
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
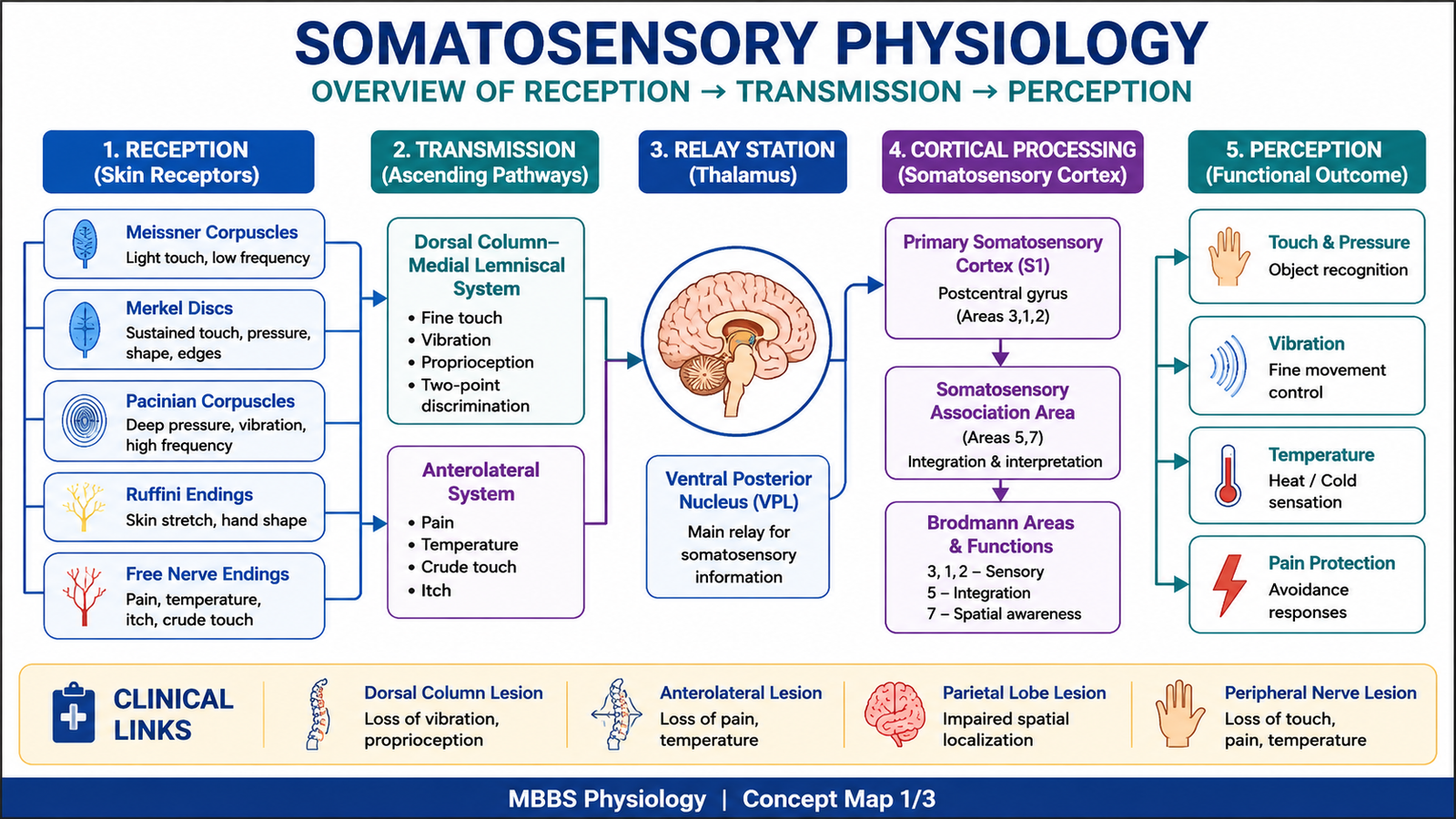
Somatic sensation allows the body to detect touch, pressure, vibration, pain, temperature, and body position. These sensations arise mainly from receptors in the skin, muscles, joints, and connective tissues and are carried to the spinal cord, brainstem, thalamus, and cerebral cortex.
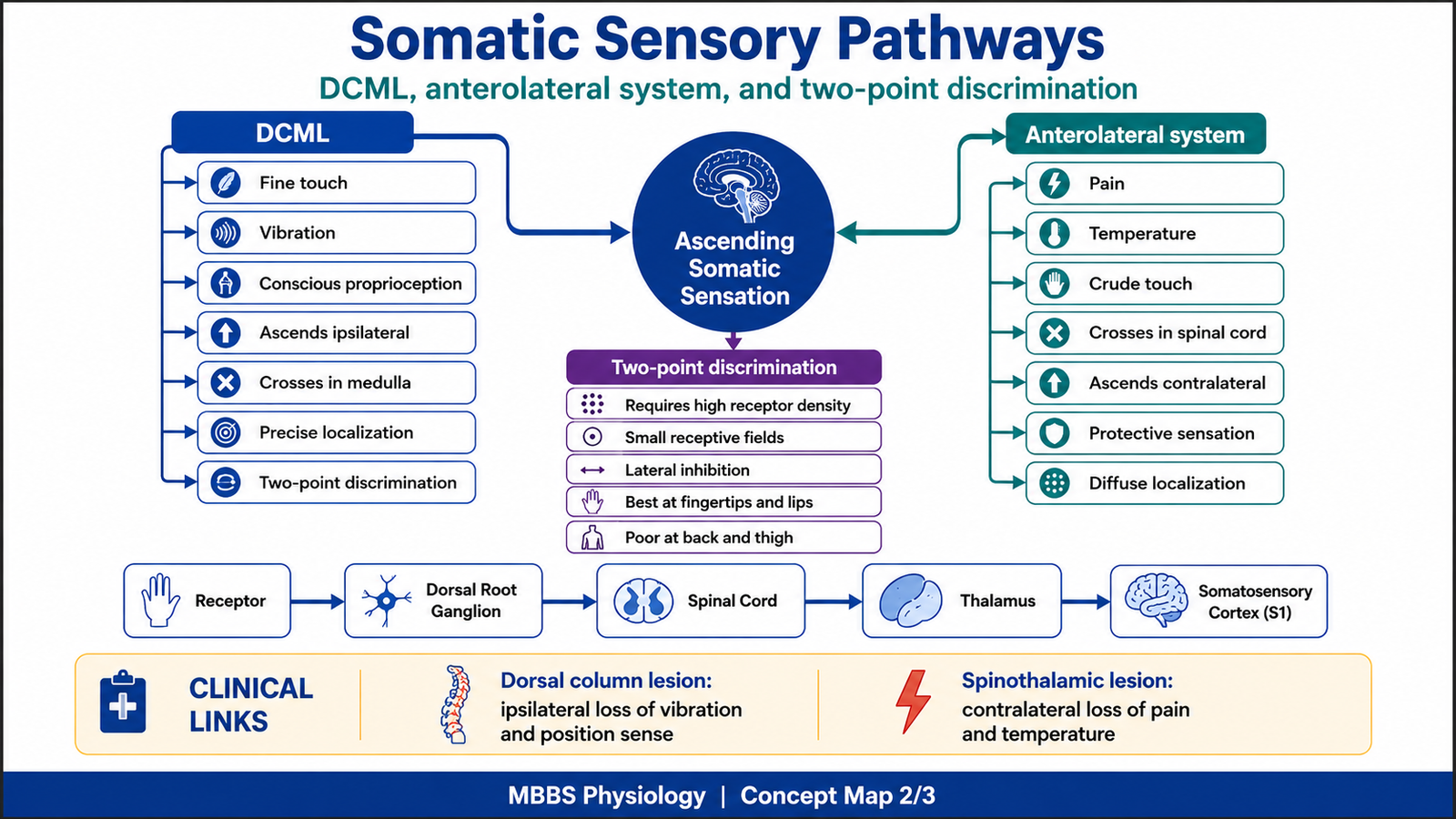
This topic is important because sensory pathways explain how the body recognizes what type of stimulus is present, where it is located, how strong it is, and whether it is harmful. The dorsal column–medial lemniscal pathway mainly carries fine touch, vibration, and conscious proprioception, while the anterolateral system mainly carries pain, temperature, crude touch, pressure, itch, and tickle.
Clinically, damage to these pathways produces characteristic sensory losses. For example, dorsal column lesions impair vibration and position sense, while spinothalamic tract lesions affect pain and temperature. Understanding these pathways is essential for neurological examination, localization of spinal cord lesions, and interpretation of sensory deficits.
🔹 2️⃣ Foundation Concepts
Key definitions
- Somatic sensation: Sensory information from skin, muscles, joints, and body wall.
- Modality: Type of sensation, such as touch, pain, temperature, vibration, or proprioception.
- Receptor: Specialized sensory ending that converts stimulus energy into electrical signals.
- Transduction: Conversion of physical or chemical stimulus into receptor potential.
- Receptor potential: A graded electrical change in the receptor ending.
- Action potential: Electrical impulse generated when threshold is reached.
- Ascending pathway: A sensory pathway that carries information from the body toward the brain.
- First-order neuron: Sensory neuron whose cell body lies in the dorsal root ganglion.
- Second-order neuron: Neuron that receives input from first-order neuron and crosses to the opposite side in most pathways.
- Third-order neuron: Thalamic neuron that projects to the sensory cortex.
- Somatotopy: Ordered representation of body parts in a pathway or cortex.
- Discriminative touch: Fine touch that allows localization, texture recognition, and two-point discrimination.
- Nondiscriminative touch: Crude touch that indicates contact but gives poor localization.
- Nociception: Detection of potentially damaging stimuli causing pain.
- Somatosensory cortex: Cortical area in the parietal lobe responsible for conscious perception of body sensations.
Basic overview
- Sensory receptors detect different forms of energy.
- Receptors generate local receptor potentials.
- If threshold is reached, action potentials travel along sensory nerve fibers.
- Sensory information enters the spinal cord through dorsal roots.
- Different modalities ascend through different spinal cord pathways.
- The thalamus acts as the major relay station.
- The cerebral cortex interprets the sensation consciously.
- Sensory pathways are organized so that body location and modality are preserved.
🔹 3️⃣ Core Learning — Curriculum Coverage
A. Tactile Receptors of Skin and Their Functional Specialization
🧠 CORE
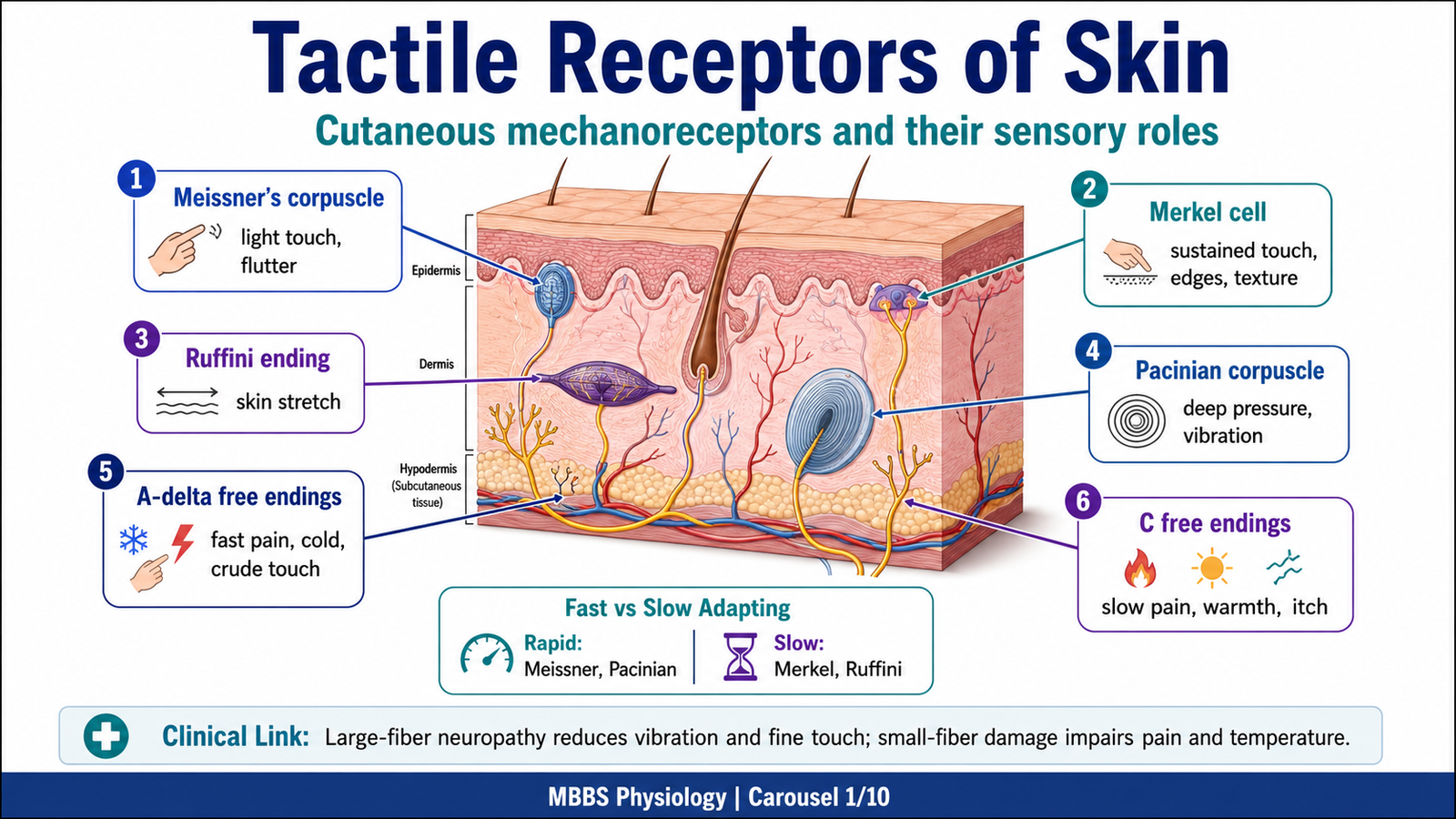
- Tactile receptors convert mechanical stimuli into nerve impulses.
- They differ in structure, depth, adaptation rate, and function.
- Meissner’s corpuscles detect light touch and low-frequency vibration.
- Pacinian corpuscles detect deep pressure and high-frequency vibration.
- Merkel cells detect sustained touch, pressure, texture, and edges.
- Ruffini endings detect skin stretch and sustained pressure.
- A-delta and C free nerve endings carry pain, temperature, crude touch, itch, and tickle.
- Different receptors allow the skin to analyze both simple contact and complex object features.
🔬 CONCEPT EXPLAINED
To understand somatic sensation, the first step is to understand how the skin detects stimuli. The skin is not simply a passive covering. It contains specialized sensory receptors that act as biological transducers. When a mechanical force such as touch, pressure, vibration, or stretch is applied to the skin, the receptor ending is deformed. This deformation changes ion permeability in the sensory nerve ending, producing a receptor potential. If the receptor potential reaches threshold, action potentials are generated and transmitted to the central nervous system.
The body needs different tactile receptors because no single receptor can detect all qualities of touch accurately. Some receptors are superficial and rapidly adapting, making them useful for detecting changing stimuli such as movement across the skin. Others are deeper and slowly adapting, making them useful for sustained pressure or stretch.
Meissner’s corpuscles are located mainly in glabrous skin such as fingertips and lips. They are superficial and rapidly adapting. Their main function is to detect light touch and movement of objects over the skin. Because they respond strongly when a stimulus begins or changes, they are important for grip control and fine tactile discrimination.
Pacinian corpuscles are deep receptors found in dermis, subcutaneous tissue, ligaments, joint capsules, and deeper connective tissues. They are rapidly adapting and highly sensitive to vibration, especially high-frequency vibration. Their capsule filters slow pressure but transmits rapid changes. Therefore, the stimulus does not merely activate the nerve ending directly; the capsule modifies the mechanical force before receptor activation. This arrangement allows Pacinian corpuscles to respond best to rapid deformation and vibration.
Merkel cells are slowly adapting superficial receptors. They detect sustained touch, pressure, texture, shape, and edges. Because their response continues during a maintained stimulus, they help the brain identify object form and surface details.
Ruffini endings are slowly adapting receptors located deeper in skin. They respond to skin stretch and sustained pressure. They contribute to perception of hand shape and finger position during object manipulation.
Free nerve endings are less structurally specialized but functionally very important. A-delta fibers are thinly myelinated and conduct relatively fast pain, cold, and crude touch. C fibers are unmyelinated and conduct slow pain, warmth, itch, and diffuse poorly localized sensations.
The functional advantage of multiple receptor types is that the nervous system can analyze the quality, intensity, duration, location, and movement of a stimulus. If these receptors or their pathways are impaired, the patient may lose fine touch, protective pain sensation, vibration sense, or the ability to recognize objects by touch.
⚠️ CLINICAL IMPORTANCE
Loss of tactile receptors or their nerve fibers causes sensory deficits. In peripheral neuropathy, patients may lose vibration, pain, temperature, and fine touch depending on which fibers are affected. Loss of protective pain sensation increases risk of unnoticed injury, ulcers, and burns. Damage to large myelinated fibers especially affects vibration sense, proprioception, and fine tactile discrimination.
B. Receptor Transduction and Sensory Coding
🧠 CORE
- Sensory transduction converts stimulus energy into electrical signals.
- Mechanical deformation opens mechanically gated ion channels.
- Receptor potential is graded, not all-or-none.
- Stronger stimulus produces larger receptor potential.
- If threshold is reached, action potentials occur.
- Stimulus intensity is coded by frequency of impulses and recruitment of receptors.
- Stimulus location is coded by labeled lines and receptive fields.
- Adaptation helps the nervous system detect changes in the environment.
🔬 CONCEPT EXPLAINED
Every sensory pathway begins with transduction. The initiating event is a stimulus such as touch, pressure, vibration, temperature change, or tissue injury. The purpose of transduction is to convert environmental or body information into a language that neurons can carry: electrical impulses.
In tactile receptors, mechanical force deforms the receptor membrane. This deformation opens mechanically gated ion channels, allowing positive ions, mainly sodium, to enter the nerve ending. As a result, the membrane becomes less negative, producing a receptor potential. If the receptor potential is large enough, it reaches threshold at the first node or trigger zone of the sensory fiber, generating action potentials.
The cause → effect relationship is important. A weak stimulus causes slight receptor deformation, small receptor potential, and low action potential frequency. A stronger stimulus causes greater deformation, larger receptor potential, and higher impulse frequency. If the stimulus is very strong, more receptors are recruited, so more sensory fibers transmit impulses to the CNS.
The body also needs to identify the type and location of sensation. The labeled line principle explains this. Each sensory pathway carries a specific type of information. For example, impulses from a vibration receptor are interpreted as vibration because they travel through a pathway labeled for vibration. Similarly, the law of projection explains that sensation is felt at the site of the peripheral receptor even though perception occurs in the brain.
Receptive field size affects localization. Fingertips have small receptive fields and high receptor density, allowing precise localization and two-point discrimination. The back has larger receptive fields and poorer localization.
Adaptation is another key property. Rapidly adapting receptors respond mainly when a stimulus begins or changes, which helps detect movement and vibration. Slowly adapting receptors continue firing during a sustained stimulus, which helps detect pressure, shape, and body position.
If transduction is impaired, a stimulus may not be converted into neural impulses. Clinically, this can appear as numbness, reduced touch, loss of vibration sense, or inability to detect harmful stimuli.
⚠️ CLINICAL IMPORTANCE
Damage to sensory receptors or peripheral nerves impairs the first step of sensory processing. For example, diabetic peripheral neuropathy damages sensory fibers and causes numbness, burning pain, and loss of protective sensation. Large fiber dysfunction affects vibration and proprioception, while small fiber dysfunction affects pain and temperature.
![]()
C. Ascending Somatic Sensory Pathways and Their Major Differences
🧠 CORE
- Ascending sensory pathways transmit body sensations to higher centers.
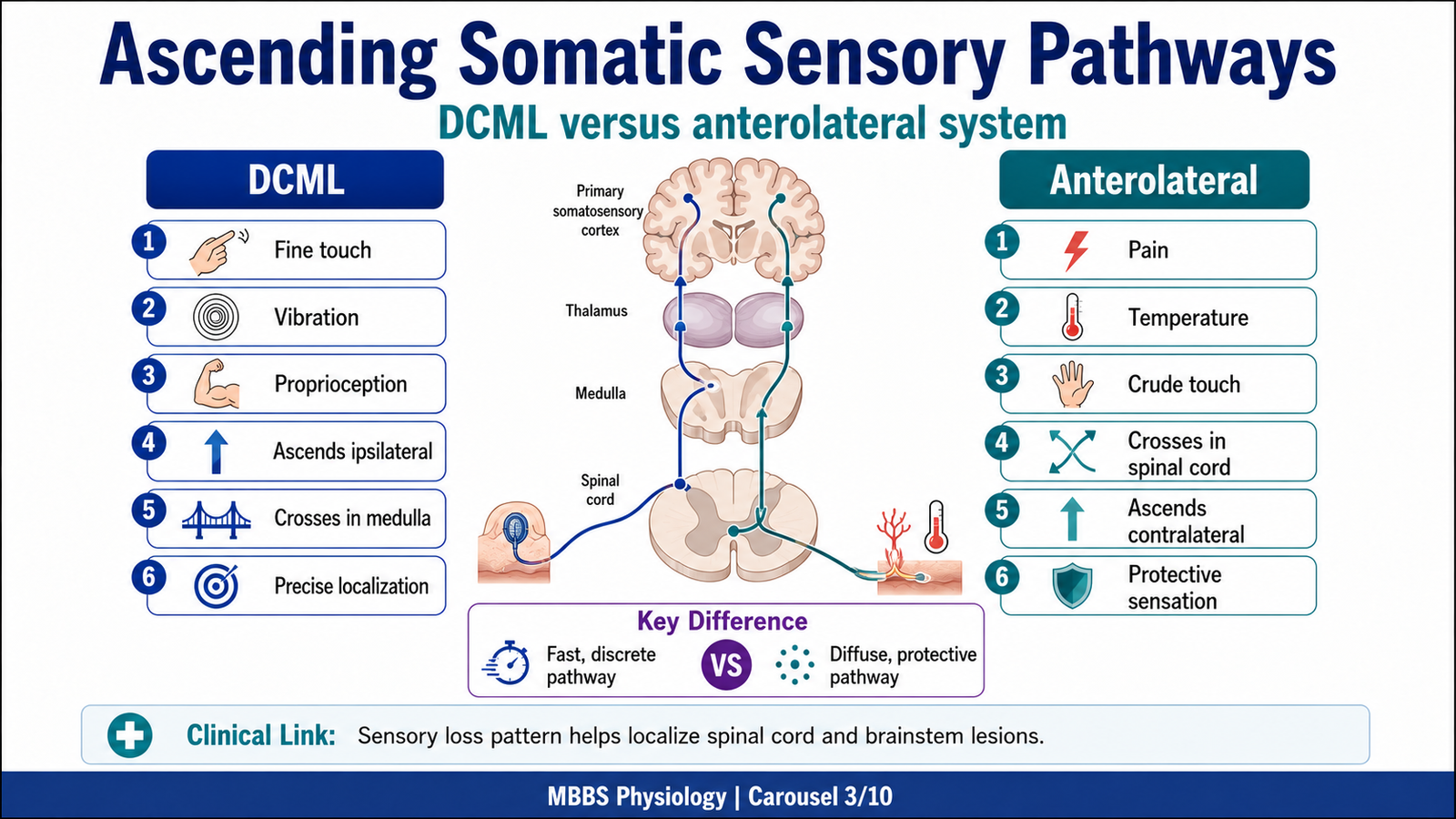
- The two major body pathways are DCML and anterolateral system.
- DCML carries fine touch, vibration, conscious proprioception, and two-point discrimination.
- Anterolateral system carries pain, temperature, crude touch, pressure, itch, and tickle.
- DCML ascends ipsilaterally in spinal cord and crosses in medulla.
- Anterolateral fibers usually cross in spinal cord soon after entry.
- Both pathways relay through thalamus before reaching cortex.
- Pathway differences help localize neurological lesions.
🔬 CONCEPT EXPLAINED
Once sensory impulses enter the spinal cord, they must ascend to the brain. The body uses different pathways because different sensations require different levels of speed, accuracy, and localization.
The dorsal column–medial lemniscal system is designed for accurate, fast, well-localized sensations. It carries fine touch, vibration, conscious proprioception, stereognosis, and two-point discrimination. These sensations require high spatial precision, so they are carried by large, myelinated fibers and remain highly organized throughout the pathway.
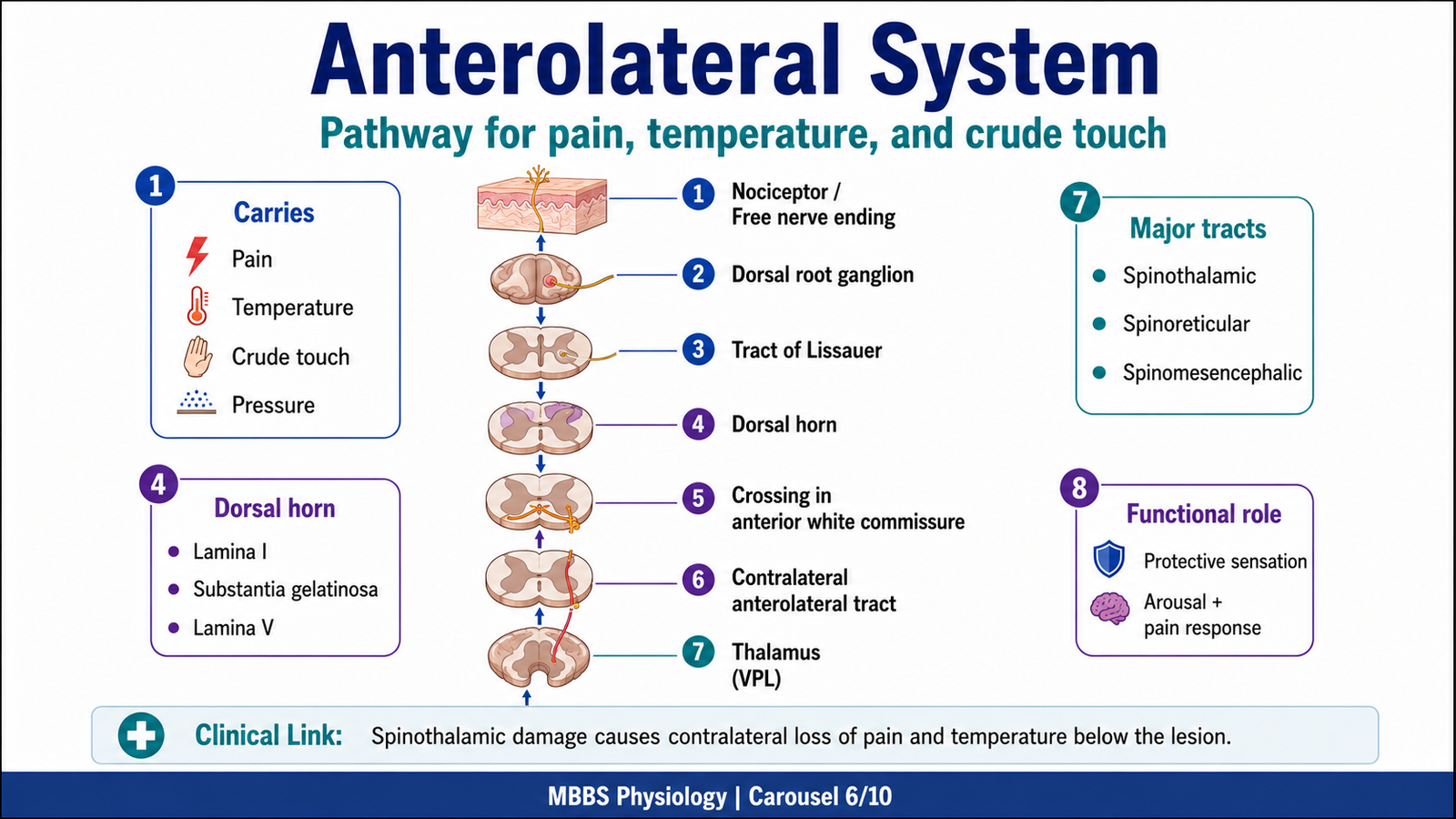
The anterolateral system is designed mainly for protective and less discriminative sensations. It carries pain, temperature, crude touch, pressure, itch, and tickle. These sensations do not always require fine localization but must alert the body to injury or environmental threat. Therefore, the pathway is more diffuse and includes multiple tracts such as spinothalamic, spinoreticular, and spinomesencephalic components.
The timing and site of crossing are clinically important. In the DCML pathway, fibers enter the spinal cord and ascend on the same side in the dorsal columns. They cross later in the medulla. Therefore, a spinal cord lesion affecting the dorsal column causes loss of fine touch, vibration, and proprioception on the same side below the lesion.
In contrast, the anterolateral system crosses in the spinal cord within a few segments after entry. Therefore, a lesion of the spinothalamic tract in the spinal cord causes loss of pain and temperature on the opposite side, usually beginning a few segments below the lesion.
The physiological advantage of having two systems is that the CNS can separately process precise discriminative information and protective nociceptive information. If these pathways fail, the pattern of sensory loss helps identify the level and side of lesion.
⚠️ CLINICAL IMPORTANCE
A hemisection of the spinal cord can produce ipsilateral loss of DCML sensations and contralateral loss of pain and temperature. This pattern is classically important in spinal cord localization and explains why understanding crossing points is essential in neurological examination.
D. Dorsal Column–Medial Lemniscal System
🧠 CORE
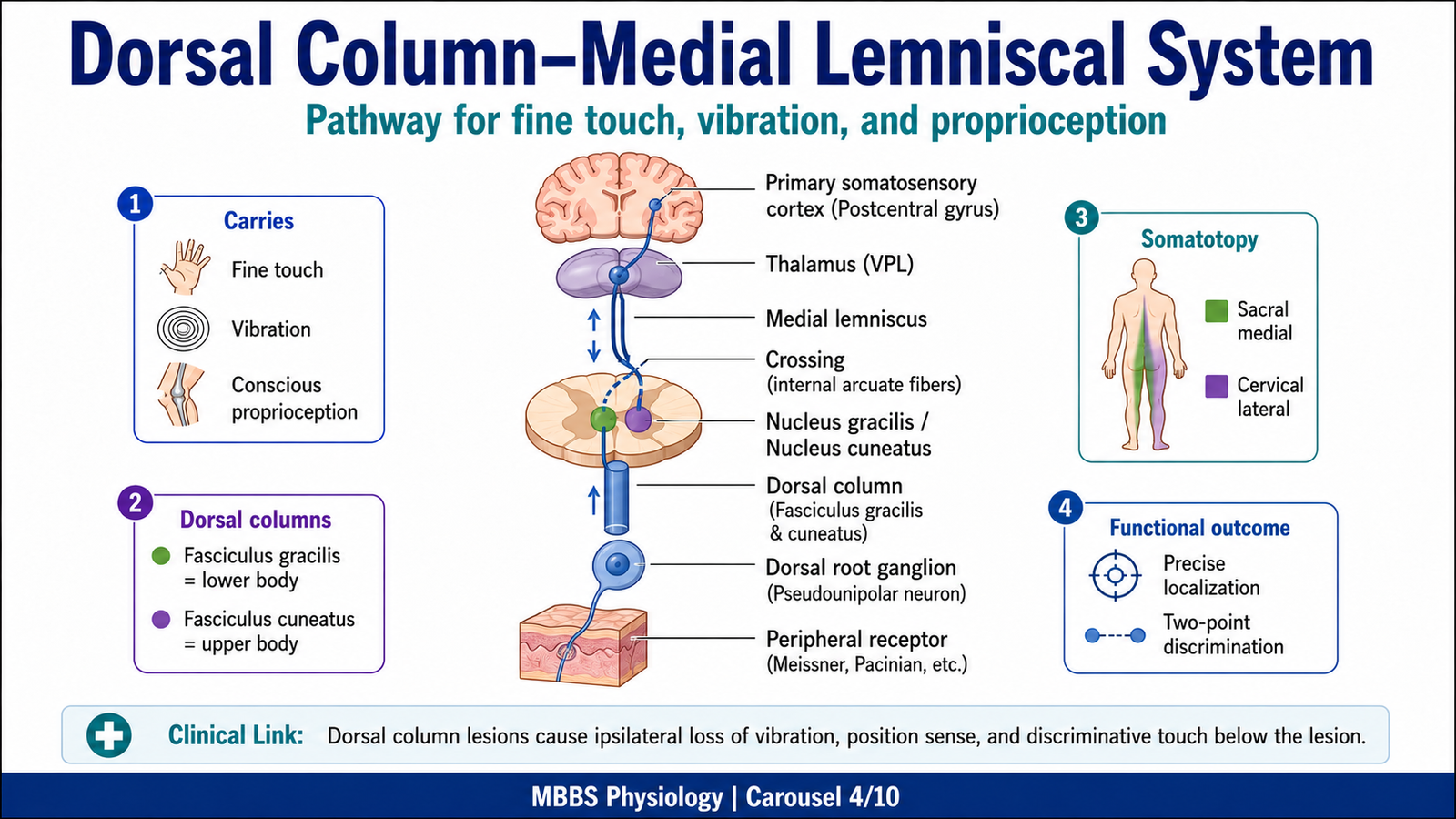
- DCML carries fine touch, vibration, conscious proprioception, and tactile discrimination.
- First-order neurons have cell bodies in dorsal root ganglia.
- Fibers ascend ipsilaterally in fasciculus gracilis and fasciculus cuneatus.
- Lower body fibers ascend in fasciculus gracilis.
- Upper body fibers ascend in fasciculus cuneatus.
- Second-order neurons lie in nucleus gracilis and nucleus cuneatus in medulla.
- Fibers cross as internal arcuate fibers and form medial lemniscus.
- Third-order neurons from thalamus project to primary somatosensory cortex.
🔬 CONCEPT EXPLAINED
The DCML pathway begins when receptors for fine touch, vibration, pressure, and proprioception are stimulated. The initiating event may be contact with an object, vibration of a tuning fork, movement of a joint, or stretch of a muscle or tendon. The purpose of this pathway is to provide the brain with accurate information about body position and detailed tactile features.
First-order neurons enter the spinal cord through dorsal roots. Their cell bodies are located in dorsal root ganglia. Unlike many pain fibers, these fibers do not immediately synapse in the spinal cord. Instead, they ascend on the same side in the dorsal column. This arrangement preserves speed and spatial precision.
The dorsal column is divided into two major fasciculi. The fasciculus gracilis carries information from the lower limb and lower trunk. It is present throughout the spinal cord and lies medially. The fasciculus cuneatus carries information from the upper trunk and upper limb. It appears above approximately the T6 level and lies laterally.
This spatial orientation is important. In the dorsal columns, sacral fibers are most medial, followed laterally by lumbar, thoracic, and cervical fibers. Therefore, as new fibers enter from higher levels, they are added laterally. This somatotopic organization helps preserve body mapping from spinal cord to cortex.
The first synapse occurs in the medulla. Fibers from fasciculus gracilis synapse in nucleus gracilis, and fibers from fasciculus cuneatus synapse in nucleus cuneatus. Second-order neurons then cross to the opposite side as internal arcuate fibers. After crossing, they form the medial lemniscus and ascend through the brainstem to the thalamus, mainly the ventral posterolateral nucleus.
Third-order neurons project from the thalamus to the primary somatosensory cortex in the postcentral gyrus. Here the sensation becomes conscious and accurately localized.
The functional advantage of DCML is precision. It allows the brain to know the exact position of limbs, identify object shape and texture, detect vibration, and distinguish two close points on the skin. If this system is impaired, the patient may have sensory ataxia, positive Romberg sign, loss of vibration sense, impaired joint position sense, and poor tactile discrimination.
⚠️ CLINICAL IMPORTANCE
Dorsal column damage produces ipsilateral loss of vibration, conscious proprioception, fine touch, and two-point discrimination below the lesion. Patients may walk unsteadily because they cannot sense limb position, especially when visual input is removed.
E. Two-Point Discrimination and Spatial Localization
🧠 CORE
- Two-point discrimination tests the ability to distinguish two nearby stimuli.
- It depends on receptor density, receptive field size, and cortical representation.
- Fingertips and lips have excellent two-point discrimination.
- Back and thigh have poor two-point discrimination.
- DCML pathway is essential for fine tactile discrimination.
- Lateral inhibition sharpens sensory localization.
- The somatosensory cortex interprets spatial detail.
- It is clinically useful for testing cortical sensory function.
🔬 CONCEPT EXPLAINED
Two-point discrimination is the ability to perceive two simultaneous points of contact as separate rather than one. The initiating event is stimulation of two nearby skin points. The purpose of this mechanism is to allow precise tactile recognition, especially in areas used for fine manipulation.
This ability depends on small receptive fields and high receptor density. In the fingertips, many receptors are packed into a small area, and each sensory neuron receives information from a small region of skin. Therefore, two nearby stimuli activate separate sensory channels. In the back, receptive fields are large and receptor density is low, so two nearby stimuli may activate the same sensory field and are perceived as one point.
The DCML pathway carries this precise spatial information to the cortex. Lateral inhibition further improves localization. When a central sensory neuron is strongly activated, it inhibits neighboring pathways. This reduces spread of excitation and sharpens contrast between the stimulated and surrounding areas.
The cause → effect relationship is clear: high receptor density plus small receptive fields plus lateral inhibition leads to accurate localization. Low receptor density, large receptive fields, or pathway damage leads to poor discrimination.
The physiological advantage is that the hand can identify object edges, shape, and texture without vision. If impaired, patients may fail to recognize objects by touch or may be unable to localize tactile stimuli accurately.
⚠️ CLINICAL IMPORTANCE
Impaired two-point discrimination may occur in peripheral nerve lesions, dorsal column disease, thalamic lesions, or cortical sensory area damage. It is especially useful in assessing fine sensory function of the hand.

F. Anterolateral System: Pain, Temperature, Crude Touch and Protective Sensations
🧠 CORE
- Anterolateral system carries pain, temperature, crude touch, pressure, itch, and tickle.
- First-order neurons enter the spinal cord through dorsal roots.
- Many fibers synapse in dorsal horn laminae.
- Second-order neurons cross in anterior white commissure.
- Fibers ascend mainly in contralateral anterolateral funiculus.
- Major components include spinothalamic, spinoreticular, and spinomesencephalic pathways.
- It is less precise than DCML but highly protective.
- It has strong clinical importance in pain and temperature loss.
🔬 CONCEPT EXPLAINED
The anterolateral system begins when potentially harmful or less precisely localized stimuli activate receptors. The initiating event may be tissue injury, extreme heat, cold, strong pressure, itch-producing chemical mediators, or crude mechanical contact. The purpose of this system is protection. It alerts the body to actual or potential damage so that withdrawal, autonomic responses, emotional reactions, and protective behavior can occur.
Pain and temperature receptors are mainly free nerve endings. Tissue injury releases chemical mediators such as potassium ions, prostaglandins, bradykinin, histamine, and other inflammatory substances. These substances activate or sensitize nociceptors. Mechanical or thermal stimuli can also directly activate receptor channels.
First-order neurons have cell bodies in dorsal root ganglia and enter the spinal cord. Many pain and temperature fibers ascend or descend one or two segments in the tract of Lissauer before synapsing in the dorsal horn. Their central endings terminate mainly in specific laminae of spinal gray matter. Pain and temperature fibers commonly terminate in lamina I, lamina II/substantia gelatinosa, and lamina V. Crude touch and pressure may also involve deeper dorsal horn neurons.
Second-order neurons cross to the opposite side through the anterior white commissure, usually within one to two spinal segments. They then ascend in the anterolateral funiculus. Because crossing occurs early in the spinal cord, unilateral spinal cord lesions produce contralateral loss of pain and temperature below the lesion.
The anterolateral system is functionally organized into submodalities. The lateral spinothalamic tract carries pain and temperature. The anterior spinothalamic tract carries crude touch and pressure. The spinoreticular pathway projects to reticular formation and contributes to arousal and emotional-affective aspects of pain. The spinomesencephalic pathway projects to midbrain areas and participates in pain modulation and orienting responses.
Compared with DCML, the anterolateral system has slower conduction, broader receptive fields, and less precise localization. However, its advantage is survival. It rapidly warns the body of harmful stimuli and activates protective reflexes and behavioral responses.
If the anterolateral system is impaired, the patient may lose pain and temperature sensation on the opposite side of the body. This is dangerous because injury, burns, or infection may go unnoticed.
⚠️ CLINICAL IMPORTANCE
Damage to the spinothalamic tract causes contralateral loss of pain and temperature below the lesion. Syringomyelia can damage crossing fibers in the anterior white commissure, producing bilateral segmental loss of pain and temperature while sparing dorsal column sensations.
G. Submodalities of Nondiscriminative Touch, Temperature and Nociception
🧠 CORE
- Nondiscriminative touch is crude and poorly localized.
- Crude touch and pressure are carried mainly by anterolateral pathways.
- Temperature is carried by cold and warmth receptors.
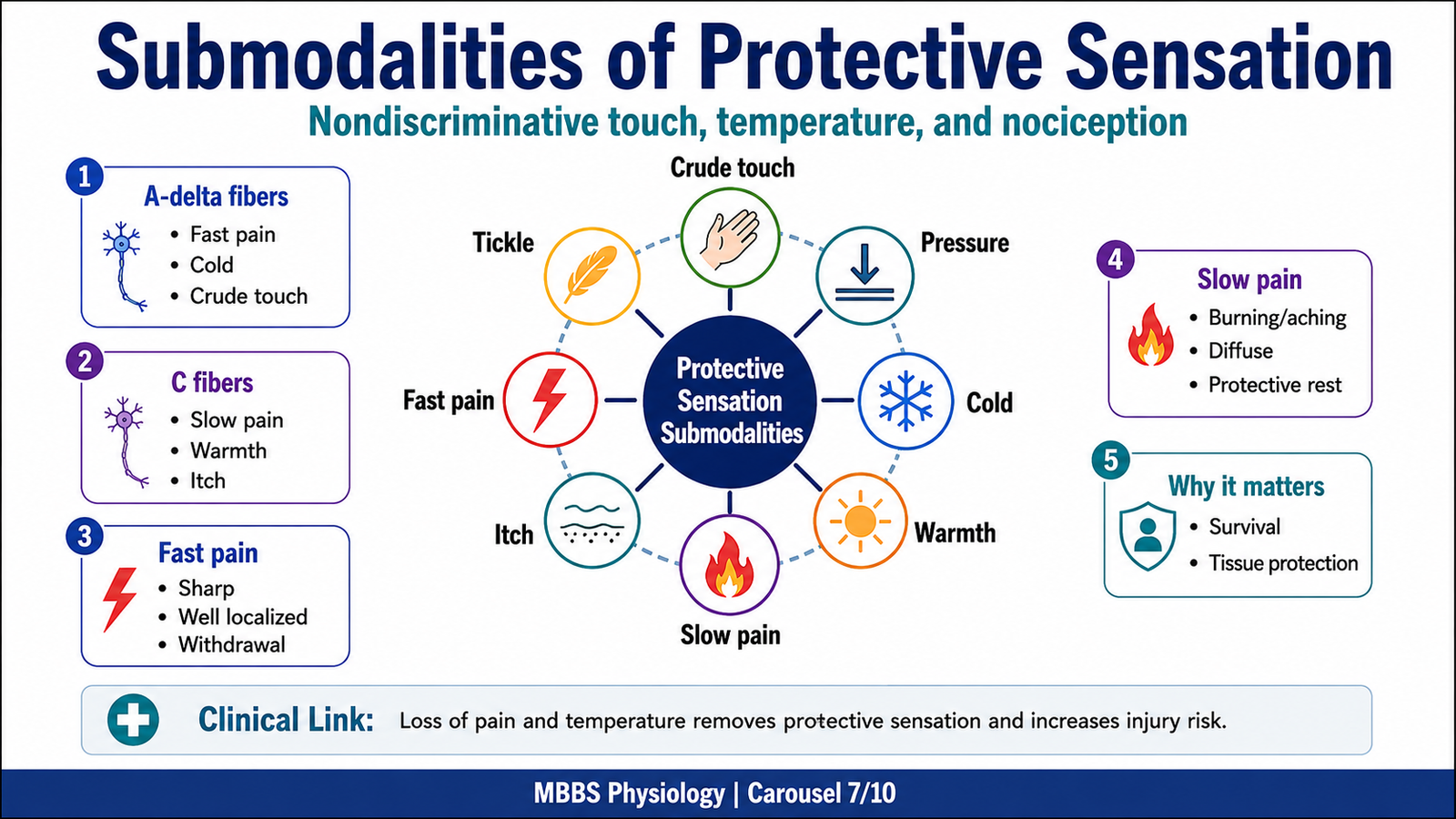
- Nociception includes fast pain, slow pain, and deep pain.
- A-delta fibers carry fast, sharp, well-localized pain.
- C fibers carry slow, dull, burning, poorly localized pain.
- Itch and tickle are protective cutaneous sensations.
- These modalities are important for survival rather than fine discrimination.
🔬 CONCEPT EXPLAINED
Not all touch requires precise localization. Nondiscriminative touch tells the brain that contact has occurred but does not provide detailed information about shape, texture, or exact location. This type of touch is useful when the body simply needs awareness of contact or pressure.
Temperature sensation allows the body to detect cold and warmth. Cold receptors are generally more numerous and respond to cooling of skin, while warmth receptors respond to heating. Extreme temperatures may activate nociceptors and produce pain because very hot or very cold stimuli can damage tissue.
Nociception is the sensory process by which harmful stimuli are detected. Fast pain is usually sharp and well localized. It is carried by A-delta fibers and helps produce rapid withdrawal from harmful stimuli. Slow pain is dull, aching, burning, or throbbing. It is carried by C fibers and is often associated with tissue injury and inflammation.
The mechanism begins when damaging or potentially damaging stimuli activate free nerve endings. Chemical mediators released from injured tissue increase receptor excitability. This sensitization explains why inflamed tissue becomes painful even with mild touch or movement.
The body needs these submodalities because they serve different protective functions. Fast pain produces immediate withdrawal. Slow pain promotes rest and protection of the injured area. Temperature sensation prevents burns and frost injury. Itch promotes removal of irritants from the skin.
If these sensations fail, the patient may be unable to detect harmful heat, cold, injury, or skin irritation. If the system becomes overactive, chronic pain, hyperalgesia, or allodynia may occur.
⚠️ CLINICAL IMPORTANCE
Loss of pain and temperature is clinically dangerous because protective sensation is lost. Excessive nociceptor sensitization contributes to inflammatory pain, neuropathic pain, hyperalgesia, and allodynia.
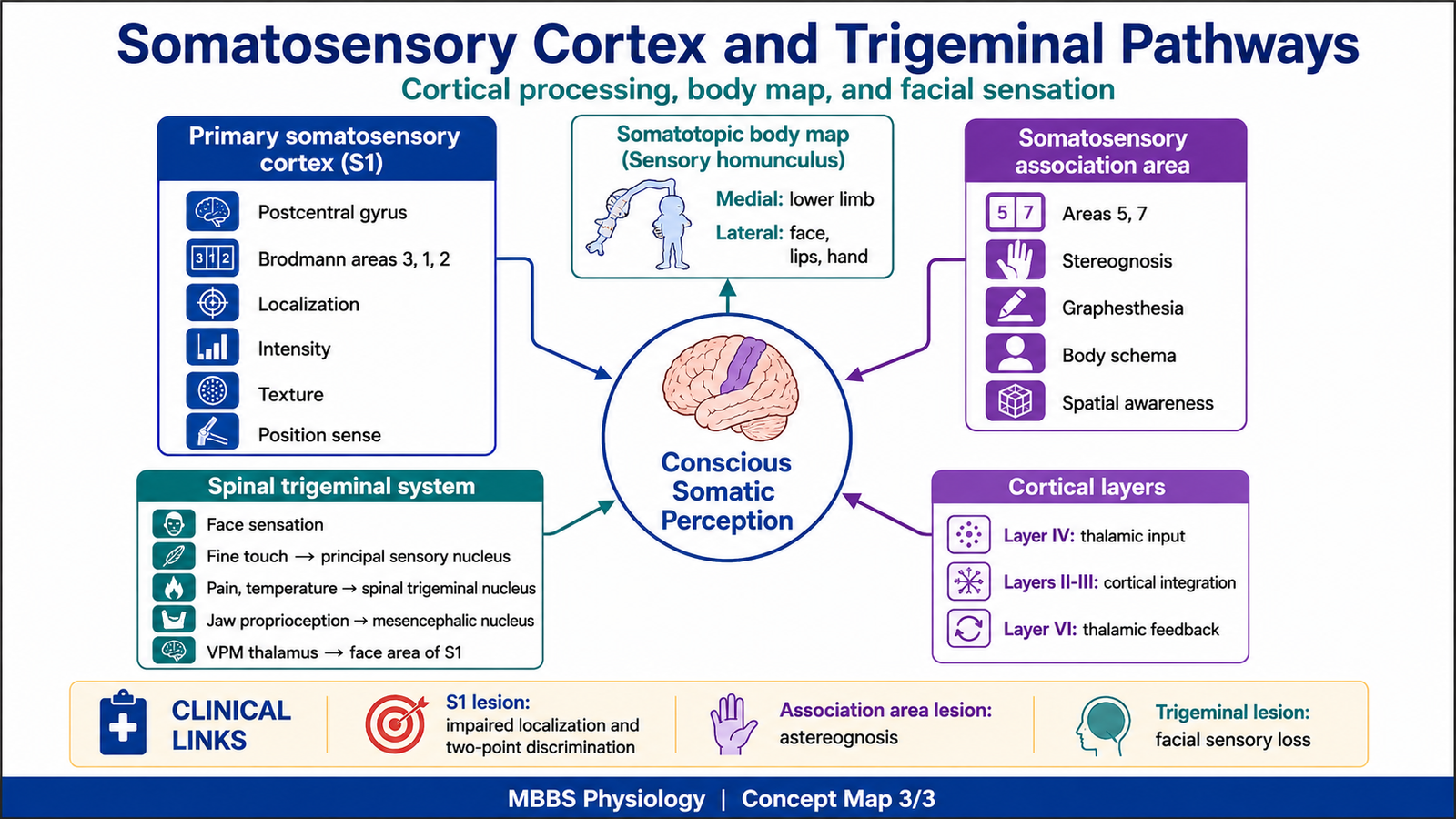
H. Somatosensory Cortex I: Body Representation and Functions
🧠 CORE
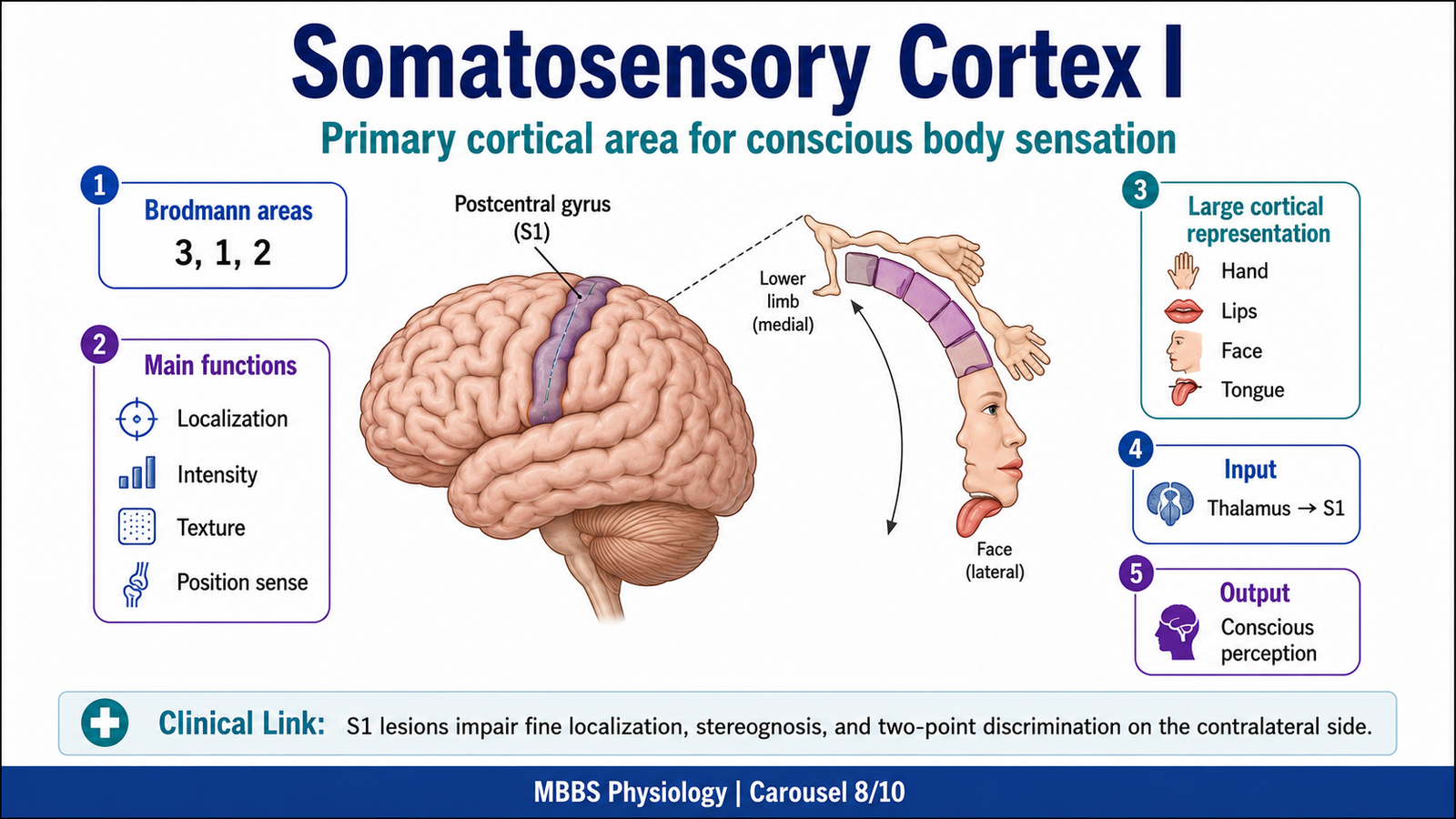
- Primary somatosensory cortex lies in the postcentral gyrus.
- It receives input mainly from thalamic sensory nuclei.
- It corresponds mainly to Brodmann areas 3, 1, and 2.
- Body parts are represented somatotopically as sensory homunculus.
- Large cortical areas represent hands, lips, face, and tongue.
- It allows localization, intensity recognition, and modality discrimination.
- It supports stereognosis and texture recognition.
- Damage causes cortical sensory deficits.
🔬 CONCEPT EXPLAINED
After sensory information reaches the thalamus, it is projected to the primary somatosensory cortex in the postcentral gyrus of the parietal lobe. The purpose of this cortical area is conscious interpretation of somatic sensation. The spinal cord and brainstem transmit information, but the cortex allows the person to know exactly what the stimulus is, where it is, and what it means.
Somatosensory cortex I is organized as a sensory map of the body. This is called the sensory homunculus. The lower limb is represented medially, while trunk, upper limb, hand, face, lips, and tongue are represented more laterally. The size of cortical representation is not proportional to body size. Instead, it reflects sensory importance and receptor density. Therefore, the hands, lips, face, and tongue occupy large cortical areas because they require highly accurate sensory discrimination.
Brodmann areas 3, 1, and 2 form the primary somatosensory cortex. Area 3 receives major thalamic input and is especially important for basic sensory reception. Area 1 is important for texture processing. Area 2 contributes to size, shape, and proprioceptive interpretation. These areas work together rather than as completely isolated units.
The functions of somatosensory area I include localization of touch, judgment of stimulus intensity, discrimination of texture, recognition of object shape, awareness of body position, and comparison of sensory inputs from different body parts. This area is also essential for stereognosis, which is the ability to recognize an object by touch without seeing it.
If somatosensory cortex I fails, basic sensation may not be completely lost because some pathways still reach other brain regions, but discriminative sensory function is impaired. The patient may feel that something touched the skin but may be unable to localize it accurately or identify the object.
⚠️ CLINICAL IMPORTANCE
Lesions of the postcentral gyrus cause contralateral impairment of fine touch, localization, two-point discrimination, stereognosis, and graphesthesia. The sensory loss is more marked in body parts represented by the damaged cortical region.
I. Brodmann Areas of Cerebral Cortex and Their Major Functions
🧠 CORE
- Brodmann areas are cortical regions classified by microscopic structure.
- Areas 3, 1, and 2 form primary somatosensory cortex.
- Areas 5 and 7 form somatosensory association cortex.
- Area 4 is primary motor cortex.
- Area 6 is premotor and supplementary motor cortex.
- Areas 17, 18, and 19 relate to vision.
- Areas 41 and 42 relate to hearing.
- Areas 44 and 45 are involved in motor speech.
🔬 CONCEPT EXPLAINED
Brodmann divided the cerebral cortex into numbered areas based on differences in cellular organization. These areas are useful because structure and function are related. Although modern neuroscience recognizes that functions are distributed across networks, Brodmann areas remain important in undergraduate anatomy and physiology.
For somatic sensation, the most important areas are 3, 1, and 2, located in the postcentral gyrus. They receive sensory input from the thalamus and process conscious somatic sensation. Areas 5 and 7, located posteriorly in the parietal cortex, form the somatosensory association area. They interpret sensory information at a higher level and connect it with past experience, body awareness, and spatial orientation.
Other important areas include area 4, the primary motor cortex in the precentral gyrus; area 6, premotor and supplementary motor cortex; area 17, primary visual cortex; areas 18 and 19, visual association cortex; areas 41 and 42, auditory cortex; and areas 44 and 45, Broca’s motor speech area in the dominant hemisphere.
The physiological advantage of cortical specialization is efficient processing. Primary areas receive and analyze basic sensory or motor signals, while association areas interpret meaning and plan complex responses.
⚠️ CLINICAL IMPORTANCE
Damage to specific Brodmann areas produces predictable deficits. Lesions of areas 3, 1, and 2 impair contralateral somatic sensation. Lesions of areas 5 and 7 may cause sensory neglect, astereognosis, or difficulty integrating sensory information despite relatively preserved primary sensation.
J. Layers of Somatosensory Cortex and Their Functions
🧠 CORE
- Cerebral cortex has six histological layers.
- Layer IV receives major thalamic sensory input.
- Layers II and III communicate with other cortical areas.
- Layer V sends output to subcortical structures.
- Layer VI sends feedback to thalamus.
- Somatosensory cortex has a well-developed granular layer IV.
- Cortical columns process specific sensory inputs.
- Layered organization supports analysis, integration, and feedback control.
🔬 CONCEPT EXPLAINED
The cerebral cortex is not a uniform sheet. It is arranged into six layers, each with characteristic inputs and outputs. This layered structure allows sensory information to be received, processed, shared, and regulated.
In the somatosensory cortex, thalamic sensory fibers mainly terminate in layer IV, the internal granular layer. This layer is especially prominent in sensory cortex because it receives large amounts of incoming sensory information. From layer IV, signals spread vertically and horizontally to other cortical layers and neighboring cortical columns.
Layers II and III are important for communication between cortical areas. They allow sensory information from one region to be compared and integrated with information from other regions. This is necessary for recognizing complex patterns such as texture and shape.
Layer V contains large output neurons that project to subcortical structures, including brainstem and spinal cord-related systems. Layer VI sends feedback projections to the thalamus. This feedback helps regulate sensory transmission and may enhance or suppress incoming sensory information depending on attention and context.
The purpose of cortical layering is not simply anatomical organization. It allows the cortex to receive input, interpret it, compare it with other information, send outputs, and regulate its own sensory inflow. This is why sensation is not passive; it is actively processed and shaped by attention, previous experience, and cortical networks.
If cortical organization is damaged, sensation may be present but poorly interpreted. The patient may detect touch but fail to recognize its meaning.
⚠️ CLINICAL IMPORTANCE
Cortical lesions can produce higher sensory deficits such as astereognosis, agraphesthesia, impaired two-point discrimination, and sensory neglect. These deficits show that cortical processing is essential for interpretation, not merely detection.
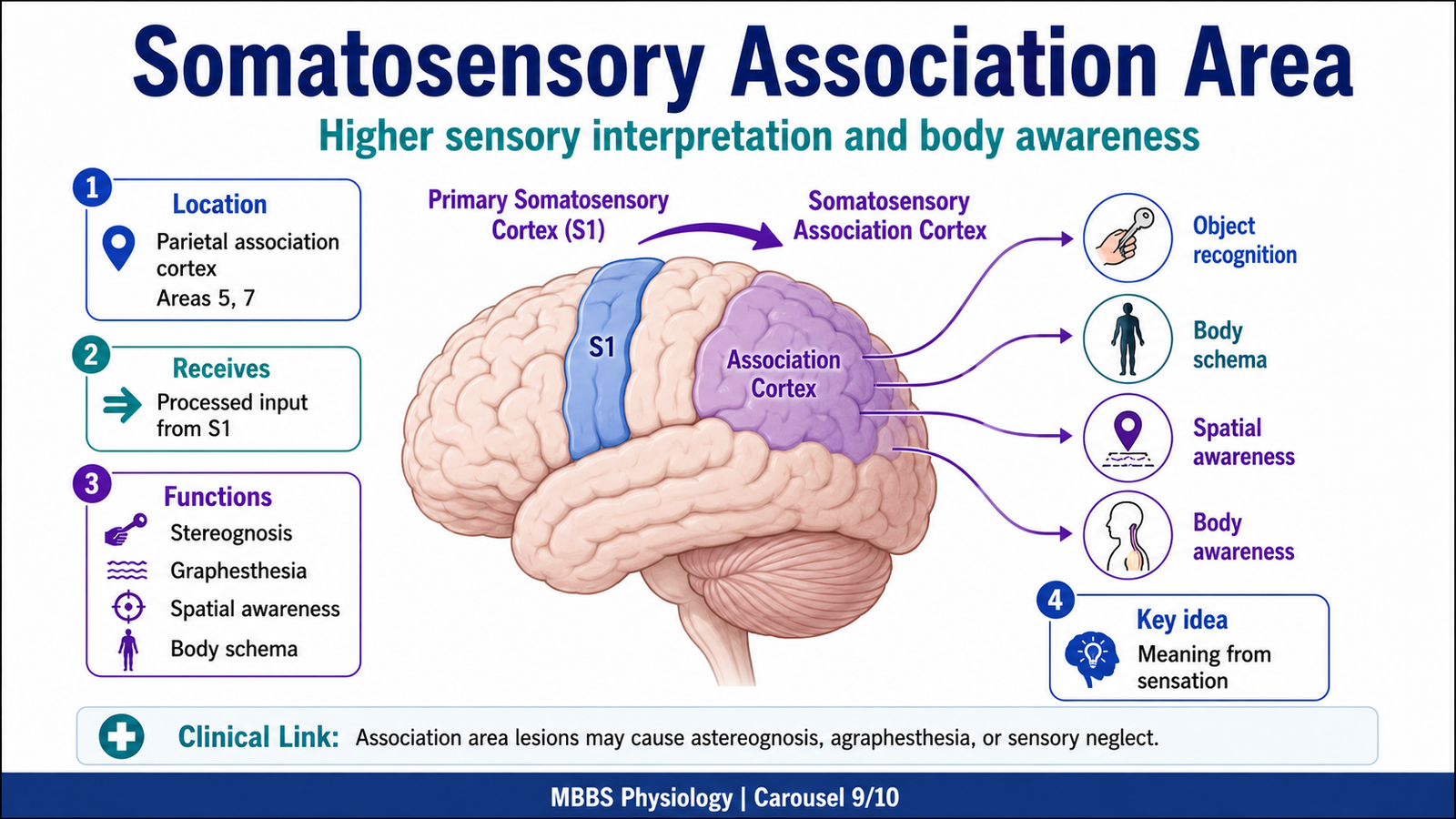
K. Somatosensory Association Area
🧠 CORE
- Somatosensory association cortex lies posterior to primary sensory cortex.
- It includes mainly Brodmann areas 5 and 7.
- It integrates touch, pressure, proprioception, and visual-spatial information.
- It helps identify object shape and meaning.
- It contributes to body schema and spatial awareness.
- It allows comparison of current sensory input with memory.
- It supports stereognosis and complex tactile recognition.
- Lesions produce higher sensory disturbances.
🔬 CONCEPT EXPLAINED
Primary somatosensory cortex tells the brain that a stimulus has occurred and identifies basic features such as location, intensity, and modality. However, meaningful interpretation requires association cortex. The somatosensory association area receives processed input from primary sensory cortex and integrates it with memory, attention, and spatial awareness.
For example, when a person holds a key in the hand with eyes closed, primary sensory cortex detects pressure, edges, texture, and position of fingers. The association cortex integrates these features and compares them with stored sensory memory. As a result, the person recognizes the object as a key. This ability is called stereognosis.
The association cortex also contributes to body schema, which is the brain’s internal awareness of body parts and their position in space. This becomes important during movement, posture, tool use, and interaction with the environment.
If the association area is damaged, elementary sensation may remain present, but the patient cannot interpret complex sensory information. The patient may feel an object but cannot identify it by touch. In some parietal lesions, the patient may ignore one side of the body or space.
⚠️ CLINICAL IMPORTANCE
Lesions of somatosensory association cortex may cause astereognosis, agraphesthesia, impaired spatial awareness, and sensory neglect. These are important cortical sensory signs in neurological examination.
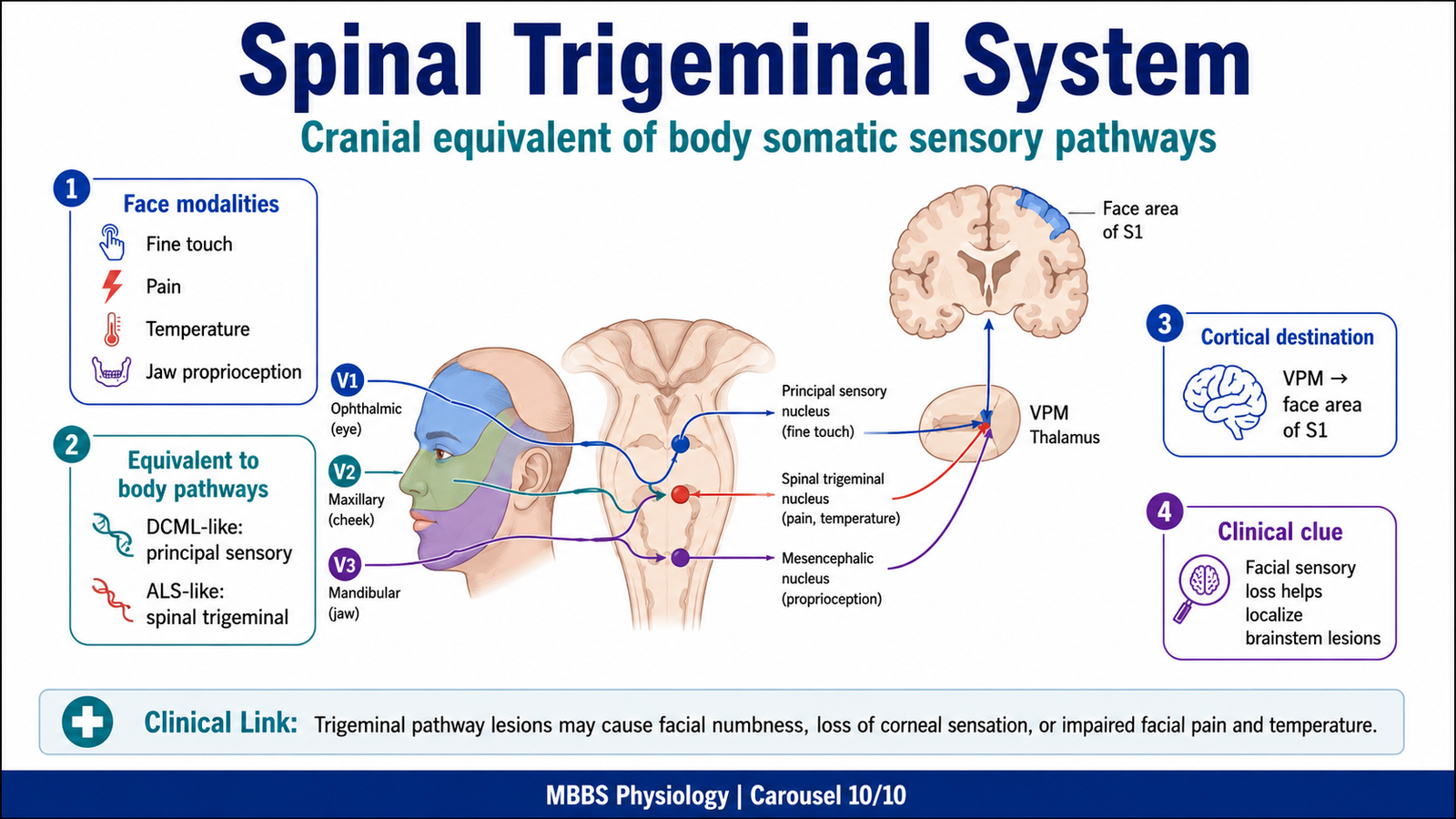
L. Equivalent Components of the Spinal Trigeminal System
🧠 CORE
- Trigeminal system carries somatic sensation from face, oral cavity, nasal cavity, and anterior scalp.
- It is the cranial equivalent of body somatic sensory pathways.
- Fine touch from face uses principal sensory nucleus of trigeminal nerve.
- Pain and temperature from face use spinal trigeminal nucleus and tract.
- Mesencephalic nucleus carries proprioception from jaw muscles and periodontal ligaments.
- Trigeminal sensory fibers project to thalamus and then sensory cortex.
- Face is represented laterally in somatosensory cortex.
- Lesions produce facial sensory loss depending on component involved.
🔬 CONCEPT EXPLAINED
The body uses spinal pathways for trunk and limbs, but the face requires an equivalent cranial nerve system. The trigeminal nerve is the main sensory nerve of the face. It carries touch, pain, temperature, and proprioceptive information from the face, scalp anteriorly, cornea, oral cavity, nasal cavity, teeth, and jaw structures.
The principal sensory nucleus of trigeminal nerve is functionally comparable to the DCML system for the face. It receives fine touch and pressure information and helps transmit discriminative facial sensation.
The spinal trigeminal nucleus and tract are functionally comparable to the anterolateral system. Pain and temperature fibers from the face descend in the spinal trigeminal tract and synapse in the spinal trigeminal nucleus. From there, second-order neurons cross and ascend to the thalamus.
The mesencephalic nucleus is unique because it contains primary sensory neuron cell bodies inside the CNS rather than in a peripheral ganglion. It carries proprioceptive information from muscles of mastication and periodontal ligaments, which is important for jaw reflexes and bite control.
The trigeminal system then relays information to the thalamus, especially the ventral posteromedial nucleus, and then to the face area of the primary somatosensory cortex.
The physiological advantage of this system is that facial sensation is processed with the same principles as body sensation but through specialized cranial nerve pathways. If impaired, patients may lose facial touch, pain, temperature, corneal reflex, or jaw proprioception depending on the lesion site.
⚠️ CLINICAL IMPORTANCE
Damage to trigeminal sensory pathways may cause facial numbness, loss of corneal reflex, impaired facial pain and temperature sensation, or trigeminal neuralgia-like symptoms. Spinal trigeminal lesions are especially important in brainstem localization.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Function | Outcome |
|---|---|---|
| Meissner’s corpuscles | Detect light touch and movement over skin | Fine tactile control and grip adjustment |
| Pacinian corpuscles | Detect deep pressure and vibration | Vibration sense and detection of rapid mechanical changes |
| Merkel cells | Detect sustained pressure, edges, texture | Shape and texture recognition |
| Ruffini endings | Detect skin stretch | Hand posture and object manipulation |
| Free nerve endings | Detect pain, temperature, itch, crude touch | Protective sensation |
| Dorsal root ganglion | Houses first-order sensory neuron cell bodies | Entry point for body sensory signals |
| Dorsal columns | Carry fine touch, vibration, proprioception ipsilaterally | Precise sensory transmission |
| Fasciculus gracilis | Carries lower body DCML sensations | Lower limb and lower trunk sensory mapping |
| Fasciculus cuneatus | Carries upper body DCML sensations | Upper limb and upper trunk sensory mapping |
| Medial lemniscus | Carries crossed DCML fibers to thalamus | Conscious fine sensory pathway |
| Anterolateral funiculus | Carries crossed pain, temperature, crude touch | Protective sensory transmission |
| Thalamus | Relays sensory input to cortex | Conscious sensory awareness |
| Primary somatosensory cortex | Localizes and identifies sensory modality | Perception of touch, pain, temperature, position |
| Somatosensory association cortex | Integrates sensory meaning | Object recognition and body awareness |
| Spinal trigeminal nucleus | Carries facial pain and temperature | Cranial equivalent of anterolateral system |
| Principal trigeminal nucleus | Carries facial fine touch | Cranial equivalent of discriminative touch pathway |
The integrated functional story is simple: receptors detect the stimulus, peripheral nerves carry the signal, spinal cord and brainstem pathways organize and transmit it, the thalamus relays it, and the cortex interprets it. When any structure in this chain is damaged, the type and side of sensory loss depend on which pathway is affected and where the lesion occurs.
🩺 5️⃣ Clinical Correlation
1. Dorsal Column Lesion
Damage to the dorsal column impairs vibration sense, conscious proprioception, fine touch, and two-point discrimination on the same side below a spinal cord lesion. Because proprioceptive input is reduced, the patient may develop sensory ataxia. The Romberg test may become positive because the patient depends heavily on vision to maintain posture.
2. Spinothalamic Tract Lesion
Damage to the spinothalamic tract causes loss of pain and temperature on the opposite side below the lesion. This occurs because anterolateral fibers cross in the spinal cord soon after entry. Clinically, this helps localize spinal cord lesions.
3. Syringomyelia
In syringomyelia, a cavity may develop near the central canal of the spinal cord. This can damage crossing spinothalamic fibers in the anterior white commissure. As a result, there is bilateral segmental loss of pain and temperature, often with preservation of fine touch and proprioception.
4. Peripheral Neuropathy
Peripheral nerve damage affects sensory transmission before signals enter the spinal cord. Depending on fiber type, patients may lose vibration, pain, temperature, or fine touch. Small fiber neuropathy affects pain and temperature more, while large fiber neuropathy affects vibration, proprioception, and reflexes.
5. Cortical Sensory Lesion
Lesions of the primary somatosensory cortex cause contralateral sensory impairment, especially loss of fine localization, two-point discrimination, stereognosis, and graphesthesia. Lesions of association cortex may allow basic sensation but impair interpretation of sensory meaning.
6. Trigeminal Sensory Lesion
Damage to trigeminal sensory pathways causes facial sensory loss. Lesions involving the spinal trigeminal nucleus affect facial pain and temperature, while lesions involving the principal sensory nucleus affect fine touch. Loss of corneal sensation may impair the corneal reflex and increase risk of corneal injury.
📌 6️⃣ Summary Points
- Somatic sensation includes touch, pressure, vibration, pain, temperature, and proprioception.
- DCML carries fine touch, vibration, conscious proprioception, stereognosis, and two-point discrimination.
- Anterolateral system carries pain, temperature, crude touch, pressure, itch, and tickle.
- DCML ascends ipsilaterally in spinal cord and crosses in the medulla.
- Anterolateral fibers cross in the spinal cord through the anterior white commissure.
- Fasciculus gracilis carries lower body sensations and lies medially.
- Fasciculus cuneatus carries upper body sensations and lies laterally.
- Two-point discrimination is best where receptor density is high and receptive fields are small.
- Primary somatosensory cortex lies in the postcentral gyrus and corresponds mainly to Brodmann areas 3, 1, and 2.
- Somatosensory association cortex, mainly areas 5 and 7, gives meaning to sensory input.
- Layer IV of sensory cortex receives major thalamic sensory input.
- Spinal trigeminal nucleus is the cranial equivalent of anterolateral pain and temperature pathways for the face.