
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
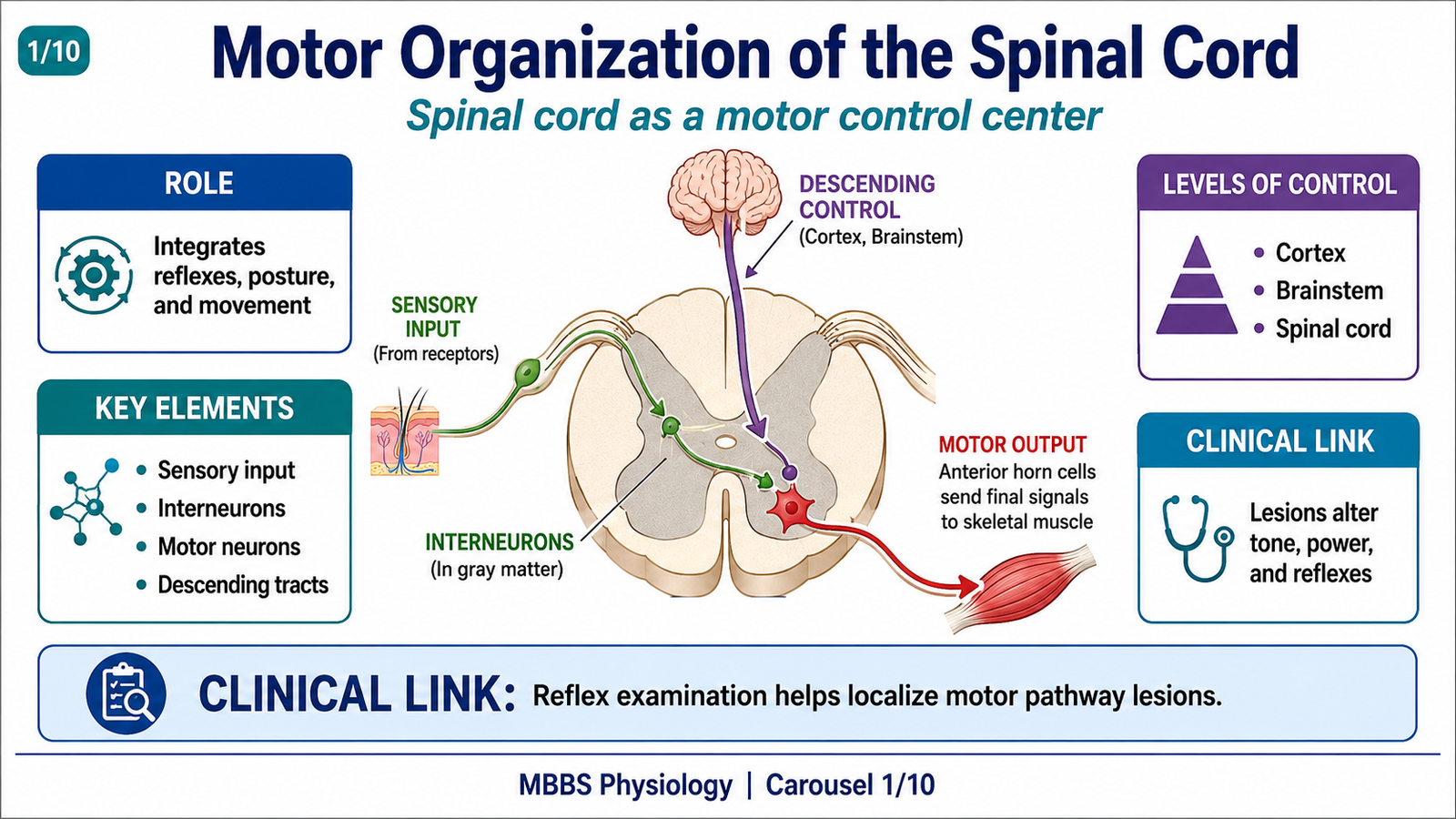
The spinal cord is not merely a pathway between the brain and the body; it is an active motor control center. It receives commands from higher centers, processes sensory input, and produces rapid motor responses through reflex circuits.
Motor organization of the spinal cord is mainly located in the anterior grey horn, where lower motor neurons supply skeletal muscles. These neurons form the final pathway through which all voluntary and reflex movements are expressed.
Spinal reflexes are essential for posture, muscle tone, protection from injury, and smooth voluntary movement. They allow the body to respond quickly without waiting for conscious brain processing.
Clinically, damage to spinal motor pathways produces important signs such as weakness, altered tone, exaggerated reflexes, absent reflexes, spasticity, flaccidity, and abnormal plantar response. Therefore, understanding spinal motor organization is essential for clinical neurology.
This topic connects physiology, neuroanatomy, and clinical examination because tendon jerks, muscle tone, withdrawal reflexes, and UMN/LMN signs are all based on spinal cord motor circuits.
🔹 2️⃣ Foundation Concepts
Key Definitions
• Motor control means regulation of skeletal muscle activity to produce posture, movement, and reflex responses.
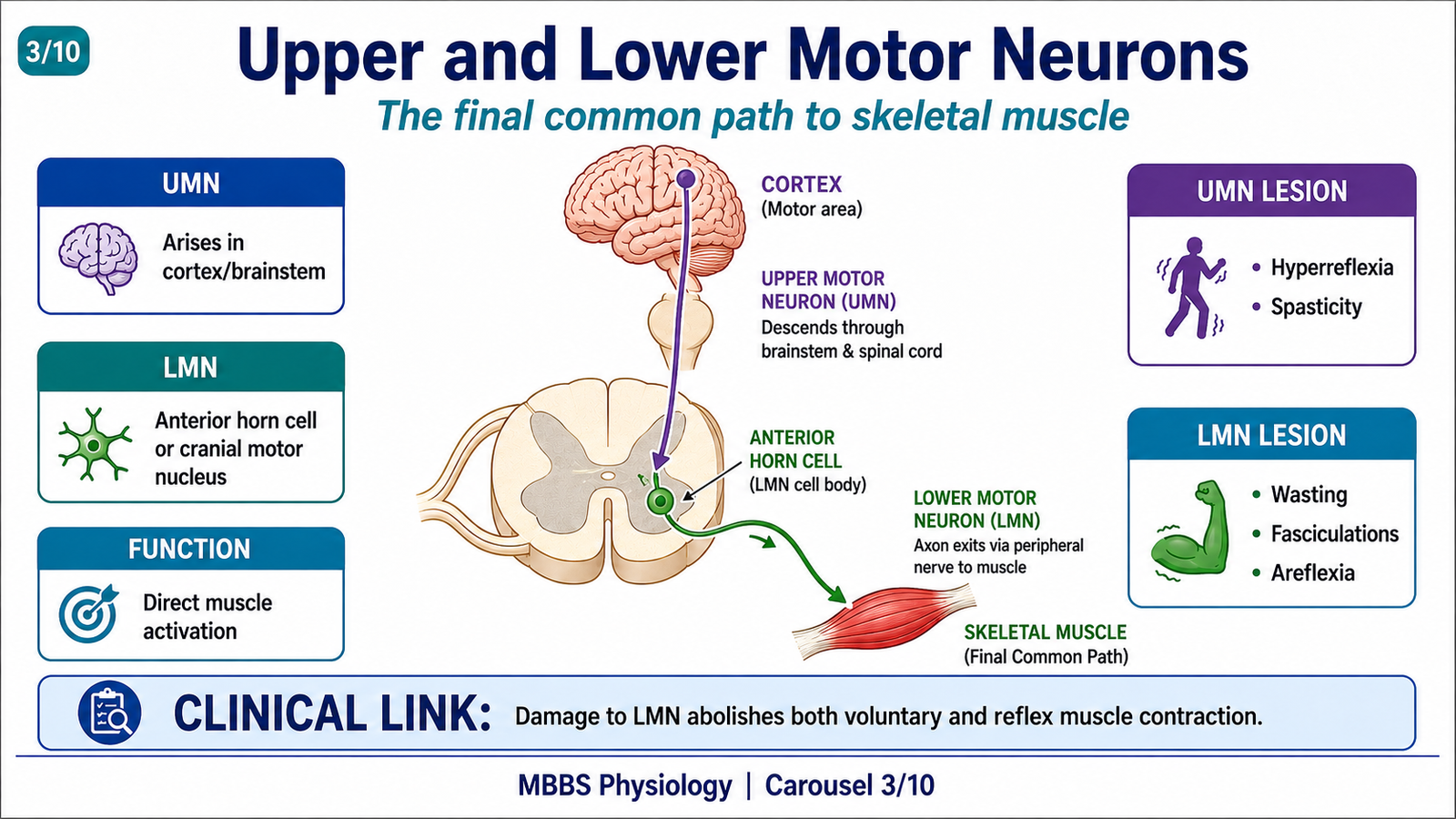
• Upper motor neurons (UMNs) are neurons in the brain and brainstem that control lower motor neurons.
• Lower motor neurons (LMNs) are neurons in the anterior horn of spinal cord or motor nuclei of cranial nerves that directly supply skeletal muscle.
• Anterior horn cells are motor neurons present in the ventral grey horn of the spinal cord.
• Final common path means the lower motor neuron pathway through which all motor commands finally reach skeletal muscle.
• Reflex action is an automatic, involuntary response to a stimulus.
• Reflex arc is the neural pathway responsible for a reflex response.
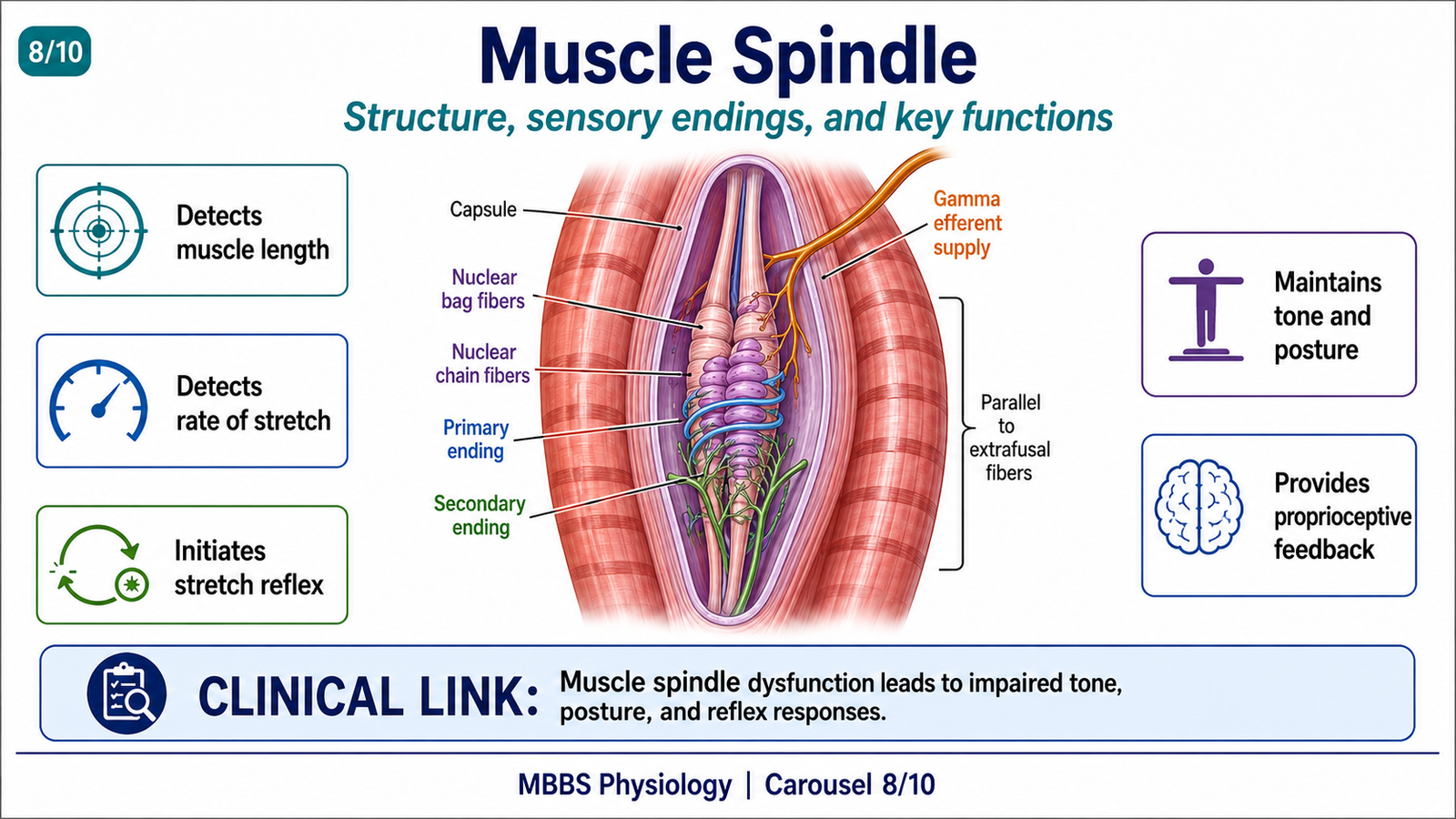
• Muscle spindle is a stretch receptor present inside skeletal muscle that detects muscle length and rate of stretch.
• Golgi tendon organ is a tension receptor present in tendons that detects muscle tension.
• Stretch reflex is contraction of a muscle in response to its stretch.
• Polysynaptic reflex is a reflex involving one or more interneurons between sensory and motor neurons.
• Reciprocal inhibition means inhibition of antagonist muscles during contraction of agonist muscles.
Essential Terminology
• Agonist muscle: main muscle producing a movement.
• Antagonist muscle: muscle opposing the action of agonist.
• Alpha motor neuron: supplies extrafusal skeletal muscle fibers and causes muscle contraction.
• Gamma motor neuron: supplies intrafusal fibers of muscle spindle and adjusts spindle sensitivity.
• Extrafusal muscle fibers: ordinary skeletal muscle fibers that produce force.
• Intrafusal muscle fibers: specialized fibers inside muscle spindle that detect stretch.
• Ia afferent fibers: rapidly conducting sensory fibers from muscle spindle, especially sensitive to dynamic stretch.
• II afferent fibers: sensory fibers from muscle spindle, especially related to static muscle length.
• Ib afferent fibers: sensory fibers from Golgi tendon organ.
• Monosynaptic reflex: reflex with one synapse between afferent and efferent neurons.
• Segmental integration: reflex processing within one spinal cord segment.
• Intersegmental integration: reflex processing involving multiple spinal cord segments.
Basic Overview
• The spinal cord contains motor neurons, sensory neurons, interneurons, and reflex circuits.
• Motor output leaves through anterior roots and reaches skeletal muscles.
• Sensory input enters through posterior roots and influences motor activity.
• Spinal reflexes help maintain muscle tone, posture, and protective movements.
• Higher centers regulate spinal reflexes but many reflex circuits are organized locally in the spinal cord.
• Muscle spindle mainly detects stretch; Golgi tendon organ mainly detects tension.
• Reflex activity is important in clinical examination because abnormal reflexes help localize neurological lesions.
🔹 3️⃣ Core Learning — Curriculum Coverage
MOTOR ORGANIZATION OF THE SPINAL CORD
🧠 CORE
- The spinal cord contains motor neurons, interneurons, sensory inputs, and descending motor pathways.
- Motor neurons are mainly located in the anterior horn of gray matter.
- Lower motor neurons directly innervate skeletal muscles.
- Interneurons integrate sensory input and coordinate motor output.
- Descending pathways from the brain regulate spinal reflexes and voluntary movement.
- The spinal cord can generate simple automatic motor responses without conscious control.
- All skeletal muscle activity finally depends on lower motor neuron discharge.
🔬 CONCEPT EXPLAINED
To understand spinal motor control, the spinal cord should be viewed as a functional motor center, not simply as a conducting pathway. The brain plans and initiates many voluntary movements, but the spinal cord organizes the final motor output by activating the correct groups of muscles.
The anterior horn of the spinal cord contains motor neurons that supply skeletal muscles. These neurons receive inputs from sensory receptors, interneurons, and descending tracts from the brain. After receiving and integrating these signals, they send impulses through peripheral nerves to muscles.
The spinal cord is especially important because it can produce reflex movements without waiting for conscious processing in the brain. For example, if a person touches a hot object, the spinal cord can rapidly activate flexor muscles to withdraw the limb. This protects the body before the person consciously feels pain.
Motor activity is therefore organized at different levels. The spinal cord handles basic reflexes and local motor patterns. The brainstem helps regulate posture and balance. The motor cortex controls skilled voluntary movement. These levels work together so that movement is coordinated, purposeful, and safe.
If spinal motor organization fails, muscle activity becomes abnormal. Depending on the site of damage, the patient may develop weakness, loss of reflexes, exaggerated reflexes, spasticity, abnormal posture, or loss of protective withdrawal responses.
⚠️ CLINICAL IMPORTANCE
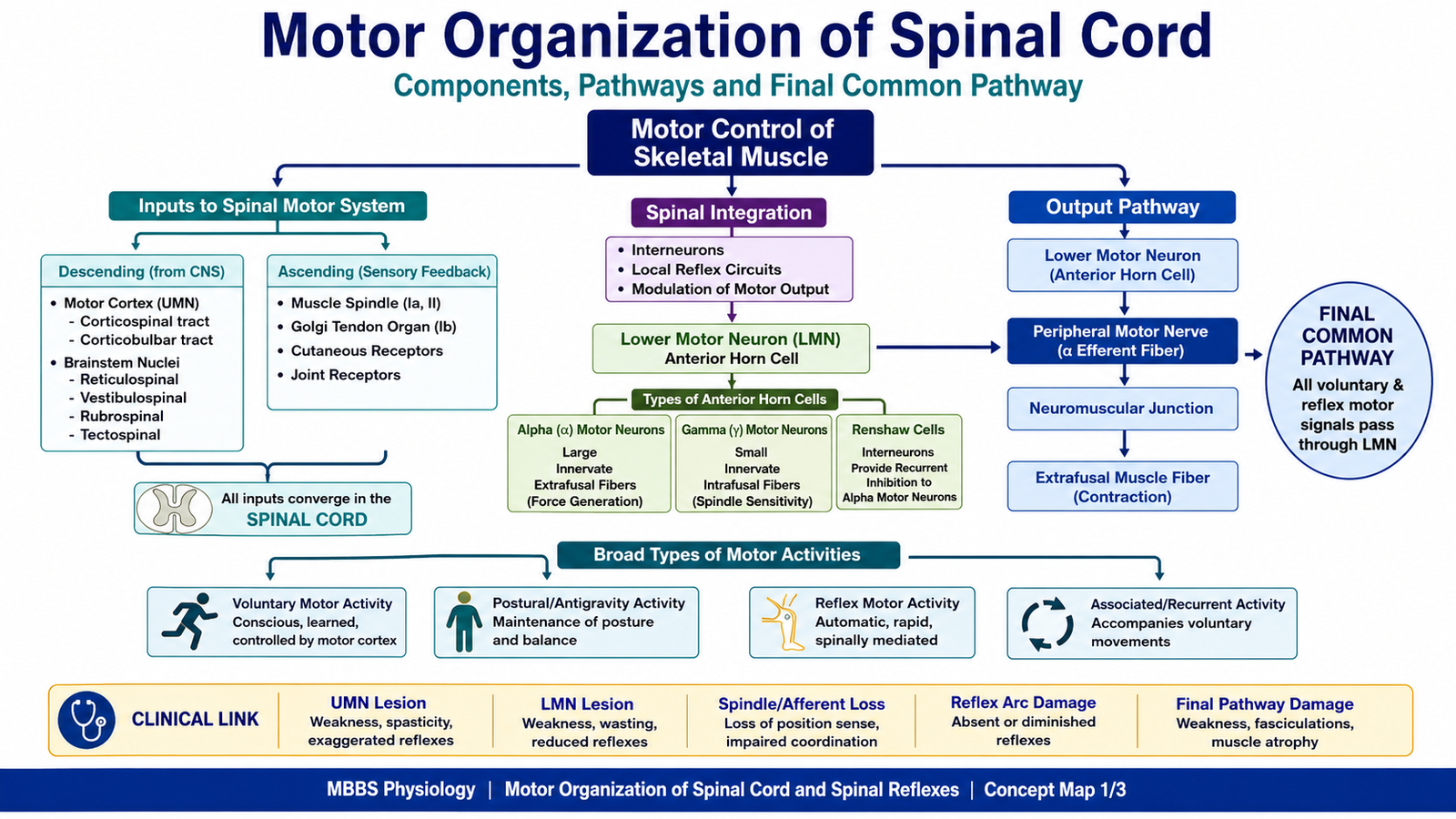
Damage to the spinal cord or its motor pathways can produce major motor deficits. A lesion affecting lower motor neurons causes weakness, wasting, fasciculations, and reduced reflexes. A lesion affecting upper motor neuron control often causes spasticity, exaggerated reflexes, and abnormal plantar response. Reflex examination is therefore a powerful clinical tool for localizing neurological lesions.
COMPONENTS OF THE NERVOUS SYSTEM INVOLVED IN MOTOR CONTROL
🧠 CORE
- Motor control involves the cerebral cortex, basal ganglia, cerebellum, brainstem, spinal cord, peripheral nerves, neuromuscular junctions, and muscles.
- The motor cortex initiates voluntary skilled movement.
- The basal ganglia help select and smooth motor programs.
- The cerebellum coordinates timing, balance, and accuracy.
- The brainstem regulates posture, muscle tone, and basic motor patterns.
- The spinal cord integrates reflexes and sends final motor output.
- Peripheral nerves transmit impulses to skeletal muscles.
🔬 CONCEPT EXPLAINED
Motor control requires cooperation between multiple parts of the nervous system. The cerebral cortex is responsible for voluntary movement, especially skilled and precise movements such as writing or picking up small objects. However, the cortex does not act alone.
The basal ganglia help select the appropriate motor plan and suppress unwanted movements. The cerebellum compares intended movement with actual movement and corrects errors. The brainstem contributes to posture, balance, and automatic motor activities. Finally, the spinal cord converts motor commands into actual muscle activity through lower motor neurons.
This organization exists because movement must be both planned and adjusted. For example, walking requires cortical intention, spinal rhythm, sensory feedback, cerebellar coordination, and postural support from brainstem pathways. Without this integration, movement becomes weak, poorly coordinated, stiff, or uncontrolled.
The spinal cord is the final segment of this system before skeletal muscle. It receives descending commands from higher centers and also local sensory input from muscles, tendons, and skin. It then produces appropriate motor output through anterior horn cells.
⚠️ CLINICAL IMPORTANCE
Lesions at different levels produce different motor abnormalities. Cerebellar disease causes ataxia and incoordination. Basal ganglia disease causes abnormal tone and movement disorders. Spinal cord or peripheral nerve lesions cause weakness and reflex changes. Therefore, clinical examination of movement, tone, coordination, and reflexes helps identify the level of nervous system damage.

UPPER MOTOR NEURONS, LOWER MOTOR NEURONS AND FINAL COMMON PATH
🧠 CORE
- Upper motor neurons originate in the brain and influence lower motor neurons.
- Lower motor neurons are located in anterior horn cells or cranial nerve motor nuclei.
- Lower motor neurons directly supply skeletal muscles.
- The lower motor neuron is called the final common path.
- Voluntary, reflex, and postural signals all ultimately act through lower motor neurons.
- Damage to UMN and LMN produces different clinical signs.
- The integrity of LMN is essential for any skeletal muscle contraction.
🔬 CONCEPT EXPLAINED
Motor signals reach skeletal muscle through a two-neuron concept. The upper motor neuron begins in higher centers such as the motor cortex or brainstem and descends toward the spinal cord. It does not usually supply muscle directly. Instead, it influences lower motor neurons.
The lower motor neuron is located in the anterior horn of the spinal cord. Its axon leaves through the ventral root, travels in a peripheral nerve, reaches the neuromuscular junction, and activates skeletal muscle. Because every voluntary or reflex motor command must finally pass through this neuron, it is called the final common path.
This concept is very important. A muscle cannot contract voluntarily or reflexly if its lower motor neuron is destroyed. Even if the brain sends a perfect command, the muscle will not receive it. Therefore, lower motor neurons are the final link between the nervous system and skeletal muscle.
Upper motor neurons mainly regulate and control lower motor neuron activity. They can facilitate or inhibit spinal reflexes, adjust tone, and control voluntary movement. When upper motor neuron control is lost, spinal reflex circuits may become overactive, producing increased tone and exaggerated reflexes.
⚠️ CLINICAL IMPORTANCE
Lower motor neuron lesions cause flaccid weakness, muscle wasting, fasciculations, and reduced or absent reflexes because the muscle loses its direct neural supply. Upper motor neuron lesions cause weakness with increased tone, exaggerated deep tendon reflexes, clonus, and Babinski sign because inhibitory control over spinal reflexes is reduced.
TYPES OF ANTERIOR HORN CELLS AND THEIR FUNCTIONS
🧠 CORE
- Anterior horn contains motor neurons and interneurons involved in motor control.
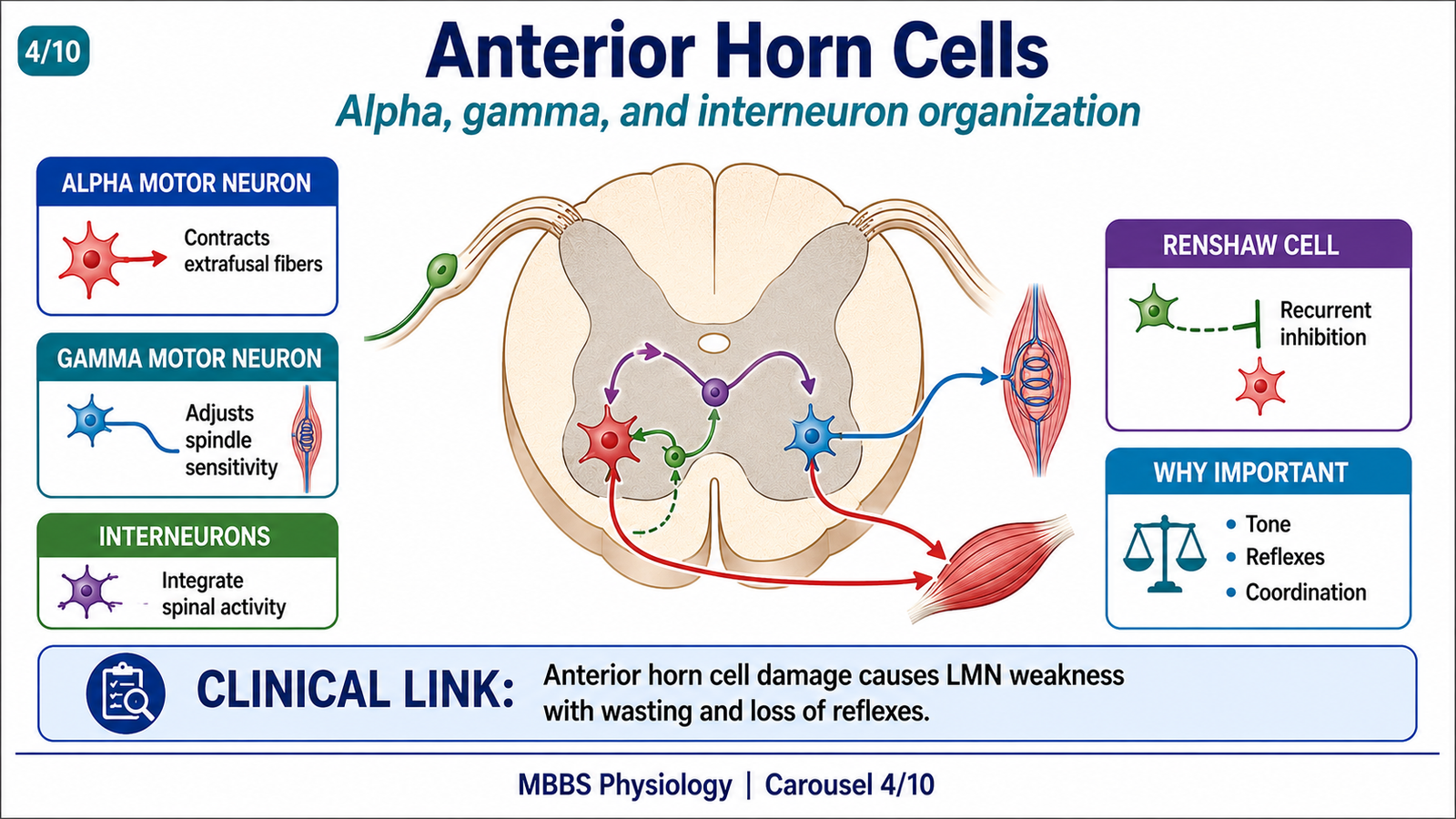
- Alpha motor neurons supply extrafusal skeletal muscle fibers.
- Gamma motor neurons supply intrafusal muscle spindle fibers.
- Alpha neurons produce actual muscle contraction.
- Gamma neurons adjust sensitivity of muscle spindles.
- Interneurons coordinate reflex activity within spinal cord.
- Renshaw cells provide recurrent inhibition of motor neurons.
🔬 CONCEPT EXPLAINED
The anterior horn of the spinal cord contains different cells that support motor function. The most important are alpha motor neurons and gamma motor neurons.
Alpha motor neurons are large neurons that supply ordinary skeletal muscle fibers, called extrafusal fibers. When alpha motor neurons fire, the muscle contracts and produces force. Therefore, alpha motor neurons are responsible for the visible motor action.
Gamma motor neurons supply the contractile ends of intrafusal fibers within muscle spindles. Their main function is not to produce strong muscle contraction, but to adjust the sensitivity of the muscle spindle. This is important because the spindle must remain sensitive during both rest and voluntary contraction.
The spinal cord also contains interneurons. These interneurons connect sensory neurons to motor neurons and coordinate complex reflexes. Some interneurons excite motor neurons, while others inhibit them. Renshaw cells are inhibitory interneurons that receive input from alpha motor neuron collaterals and then inhibit the same or nearby motor neurons. This prevents excessive motor neuron discharge and helps smooth motor output.
Therefore, anterior horn cells do not work as isolated motor switches. They form an organized motor network that controls muscle contraction, tone, reflex sensitivity, and coordination between agonist and antagonist muscles.
⚠️ CLINICAL IMPORTANCE
Diseases affecting anterior horn cells, such as poliomyelitis or motor neuron disease, damage lower motor neurons. This produces flaccid paralysis, muscle atrophy, fasciculations, and loss of reflexes. Because the anterior horn cells are the final motor neurons, their damage severely affects movement.
BROAD TYPES OF MOTOR ACTIVITIES
🧠 CORE
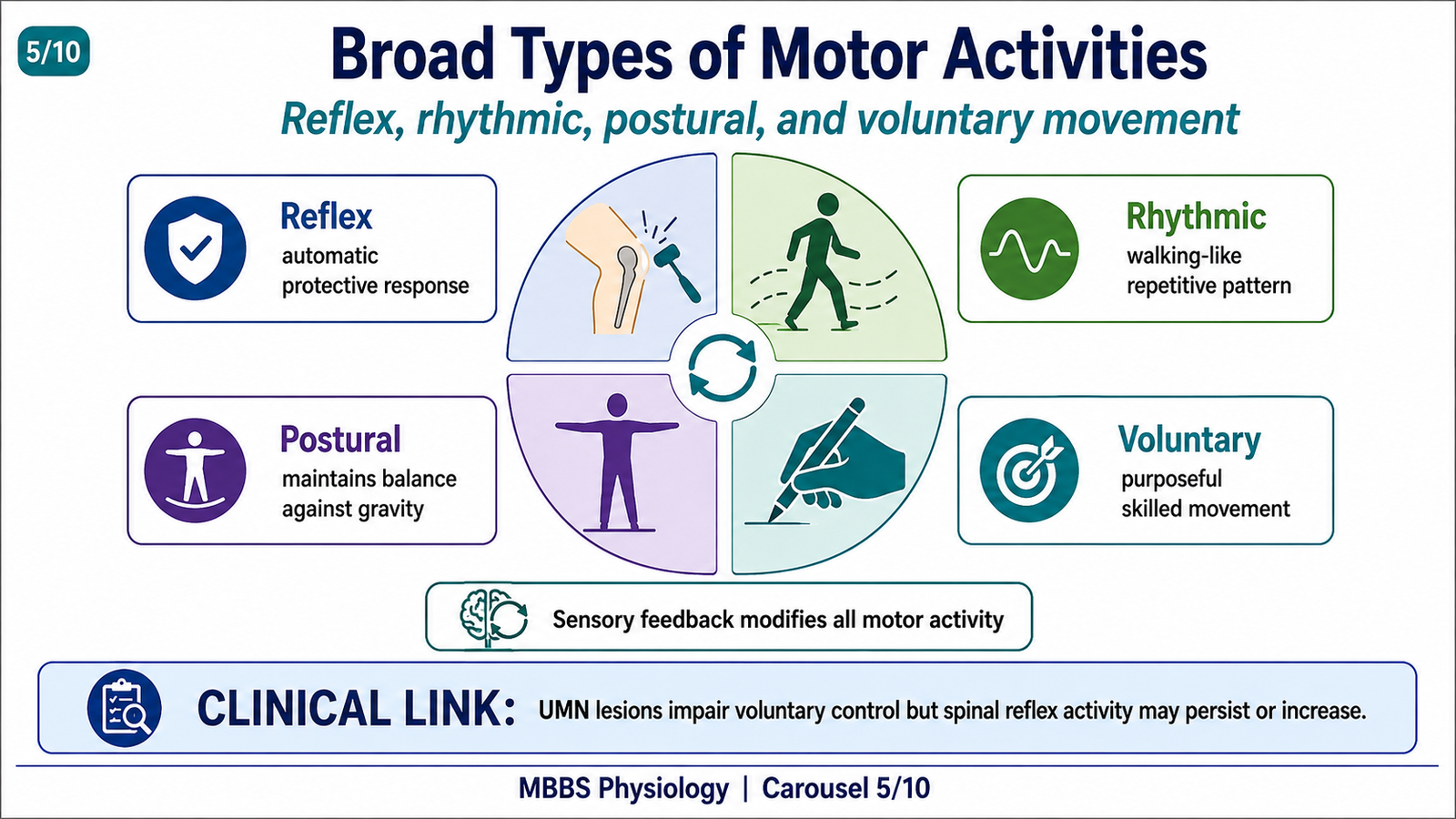
- Motor activities may be reflex, rhythmic, postural, or voluntary.
- Reflex movements are automatic and protective.
- Rhythmic movements include walking-like patterns.
- Postural movements maintain body position against gravity.
- Voluntary movements are purposeful and controlled by higher centers.
- Spinal cord participates in all these activities.
- Sensory feedback continuously modifies motor output.
🔬 CONCEPT EXPLAINED
Motor activity is not a single type of movement. The body uses different forms of motor control depending on the need.
Reflex movements are rapid and automatic. They protect the body and maintain muscle tone. For example, the stretch reflex helps maintain posture by resisting sudden stretching of muscles.
Rhythmic movements are repeated patterns such as walking. Although walking is initiated and controlled by the brain, spinal circuits can generate basic alternating flexion and extension patterns.
Postural movements maintain balance and body position. They depend on spinal reflexes, vestibular input, proprioception, and brainstem control.
Voluntary movements are conscious and purposeful. These movements are planned by the cerebral cortex but executed through spinal motor neurons.
This classification shows why the spinal cord is so important. It is involved not only in reflexes but also in posture and voluntary motor activity. Higher centers may decide the movement, but the spinal cord organizes the final output to muscles.
⚠️ CLINICAL IMPORTANCE
When descending pathways are damaged, voluntary movement becomes weak, but spinal reflexes may remain or become exaggerated. This explains why patients with upper motor neuron lesions may have paralysis along with increased tone and hyperreflexia.
REFLEX ACTION AND COMPONENTS OF REFLEX ARC
🧠 CORE
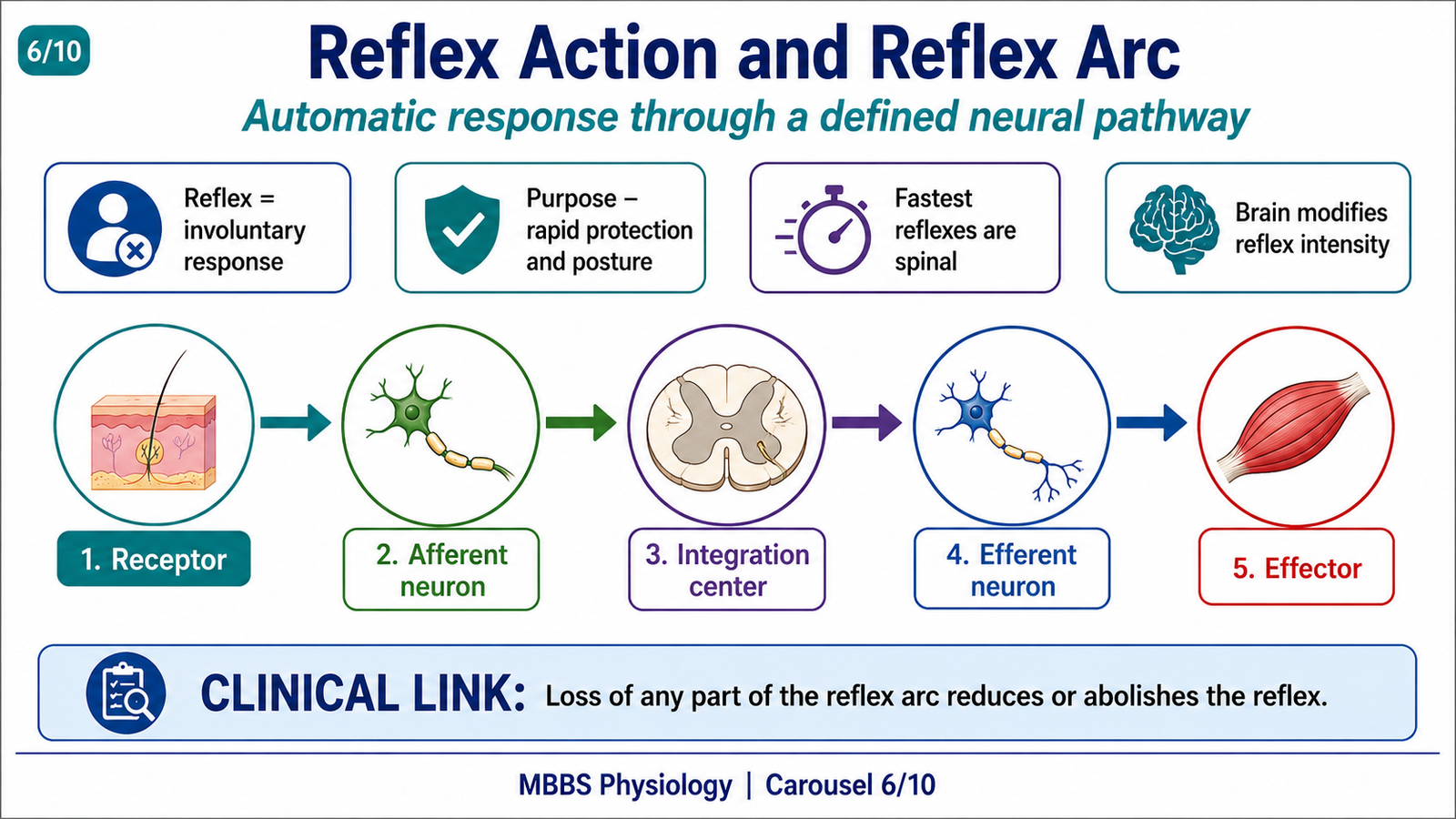
- A reflex is an automatic response to a stimulus.
- Reflex arc includes receptor, afferent neuron, integration center, efferent neuron, and effector.
- Reflexes may be monosynaptic or polysynaptic.
- Reflexes may be spinal, brainstem, or cortical depending on level of integration.
- Reflexes protect the body and maintain posture.
- Reflexes are modified by descending pathways.
- Clinical reflex testing checks integrity of the reflex arc.
🔬 CONCEPT EXPLAINED
A reflex is an involuntary response that occurs when a stimulus activates a receptor and produces a motor response through a defined neural pathway. This pathway is called a reflex arc.
The first component is the receptor, which detects the stimulus. For example, a muscle spindle detects stretch. The second component is the afferent neuron, which carries sensory information into the spinal cord. The third component is the integration center, where the sensory signal is processed. In simple reflexes, this may be a direct synapse with a motor neuron. In complex reflexes, interneurons are involved. The fourth component is the efferent neuron, usually a lower motor neuron. The final component is the effector, usually skeletal muscle.
The reflex arc exists because the body needs rapid responses. If every protective response required conscious decision-making, reaction time would be too slow. Reflexes allow the body to respond immediately while the brain is simultaneously informed.
Reflexes are not completely independent of the brain. Descending pathways can increase or decrease reflex activity. This is why emotional state, posture, attention, and neurological lesions can alter reflex responses.
⚠️ CLINICAL IMPORTANCE
If any component of the reflex arc is damaged, the reflex may be reduced or absent. Damage to the receptor, sensory nerve, spinal segment, motor neuron, peripheral nerve, neuromuscular junction, or muscle can all impair reflexes. Exaggerated reflexes usually indicate loss of descending inhibitory control from upper motor neurons.
TYPES OF REFLEXES AND THEIR LEVEL OF INTEGRATION
🧠 CORE
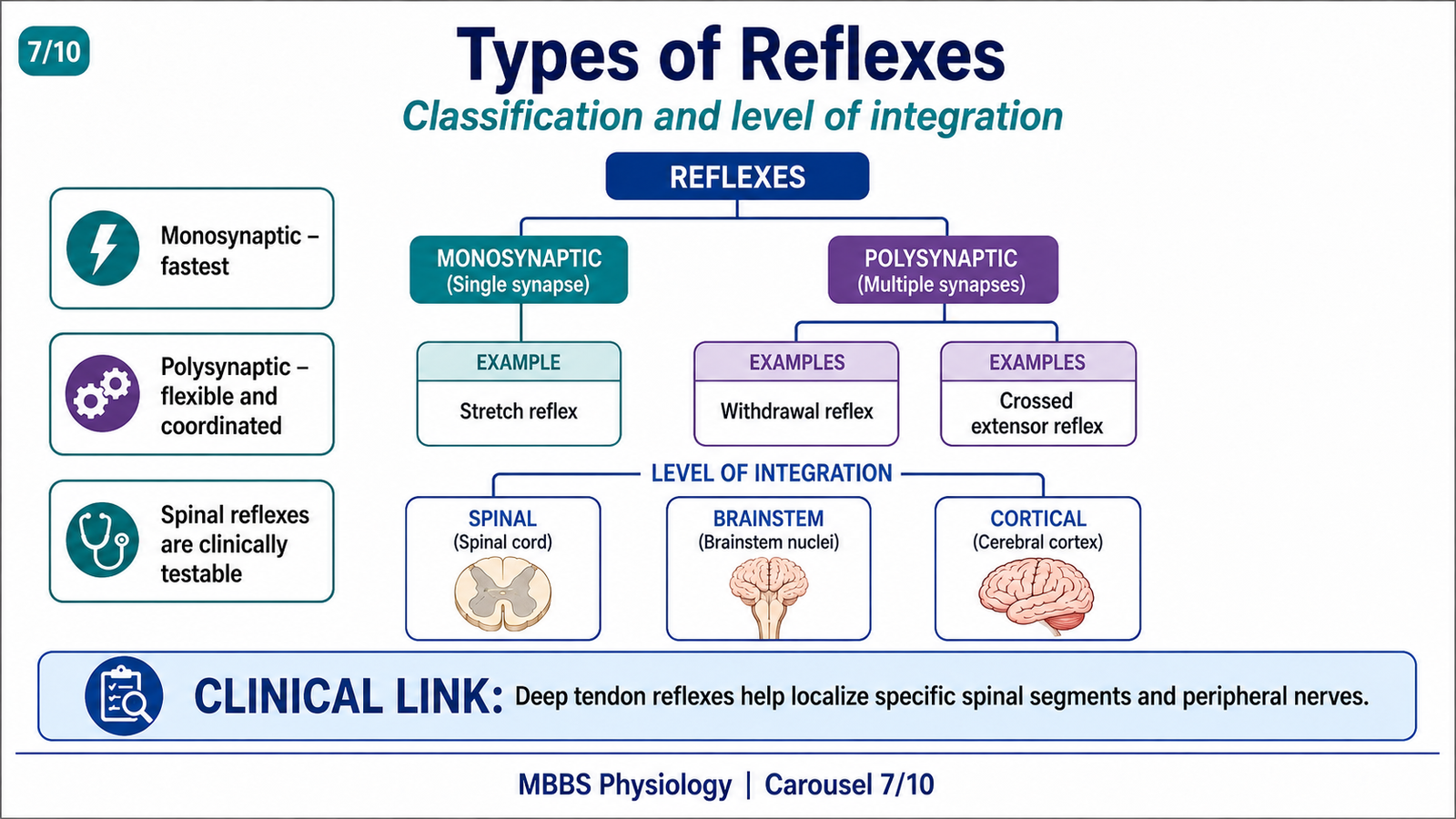
- Reflexes may be classified by synapses, receptor type, response, or integration level.
- Monosynaptic reflexes have one synapse.
- Polysynaptic reflexes involve interneurons.
- Spinal reflexes are integrated in the spinal cord.
- Brainstem reflexes are integrated in brainstem centers.
- Cortical reflexes involve higher brain processing.
- Reflex classification helps clinical localization.
🔬 CONCEPT EXPLAINED
Reflexes can be classified in several ways. Based on synapses, reflexes are either monosynaptic or polysynaptic. A monosynaptic reflex has one synapse between the sensory neuron and motor neuron. The stretch reflex is the classic example. A polysynaptic reflex has one or more interneurons between the sensory and motor neurons. Withdrawal reflex is an example.
Based on level of integration, reflexes may be spinal, brainstem, or cortical. Spinal reflexes are integrated within the spinal cord and can occur without conscious brain input. Brainstem reflexes involve nuclei in the brainstem, such as certain postural and cranial reflexes. Cortical reflexes require higher processing and are more complex.
This classification is useful because reflexes help localize lesions. For example, loss of a spinal reflex may suggest a lesion in the peripheral nerve or spinal segment involved. Exaggeration of a spinal reflex may suggest damage to descending upper motor neuron pathways.
⚠️ CLINICAL IMPORTANCE
Deep tendon reflexes such as knee jerk and ankle jerk are spinal reflexes. Their testing helps assess specific spinal segments and peripheral nerves. For example, the knee jerk mainly tests L2–L4 segments through the femoral nerve.
STRUCTURAL ORGANIZATION OF MUSCLE SPINDLE
🧠 CORE
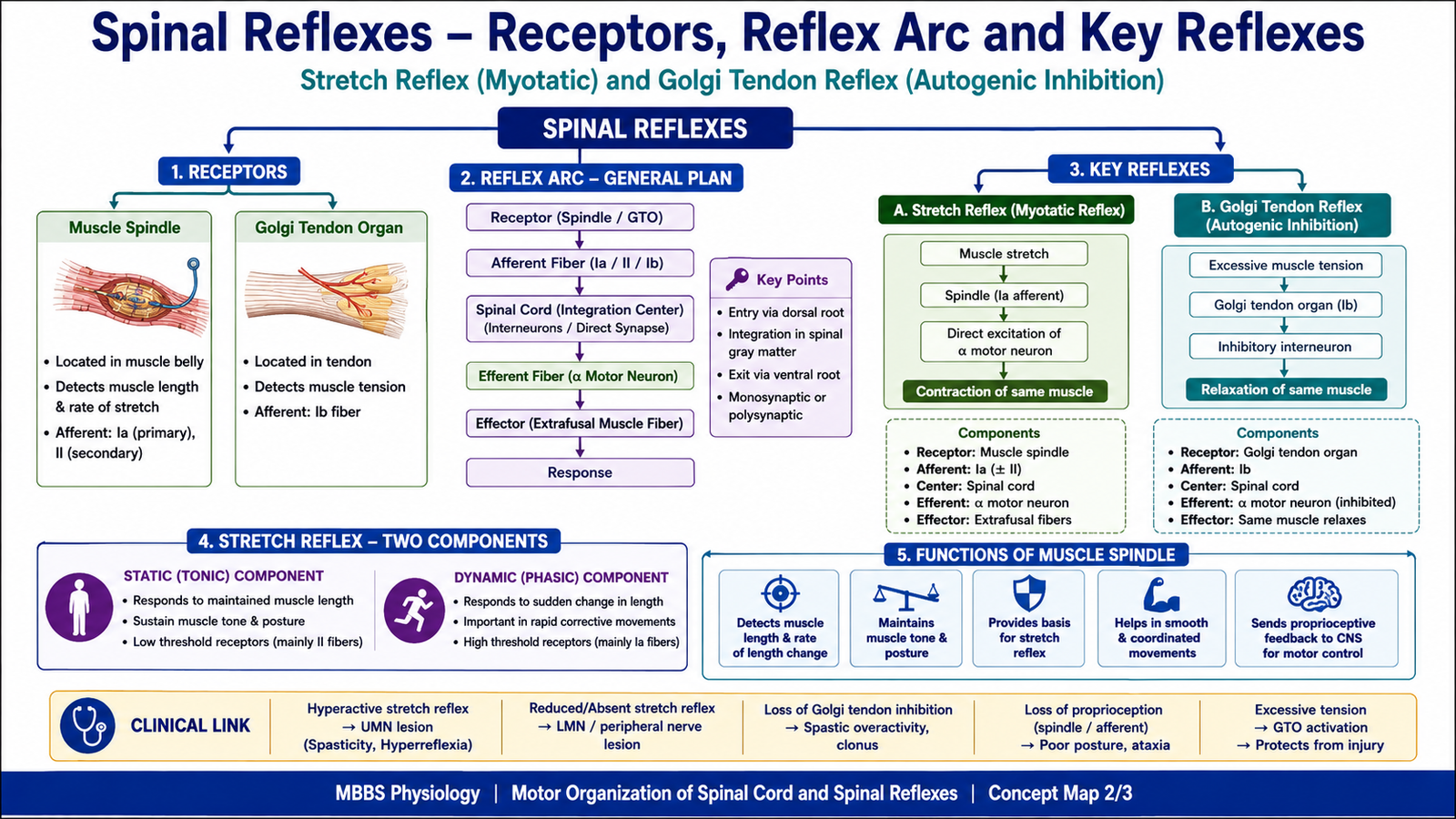
- Muscle spindle is a stretch receptor located within skeletal muscle.
- It lies parallel to extrafusal muscle fibers.
- It contains intrafusal fibers enclosed in a capsule.
- Intrafusal fibers include nuclear bag and nuclear chain fibers.
- Sensory endings include primary and secondary endings.
- Motor supply is by gamma motor neurons.
- Muscle spindle detects muscle length and rate of stretch.
🔬 CONCEPT EXPLAINED
To understand the stretch reflex, the structure of the muscle spindle must be clear. A muscle spindle is a specialized sensory receptor present inside skeletal muscle. It lies parallel to the ordinary force-producing extrafusal muscle fibers.
Inside the spindle are small specialized fibers called intrafusal fibers. These fibers do not produce major muscle force. Instead, they detect changes in muscle length. Intrafusal fibers are enclosed in a connective tissue capsule and have a central non-contractile region with sensory endings.
There are two main types of intrafusal fibers: nuclear bag fibers and nuclear chain fibers. Nuclear bag fibers are especially important for detecting dynamic changes, meaning how quickly muscle length is changing. Nuclear chain fibers are more important for detecting static muscle length.
Sensory endings wrap around the central region. Primary endings detect both the rate of stretch and the amount of stretch. Secondary endings mainly detect maintained muscle length. The contractile ends of intrafusal fibers receive gamma motor neuron supply. When gamma motor neurons activate these ends, they stretch the central sensory region and keep the spindle sensitive.
The muscle spindle exists because the nervous system needs continuous information about muscle length. Without this information, the body would not be able to maintain posture, muscle tone, or smooth voluntary movement.
⚠️ CLINICAL IMPORTANCE
Muscle spindle function is responsible for deep tendon reflexes. If spindle afferents, spinal segments, or motor neurons are damaged, stretch reflexes are reduced. If descending inhibition is lost, spindle-mediated reflexes may become exaggerated.
STRETCH REFLEX
🧠 CORE
- Stretch reflex is contraction of a muscle in response to its stretch.
- It is the simplest and most important spinal reflex.
- Muscle spindle is the receptor.
- Ia afferent fibers carry impulses to the spinal cord.
- Alpha motor neurons activate the stretched muscle.
- It is mainly monosynaptic.
- It maintains muscle tone and posture.
🔬 CONCEPT EXPLAINED
The stretch reflex occurs when a muscle is suddenly stretched. The stimulus is muscle stretch, the receptor is the muscle spindle, and the response is contraction of the same muscle.
For example, during the knee jerk reflex, tapping the patellar tendon stretches the quadriceps muscle. This stretch activates muscle spindles inside the quadriceps. The spindle sends impulses through Ia afferent fibers into the spinal cord. These fibers synapse directly with alpha motor neurons supplying the quadriceps. The alpha motor neurons then activate extrafusal muscle fibers, causing contraction of the quadriceps and extension of the knee.
The purpose of this reflex is to resist sudden changes in muscle length. If a muscle is unexpectedly stretched, contraction of that same muscle helps restore its original length. This is essential for posture. When a person is standing, gravity continuously tends to stretch antigravity muscles. Stretch reflexes automatically oppose this stretch and help maintain upright posture.
The stretch reflex also supports muscle tone. Muscle tone is not a fixed property of muscle; it depends partly on continuous low-level activity of spinal motor neurons influenced by muscle spindle input.
This reflex is mainly monosynaptic, which makes it very fast. However, associated interneurons also inhibit antagonist muscles, allowing smooth movement.
⚠️ CLINICAL IMPORTANCE
Deep tendon reflexes are examples of stretch reflexes. Increased stretch reflexes suggest upper motor neuron lesions. Reduced or absent reflexes suggest lower motor neuron damage, peripheral neuropathy, muscle disease, or interruption of the reflex arc.
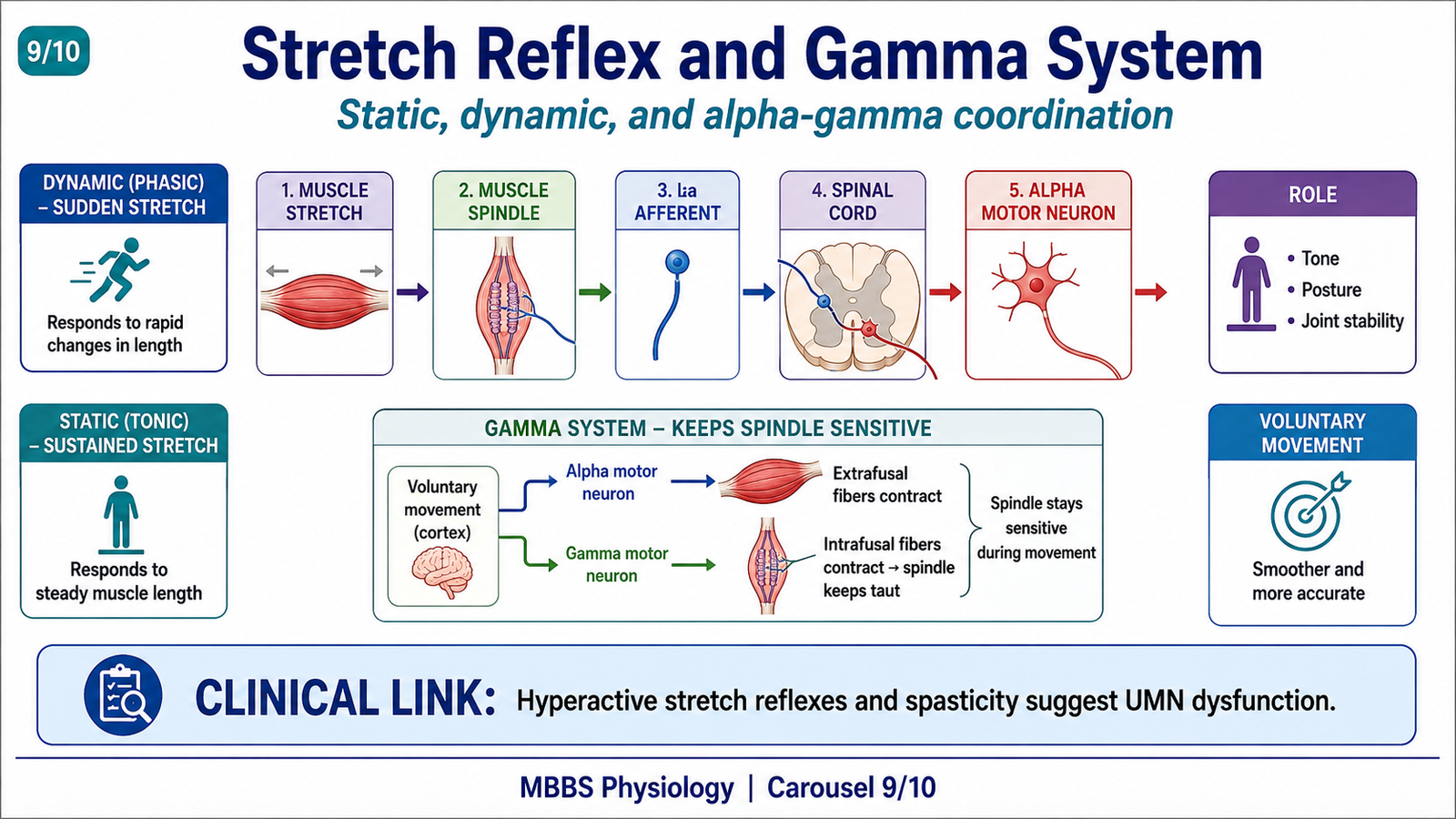
STATIC TONIC AND DYNAMIC PHASIC STRETCH REFLEX
🧠 CORE
- Stretch reflex has dynamic and static components.
- Dynamic stretch reflex responds to sudden rapid stretch.
- Static stretch reflex responds to maintained stretch.
- Nuclear bag fibers are more involved in dynamic response.
- Nuclear chain fibers contribute more to static response.
- Dynamic response helps correct sudden disturbances.
- Static response helps maintain posture and tone.
🔬 CONCEPT EXPLAINED
The stretch reflex is not a single uniform response. It has two important components: dynamic phasic and static tonic.
The dynamic phasic stretch reflex occurs when a muscle is suddenly and rapidly stretched. Muscle spindle primary endings discharge strongly because they detect the rate of change of muscle length. This produces a quick contraction of the stretched muscle. The dynamic response is useful for correcting sudden disturbances. For example, if a person begins to sway forward while standing, rapid stretch of postural muscles triggers a quick corrective contraction.
The static tonic stretch reflex occurs during sustained stretch. It depends on continued spindle activity during maintained muscle lengthening. This response is important for maintaining posture and muscle tone over time. It prevents muscles from becoming excessively lengthened during prolonged standing or postural activity.
The body needs both components. Dynamic response protects against sudden changes, while static response maintains stable posture. Together, they allow the nervous system to continuously monitor and regulate muscle length.
⚠️ CLINICAL IMPORTANCE
Exaggerated dynamic stretch reflex may appear as brisk tendon jerks or clonus in upper motor neuron lesions. Increased static stretch reflex contributes to spasticity, where muscles resist passive stretch abnormally.
FUNCTIONS OF MUSCLE SPINDLE
🧠 CORE
- Detects muscle length.
- Detects rate of change of muscle length.
- Initiates stretch reflex.
- Helps maintain muscle tone.
- Supports posture.
- Provides proprioceptive feedback.
- Assists smooth voluntary movement.
🔬 CONCEPT EXPLAINED
The muscle spindle is a key proprioceptor. Its first function is to detect the length of muscle. This tells the spinal cord and brain how stretched or shortened a muscle is at any moment.
Its second function is to detect the rate at which muscle length is changing. This is important because sudden stretch may threaten posture or joint stability. The spindle rapidly informs the spinal cord, which produces corrective contraction through the stretch reflex.
The spindle also helps maintain muscle tone. Continuous low-level spindle discharge helps keep alpha motor neurons slightly active, producing normal resting tone. This tone allows muscles to respond quickly when movement is required.
Another important function is its role in voluntary movement. During voluntary contraction, alpha motor neurons shorten extrafusal fibers. If the spindle became slack, it would stop providing useful sensory information. Gamma motor neurons prevent this by contracting the ends of intrafusal fibers, keeping the spindle sensitive. This allows the nervous system to monitor muscle length even during active movement.
Therefore, the muscle spindle is not only a reflex receptor. It is also a continuous feedback device for posture, tone, and coordinated motor control.
⚠️ CLINICAL IMPORTANCE
Loss of proprioceptive feedback from muscle spindles causes poor coordination and impaired posture. Excessive spindle sensitivity contributes to hyperreflexia and spasticity in upper motor neuron lesions.
GAMMA EFFERENT SYSTEM AND ITS ROLE IN VOLUNTARY MOTOR ACTIVITY
🧠 CORE
- Gamma motor neurons supply intrafusal muscle fibers.
- They adjust muscle spindle sensitivity.
- Gamma activity keeps spindles responsive during muscle contraction.
- Alpha-gamma coactivation occurs during voluntary movement.
- Gamma system helps maintain muscle tone.
- It improves accuracy of movement.
- It supports posture and reflex control.
🔬 CONCEPT EXPLAINED
The gamma efferent system is essential because muscle spindles must remain sensitive in different muscle states. If only extrafusal fibers contracted during voluntary movement, the whole muscle would shorten. This shortening could make the muscle spindle slack. A slack spindle cannot detect stretch properly.
To prevent this, the nervous system activates both alpha and gamma motor neurons during voluntary contraction. This is called alpha-gamma coactivation. Alpha motor neurons contract extrafusal fibers, producing movement. At the same time, gamma motor neurons contract the ends of intrafusal fibers. This stretches the central sensory region of the spindle and keeps it responsive.
The purpose of the gamma system is therefore to maintain spindle sensitivity. This allows continuous feedback about muscle length during movement. As a result, voluntary movements become smoother and more accurate.
Gamma activity also contributes to muscle tone. Increased gamma discharge makes spindles more sensitive, increasing reflex activation of alpha motor neurons. Decreased gamma activity reduces spindle sensitivity and lowers tone.
⚠️ CLINICAL IMPORTANCE
In upper motor neuron lesions, increased gamma activity and loss of descending inhibition may contribute to spasticity and exaggerated stretch reflexes. Clinically, this appears as increased resistance to passive movement and brisk tendon reflexes.
PHYSIOLOGICAL SIGNIFICANCE OF STRETCH REFLEX
🧠 CORE
- Maintains muscle length.
- Maintains posture.
- Contributes to muscle tone.
- Stabilizes joints.
- Smooths voluntary movement.
- Protects muscles from sudden stretch.
- Provides clinical deep tendon reflexes.
🔬 CONCEPT EXPLAINED
The stretch reflex is physiologically important because it acts as a negative feedback mechanism for muscle length. When a muscle is stretched, the reflex causes it to contract. This contraction opposes the stretch and helps restore the muscle to its previous length.
This mechanism is important during posture. When standing, gravity tends to stretch antigravity muscles such as quadriceps, gastrocnemius, and back muscles. Muscle spindles detect this stretch and activate reflex contraction. This helps prevent collapse and maintains upright posture.
The stretch reflex also stabilizes joints. If an external force suddenly stretches muscles around a joint, reflex contraction helps resist excessive movement. This protects joints and maintains balance.
During voluntary movement, the stretch reflex helps smooth motor activity. If a movement is disturbed unexpectedly, spindle feedback allows rapid correction before conscious control is fully involved.
⚠️ CLINICAL IMPORTANCE
Deep tendon reflex testing evaluates stretch reflex pathways. Hyperreflexia indicates increased excitability of spinal reflex circuits, commonly due to upper motor neuron lesions. Hyporeflexia or areflexia indicates damage to the reflex arc or lower motor neuron system.
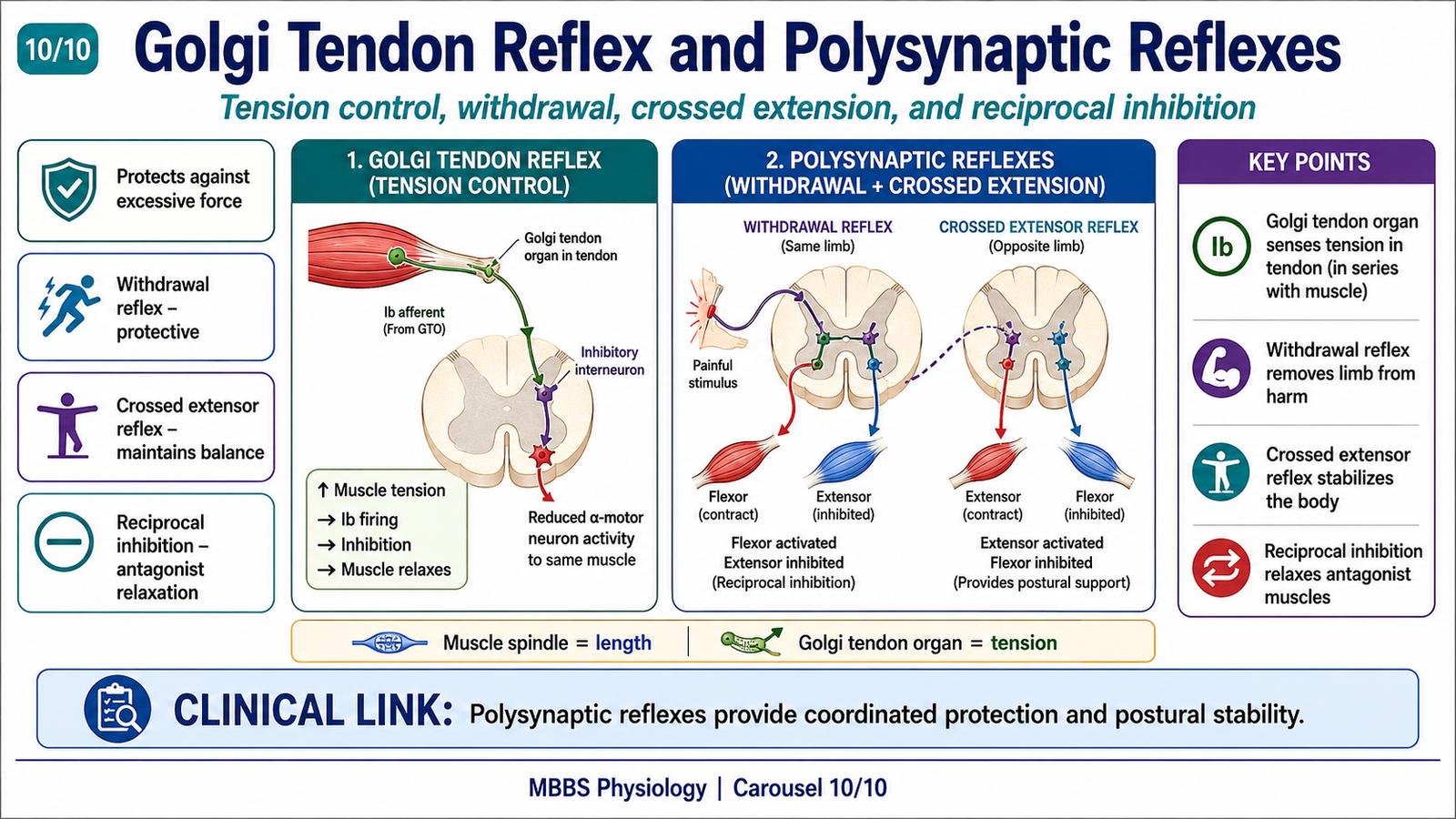
GOLGI TENDON REFLEX
🧠 CORE
- Golgi tendon organ is a tension receptor in tendons.
- It lies in series with muscle fibers.
- It detects muscle tension.
- Ib afferent fibers carry impulses to spinal cord.
- It inhibits the same muscle through inhibitory interneurons.
- It protects muscle and tendon from excessive tension.
- It helps regulate force during movement.
🔬 CONCEPT EXPLAINED
The Golgi tendon reflex is different from the stretch reflex. The receptor is the Golgi tendon organ, located in the tendon near the junction between muscle and tendon. Unlike the muscle spindle, which lies parallel to muscle fibers and detects length, the Golgi tendon organ lies in series with muscle fibers and detects tension.
When a muscle contracts strongly, tension increases in the tendon. The Golgi tendon organ detects this tension and sends impulses through Ib afferent fibers into the spinal cord. These fibers activate inhibitory interneurons. The inhibitory interneurons reduce alpha motor neuron activity to the same muscle. As a result, the contracting muscle relaxes.
This reflex is called an inverse stretch reflex because instead of causing contraction, it causes relaxation when tension becomes excessive. The purpose is protective. It prevents excessive force from damaging muscles, tendons, or joints.
The Golgi tendon organ also helps regulate force during normal movement. It provides feedback about how much tension the muscle is producing, allowing the nervous system to adjust contraction strength smoothly.
⚠️ CLINICAL IMPORTANCE
Abnormal regulation of muscle tension can contribute to poor motor control. The Golgi tendon reflex is also important conceptually for understanding protective inhibition and force regulation during posture and movement.
DIFFERENCE BETWEEN MUSCLE SPINDLE AND GOLGI TENDON ORGAN
🧠 CORE
- Muscle spindle detects muscle length and stretch.
- Golgi tendon organ detects muscle tension.
- Muscle spindle lies parallel to muscle fibers.
- Golgi tendon organ lies in series with muscle fibers.
- Muscle spindle uses mainly Ia and II afferents.
- Golgi tendon organ uses Ib afferents.
- Muscle spindle facilitates contraction; Golgi tendon organ inhibits excessive contraction.
🔬 CONCEPT EXPLAINED
Muscle spindle and Golgi tendon organ are both proprioceptors, but they monitor different mechanical properties.
The muscle spindle is located within the muscle belly and lies parallel to extrafusal fibers. Because of this arrangement, it is stretched when the whole muscle is stretched. Its main function is to detect muscle length and rate of change of length. When activated, it causes contraction of the same muscle through the stretch reflex.
The Golgi tendon organ is located in the tendon and lies in series with muscle fibers. Because of this arrangement, it is activated mainly by tension produced during muscle contraction. When tension becomes high, it inhibits the same muscle through interneurons, preventing excessive force.
Therefore, the spindle protects and regulates muscle length, while the Golgi tendon organ protects and regulates muscle tension. Both work together to make movement smooth, safe, and coordinated.
⚠️ CLINICAL IMPORTANCE
Understanding the difference between these receptors is commonly tested. Muscle spindle is linked with stretch reflex and tone, while Golgi tendon organ is linked with inverse stretch reflex and tension regulation.
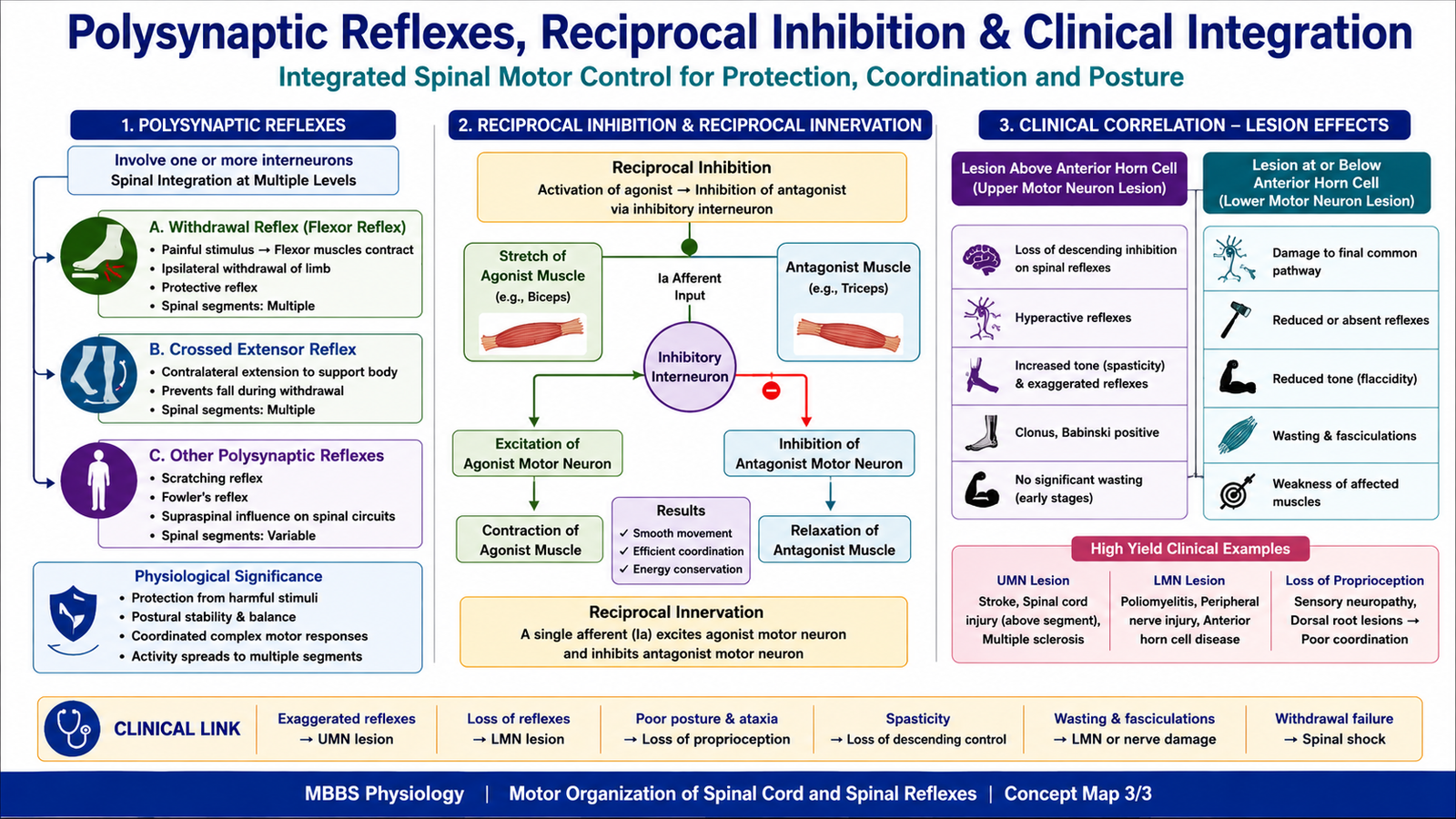
POLYSYNAPTIC REFLEXES AND THEIR LEVEL OF INTEGRATION
🧠 CORE
- Polysynaptic reflexes involve one or more interneurons.
- They are slower than monosynaptic reflexes but more flexible.
- They may involve many spinal segments.
- Important examples include withdrawal reflex, crossed extensor reflex, and reciprocal inhibition.
- They integrate sensory input from pain, touch, muscles, and joints.
- They produce coordinated motor responses.
- Their integration is mainly spinal but modified by higher centers.
🔬 CONCEPT EXPLAINED
Polysynaptic reflexes are reflexes in which sensory neurons do not directly synapse with motor neurons. Instead, one or more interneurons are present between afferent and efferent pathways. This makes the reflex slower than a monosynaptic reflex, but it also makes it more adaptable and coordinated.
A good example is the withdrawal reflex. When a painful stimulus affects the foot, pain fibers enter the spinal cord and activate interneurons. These interneurons excite flexor motor neurons, causing the limb to withdraw. At the same time, they inhibit extensor motor neurons so that the movement is not opposed.
Another important example is the crossed extensor reflex. If one limb withdraws from a painful stimulus, the opposite limb must extend to support body weight. Interneurons cross to the opposite side of the spinal cord and activate extensor muscles while inhibiting flexors. This maintains balance.
Polysynaptic reflexes may involve multiple spinal segments. This allows several muscles to act together in a coordinated pattern. The brain can also modify these reflexes depending on posture, attention, and context.
⚠️ CLINICAL IMPORTANCE
Polysynaptic reflexes are important in protective withdrawal and posture. In spinal cord lesions, reflex patterns may become abnormal because descending control is lost. Primitive or exaggerated reflex responses may appear below the level of lesion.
PHYSIOLOGICAL SIGNIFICANCE OF POLYSYNAPTIC REFLEXES
🧠 CORE
- They protect the body from harmful stimuli.
- They coordinate multiple muscle groups.
- They allow withdrawal from pain.
- They maintain balance through crossed extensor activity.
- They support posture and locomotor patterns.
- They allow inhibition of antagonist muscles.
- They are adaptable because interneurons modify responses.
🔬 CONCEPT EXPLAINED
Polysynaptic reflexes are physiologically significant because real-life movements usually require coordination of multiple muscles. A simple direct reflex is useful for rapid response, but complex protective and postural actions require interneurons.
For example, when the foot steps on a sharp object, simply contracting one muscle is not enough. The flexors of that limb must contract, extensors must relax, and the opposite limb must extend to support the body. This coordinated response is possible because polysynaptic circuits connect many motor neuron pools across different spinal segments.
Polysynaptic reflexes also allow the nervous system to adjust responses according to stimulus strength. A weak painful stimulus may produce mild withdrawal, while a strong stimulus may produce a stronger and more widespread response. This graded response is possible because interneuronal networks can recruit more motor neurons.
Thus, polysynaptic reflexes provide protection, coordination, posture, and adaptability.
⚠️ CLINICAL IMPORTANCE
Loss of polysynaptic reflexes can impair protective responses. Exaggeration of these reflexes may occur after loss of descending inhibition, especially in spinal cord injury or upper motor neuron lesions.
RECIPROCAL INHIBITION AND RECIPROCAL INNERVATION
🧠 CORE
- Reciprocal innervation means coordinated activation of agonists and inhibition of antagonists.
- Reciprocal inhibition is the inhibitory component of this process.
- It occurs through inhibitory interneurons in the spinal cord.
- It allows smooth movement around joints.
- It is important in stretch reflex and withdrawal reflex.
- It prevents opposing muscles from contracting strongly at the same time.
- It improves efficiency and coordination of movement.
🔬 CONCEPT EXPLAINED
Movement around a joint requires cooperation between agonist and antagonist muscles. When one muscle contracts, the opposite muscle must usually relax. This principle is called reciprocal innervation.
For example, during knee extension, the quadriceps contracts while the hamstrings relax. If both contracted strongly at the same time, movement would be stiff, inefficient, and difficult.
The mechanism responsible for relaxation of the antagonist is called reciprocal inhibition. In the stretch reflex, Ia afferent fibers from the stretched muscle excite alpha motor neurons supplying that same muscle. At the same time, collateral branches activate inhibitory interneurons that inhibit alpha motor neurons supplying the antagonist muscle.
This arrangement exists because smooth movement requires not only activation but also selective inhibition. Motor control is therefore based on coordinated excitation and inhibition.
⚠️ CLINICAL IMPORTANCE
Failure of reciprocal inhibition can produce stiffness and abnormal co-contraction of muscles. In upper motor neuron lesions, abnormal reflex activity and impaired inhibitory control contribute to spasticity and difficulty in smooth voluntary movement.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Function | Functional Outcome |
|---|---|---|
| Anterior horn cells | Send motor commands to skeletal muscle | Final motor output |
| Alpha motor neurons | Supply extrafusal fibers | Muscle contraction and force generation |
| Gamma motor neurons | Supply intrafusal fibers | Adjust muscle spindle sensitivity |
| Muscle spindle | Detects muscle length and stretch | Stretch reflex, tone, posture |
| Golgi tendon organ | Detects tendon tension | Protection from excessive force |
| Ia afferent fibers | Carry spindle stretch information | Rapid monosynaptic reflex |
| Ib afferent fibers | Carry tendon tension information | Autogenic inhibition |
| Interneurons | Coordinate excitation and inhibition | Polysynaptic reflexes and reciprocal inhibition |
| Descending motor pathways | Modify spinal circuits | Voluntary control and reflex regulation |
| Extrafusal muscle fibers | Produce contraction | Movement and posture |
| Intrafusal muscle fibers | Sense stretch | Proprioceptive feedback |
The spinal motor system works through continuous integration. Muscle spindles inform the spinal cord about muscle length, Golgi tendon organs inform it about muscle tension, and sensory receptors in skin and joints provide additional feedback. The spinal cord processes this information through motor neurons and interneurons. Descending pathways from the brain modify the output according to voluntary intention and posture.
Therefore, movement is not produced by muscle contraction alone. It depends on a complete system: receptor detection, sensory transmission, spinal integration, motor neuron discharge, muscle contraction, and feedback correction.
🩺 5️⃣ Clinical Correlation
1. Upper Motor Neuron Lesion
An upper motor neuron lesion reduces descending control over spinal motor circuits. As a result, spinal reflexes become overactive.
Important features:
- Weakness
- Increased muscle tone
- Hyperreflexia
- Clonus
- Spasticity
- Babinski sign
Cause → Effect:
Loss of descending inhibition → increased spinal reflex excitability → exaggerated stretch reflexes and spasticity.
2. Lower Motor Neuron Lesion
A lower motor neuron lesion damages the final common path to skeletal muscle. Because the muscle loses its direct motor supply, both voluntary and reflex contractions are impaired.
Important features:
- Flaccid weakness
- Muscle wasting
- Fasciculations
- Hypotonia
- Reduced or absent reflexes
Cause → Effect:
Damage to anterior horn cell or peripheral motor axon → loss of muscle activation → weakness, wasting, and absent reflexes.
3. Peripheral Neuropathy
Peripheral neuropathy may damage sensory or motor components of the reflex arc. If sensory afferents are affected, the spinal cord does not receive stretch information. If motor efferents are affected, muscle cannot contract properly.
Important exam point:
Reduced ankle jerk is common in peripheral neuropathy.
Cause → Effect:
Peripheral nerve damage → interrupted reflex arc → reduced or absent tendon reflexes.
4. Spinal Cord Injury
Spinal cord injury interrupts descending motor pathways and may also damage spinal segments. Initially, reflexes may be absent due to spinal shock. Later, reflexes below the lesion may become exaggerated because descending inhibition is lost.
Cause → Effect:
Spinal cord damage → loss of brain control over spinal circuits → abnormal tone, reflexes, and voluntary movement.
5. Spasticity
Spasticity is increased resistance to passive stretch, commonly due to upper motor neuron lesions. It is associated with exaggerated stretch reflex activity.
Cause → Effect:
Loss of inhibitory descending control → increased gamma and alpha motor neuron excitability → exaggerated stretch reflex → velocity-dependent increase in tone.
6. Loss of Proprioception
Damage to proprioceptive pathways affects information from muscle spindles and joints. The patient may have poor coordination and difficulty maintaining posture, especially when visual input is removed.
Cause → Effect:
Loss of sensory feedback → poor awareness of limb position → unsteady movement and posture.
📌 6️⃣ Summary Points
- The spinal cord is a motor control center, not just a conducting pathway.
- Lower motor neurons are the final common path for skeletal muscle activity.
- Alpha motor neurons supply extrafusal fibers and produce contraction.
- Gamma motor neurons supply intrafusal fibers and maintain muscle spindle sensitivity.
- Muscle spindle detects muscle length and rate of stretch.
- Stretch reflex is mainly monosynaptic and maintains tone and posture.
- Dynamic stretch reflex responds to sudden stretch; static stretch reflex responds to maintained stretch.
- Golgi tendon organ detects muscle tension and produces inhibitory relaxation of the same muscle.
- Muscle spindle lies parallel to muscle fibers; Golgi tendon organ lies in series with muscle fibers.
- Polysynaptic reflexes involve interneurons and coordinate protective responses.
- Reciprocal inhibition allows agonist contraction with antagonist relaxation.
- Hyperreflexia suggests UMN lesion; hyporeflexia suggests LMN/reflex arc lesion.