
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Voluntary movement is not produced by muscles alone; it is planned, initiated, refined, and controlled by higher motor areas of the cerebral cortex and descending motor pathways. The cerebral cortex, especially the frontal lobe, sends commands through the corticospinal and corticobulbar systems to activate spinal and cranial nerve motor neurons. These pathways allow skilled, purposeful, and precise movements such as writing, speaking, walking, and facial expression.
The motor cortex lies mainly in the frontal lobe, anterior to the central sulcus. Its signals descend through the internal capsule, brainstem, and spinal cord before reaching lower motor neurons. Cortical motor control is clinically important because damage to the upper motor neuron pathway produces weakness, spasticity, hyperreflexia, Babinski sign, and abnormal postures such as decorticate or decerebrate rigidity. Understanding this topic helps students connect neuroanatomy, physiology, and clinical neurology into one integrated motor control system.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Motor cortex: Cortical areas of the brain that plan, initiate, and control voluntary movements.
- Upper motor neuron: A neuron whose cell body lies in the cerebral cortex or brainstem and whose axon descends to influence lower motor neurons.
- Lower motor neuron: A neuron whose cell body lies in the anterior horn of the spinal cord or motor cranial nerve nuclei and whose axon directly supplies skeletal muscle.
- Pyramidal pathway: The corticospinal and corticobulbar tracts that arise mainly from the cerebral cortex and pass through the pyramids of the medulla.
- Corticospinal tract: Descending pathway from cerebral cortex to spinal cord motor neurons; important for voluntary control of limb and trunk muscles.
- Corticobulbar tract: Descending pathway from cerebral cortex to motor nuclei of cranial nerves in the brainstem; important for voluntary control of face, tongue, pharynx, and larynx.
- Extrapyramidal system: Descending motor control system outside the direct pyramidal pathway, involving basal ganglia, brainstem nuclei, cerebellum, and descending tracts such as rubrospinal, reticulospinal, vestibulospinal, and tectospinal tracts.
- Descending tracts: Nerve pathways that carry motor commands from brain to spinal cord.
- Decorticate rigidity: Abnormal flexor posturing due to lesion above the red nucleus, with upper limb flexion and lower limb extension.
- Decerebrate rigidity: Abnormal extensor posturing due to lesion below the red nucleus, with extension of upper and lower limbs.
Essential Terminology
- Precentral gyrus: Site of primary motor cortex.
- Central sulcus: Sulcus separating frontal and parietal lobes.
- Motor homunculus: Somatotopic map of body representation in the primary motor cortex.
- Internal capsule: Major white matter pathway carrying corticospinal and corticobulbar fibers.
- Pyramidal decussation: Crossing of most corticospinal fibers in the lower medulla.
- Lateral corticospinal tract: Crossed corticospinal tract controlling distal limb muscles.
- Anterior corticospinal tract: Mostly uncrossed tract controlling axial and proximal muscles.
- Red nucleus: Midbrain nucleus that gives rise to the rubrospinal tract.
- Reticular formation: Brainstem network involved in posture, tone, and automatic motor control.
- Vestibular nuclei: Brainstem nuclei that help maintain balance and extensor tone.
Basic Overview
- Voluntary movement begins with planning in association and premotor areas.
- The primary motor cortex sends final cortical commands for skilled voluntary movement.
- Motor signals descend through corticospinal and corticobulbar pathways.
- These pathways do not directly stimulate most muscles; they influence lower motor neurons and interneurons.
- The pyramidal system is especially important for fine, skilled, fractionated movement.
- The extrapyramidal system adjusts posture, tone, balance, and background motor activity.
- Red nucleus and rubrospinal tract assist motor control, especially flexor-related movements.
- UMN lesions produce weakness with increased tone and exaggerated reflexes.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPTUAL HEADING 1
Functional Organization and Motor Functions of Cortical Motor Areas
🧠 CORE
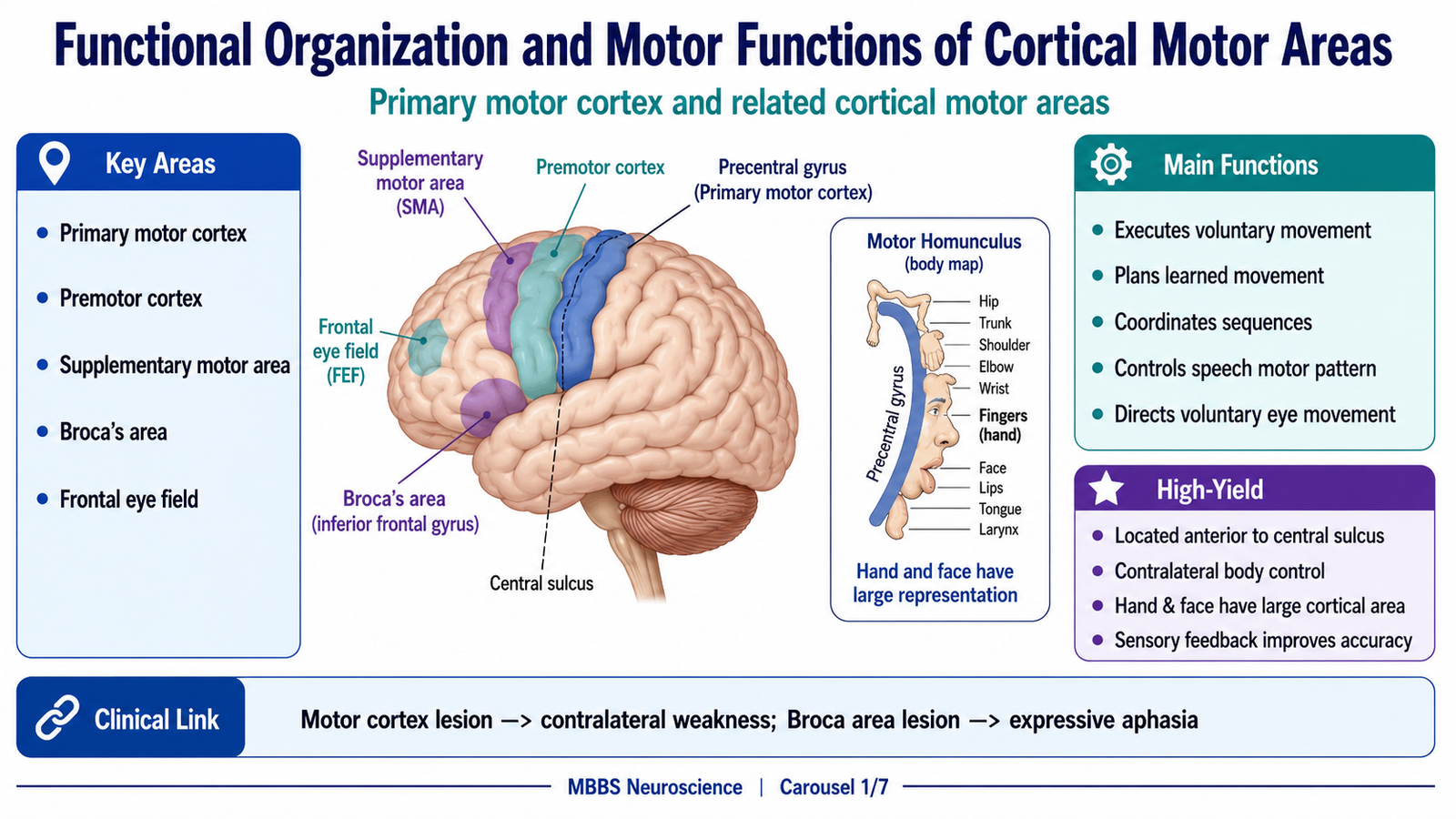
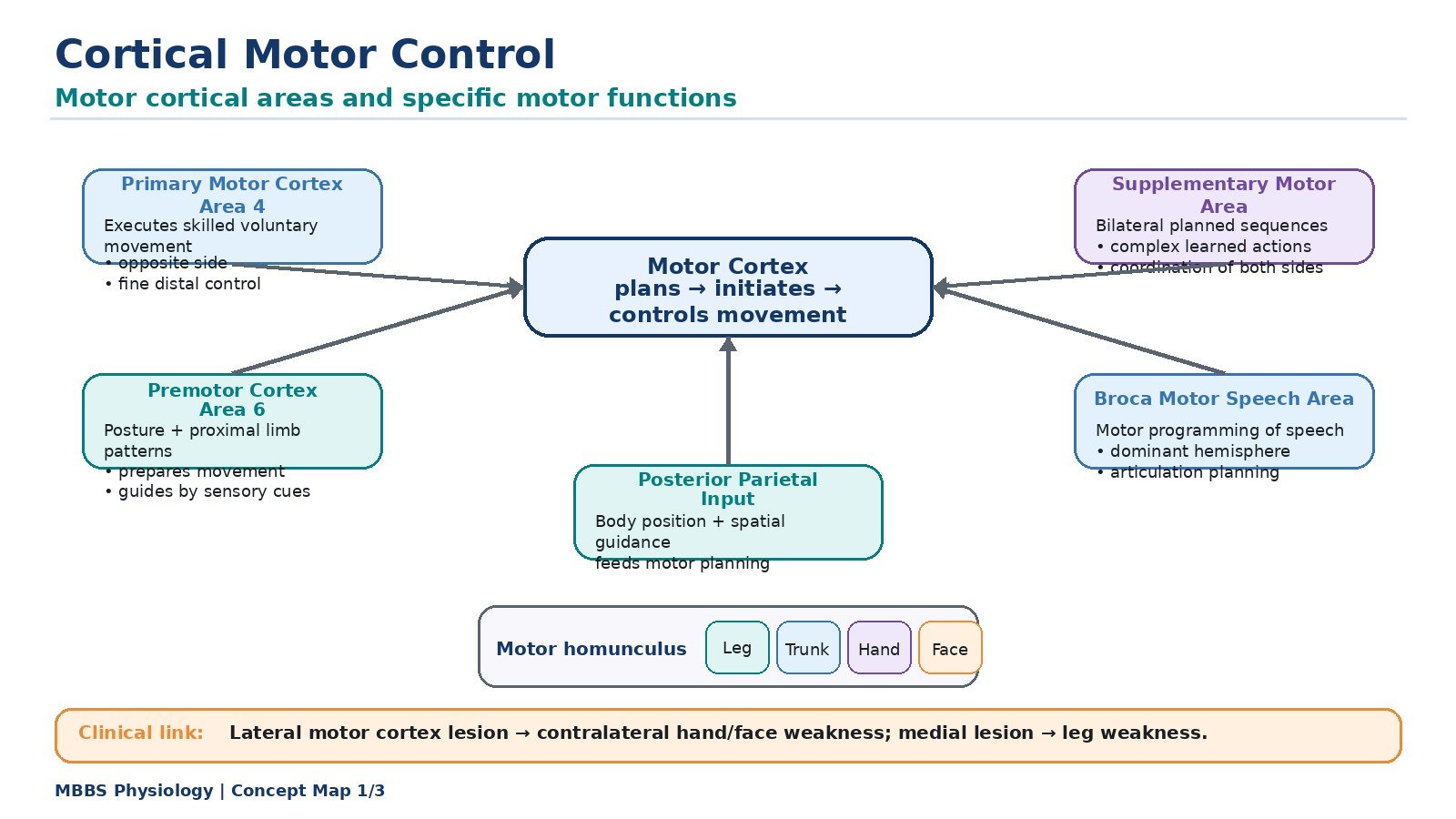
- Motor cortex is mainly located in the frontal lobe anterior to the central sulcus.
- Primary motor cortex lies in the precentral gyrus and executes voluntary movement.
- Premotor cortex prepares movements guided by external sensory cues.
- Supplementary motor area organizes complex, learned, and sequential movements.
- Motor cortex is arranged somatotopically as the motor homunculus.
- Broca’s area controls motor programming of speech in the dominant hemisphere.
- Frontal eye field controls voluntary conjugate eye movements.
- Sensory feedback from somatosensory cortex is essential for accurate movement.
🔬 CONCEPT EXPLAINED
To understand cortical motor control, first remember that voluntary movement is not produced by a single “motor command.” A purposeful movement requires intention, planning, selection of muscles, adjustment of posture, initiation of contraction, and continuous correction. These functions are distributed across several cortical and subcortical areas, but the cerebral cortex provides the highest level of voluntary motor control.
The primary motor cortex is located in the precentral gyrus of the frontal lobe. It is the major cortical area for the execution of voluntary movement. It contains large pyramidal neurons, including Betz cells, which contribute fibers to the corticospinal tract. The primary motor cortex is especially important for skilled, precise, fractionated movements, such as independent finger movement, writing, holding instruments, and controlled facial movement.
The primary motor cortex is arranged as a motor homunculus. This means that different body parts are represented in specific regions of the precentral gyrus. The lower limb is represented medially, while trunk, upper limb, hand, face, lips, and tongue are represented more laterally. The size of cortical representation depends on the precision of movement required, not on the size of the body part. Therefore, the hand, lips, tongue, and face have large cortical areas because they perform highly skilled movements.
The premotor cortex lies anterior to the primary motor cortex. It prepares movements, especially those guided by sensory cues. For example, when a person sees a cup and reaches toward it, the premotor cortex helps organize the movement according to the position and shape of the object. It links sensory information with motor preparation.
The supplementary motor area lies mainly on the medial surface of the frontal lobe. It is important for planning complex, learned, sequential, and bilateral movements. For example, coordinated movements of both hands or a learned sequence of finger movements require supplementary motor area activity before the movement is executed.
The Broca’s area, present in the dominant frontal lobe, is a motor speech planning area. It does not simply contract speech muscles; rather, it organizes the complex motor pattern required for speech. It coordinates movements of the lips, tongue, larynx, pharynx, and respiratory muscles so that speech becomes meaningful and fluent.
The frontal eye field controls voluntary conjugate eye movements. It helps direct both eyes toward a target. This is important because many motor actions require visual orientation before body movement occurs.
The motor cortex does not work independently. It receives information from somatosensory cortex, basal ganglia, cerebellum, and thalamus. Sensory feedback tells the cortex about joint position, muscle stretch, pressure, and touch. Without this feedback, movement becomes clumsy even if muscle power is preserved. Therefore, cortical motor control is a sensory-motor process, not a purely motor process.
As a result, voluntary movement is produced by a coordinated cortical network. Association areas form the intention, premotor and supplementary areas plan the motor program, primary motor cortex sends the command, and sensory feedback modifies the movement continuously.
⚠️ CLINICAL IMPORTANCE
Damage to the primary motor cortex causes weakness on the opposite side of the body because most corticospinal fibers cross in the lower medulla. Lesion of the lateral motor cortex commonly affects opposite face and upper limb, while lesion of the medial motor cortex affects the opposite lower limb. Damage to Broca’s area causes expressive aphasia. Damage to premotor or supplementary motor areas may cause difficulty in planning learned movements even when basic strength is preserved.
MAJOR CONCEPTUAL HEADING 2
Transmission of Motor Signals from Motor Cortex to Muscles
🧠 CORE
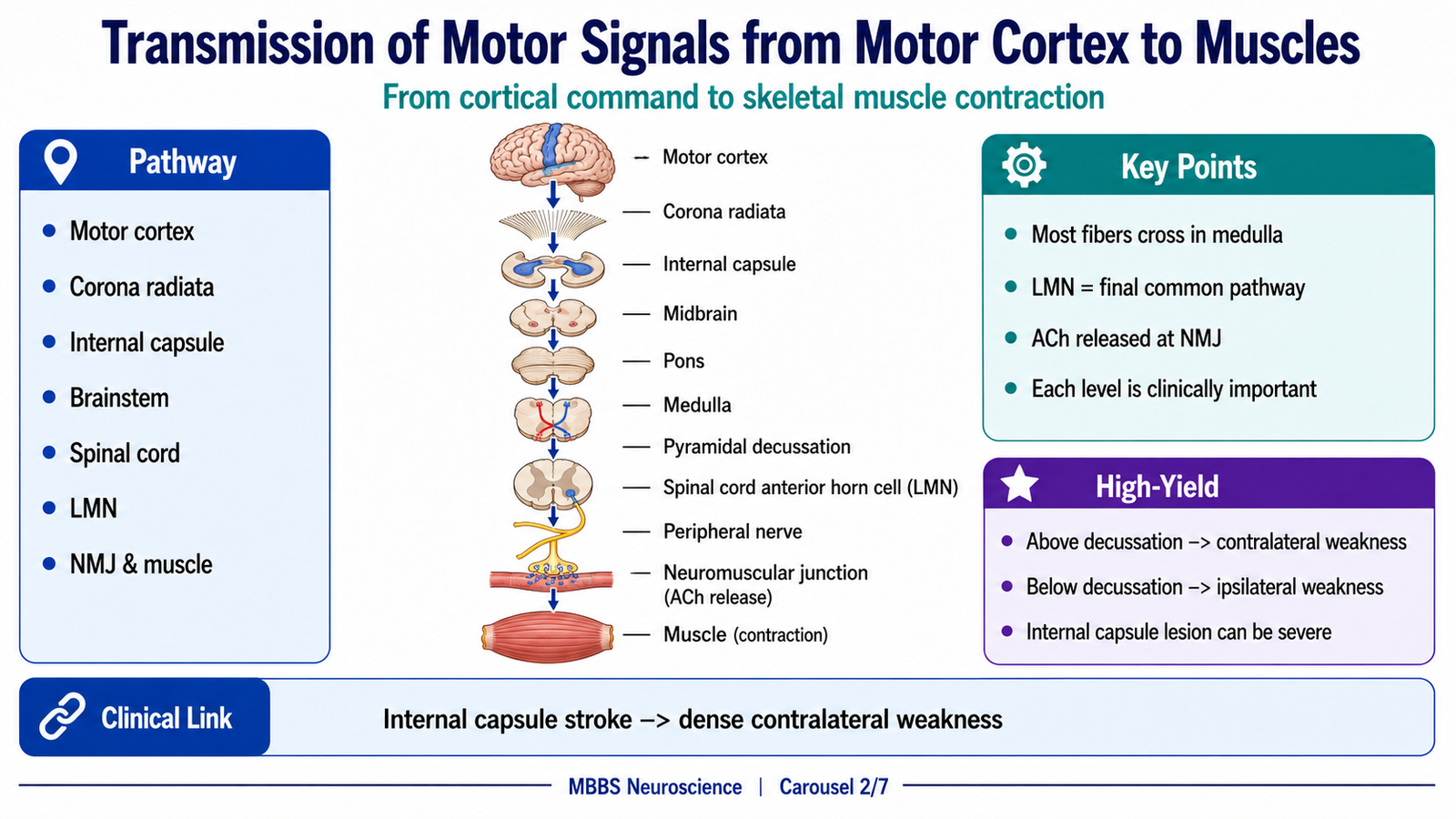
- Motor signals arise from cortical motor areas and descend through white matter pathways.
- Fibers pass through corona radiata and internal capsule.
- They descend through midbrain, pons, and medulla.
- Most corticospinal fibers cross at the pyramidal decussation.
- Descending fibers act on spinal interneurons and anterior horn motor neurons.
- Lower motor neurons directly supply skeletal muscle.
- Neuromuscular junction converts nerve impulse into muscle contraction.
🔬 CONCEPT EXPLAINED
After the motor cortex has planned and initiated a movement, the signal must reach skeletal muscle. The cerebral cortex cannot contract muscle directly. It influences lower motor neurons, which form the final common pathway to skeletal muscle.
The motor command begins mainly in pyramidal neurons of the motor cortex. Their axons descend through the corona radiata, then converge into the internal capsule. The internal capsule is very important clinically because many motor fibers are tightly packed in a small area. Therefore, a small lesion in the internal capsule can produce severe weakness of the opposite face, arm, and leg.
From the internal capsule, the fibers pass through the cerebral peduncle of the midbrain, then descend through the pons, and enter the medullary pyramids. At the lower medulla, most corticospinal fibers cross to the opposite side at the pyramidal decussation. These crossed fibers then descend in the spinal cord as the lateral corticospinal tract.
When the fibers reach the appropriate spinal cord level, they influence interneurons and anterior horn motor neurons. Interneurons are important because voluntary movement usually requires coordinated activation and inhibition of several muscle groups. For example, flexion of the elbow requires activation of biceps and relaxation of triceps. This coordination is achieved through spinal circuits under descending cortical control.
The anterior horn motor neuron then carries the final motor signal through the peripheral nerve to skeletal muscle. At the neuromuscular junction, acetylcholine is released from the motor nerve terminal. This produces depolarization of the muscle membrane, leading to excitation-contraction coupling and muscle contraction.
Therefore, voluntary movement depends on a continuous chain: cortical command → descending tract → spinal motor circuit → lower motor neuron → peripheral nerve → neuromuscular junction → muscle contraction. If any level of this chain fails, movement becomes abnormal. Cortical and descending tract lesions produce upper motor neuron signs, while anterior horn cell, peripheral nerve, neuromuscular junction, or muscle lesions produce lower motor neuron or muscular signs.
⚠️ CLINICAL IMPORTANCE
A lesion above the pyramidal decussation produces weakness on the opposite side of the body. A lesion below the decussation in the spinal cord produces weakness on the same side below the lesion. Internal capsule lesions are often severe because motor fibers are compactly arranged there.
MAJOR CONCEPTUAL HEADING 3
Pyramidal Pathway: Corticospinal and Corticobulbar Tracts
🧠 CORE
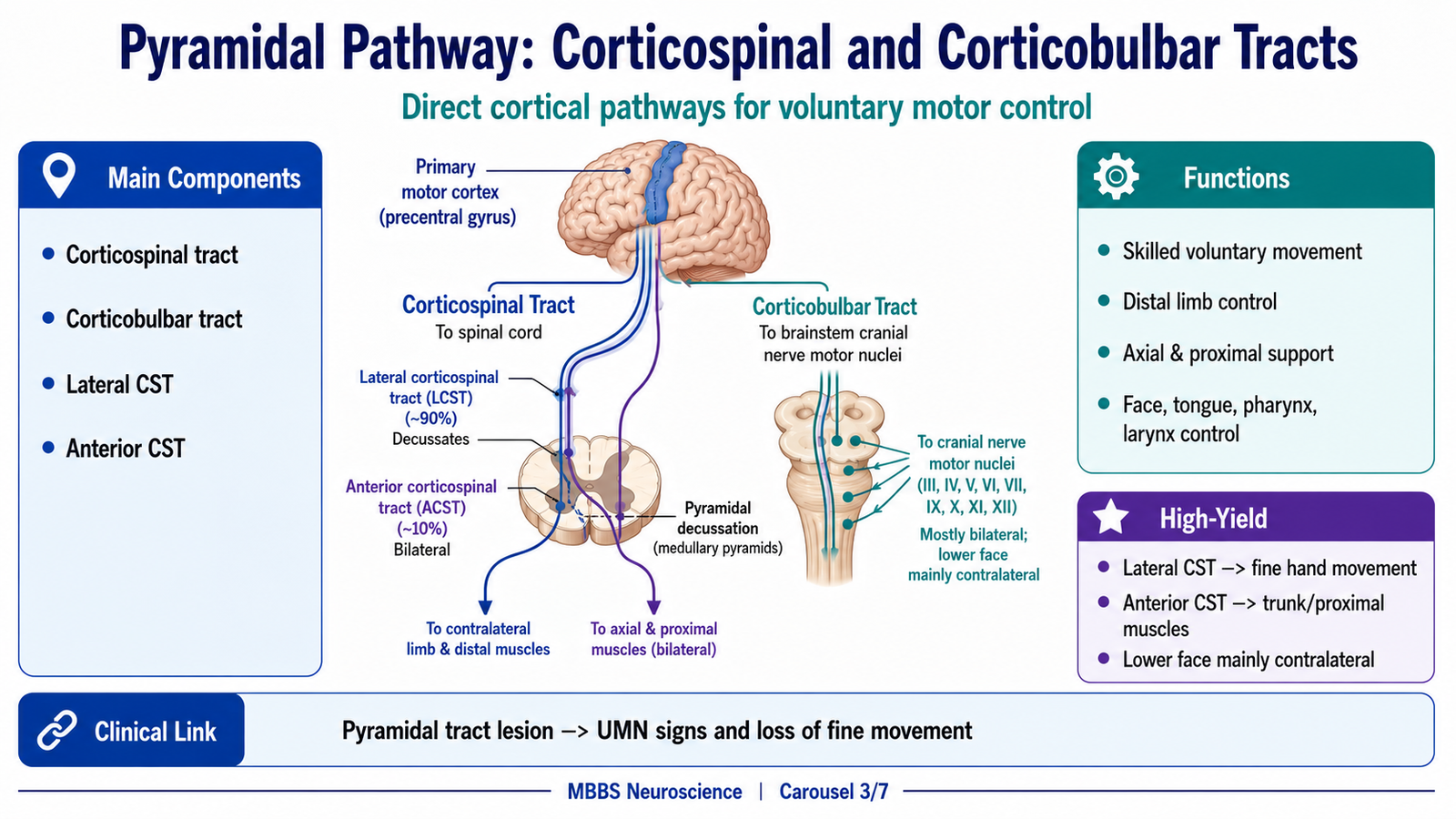
- Pyramidal pathway includes corticospinal and corticobulbar tracts.
- It arises mainly from primary motor, premotor, supplementary motor, and somatosensory areas.
- Corticospinal tract controls voluntary movements of trunk and limbs.
- Corticobulbar tract controls voluntary movements of cranial nerve motor muscles.
- Lateral corticospinal tract controls distal limb muscles and fine skilled movements.
- Anterior corticospinal tract controls axial and proximal muscles.
- Pyramidal system is essential for skilled voluntary movement.
🔬 CONCEPT EXPLAINED
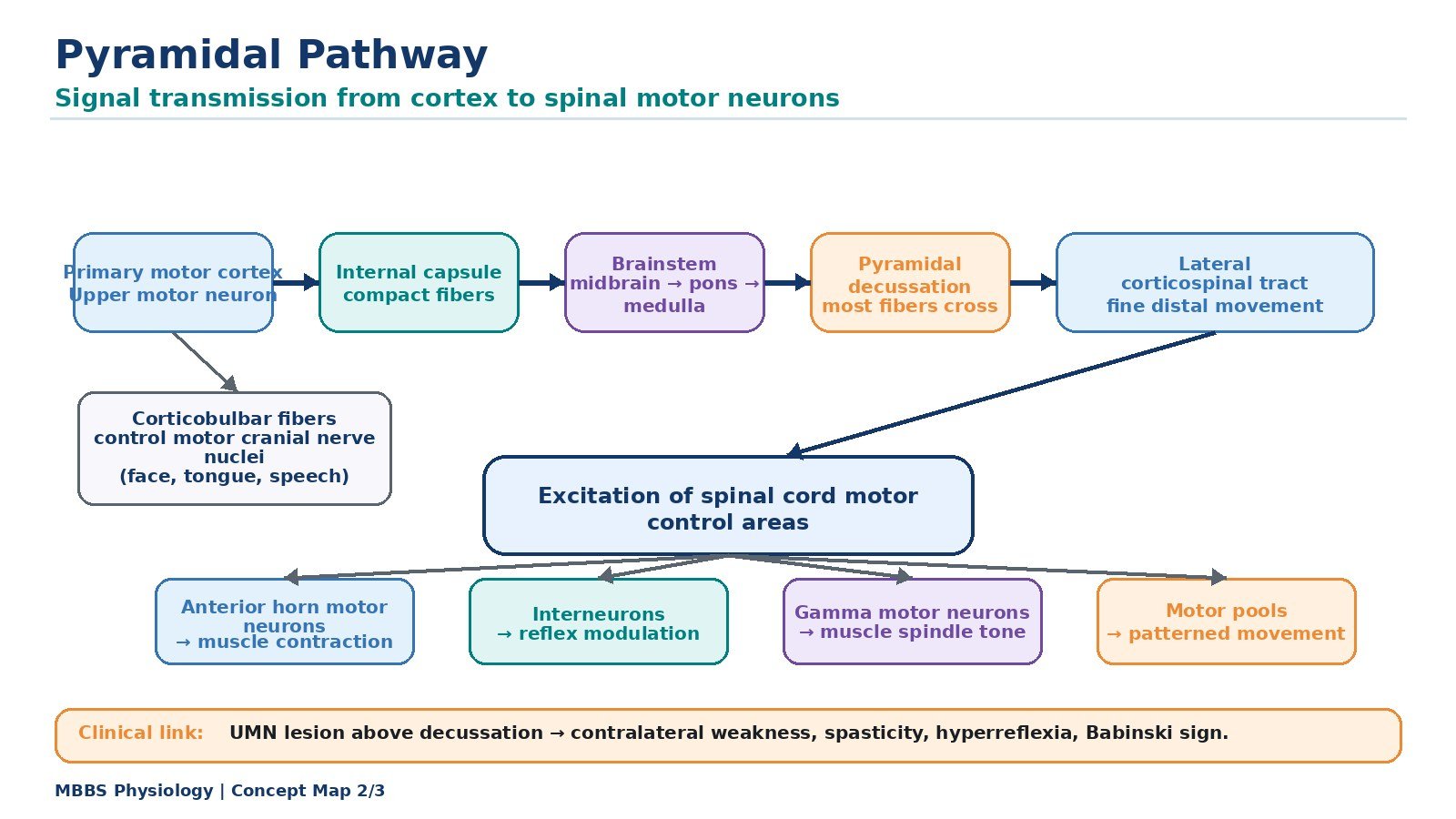
The pyramidal pathway is the major direct pathway by which the cerebral cortex controls voluntary movement. It is called pyramidal because its corticospinal fibers pass through the pyramids of the medulla. It includes two major components: the corticospinal tract and the corticobulbar tract.
The corticospinal tract carries signals from the cerebral cortex to the spinal cord. Although many fibers arise from the primary motor cortex, important contributions also come from premotor cortex, supplementary motor area, and somatosensory cortex. This mixed origin shows that voluntary movement requires both motor command and sensory guidance.
Most corticospinal fibers cross at the lower medulla. After crossing, they descend as the lateral corticospinal tract. This tract is especially important for distal limb muscles, particularly the muscles of the hand and fingers. It allows skilled, precise, independent movements such as writing, buttoning clothes, using instruments, and performing clinical skills. Because of this, corticospinal tract damage causes prominent loss of fine voluntary movement.
A smaller group of corticospinal fibers descends as the anterior corticospinal tract. These fibers are mainly involved in control of axial and proximal muscles. They often have bilateral influence, which is why trunk muscles may be less severely affected by a unilateral corticospinal lesion compared with hand muscles.
The corticobulbar tract carries motor commands from the cortex to cranial nerve motor nuclei in the brainstem. It controls muscles of the face, jaw, tongue, pharynx, larynx, and neck. These muscles are required for facial expression, chewing, swallowing, articulation, and speech. Many cranial nerve motor nuclei receive bilateral cortical innervation. However, the lower facial muscles and some tongue movements receive predominantly contralateral cortical control. This explains why an upper motor neuron facial lesion mainly affects the lower half of the opposite face, while forehead movement is relatively spared.
The pyramidal pathway exists because the body needs precise voluntary control beyond simple reflexes and posture. Spinal and brainstem systems can generate basic motor patterns, but skilled human movements require direct cortical influence. Therefore, the pyramidal pathway is the anatomical and physiological basis of fine voluntary motor control.
⚠️ CLINICAL IMPORTANCE
Damage to the pyramidal pathway produces upper motor neuron signs, including weakness, loss of fine movement, spasticity, hyperreflexia, clonus, and Babinski sign. Corticobulbar lesions may cause lower facial weakness, dysarthria, dysphagia, or tongue deviation depending on the fibers involved.
MAJOR CONCEPTUAL HEADING 4
Excitation of Spinal Motor Control Areas by Primary Motor Cortex
🧠 CORE
- Primary motor cortex activates spinal motor circuits.
- Corticospinal fibers influence interneurons and anterior horn motor neurons.
- Alpha motor neurons produce skeletal muscle contraction.
- Gamma motor neurons regulate muscle spindle sensitivity.
- Distal muscles receive strong corticospinal control.
- Cortical control regulates spinal reflex excitability.
- Spinal circuits help coordinate agonist and antagonist muscles.
🔬 CONCEPT EXPLAINED
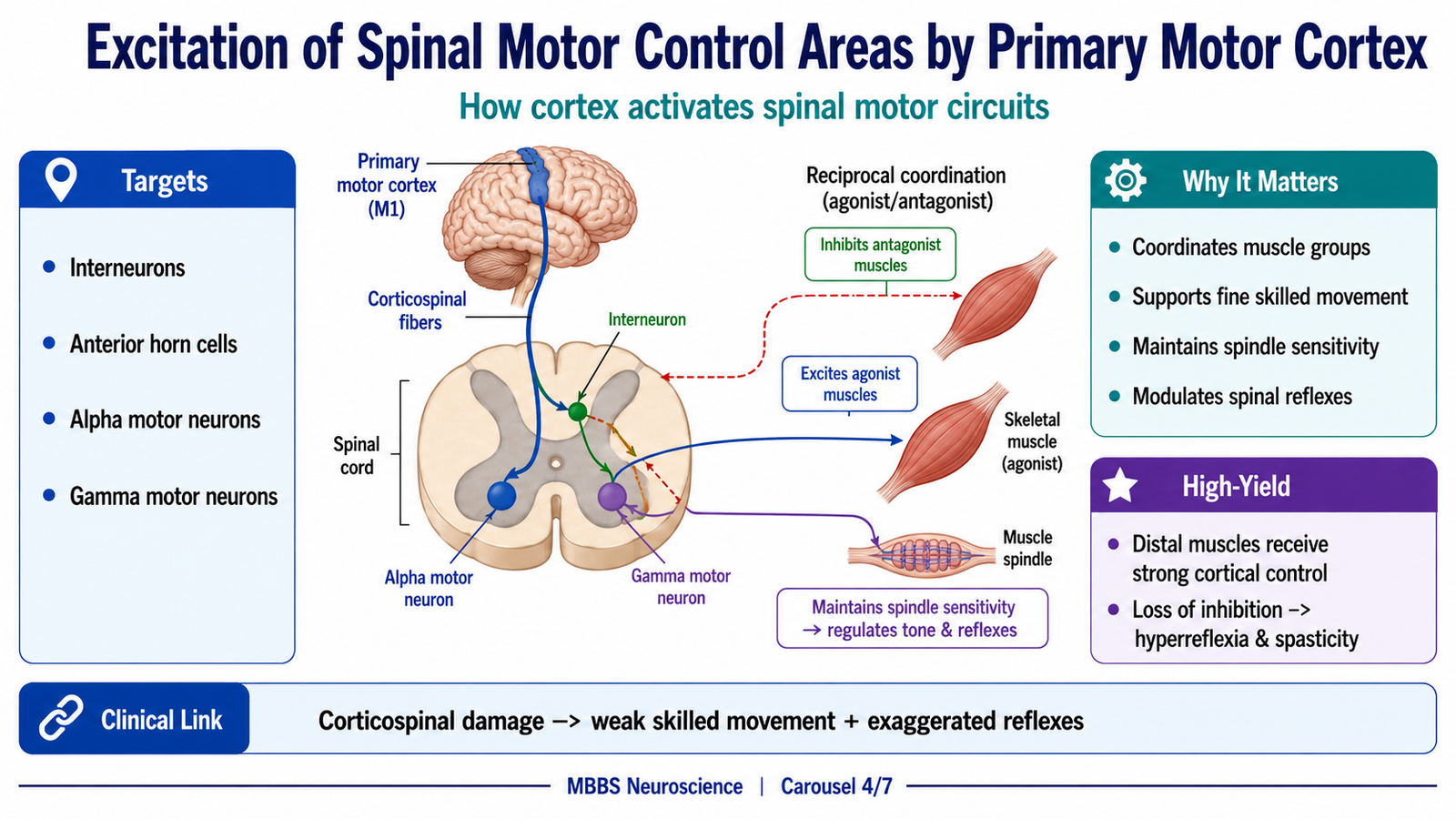
The primary motor cortex does not produce movement by acting on muscles directly. It excites and regulates spinal motor control areas. These include anterior horn motor neurons, interneurons, and reflex circuits. The spinal cord is therefore not a passive cable; it is an active motor control center that receives direction from the cortex.
When the primary motor cortex sends a command through the corticospinal tract, the fibers terminate at the appropriate spinal cord levels. Many corticospinal fibers end on interneurons. These interneurons coordinate groups of muscles so that movement becomes organized. For example, when flexor muscles contract, antagonist extensor muscles must be inhibited. This reciprocal activity is coordinated through spinal interneurons.
Some corticospinal fibers, especially those controlling fine hand movements, have more direct influence on anterior horn motor neurons. This direct corticospinal influence is important for fractionated movement, meaning the ability to move one finger separately from another. This is why corticospinal tract lesions severely affect skilled hand function.
The motor cortex also influences alpha motor neurons and gamma motor neurons. Alpha motor neurons supply extrafusal muscle fibers and produce contraction. Gamma motor neurons supply intrafusal fibers of muscle spindles and regulate spindle sensitivity. During voluntary contraction, gamma activity helps keep muscle spindles responsive, so the nervous system continues to receive accurate information about muscle length and stretch.
Another important function of cortical control is regulation of spinal reflexes. Normal descending pathways keep reflex circuits under control. They allow reflexes to support movement without becoming excessive. When upper motor neuron control is lost, spinal reflex circuits become hyperexcitable. This produces exaggerated tendon reflexes, clonus, and spasticity.
Therefore, the primary motor cortex excites spinal motor control areas in a selective and regulated way. It activates muscles needed for voluntary movement, coordinates agonist-antagonist activity, maintains sensory feedback through gamma motor control, and prevents excessive reflex activity.
⚠️ CLINICAL IMPORTANCE
Loss of cortical control over spinal motor circuits produces weakness with increased reflex activity. Fine voluntary movement is lost, especially in distal muscles. At the same time, spinal reflexes become exaggerated because descending inhibitory regulation is reduced.
MAJOR CONCEPTUAL HEADING 5
Extrapyramidal System and Functions of Descending Tracts
🧠 CORE
- Extrapyramidal system controls posture, tone, balance, and automatic movement.
- It includes basal ganglia, cerebellum, thalamus, brainstem nuclei, and descending tracts.
- Reticulospinal tracts regulate tone, posture, reflexes, and locomotor activity.
- Vestibulospinal tracts maintain balance and antigravity extensor tone.
- Tectospinal tract coordinates reflex head and neck movements.
- Extrapyramidal pathways support pyramidal voluntary movement.
- Dysfunction causes abnormal tone, posture, and involuntary movements.
🔬 CONCEPT EXPLAINED
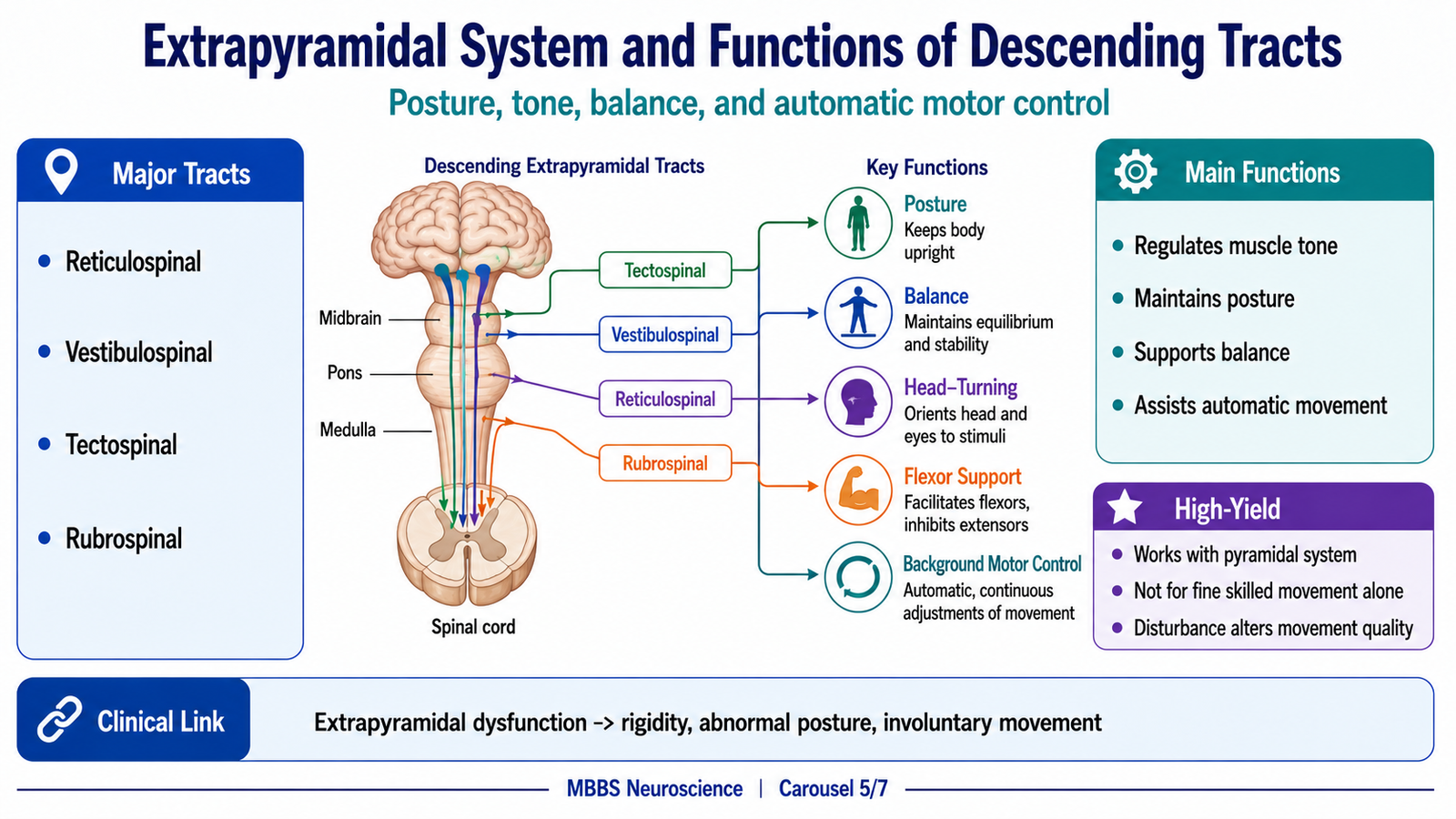
The pyramidal pathway provides skilled voluntary control, but voluntary movement cannot occur effectively unless the body has stable posture, appropriate tone, and balance. These background motor functions are mainly regulated by the extrapyramidal system.
The extrapyramidal system includes motor control circuits outside the direct corticospinal and corticobulbar pyramidal pathway. It involves the basal ganglia, cerebellum, thalamus, red nucleus, reticular formation, vestibular nuclei, and other brainstem centers. These structures influence the spinal cord through several descending tracts.
The reticulospinal tracts arise from the reticular formation of the brainstem. They regulate muscle tone, posture, spinal reflex activity, and locomotor patterns. Some reticulospinal influences facilitate extensor tone, while others inhibit excessive muscle tone. Normal movement requires a balance between facilitation and inhibition. If this balance is disturbed, tone may become abnormally increased.
The vestibulospinal tracts arise from vestibular nuclei. They are important for balance and antigravity posture. When a person stands upright, gravity tends to flex the body and make it fall. Vestibulospinal pathways activate extensor muscles that oppose gravity and help maintain posture. They also respond to changes in head position and vestibular input to prevent falling.
The tectospinal tract arises from the superior colliculus. It helps coordinate reflex turning of the head and neck in response to visual and auditory stimuli. For example, when a sudden sound or visual stimulus appears, tectospinal activity helps orient the head and eyes toward the stimulus.
The functions of descending tracts can be understood as a division of labor. The corticospinal tract controls skilled voluntary movement. The rubrospinal tract assists flexor activity. The reticulospinal tracts regulate posture, tone, and reflexes. The vestibulospinal tracts maintain balance and extensor tone. The tectospinal tract helps orient head and neck movements. These pathways work together, not separately.
For example, when a student reaches for a pen, the corticospinal tract controls hand and finger movement, reticulospinal pathways adjust tone, vestibulospinal pathways maintain balance, and sensory feedback corrects the movement. Therefore, normal movement is the result of integrated pyramidal and extrapyramidal activity.
⚠️ CLINICAL IMPORTANCE
Extrapyramidal lesions usually do not cause simple paralysis. Instead, they cause abnormal tone, posture, automatic movement, or involuntary movement. Reticulospinal imbalance contributes to spasticity. Vestibulospinal dominance contributes to extensor posturing. Basal ganglia dysfunction may produce rigidity, tremor, bradykinesia, or involuntary movements.
MAJOR CONCEPTUAL HEADING 6
Red Nucleus and Rubrospinal Control of Spinal Motor Areas
🧠 CORE
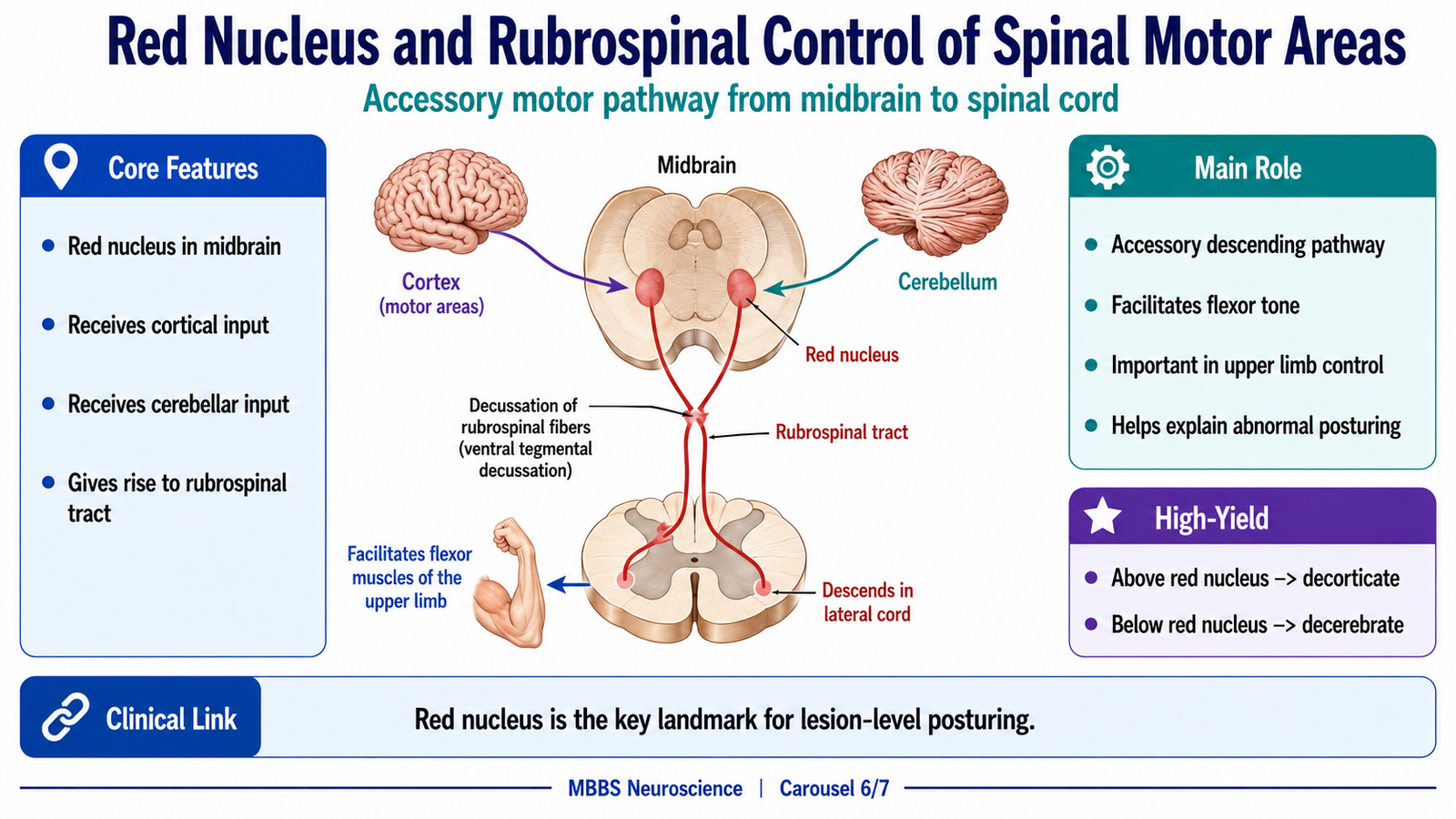
- Red nucleus is located in the midbrain.
- It receives input from motor cortex and cerebellum.
- It gives rise to the rubrospinal tract.
- Rubrospinal fibers cross and descend mainly in the lateral spinal cord.
- Rubrospinal tract facilitates flexor activity, especially in the upper limb.
- It acts as an accessory descending motor pathway.
- It is important in understanding decorticate and decerebrate rigidity.
🔬 CONCEPT EXPLAINED
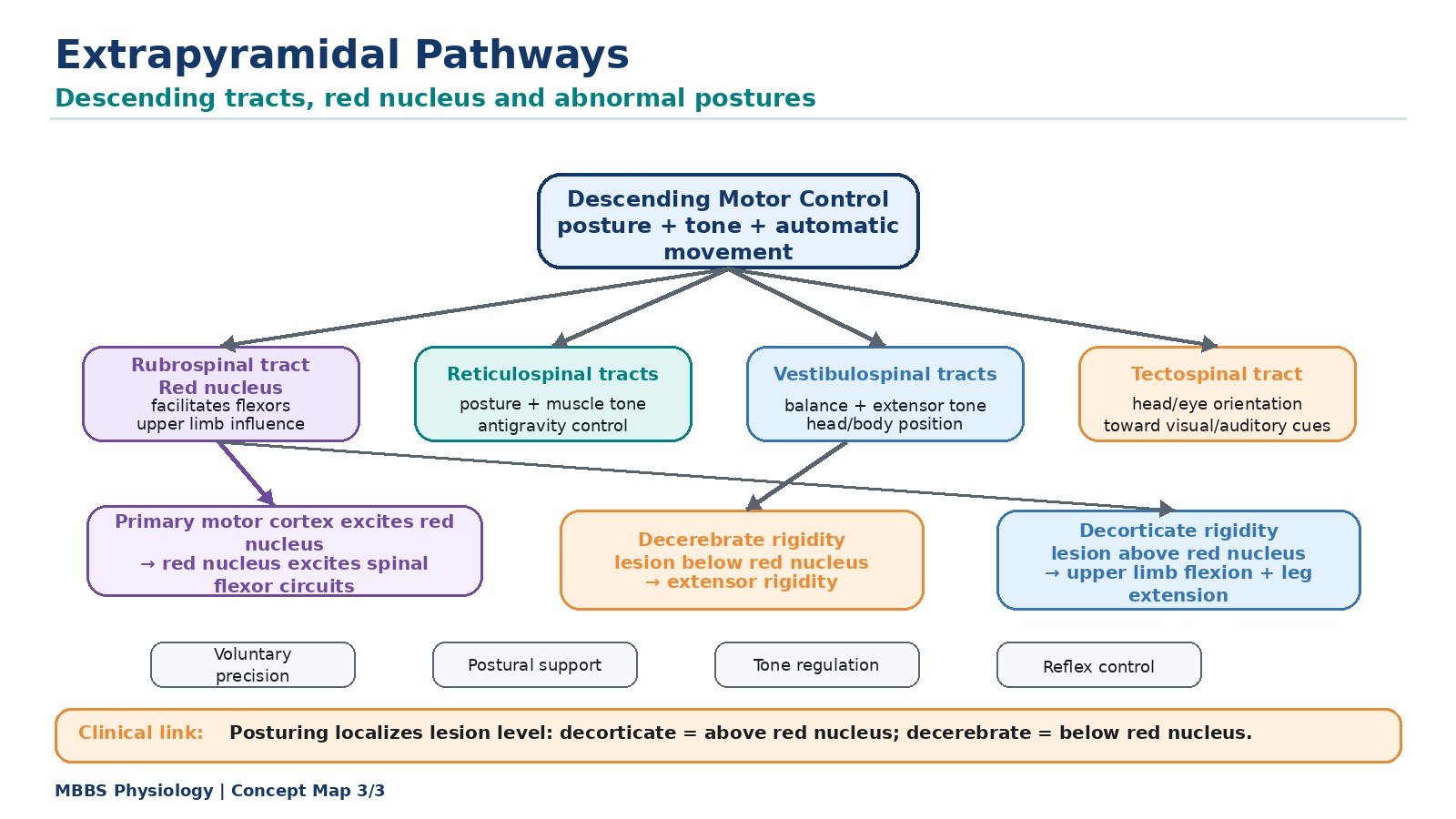
The red nucleus is an important motor nucleus in the midbrain. It forms a functional link between the cerebral cortex, cerebellum, and spinal cord. Although the corticospinal tract is the dominant voluntary motor pathway in humans, the red nucleus remains important for understanding descending motor control and abnormal posturing.
The red nucleus receives input from the motor cortex and cerebellum. It gives rise to the rubrospinal tract, which crosses shortly after origin and descends in the lateral part of the spinal cord. This tract influences spinal interneurons and motor neurons, especially those related to flexor muscle activity of the upper limb.
The rubrospinal tract provides an accessory pathway through which cortical and cerebellar signals can influence spinal motor circuits. Its role is more prominent in animals, but in humans it still contributes to motor coordination and has major clinical importance in abnormal postures.
The red nucleus becomes especially important when higher motor control is damaged. If a lesion occurs above the red nucleus, cortical control is lost but the red nucleus remains active. Its rubrospinal output continues to facilitate flexor tone, especially in the upper limb. This contributes to decorticate rigidity, where upper limbs are flexed.
If a lesion occurs at or below the level of the red nucleus, rubrospinal flexor influence is lost. In this situation, extensor pathways such as vestibulospinal and pontine reticulospinal tracts dominate. This produces decerebrate rigidity, where upper and lower limbs are extended.
Therefore, the red nucleus is not only a structure to memorize; it is a key lesion-level landmark. It helps students understand why different brain injuries produce different abnormal postures.
⚠️ CLINICAL IMPORTANCE
A lesion above the red nucleus causes decorticate posturing because rubrospinal flexor influence remains active. A lesion below the red nucleus causes decerebrate posturing because rubrospinal flexor influence is lost and extensor pathways dominate. This is a high-yield examination concept.
MAJOR CONCEPTUAL HEADING 7
Upper Motor Neuron Lesion, Decorticate Rigidity and Decerebrate Rigidity
🧠 CORE
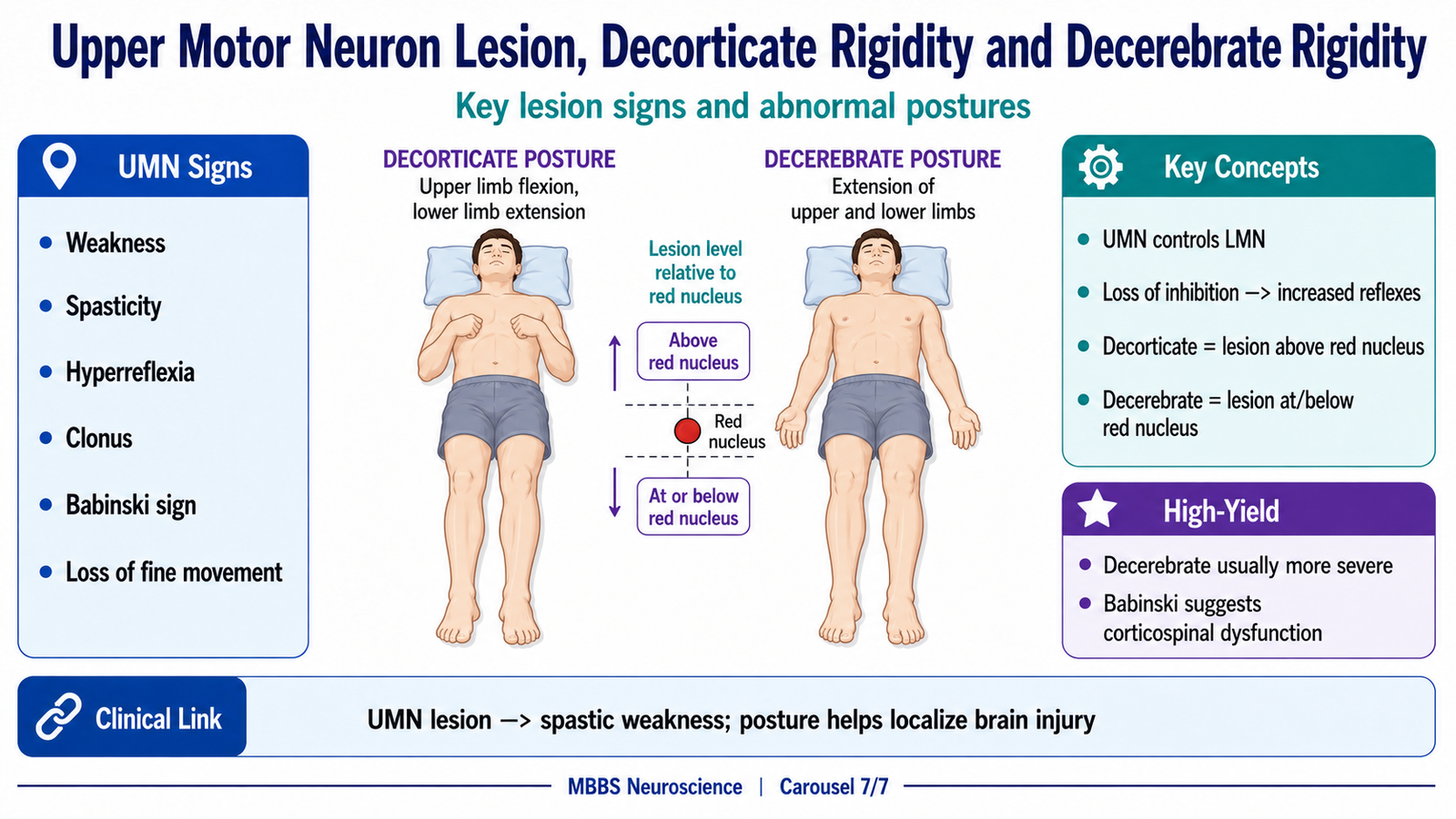
- UMNs arise from cerebral cortex and brainstem motor centers.
- UMNs control lower motor neurons directly or through interneurons.
- UMN lesions cause weakness with increased tone and increased reflexes.
- Babinski sign indicates corticospinal tract dysfunction.
- Decorticate rigidity usually indicates lesion above red nucleus.
- Decerebrate rigidity usually indicates lesion at or below red nucleus.
- Abnormal postures reflect imbalance between flexor and extensor descending pathways.
🔬 CONCEPT EXPLAINED
The upper motor neuron system includes neurons in the motor cortex and brainstem that control lower motor neurons. These pathways do not directly supply skeletal muscle. Instead, they regulate anterior horn cells and cranial nerve motor nuclei. Normal movement requires both excitation and inhibition from upper motor neurons.
When the UMN system is intact, it allows voluntary movement and keeps spinal reflexes under control. It prevents excessive reflex activity and inappropriate muscle contraction. It also allows skilled movement through corticospinal control.
When an UMN lesion occurs, two major effects appear. First, voluntary motor command is reduced, so the patient develops weakness. Second, descending inhibitory control over spinal reflex circuits is lost, so reflexes become exaggerated. This produces hyperreflexia, increased tone, clonus, and spasticity.
The weakness in UMN lesions usually affects groups of muscles rather than individual muscles. This is because the lesion affects descending motor pathways, not a single peripheral nerve. Muscle wasting is usually mild and due to disuse because the lower motor neuron connection to muscle remains intact.
A classic sign of corticospinal tract lesion is the Babinski sign. In a normal adult, stroking the lateral sole produces plantar flexion of toes. In an UMN lesion, the great toe extends and other toes may fan out. This occurs because corticospinal control over primitive spinal reflex responses is lost.
Decorticate and decerebrate rigidity are severe forms of abnormal posturing due to major brain injury. They occur because higher motor control is lost and brainstem pathways become unbalanced.
In decorticate rigidity, the lesion is usually above the red nucleus. Cortical control is lost, but the red nucleus remains active. Since the rubrospinal tract facilitates upper limb flexor tone, the upper limbs become flexed. The lower limbs are extended because extensor pathways remain active. Therefore, decorticate posture means upper limb flexion with lower limb extension.
In decerebrate rigidity, the lesion is at or below the level of the red nucleus. Rubrospinal flexor influence is lost. Vestibulospinal and pontine reticulospinal extensor influences dominate. As a result, both upper and lower limbs become extended. Therefore, decerebrate posture means extension of all limbs.
These postures are clinically important because they help localize the level of severe brain injury. Decorticate posture suggests damage above the red nucleus, while decerebrate posture suggests brainstem involvement at or below the red nucleus and is usually more serious.
⚠️ CLINICAL IMPORTANCE
UMN lesions produce weakness, spasticity, hyperreflexia, clonus, loss of fine voluntary movement, and Babinski sign. Decorticate rigidity shows upper limb flexion and lower limb extension. Decerebrate rigidity shows extension of both upper and lower limbs. The key exam concept is the relation of the lesion to the red nucleus.
⚙️ 4️⃣ Functional Flow
A. Transmission of Voluntary Motor Signal from Cortex to Muscle
- Motor intention is formed in cortical association areas.
- Premotor and supplementary motor areas plan the movement.
- Primary motor cortex generates the main voluntary motor command.
- Axons descend through corona radiata.
- Fibers converge in the internal capsule.
- Fibers pass through midbrain, pons, and medullary pyramids.
- Most corticospinal fibers cross in the lower medulla at pyramidal decussation.
- Lateral corticospinal fibers descend to the appropriate spinal cord segment.
- Corticospinal fibers excite spinal interneurons and anterior horn motor neurons.
- Lower motor neurons carry impulses through peripheral nerves.
- Acetylcholine is released at the neuromuscular junction.
- Muscle fibers depolarize and contract.
B. Mechanism of Fine Skilled Movement
- Primary motor cortex activates corticospinal neurons.
- Lateral corticospinal tract carries commands to distal limb motor circuits.
- Spinal interneurons coordinate agonist and antagonist muscles.
- Direct cortical influence helps activate selected distal motor neurons.
- Sensory feedback from joints, muscles, and skin modifies movement.
- Cerebellum adjusts timing, force, and accuracy.
- Final result is smooth, precise, fractionated movement.
C. Mechanism of Extrapyramidal Support During Movement
- Cortex initiates voluntary movement.
- Basal ganglia help select the desired motor program and suppress unwanted activity.
- Cerebellum helps correct timing and accuracy.
- Reticulospinal tracts regulate tone and posture.
- Vestibulospinal tracts maintain balance and antigravity extensor activity.
- Tectospinal tract helps orient head and neck toward sensory stimuli.
- Voluntary movement occurs on a stable postural background.
D. Mechanism of UMN Signs
- UMN pathway is damaged.
- Voluntary descending command decreases.
- Weakness develops.
- Descending inhibitory control over spinal reflexes is reduced.
- Reflex circuits become hyperexcitable.
- Deep tendon reflexes become exaggerated.
- Muscle tone increases, producing spasticity.
- Primitive plantar response appears, producing Babinski sign.
E. Mechanism of Decorticate Rigidity
- Lesion occurs above the red nucleus.
- Cortical control of descending motor pathways is lost.
- Red nucleus remains functional.
- Rubrospinal tract facilitates upper limb flexor tone.
- Extensor pathways remain active in lower limbs.
- Upper limbs flex and lower limbs extend.
F. Mechanism of Decerebrate Rigidity
- Lesion occurs at or below the red nucleus.
- Cortical control is lost.
- Rubrospinal flexor influence is also lost.
- Vestibulospinal and pontine reticulospinal extensor influences dominate.
- Extensor tone increases in upper and lower limbs.
- All limbs become extended.
🩺 5️⃣ Clinical Correlation
1. Motor Cortex Lesion
A lesion of the primary motor cortex causes weakness on the opposite side of the body. The affected body part depends on the motor homunculus. Lateral cortical lesions commonly affect face and upper limb, while medial cortical lesions affect the lower limb. Fine voluntary movement is especially impaired.
2. Internal Capsule Stroke
The internal capsule carries tightly packed corticospinal and corticobulbar fibers. Therefore, a small stroke or hemorrhage may cause severe contralateral weakness of face, arm, and leg. This is a classic example of structure-function correlation.
3. Corticospinal Tract Lesion
Corticospinal tract damage produces upper motor neuron signs below the level of lesion. These include weakness, spasticity, hyperreflexia, clonus, and Babinski sign. Fine hand movements are especially affected because distal muscles depend strongly on corticospinal control.
4. Corticobulbar Tract Lesion
Corticobulbar damage may cause lower facial weakness, dysarthria, dysphagia, or tongue movement abnormalities. Many cranial nerve nuclei receive bilateral cortical input, so unilateral lesions may produce milder deficits except in areas with mainly contralateral control.
5. Extrapyramidal Dysfunction
Extrapyramidal lesions mainly disturb movement quality rather than causing pure paralysis. Patients may develop abnormal tone, rigidity, tremor, bradykinesia, choreiform movements, or abnormal posture. These occur because posture, tone, and automatic motor control are disturbed.
6. Decorticate Rigidity
Decorticate rigidity usually indicates a lesion above the red nucleus. The upper limbs are flexed because rubrospinal flexor influence remains active. Lower limbs are extended due to extensor pathway activity. It is a sign of severe brain injury.
7. Decerebrate Rigidity
Decerebrate rigidity usually indicates lesion at or below the red nucleus. Both upper and lower limbs are extended because rubrospinal flexor influence is lost and vestibulospinal/reticulospinal extensor tone dominates. It usually suggests more serious brainstem involvement.
8. UMN versus LMN Lesion
UMN lesions produce weakness with increased tone, exaggerated reflexes, and Babinski sign. LMN lesions produce weakness with reduced tone, reduced reflexes, fasciculations, and marked wasting. This difference occurs because UMN lesions remove descending control, while LMN lesions damage the final pathway to muscle.
📌 6️⃣ Summary Points
- The primary motor cortex is located in the precentral gyrus of the frontal lobe.
- The motor homunculus represents body parts according to precision of control, not body size.
- Hands, face, lips, and tongue have large cortical representation because they need fine motor control.
- The pyramidal pathway includes corticospinal and corticobulbar tracts.
- Most corticospinal fibers cross in the lower medulla at the pyramidal decussation.
- The lateral corticospinal tract controls fine skilled movements of distal limbs.
- The corticobulbar tract controls cranial nerve motor nuclei for face, jaw, tongue, swallowing, and speech.
- Extrapyramidal pathways regulate posture, tone, balance, and automatic motor activity.
- The red nucleus gives rise to the rubrospinal tract and facilitates upper limb flexor tone.
- UMN lesions produce weakness, spasticity, hyperreflexia, clonus, and Babinski sign.
- Decorticate rigidity means upper limb flexion with lower limb extension and usually indicates lesion above the red nucleus.
- Decerebrate rigidity means extension of upper and lower limbs and usually indicates lesion at or below the red nucleus.