
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
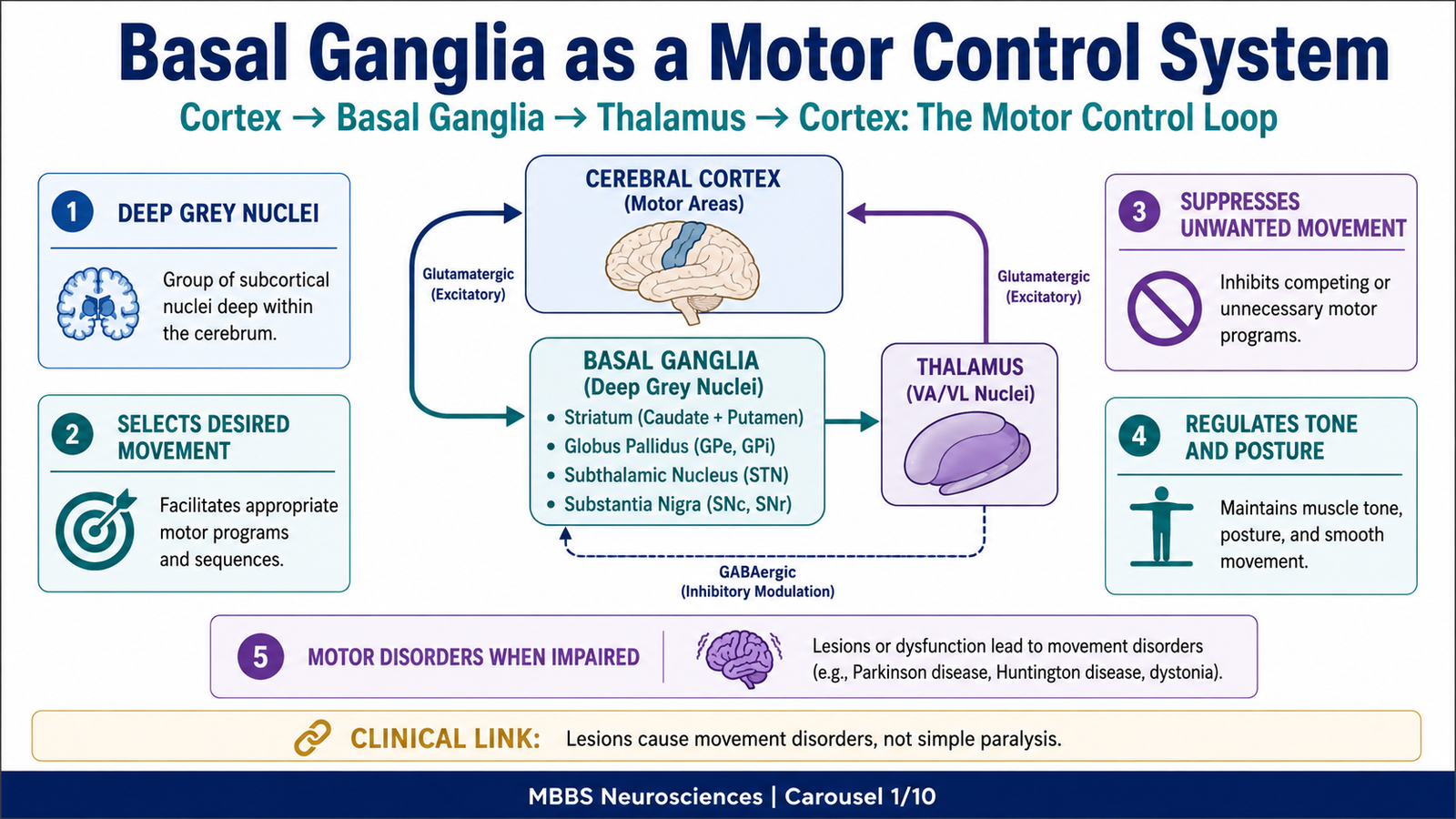
The basal ganglia are a group of deep grey matter nuclei located mainly within the cerebral hemispheres and closely connected with the cerebral cortex, thalamus, brainstem, and motor pathways. They are not directly responsible for producing muscle contraction, but they are essential for planning, selecting, initiating, scaling, and smoothing voluntary movements.
The basal ganglia are especially important in controlling automatic associated movements, such as arm swinging during walking, facial expression during speech, posture-related adjustments, and learned motor patterns. Their activity allows useful motor programs to be facilitated while unwanted competing movements are suppressed.
Clinically, basal ganglia are highly important because their dysfunction produces major movement disorders such as Parkinson disease, chorea, athetosis, hemiballismus, rigidity, tremor, and abnormal posture. These disorders help students understand that normal movement requires not only pyramidal motor pathways but also powerful extrapyramidal control systems.
In anatomy, the basal ganglia are studied as deep nuclei related to the internal capsule, lateral ventricle, thalamus, and midbrain. In physiology, they are studied through their direct pathway, indirect pathway, putamen circuit, caudate circuit, and dopaminergic modulation.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Basal ganglia / basal nuclei: Deep grey matter nuclei involved mainly in motor control, motor planning, posture, muscle tone, habit formation, and cognitive aspects of movement.
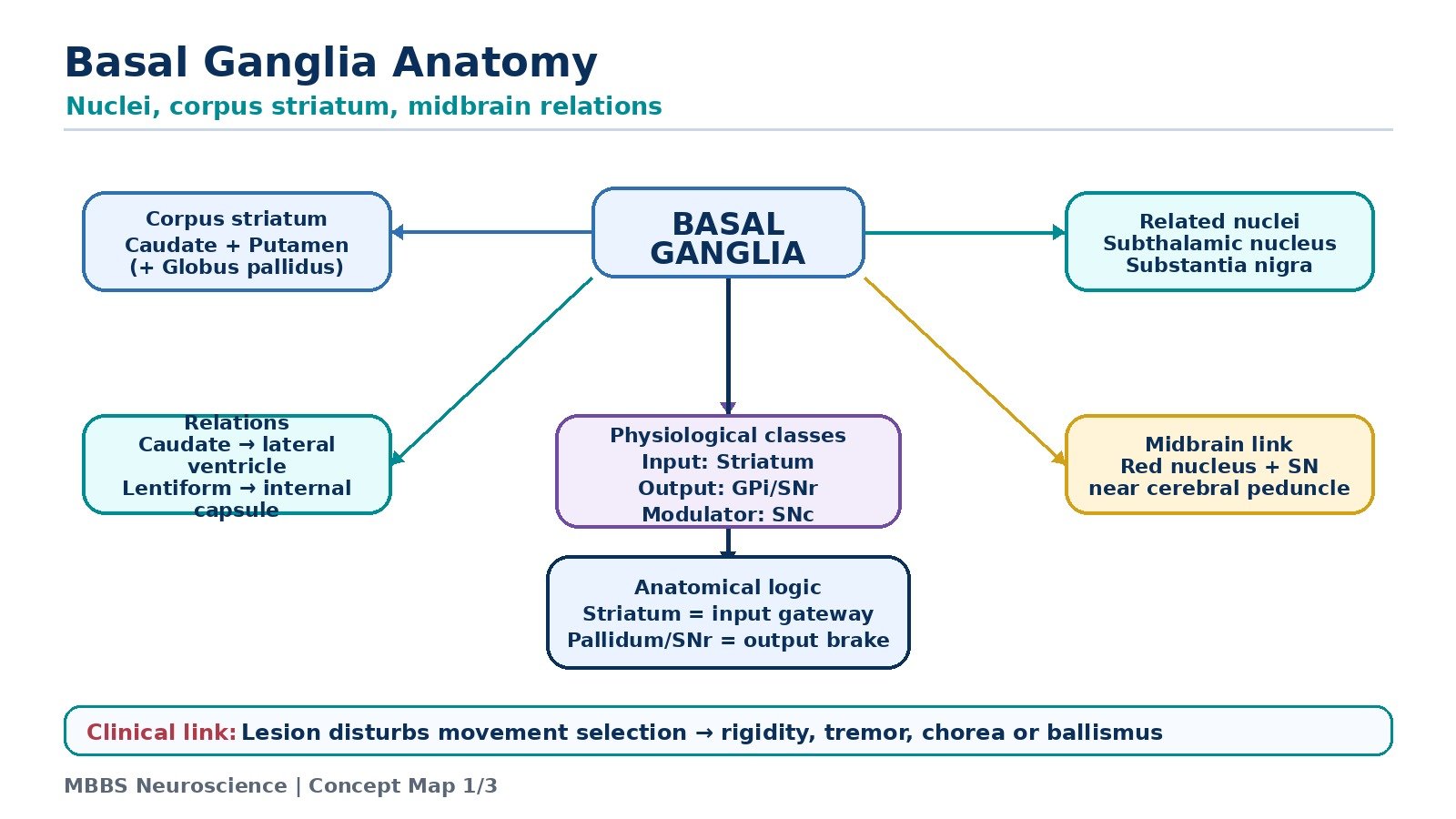
- Corpus striatum: A major basal ganglia mass made up of the caudate nucleus and lentiform nucleus.
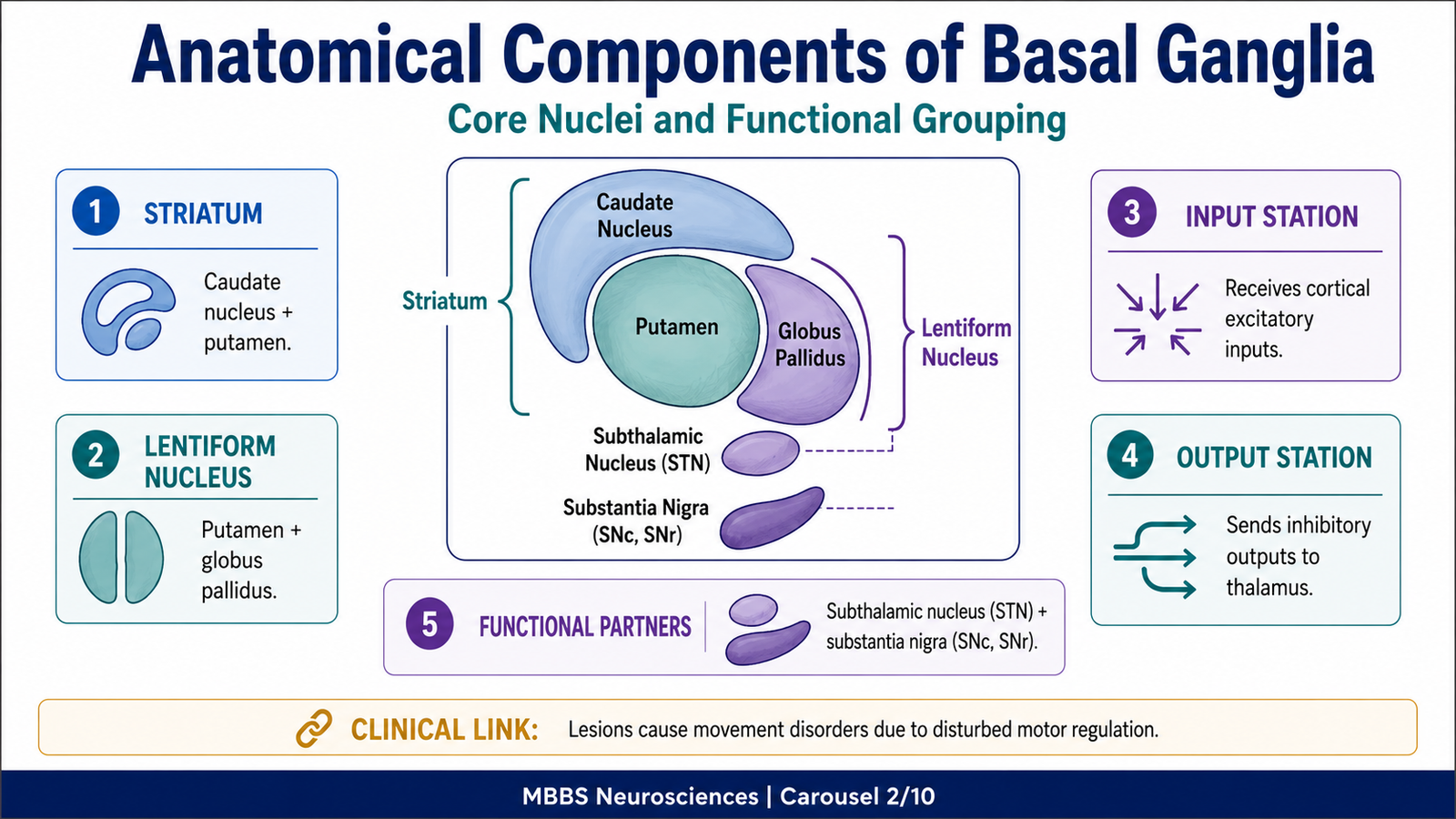
- Striatum: Functional input part of basal ganglia, mainly formed by caudate nucleus and putamen.
- Lentiform nucleus: Lens-shaped grey matter made up of putamen laterally and globus pallidus medially.
- Globus pallidus: Major output nucleus of basal ganglia, divided into external segment and internal segment.
- Subthalamic nucleus: A functionally important nucleus of the indirect pathway.
- Substantia nigra: Midbrain nucleus with dopaminergic and output functions; especially important in Parkinson disease.
- Red nucleus: Midbrain motor nucleus related to motor coordination and extrapyramidal pathways.
- Direct pathway: Basal ganglia pathway that facilitates wanted movement.
- Indirect pathway: Basal ganglia pathway that suppresses unwanted movement.
- Putamen circuit: Basal ganglia circuit mainly concerned with execution of learned motor patterns.
- Caudate circuit: Basal ganglia circuit mainly concerned with cognitive planning and sequencing of movement.
🔹 3️⃣ Core Learning — Curriculum Coverage
BASAL GANGLIA AS A MOTOR CONTROL SYSTEM
🧠 CORE
- Basal ganglia are deep grey matter nuclei involved in motor regulation.
- They work with the cerebral cortex, thalamus, and brainstem.
- They do not directly send motor commands to spinal motor neurons.
- Their main role is to select desired motor programs and suppress unwanted ones.
- They regulate muscle tone, posture, automatic movements, and learned movement patterns.
- Dysfunction produces movement disorders rather than simple paralysis.
- They form part of the extrapyramidal motor system.
- Their major physiological logic is balance between movement facilitation and movement inhibition.
🔬 CONCEPT EXPLAINED
To understand basal ganglia, students must first understand that voluntary movement is not only a matter of “command from motor cortex to muscle.” Before a movement occurs, the nervous system must decide which movement should occur, how strongly it should occur, when it should start, and which unwanted movements must be prevented. This is where the basal ganglia become essential.
The basal ganglia act like a motor selection and filtering system. The cerebral cortex sends information about intended movements to the basal ganglia. The basal ganglia process this information and influence the thalamus, which then modifies motor cortical activity. Therefore, the basal ganglia control movement indirectly by influencing the activity of the motor cortex.
The body needs this system because many possible motor programs are available at any time. For example, when a person reaches for a cup, the nervous system must activate the correct shoulder, elbow, wrist, and finger movements, while suppressing unnecessary movements of the opposite limb, trunk, or face. Basal ganglia allow the correct movement pattern to be released smoothly.
A very important concept is that basal ganglia dysfunction usually does not cause loss of power like corticospinal tract damage. Instead, it causes abnormal movement control. Movements may become too little, too slow, too rigid, excessive, irregular, or poorly selected. This is why basal ganglia lesions produce disorders such as hypokinesia, bradykinesia, rigidity, tremor, chorea, athetosis, and ballismus.
⚠️ CLINICAL IMPORTANCE
When basal ganglia fail, the problem is usually not complete paralysis. Instead, the patient develops abnormal regulation of movement. In Parkinson disease, movement becomes reduced and slow. In chorea, unwanted irregular movements appear. In hemiballismus, violent flinging movements occur. This shows that basal ganglia normally maintain a balance between allowing useful movement and suppressing unwanted movement.
ANATOMICAL COMPONENTS OF BASAL GANGLIA
🧠 CORE
- Anatomically, basal nuclei include caudate nucleus, putamen, globus pallidus, claustrum, and amygdaloid body.
- Functionally, the most important basal ganglia are caudate nucleus, putamen, globus pallidus, subthalamic nucleus, and substantia nigra.
- Caudate nucleus and putamen form the striatum.
- Putamen and globus pallidus form the lentiform nucleus.
- Caudate nucleus and lentiform nucleus together form the corpus striatum.
- Internal capsule separates caudate nucleus and thalamus medially from lentiform nucleus laterally.
- Substantia nigra and subthalamic nucleus are not part of corpus striatum anatomically but are essential functionally.
🔬 CONCEPT EXPLAINED
The basal ganglia are described differently in anatomy and physiology. Anatomically, they are deep masses of grey matter located within the cerebral hemispheres. The important anatomical components are the caudate nucleus, lentiform nucleus, claustrum, and amygdaloid body. However, in physiology, the term basal ganglia is used more functionally and includes nuclei that participate in motor circuits, especially the caudate nucleus, putamen, globus pallidus, subthalamic nucleus, and substantia nigra.
The caudate nucleus and putamen are closely related developmentally and functionally. Together, they form the striatum, which receives major input from the cerebral cortex. The striatum is called the input station of the basal ganglia because cortical signals enter basal ganglia circuits mainly through the caudate nucleus and putamen.
The globus pallidus is the major output region. It has two parts: the external segment and the internal segment. The internal segment is especially important because it sends inhibitory output to the thalamus. Through the thalamus, the globus pallidus controls how strongly the motor cortex becomes activated.
The subthalamic nucleus is located below the thalamus and is especially important in the indirect pathway. It excites the internal segment of globus pallidus, which increases inhibition of the thalamus and suppresses movement. If this nucleus is damaged, unwanted excessive movements may occur.
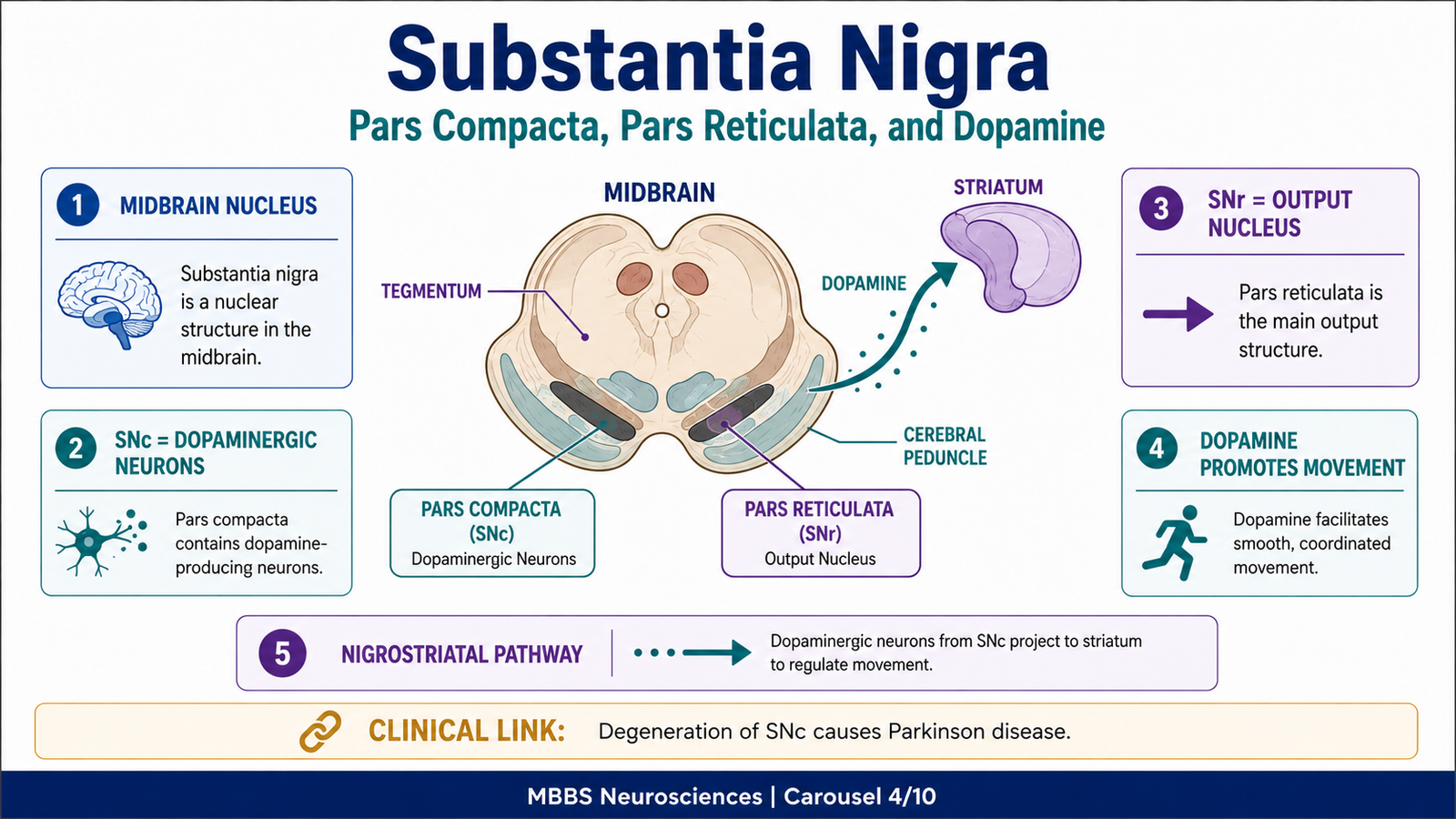
The substantia nigra lies in the midbrain. It has two functionally important parts: pars compacta, which provides dopamine to the striatum, and pars reticulata, which acts as an output nucleus similar to the internal globus pallidus. Dopamine from substantia nigra is essential for normal movement control. Loss of this dopamine is the major mechanism in Parkinson disease.
Therefore, the anatomical arrangement of basal ganglia supports their function: input enters through striatum, processing occurs through direct and indirect pathways, and output influences thalamus and motor cortex.
⚠️ CLINICAL IMPORTANCE
The close anatomical relation of basal ganglia to the internal capsule is clinically important. A lesion in the internal capsule causes upper motor neuron weakness because corticospinal fibers are damaged. In contrast, a lesion in basal ganglia causes abnormal movement, tone, or posture because motor regulation circuits are disturbed.
CORPUS STRIATUM: STRUCTURE AND RELATIONS
🧠 CORE
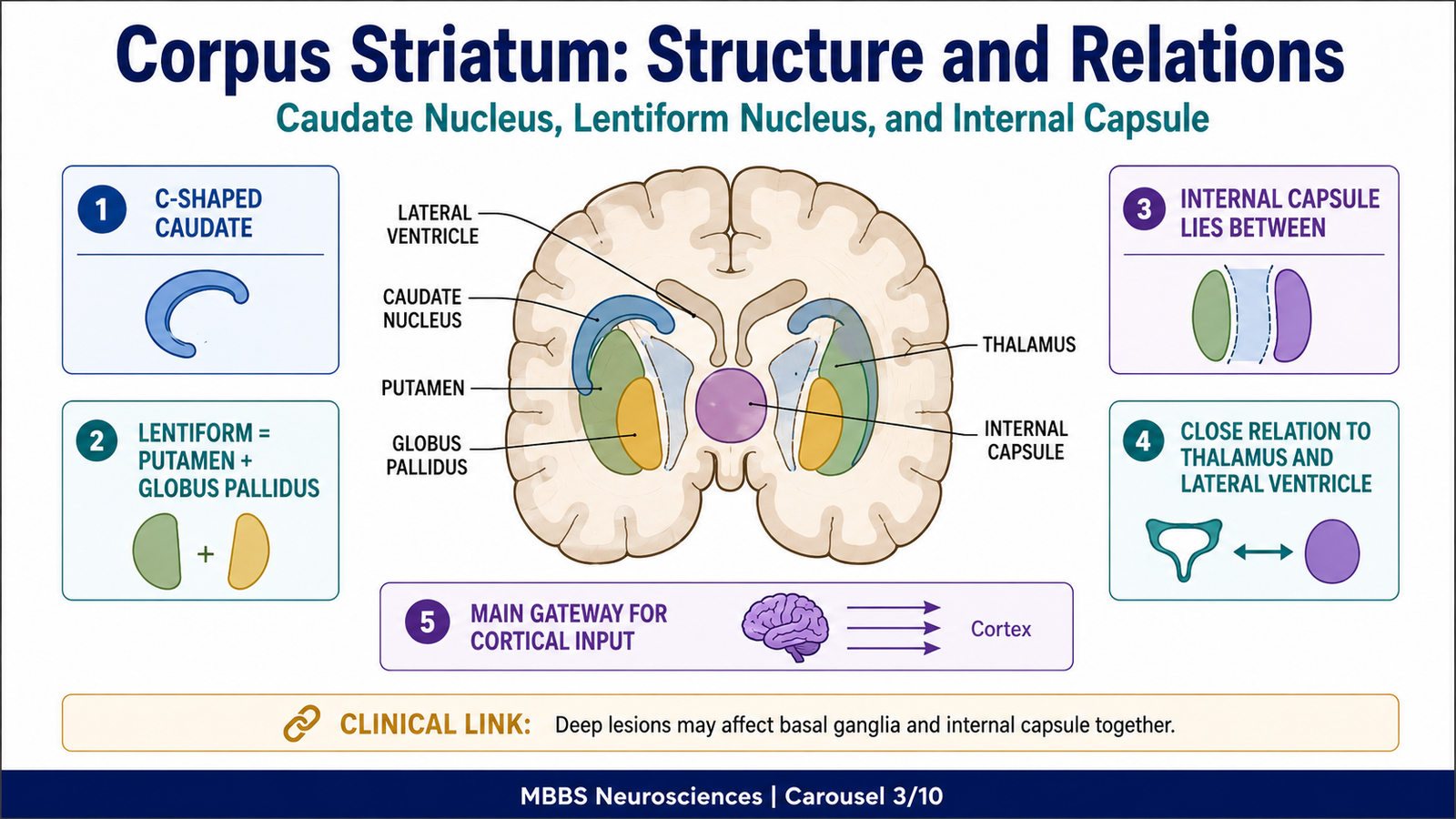
- Corpus striatum consists of caudate nucleus and lentiform nucleus.
- Lentiform nucleus consists of putamen and globus pallidus.
- Caudate nucleus is C-shaped and follows the lateral ventricle.
- Putamen lies lateral to globus pallidus.
- Internal capsule separates caudate nucleus and thalamus from lentiform nucleus.
- Corpus striatum is deeply related to lateral ventricle, thalamus, and internal capsule.
- Striatum is the major input area of basal ganglia.
- Globus pallidus is the major output part within the corpus striatum.
🔬 CONCEPT EXPLAINED
The corpus striatum is the main mass of basal ganglia within the cerebral hemisphere. It is called “striated” because strands of grey matter pass through the internal capsule, giving a striped appearance. Structurally, it is made of the caudate nucleus and lentiform nucleus.
The caudate nucleus is a curved C-shaped nucleus. It has a head, body, and tail. The head of caudate lies near the anterior horn of the lateral ventricle. The body follows the body of the lateral ventricle, and the tail curves downward and forward into the temporal lobe. This shape is important because it shows the close relationship of the caudate nucleus with the ventricular system.
The lentiform nucleus lies lateral to the internal capsule. It has two parts: the lateral putamen and medial globus pallidus. The putamen is more closely related functionally to the caudate nucleus, while globus pallidus is more important as an output nucleus.
The internal capsule is a major white matter structure that lies between the caudate nucleus and thalamus medially and the lentiform nucleus laterally. This relation is very important because corticospinal and corticobulbar fibers pass through the internal capsule. Therefore, deep brain lesions in this region can produce either motor weakness, movement disorders, or both depending on the exact site involved.
The structural design of corpus striatum supports its function. The striatum receives widespread input from the cerebral cortex. These cortical inputs are processed by the basal ganglia and then influence motor cortex through thalamic feedback. In this way, the corpus striatum acts as a gateway through which cortical motor plans enter basal ganglia circuits.
⚠️ CLINICAL IMPORTANCE
Because the corpus striatum is closely related to the internal capsule, vascular lesions in this region may produce mixed clinical pictures. Damage to internal capsule causes contralateral weakness, while damage to basal ganglia produces abnormal tone and movements. This anatomical relationship is frequently tested in neuroanatomy and clinical neuroscience.
RED NUCLEUS: STRUCTURE, RELATIONS AND MOTOR ROLE
🧠 CORE
- Red nucleus is located in the midbrain tegmentum.
- It lies at the level of the superior colliculus.
- It is related to motor coordination and extrapyramidal control.
- It receives input from cerebellum and cerebral cortex.
- It gives rise to the rubrospinal tract in many animals.
- In humans, its direct motor role is less dominant than corticospinal control.
- It is functionally linked with posture, tone, and coordinated limb movement.
- It forms part of the brainstem motor control network.
🔬 CONCEPT EXPLAINED
The red nucleus is a rounded motor nucleus located in the tegmentum of the midbrain. It appears reddish because of its rich blood supply and iron-containing pigment. Anatomically, it is found at the level of the superior colliculus and is related to important midbrain structures such as the substantia nigra, cerebral peduncle, and oculomotor nerve region.
The red nucleus is important because it acts as a relay between higher motor centers, cerebellum, and brainstem motor pathways. It receives input from the cerebellum, especially through the superior cerebellar peduncle, and also receives cortical input. This allows it to participate in coordination between planned movement and postural adjustment.
In lower animals, the red nucleus gives rise to a prominent rubrospinal tract, which helps control flexor muscles of limbs. In humans, the corticospinal tract is much more dominant, so the rubrospinal tract is relatively less important. However, the red nucleus remains functionally important as part of the extrapyramidal system and motor coordination network.
The body needs red nucleus connections because voluntary movement must be coordinated with posture and tone. When the cortex plans a movement, the body must simultaneously adjust background muscle activity. The red nucleus helps link motor planning, cerebellar correction, and brainstem motor output.
⚠️ CLINICAL IMPORTANCE
Lesions involving the red nucleus region may disturb motor coordination and tone. Although isolated red nucleus lesions are uncommon in undergraduate clinical examples, its role is important in understanding extrapyramidal motor control and brainstem motor pathways.
SUBSTANTIA NIGRA: STRUCTURE, RELATIONS AND FUNCTIONAL IMPORTANCE
🧠 CORE
- Substantia nigra is located in the midbrain.
- It lies between the tegmentum and cerebral peduncle.
- It has two main parts: pars compacta and pars reticulata.
- Pars compacta contains dopaminergic neurons.
- Pars reticulata acts as an output nucleus of basal ganglia.
- Dopamine from pars compacta acts on the striatum.
- Dopamine facilitates movement by supporting direct pathway and reducing indirect pathway activity.
- Degeneration of pars compacta causes Parkinson disease.
🔬 CONCEPT EXPLAINED
The substantia nigra is one of the most clinically important nuclei related to the basal ganglia. It is located in the midbrain and appears dark because neurons in its pars compacta contain neuromelanin pigment. It lies dorsal to the cerebral peduncle and ventral to the midbrain tegmentum.
Substantia nigra has two main parts. The pars compacta contains dopaminergic neurons that project to the striatum. This connection is called the nigrostriatal pathway. The pars reticulata acts more like an output nucleus and is functionally similar to the internal segment of globus pallidus.
Dopamine is essential for normal basal ganglia function. It does not simply “cause movement” directly. Instead, it adjusts the balance between movement-facilitating and movement-inhibiting pathways. Dopamine stimulates the direct pathway through D1 receptors and inhibits the indirect pathway through D2 receptors. Both effects favor movement.
This mechanism becomes important because movement requires both activation of desired motor programs and suppression of excessive inhibition. When dopamine is adequate, the thalamus can stimulate the motor cortex appropriately. As a result, voluntary movements become smooth, timely, and properly scaled.
If dopaminergic neurons of pars compacta degenerate, striatal dopamine falls. The direct pathway becomes underactive and the indirect pathway becomes overactive. This increases inhibition of the thalamus. As a result, the motor cortex receives reduced excitatory drive. Clinically, this produces bradykinesia, hypokinesia, rigidity, resting tremor, and postural instability, which are typical features of Parkinson disease.
⚠️ CLINICAL IMPORTANCE
Substantia nigra degeneration is the key pathological basis of Parkinson disease. The cause-effect logic is:
Loss of dopamine → reduced direct pathway activity + increased indirect pathway activity → excessive inhibition of thalamus → reduced motor cortical activation → slow and reduced movement.
This is one of the most important basal ganglia concepts for MBBS students.
ANATOMICAL AND PHYSIOLOGICAL CLASSIFICATION OF BASAL GANGLIA
🧠 CORE
- Anatomical classification is based on structural location.
- Physiological classification is based on functional role in circuits.
- Anatomical basal nuclei include caudate nucleus, lentiform nucleus, claustrum, and amygdaloid body.
- Lentiform nucleus includes putamen and globus pallidus.
- Physiological basal ganglia include striatum, globus pallidus, substantia nigra, and subthalamic nucleus.
- Striatum acts mainly as input station.
- Globus pallidus and substantia nigra pars reticulata act mainly as output stations.
- Subthalamic nucleus is important in the indirect pathway.
🔬 CONCEPT EXPLAINED
The basal ganglia can be classified in two ways because anatomy and physiology look at them from different viewpoints.
The anatomical classification focuses on deep grey matter masses in the cerebral hemisphere. In this view, the basal nuclei include the caudate nucleus, lentiform nucleus, claustrum, and amygdaloid body. The lentiform nucleus is further divided into putamen and globus pallidus. This classification is important for identifying structures on brain sections and understanding relations with the internal capsule and ventricles.
The physiological classification focuses on nuclei that participate in basal ganglia motor circuits. In this view, the important components are the striatum, globus pallidus, substantia nigra, and subthalamic nucleus. The striatum receives cortical input. The globus pallidus and substantia nigra pars reticulata provide major output. The subthalamic nucleus modifies the indirect pathway.
This difference matters because some structures are anatomically present near basal ganglia but are not central to motor circuits, while some structures outside the cerebral hemisphere, such as substantia nigra and subthalamic nucleus, are essential physiologically.
Therefore, students should remember that basal ganglia are not just a group of nuclei but a functional circuit system. Their importance lies in how information flows through them to regulate movement.
⚠️ CLINICAL IMPORTANCE
Clinical movement disorders are better understood using physiological classification. Parkinson disease is not explained simply by anatomical location; it is explained by loss of dopaminergic modulation in the functional basal ganglia circuit.
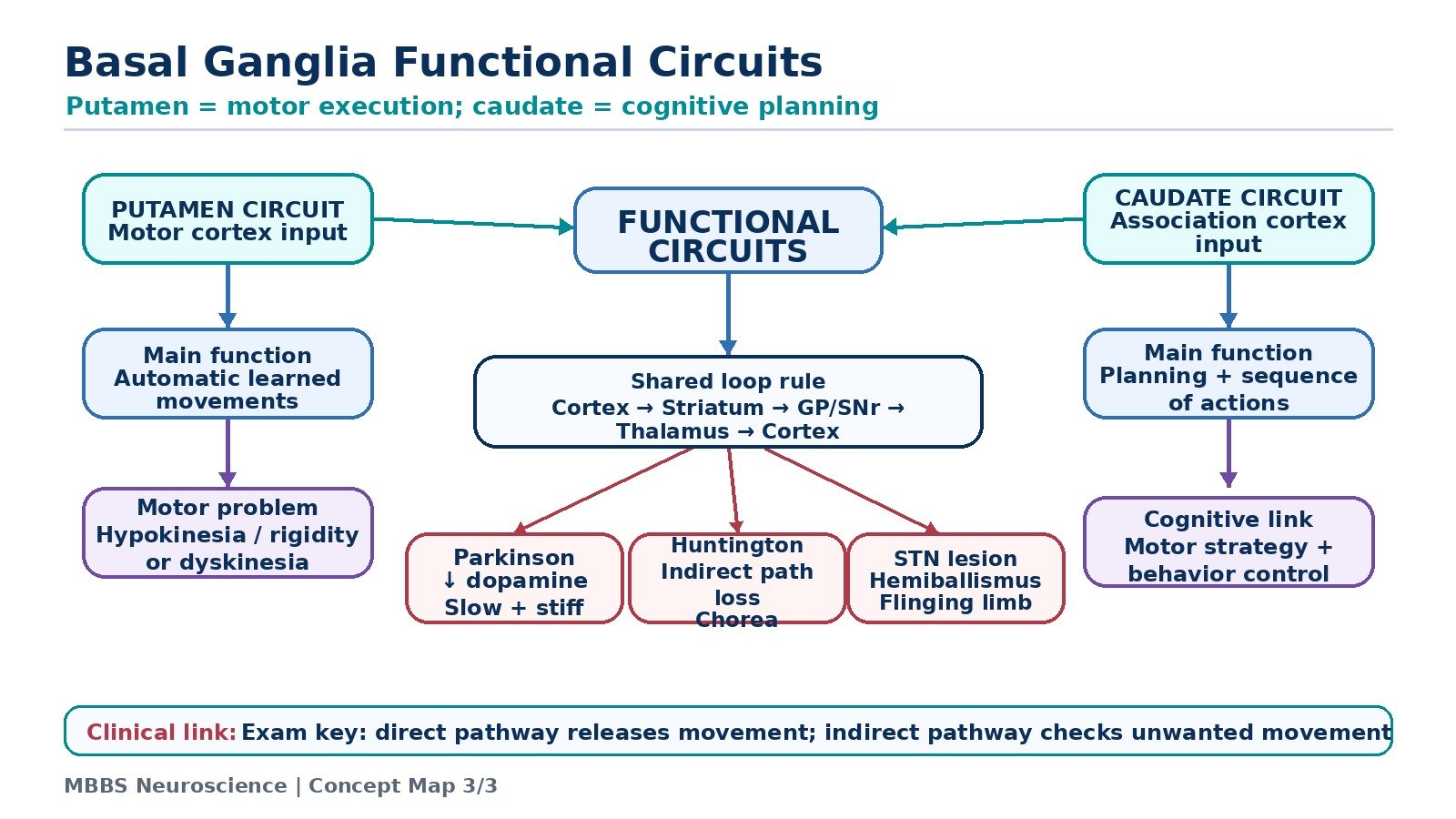
FUNCTIONAL CIRCUITS OF BASAL GANGLIA
🧠 CORE
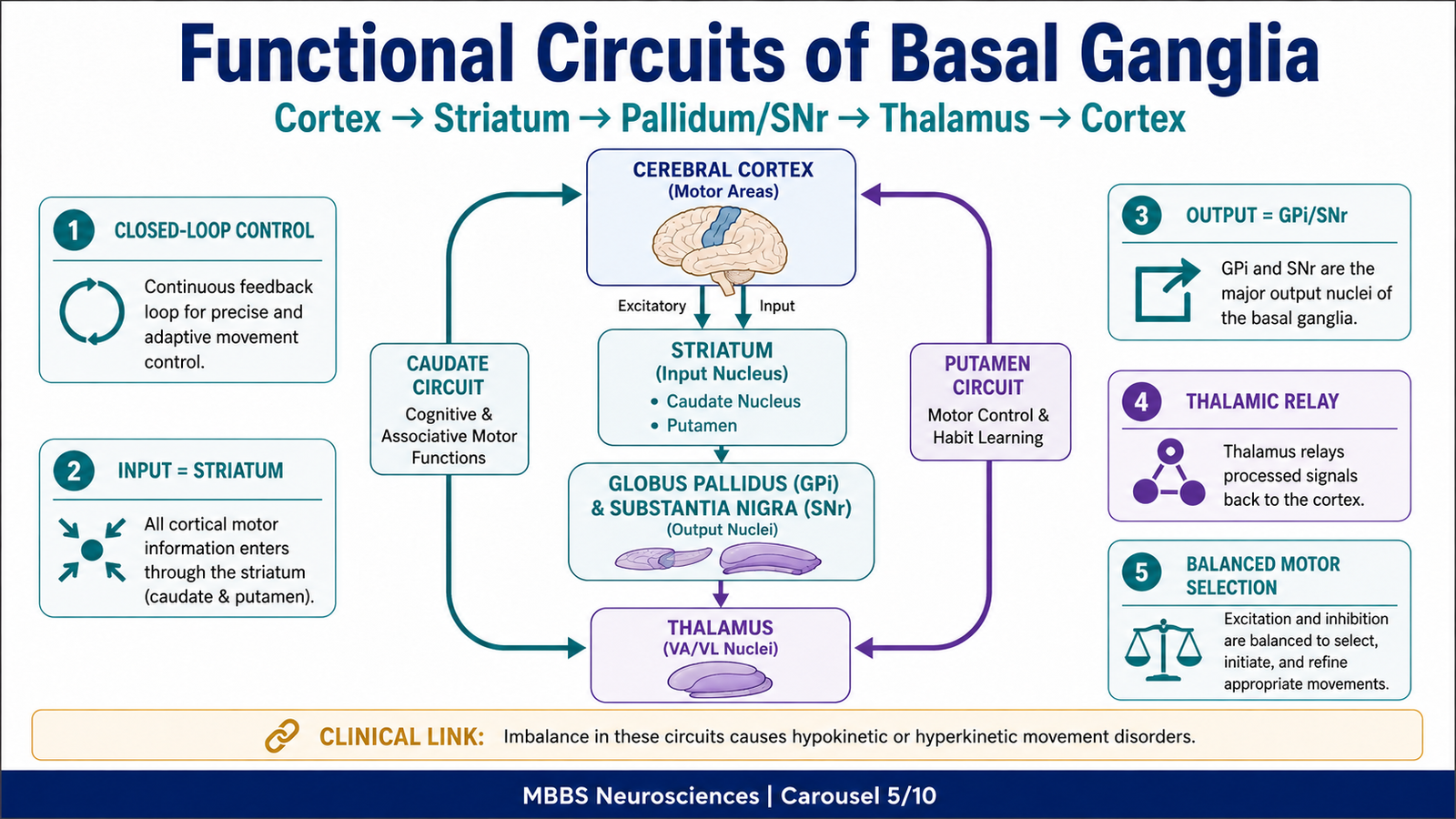
- Basal ganglia circuits are closed loops connecting cortex, basal ganglia, thalamus, and cortex again.
- Major motor circuits include putamen circuit and caudate circuit.
- The putamen circuit is mainly related to learned motor patterns.
- The caudate circuit is mainly related to cognitive planning of movement.
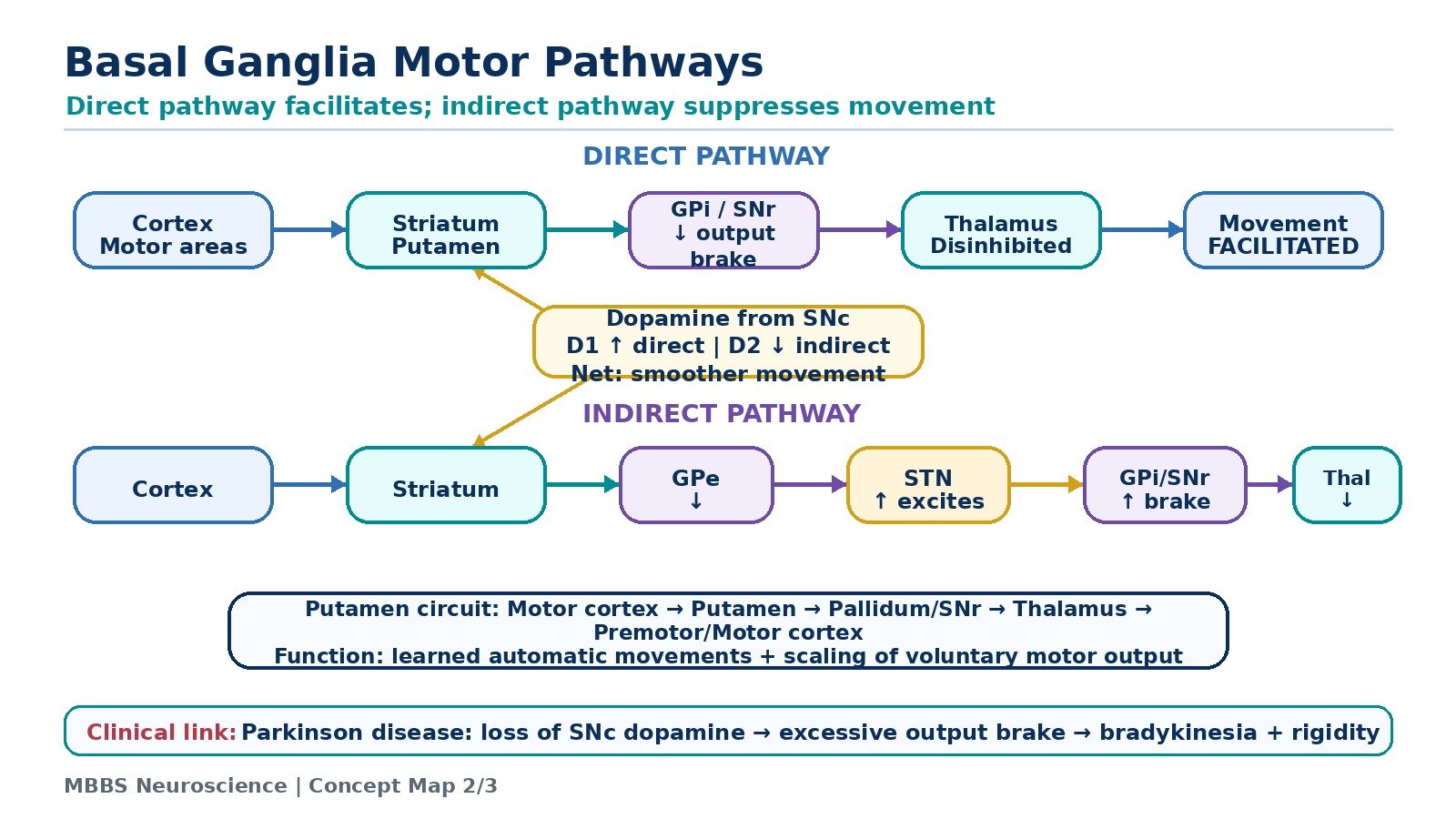
- Direct pathway facilitates desired movement.
- Indirect pathway suppresses unwanted movement.
- Dopamine modulates both direct and indirect pathways.
- Balanced activity produces smooth and purposeful movement.
🔬 CONCEPT EXPLAINED
Basal ganglia do not work as isolated nuclei. They work through functional circuits. A circuit means information starts from the cerebral cortex, passes through basal ganglia nuclei, reaches the thalamus, and returns back to the cortex. This loop allows basal ganglia to influence cortical motor output.
The general circuit is:
Cerebral cortex → Striatum → Pallidum/Substantia nigra → Thalamus → Cerebral cortex
The cerebral cortex sends excitatory signals to the striatum. The striatum processes the signal and influences globus pallidus and substantia nigra. These output nuclei regulate thalamic activity. The thalamus then excites the motor cortex. In this way, the basal ganglia decide how much motor cortex should be activated.
There are two major motor-related circuits. The putamen circuit begins mainly from motor and premotor cortical areas and passes through the putamen. It is concerned with execution of learned motor patterns. The caudate circuit begins from association areas of the cortex and passes through the caudate nucleus. It is concerned with planning, sequencing, and cognitive control of movement.
The direct and indirect pathways are not separate actions of the body; they are internal processing routes within the basal ganglia. The direct pathway reduces inhibition of thalamus and facilitates movement. The indirect pathway increases inhibition of thalamus and suppresses unwanted movement. Normal movement depends on a balance between these two systems.
⚠️ CLINICAL IMPORTANCE
If the movement-facilitating system is weak, movement becomes slow and reduced, as in Parkinson disease. If the movement-suppressing system is weak, unwanted movements appear, as in chorea or hemiballismus.
DIRECT AND INDIRECT PATHWAYS OF BASAL GANGLIA
🧠 CORE
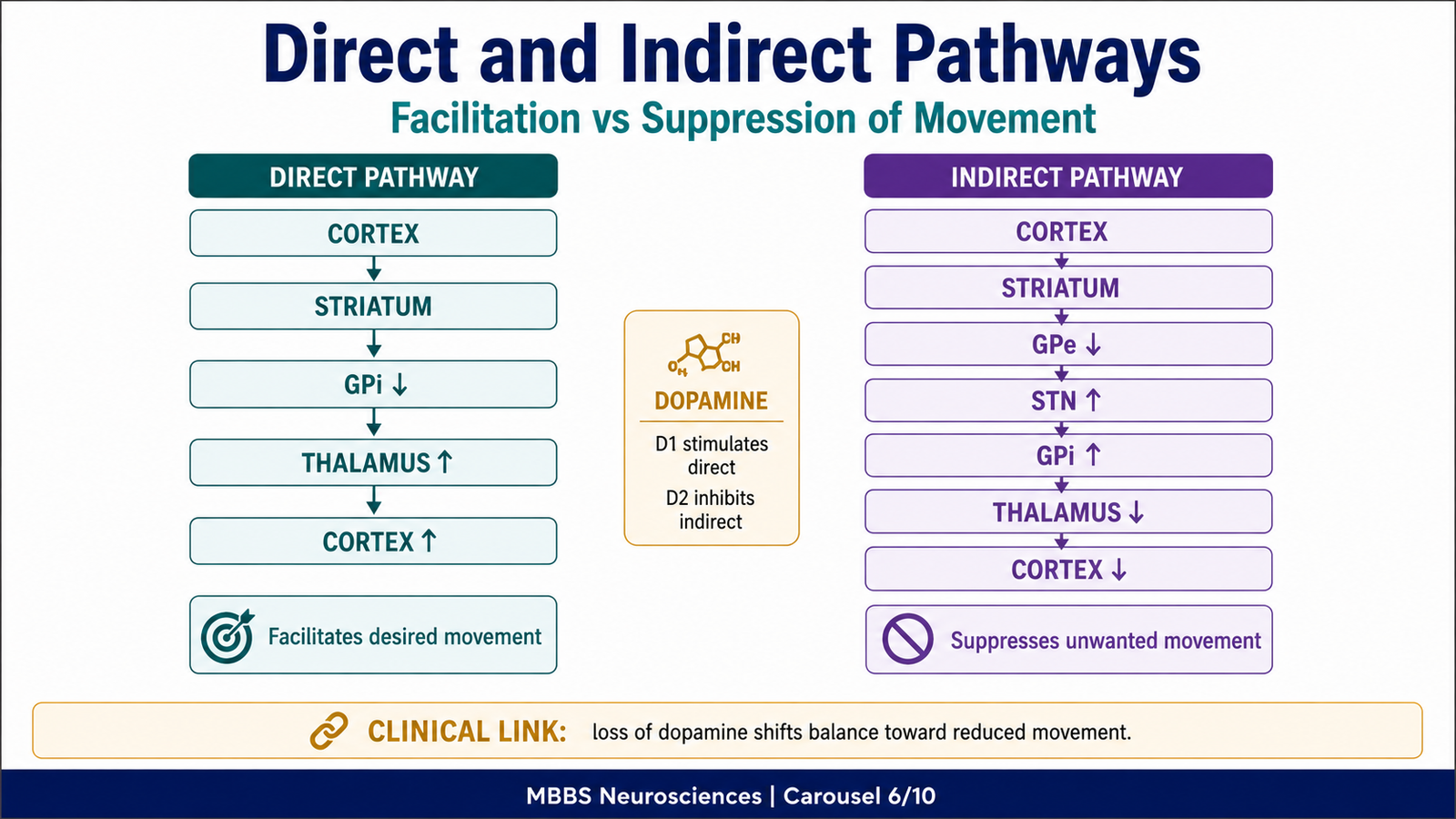
- Direct pathway facilitates desired movement.
- Indirect pathway suppresses unwanted movement.
- Both pathways begin from cortex and striatum.
- Direct pathway inhibits internal globus pallidus.
- This reduces inhibition of thalamus.
- Indirect pathway increases activity of internal globus pallidus.
- This increases inhibition of thalamus.
- Dopamine promotes movement by enhancing direct pathway and reducing indirect pathway.
🔬 CONCEPT EXPLAINED
To understand basal ganglia physiology, the direct and indirect pathways must be understood as a balance between releasing movement and braking movement.
Direct Pathway
The direct pathway exists to facilitate desired movement. When the cerebral cortex plans a movement, it sends excitatory input to the striatum. The striatum then inhibits the internal segment of globus pallidus. Normally, the internal globus pallidus inhibits the thalamus. Therefore, when the striatum inhibits the internal globus pallidus, the thalamus is released from inhibition.
This is called disinhibition. The thalamus can now excite the motor cortex more strongly. As a result, the selected movement is facilitated.
The sequence is:
Cortex excites striatum → striatum inhibits internal globus pallidus → internal globus pallidus inhibits thalamus less → thalamus excites motor cortex more → desired movement increases.
The physiological advantage of this pathway is that useful motor programs can be selected and released efficiently.
Indirect Pathway
The indirect pathway exists to suppress unwanted movement. In this pathway, the cortex excites the striatum. The striatum inhibits the external segment of globus pallidus. Normally, the external globus pallidus inhibits the subthalamic nucleus. When the external globus pallidus is inhibited, the subthalamic nucleus becomes more active.
The subthalamic nucleus then excites the internal globus pallidus. The internal globus pallidus increases inhibition of the thalamus. As a result, thalamic excitation of motor cortex decreases, and unwanted movement is suppressed.
The sequence is:
Cortex excites striatum → striatum inhibits external globus pallidus → subthalamic nucleus becomes more active → subthalamic nucleus excites internal globus pallidus → internal globus pallidus strongly inhibits thalamus → motor cortex receives less excitation → unwanted movement decreases.
The physiological advantage of this pathway is that competing or inappropriate motor programs are prevented from appearing.
Dopamine Modulation
Dopamine from substantia nigra pars compacta modulates both pathways. It stimulates D1 receptors in the direct pathway, increasing movement facilitation. It inhibits D2 receptors in the indirect pathway, reducing excessive movement suppression. Therefore, dopamine has an overall movement-promoting effect.
⚠️ CLINICAL IMPORTANCE
Loss of dopamine in Parkinson disease reduces direct pathway activity and increases indirect pathway activity. Both changes reduce thalamic excitation of motor cortex. This produces slow movement, reduced facial expression, rigidity, and difficulty initiating movement.
Damage to the subthalamic nucleus reduces indirect pathway braking. This causes excessive movement, especially hemiballismus.
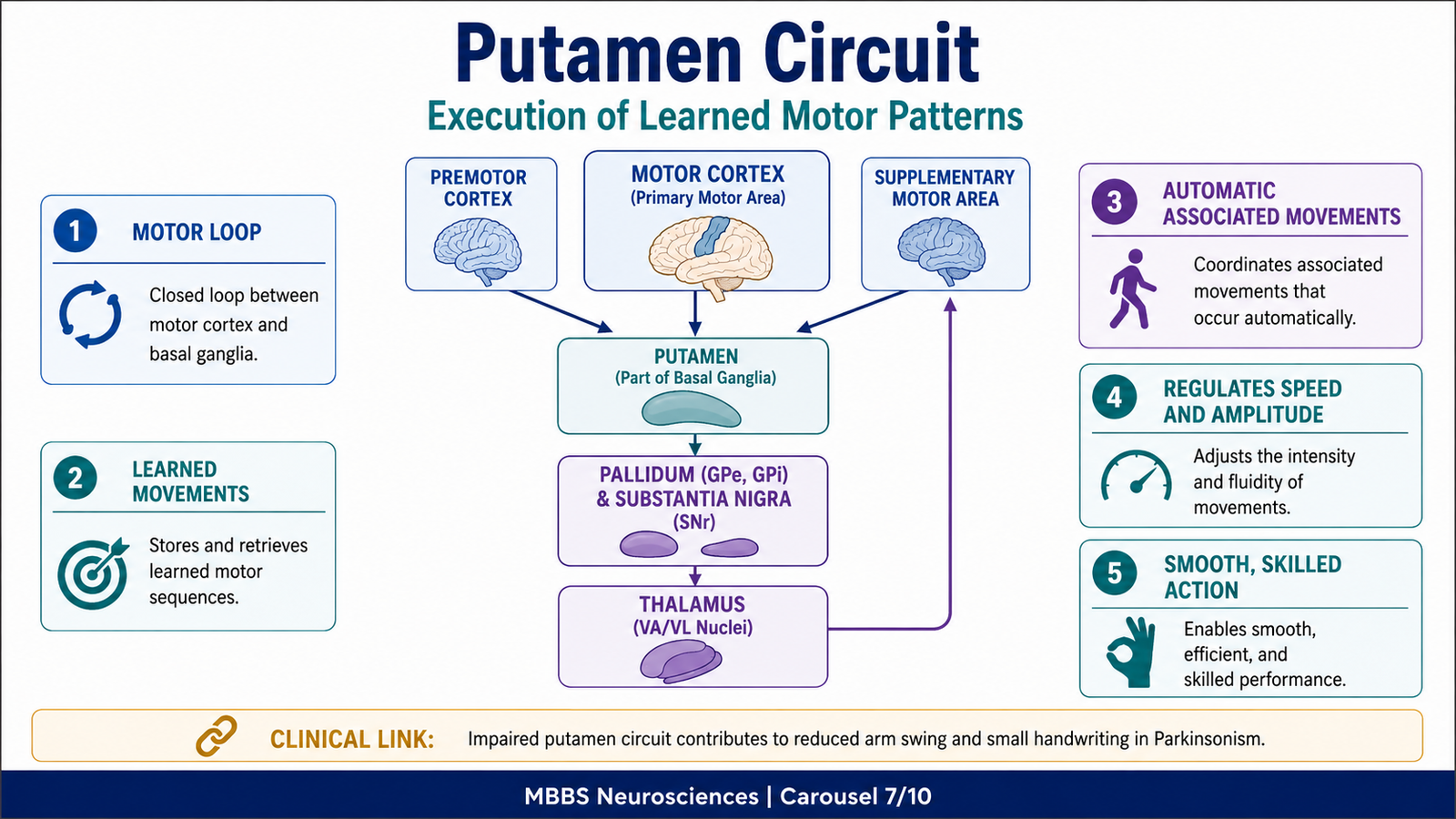
PUTAMEN CIRCUIT: CONNECTIONS AND FUNCTIONS
🧠 CORE
- Putamen circuit is mainly a motor circuit.
- It begins from motor, premotor, and supplementary motor cortices.
- Signals pass to putamen.
- Putamen influences globus pallidus and substantia nigra.
- Output passes to thalamus.
- Thalamus projects back to motor cortical areas.
- It controls learned and automatic motor patterns.
- It helps regulate timing, amplitude, direction, and smoothness of movement.
🔬 CONCEPT EXPLAINED
The putamen circuit is the basal ganglia circuit most directly related to execution of learned motor activity. It is especially important for movements that become smooth and automatic after practice.
The circuit begins in motor-related cortical areas, including the primary motor cortex, premotor cortex, and supplementary motor area. These cortical areas send excitatory signals to the putamen. The putamen processes this information and sends signals through basal ganglia output pathways involving globus pallidus and substantia nigra. The processed output reaches the thalamus, which then projects back to motor cortical areas.
The functional logic of the putamen circuit is that learned motor programs must be selected and scaled properly. For example, writing, typing, speaking, walking, and using instruments all require repeated learned patterns. Once learned, these movements should not require continuous conscious control of every small muscle contraction. The putamen circuit helps release these patterns smoothly.
This circuit also helps determine the amplitude, speed, direction, and timing of movement. If a person wants to move the hand toward a target, the movement must not be too weak, too strong, too slow, too fast, or interrupted by unnecessary muscle activity. The putamen circuit helps regulate these features.
The putamen circuit also contributes to automatic associated movements. For example, during walking, the arms swing rhythmically without conscious effort. In Parkinson disease, this automatic arm swing is reduced because basal ganglia motor regulation is impaired.
⚠️ CLINICAL IMPORTANCE
Damage or dysfunction of the putamen circuit causes problems in learned motor activity. Movements may become slow, rigid, poorly scaled, or abnormal. Parkinsonian features such as reduced arm swing, masked face, difficulty initiating walking, and small handwriting reflect impaired basal ganglia regulation of learned and automatic motor patterns.
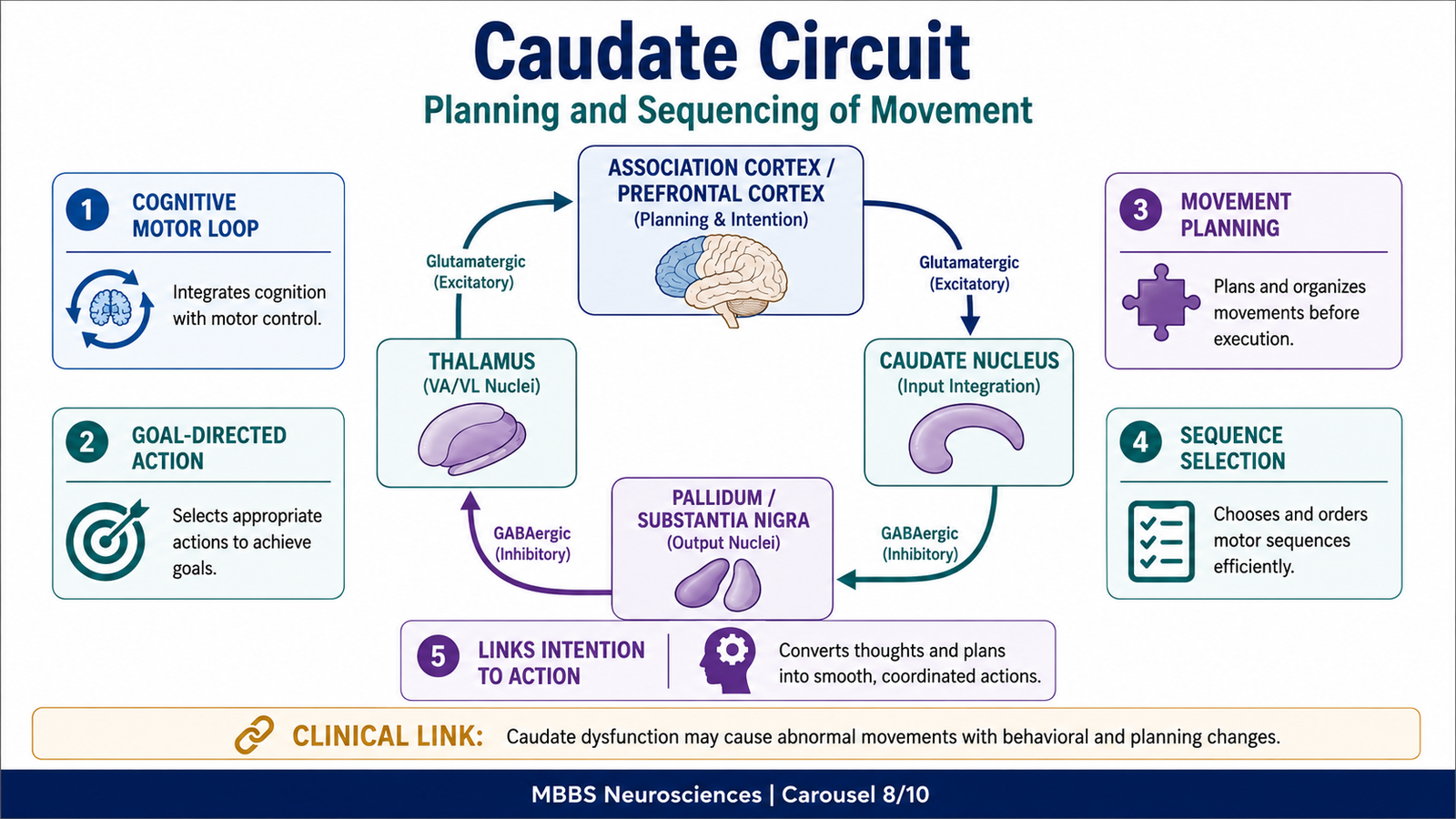
CAUDATE CIRCUIT: CONNECTIONS AND FUNCTIONS
🧠 CORE
- Caudate circuit is mainly a cognitive motor planning circuit.
- It begins from association areas of cerebral cortex.
- Signals pass to caudate nucleus.
- Caudate output influences globus pallidus and substantia nigra.
- Output passes through thalamus back to prefrontal and motor planning areas.
- It helps plan sequential movement.
- It links thought, intention, and motor action.
- It is important for goal-directed behavior.
🔬 CONCEPT EXPLAINED
The caudate circuit is different from the putamen circuit because it is more related to planning and cognitive control of movement rather than direct execution of learned motor patterns.
The caudate nucleus receives input from association areas of the cerebral cortex. These areas are involved in thinking, planning, sensory interpretation, decision-making, and goal-directed behavior. From the caudate nucleus, information passes through basal ganglia output nuclei and then reaches the thalamus. The thalamus projects back mainly to prefrontal and motor planning areas of the cortex.
The body needs this circuit because many movements begin as ideas or intentions before becoming motor commands. For example, deciding to stand up, walk to a shelf, pick a book, and open it requires planning a sequence of actions. The caudate circuit helps convert cognitive intention into organized motor behavior.
The caudate circuit is especially important in selecting the correct motor plan according to context. A person may know many possible actions, but only one action may be appropriate at a particular time. The caudate circuit helps choose the correct sequence and suppress inappropriate alternatives.
This circuit is also important for behavioral flexibility. If the environment changes, the motor plan must be adjusted. The caudate circuit helps link sensory information, decision-making, and action planning.
⚠️ CLINICAL IMPORTANCE
Caudate dysfunction may produce abnormal involuntary movements and disorganized motor behavior. In Huntington disease, degeneration involving the striatum, especially caudate-related circuits, causes choreiform movements and cognitive-behavioral changes. At MBBS level, the key concept is that caudate circuit is related not only to movement but also to planning and behavioral control of movement.
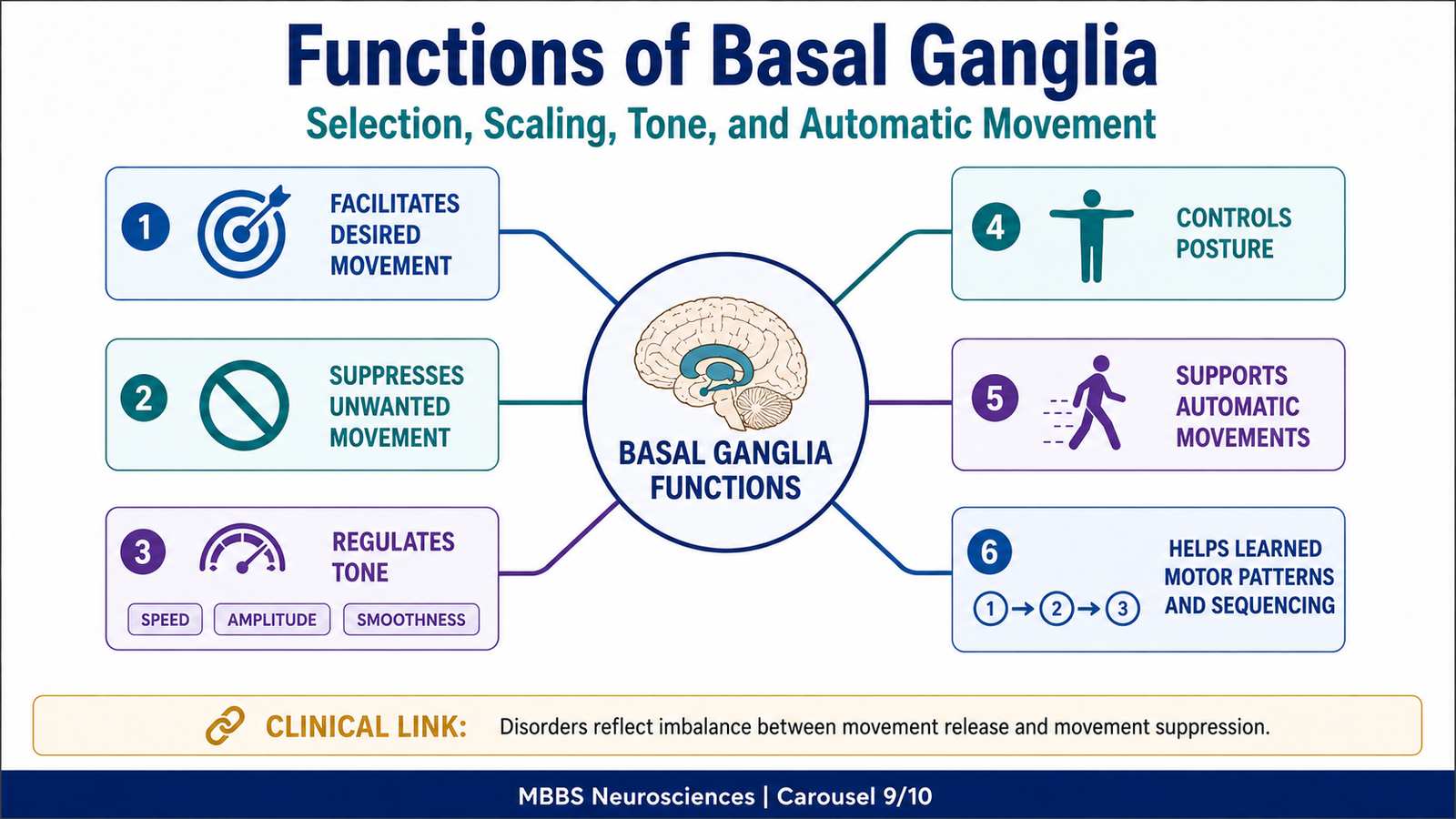
FUNCTIONS OF BASAL GANGLIA
🧠 CORE
- Basal ganglia facilitate desired voluntary movement.
- They suppress unwanted motor activity.
- They regulate muscle tone.
- They help control posture.
- They support automatic associated movements.
- They help execute learned motor programs.
- They contribute to planning and sequencing of movement.
- They help scale force, speed, and amplitude of movement.
🔬 CONCEPT EXPLAINED
The functions of basal ganglia can be understood by asking: what problems would occur if the brain could command movement but could not properly select, regulate, or suppress motor programs?
First, basal ganglia help in initiation and facilitation of desired movement. They allow the motor cortex to become active enough for a selected movement. This does not mean that basal ganglia directly activate muscles. Rather, they regulate how strongly the motor cortex is allowed to act.
Second, basal ganglia help in suppression of unwanted movement. During any action, many competing motor patterns must be inhibited. If this suppression fails, involuntary movements appear.
Third, basal ganglia regulate muscle tone and posture. Normal posture requires background muscle activity, not complete relaxation. Basal ganglia help maintain appropriate tone so that movement can occur smoothly from a stable base.
Fourth, basal ganglia control automatic associated movements. These are movements that accompany voluntary activity without conscious effort, such as arm swinging while walking or facial expression during emotional speech. In Parkinson disease, these automatic movements are reduced.
Fifth, basal ganglia help in learned motor patterns. Repeated actions become smoother and more automatic through basal ganglia circuits. This is why activities like writing, typing, driving, and speaking become more efficient with practice.
Sixth, basal ganglia help in motor planning and sequencing, especially through the caudate circuit. Movement is not always a single action; it often requires a sequence. Basal ganglia help arrange these sequences in a meaningful order.
Therefore, basal ganglia function is best summarized as motor programming, selection, scaling, inhibition, and automation.
⚠️ CLINICAL IMPORTANCE
Basal ganglia lesions produce characteristic movement disorders. Reduced movement suggests excessive inhibition of motor cortex, while excessive involuntary movement suggests failure of inhibitory control. This cause-effect relationship is essential for understanding basal ganglia clinical problems.
CLINICAL PROBLEMS RELATED TO BASAL GANGLIA
🧠 CORE
- Basal ganglia disorders commonly produce abnormal movements.
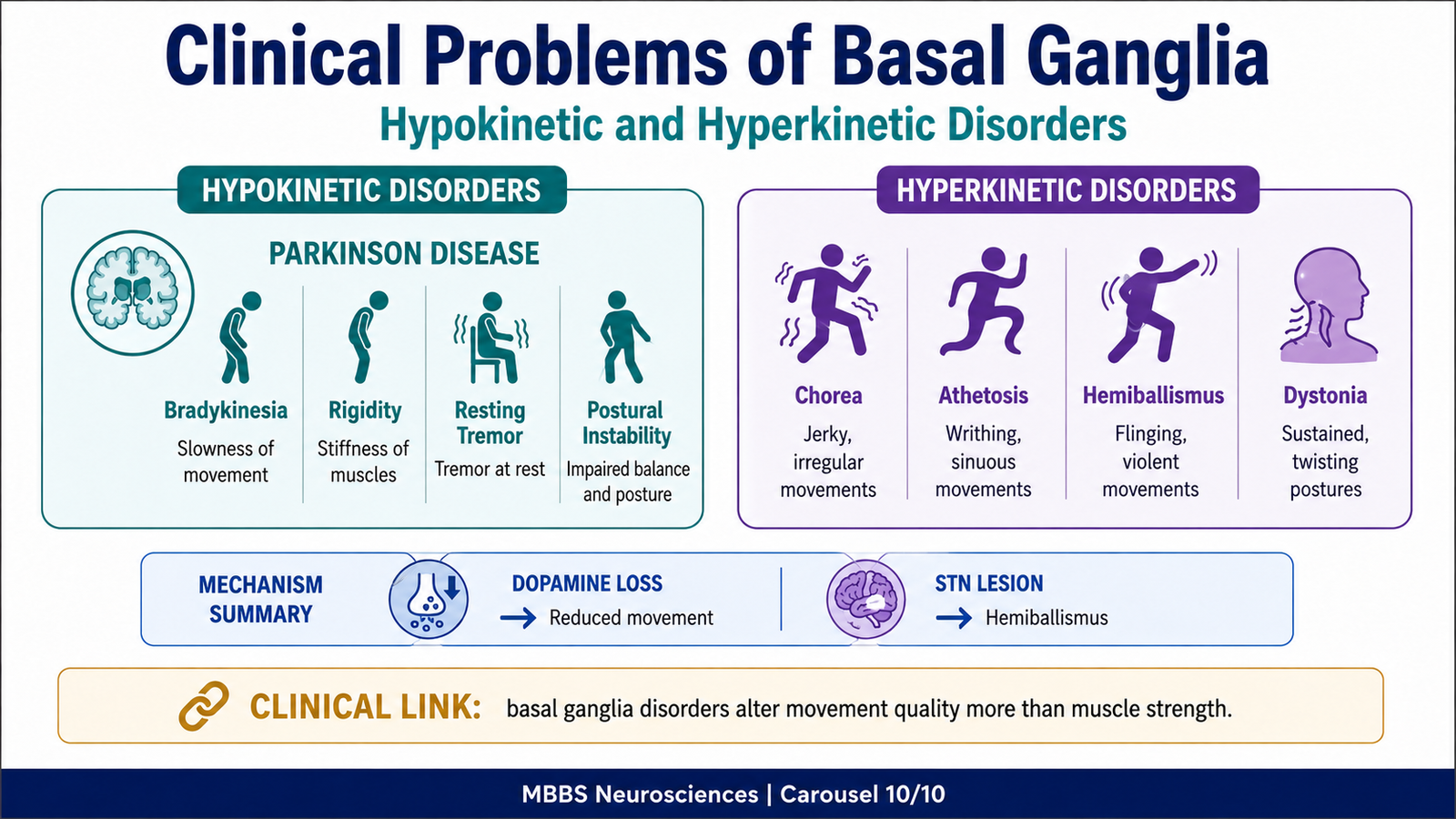
- Parkinson disease causes hypokinesia, bradykinesia, rigidity, resting tremor, and postural instability.
- Chorea causes rapid, irregular, purposeless movements.
- Athetosis causes slow writhing movements.
- Hemiballismus causes violent flinging movements.
- Dystonia causes sustained abnormal posture or twisting movements.
- Basal ganglia lesions usually do not cause primary paralysis.
- Clinical features depend on whether movement facilitation or movement inhibition is disturbed.
🔬 CONCEPT EXPLAINED
Basal ganglia clinical disorders are best understood through pathway imbalance.
Parkinson Disease
Parkinson disease occurs due to degeneration of dopaminergic neurons in substantia nigra pars compacta. Dopamine normally facilitates movement by stimulating the direct pathway and inhibiting the indirect pathway. When dopamine is lost, the direct pathway becomes weak and the indirect pathway becomes overactive. This causes excessive inhibition of the thalamus.
As a result, the motor cortex receives less excitatory input. The patient develops bradykinesia, which means slow movement, and hypokinesia, which means reduced movement. Rigidity occurs because tone regulation is disturbed. Resting tremor occurs due to abnormal oscillatory activity in motor circuits. Postural instability occurs because automatic postural adjustments become defective.
Common features include mask-like face, reduced arm swing, shuffling gait, difficulty initiating movement, cogwheel rigidity, and resting tremor.
Chorea
Chorea consists of rapid, irregular, jerky, purposeless movements. It occurs when basal ganglia fail to suppress unwanted motor programs. Huntington disease is a classic example. At undergraduate level, students should understand that chorea reflects excessive unwanted movement due to defective inhibitory control.
Athetosis
Athetosis consists of slow, writhing movements, commonly affecting distal limbs. It reflects abnormal basal ganglia control of sustained motor activity and posture.
Hemiballismus
Hemiballismus is characterized by violent flinging movements, usually affecting one side of the body. It classically occurs due to lesion of the contralateral subthalamic nucleus. The mechanism is loss of indirect pathway braking. When the subthalamic nucleus is damaged, it cannot excite the internal globus pallidus effectively. Thalamic inhibition decreases, motor cortex becomes overactive, and large involuntary movements occur.
Dystonia
Dystonia consists of sustained involuntary muscle contractions causing twisting movements or abnormal postures. It reflects abnormal basal ganglia regulation of tone and movement pattern selection.
⚠️ CLINICAL IMPORTANCE
Basal ganglia disorders are often classified into:
- Hypokinetic disorders: Movement is reduced, as in Parkinson disease.
- Hyperkinetic disorders: Movement is excessive, as in chorea, athetosis, dystonia, and hemiballismus.
This classification is clinically useful because it links symptoms directly to basal ganglia pathway imbalance.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Function | Outcome |
|---|---|---|
| Caudate nucleus | Cognitive planning and sequencing of movement | Helps convert intention into organized motor action |
| Putamen | Learned motor pattern control | Smooth execution of automatic and practiced movements |
| Globus pallidus internal segment | Major inhibitory output to thalamus | Regulates how much motor cortex is activated |
| Globus pallidus external segment | Part of indirect pathway | Helps suppress unwanted movements |
| Subthalamic nucleus | Excites internal globus pallidus | Strengthens movement inhibition |
| Substantia nigra pars compacta | Dopamine supply to striatum | Facilitates movement |
| Substantia nigra pars reticulata | Output nucleus similar to globus pallidus internal segment | Helps regulate thalamic and brainstem motor activity |
| Red nucleus | Brainstem motor coordination | Links cerebellar and motor control pathways |
| Thalamus | Relay back to motor cortex | Modifies cortical motor output |
| Motor cortex | Final cortical motor planning and execution | Produces voluntary movement through descending pathways |
The basal ganglia system is therefore an integrated motor control loop. The cortex proposes a movement, the basal ganglia select and regulate it, the thalamus feeds the processed signal back to cortex, and the cortex sends final motor commands through descending pathways.
🩺 5️⃣ Clinical Correlation
Parkinson Disease
- Cause: Degeneration of dopaminergic neurons in substantia nigra pars compacta.
- Mechanism: Reduced dopamine causes decreased direct pathway activity and increased indirect pathway activity.
- Effect: Excessive inhibition of thalamus reduces motor cortical activation.
- Clinical features: Bradykinesia, rigidity, resting tremor, mask-like face, reduced arm swing, shuffling gait, postural instability.
- Exam concept: Parkinson disease is a hypokinetic basal ganglia disorder.
Chorea
- Cause: Dysfunction of striatal inhibitory control, classically seen in Huntington disease.
- Mechanism: Failure to suppress unwanted motor programs.
- Effect: Excessive irregular movements appear.
- Clinical features: Rapid, jerky, purposeless movements.
- Exam concept: Chorea is a hyperkinetic movement disorder.
Athetosis
- Cause: Basal ganglia dysfunction affecting sustained motor control.
- Mechanism: Abnormal regulation of slow motor activity and posture.
- Effect: Slow writhing involuntary movements.
- Clinical features: Snake-like movements, commonly of hands and fingers.
- Exam concept: Athetosis is slower than chorea.
Hemiballismus
- Cause: Lesion of contralateral subthalamic nucleus.
- Mechanism: Reduced activation of internal globus pallidus causes reduced thalamic inhibition.
- Effect: Motor cortex becomes excessively active.
- Clinical features: Violent flinging movements of limbs on one side.
- Exam concept: Subthalamic nucleus lesion causes hemiballismus.
Dystonia
- Cause: Abnormal basal ganglia regulation of tone and posture.
- Mechanism: Sustained involuntary muscle contraction.
- Effect: Twisting movements or abnormal posture.
- Clinical features: Neck twisting, abnormal limb posture, sustained spasms.
- Exam concept: Dystonia reflects abnormal tone and motor pattern control.
📌 6️⃣ Summary Points
- Basal ganglia regulate movement indirectly by influencing the motor cortex through the thalamus.
- They do not directly supply lower motor neurons; therefore, lesions usually cause movement disorders rather than simple paralysis.
- Corpus striatum consists of caudate nucleus and lentiform nucleus.
- Lentiform nucleus consists of putamen and globus pallidus.
- Striatum means caudate nucleus plus putamen and acts mainly as the input station of basal ganglia.
- Globus pallidus internal segment and substantia nigra pars reticulata are major output nuclei.
- Direct pathway facilitates desired movement by disinhibiting the thalamus.
- Indirect pathway suppresses unwanted movement by increasing inhibition of the thalamus.
- Dopamine from substantia nigra pars compacta promotes movement by stimulating the direct pathway and inhibiting the indirect pathway.
- Putamen circuit controls learned and automatic motor patterns.
- Caudate circuit controls cognitive planning and sequencing of movement.
- Parkinson disease is due to loss of nigrostriatal dopamine and causes hypokinetic features.
- Subthalamic nucleus lesion causes hemiballismus due to loss of movement suppression.
- Hyperkinetic basal ganglia disorders include chorea, athetosis, dystonia, and hemiballismus.
- The key basal ganglia principle is: desired movement is released, unwanted movement is suppressed.