxation.
⚠️ CLINICAL IMPORTANCE
- Disturbance of ion channels may produce arrhythmias.
- Prolonged QT interval predisposes to ventricular tachyarrhythmias.
- Hyperkalemia alters repolarization and may cause cardiac arrest.
- Sodium channel abnormalities may impair conduction velocity.
Slow Calcium Channels and Plateau Significance
🧠 CORE
- L-type calcium channels open slowly.
- Calcium influx prolongs depolarization.
- Plateau increases contraction duration.
- Prevents repeated rapid stimulation.
- Coordinates effective ventricular pumping.
- Important in SA and AV nodal conduction.
🔬 CONCEPT EXPLAINED
Slow calcium channels remain open much longer than fast sodium channels. Their prolonged opening allows continuous calcium influx into cardiac cells. Calcium entering through these channels both sustains membrane depolarization and triggers contraction.
The plateau phase ensures that contraction lasts long enough for complete ventricular ejection. Because depolarization remains prolonged, the myocardium stays refractory and cannot undergo repeated rapid contractions.
This mechanism prevents tetany, which would be fatal in the heart because relaxation is necessary for ventricular filling.
Pacemaker tissues such as SA and AV nodes rely heavily on calcium channels for depolarization because they contain fewer fast sodium channels.
⚠️ CLINICAL IMPORTANCE
- Calcium channel blockers reduce heart rate and conduction.
- Abnormal calcium channel activity contributes to arrhythmias.
- Reduced calcium influx weakens myocardial contraction.
- Nodal dysfunction may produce heart block.
Refractory Periods of Cardiac Muscle
🧠 CORE
- Cardiac muscle has prolonged refractory period.
- Absolute refractory period prevents re-excitation.
- Relative refractory period allows stronger stimulus response.
- Effective refractory period protects coordinated contraction.
- Refractory period is longer than skeletal muscle.
- Prevents tetanic contraction in heart.
🔬 CONCEPT EXPLAINED
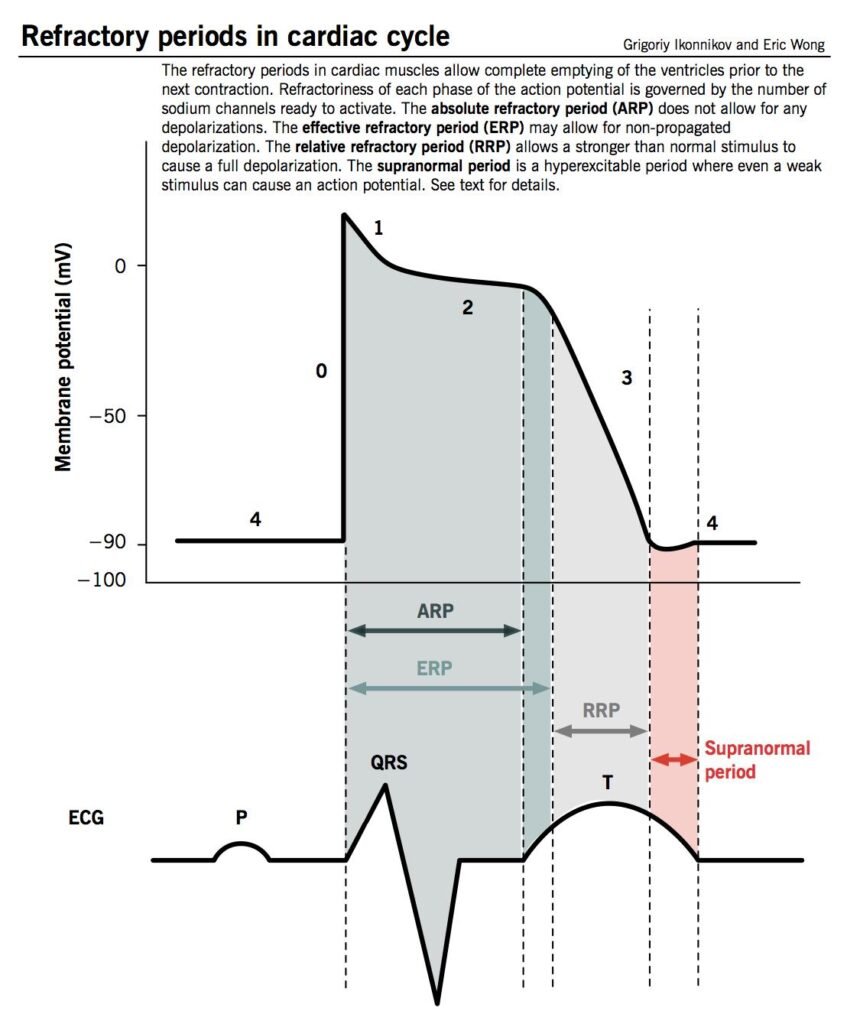
Absolute Refractory Period
During this phase no stimulus can produce another action potential because sodium channels remain inactivated.
Relative Refractory Period
A very strong stimulus may produce excitation because some sodium channels recover.
Effective Refractory Period
Period during which propagated action potentials cannot occur effectively.
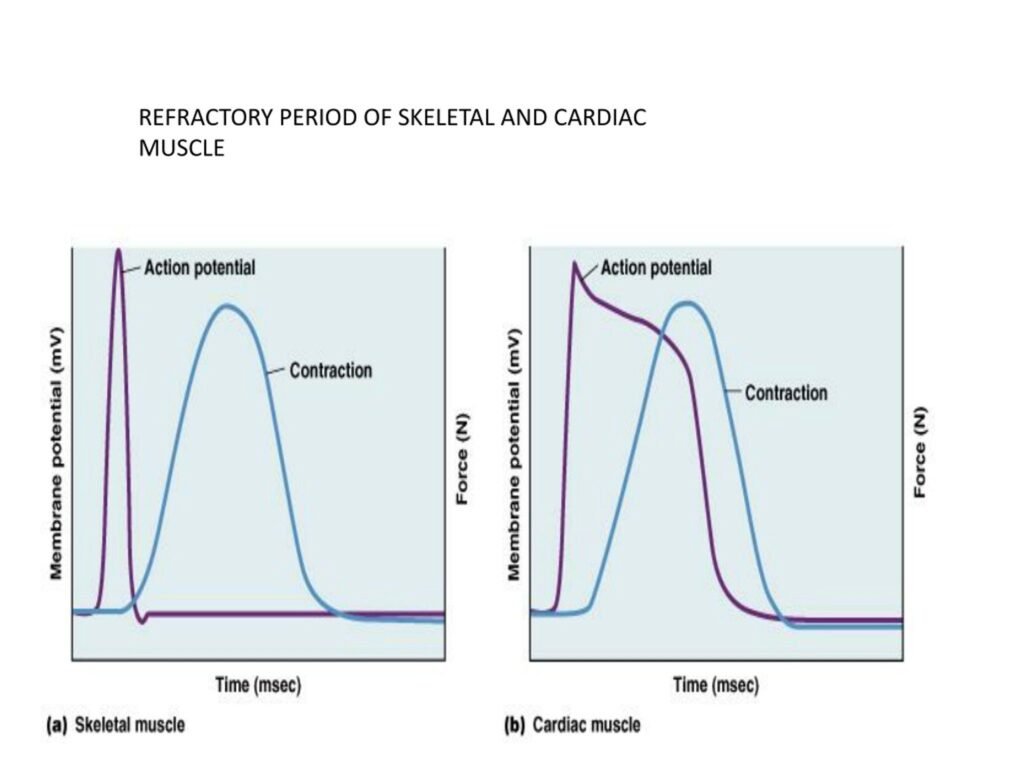
The cardiac refractory period almost equals the duration of contraction. Therefore, another contraction cannot begin before relaxation occurs.
In skeletal muscle, refractory periods are very short, allowing repeated summation and tetany. Such tetany is beneficial in skeletal muscle but incompatible with cardiac pumping.
⚠️ CLINICAL IMPORTANCE
- Shortened refractory periods predispose to re-entry arrhythmias.
- Antiarrhythmic drugs often prolong refractory periods.
- Ventricular fibrillation results from abnormal electrical re-excitation.
- Tetanic cardiac contraction would prevent effective circulation.
Chronotropic, Inotropic, and Dromotropic Effects
🧠 CORE
- Chronotropic effects alter heart rate.
- Inotropic effects alter force of contraction.
- Dromotropic effects alter conduction velocity.
- Sympathetic stimulation increases all three effects.
- Parasympathetic stimulation mainly decreases heart rate.
- Calcium strongly influences contractility.
🔬 CONCEPT EXPLAINED
Chronotropic Effects
These influence SA node firing rate. Sympathetic stimulation increases depolarization rate and heart rate through norepinephrine action. Parasympathetic stimulation through vagus nerve slows SA node activity.
Inotropic Effects
These affect force of myocardial contraction. Increased calcium availability enhances actin-myosin interaction producing stronger contractions.
Dromotropic Effects
These affect conduction velocity especially through AV node. Sympathetic stimulation increases conduction while parasympathetic activity slows AV nodal transmission.
These regulatory mechanisms allow rapid cardiovascular adaptation during exercise, stress, and rest.
⚠️ CLINICAL IMPORTANCE
- Positive chronotropic effects may cause tachycardia.
- Negative dromotropic drugs are used in supraventricular tachycardia.
- Reduced inotropic state contributes to heart failure.
- Excess sympathetic stimulation predisposes to arrhythmias.
Cardiac vs Skeletal Muscle Excitation–Contraction Coupling
🧠 CORE
- Both muscles use actin-myosin interaction.
- Cardiac muscle depends on extracellular calcium.
- Skeletal muscle mainly uses SR calcium stores.
- Cardiac refractory period is prolonged.
- Tetany occurs in skeletal but not cardiac muscle.
- Cardiac cells are electrically coupled by gap junctions.
🔬 CONCEPT EXPLAINED
Skeletal muscle excitation–contraction coupling occurs rapidly through direct mechanical linkage between T-tubules and sarcoplasmic reticulum. In cardiac muscle, calcium entry through membrane channels is essential for triggering calcium release from SR.
Cardiac muscle action potentials are much longer because of plateau formation. This prolonged depolarization produces long refractory periods preventing summation and tetany.
Functionally, skeletal muscle is designed for variable force generation and sustained contraction, whereas cardiac muscle is specialized for rhythmic pumping without fatigue.
⚠️ CLINICAL IMPORTANCE
- Hypocalcemia affects cardiac function more significantly than skeletal muscle.
- Tetanic cardiac contraction would stop circulation.
- Defective gap junction conduction contributes to arrhythmias.
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| Gap junctions | Electrical conduction between cells | Coordinated contraction |
| L-type calcium channels | Calcium entry during plateau | Sustained contraction |
| Sarcoplasmic reticulum | Calcium storage and release | Efficient contraction |
| Troponin complex | Controls actin-myosin interaction | Force generation |
| Long refractory period | Prevents repeated excitation | Rhythmic pumping |
| SA node | Pacemaker activity | Heart rhythm generation |
🩺 5️⃣ Clinical Correlation
Arrhythmias
Abnormal ion channel activity or disturbed conduction pathways may produce arrhythmias such as atrial fibrillation, ventricular tachycardia, or heart block.
Heart Failure
Defective calcium handling reduces myocardial contractility leading to reduced cardiac output and heart failure symptoms.
Hyperkalemia
Increased extracellular potassium reduces membrane excitability and may produce fatal conduction disturbances.
Calcium Channel Blockers
These drugs inhibit L-type calcium channels causing:
- Reduced heart rate
- Reduced AV conduction
- Reduced myocardial contractility
Used in hypertension and arrhythmias.
Long QT Syndrome
Prolonged ventricular repolarization increases risk of ventricular arrhythmias and sudden cardiac death.
📌 6️⃣ Summary Points
- Cardiac muscle action potential contains a prolonged plateau phase.
- Plateau phase is mainly due to slow calcium channel opening.
- Cardiac contraction depends on extracellular calcium entry.
- Calcium-induced calcium release is central in cardiac muscle.
- Long refractory period prevents tetanic contraction.
- Cardiac muscle acts as a functional syncytium through gap junctions.
- Chronotropic effects alter heart rate.
- Inotropic effects alter force of contraction.
- Dromotropic effects alter conduction velocity.
- Skeletal muscle can undergo tetany but cardiac muscle cannot.
- Antiarrhythmic drugs often modify ion channel activity.
- Disturbed electrophysiology may cause life-threatening arrhythmias.