
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
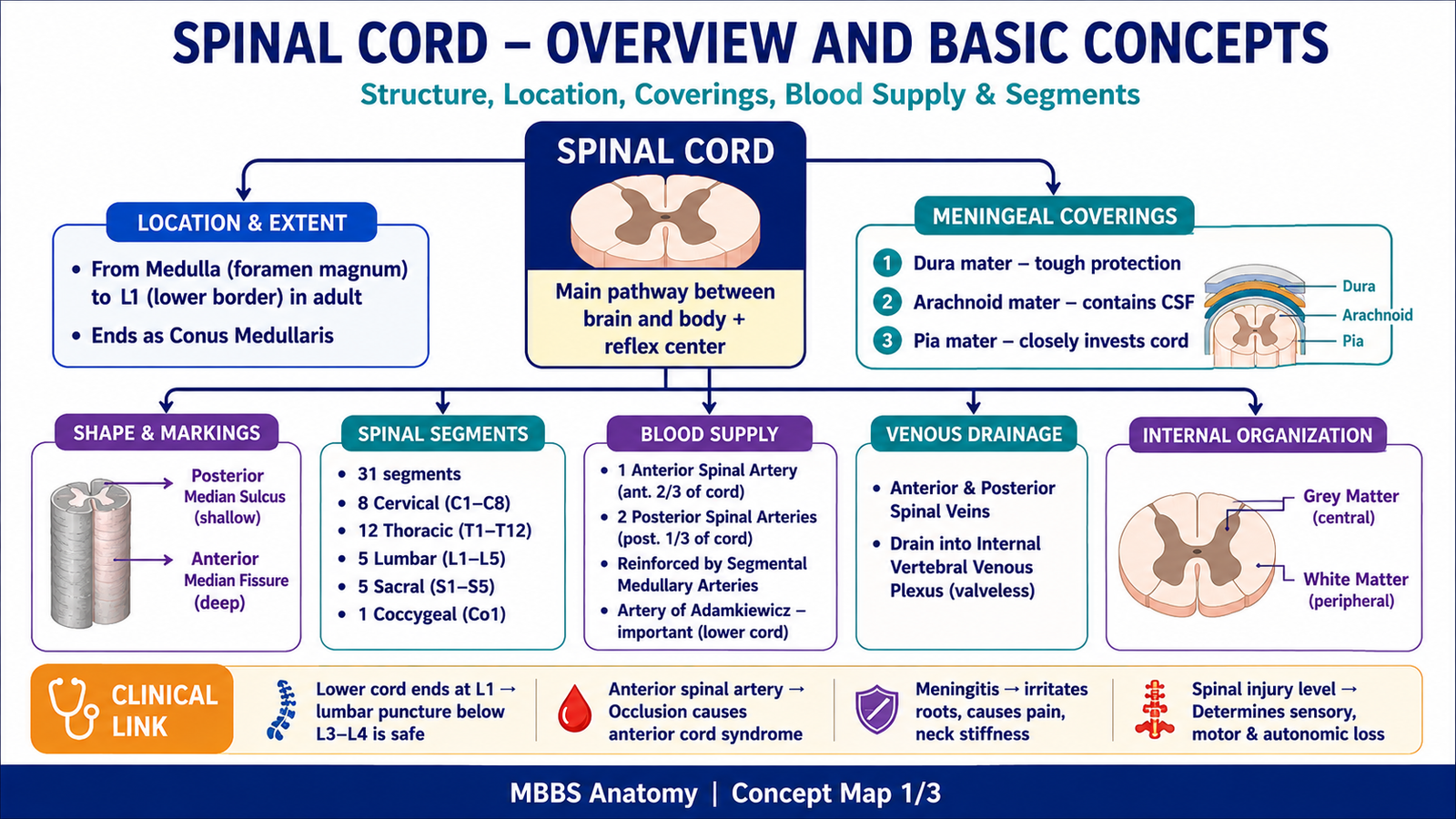
The spinal cord is the long cylindrical part of the central nervous system present inside the vertebral canal. It acts as the main pathway between the brain and the body, carrying sensory information upward and motor commands downward. It also serves as an important reflex center, allowing rapid protective responses without waiting for conscious brain processing.
Anatomically, the spinal cord extends from the medulla oblongata at the foramen magnum to approximately the lower border of the L1 vertebra in adults. It is protected by the vertebral column, meninges, cerebrospinal fluid, and vascular supply. Clinically, spinal cord injury is important because damage at different levels produces characteristic sensory loss, motor weakness, reflex changes, and autonomic dysfunction.
To understand the spinal cord properly, students must link its gross anatomy, internal grey and white matter organization, microscopic appearance at different levels, embryological development, ascending sensory tracts, descending motor tracts, and clinical consequences of lesions.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Spinal cord: Cylindrical part of the CNS present in the vertebral canal, responsible for sensory conduction, motor conduction, and reflex activity.
- Grey matter: Central H-shaped area containing neuronal cell bodies, dendrites, synapses, and neuroglia.
- White matter: Peripheral area containing myelinated ascending and descending nerve fibers.
- Anterior horn: Ventral grey matter containing lower motor neurons supplying skeletal muscles.
- Posterior horn: Dorsal grey matter receiving sensory input.
- Lateral horn: Autonomic grey matter, prominent mainly in thoracic and upper lumbar segments.
- Ascending tracts: White matter pathways carrying sensory impulses from the body to the brain.
- Descending tracts: White matter pathways carrying motor commands from the brain to the spinal cord.
- Pyramidal tracts: Corticospinal motor pathways controlling voluntary skilled movements.
- Extrapyramidal tracts: Descending pathways controlling posture, tone, balance, and automatic movements.
- Rexed laminae: Functional layers of spinal grey matter arranged according to neuronal groups.
- Alar plate: Dorsal embryological region of neural tube forming sensory parts of spinal cord.
- Basal plate: Ventral embryological region of neural tube forming motor parts of spinal cord.
Essential Terminology
- Anterior median fissure: Deep groove on the anterior surface of spinal cord.
- Posterior median sulcus: Shallow groove on posterior surface.
- Central canal: Small canal in grey matter containing CSF, lined by ependymal cells.
- Funiculus: Column of white matter; anterior, lateral, or posterior.
- Rootlets: Small nerve fibers forming anterior and posterior roots.
- Spinal segment: Part of spinal cord giving rise to one pair of spinal nerves.
- Decussation: Crossing of nerve fibers from one side to the other.
- Somatotopy: Ordered arrangement of body regions within neural pathways.
Basic Overview
- The spinal cord has 31 segments: 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, and 1 coccygeal.
- It is shorter than the vertebral canal in adults, so lower spinal nerve roots descend as the cauda equina.
- Grey matter is central and white matter is peripheral.
- Sensory information enters through posterior roots.
- Motor information exits through anterior roots.
- Ascending tracts carry touch, proprioception, pain, and temperature.
- Descending tracts control voluntary movement, posture, tone, and reflex modulation.
- Embryologically, the dorsal alar plate becomes sensory, while the ventral basal plate becomes motor.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPT 1: Gross Anatomy of the Spinal Cord
🧠 CORE
- The spinal cord is a cylindrical CNS structure located within the vertebral canal.
- It extends from the medulla oblongata to the lower border of L1 vertebra in adults.
- It has cervical and lumbosacral enlargements for limb innervation.
- Its surface shows anterior median fissure and posterior median sulcus.
- It is divided into spinal segments giving rise to spinal nerves.
- Grey matter lies centrally and white matter peripherally.
- The cord is protected by vertebrae, meninges, CSF, and blood supply.
🔬 CONCEPT EXPLAINED
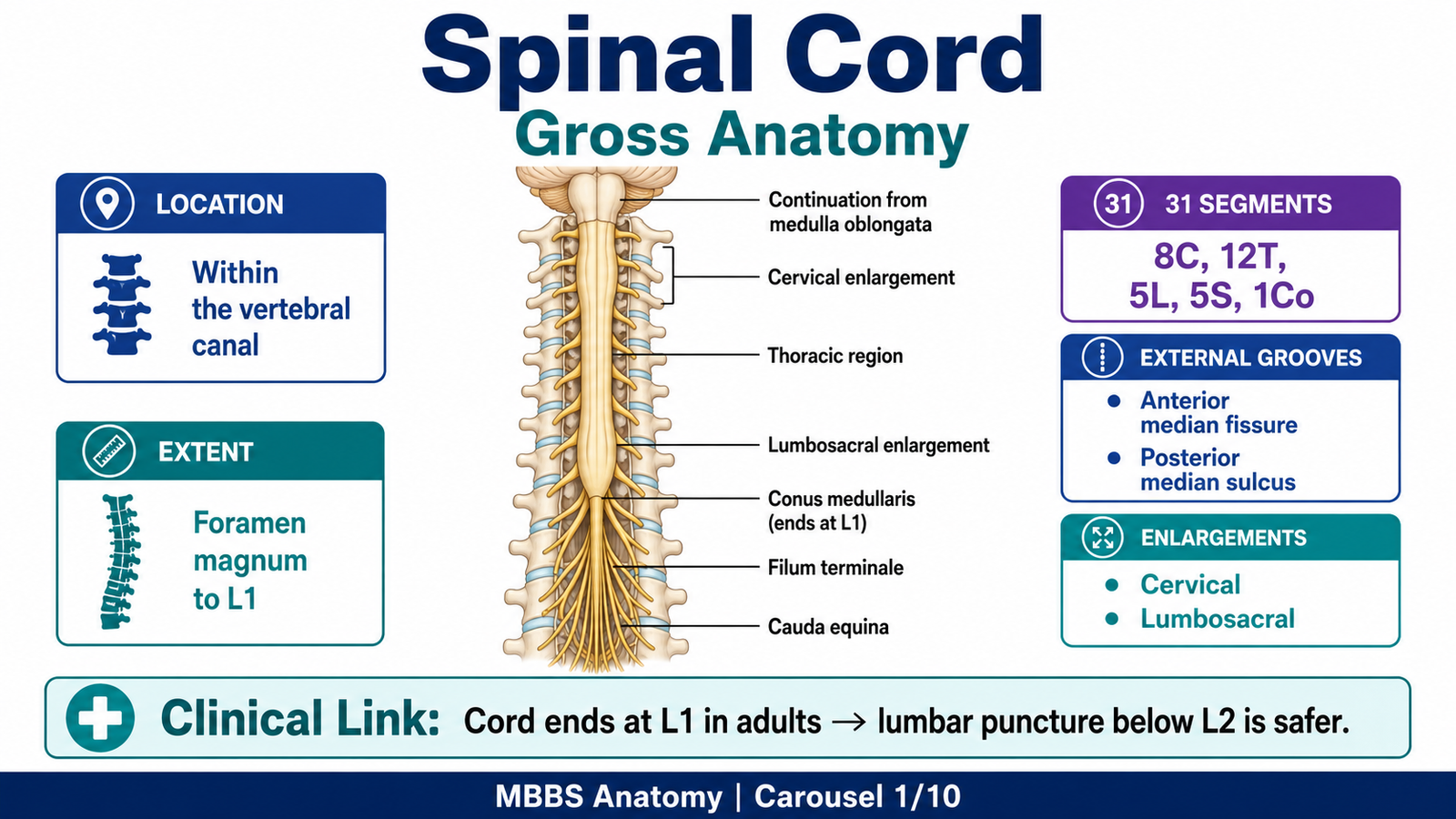
The spinal cord is the main communication cable between the brain and the body. It is continuous superiorly with the medulla oblongata at the foramen magnum and ends inferiorly as the conus medullaris around the lower border of the first lumbar vertebra in adults. From the conus medullaris, a delicate fibrous strand called the filum terminale descends to anchor the cord inferiorly.
The cord is not uniform in thickness. It has two important enlargements: the cervical enlargement and the lumbosacral enlargement. These enlargements exist because more neurons and nerve fibers are needed to supply the upper and lower limbs. Therefore, structure directly supports function: regions supplying limbs require more grey matter for motor neurons and more white matter for sensory and motor pathways.
Externally, the spinal cord has important grooves and sulci. The anterior median fissure is a deep groove on the anterior surface, while the posterior median sulcus is a shallower groove on the posterior surface. These markings help divide the cord into right and left halves and also help orient the cord in transverse sections.
The spinal cord is organized into 31 segments, and each segment gives rise to a pair of spinal nerves. These segments are cervical, thoracic, lumbar, sacral, and coccygeal. However, because the vertebral column grows faster than the spinal cord during development, the spinal cord ends higher than the vertebral canal. As a result, lower lumbar and sacral nerve roots descend within the vertebral canal before exiting, forming the cauda equina.
⚠️ CLINICAL IMPORTANCE
A spinal cord lesion produces signs according to the level of injury. For example, cervical cord injury may affect all four limbs, while lumbar or sacral lesions mainly affect lower limbs and pelvic functions. Because lower nerve roots descend as the cauda equina, lumbar puncture is safely performed below the end of the spinal cord, usually at L3–L4 or L4–L5.
MAJOR CONCEPT 2: Meningeal Coverings and Protection of the Spinal Cord
🧠 CORE
- The spinal cord is covered by three meninges: dura mater, arachnoid mater, and pia mater.
- Spinal dura forms a protective dural sac.
- Arachnoid mater encloses the subarachnoid space containing CSF.
- Pia mater closely invests the spinal cord surface.
- Denticulate ligaments stabilize the cord laterally.
- Filum terminale anchors the cord inferiorly.
- Meninges protect the cord from mechanical injury.
🔬 CONCEPT EXPLAINED
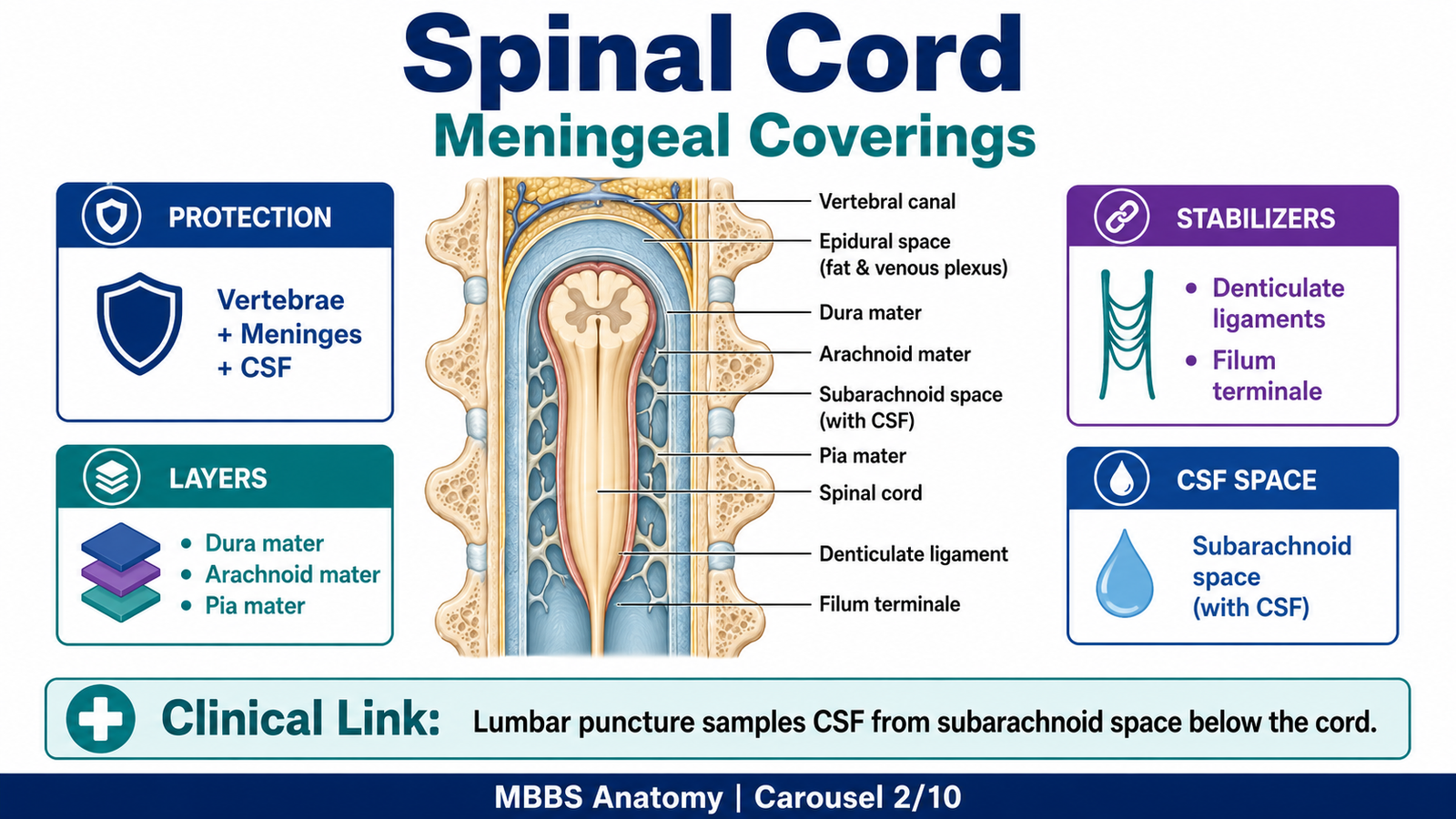
The spinal cord is delicate neural tissue, so it requires strong protection. This protection is provided by the vertebral canal externally and by meninges internally. The outermost meningeal layer is the dura mater, a tough fibrous covering. In the vertebral canal, the dura forms a dural sac that extends below the end of the spinal cord, creating a safe region for lumbar puncture.
Deep to dura is the arachnoid mater, which is a thin membrane. The space between arachnoid and pia is the subarachnoid space, containing cerebrospinal fluid. CSF cushions the spinal cord and reduces mechanical stress during movements of the vertebral column.
The innermost layer is the pia mater, which closely follows the surface of the spinal cord. Pia forms the denticulate ligaments, which attach laterally to the dura and stabilize the cord. Inferiorly, pia continues as the filum terminale, anchoring the cord to the coccyx.
The structure-function relationship is clear: dura provides strength, CSF provides cushioning, pia provides close vascular and supportive contact, denticulate ligaments prevent excessive side-to-side movement, and filum terminale maintains longitudinal stability.
⚠️ CLINICAL IMPORTANCE
Inflammation of meninges is called meningitis and may irritate spinal nerve roots, causing neck stiffness and back pain. Epidural or subarachnoid spaces are clinically important for anesthesia, lumbar puncture, and CSF examination.
MAJOR CONCEPT 3: Blood Supply and Venous Drainage of the Spinal Cord
🧠 CORE
- The spinal cord receives arterial supply from anterior and posterior spinal arteries.
- The anterior spinal artery supplies the anterior two-thirds of the cord.
- Posterior spinal arteries supply the posterior one-third.
- Segmental medullary arteries reinforce spinal arteries.
- The artery of Adamkiewicz is an important large segmental artery.
- Venous drainage occurs through anterior and posterior spinal veins.
- Venous blood drains into internal vertebral venous plexus.
🔬 CONCEPT EXPLAINED
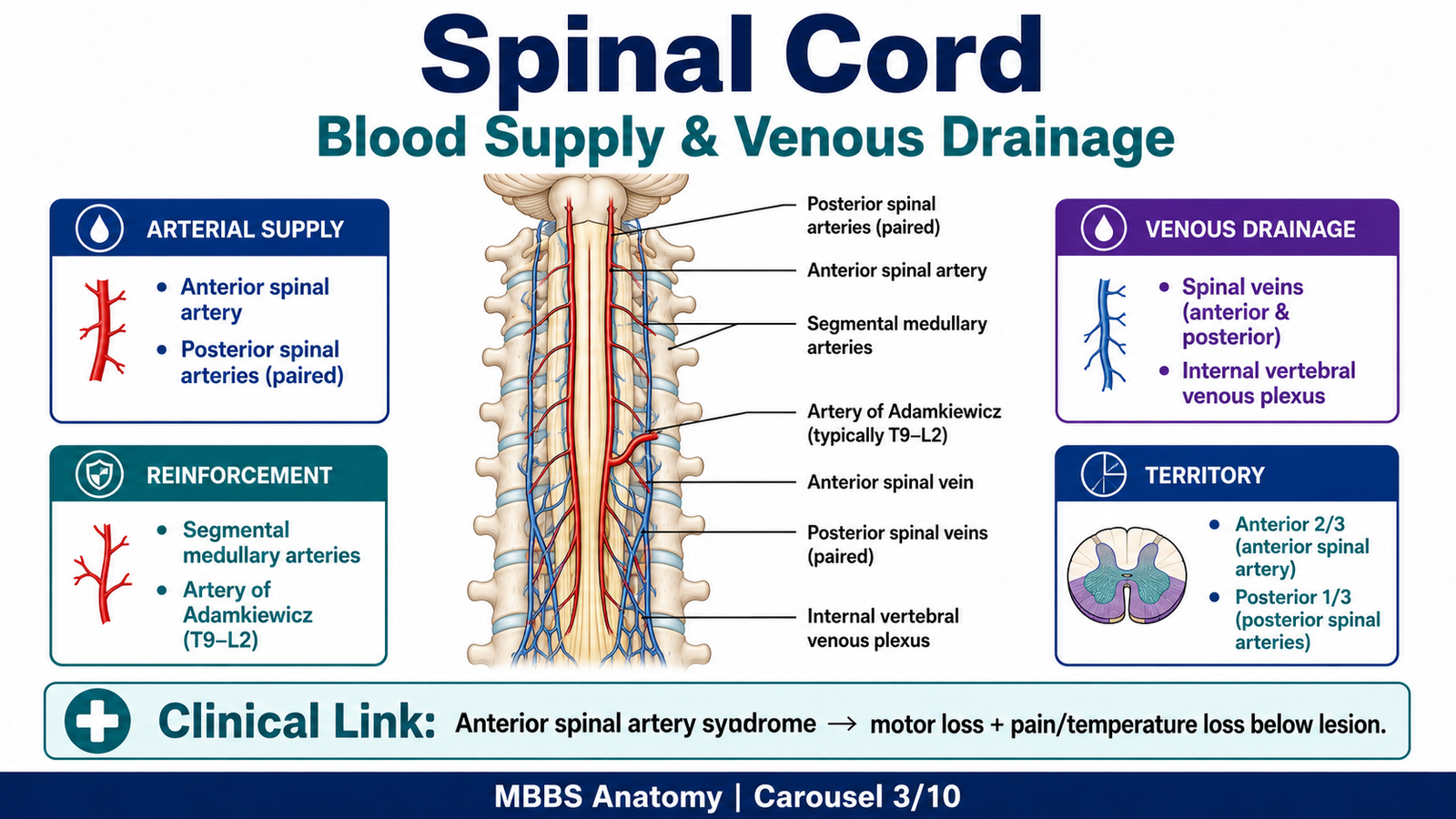
The spinal cord requires continuous blood supply because neurons are highly dependent on oxygen and glucose. The main arterial supply comes from one anterior spinal artery and two posterior spinal arteries. The anterior spinal artery runs along the anterior median fissure and supplies the anterior two-thirds of the spinal cord, including anterior horns and much of the lateral white matter. This region contains important motor neurons and descending motor tracts.
The posterior spinal arteries supply the posterior one-third of the cord, including posterior columns and parts of posterior horns. Because posterior columns carry fine touch, vibration, and conscious proprioception, posterior spinal artery compromise may affect these sensory modalities.
The longitudinal spinal arteries alone are not enough for the whole cord. They are reinforced by segmental medullary arteries, which enter through intervertebral foramina. The most important of these is the artery of Adamkiewicz, usually supplying the lower thoracic and lumbar cord. Damage to this artery can produce serious ischemia of the lower spinal cord.
Venous drainage occurs through spinal veins that communicate with the internal vertebral venous plexus. This plexus is valveless, which allows blood to flow in different directions depending on pressure changes. This anatomical feature explains why infections or malignancy can spread to the vertebral canal.
⚠️ CLINICAL IMPORTANCE
Occlusion of the anterior spinal artery produces anterior cord syndrome, causing bilateral motor weakness and loss of pain and temperature below the lesion, while posterior column sensations may be relatively preserved. This occurs because the anterior spinal artery supplies corticospinal tracts and spinothalamic pathways but not most of the posterior columns.
MAJOR CONCEPT 4: Internal Organization — Grey Matter and White Matter
🧠 CORE
- Grey matter is central and H-shaped in transverse section.
- White matter surrounds grey matter externally.
- Grey matter contains neuronal cell bodies and synapses.
- White matter contains myelinated ascending and descending tracts.
- Grey matter is divided into anterior, posterior, and lateral horns.
- White matter is divided into anterior, lateral, and posterior funiculi.
- The amount of grey and white matter varies at different spinal levels.
🔬 CONCEPT EXPLAINED
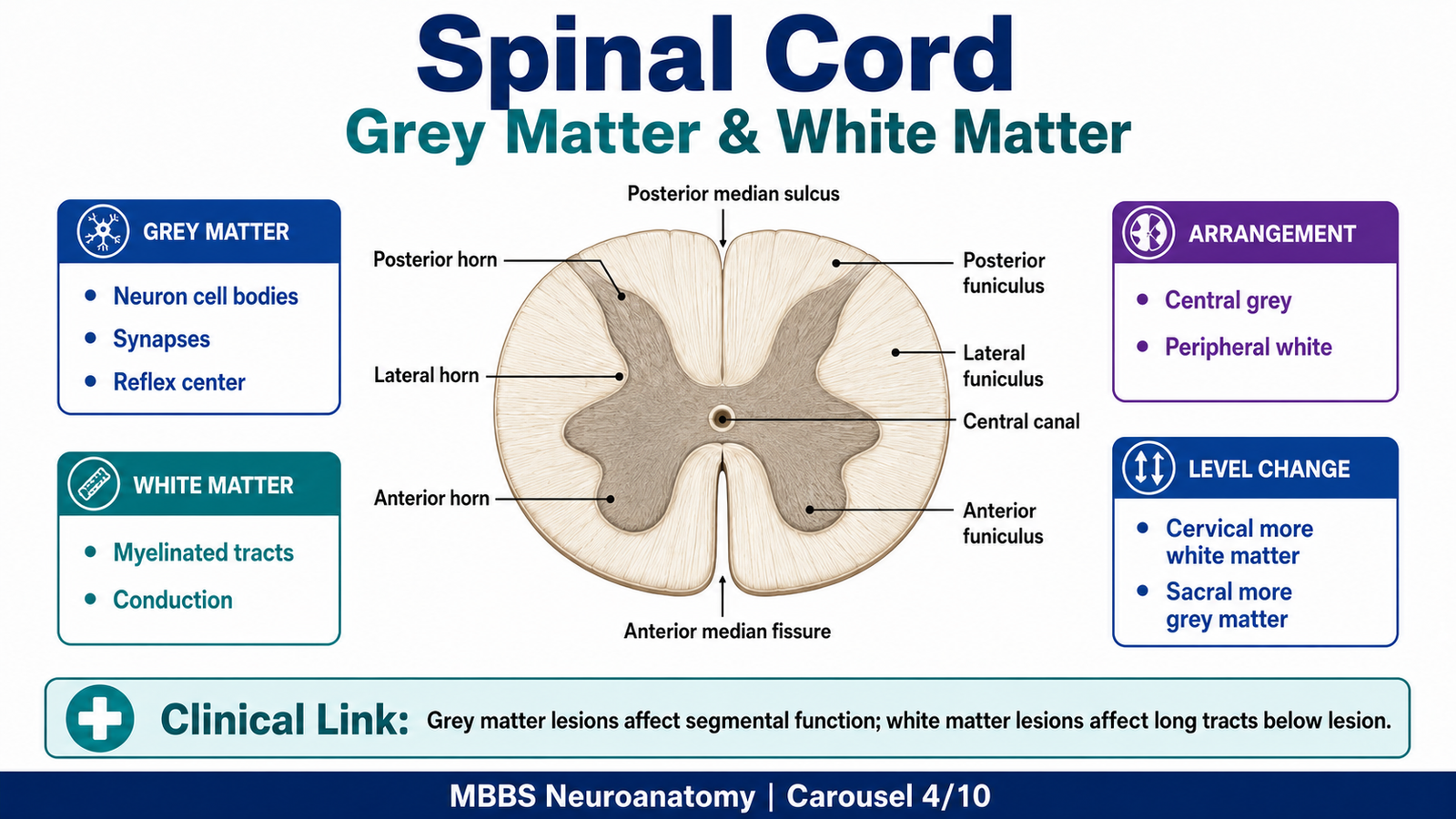
In transverse section, the spinal cord shows a central butterfly or H-shaped grey matter surrounded by peripheral white matter. This arrangement reflects function. Grey matter contains neuronal cell bodies, dendrites, synapses, and neuroglia, so it is the main processing region of the cord. White matter contains myelinated axons arranged into tracts, so it is the main conduction region.
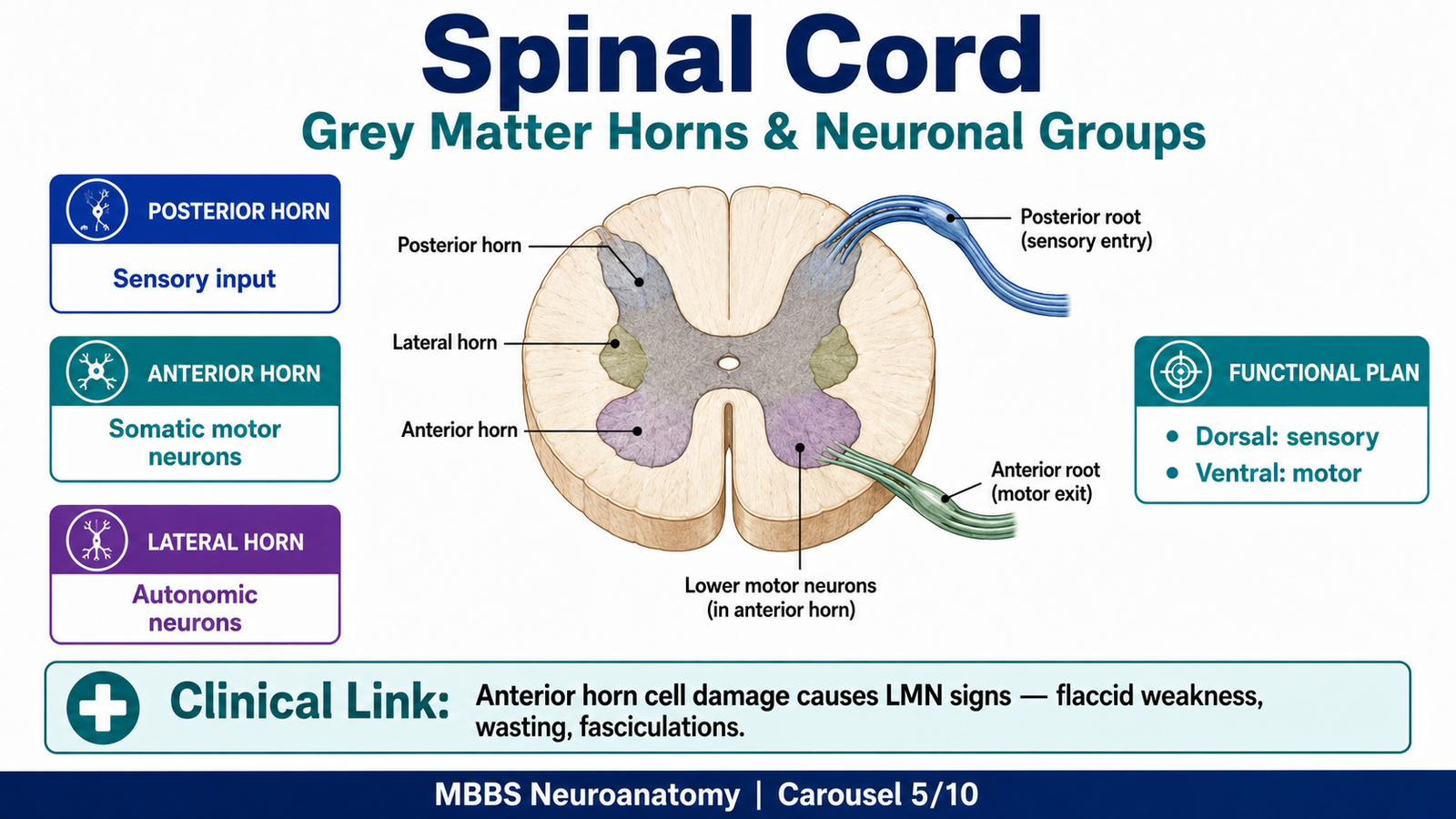
The grey matter is divided into horns. The posterior horn receives sensory input from the body through posterior roots. The anterior horn contains lower motor neurons whose axons leave through anterior roots to supply skeletal muscles. The lateral horn contains autonomic neurons and is especially visible in thoracic and upper lumbar segments, where sympathetic preganglionic neurons are located.
The white matter is divided into posterior, lateral, and anterior funiculi. Ascending tracts carry sensory information upward, while descending tracts carry motor commands downward. The posterior funiculus mainly contains dorsal column pathways. The lateral funiculus contains important ascending and descending tracts such as spinothalamic and lateral corticospinal tracts. The anterior funiculus contains anterior corticospinal and other descending pathways.
The amount of grey and white matter changes at different levels. Cervical segments contain more white matter because they contain ascending and descending fibers for most of the body. Sacral segments contain less white matter because fewer fibers remain at lower levels. Limb enlargements contain more grey matter because they contain large numbers of neurons supplying limb muscles.
⚠️ CLINICAL IMPORTANCE
Damage to grey matter mainly affects segmental reflexes and lower motor neurons at the level of lesion. Damage to white matter affects long tracts, producing sensory or motor deficits below the lesion. Therefore, clinical signs depend on whether the lesion involves horns, roots, or specific tracts.
MAJOR CONCEPT 5: Distribution of Grey Matter into Horns and Neuronal Groups
🧠 CORE
- Posterior horn receives sensory impulses.
- Anterior horn contains somatic motor neurons.
- Lateral horn contains autonomic neurons.
- Sensory neurons enter through posterior roots.
- Motor neurons exit through anterior roots.
- Grey matter organization reflects function.
- Different horns show different microscopic and functional roles.
🔬 CONCEPT EXPLAINED
The spinal cord grey matter is not randomly arranged. It is functionally organized according to the type of information being processed. The posterior horn is sensory. It receives incoming impulses from skin, muscles, joints, and viscera. Pain, temperature, touch, and proprioceptive signals enter the cord through posterior roots and synapse in specific parts of the posterior horn or ascend directly in white matter.
The anterior horn is motor. It contains lower motor neurons that send axons through the anterior roots to skeletal muscles. These motor neurons are larger because they must send long axons to peripheral muscles. The size of the anterior horn is especially large in cervical and lumbosacral enlargements because these regions supply limb muscles requiring fine and powerful movements.
The lateral horn is autonomic. It is most prominent in thoracic and upper lumbar segments, where it contains sympathetic preganglionic neurons. In sacral segments, parasympathetic preganglionic neurons are present, although a distinct lateral horn may not be as obvious.
This arrangement follows a dorsal sensory and ventral motor pattern. Sensory input enters posteriorly, motor output leaves anteriorly, and autonomic output lies between sensory and motor areas in selected segments.
⚠️ CLINICAL IMPORTANCE
Damage to the anterior horn causes lower motor neuron signs such as flaccid paralysis, muscle wasting, fasciculations, and reduced reflexes. Poliomyelitis classically damages anterior horn cells. Posterior horn lesions affect sensory processing, while lateral horn lesions can disturb autonomic functions such as sweating, vasomotor tone, and visceral control.
MAJOR CONCEPT 6: Rexed Laminae of the Spinal Cord
🧠 CORE
- Rexed laminae are functional layers of spinal grey matter.
- They are numbered I to X.
- Laminae I–VI are mainly sensory.
- Lamina VII contains interneurons and autonomic neurons.
- Laminae VIII–IX are mainly motor.
- Lamina X surrounds the central canal.
- Rexed laminae help explain sensory and motor processing.
🔬 CONCEPT EXPLAINED
Rexed laminae describe the spinal grey matter according to neuronal organization rather than simple horn anatomy. This is important because different parts of grey matter process different types of information.
The posterior horn contains laminae involved in sensory processing. Superficial laminae receive pain and temperature input. Deeper laminae receive touch and proprioceptive information and interact with interneurons. Lamina VII lies in the intermediate zone and contains interneurons, autonomic neurons, and important nuclei such as Clarke’s column in certain segments. Lamina IX contains large lower motor neurons that supply skeletal muscles.
Lamina X surrounds the central canal. Although small, it is part of the central grey matter and participates in commissural connections between the two sides of the cord.
The practical importance of Rexed laminae is that it links microscopic structure with function. Instead of memorizing grey matter as a simple H shape, students should understand that different layers are specialized for pain, touch, proprioception, autonomic function, interneuronal integration, and motor output.
⚠️ CLINICAL IMPORTANCE
Pain pathways involve specific posterior horn laminae. Therefore, lesions or modulation in these regions can alter pain perception. Motor neuron disease affects motor neuronal pools in anterior horn regions, especially lamina IX.
MAJOR CONCEPT 7: Histology of Spinal Cord at Different Levels
🧠 CORE
- Spinal cord histology shows central grey matter and peripheral white matter.
- Grey matter contains neurons, glial cells, neuropil, and central canal.
- White matter contains myelinated axons arranged in tracts.
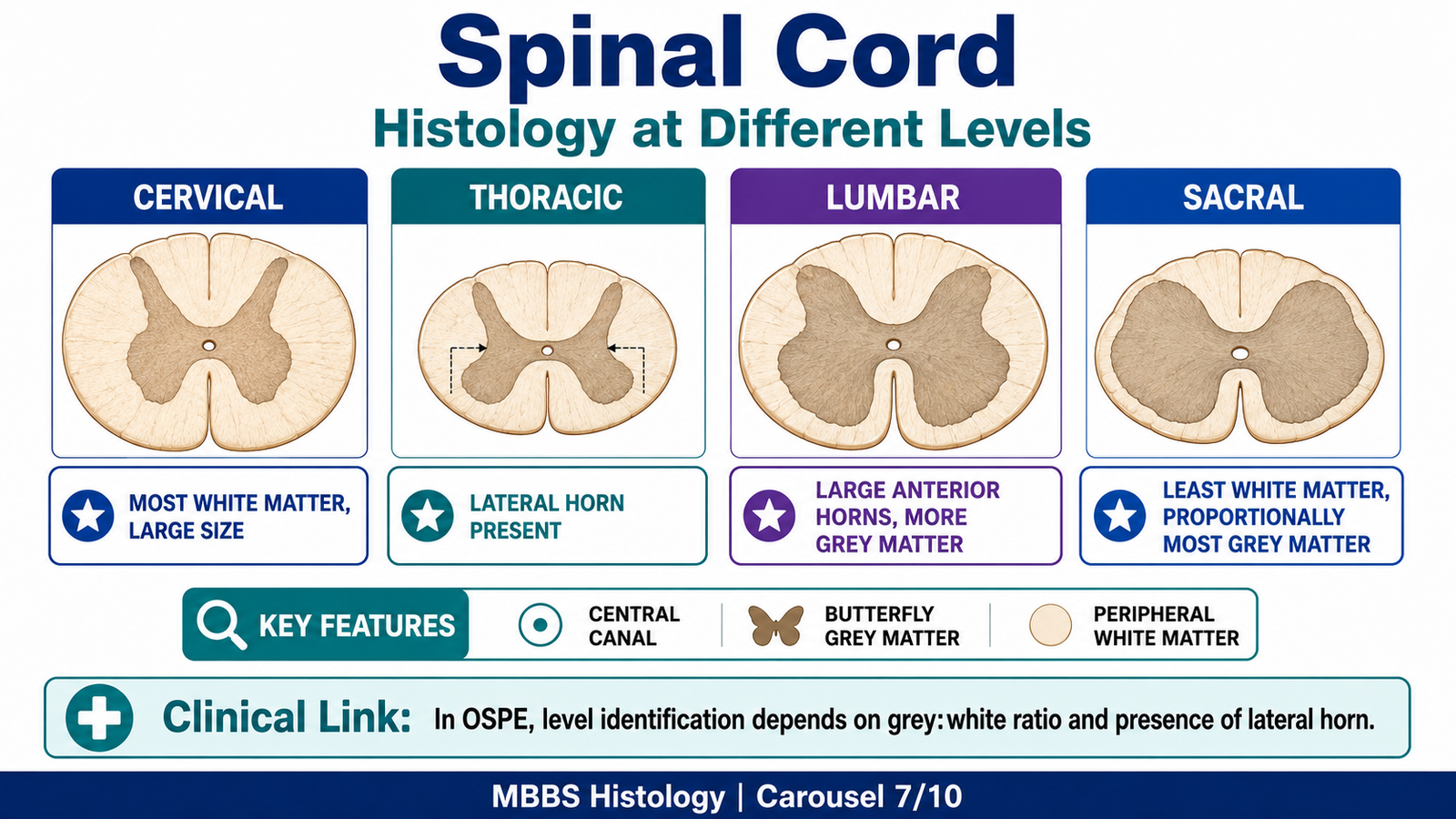
- Cervical cord has abundant white matter and large anterior horns.
- Thoracic cord has lateral horns.
- Lumbar cord has large anterior horns and less white matter than cervical cord.
- Sacral cord has proportionally more grey matter and less white matter.
🔬 CONCEPT EXPLAINED
Under light microscopy, a transverse section of spinal cord is recognized by its central H-shaped or butterfly-shaped grey matter surrounded by white matter. The central canal lies in the middle and is lined by ependymal cells. Around the central canal is grey commissure, which connects the right and left halves of grey matter.
The grey matter appears darker because it contains neuronal cell bodies, dendrites, synapses, and neuroglia. Large multipolar neurons are especially visible in the anterior horn. The white matter appears paler because it contains many myelinated axons. Myelin is lipid-rich and may appear as clear spaces in routine histological preparation.
Microscopic Appearance and Recognition Features
In an exam slide, spinal cord is identified by:
- Central butterfly-shaped grey matter.
- Peripheral white matter.
- Central canal in the middle.
- Anterior median fissure deeper than posterior median sulcus.
- Anterior horns usually broader and rounded.
- Posterior horns narrower and reaching toward the posterior surface.
- Level-specific differences in grey and white matter.
Cell Arrangement
The spinal cord does not show layered cortical organization like the cerebral cortex or cerebellum. Instead, neurons are arranged in functional groups within grey matter. Large motor neurons are present in the anterior horn. Sensory interneurons and projection neurons are present in the posterior horn. Autonomic neurons are present in lateral horn regions.
Tissue Layers and Structure → Function Relationship
Although spinal cord is not arranged in classical tissue layers, it has a clear functional arrangement:
- Central grey matter → processing, synapses, reflex integration.
- Peripheral white matter → rapid conduction through myelinated tracts.
- Central canal → CSF-containing remnant of neural tube cavity.
- Anterior horn → motor output.
- Posterior horn → sensory input.
- Lateral horn → autonomic output.
Therefore, the microscopic arrangement supports function: incoming sensory signals enter posteriorly, are processed in grey matter, and motor responses exit anteriorly, while long tracts in white matter connect the cord with the brain.
Cervical Level
The cervical spinal cord has the greatest amount of white matter because it contains ascending sensory fibers from almost the whole body and descending motor fibers going to most lower segments. The anterior horns are large in the cervical enlargement because they supply upper limb muscles.
Recognition features:
- Large overall size.
- Abundant white matter.
- Large anterior horns in cervical enlargement.
- Posterior columns divided into fasciculus gracilis and fasciculus cuneatus above T6.
Thoracic Level
Thoracic spinal cord has relatively smaller grey matter because it does not supply large limb muscles. A key recognition feature is the lateral horn, which contains sympathetic preganglionic neurons.
Recognition features:
- Smaller anterior horns.
- Prominent lateral horn.
- Relatively large white matter compared with grey matter.
- Clarke’s column may be present in lower cervical to upper lumbar regions, especially thoracic levels.
Lumbar Level
Lumbar spinal cord has larger anterior horns because it supplies lower limb muscles. White matter is less than cervical level because fewer ascending and descending fibers are present.
Recognition features:
- Large anterior horns.
- More grey matter than thoracic level.
- Less white matter than cervical level.
- No prominent lateral horn like thoracic level.
Sacral Level
Sacral spinal cord has relatively more grey matter and less white matter. This is because many long tracts have already terminated or originated at higher levels.
Recognition features:
- Small overall size.
- Thin rim of white matter.
- Relatively large grey matter.
- Less distinct separation of white columns.
Drawing and Labeling of Transverse Section
For drawing spinal cord sections, students should label:
- Anterior median fissure.
- Posterior median sulcus.
- Central canal.
- Anterior horn.
- Posterior horn.
- Lateral horn where applicable.
- Anterior funiculus.
- Lateral funiculus.
- Posterior funiculus.
- Anterior root.
- Posterior root.
- Grey commissure.
- White commissure.
⚠️ CLINICAL IMPORTANCE
Histological recognition is important in OSPE and practical exams. A common mistake is confusing spinal cord with peripheral nerve. Peripheral nerve shows bundles of nerve fibers with connective tissue coverings, while spinal cord shows central grey matter and peripheral white matter. Another common mistake is failing to identify the spinal level; the amount of grey matter, white matter, and presence of lateral horn help determine the level.
MAJOR CONCEPT 8: Development of Spinal Cord — Alar Plate and Basal Plate
🧠 CORE
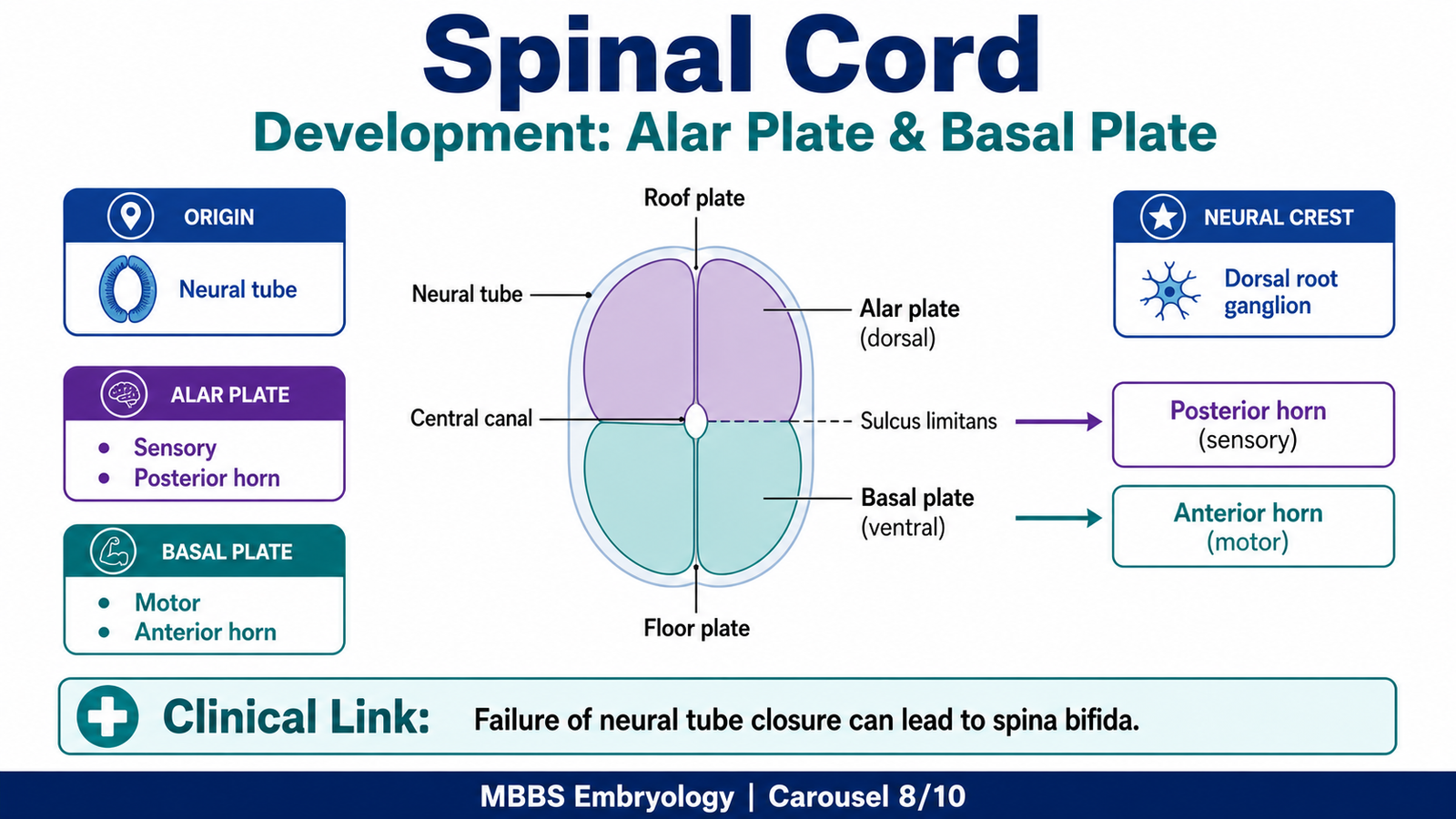
- The spinal cord develops from the neural tube.
- The neural tube cavity becomes the central canal.
- Alar plate forms sensory regions.
- Basal plate forms motor regions.
- Sulcus limitans separates alar and basal plates.
- Roof plate and floor plate are mainly non-neuronal organizing regions.
- Development explains adult dorsal sensory and ventral motor organization.
🔬 CONCEPT EXPLAINED
The spinal cord develops from the caudal part of the neural tube, which forms during neurulation. The neural tube is initially a simple epithelial tube, but its walls thicken as neuroepithelial cells proliferate. The central cavity remains as the central canal of the adult spinal cord.
As development proceeds, the neural tube differentiates into regions. The dorsal part forms the alar plate, and the ventral part forms the basal plate. These two plates are separated by a longitudinal groove called the sulcus limitans. This developmental division is extremely important because it explains the adult functional organization of the spinal cord.
The alar plate gives rise to sensory areas of the spinal cord, mainly the posterior horn. Therefore, sensory fibers entering through posterior roots synapse in regions derived from the alar plate. The basal plate gives rise to motor areas, mainly the anterior horn. Therefore, motor neurons leaving through anterior roots are derived from basal plate regions.
The roof plate and floor plate are thin dorsal and ventral midline regions. They are less involved in forming major neuronal columns but help organize patterning during development.
Developmental Origin
- Neural ectoderm → neural tube.
- Neural tube → spinal cord and brain.
- Neural tube cavity → central canal.
- Alar plate → sensory grey matter.
- Basal plate → motor grey matter.
- Neural crest cells → dorsal root ganglia and peripheral nervous system components.
Key Developmental Steps
- Neural plate forms from ectoderm.
- Neural plate folds to form neural tube.
- Caudal neural tube becomes spinal cord.
- Neuroepithelial cells proliferate and form mantle layer and marginal layer.
- Mantle layer forms grey matter.
- Marginal layer forms white matter.
- Alar plate differentiates into sensory regions.
- Basal plate differentiates into motor regions.
- Neural crest cells form dorsal root ganglia.
- Axons enter and leave the cord to form sensory and motor roots.
Timeline
- Week 3: Neural plate and neural tube formation begins.
- Week 4: Neural tube closure occurs.
- Early fetal period: Grey and white matter organization becomes clearer.
- Later fetal life: Myelination begins and continues after birth.
- Postnatal period: Myelination continues, supporting improved motor control and sensory conduction.
Major Derivatives
- Alar plate → posterior horn sensory neurons.
- Basal plate → anterior horn motor neurons.
- Intermediate regions → autonomic neurons in selected segments.
- Mantle layer → grey matter.
- Marginal layer → white matter.
- Central canal → remnant of neural tube cavity.
- Neural crest → dorsal root ganglia, autonomic ganglia, Schwann cells, and sensory neurons.
Development → Adult Structure Link
The adult spinal cord has posterior sensory horns and anterior motor horns because the embryonic alar plate lies dorsally and the basal plate lies ventrally. This developmental arrangement is preserved throughout life. Therefore, sensory fibers enter dorsally through posterior roots, and motor fibers exit ventrally through anterior roots.
Common Developmental Defects
Failure of neural tube closure can produce spina bifida. In mild forms, vertebral arches fail to fuse, but neural tissue may remain normal. In severe forms, meninges and spinal cord may protrude, causing neurological deficits. These defects are clinically important because they show how early embryological failure can affect adult structure and function.
⚠️ CLINICAL IMPORTANCE
Spina bifida and related neural tube defects may cause weakness, sensory loss, bladder and bowel dysfunction, and orthopedic deformities. Folic acid deficiency increases the risk of neural tube defects, so folic acid supplementation before conception and during early pregnancy is important.
MAJOR CONCEPT 9: Ascending Tracts of the Spinal Cord
🧠 CORE
- Ascending tracts carry sensory information from body to brain.
- Major pathways include dorsal column–medial lemniscal system and anterolateral spinothalamic tract.
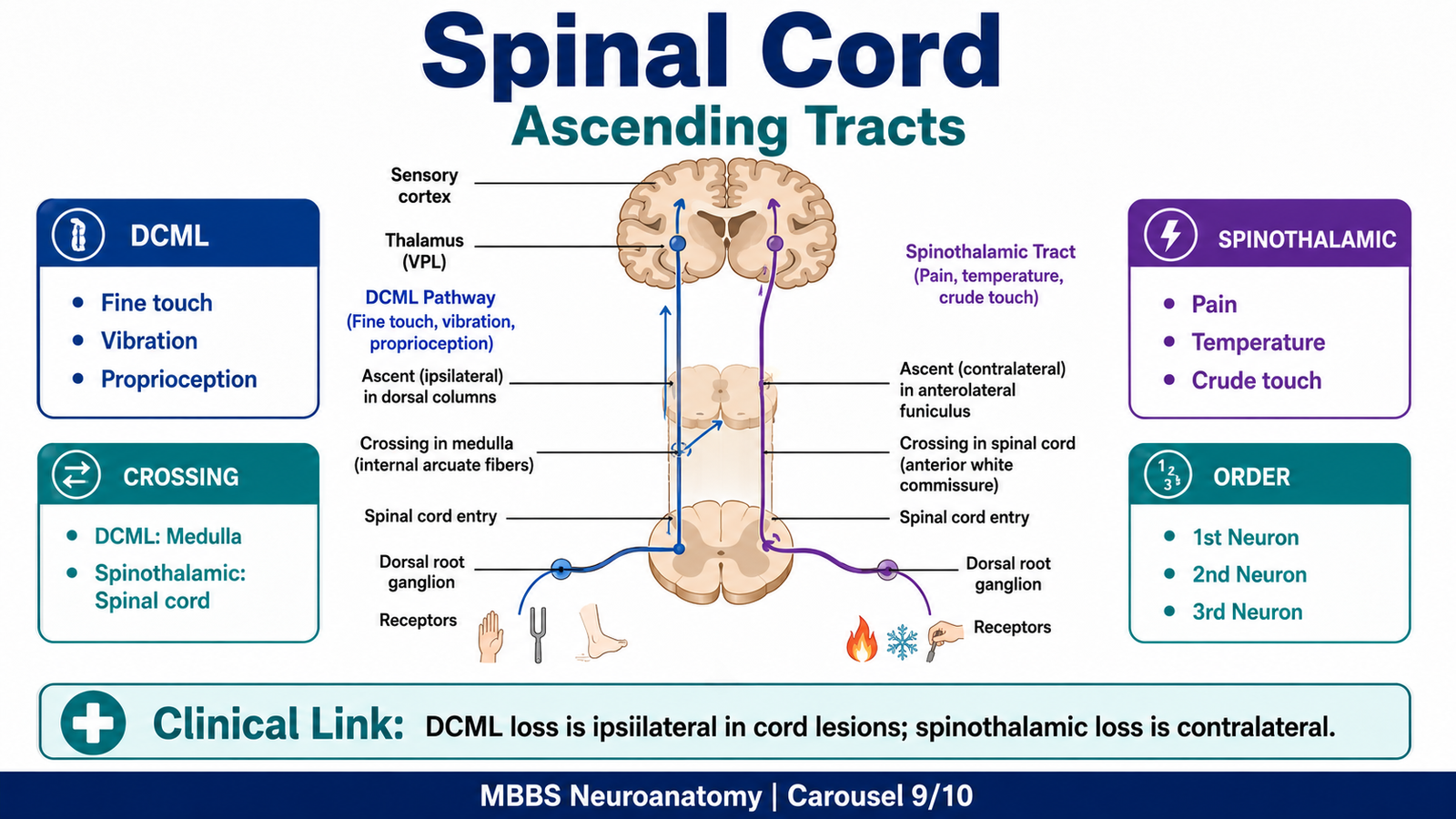
- Dorsal column carries fine touch, vibration, and conscious proprioception.
- Spinothalamic tract carries pain, temperature, and crude touch.
- Sensory pathways use first-, second-, and third-order neurons.
- Decussation level differs between pathways.
- Lesions produce characteristic sensory loss.
🔬 CONCEPT EXPLAINED
Ascending tracts are white matter pathways that carry sensory information from peripheral receptors to higher centers. Sensory pathways usually use a chain of three neurons. The first-order neuron carries information from receptor to CNS. The second-order neuron crosses and ascends. The third-order neuron projects from thalamus to cerebral cortex.
The two most important ascending pathways for MBBS students are the dorsal column–medial lemniscal system and the anterolateral spinothalamic tract.
Dorsal Column–Medial Lemniscal System
The dorsal column–medial lemniscal system carries:
- Fine/discriminative touch.
- Vibration sense.
- Conscious proprioception.
- Two-point discrimination.
- Stereognosis.
Origin, Pathway and Termination
First-order neurons have cell bodies in the dorsal root ganglia. Their peripheral processes receive sensory information from receptors in skin, muscles, tendons, and joints. Their central processes enter the spinal cord through posterior roots and ascend ipsilaterally in the posterior column.
The posterior column has two fasciculi:
- Fasciculus gracilis: Carries sensations from lower limb and lower trunk. Present throughout the cord.
- Fasciculus cuneatus: Carries sensations from upper limb and upper trunk. Present above T6.
These fibers ascend to the medulla, where they synapse in the nucleus gracilis and nucleus cuneatus. Second-order neurons then cross as internal arcuate fibers and form the medial lemniscus. The medial lemniscus ascends to the thalamus, mainly the ventral posterolateral nucleus. Third-order neurons then project to the primary somatosensory cortex.
Why This Pathway Exists
This pathway allows precise awareness of body position and detailed touch. It is essential for coordinated movement because the brain must know where body parts are before it can control them accurately.
Clinical Failure
If the dorsal column is damaged in the spinal cord, loss of vibration, fine touch, and conscious proprioception occurs on the same side below the lesion, because fibers have not yet crossed in the medulla.
Anterolateral Spinothalamic Tract
The spinothalamic tract carries:
- Pain.
- Temperature.
- Crude touch.
- Pressure.
Origin, Pathway and Termination
First-order neurons have cell bodies in dorsal root ganglia. Their fibers enter the posterior horn and synapse with second-order neurons. The second-order neurons cross in the spinal cord through the anterior white commissure, usually within one or two segments of entry. After crossing, they ascend in the opposite anterolateral funiculus as the spinothalamic tract.
These fibers ascend to the thalamus, mainly the ventral posterolateral nucleus. Third-order neurons project to the primary somatosensory cortex, where pain, temperature, and crude touch are consciously perceived.
Why This Pathway Exists
Pain and temperature pathways are protective. Pain warns the body of tissue damage, while temperature sensation helps prevent burns, frost injury, and environmental harm. The pathway crosses early in the spinal cord, which explains the pattern of sensory loss in hemisection lesions.
Clinical Failure
Damage to the spinothalamic tract causes loss of pain and temperature on the opposite side below the lesion, usually beginning a few segments below the level of damage.
⚠️ CLINICAL IMPORTANCE
The difference in crossing level is highly tested. Dorsal column fibers cross in the medulla, so spinal cord lesions cause ipsilateral dorsal column loss. Spinothalamic fibers cross in the spinal cord, so cord lesions cause contralateral pain and temperature loss.
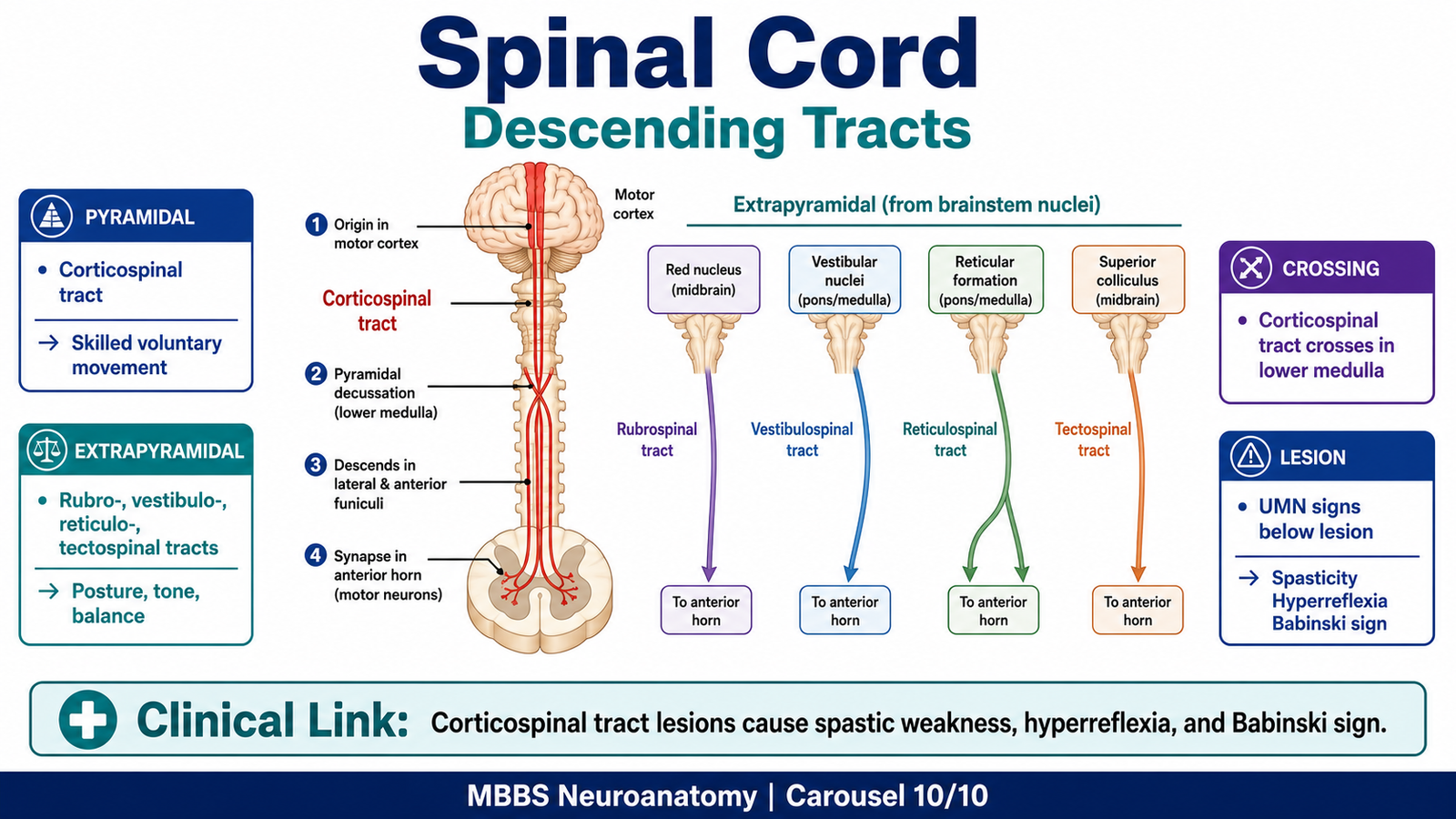
MAJOR CONCEPT 10: Descending Tracts of the Spinal Cord
🧠 CORE
- Descending tracts carry motor commands from brain to spinal cord.
- Pyramidal tracts control voluntary skilled movements.
- Extrapyramidal tracts control posture, tone, balance, and automatic movements.
- Corticospinal tract is the main pyramidal pathway.
- Most corticospinal fibers cross in the pyramidal decussation.
- Descending tracts influence lower motor neurons.
- Lesions produce upper motor neuron signs below the lesion.
🔬 CONCEPT EXPLAINED
Descending tracts allow the brain to control movement. The final pathway to skeletal muscle is the lower motor neuron in the anterior horn. However, these lower motor neurons are controlled by descending upper motor neuron pathways from the cerebral cortex and brainstem.
Descending tracts are divided into pyramidal and extrapyramidal systems. This division helps students understand the difference between fine voluntary movement and background postural control.
Pyramidal Tracts
The pyramidal system mainly includes the corticospinal tracts. These tracts originate from the motor cortex and adjacent cortical areas. Fibers descend through the internal capsule, brainstem, and pyramids of the medulla.
At the lower medulla, most fibers cross in the pyramidal decussation and descend in the opposite lateral funiculus as the lateral corticospinal tract. A smaller number of fibers descend uncrossed as the anterior corticospinal tract, many of which cross near their termination.
Origin, Pathway and Termination
- Origin: Primary motor cortex, premotor cortex, and somatosensory cortex.
- Pathway: Corona radiata → internal capsule → cerebral peduncle → pons → medullary pyramids.
- Decussation: Most fibers cross in lower medulla.
- Spinal course: Lateral corticospinal tract in lateral funiculus; anterior corticospinal tract in anterior funiculus.
- Termination: Interneurons and lower motor neurons in anterior horn.
Function
The corticospinal tract controls voluntary, skilled, fractionated movements, especially of distal limb muscles such as hand and fingers. It allows precise movement needed for writing, buttoning, and fine manipulation.
Clinical Failure
Damage to corticospinal tract above the anterior horn causes upper motor neuron signs below the lesion: weakness, spasticity, hyperreflexia, clonus, and Babinski sign.
Extrapyramidal Tracts
Extrapyramidal tracts arise mainly from brainstem nuclei and regulate posture, muscle tone, balance, head-eye coordination, and automatic motor activities. They do not primarily control fine voluntary movement like the corticospinal tract.
Important extrapyramidal tracts include:
- Rubrospinal tract: Influences flexor muscles, especially in upper limb.
- Vestibulospinal tracts: Maintain balance and extensor tone.
- Reticulospinal tracts: Regulate posture, tone, reflex activity, and locomotor patterns.
- Tectospinal tract: Coordinates head and neck movements in response to visual and auditory stimuli.
Origin, Pathway and Termination
- Rubrospinal tract originates from red nucleus.
- Vestibulospinal tracts originate from vestibular nuclei.
- Reticulospinal tracts originate from reticular formation.
- Tectospinal tract originates from superior colliculus.
- These tracts descend in anterior or lateral funiculi.
- They terminate on interneurons and motor neurons in spinal grey matter.
Function
These tracts provide automatic background control for movement. When a person stands, walks, turns the head toward a sound, or maintains balance, extrapyramidal pathways continuously adjust muscle tone and posture.
Difference Between Pyramidal and Extrapyramidal Tracts
| Feature | Pyramidal Tracts | Extrapyramidal Tracts |
|---|---|---|
| Main pathway | Corticospinal tract | Rubrospinal, vestibulospinal, reticulospinal, tectospinal |
| Main origin | Cerebral cortex | Brainstem nuclei |
| Main function | Voluntary skilled movement | Posture, tone, balance, automatic movement |
| Muscle control | Distal limb muscles especially | Axial and proximal muscles mainly |
| Clinical lesion | UMN weakness, spasticity, Babinski sign | Abnormal tone, posture, coordination, involuntary movement patterns |
| Example function | Writing with fingers | Maintaining upright posture |
⚠️ CLINICAL IMPORTANCE
A pyramidal tract lesion causes weakness and loss of fine voluntary control. Extrapyramidal dysfunction causes abnormal tone, posture, balance, and automatic movement control. In spinal cord lesions, corticospinal tract damage is tested by weakness, increased reflexes, and Babinski sign below the lesion.
MAJOR CONCEPT 11: Integrated Spinal Cord Reflex and Functional Organization
🧠 CORE
- The spinal cord is not only a pathway but also a reflex center.
- Sensory input enters through posterior roots.
- Motor output exits through anterior roots.
- Interneurons connect sensory and motor neurons.
- Reflexes allow rapid protective responses.
- Long tracts allow brain control and awareness.
- Segmental organization explains neurological localization.
🔬 CONCEPT EXPLAINED
The spinal cord works at two levels. First, it acts as a conduction pathway between the body and brain. Second, it acts as a local reflex center. This dual function is possible because the spinal cord contains both white matter tracts and grey matter neuronal circuits.
In a simple reflex, a stimulus activates a receptor. The sensory impulse travels through a peripheral nerve and enters the spinal cord through the posterior root. It may synapse directly or through interneurons in grey matter. The motor response leaves through the anterior root and activates skeletal muscle. This produces a rapid response before conscious perception is fully processed by the brain.
At the same time, ascending fibers carry information to the brain so the person becomes aware of the stimulus. Descending fibers from the brain adjust spinal reflexes and voluntary movement. Therefore, the spinal cord is both independent and controlled: it can produce reflexes locally, but its activity is refined by higher centers.
⚠️ CLINICAL IMPORTANCE
In complete spinal cord transection, pathways between brain and spinal cord are interrupted. Initially, spinal shock may occur with loss of reflexes. Later, reflexes may return exaggerated because descending inhibitory control is lost. This explains why chronic upper motor neuron lesions show hyperreflexia and spasticity.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Function | Outcome |
|---|---|---|
| Vertebral canal | Bony protection | Prevents direct injury to cord |
| Meninges and CSF | Cushion and stabilize cord | Protect neural tissue during movement |
| Cervical enlargement | More neurons for upper limb | Fine and powerful upper limb control |
| Lumbosacral enlargement | More neurons for lower limb | Lower limb movement and gait |
| Grey matter | Synapses and processing | Reflexes and segmental control |
| White matter | Ascending and descending conduction | Brain-body communication |
| Posterior horn | Sensory reception | Sensory processing |
| Anterior horn | Motor output | Skeletal muscle contraction |
| Lateral horn | Autonomic output | Sympathetic/parasympathetic control |
| Dorsal columns | Fine touch, vibration, proprioception | Body position awareness |
| Spinothalamic tract | Pain and temperature | Protective sensation |
| Corticospinal tract | Skilled voluntary movement | Fine motor control |
| Extrapyramidal tracts | Tone and posture | Balance and automatic movement |
| Alar plate | Sensory development | Adult posterior horn |
| Basal plate | Motor development | Adult anterior horn |
The spinal cord is therefore an integrated structure where gross anatomy, microscopic arrangement, embryological development, and neural pathways all support one major function: controlled interaction between the body and brain.
🩺 5️⃣ Clinical Correlation
1. Spinal Cord Hemisection — Brown-Séquard Syndrome
If one half of the spinal cord is damaged, different tracts are affected differently.
- Ipsilateral corticospinal tract damage → upper motor neuron weakness below lesion.
- Ipsilateral dorsal column damage → loss of vibration, fine touch, and proprioception below lesion.
- Contralateral spinothalamic damage → loss of pain and temperature below lesion.
This pattern occurs because dorsal column and corticospinal fibers cross in the medulla, while spinothalamic fibers cross in the spinal cord.
2. Anterior Cord Syndrome
Damage to anterior spinal artery affects the anterior two-thirds of spinal cord.
- Corticospinal tract involvement → motor weakness.
- Spinothalamic tract involvement → loss of pain and temperature.
- Dorsal column sparing → vibration and proprioception may remain preserved.
This is a common exam concept because it directly links blood supply with tract function.
3. Posterior Column Lesion
Posterior column damage causes loss of:
- Vibration sense.
- Conscious proprioception.
- Fine touch.
- Sensory ataxia.
The patient may walk unsteadily because the brain does not receive accurate position sense from limbs.
4. Anterior Horn Cell Disease
Damage to anterior horn cells affects lower motor neurons.
Clinical effects:
- Flaccid paralysis.
- Muscle wasting.
- Fasciculations.
- Reduced reflexes.
- No sensory loss if sensory pathways are spared.
Poliomyelitis is a classical example.
5. Corticospinal Tract Lesion
Damage to corticospinal tract produces upper motor neuron signs:
- Weakness below lesion.
- Spasticity.
- Hyperreflexia.
- Clonus.
- Babinski sign.
This occurs because descending control over spinal reflexes is lost.
6. Spina Bifida
Spina bifida results from defective closure of the neural tube or vertebral arches.
Functional consequences may include:
- Lower limb weakness.
- Sensory loss.
- Bladder and bowel dysfunction.
- Orthopedic deformities.
This condition links embryological development with adult neurological function.
📌 6️⃣ Summary Points
- The spinal cord extends from the medulla to about the lower border of L1 in adults.
- Grey matter is central and H-shaped; white matter is peripheral.
- Posterior horn is sensory, anterior horn is motor, and lateral horn is autonomic.
- Cervical cord has the most white matter because it contains fibers for most of the body.
- Thoracic cord is recognized by a lateral horn.
- Dorsal column carries fine touch, vibration, and conscious proprioception.
- Spinothalamic tract carries pain, temperature, and crude touch.
- Dorsal column crosses in the medulla; spinothalamic tract crosses in the spinal cord.
- Corticospinal tract controls voluntary skilled movement.
- Extrapyramidal tracts control posture, tone, balance, and automatic movement.
- Alar plate forms sensory posterior horn; basal plate forms motor anterior horn.
- Anterior spinal artery supplies anterior two-thirds of cord, so its occlusion affects motor and pain-temperature pathways.