
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Electrocardiography (ECG) is the graphical recording of the electrical activity of the heart. It is one of the most important non-invasive investigations used in medicine for assessing heart function and diagnosing cardiovascular diseases. The electrical impulses generated within the heart spread through the atria and ventricles in an organized manner, producing characteristic ECG waves and intervals.
Understanding ECG helps students correlate cardiac conduction with mechanical contraction of the heart. It also provides the basis for recognizing arrhythmias, myocardial infarction, conduction defects, and electrolyte disturbances. In community medicine, cardiovascular diseases are among the leading causes of morbidity and mortality worldwide. Knowledge of cardiovascular risk factors and prevention strategies is essential for reducing disease burden in the community.
This topic integrates physiology with preventive medicine by linking cardiac electrical activity with cardiovascular health promotion and disease prevention.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Electrocardiogram (ECG): Graphic recording of electrical activity of the heart.
- Depolarization: Electrical activation of cardiac muscle cells.
- Repolarization: Recovery phase of cardiac muscle after depolarization.
- Lead: Electrical viewpoint used to record cardiac activity.
- Cardiovascular disease (CVD): Diseases involving the heart and blood vessels.
- Risk factor: Any factor increasing the likelihood of disease development.
- Modifiable risk factor: Risk factor that can be changed or controlled.
- Non-modifiable risk factor: Risk factor that cannot be altered.
Essential Terminology
- P wave
- QRS complex
- T wave
- PR interval
- ST segment
- QT interval
- Limb leads
- Chest leads
- Calibration
- Heart rate
- Conduction system
- Hypertension
- Atherosclerosis
Basic Overview
- ECG records electrical activity, not mechanical contraction.
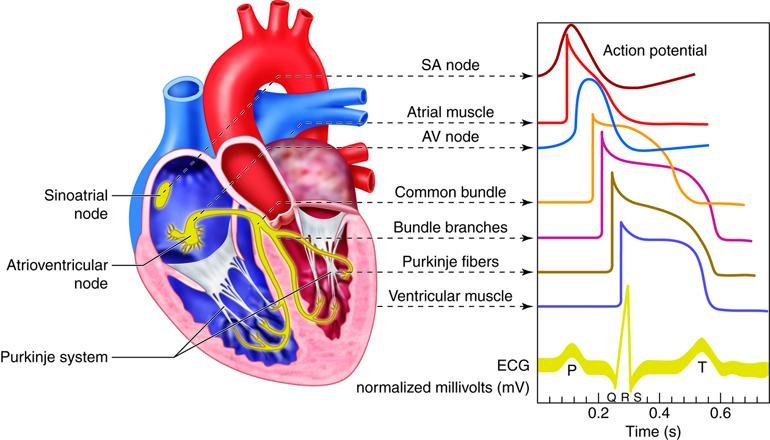
- SA node initiates cardiac impulse.
- Impulse travels through AV node → Bundle of His → Purkinje fibers.
- ECG paper contains standardized squares for time and voltage measurement.
- Cardiovascular diseases are strongly associated with lifestyle and metabolic risk factors.
- Prevention strategies aim to reduce morbidity and mortality.
🔹 3️⃣ Core Learning — Curriculum Coverage
ELECTRICAL ACTIVITY OF THE HEART AND BASIS OF ECG
🧠 CORE
- Heart functions as an electrical syncytium.
- SA node acts as the natural pacemaker.
- Electrical impulse spreads through atria then ventricles.
- ECG reflects sequential depolarization and repolarization.
- Surface electrodes detect electrical potentials.
- ECG does not directly measure contraction strength.
- Conduction pathway maintains coordinated pumping.
- Different cardiac regions depolarize at different times.
🔬 CONCEPT EXPLAINED
The heart possesses an intrinsic conduction system that generates and conducts electrical impulses automatically. The sinoatrial (SA) node located in the right atrium initiates the impulse because it has the highest rate of spontaneous depolarization.
The impulse spreads across both atria causing atrial depolarization and contraction. It then reaches the atrioventricular (AV) node, where conduction slows briefly. This delay allows adequate ventricular filling before ventricular contraction.
After passing through the AV node, impulses travel rapidly through the Bundle of His, bundle branches, and Purkinje fibers to activate ventricular myocardium. This coordinated spread produces efficient ventricular contraction.
Electrodes placed on the body surface detect these electrical changes and convert them into ECG tracings.
⚠️ CLINICAL IMPORTANCE
- SA node dysfunction may cause arrhythmias.
- AV nodal block delays ventricular activation.
- Ventricular conduction defects widen QRS complex.
- Myocardial ischemia alters ECG patterns.
- ECG is essential in emergency cardiac diagnosis.
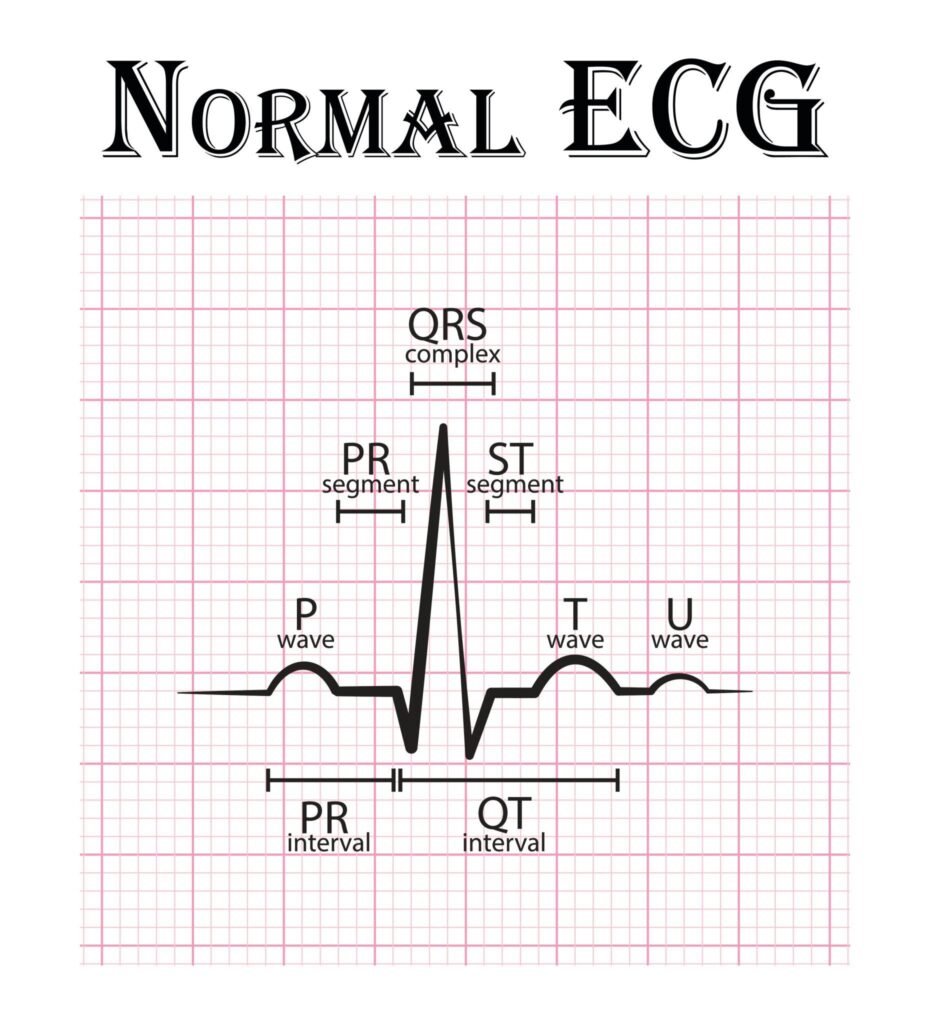
NORMAL ECG WAVES, SEGMENTS, INTERVALS AND VOLTAGES
🧠 CORE
- ECG consists of waves, segments, and intervals.
- P wave represents atrial depolarization.
- QRS complex represents ventricular depolarization.
- T wave represents ventricular repolarization.
- PR interval reflects AV conduction time.
- ST segment represents ventricular plateau phase.
- QT interval reflects total ventricular electrical activity.
- Standard voltages and durations are clinically important.
🔬 CONCEPT EXPLAINED
P Wave
The P wave occurs when atrial muscle depolarizes. It is normally small and rounded because atrial muscle mass is limited.
Normal duration:
- Less than 0.12 second
Normal voltage:
- Less than 2.5 mm
QRS Complex
The QRS complex reflects rapid ventricular depolarization. Ventricles contain large muscle mass; therefore, the complex is tall and sharp.
Normal duration:
- 0.06–0.10 second
Components:
- Q wave = initial negative deflection
- R wave = positive deflection
- S wave = negative deflection after R wave
T Wave
The T wave represents ventricular repolarization. It is broader because repolarization occurs more slowly than depolarization.
PR Interval
Represents conduction from atria through AV node to ventricles.
Normal duration:
- 0.12–0.20 second
ST Segment
Represents period between ventricular depolarization and repolarization.
Normally:
- Isoelectric (flat)
QT Interval
Represents total duration of ventricular depolarization and repolarization.
Depends on:
- Heart rate
⚠️ CLINICAL IMPORTANCE
- Prolonged PR interval indicates AV block.
- ST elevation suggests myocardial infarction.
- Tall peaked T waves may occur in hyperkalemia.
- Prolonged QT interval predisposes to arrhythmias.
- Abnormal Q waves may indicate previous infarction.
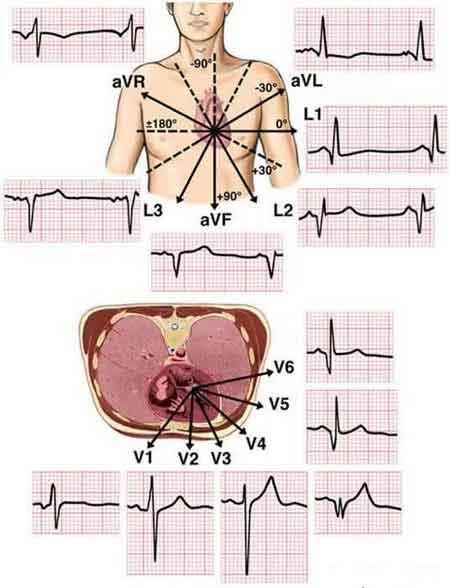
ECG LEADS, RECORDING AND CALIBRATION
🧠 CORE
- ECG requires proper lead placement.
- Limb leads record frontal plane activity.
- Chest leads record horizontal plane activity.
- Standard ECG uses 12 leads.
- Calibration ensures accurate interpretation.
- ECG paper speed affects time calculations.
- Voltage measurements depend on standardization.
🔬 CONCEPT EXPLAINED
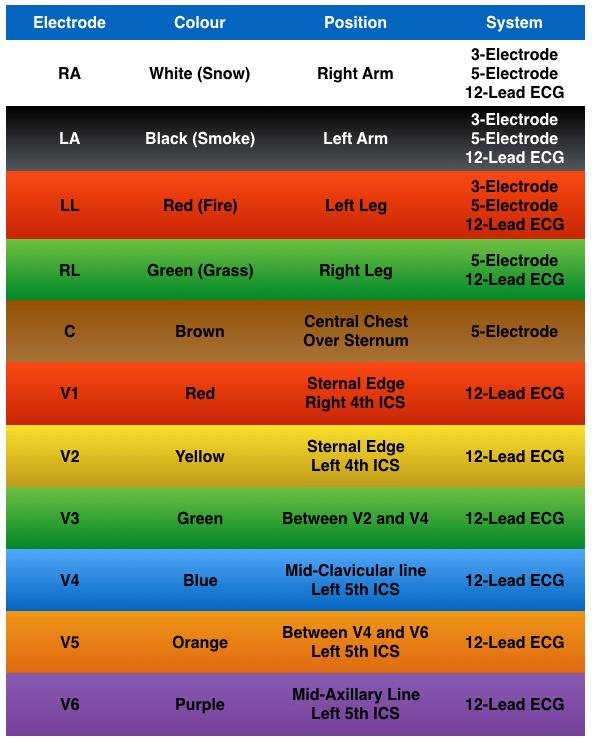
Limb Leads
Bipolar Leads
- Lead I
- Lead II
- Lead III
These compare electrical potentials between limbs.
Augmented Leads
- aVR
- aVL
- aVF
Provide additional frontal plane views.
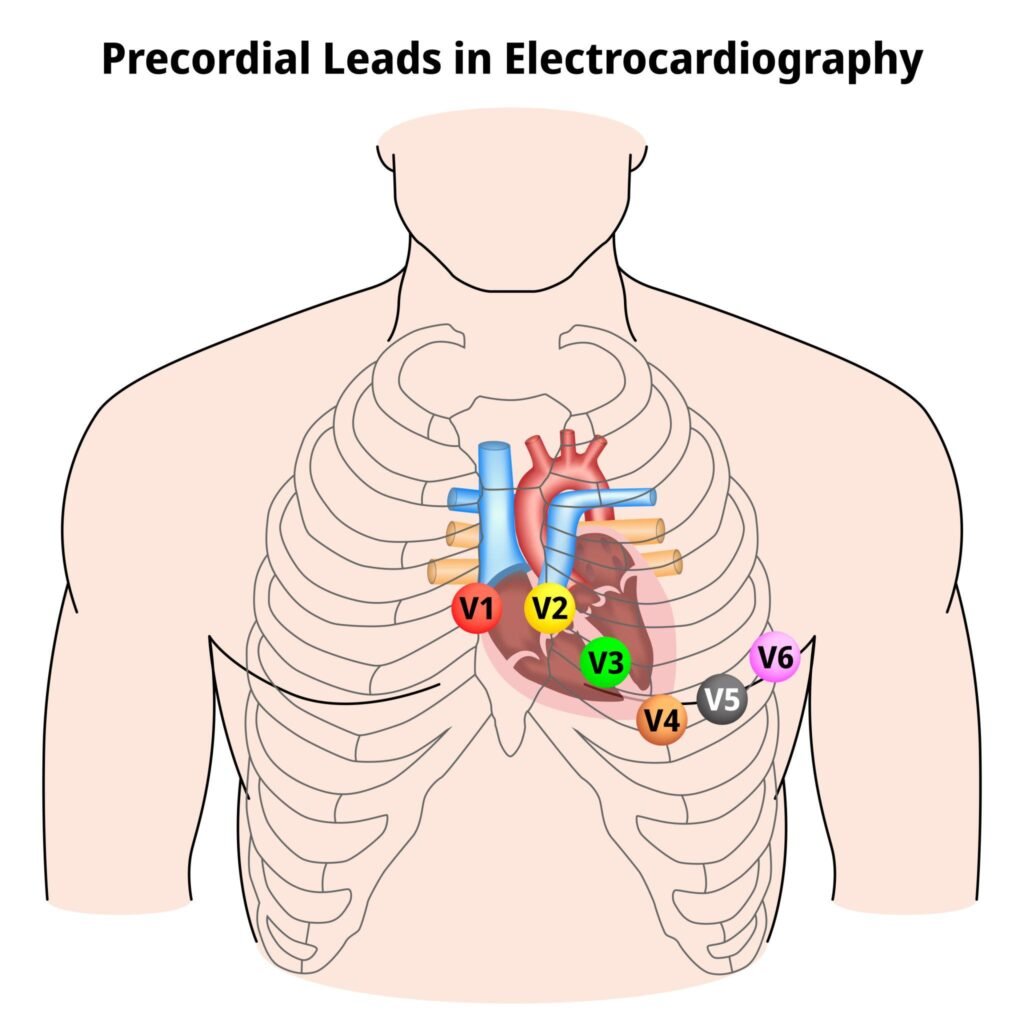
Chest Leads
- V1–V6
Placed on chest wall to assess ventricular activity in horizontal plane.
ECG Recording
To record ECG:
- Patient lies relaxed.
- Electrodes are attached to limbs and chest.
- Electrical signals are amplified.
- ECG machine records waves on graph paper.
ECG Paper and Calibration
Standard ECG paper:
- Speed = 25 mm/sec
- 1 small square = 0.04 sec
- 1 large square = 0.20 sec
Voltage calibration:
- 10 mm = 1 mV
This standardization allows comparison between recordings.
⚠️ CLINICAL IMPORTANCE
- Incorrect lead placement causes false interpretation.
- Calibration errors alter wave measurements.
- Chest leads help localize myocardial infarction.
- ECG monitoring is vital in ICU and emergency care.
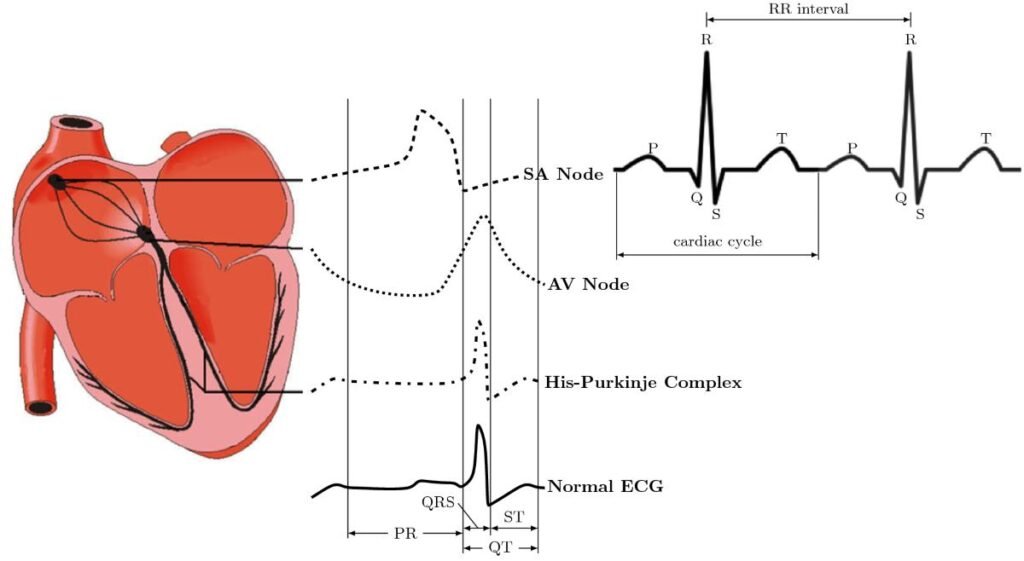
AV NODAL AND VENTRICULAR CONDUCTION IN ECG FORMATION
🧠 CORE
- AV node slows conduction.
- Delay permits ventricular filling.
- Ventricular conduction is rapid.
- Purkinje fibers distribute impulses efficiently.
- Conduction timing determines ECG pattern.
- Coordinated conduction maintains cardiac output.
🔬 CONCEPT EXPLAINED
The AV node has slow conduction velocity due to fewer gap junctions and smaller fibers. This physiological delay produces the PR interval and allows atria to complete contraction before ventricles begin systole.
The His-Purkinje system conducts impulses rapidly, producing synchronized ventricular depolarization. Rapid conduction generates the narrow QRS complex seen in normal ECG.
If conduction slows abnormally, ECG intervals become prolonged.
⚠️ CLINICAL IMPORTANCE
- AV block prolongs PR interval.
- Bundle branch block widens QRS complex.
- Ventricular arrhythmias may impair cardiac output.
- Conduction abnormalities may lead to syncope.
CARDIOVASCULAR RISK FACTORS
🧠 CORE
- Cardiovascular diseases are multifactorial.
- Risk factors increase disease probability.
- Some risk factors are modifiable.
- Others are non-modifiable.
- Lifestyle strongly affects cardiovascular health.
- Prevention reduces disease burden.
- Hypertension and smoking are major contributors.
🔬 CONCEPT EXPLAINED
Cardiovascular diseases such as ischemic heart disease and stroke develop due to interaction between genetic predisposition and environmental influences. Risk factors damage blood vessels, accelerate atherosclerosis, increase cardiac workload, and impair circulation.
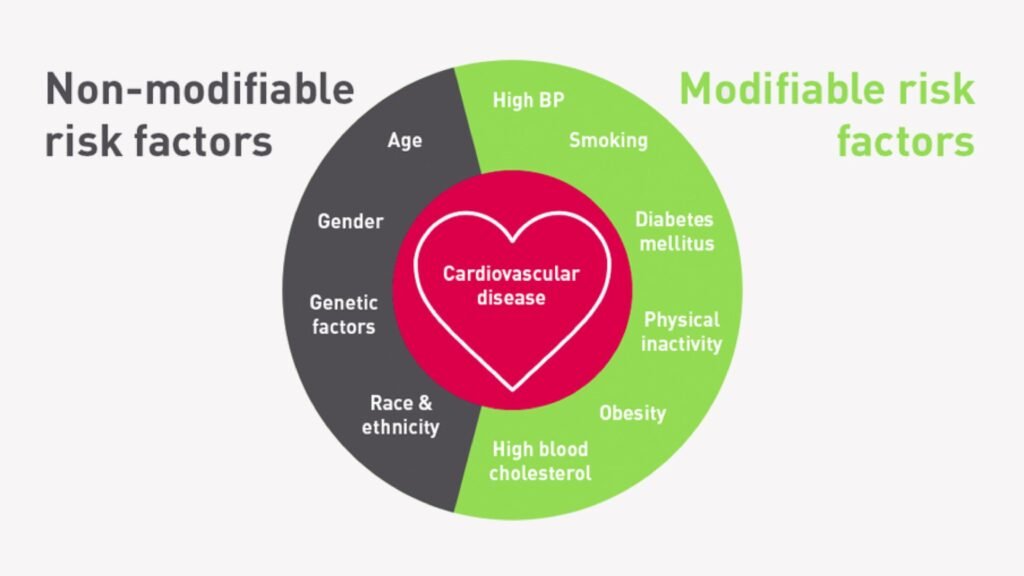
Non-Modifiable Risk Factors
- Age
- Male gender
- Family history
- Genetic predisposition
These factors cannot be changed but help identify high-risk individuals.
Modifiable Risk Factors
- Hypertension
- Smoking
- Diabetes mellitus
- Obesity
- Sedentary lifestyle
- High-fat diet
- Hyperlipidemia
- Stress
- Alcohol abuse
These can be prevented or controlled through lifestyle changes and medical interventions.
⚠️ CLINICAL IMPORTANCE
- Smoking accelerates atherosclerosis.
- Hypertension damages arteries and heart.
- Diabetes increases risk of coronary artery disease.
- Obesity contributes to metabolic syndrome.
- Multiple risk factors greatly increase cardiovascular mortality.
PREVENTION OF CARDIOVASCULAR DISEASES
🧠 CORE
- Prevention reduces disease occurrence and complications.
- Prevention exists at four levels.
- Community education is essential.
- Early diagnosis improves prognosis.
- Lifestyle modification is highly effective.
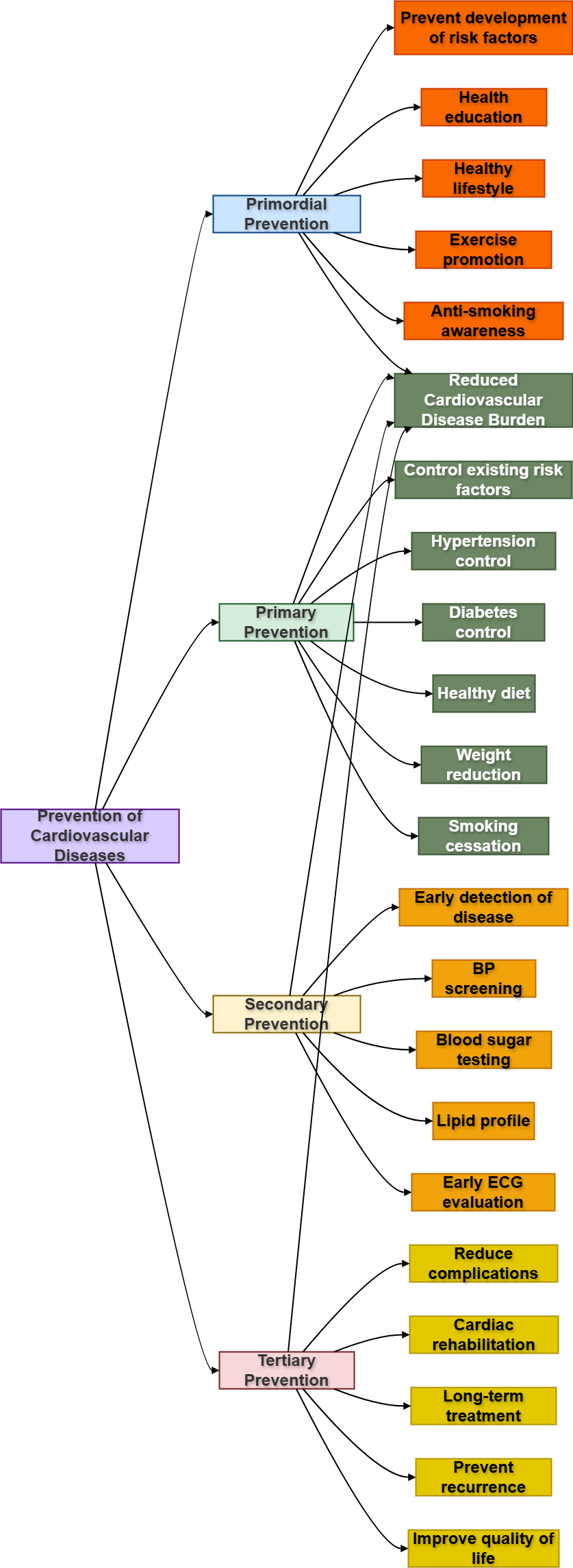
🔬 CONCEPT EXPLAINED
Primordial Prevention
Prevents development of risk factors themselves.
Examples:
- Healthy childhood lifestyle
- Public health education
- Promotion of exercise
Primary Prevention
Controls existing risk factors before disease develops.
Examples:
- Smoking cessation
- Blood pressure control
- Healthy diet
Secondary Prevention
Early detection and treatment of disease.
Examples:
- Screening programs
- Early ECG monitoring
- Diabetes control
Tertiary Prevention
Reduces complications and disability after disease develops.
Examples:
- Cardiac rehabilitation
- Long-term medications
- Lifestyle counseling after myocardial infarction
⚠️ CLINICAL IMPORTANCE
- Prevention lowers healthcare burden.
- Community interventions reduce mortality.
- Early management improves survival rates.
- Rehabilitation improves quality of life.
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| SA node | Initiates impulse | Controls heart rhythm |
| AV node | Delays conduction | Allows ventricular filling |
| Purkinje fibers | Rapid impulse conduction | Coordinated ventricular contraction |
| ECG leads | Detect electrical activity | Diagnostic cardiac recording |
| Coronary arteries | Supply myocardium | Maintain cardiac function |
| Healthy lifestyle | Reduces risk factors | Prevents cardiovascular disease |
🩺 5️⃣ Clinical Correlation
Myocardial Infarction
- ST elevation may indicate acute infarction.
- Coronary artery blockage causes myocardial ischemia.
Heart Block
- Delayed AV conduction prolongs PR interval.
- Severe block may reduce cardiac output.
Hypertension
- Major modifiable cardiovascular risk factor.
- Causes vascular and cardiac damage over time.
Arrhythmias
- Abnormal impulse generation or conduction.
- ECG helps identify rhythm disturbances.
Atherosclerosis
- Plaque formation narrows arteries.
- Leads to ischemic heart disease and stroke.
📌 6️⃣ Summary Points
- ECG records electrical activity, not contraction force.
- P wave represents atrial depolarization.
- QRS complex represents ventricular depolarization.
- T wave represents ventricular repolarization.
- Normal PR interval = 0.12–0.20 sec.
- Standard ECG paper speed = 25 mm/sec.
- 10 mm equals 1 mV calibration.
- AV nodal delay allows ventricular filling.
- Smoking and hypertension are major modifiable risk factors.
- Age and family history are non-modifiable risk factors.
- Prevention of cardiovascular disease occurs at four levels.
- ECG is essential for diagnosing arrhythmias and myocardial infarction.