
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
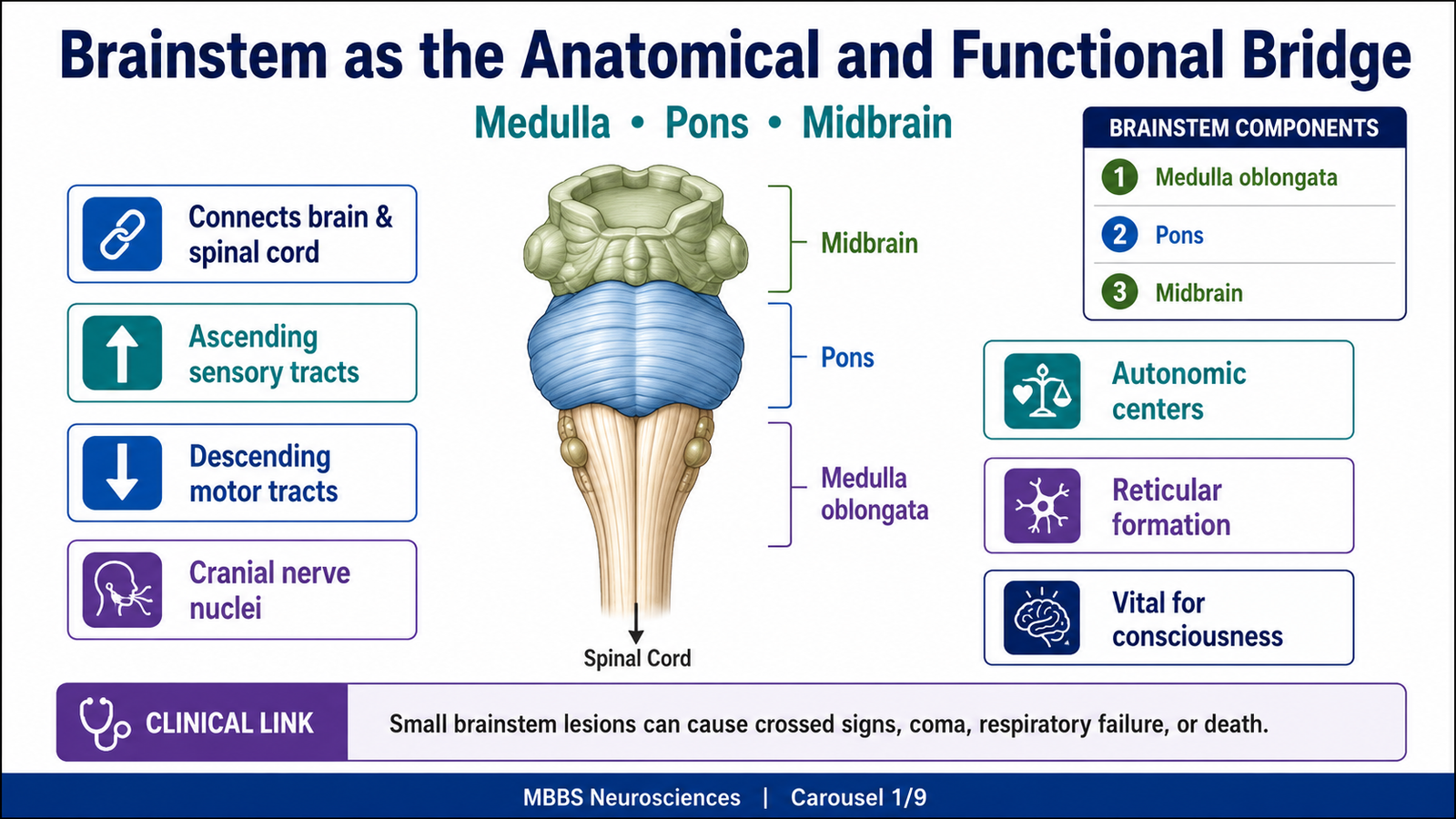
The brainstem is the stalk-like part of the brain that connects the cerebral hemispheres with the spinal cord. It lies in the posterior cranial fossa, anterior to the cerebellum, and consists of the midbrain, pons, and medulla oblongata. It is a vital region because almost all ascending sensory pathways and descending motor pathways pass through it. The brainstem also contains nuclei of most cranial nerves, making it essential for eye movements, facial movements, swallowing, hearing, balance, respiration, and cardiovascular control.
A major functional system within the brainstem is the reticular formation, especially the reticular activating system (RAS), which helps maintain wakefulness, alertness, and consciousness. Damage to the brainstem may therefore produce serious clinical conditions such as cranial nerve palsies, respiratory failure, coma, and brain death. Understanding the brainstem is clinically important because even small lesions can produce life-threatening consequences.
🔹 2️⃣ Foundation Concepts
Key Definitions
• Brainstem: The part of the brain connecting the cerebrum with the spinal cord; composed of midbrain, pons, and medulla.
• Medulla oblongata: The lowest part of the brainstem, continuous below with the spinal cord.
• Pons: The middle part of the brainstem, situated between medulla and midbrain.
• Midbrain: The upper part of the brainstem, connecting the pons with the diencephalon.
• Reticular formation: A diffuse network of neurons and fibers extending through the brainstem.
• Reticular activating system (RAS): The ascending component of the reticular formation that activates the cerebral cortex and maintains wakefulness.
• Consciousness: A state of awareness of self and environment, requiring both cortical function and brainstem activating mechanisms.
• Coma: A state of unarousable unconsciousness due to severe dysfunction of the cerebral hemispheres, brainstem RAS, or both.
• Brain death: Irreversible loss of all brain function, including brainstem function.
Essential Terminology
• Cranial nerve nuclei: Groups of neurons in the brainstem that give origin to cranial nerves or receive sensory input from them.
• Motor decussation: Crossing of corticospinal fibers in the lower medulla.
• Sensory decussation: Crossing of internal arcuate fibers from gracile and cuneate nuclei in the medulla.
• Inferior olivary nucleus: A large nucleus in the medulla involved in motor learning through cerebellar connections.
• Tegmentum: Central part of the brainstem containing cranial nerve nuclei, reticular formation, and ascending/descending tracts.
• Basilar pons: Ventral part of pons containing pontine nuclei and transverse pontocerebellar fibers.
• Colliculi: Dorsal midbrain elevations involved in visual and auditory reflexes.
Basic Overview
• The brainstem is divided into medulla, pons, and midbrain.
• It contains important ascending sensory pathways, descending motor pathways, cranial nerve nuclei, and autonomic centers.
• The medulla controls vital functions such as respiration, cardiovascular regulation, swallowing, coughing, and vomiting.
• The pons helps coordinate respiration, facial sensation, facial expression, hearing, balance, and cerebellar communication.
• The midbrain controls eye movements, visual reflexes, auditory reflexes, motor modulation, and consciousness pathways.
• The RAS keeps the cerebral cortex activated and awake.
• Brainstem injury can cause coma, respiratory arrest, cranial nerve deficits, and death.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPTUAL HEADING 1
Brainstem as the Anatomical and Functional Bridge of the Nervous System
🧠 CORE
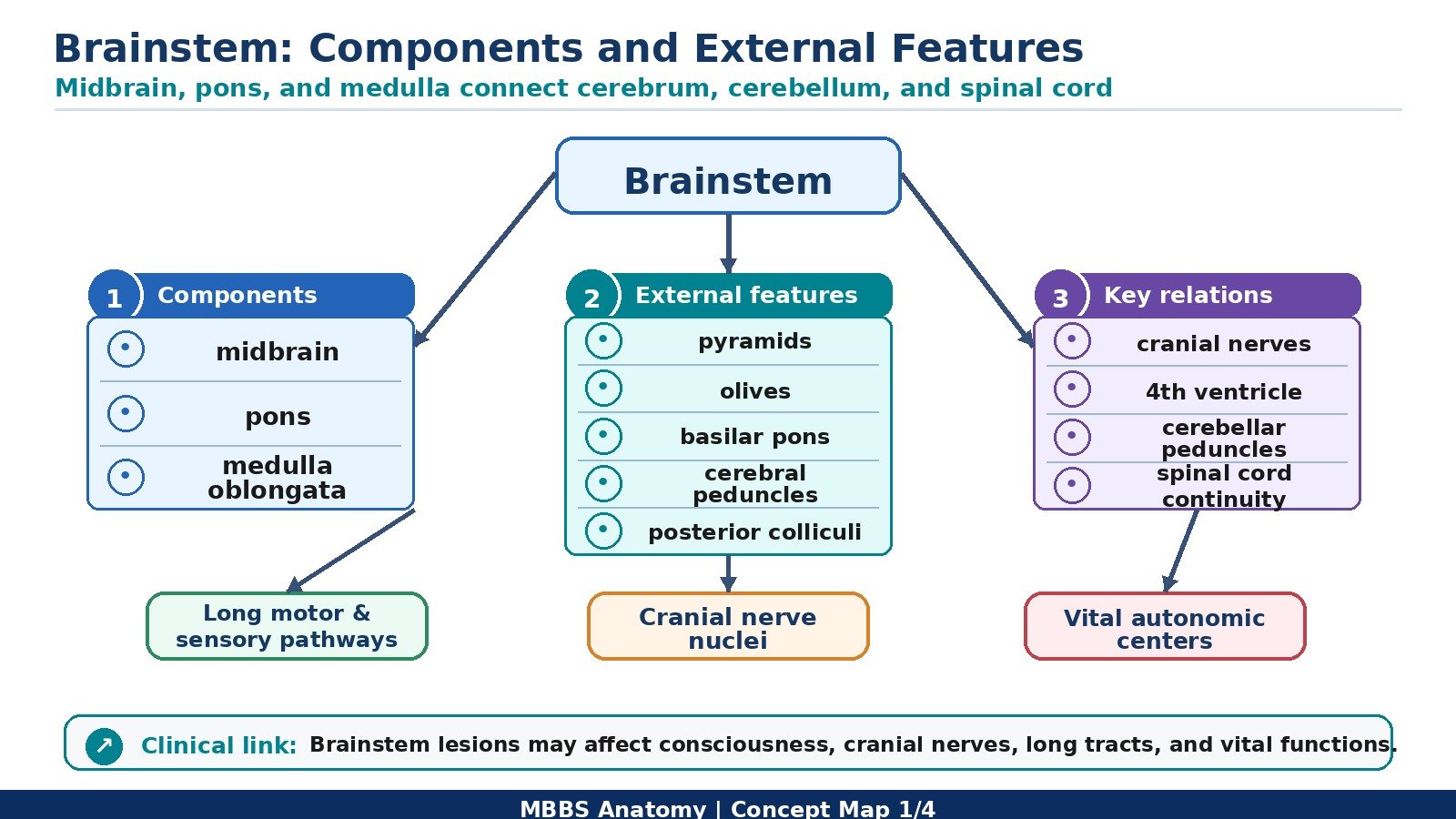
• The brainstem consists of medulla oblongata, pons, and midbrain.
• It connects the spinal cord below with the diencephalon and cerebrum above.
• It contains ascending sensory tracts and descending motor tracts.
• It contains nuclei of cranial nerves III to XII, except part of XI.
• It houses autonomic centers for respiration, cardiovascular control, swallowing, vomiting, and arousal.
• It is closely related posteriorly to the cerebellum.
• It is essential for life because it controls involuntary functions and consciousness.
🔬 CONCEPT EXPLAINED
The brainstem is the central connecting pathway between the spinal cord and higher brain centers. All major sensory information from the body must pass through the brainstem before reaching the thalamus and cerebral cortex. Similarly, most motor commands from the cerebral cortex descend through the brainstem before reaching the spinal cord and peripheral muscles. Therefore, the brainstem acts as both a conduction pathway and a processing center.
The brainstem is not simply a bundle of fibers. It contains important nuclei that control cranial nerves, autonomic functions, posture, reflexes, and arousal. Because the brainstem is compact, many important structures lie very close to each other. This explains why small lesions in the brainstem can produce multiple signs at the same time, such as cranial nerve palsy on one side and motor weakness on the opposite side.
The brainstem is divided into three parts from below upward: medulla, pons, and midbrain. The medulla continues below as the spinal cord. The pons lies above the medulla and forms a bridge between the cerebrum and cerebellum. The midbrain lies above the pons and connects the brainstem with the diencephalon.
The brainstem also contains the reticular formation, a diffuse network of neurons that extends throughout its length. This network participates in autonomic control, motor tone, pain modulation, sleep-wake regulation, and consciousness. Therefore, the brainstem is essential not only for movement and sensation, but also for survival and awareness.
⚠️ CLINICAL IMPORTANCE
Damage to the brainstem can cause severe neurological deficits because vital pathways and cranial nerve nuclei are closely packed. Lesions may produce limb weakness, sensory loss, cranial nerve palsies, abnormal respiration, coma, or death. Brainstem function is also central in the clinical diagnosis of brain death.
MAJOR CONCEPTUAL HEADING 2
External Features of the Brainstem
🧠 CORE
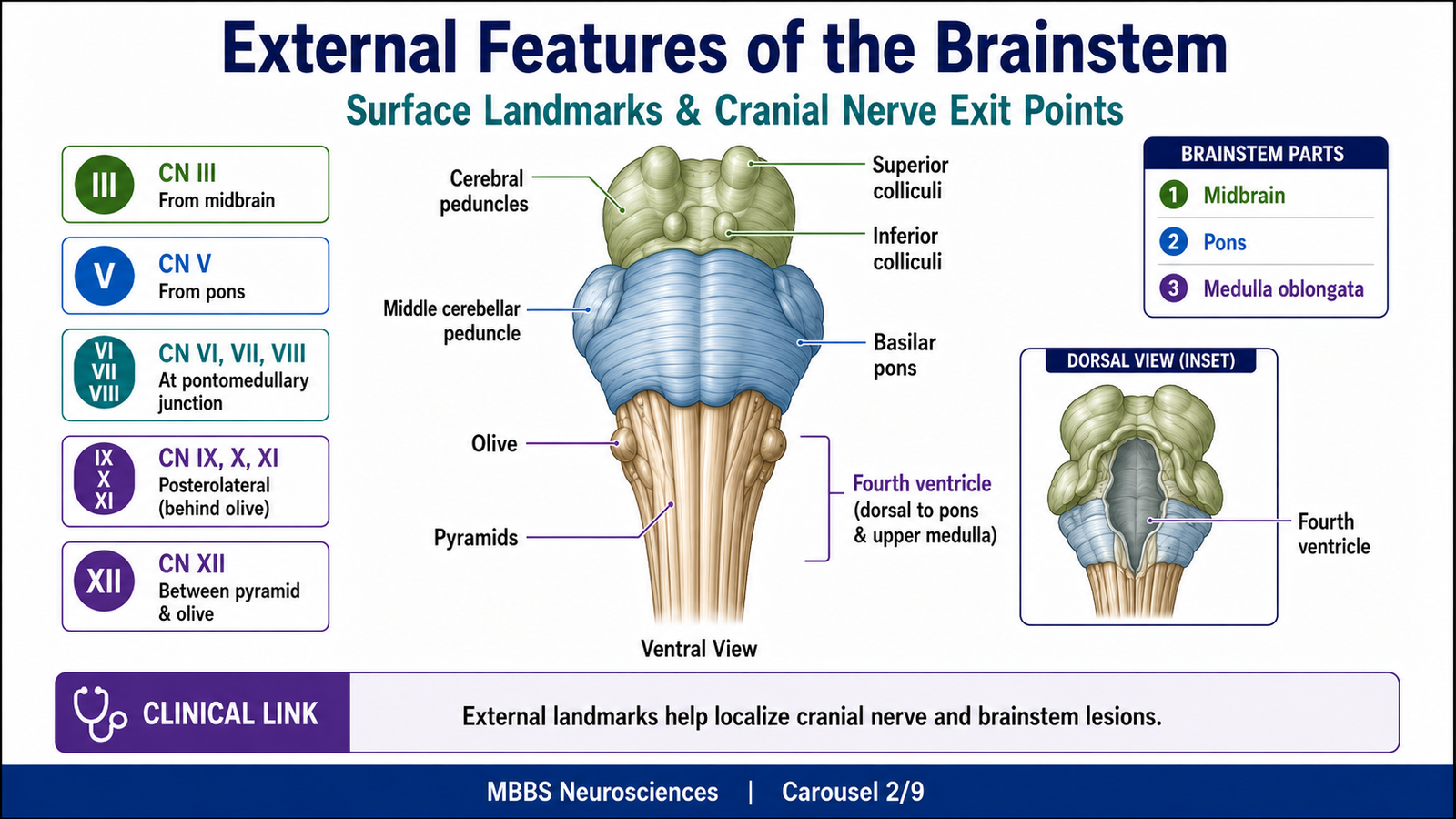
• The brainstem has ventral, dorsal, and lateral surfaces.
• The medulla shows pyramids, olives, and cranial nerve rootlets.
• The pons has a broad ventral surface with transverse fibers.
• The midbrain shows cerebral peduncles ventrally and colliculi dorsally.
• The fourth ventricle lies posterior to the pons and upper medulla.
• Cranial nerves emerge from characteristic brainstem levels.
• External landmarks help localize brainstem lesions clinically.
🔬 CONCEPT EXPLAINED
The external features of the brainstem help students understand the internal arrangement of nuclei and tracts. Since cranial nerves emerge from specific levels, external anatomy is directly linked with clinical localization.
Medulla Oblongata — External Features
The medulla is the lowest part of the brainstem. On its anterior surface, the most prominent structures are the pyramids, which contain corticospinal fibers descending from the motor cortex to the spinal cord. Near the lower medulla, many of these fibers cross to the opposite side at the pyramidal decussation. This crossing explains why lesions of one cerebral hemisphere usually affect the opposite side of the body.
Lateral to each pyramid is the olive, produced by the underlying inferior olivary nucleus. The inferior olive is connected with the cerebellum and contributes to motor coordination and motor learning.
Cranial nerve rootlets are also seen on the medulla. The hypoglossal nerve (XII) emerges between the pyramid and olive. The glossopharyngeal (IX), vagus (X), and accessory (XI) nerves emerge posterior to the olive. These nerves are related to swallowing, speech, taste, autonomic control, and movements of the pharynx and larynx.
Posteriorly, the lower medulla contains gracile and cuneate tubercles formed by underlying gracile and cuneate nuclei. These nuclei are part of the dorsal column-medial lemniscus pathway, which carries fine touch, vibration, and conscious proprioception.
Pons — External Features
The pons lies between the medulla and midbrain. Its anterior surface is broad and convex. It contains transverse pontine fibers that pass laterally into the middle cerebellar peduncle. These fibers connect the cerebral cortex with the cerebellum through pontine nuclei, helping coordinate voluntary movement.
The trigeminal nerve (V) emerges from the lateral aspect of the pons. At the pontomedullary junction, the abducens (VI), facial (VII), and vestibulocochlear (VIII) nerves emerge. These nerves are involved in eye movement, facial expression, taste, hearing, and balance.
Posteriorly, the pons forms the upper part of the floor of the fourth ventricle. This is important because cranial nerve nuclei lie beneath the floor of the fourth ventricle, so lesions in this region can affect multiple cranial nerve functions.
Midbrain — External Features
The midbrain is the shortest part of the brainstem. On its anterior surface, it contains the cerebral peduncles, which carry descending motor fibers from the cerebral cortex. Between the cerebral peduncles is the interpeduncular fossa, from which the oculomotor nerve (III) emerges.
Posteriorly, the midbrain shows four rounded elevations called the corpora quadrigemina. The upper pair are the superior colliculi, involved in visual reflexes. The lower pair are the inferior colliculi, involved in auditory reflexes. The trochlear nerve (IV) emerges from the dorsal surface of the midbrain, making it unique among cranial nerves.
⚠️ CLINICAL IMPORTANCE
External brainstem landmarks help localize lesions. For example, facial weakness with abducens palsy suggests a pontine lesion, while tongue deviation with contralateral hemiparesis suggests a medullary lesion involving the hypoglossal nerve and corticospinal tract.
MAJOR CONCEPTUAL HEADING 3
Internal Structure of the Medulla
🧠 CORE
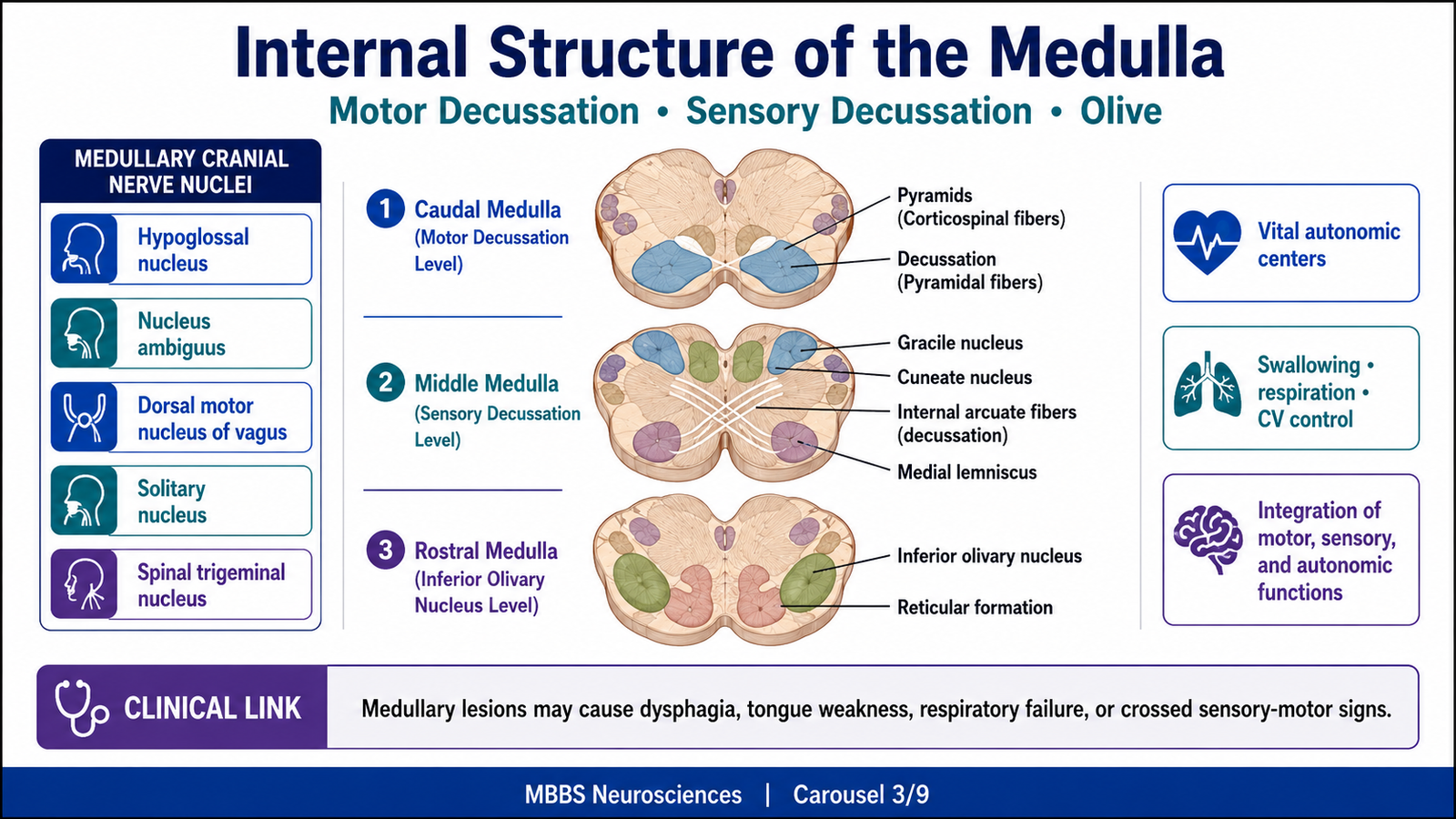
• The medulla contains ascending sensory tracts, descending motor tracts, cranial nerve nuclei, and autonomic centers.
• The lower medulla contains the motor decussation.
• The middle medulla contains the sensory decussation.
• The upper medulla contains the inferior olivary nuclei.
• Cranial nerve nuclei in the medulla are mainly related to IX, X, XI, and XII.
• The medulla controls vital autonomic functions.
• Medullary lesions can be life-threatening.
🔬 CONCEPT EXPLAINED
The medulla is continuous with the spinal cord, so its lower part resembles the spinal cord. As it ascends, the medulla becomes more complex because sensory fibers cross, motor fibers cross, cranial nerve nuclei appear, and the fourth ventricle opens posteriorly.
To understand medullary sections, it is useful to study three important levels: motor decussation, sensory decussation, and inferior olivary nucleus level.
Transverse Section of Medulla at the Level of Motor Decussation
At the lower medulla, the major event is the crossing of corticospinal fibers. These fibers descend from the motor cortex through the internal capsule, brainstem, and pyramids. At the pyramidal decussation, most corticospinal fibers cross to the opposite side and continue as the lateral corticospinal tract.
This crossing is functionally important because it explains contralateral motor control. The left motor cortex controls the right side of the body, and the right motor cortex controls the left side.
At this level, the central canal is still present posteriorly. The gray matter begins to reorganize compared with the spinal cord. The spinal nucleus and tract of the trigeminal nerve may be seen laterally, carrying pain and temperature sensation from the face.
Functional Meaning
The motor decussation exists so that each cerebral hemisphere controls skilled voluntary movement of the opposite side of the body. If this crossing is damaged, corticospinal control below the lesion is affected.
Transverse Section of Medulla at the Level of Sensory Decussation
At the next important level, the gracile nucleus and cuneate nucleus receive fibers from the dorsal columns. These nuclei process fine touch, vibration, and conscious proprioception from the body.
Neurons from these nuclei send axons that curve anteriorly and medially as internal arcuate fibers. These fibers cross the midline to form the medial lemniscus. This crossing is called the sensory decussation.
After crossing, the medial lemniscus ascends through the brainstem to the thalamus. From the thalamus, sensory information reaches the cerebral cortex for conscious perception.
Functional Meaning
The sensory decussation allows fine touch, vibration, and proprioception from one side of the body to be represented in the opposite cerebral hemisphere. Therefore, a lesion above the sensory decussation causes contralateral loss of these sensations, while a lesion below it affects the ipsilateral side.
Transverse Section of Medulla at the Level of Inferior Olivary Nuclei
At the upper medulla, the most prominent structure is the inferior olivary nucleus. It appears as a folded gray matter mass and produces the external swelling called the olive. The inferior olive sends fibers to the cerebellum through the inferior cerebellar peduncle.
The inferior olivary nucleus helps in motor coordination and motor learning. It does not directly initiate movement but provides information to the cerebellum so that movements can be adjusted and refined.
At this level, the fourth ventricle is present posteriorly. Important cranial nerve nuclei are arranged in the tegmentum. The pyramids remain anteriorly, carrying corticospinal fibers. The medial lemniscus continues to ascend. The reticular formation occupies the central region.
Cranial Nerve Nuclei Present Within the Medulla
The medulla contains nuclei related mainly to cranial nerves IX, X, XI, and XII, with some components of V and VIII.
Hypoglossal Nucleus
The hypoglossal nucleus gives motor fibers to the tongue. It controls tongue movements required for speech, swallowing, and manipulation of food.
Damage causes ipsilateral tongue weakness. On protrusion, the tongue deviates toward the side of the lesion because the normal genioglossus muscle pushes the tongue toward the weak side.
Dorsal Motor Nucleus of Vagus
This nucleus provides parasympathetic output through the vagus nerve to thoracic and abdominal organs. It contributes to autonomic regulation of heart rate, gastrointestinal motility, and visceral function.
Nucleus Ambiguus
The nucleus ambiguus gives motor fibers through IX and X to muscles of the pharynx, larynx, and soft palate. It is essential for swallowing, phonation, and gag reflex.
Damage may cause dysphagia, hoarseness of voice, nasal regurgitation, and loss of gag reflex.
Solitary Nucleus
The solitary nucleus receives taste sensation from cranial nerves VII, IX, and X and visceral sensory input from IX and X. It plays an important role in reflex control of cardiovascular, respiratory, and digestive functions.
Spinal Nucleus of Trigeminal Nerve
This nucleus receives pain and temperature sensation from the face. It extends down into the medulla and upper cervical spinal cord.
Vestibular Nuclei
Vestibular nuclei are located partly in the medulla and partly in the pons. They receive input related to balance and head position.
⚠️ CLINICAL IMPORTANCE
Medullary lesions may affect respiration, blood pressure, swallowing, speech, and tongue movement. Lateral medullary syndrome classically affects swallowing, facial pain-temperature sensation, body pain-temperature sensation, vestibular function, and cerebellar coordination. Even small medullary lesions can be dangerous because vital autonomic centers are located here.
MAJOR CONCEPTUAL HEADING 4
Internal Structure of the Pons
🧠 CORE
• The pons is divided into ventral basilar pons and dorsal tegmentum.
• It contains pontine nuclei and transverse pontocerebellar fibers.
• It connects the cerebral cortex with the cerebellum.
• Cranial nerve nuclei in the pons are related to V, VI, VII, and VIII.
• The caudal pons contains facial and abducens nerve nuclei.
• The cranial pons contains trigeminal nuclei and pontine respiratory centers.
• Pontine lesions affect facial sensation, facial movement, eye movement, hearing, balance, and respiration.
🔬 CONCEPT EXPLAINED
The pons is named because it acts as a bridge. Structurally, it connects the cerebral cortex with the cerebellum through pontine nuclei and transverse fibers. Functionally, it helps integrate motor commands with cerebellar coordination. It also contains cranial nerve nuclei involved in facial sensation, facial expression, lateral eye movement, hearing, and balance.
The pons has two major parts: the basilar part anteriorly and the tegmentum posteriorly. The basilar part contains descending corticospinal, corticobulbar, and corticopontine fibers, along with pontine nuclei. The pontine nuclei receive cortical input and send fibers across the midline into the cerebellum through the middle cerebellar peduncle. This pathway allows the cerebellum to compare intended movement with actual movement and improve coordination.
The tegmentum contains cranial nerve nuclei, reticular formation, ascending sensory pathways, and descending fibers.
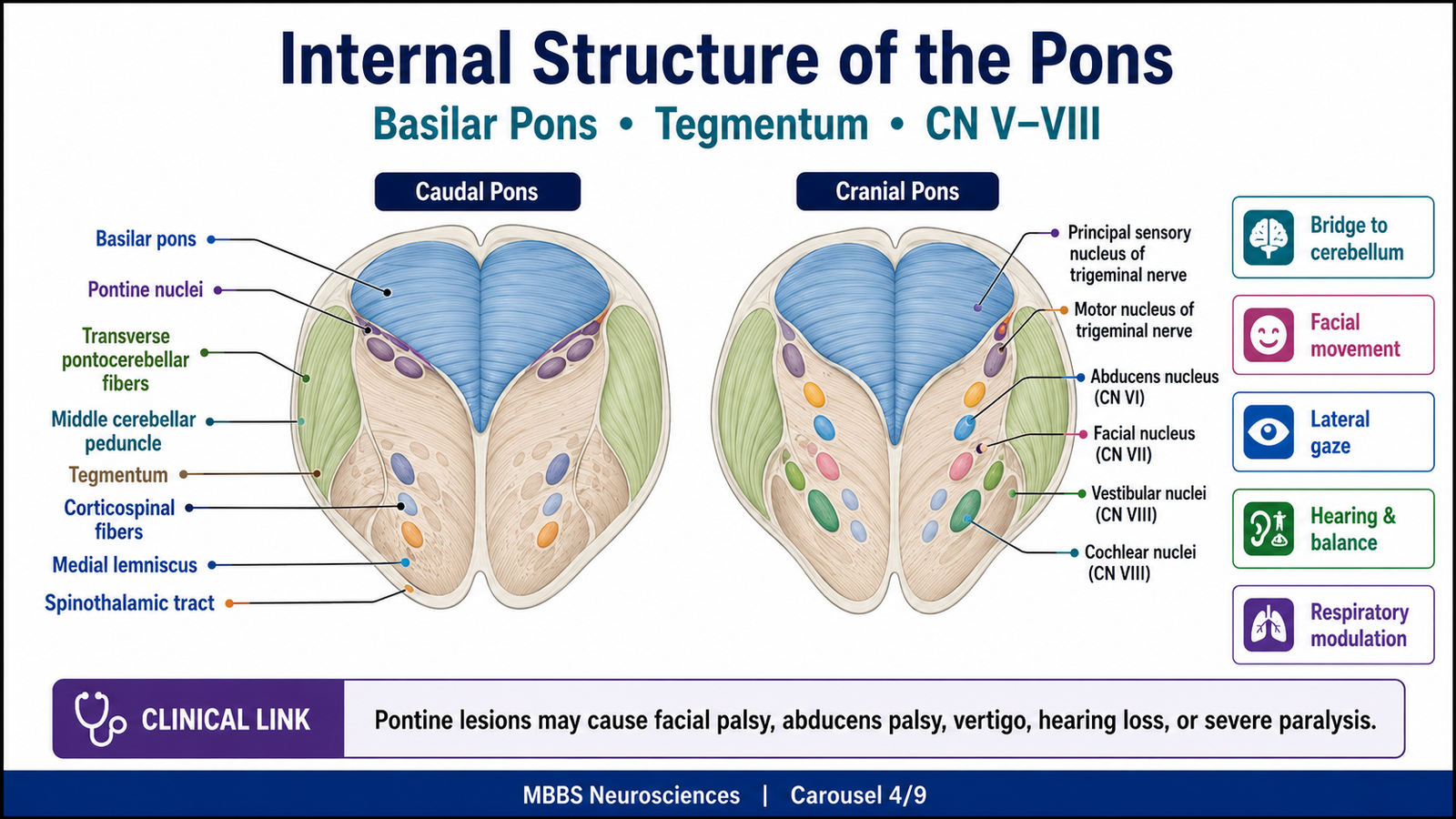
Transverse Section of Pons at Caudal Level
The caudal pons contains important nuclei related to the abducens and facial nerves.
The abducens nucleus lies near the floor of the fourth ventricle and controls the lateral rectus muscle, which abducts the eye. Close to it, facial nerve fibers loop around the abducens nucleus, forming the facial colliculus. This close relationship explains why lesions in the dorsal caudal pons may produce both abducens palsy and facial weakness.
The facial motor nucleus supplies muscles of facial expression. The superior salivatory nucleus provides parasympathetic fibers related to lacrimal, submandibular, and sublingual glands. The vestibular and cochlear nuclei are located near the pontomedullary junction and receive information related to balance and hearing.
The caudal pons also contains the medial lemniscus, spinothalamic tract, corticospinal fibers, and reticular formation.
Transverse Section of Pons at Cranial Level
The cranial pons contains nuclei related mainly to the trigeminal nerve. The principal sensory nucleus of trigeminal nerve receives touch sensation from the face. The motor nucleus of trigeminal nerve supplies muscles of mastication.
The basilar part remains prominent and contains pontine nuclei and transverse pontocerebellar fibers. These fibers continue to connect cortical motor planning areas with the cerebellum.
The cranial pons also participates in respiratory regulation. Pontine centers modify the rhythm generated by medullary respiratory centers, helping produce smooth breathing transitions between inspiration and expiration.
Cranial Nerve Nuclei Present Within the Pons
Trigeminal Nuclei
The trigeminal nerve has sensory and motor nuclei. Its sensory nuclei receive touch, pain, temperature, and proprioceptive information from the face. Its motor nucleus supplies muscles of mastication.
Abducens Nucleus
The abducens nucleus controls the lateral rectus muscle. It is essential for lateral gaze. Damage causes inability to abduct the ipsilateral eye.
Facial Nucleus
The facial nucleus supplies muscles of facial expression. Damage produces ipsilateral lower motor neuron facial paralysis.
Vestibular and Cochlear Nuclei
These nuclei are related to balance and hearing. Vestibular nuclei receive information from the semicircular canals, utricle, and saccule. Cochlear nuclei receive auditory input from the cochlea.
⚠️ CLINICAL IMPORTANCE
Pontine lesions may cause facial paralysis, impaired lateral gaze, loss of facial sensation, hearing loss, vertigo, ataxia, and respiratory disturbances. Large ventral pontine lesions can damage corticospinal tracts and produce severe paralysis while consciousness may be preserved if the RAS is spared, as in locked-in syndrome.
![]()
MAJOR CONCEPTUAL HEADING 5
Internal Structure of the Midbrain
🧠 CORE
• The midbrain lies between the pons and diencephalon.
• It contains tectum, tegmentum, and cerebral peduncles.
• The superior colliculus is related to visual reflexes.
• The inferior colliculus is related to auditory reflexes.
• Cranial nerve nuclei III and IV are located in the midbrain.
• The red nucleus and substantia nigra participate in motor control.
• The midbrain contains ascending RAS pathways important for consciousness.
🔬 CONCEPT EXPLAINED
The midbrain is the uppermost part of the brainstem. Although small, it contains important structures for eye movements, visual and auditory reflexes, motor control, and consciousness.
The dorsal part of the midbrain is called the tectum and contains the superior and inferior colliculi. The central region is the tegmentum, containing cranial nerve nuclei, red nucleus, reticular formation, and ascending sensory pathways. The anterior part contains the cerebral peduncles, which carry descending motor fibers.
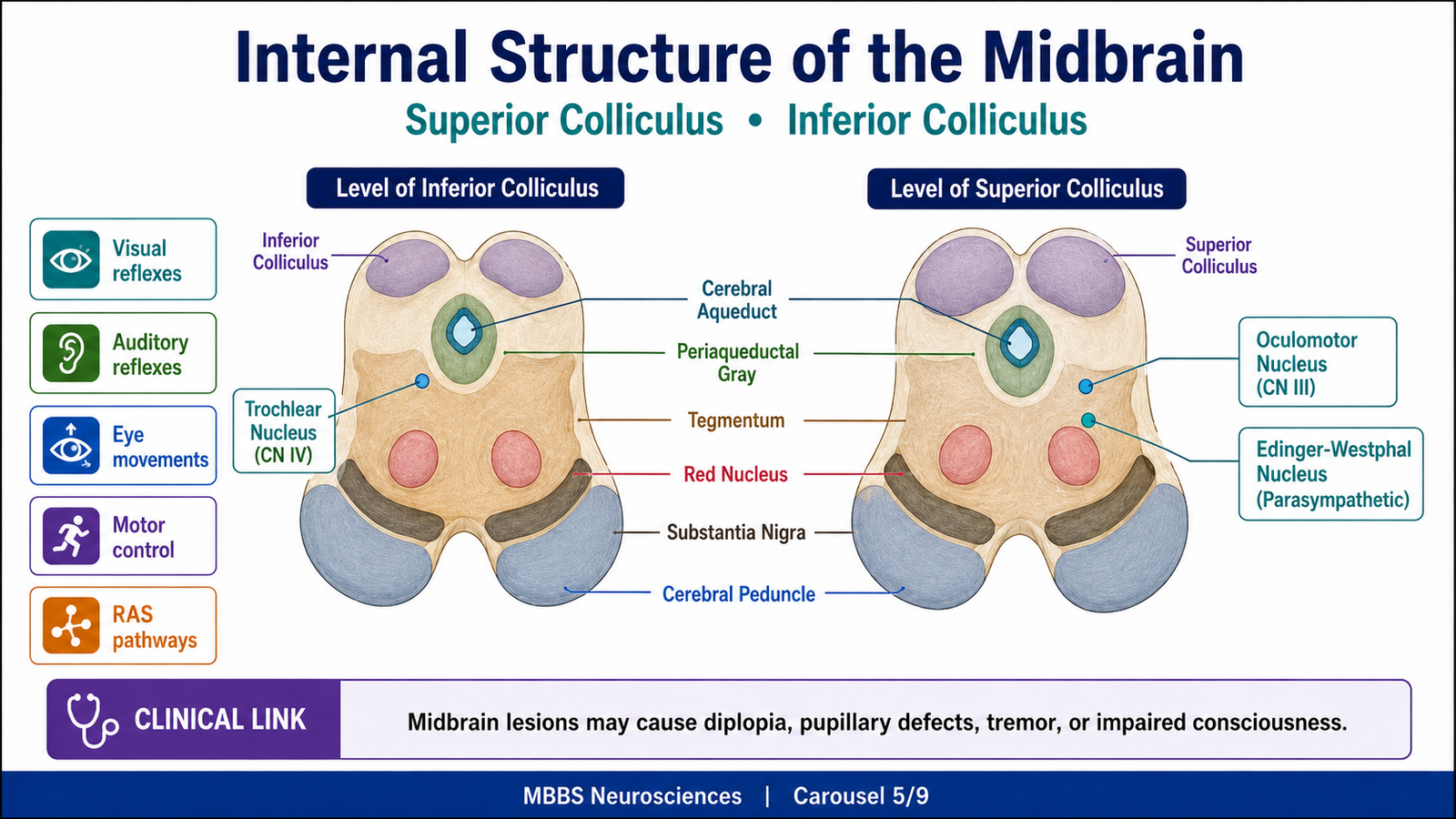
Transverse Section of Midbrain at the Level of Inferior Colliculus
The inferior colliculus is part of the auditory pathway. It receives auditory information from lower brainstem nuclei and helps coordinate reflex responses to sound. For example, sudden loud sounds can produce reflex orientation of the head and eyes.
At this level, the trochlear nucleus is present. The trochlear nerve supplies the superior oblique muscle of the eye. It is unique because it emerges from the dorsal surface of the brainstem and crosses before exiting.
The cerebral aqueduct passes through the midbrain and connects the third and fourth ventricles. Around it is periaqueductal gray matter, which participates in pain modulation and defensive responses.
Transverse Section of Midbrain at the Level of Superior Colliculus
The superior colliculus is involved in visual reflexes, especially reflex movements of the eyes and head toward visual stimuli. It receives visual input and coordinates responses through connections with eye movement nuclei.
At this level, the oculomotor nucleus and Edinger-Westphal nucleus are present. The oculomotor nucleus supplies most extraocular muscles and levator palpebrae superioris. The Edinger-Westphal nucleus provides parasympathetic fibers for pupillary constriction and accommodation.
The red nucleus is also prominent at this level. It is involved in motor coordination through connections with the cerebellum and spinal cord. The substantia nigra lies ventrally and is involved in motor control through dopaminergic connections with the basal ganglia.
Major Midbrain Structures and Their Functional Meaning
Superior Colliculus
The superior colliculus helps coordinate visual reflexes. It allows rapid orientation of the eyes and head toward visual stimuli.
Inferior Colliculus
The inferior colliculus participates in auditory reflex pathways and sound localization.
Oculomotor Nucleus
The oculomotor nucleus controls most eye movements. Damage causes ptosis, lateral deviation of the eye, diplopia, and impaired pupillary reflex if parasympathetic fibers are involved.
Trochlear Nucleus
The trochlear nucleus controls the superior oblique muscle. Damage produces vertical diplopia, especially when looking downward.
Red Nucleus
The red nucleus participates in motor coordination. It is functionally linked with cerebellar motor control.
Substantia Nigra
The substantia nigra provides dopaminergic input to basal ganglia circuits. Its degeneration is classically associated with Parkinsonian motor features, although detailed pathology is studied later.
⚠️ CLINICAL IMPORTANCE
Midbrain lesions can produce eye movement abnormalities, pupillary defects, tremor, rigidity, auditory or visual reflex impairment, and altered consciousness. Because ascending RAS fibers pass through the midbrain, midbrain damage may cause coma.
MAJOR CONCEPTUAL HEADING 6
Cranial Nerve Nuclei of the Brainstem: Functional Organization
🧠 CORE
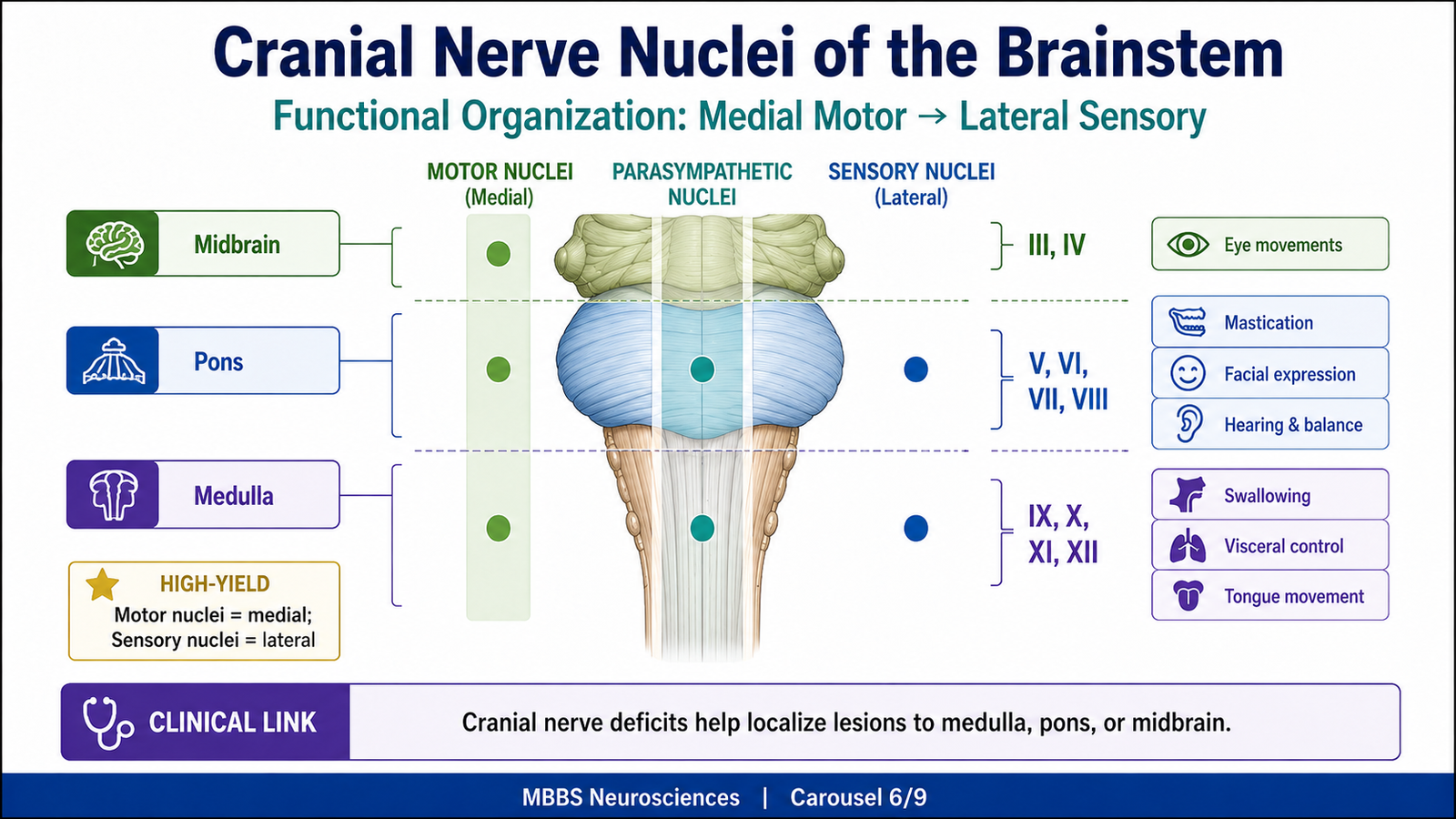
• Cranial nerve nuclei are arranged in functional columns.
• Motor nuclei tend to lie medially.
• Sensory nuclei tend to lie laterally.
• Autonomic parasympathetic nuclei lie between motor and sensory regions.
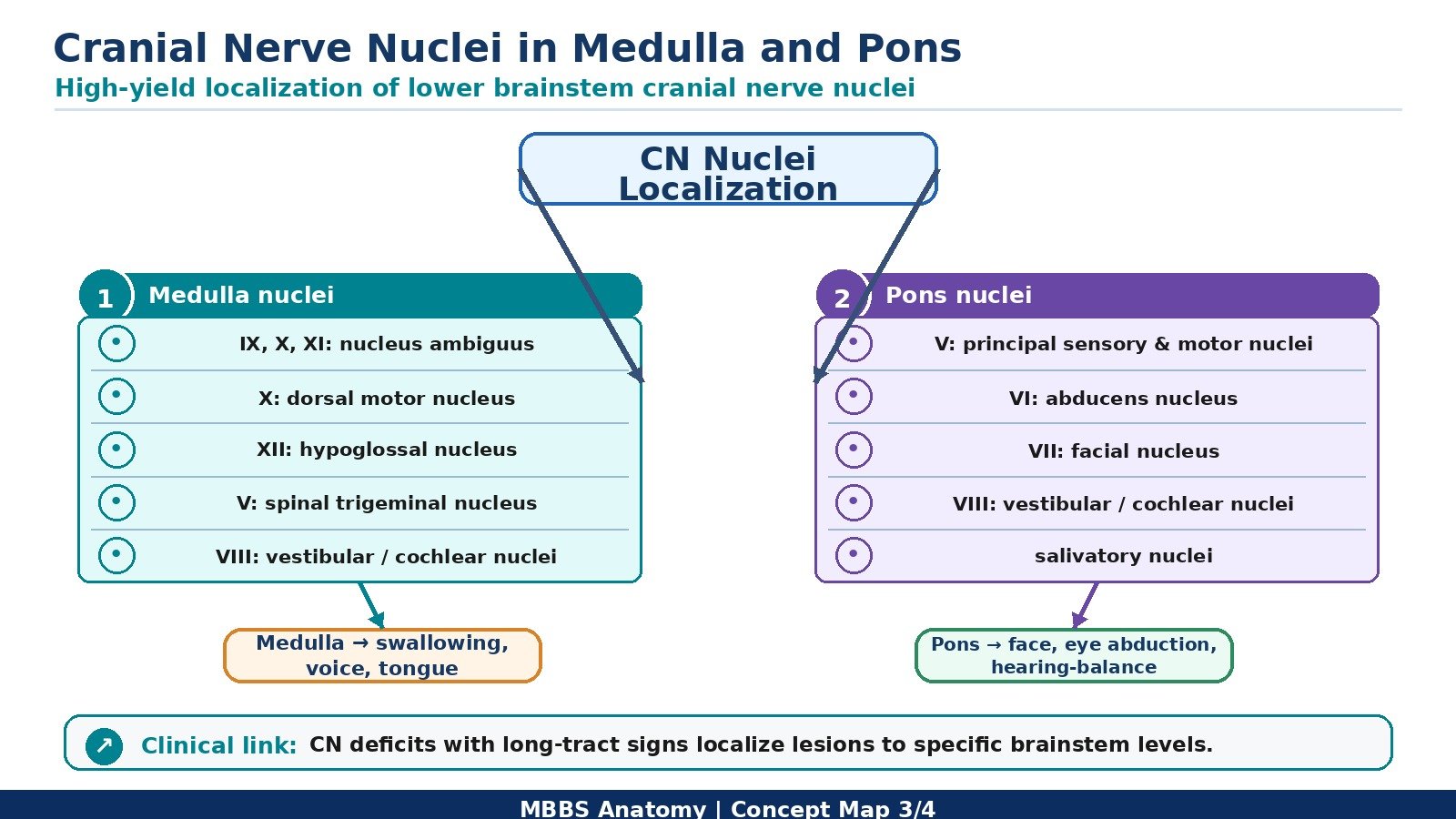
• Medulla contains nuclei mainly for IX, X, XI, and XII.
• Pons contains nuclei mainly for V, VI, VII, and VIII.
• Midbrain contains nuclei mainly for III and IV.
• This arrangement helps localize brainstem lesions.
🔬 CONCEPT EXPLAINED
The cranial nerve nuclei of the brainstem are arranged according to function. During development, the opening of the fourth ventricle spreads the alar plate laterally and keeps the basal plate medially. As a result, motor nuclei are found more medially, sensory nuclei more laterally, and autonomic nuclei between them.
This arrangement is clinically useful. If a lesion affects the medial brainstem, motor cranial nerve nuclei and corticospinal pathways are more likely to be involved. If a lesion affects the lateral brainstem, sensory nuclei, vestibular nuclei, cerebellar connections, and spinothalamic pathways may be affected.
Motor nuclei supply skeletal muscles derived from somites or branchial arches. Sensory nuclei receive information from the face, special senses, taste, and viscera. Parasympathetic nuclei control glands, smooth muscle, and visceral organs.
The brainstem therefore acts as the central control station for cranial nerve functions such as eye movements, chewing, facial expression, hearing, balance, swallowing, tongue movement, voice, taste, and visceral reflexes.
⚠️ CLINICAL IMPORTANCE
Cranial nerve nuclear involvement helps localize lesions to specific brainstem levels. For example, oculomotor palsy suggests midbrain involvement, facial and abducens palsy suggest pontine involvement, and hypoglossal or vagal signs suggest medullary involvement.
MAJOR CONCEPTUAL HEADING 7
Involuntary Functions of the Brainstem
🧠 CORE
• The brainstem controls vital involuntary functions necessary for survival.
• Medullary centers regulate respiration, cardiovascular activity, swallowing, vomiting, coughing, and sneezing.
• Pontine centers help regulate breathing rhythm.
• Brainstem reflexes protect the airway and maintain homeostasis.
• Autonomic nuclei of cranial nerves participate in parasympathetic control.
• Reticular formation coordinates autonomic, motor, and arousal responses.
• Failure of brainstem involuntary functions can cause death.
🔬 CONCEPT EXPLAINED
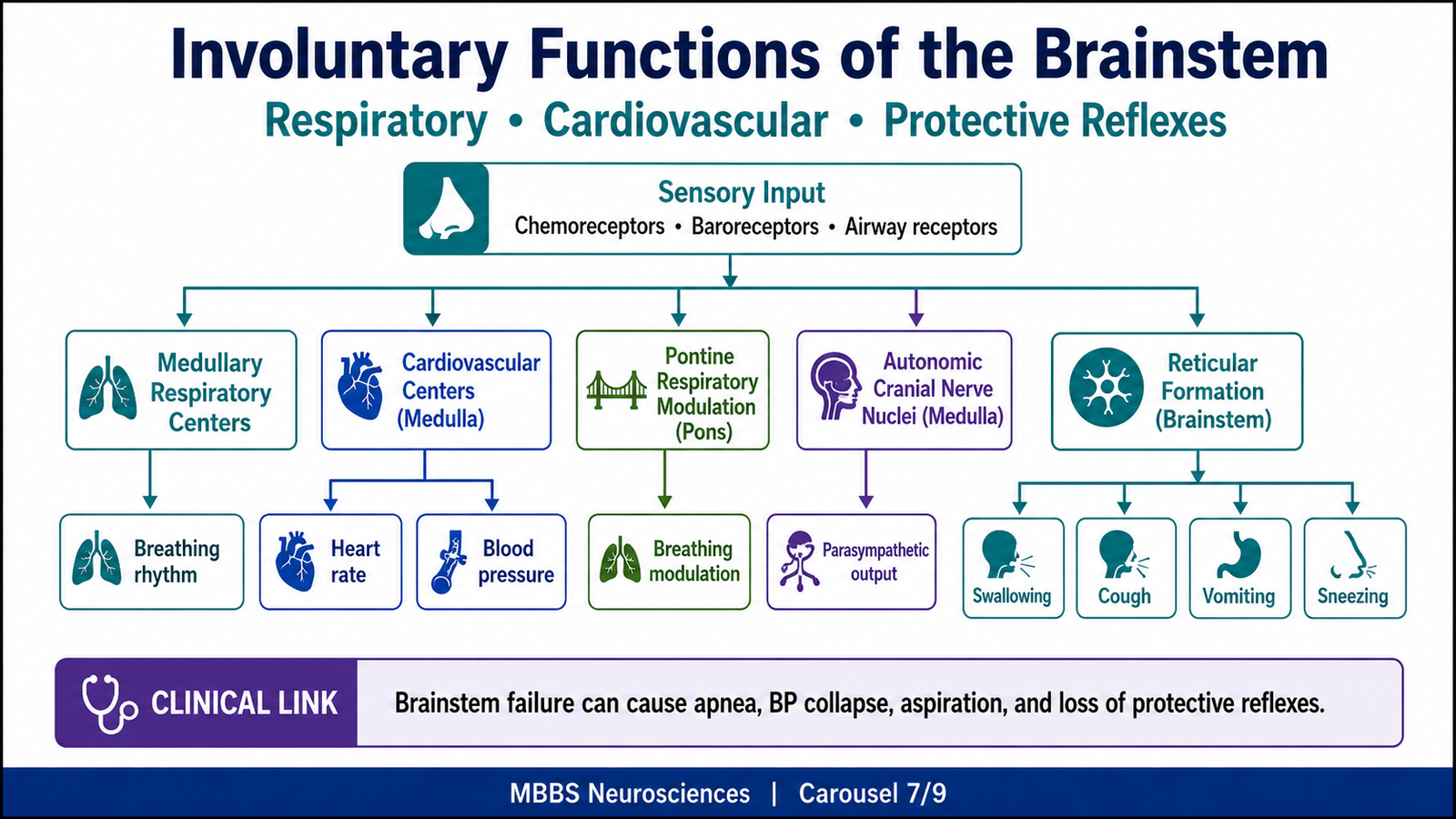
Involuntary functions are automatic body activities that occur without conscious effort. The brainstem is essential for these functions because it contains autonomic centers and reflex circuits that maintain life.
The medulla contains centers that regulate breathing and cardiovascular activity. Respiratory neurons in the medulla generate basic rhythmic breathing. Pontine centers modify this rhythm, making breathing smooth and coordinated. This arrangement exists because breathing must continue automatically whether a person is awake, asleep, or unconscious.
The cardiovascular centers in the medulla regulate heart rate, force of contraction, and blood vessel diameter. They receive input from baroreceptors and chemoreceptors and adjust autonomic output accordingly. For example, if blood pressure rises, baroreceptor input increases, causing medullary centers to reduce sympathetic activity and increase parasympathetic activity. As a result, heart rate and blood pressure decrease.
The brainstem also controls protective reflexes. Swallowing requires coordinated activity of cranial nerves V, VII, IX, X, and XII. Coughing protects the airway by removing irritants. Vomiting removes harmful gastric contents. Sneezing clears nasal passages. These reflexes depend on sensory input, brainstem integration, and motor output.
The reticular formation helps coordinate these autonomic and motor responses. It links sensory information with appropriate motor and visceral reactions. This is why brainstem damage can disturb multiple automatic functions simultaneously.
⚠️ CLINICAL IMPORTANCE
Brainstem failure may cause respiratory arrest, cardiovascular collapse, aspiration due to impaired swallowing, loss of airway reflexes, and coma. In emergency medicine, assessment of breathing, pupillary reflexes, gag reflex, and consciousness provides important clues about brainstem function.
MAJOR CONCEPTUAL HEADING 8
Reticular Formation and Reticular Activating System
🧠 CORE
• The reticular formation is a diffuse network of neurons throughout the brainstem.
• It extends from the medulla through the pons and midbrain.
• It receives sensory input from many pathways.
• It influences autonomic function, motor tone, pain modulation, sleep-wake cycles, and consciousness.
• The ascending part forms the reticular activating system.
• The RAS activates the thalamus and cerebral cortex.
• It is essential for wakefulness and alertness.
🔬 CONCEPT EXPLAINED
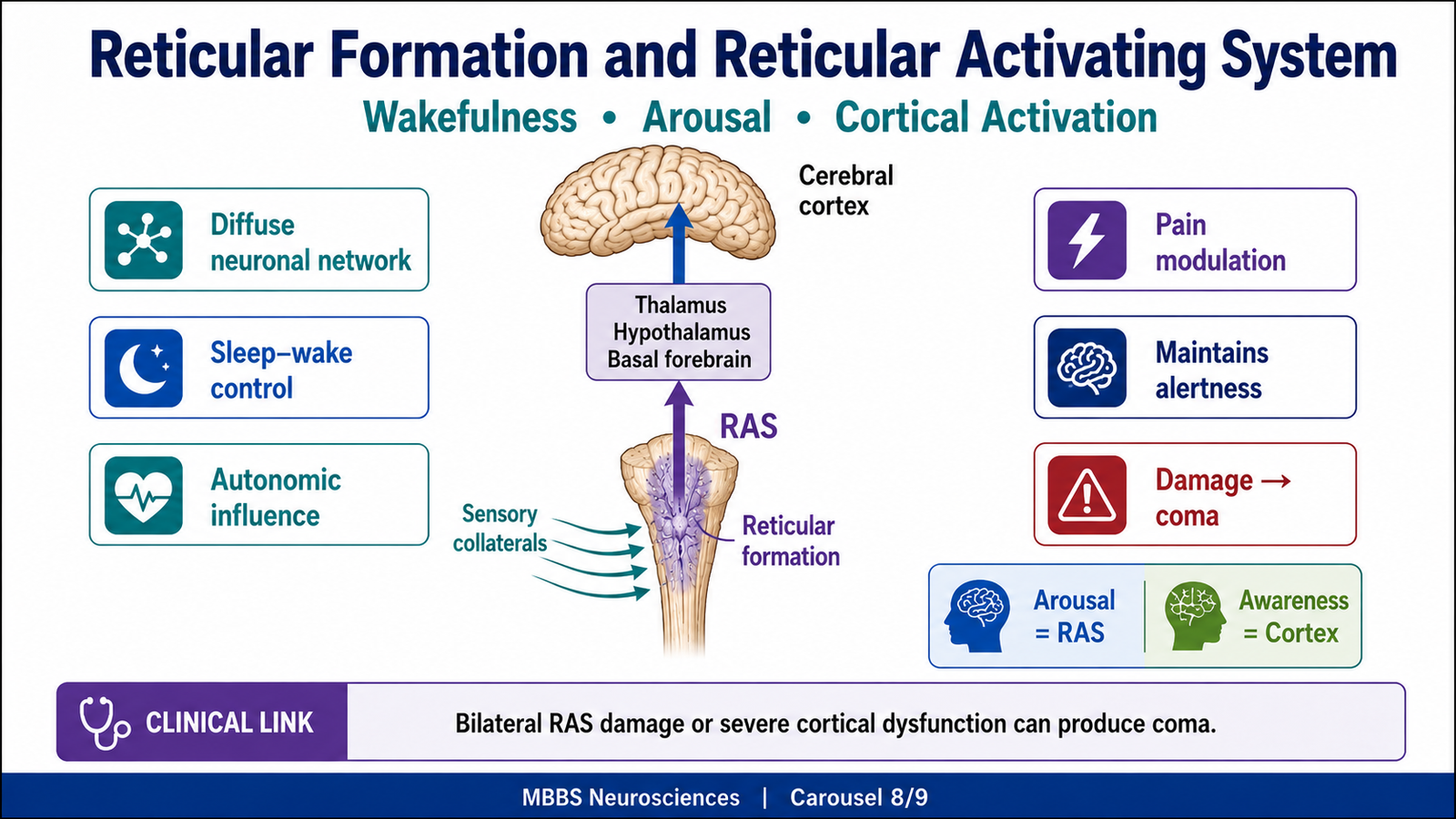
The reticular formation is not a single compact nucleus. It is a network of neurons scattered throughout the central core of the brainstem. Its name comes from its net-like appearance. Because it receives input from many sensory pathways, it acts as an integrative system that monitors the internal and external environment.
The reticular formation exists because the body needs a system that can coordinate general states of activity rather than only specific movements or sensations. For example, when a painful stimulus occurs, the body does not only perceive pain. It also becomes alert, increases autonomic activity, changes muscle tone, and prepares defensive responses. The reticular formation helps coordinate these widespread responses.
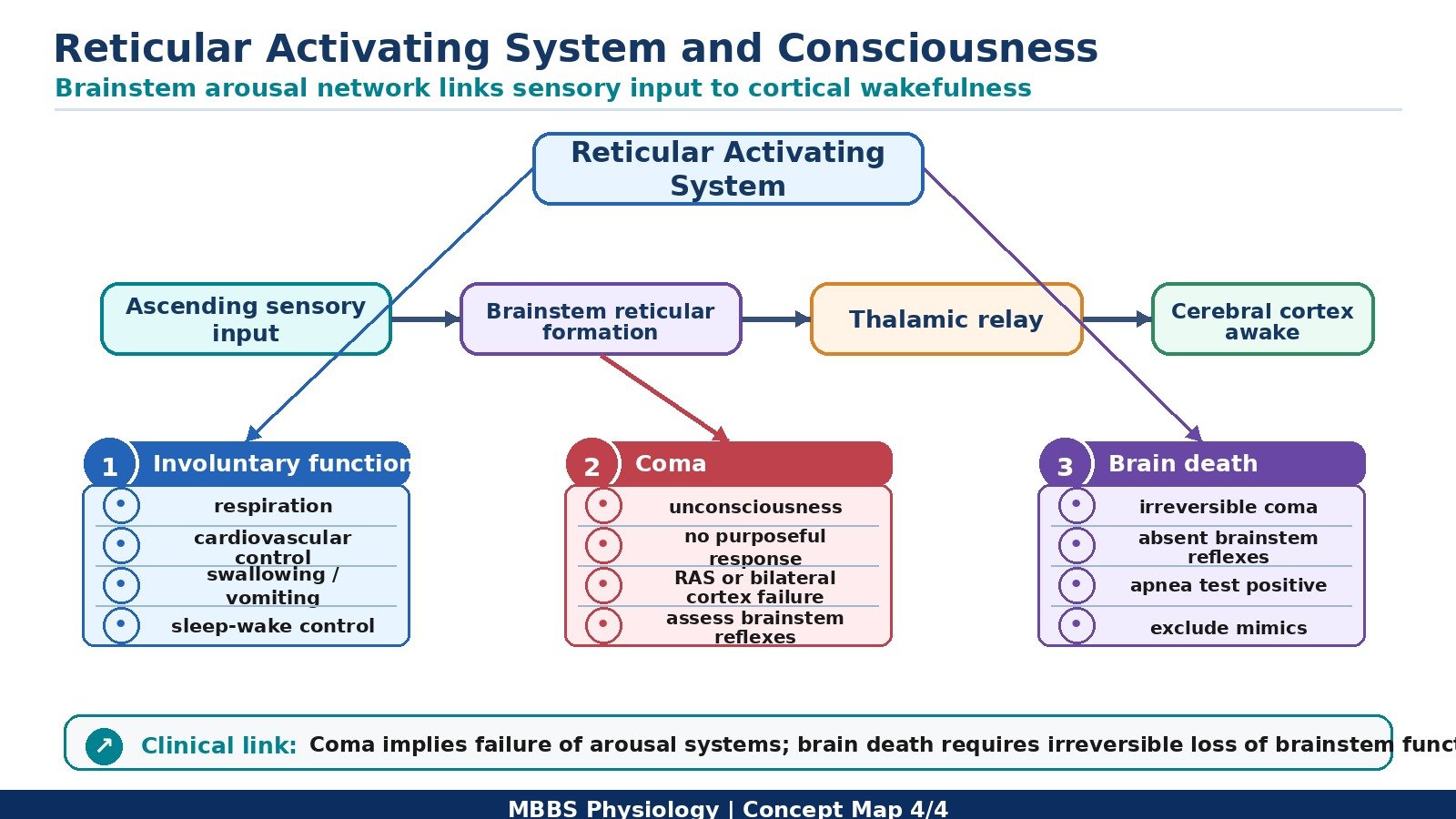
The reticular activating system (RAS) is the ascending activating component of the reticular formation. It receives collateral input from sensory pathways such as pain, touch, auditory, visual, and visceral pathways. It then projects upward to the thalamus, hypothalamus, basal forebrain, and cerebral cortex. These projections help maintain cortical activation.
Wakefulness depends on both an intact cerebral cortex and an intact RAS. The cerebral cortex provides the content of consciousness, such as thoughts, perception, memory, and awareness. The RAS provides the level of consciousness, meaning arousal and wakefulness. Therefore, consciousness requires both cortical function and brainstem activation.
The RAS uses several neurotransmitter systems, including acetylcholine, norepinephrine, serotonin, dopamine, and histamine. These systems help regulate attention, sleep-wake transitions, and alertness. At MBBS level, the key point is that the RAS maintains cortical excitability and keeps the person awake.
Structure and Functional Components of RAS
The RAS involves:
• Brainstem reticular formation
• Intralaminar nuclei of thalamus
• Hypothalamic arousal centers
• Basal forebrain activating pathways
• Diffuse projections to cerebral cortex
These components work together to maintain wakefulness. Sensory input activates the brainstem reticular formation. The RAS then activates the thalamus and cerebral cortex. The cortex becomes more responsive to incoming information, allowing awareness and attention.
How the RAS Works
When sensory stimuli enter the nervous system, collateral branches activate the reticular formation. The reticular formation sends ascending signals to the thalamus and cortex. This increases cortical activity, producing alertness. If sensory input is reduced, such as during sleep, cortical activation decreases. During wakefulness, continuous RAS activity maintains an alert state.
Therefore, the RAS works like an activating switch. It does not create specific thoughts or memories, but it keeps the cortex awake enough to process them.
Why the RAS Exists
The RAS allows the brain to respond to important stimuli. It helps a person wake up when there is danger, pain, loud sound, or strong emotional input. It also helps maintain attention during learning and purposeful activity. Without the RAS, the cortex may remain structurally intact but functionally inactive.
What Happens if the RAS Fails
If the RAS is damaged, cortical arousal is lost. The patient may become drowsy, stuporous, or comatose depending on severity. Bilateral damage to the upper brainstem or diffuse cortical dysfunction can cause coma.
⚠️ CLINICAL IMPORTANCE
RAS dysfunction is a major mechanism of coma. A patient may become unconscious due to widespread cerebral cortical dysfunction, direct brainstem RAS injury, metabolic suppression of neuronal activity, or raised intracranial pressure compressing the brainstem.
MAJOR CONCEPTUAL HEADING 9
Consciousness, Coma and Brain Death
🧠 CORE
• Consciousness requires arousal and awareness.
• Arousal depends mainly on the brainstem RAS.
• Awareness depends mainly on cerebral cortical function.
• Coma is unarousable unconsciousness.
• Coma may result from bilateral cerebral hemisphere dysfunction or brainstem RAS damage.
• Brain death is irreversible loss of all brain and brainstem function.
• Brainstem reflexes are essential in assessing coma and brain death.
🔬 CONCEPT EXPLAINED
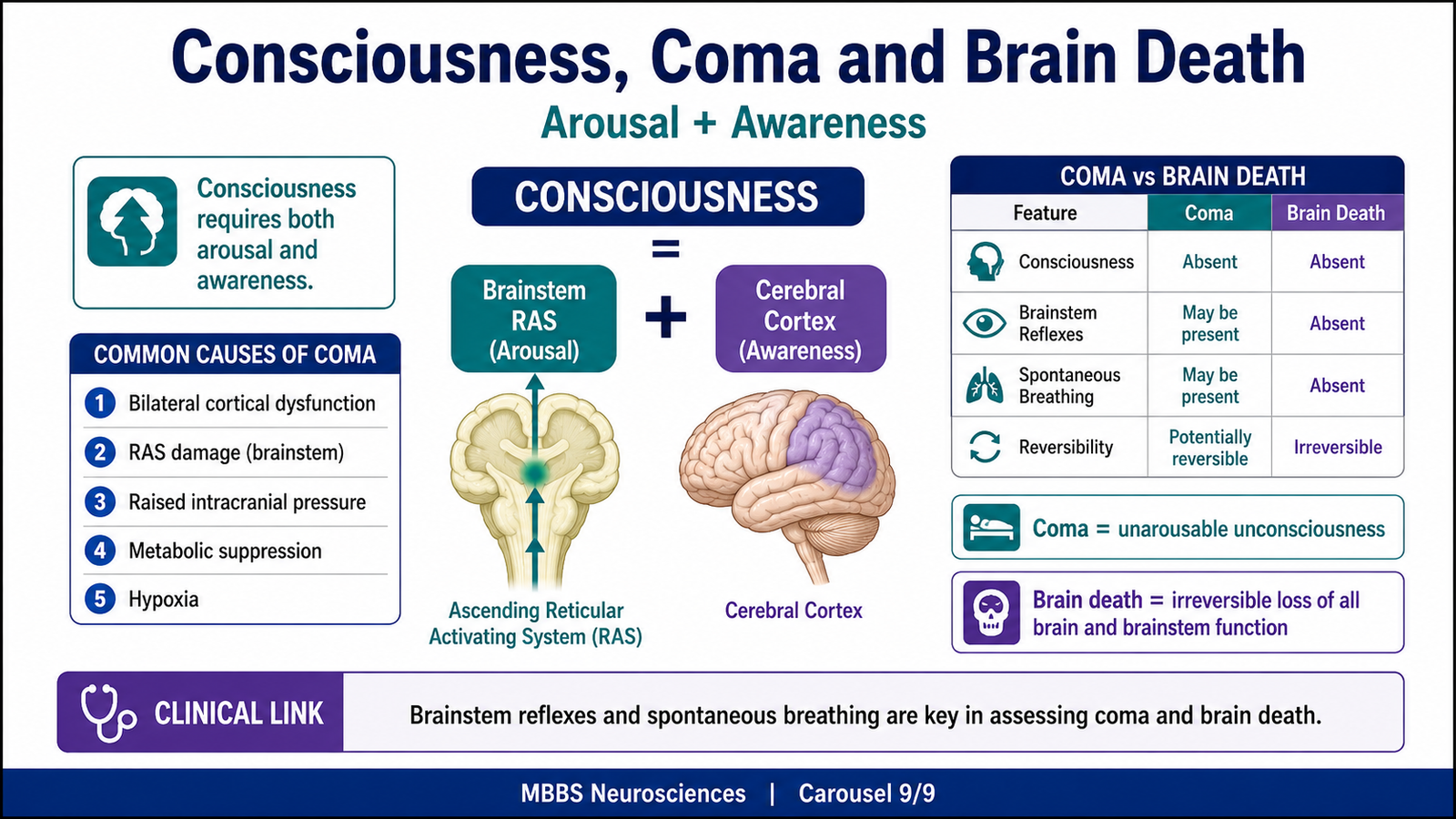
Consciousness has two major components: level of consciousness and content of consciousness. The level of consciousness means arousal or wakefulness. This depends mainly on the RAS in the brainstem and its projections to the thalamus and cortex. The content of consciousness means awareness, thinking, memory, perception, and response to environment. This depends mainly on the cerebral cortex.
This division explains important clinical situations. If the cerebral cortex is diffusely impaired, the patient may lose awareness. If the RAS is damaged, the cortex may no longer receive activating input, resulting in coma. Therefore, coma occurs when either both cerebral hemispheres are severely dysfunctional or the brainstem activating system is damaged.
Coma
Coma is a state of unarousable unconsciousness in which the patient does not open eyes, does not show awareness, and does not respond meaningfully to external stimuli. It is not the same as sleep because a sleeping person can be awakened, while a comatose patient cannot be aroused by ordinary stimuli.
Coma occurs because the neural systems responsible for arousal and awareness are severely impaired. This may happen due to structural lesions, metabolic disturbances, toxins, hypoxia, trauma, infection, or raised intracranial pressure.
Mechanism of Coma
The common mechanisms include:
• Bilateral cerebral hemisphere dysfunction
• Damage to the brainstem RAS
• Compression of the brainstem due to raised intracranial pressure
• Metabolic suppression of cortical and brainstem neuronal activity
• Hypoxia causing failure of neuronal energy metabolism
When neurons cannot maintain normal electrical activity, cortical responsiveness decreases. If the RAS cannot activate the cortex, wakefulness is lost. As a result, the patient becomes unconscious and unarousable.
Brainstem Signs in Coma
Brainstem examination is important because it helps identify severity and localization. Important signs include pupillary response, corneal reflex, gag reflex, eye movements, respiratory pattern, and motor response. Loss of brainstem reflexes suggests severe brainstem dysfunction.
Brain Death
Brain death is the irreversible loss of all functions of the brain, including the brainstem. It is not simply deep coma. In coma, some brainstem functions may remain. In brain death, brainstem reflexes and spontaneous respiration are absent.
Brain death occurs when brain injury is so severe that no recovery of brain function is possible. The brain can no longer maintain consciousness, reflexes, breathing drive, or integration of body functions.
Basic Concept of Brain Death
In brain death:
• The patient is deeply unconscious.
• There is no response to external stimuli.
• Brainstem reflexes are absent.
• Spontaneous breathing is absent.
• The condition is irreversible.
The brainstem is central to this diagnosis because it controls arousal, cranial nerve reflexes, and respiratory drive. If brainstem function is completely absent and irreversible, the brain can no longer support life as an integrated organ.
Difference Between Coma and Brain Death
| Feature | Coma | Brain Death |
|---|---|---|
| Consciousness | Absent | Absent |
| Arousability | Not arousable | Not arousable |
| Brainstem reflexes | May be present or absent | Absent |
| Spontaneous breathing | May be present or assisted | Absent |
| Reversibility | May be reversible depending on cause | Irreversible |
| Meaning | Severe brain dysfunction | Death of whole brain including brainstem |
⚠️ CLINICAL IMPORTANCE
Coma requires urgent evaluation because reversible causes such as hypoglycemia, hypoxia, drug intoxication, infection, and raised intracranial pressure may be treatable. Brain death is a diagnosis with serious medical, ethical, and legal implications and must be assessed carefully according to accepted clinical criteria.
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| Medullary pyramids | Carry corticospinal fibers | Voluntary motor control |
| Pyramidal decussation | Crossing of motor fibers | Contralateral motor control |
| Gracile and cuneate nuclei | Relay fine touch, vibration, proprioception | Conscious sensory perception |
| Sensory decussation | Crossing of sensory fibers | Contralateral sensory representation |
| Inferior olivary nucleus | Cerebellar motor learning input | Coordination and motor refinement |
| Pontine nuclei | Relay cortical signals to cerebellum | Smooth voluntary movement |
| Middle cerebellar peduncle | Carries pontocerebellar fibers | Cerebellar coordination |
| Superior colliculus | Visual reflex center | Eye/head movement toward visual stimuli |
| Inferior colliculus | Auditory reflex center | Reflex response to sound |
| Cranial nerve nuclei | Motor, sensory, autonomic cranial nerve control | Eye movement, swallowing, facial movement, hearing, balance |
| Reticular formation | Integrates autonomic, motor, sensory, arousal functions | Survival responses and alertness |
| RAS | Activates thalamus and cortex | Wakefulness and consciousness |
| Medullary respiratory centers | Generate respiratory rhythm | Automatic breathing |
| Cardiovascular centers | Control heart rate and vascular tone | Blood pressure homeostasis |
The brainstem is therefore an integrated survival center. Its anatomy explains its physiology. The pyramids explain motor control, the medial lemniscus explains sensory transmission, cranial nerve nuclei explain head and neck functions, autonomic centers explain involuntary life functions, and RAS explains consciousness. When these structures fail, the clinical outcome directly reflects the damaged function.
🩺 5️⃣ Clinical Correlation
1. Brainstem Lesions
Brainstem lesions may be caused by stroke, trauma, tumors, demyelination, compression, or raised intracranial pressure. Because the brainstem contains long tracts and cranial nerve nuclei close together, lesions often produce crossed findings: cranial nerve signs on the same side as the lesion and limb signs on the opposite side.
Key Concept
Ipsilateral cranial nerve deficit + contralateral body weakness or sensory loss = brainstem localization.
2. Medullary Lesions
Medullary damage can affect corticospinal tracts, medial lemniscus, nucleus ambiguus, hypoglossal nucleus, vestibular nuclei, and autonomic centers. This may cause weakness, sensory loss, dysphagia, hoarseness, tongue deviation, vertigo, ataxia, and respiratory or cardiovascular instability.
Exam Importance
The medulla is vital because it contains respiratory and cardiovascular centers. Severe medullary damage may rapidly become fatal.
3. Pontine Lesions
Pontine lesions may affect facial nerve nucleus, abducens nucleus, trigeminal pathways, vestibulocochlear nuclei, corticospinal tracts, and pontocerebellar fibers. Clinical features may include facial paralysis, impaired lateral gaze, loss of facial sensation, vertigo, hearing disturbance, ataxia, and limb weakness.
Exam Importance
A ventral pontine lesion can damage corticospinal tracts severely. If the RAS remains intact, consciousness may be preserved despite paralysis, producing a locked-in state.
4. Midbrain Lesions
Midbrain lesions may affect oculomotor nerve fibers, trochlear nucleus, red nucleus, substantia nigra, colliculi, and RAS pathways. Clinical features may include diplopia, ptosis, abnormal pupil, tremor, rigidity, visual reflex defects, auditory reflex defects, or coma.
Exam Importance
Midbrain involvement is especially important in altered consciousness because ascending RAS pathways pass through the upper brainstem.
5. Coma
Coma occurs when the brain cannot maintain arousal and awareness. It may result from diffuse cortical dysfunction, brainstem RAS damage, metabolic abnormalities, hypoxia, toxins, trauma, or raised intracranial pressure.
Key Clinical Manifestations
• No eye opening
• No meaningful response to voice or pain
• No awareness of environment
• Abnormal breathing pattern may occur
• Brainstem reflexes may be impaired depending on severity
Exam Importance
Coma is not sleep. Sleep is reversible with arousal. Coma is unarousable unconsciousness.
6. Brain Death
Brain death means irreversible loss of all brain function including brainstem function. The patient has no consciousness, no brainstem reflexes, and no spontaneous breathing.
Key Clinical Manifestations
• Deep unresponsiveness
• Absent pupillary reflex
• Absent corneal reflex
• Absent gag and cough reflexes
• No spontaneous respiration
• Irreversible condition
Exam Importance
Brain death is not the same as coma. In coma, some brainstem functions may remain and recovery may be possible. In brain death, brainstem function is irreversibly absent.
📌 6️⃣ Summary Points
- The brainstem consists of medulla, pons, and midbrain.
- The brainstem contains ascending sensory tracts, descending motor tracts, cranial nerve nuclei, autonomic centers, and reticular formation.
- The medulla contains pyramids, olives, sensory decussation, motor decussation, and nuclei related mainly to IX, X, XI, and XII.
- The motor decussation explains why one cerebral hemisphere controls the opposite side of the body.
- The sensory decussation forms the medial lemniscus and carries fine touch, vibration, and proprioception to the opposite cortex.
- The pons acts as a bridge between cerebral cortex and cerebellum through pontine nuclei and transverse pontocerebellar fibers.
- Cranial nerve nuclei in the pons are mainly related to V, VI, VII, and VIII.
- The midbrain contains superior and inferior colliculi, cerebral peduncles, red nucleus, substantia nigra, and nuclei of III and IV.
- The superior colliculus is related to visual reflexes, while the inferior colliculus is related to auditory reflexes.
- The reticular activating system maintains wakefulness by activating the thalamus and cerebral cortex.
- Coma occurs due to dysfunction of bilateral cerebral hemispheres, brainstem RAS, or both.
- Brain death is irreversible loss of all brain function, including brainstem reflexes and spontaneous respiration.