
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Spinal cord lesions are important because the spinal cord is the main pathway through which the brain controls muscles and receives sensory information from the body.
It lies inside the vertebral canal and contains ascending sensory tracts, descending motor tracts, anterior horn cells, interneurons, and reflex circuits.
Damage to different parts of the spinal cord produces characteristic motor, sensory, reflex, and autonomic abnormalities.
Understanding upper motor neuron and lower motor neuron lesions helps students localize neurological disease clinically.
Spinal shock, Brown-Séquard syndrome, and paraplegia are major clinical patterns that demonstrate how spinal cord physiology becomes disturbed after injury.
This topic integrates physiology with general medicine by linking motor control, muscle tone, reflexes, spinal pathways, and neurological examination findings.
It is highly relevant for MBBS students because spinal cord lesions are commonly tested in written exams, viva, clinical case discussions, and later medicine rotations.
🔹 2️⃣ Foundation Concepts
Key Definitions
• Muscle tone: Continuous, mild, involuntary contraction of skeletal muscles present even at rest.
• Upper motor neuron: Neuron or pathway from cerebral cortex or brainstem that controls lower motor neurons.
• Lower motor neuron: Final motor neuron that directly supplies skeletal muscle.
• UMN lesion: Damage to descending motor pathways above the anterior horn cell or motor cranial nerve nucleus.
• LMN lesion: Damage to anterior horn cell, nerve root, peripheral nerve, neuromuscular junction, or motor unit.
• Spinal shock: Temporary loss of spinal cord function below the level of acute spinal cord injury.
• Brown-Séquard syndrome: Hemisection of the spinal cord causing ipsilateral motor and proprioceptive loss with contralateral pain and temperature loss.
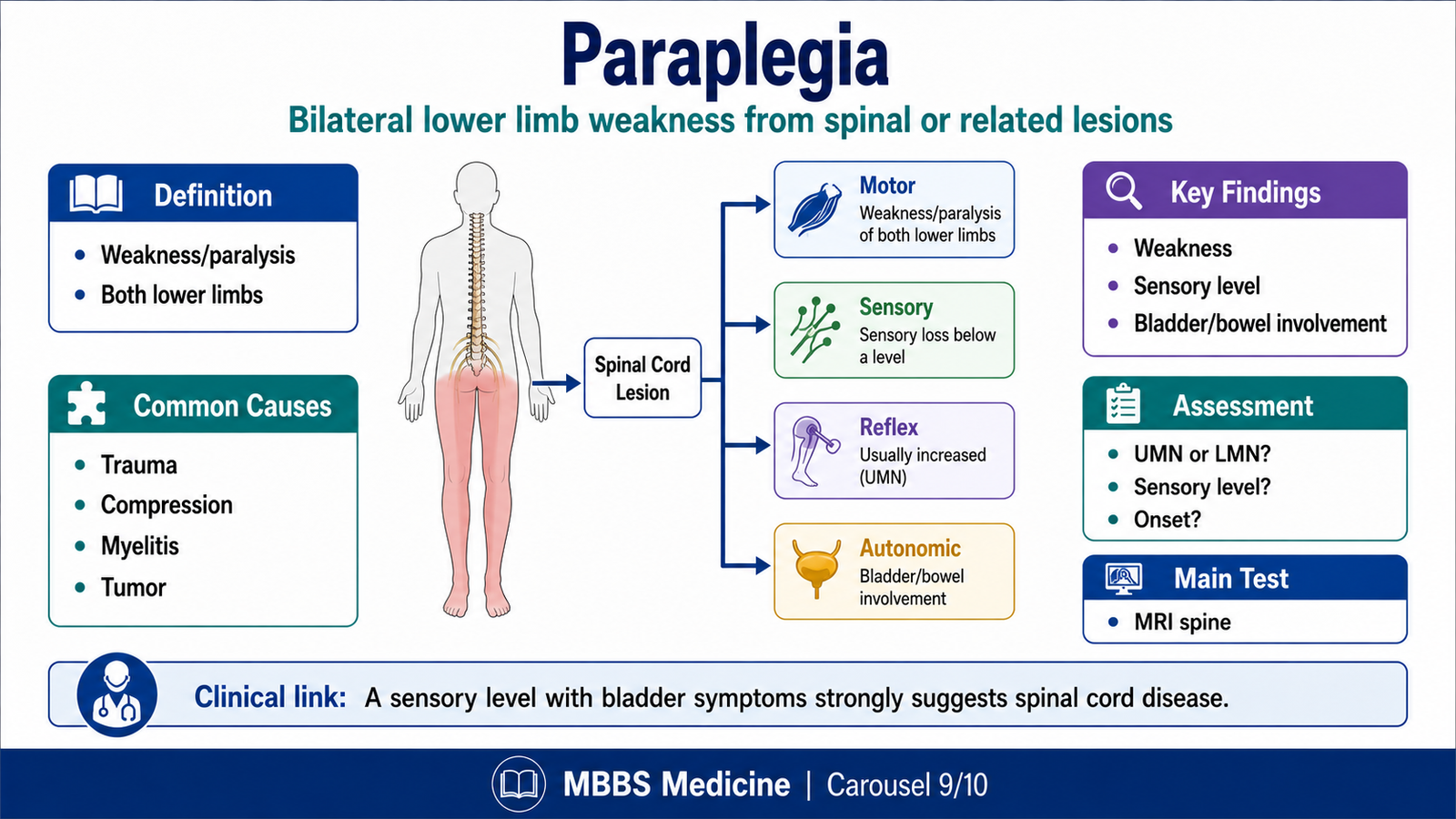
• Paraplegia: Loss or severe weakness of motor function in both lower limbs due to spinal cord, brain, or peripheral nervous system disease.
• Stroke: Acute neurological deficit due to interruption of blood supply to part of the brain.
Essential Terminology
• Pyramidal tract: Corticospinal tract responsible for skilled voluntary movement.
• Extrapyramidal system: Motor control pathways involved in posture, tone, and automatic movements.
• Deep tendon reflex: Reflex contraction of muscle after tendon stretch.
• Babinski sign: Extension of great toe with fanning of other toes, indicating UMN lesion after infancy.
• Flaccidity: Reduced muscle tone.
• Spasticity: Increased tone due to UMN lesion, usually velocity-dependent.
• Hyperreflexia: Exaggerated deep tendon reflexes.
• Hyporeflexia or areflexia: Reduced or absent reflexes.
• Fasciculation: Visible spontaneous twitching of muscle fibers due to LMN irritation.
• Sensory level: Dermatome below which sensation is impaired, suggesting spinal cord lesion.
Basic Overview
• The spinal cord carries motor commands from brain to muscles and sensory information from body to brain.
• Descending tracts control voluntary movement, posture, tone, and reflex modulation.
• Anterior horn cells form the final common pathway for skeletal muscle contraction.
• Muscle tone depends on stretch reflex activity, gamma motor neurons, muscle spindles, and descending control.
• UMN lesions remove inhibitory control over spinal reflexes, causing spasticity and hyperreflexia.
• LMN lesions damage the final pathway to muscle, causing weakness, wasting, fasciculations, and reduced reflexes.
• Acute spinal cord injury initially causes spinal shock before later UMN signs appear below the lesion.
• Brown-Séquard syndrome and paraplegia are important clinical examples of tract involvement.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPT 1 — Functional Organization of Motor Control in the Spinal Cord
🧠 CORE
• The spinal cord contains motor neurons, sensory neurons, interneurons, reflex circuits, and ascending and descending tracts.
• Anterior horn cells are lower motor neurons and form the final common pathway to skeletal muscle.
• Corticospinal tracts carry voluntary motor commands from the cerebral cortex.
• Reticulospinal and vestibulospinal pathways influence posture, tone, and antigravity activity.
• Muscle spindles detect stretch and contribute to tone and reflexes.
• Descending pathways normally regulate spinal reflex excitability.
• Damage at different levels produces different clinical signs.
🔬 CONCEPT EXPLAINED
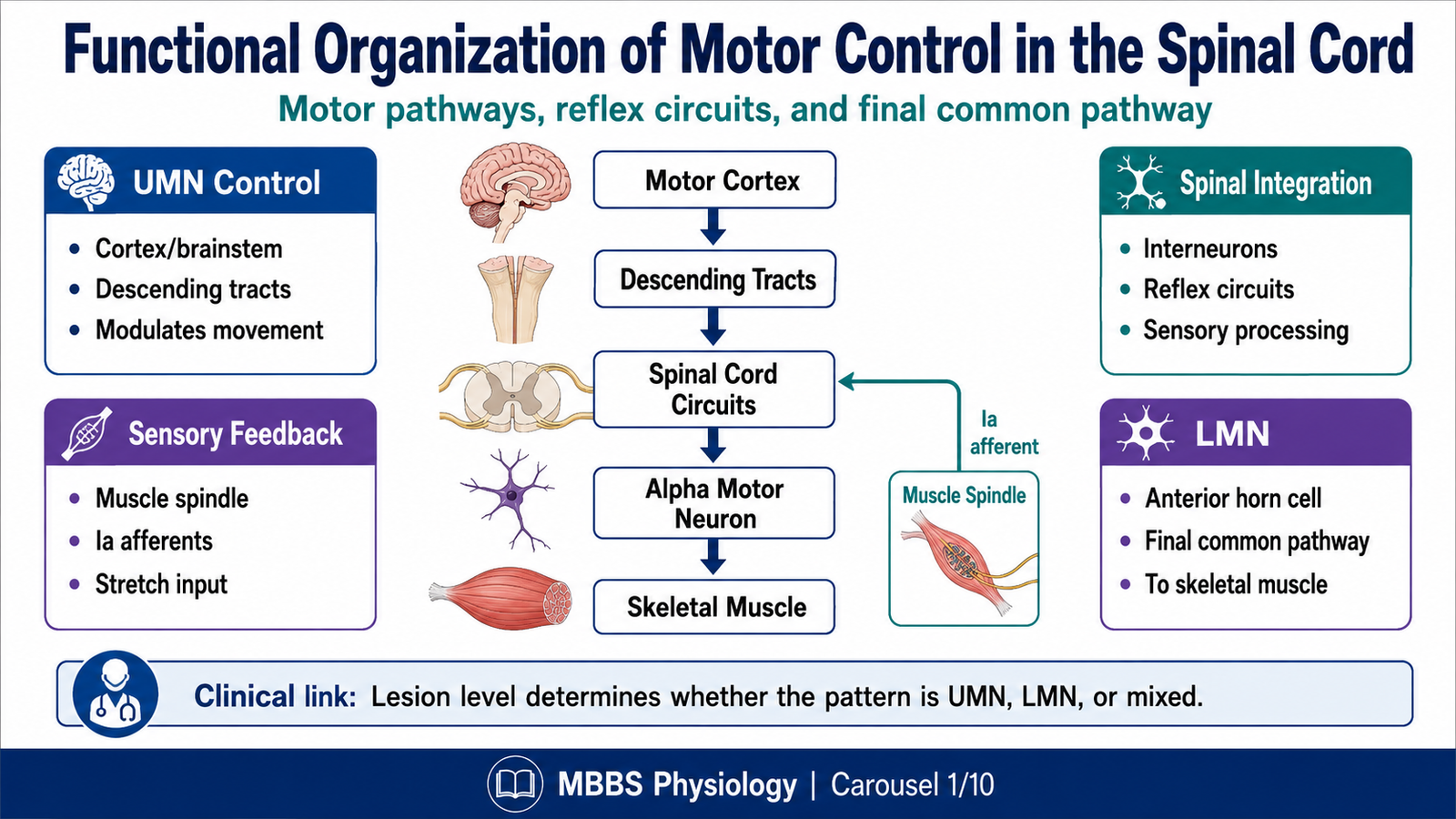
To understand spinal cord lesions, students must first understand how normal movement is produced. Voluntary movement begins in motor areas of the cerebral cortex and travels through descending motor pathways, especially the corticospinal tract. These descending fibers do not directly contract muscle. Instead, they influence lower motor neurons located in the anterior horn of the spinal cord.
The lower motor neuron is called the final common pathway because all motor influences must ultimately act through it. Whether movement is voluntary, reflex, postural, or automatic, skeletal muscle contraction occurs only when lower motor neurons send impulses through peripheral nerves to muscle fibers.
The spinal cord is not simply a cable between brain and muscle. It contains local circuits that process sensory information and generate reflex responses. Muscle spindles send information about muscle stretch to the spinal cord. This sensory input activates alpha motor neurons and helps maintain tone. Gamma motor neurons adjust the sensitivity of muscle spindles so that they continue to detect stretch during movement.
Descending pathways from the brain normally balance excitation and inhibition within the spinal cord. They allow voluntary movement while preventing excessive reflex activity. Therefore, motor control depends on a continuous interaction between brain commands, spinal reflex circuits, sensory feedback, and muscle response.
When this system is damaged, the clinical picture depends on which part is affected. If the descending upper motor neuron pathway is damaged but the lower motor neuron remains intact, spinal reflexes become overactive. If the lower motor neuron itself is damaged, the muscle loses its direct motor supply and becomes weak, flaccid, and wasted.
⚠️ CLINICAL IMPORTANCE
Motor examination helps localize lesions. Increased tone and exaggerated reflexes suggest UMN involvement, while wasting, fasciculations, and absent reflexes suggest LMN damage. This distinction is one of the most important principles in clinical neurology.
MAJOR CONCEPT 2 — Muscle Tone and Its Significance
🧠 CORE
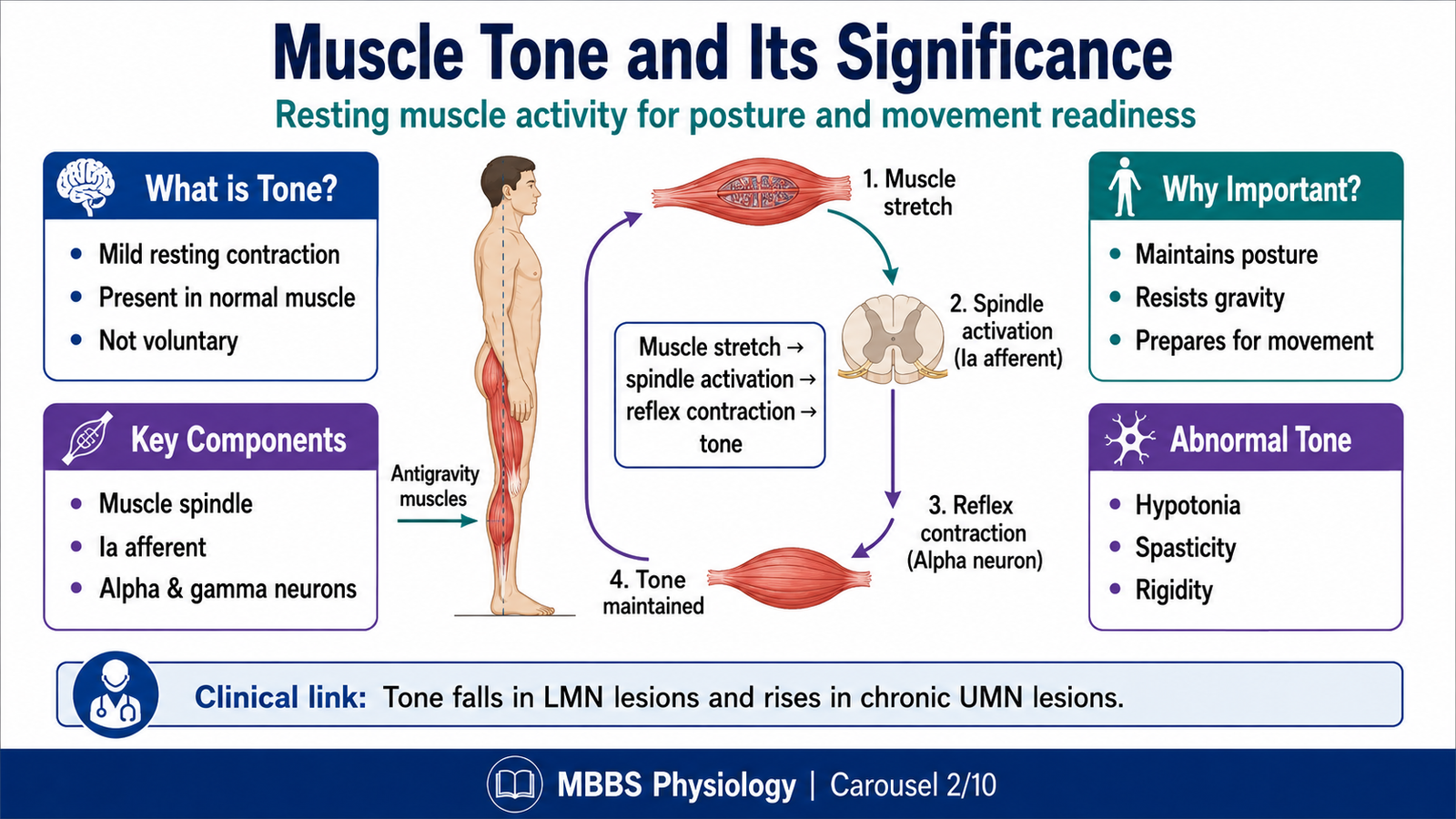
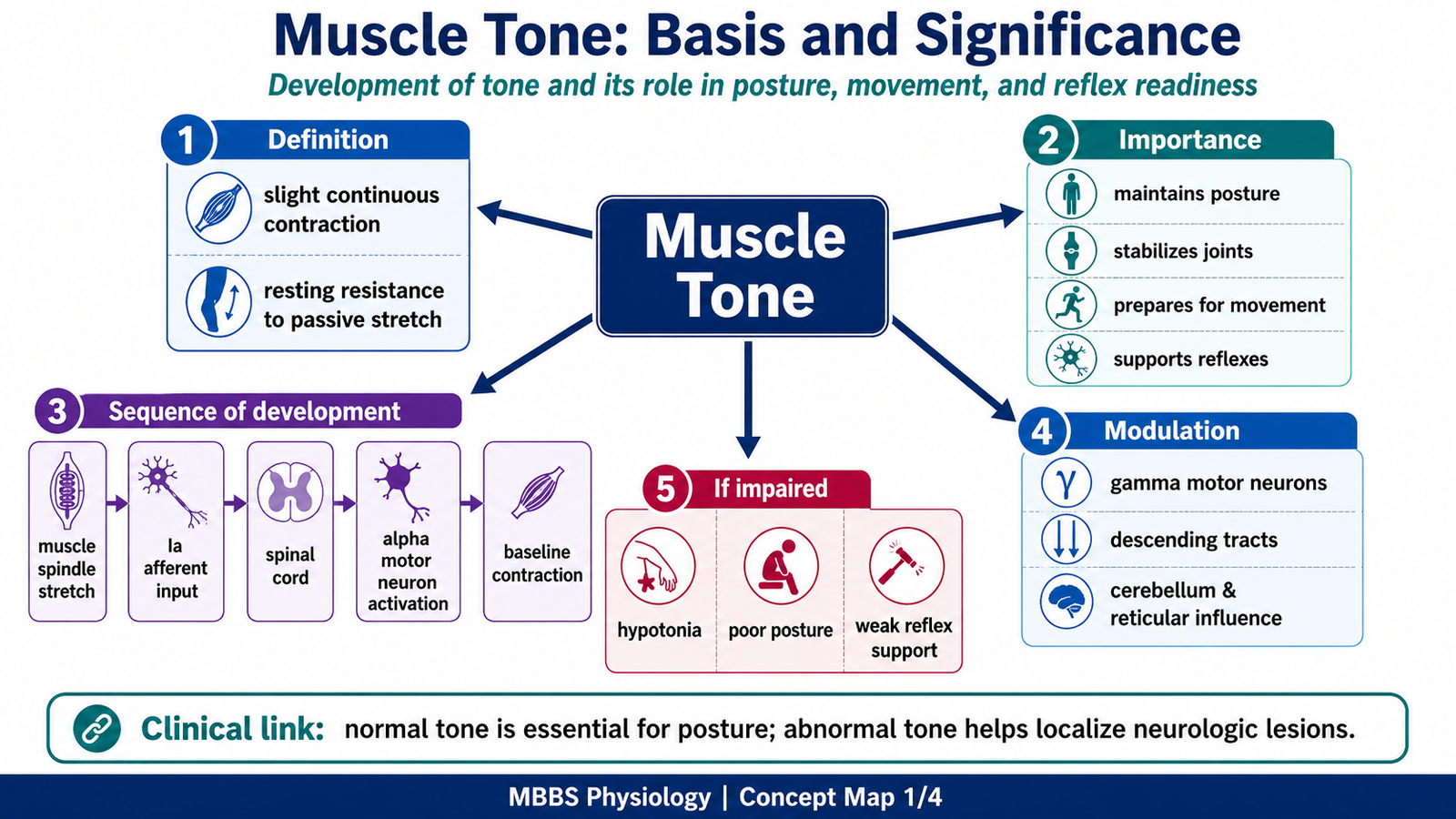
• Muscle tone is the slight continuous contraction present in resting skeletal muscle.
• It helps maintain posture and readiness for movement.
• Tone depends mainly on the stretch reflex mechanism.
• Muscle spindles, Ia afferents, alpha motor neurons, and gamma motor neurons are essential.
• Descending pathways regulate tone by controlling spinal reflex excitability.
• Normal tone prevents collapse under gravity.
• Abnormal tone is an important sign of neurological disease.
🔬 CONCEPT EXPLAINED
Muscle tone is the background activity of skeletal muscle when a person is at rest. It is not the same as voluntary contraction. It is mild, continuous, and involuntary. The body needs muscle tone because posture cannot be maintained by completely relaxed muscles. Even while standing quietly, antigravity muscles must remain partially active to prevent the body from collapsing.
The basic mechanism of tone is linked to the stretch reflex. When a muscle is slightly stretched by gravity or posture, muscle spindles detect this stretch. Sensory impulses travel through Ia afferent fibers to the spinal cord. These fibers excite alpha motor neurons, which send impulses back to the same muscle and produce slight contraction. This contraction resists excessive stretch and helps maintain posture.
Gamma motor neurons play an important role because they regulate the sensitivity of muscle spindles. If muscle spindles were not adjusted during movement, they would become slack and unable to detect stretch. Gamma motor activity keeps the spindle sensitive, allowing continuous feedback about muscle length.
Descending motor pathways regulate tone by adjusting the excitability of alpha and gamma motor neurons. Some pathways facilitate extensor tone, especially those involved in posture, while others prevent excessive tone. Normal muscle tone therefore represents a balance between spinal reflex activity and descending control from higher centers.
Tone has great clinical significance. Reduced tone suggests damage to the reflex arc, lower motor neuron, peripheral nerve, or acute spinal cord injury. Increased tone suggests loss of descending inhibitory control, especially in upper motor neuron lesions.
⚠️ CLINICAL IMPORTANCE
Abnormal tone guides diagnosis. Flaccidity is seen in LMN lesions and spinal shock. Spasticity is seen in chronic UMN lesions. Rigidity is more typical of extrapyramidal disorders such as Parkinsonism and should not be confused with spasticity.
MAJOR CONCEPT 3 — Sequence of Events During Development of Muscle Tone
🧠 CORE
• Muscle tone develops through sensory input, spinal reflex activity, and descending modulation.
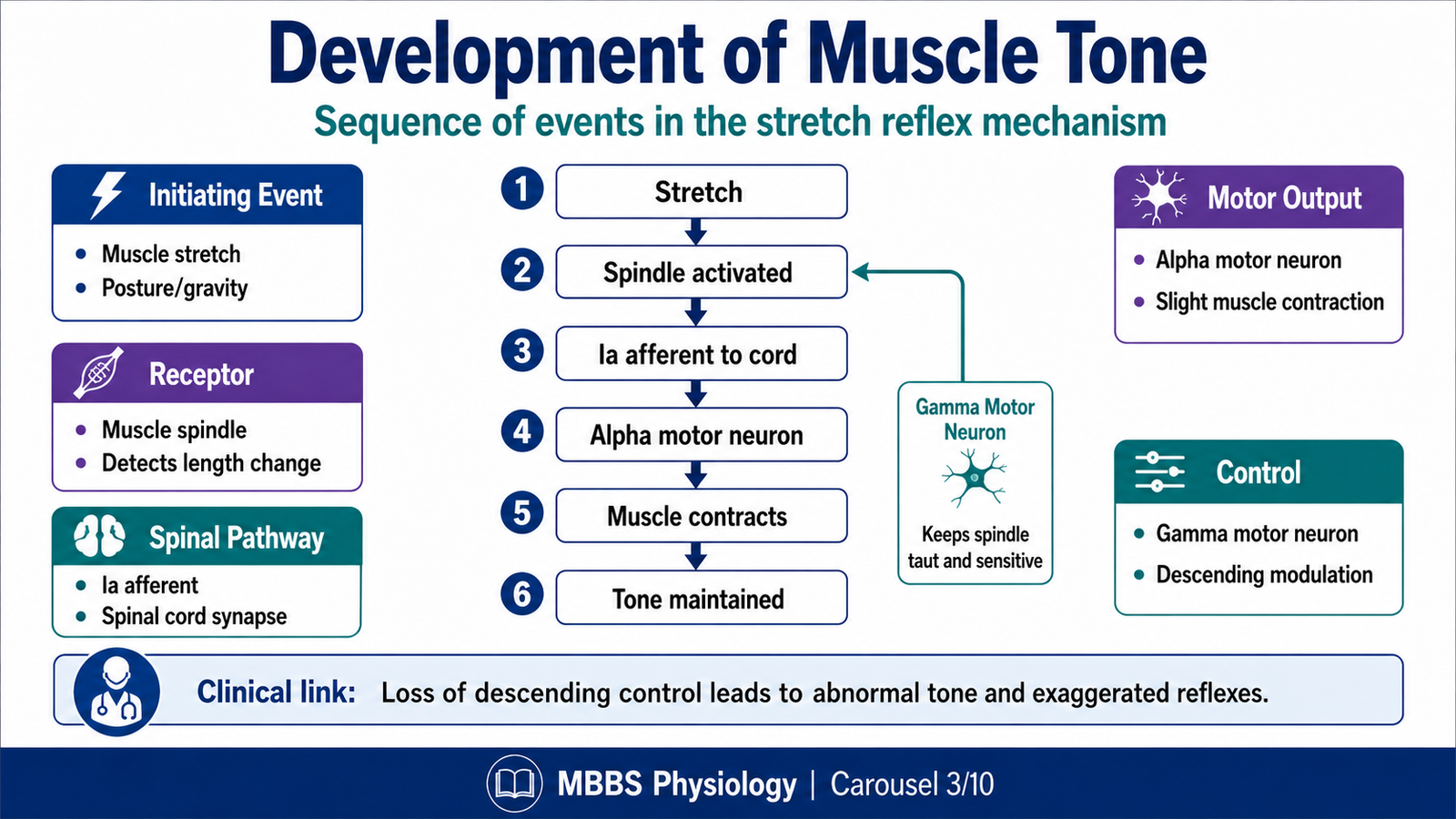
• Muscle spindle stretch is the initiating event.
• Ia afferents excite alpha motor neurons.
• Gamma motor neurons maintain spindle sensitivity.
• Descending pathways regulate the strength of reflex activity.
• Mature tone requires balanced excitation and inhibition.
• Loss of this balance produces flaccidity or spasticity.
🔬 CONCEPT EXPLAINED
The development of muscle tone begins when skeletal muscles are stretched slightly by body position, gravity, or movement. This stretch activates muscle spindles, which are specialized sensory receptors located within skeletal muscle. The purpose of these receptors is to inform the nervous system about changes in muscle length.
Once the spindle is stimulated, Ia afferent fibers carry impulses to the spinal cord. These fibers synapse mainly on alpha motor neurons supplying the same muscle. Activation of alpha motor neurons causes the muscle to contract slightly. This contraction opposes stretch and creates resting tone.
The next important component is gamma motor neuron activity. Gamma motor neurons do not contract the main force-producing extrafusal muscle fibers. Instead, they contract the ends of intrafusal fibers inside the muscle spindle. This keeps the spindle taut and sensitive. Therefore, gamma activity allows the stretch reflex to remain active during posture and movement.
As the nervous system matures, descending pathways from the brain modify this spinal reflex activity. They do not abolish tone; rather, they regulate it. They increase tone when postural support is needed and reduce excessive tone when smooth movement is required. This creates a controlled level of resting contraction.
Therefore, normal muscle tone is not produced by one structure alone. It is the outcome of stretch receptor activity, spinal reflex circuits, gamma motor neuron regulation, alpha motor neuron output, and descending control. When any part of this system fails, tone becomes abnormal.
⚠️ CLINICAL IMPORTANCE
In acute spinal cord injury, descending control is suddenly lost and spinal circuits become temporarily silent, causing flaccidity. Later, spinal reflexes recover without normal brain inhibition, producing increased tone and spasticity below the lesion.
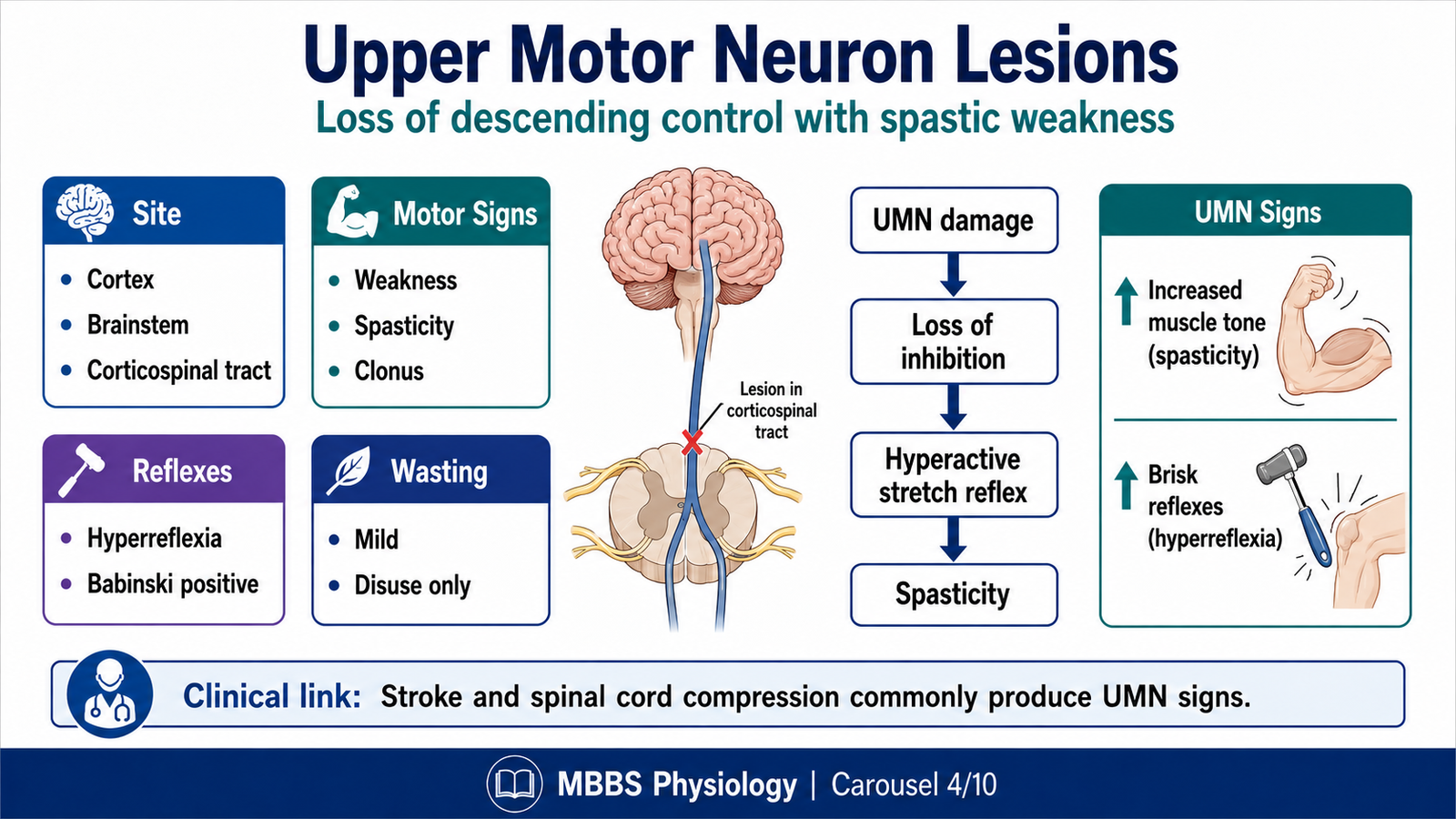
MAJOR CONCEPT 4 — Upper Motor Neuron Lesions
🧠 CORE
• UMN lesions involve motor pathways above the anterior horn cell.
• Common sites include cerebral cortex, internal capsule, brainstem, and corticospinal tract.
• Voluntary movement becomes weak, especially skilled movement.
• Muscle tone increases after the acute phase.
• Deep tendon reflexes become exaggerated.
• Babinski sign may be present.
• Muscle wasting is mild and due to disuse, not denervation.
🔬 CONCEPT EXPLAINED
An upper motor neuron lesion occurs when descending motor pathways are damaged before they reach the lower motor neuron. The lower motor neuron and muscle are still anatomically intact, but they lose normal control from higher centers.
The corticospinal tract is especially important for voluntary skilled movement. When it is damaged, the patient develops weakness or paralysis. The weakness is not due to destruction of muscle or peripheral nerve. It occurs because voluntary motor commands can no longer properly activate lower motor neurons.
Another major effect of UMN lesion is loss of descending inhibition over spinal reflex circuits. In normal physiology, the brain continuously regulates spinal reflex excitability. After UMN damage, this control is reduced. As a result, spinal reflexes become exaggerated. This causes hyperreflexia, clonus, and increased muscle tone.
Spasticity occurs because stretch reflexes become overactive. It is velocity-dependent, meaning that resistance to passive movement is greater when the limb is moved rapidly. This differs from rigidity, which is usually uniform throughout movement and is related to extrapyramidal disease.
The Babinski sign appears because the corticospinal tract normally suppresses primitive extensor plantar responses after infancy. When this suppression is lost, stroking the sole causes extension of the great toe and fanning of other toes.
⚠️ CLINICAL IMPORTANCE
UMN signs include weakness, spasticity, hyperreflexia, clonus, Babinski sign, and minimal wasting. In spinal cord lesions, UMN signs appear below the level of lesion after spinal shock resolves.
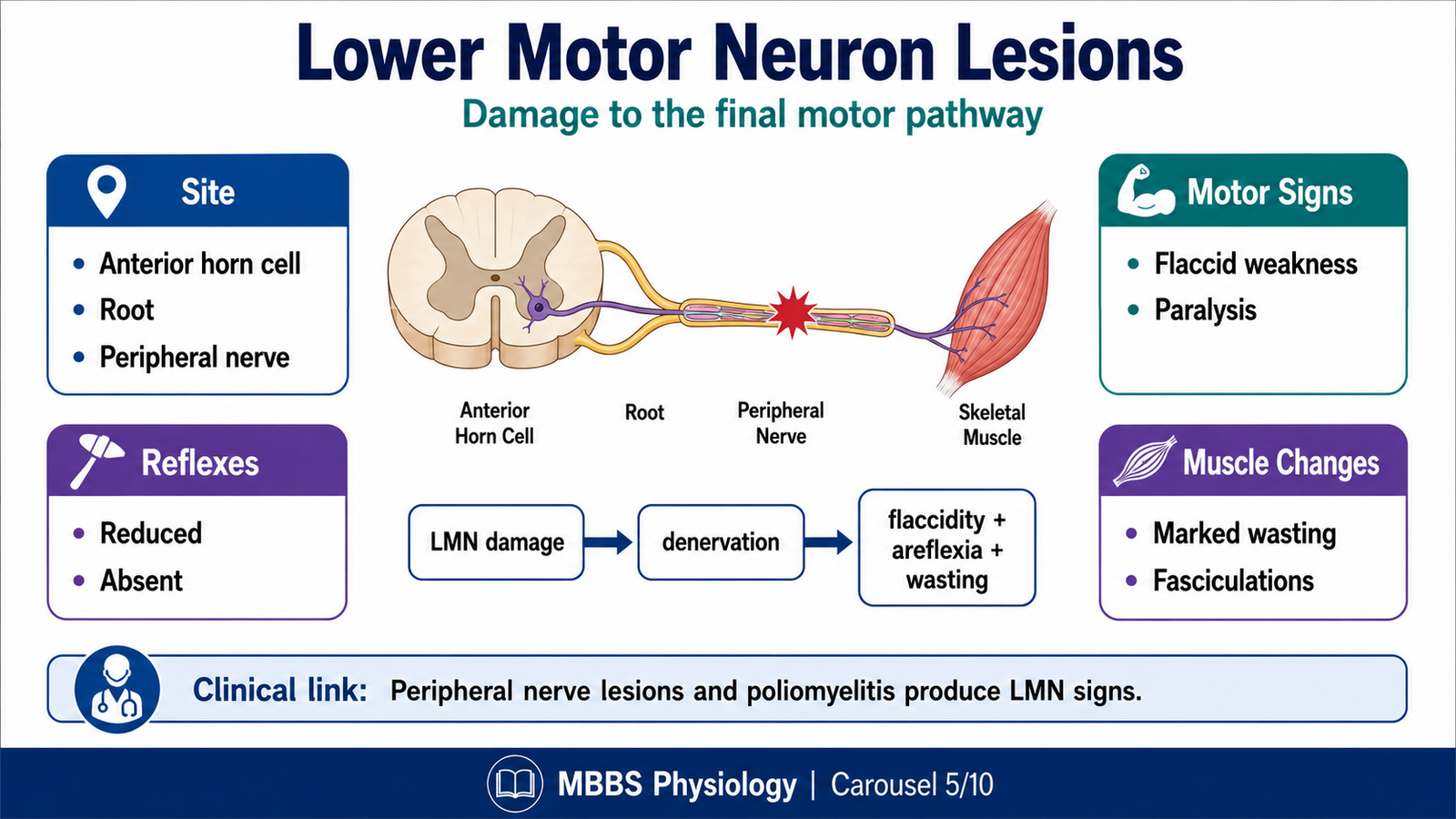
MAJOR CONCEPT 5 — Lower Motor Neuron Lesions
🧠 CORE
• LMN lesions involve anterior horn cells, nerve roots, peripheral nerves, neuromuscular junctions, or motor fibers.
• The muscle loses its direct motor supply.
• Weakness or paralysis occurs in muscles supplied by the damaged neuron.
• Muscle tone decreases.
• Reflexes are reduced or absent.
• Fasciculations may occur.
• Muscle wasting is marked due to denervation.
🔬 CONCEPT EXPLAINED
A lower motor neuron lesion damages the final pathway from spinal cord to skeletal muscle. Unlike an UMN lesion, where the muscle and peripheral nerve remain intact, an LMN lesion interrupts the actual motor supply to muscle.
When the lower motor neuron is damaged, impulses cannot reach the muscle effectively. As a result, the muscle becomes weak or paralyzed. Since the reflex arc also depends on the lower motor neuron, deep tendon reflexes are reduced or absent. This explains why LMN lesions produce hyporeflexia or areflexia.
Muscle tone decreases because resting tone requires an intact reflex arc. If the anterior horn cell, motor root, peripheral nerve, or neuromuscular transmission is damaged, the muscle cannot maintain background contraction. This produces flaccidity.
Marked muscle wasting occurs because skeletal muscle depends on neural input for trophic support. When denervation occurs, muscle fibers atrophy. Fasciculations may appear due to spontaneous discharge of damaged motor neurons, especially anterior horn cells.
Therefore, LMN lesions produce a pattern of weakness, flaccidity, reduced reflexes, wasting, and fasciculations. This pattern is clinically very different from the spastic weakness seen in UMN lesions.
⚠️ CLINICAL IMPORTANCE
LMN signs are seen in poliomyelitis, peripheral nerve injury, radiculopathy, motor neuron disease, and anterior horn cell disorders. In spinal cord lesions, LMN signs may occur at the exact level of lesion, while UMN signs occur below the lesion.
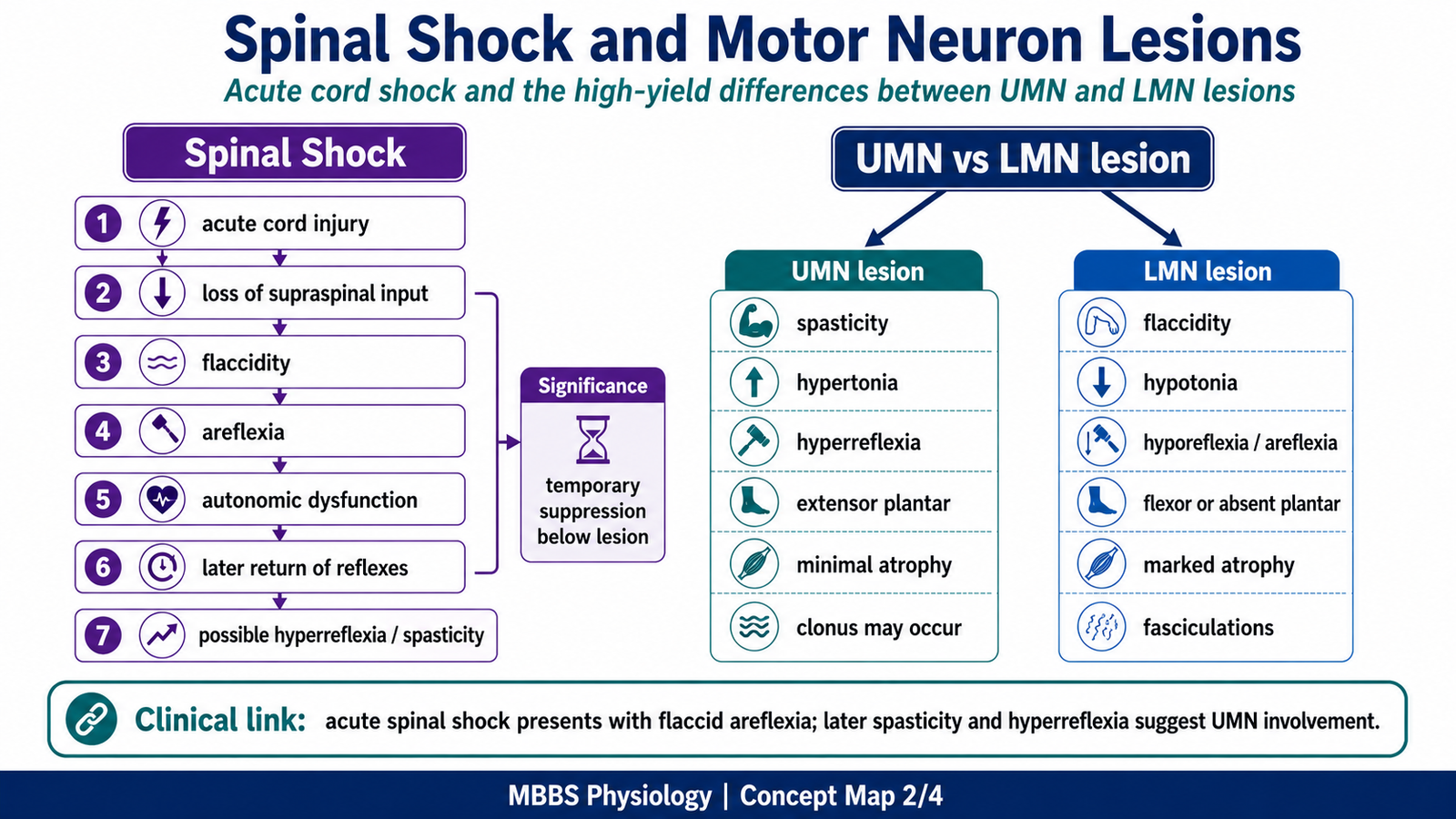
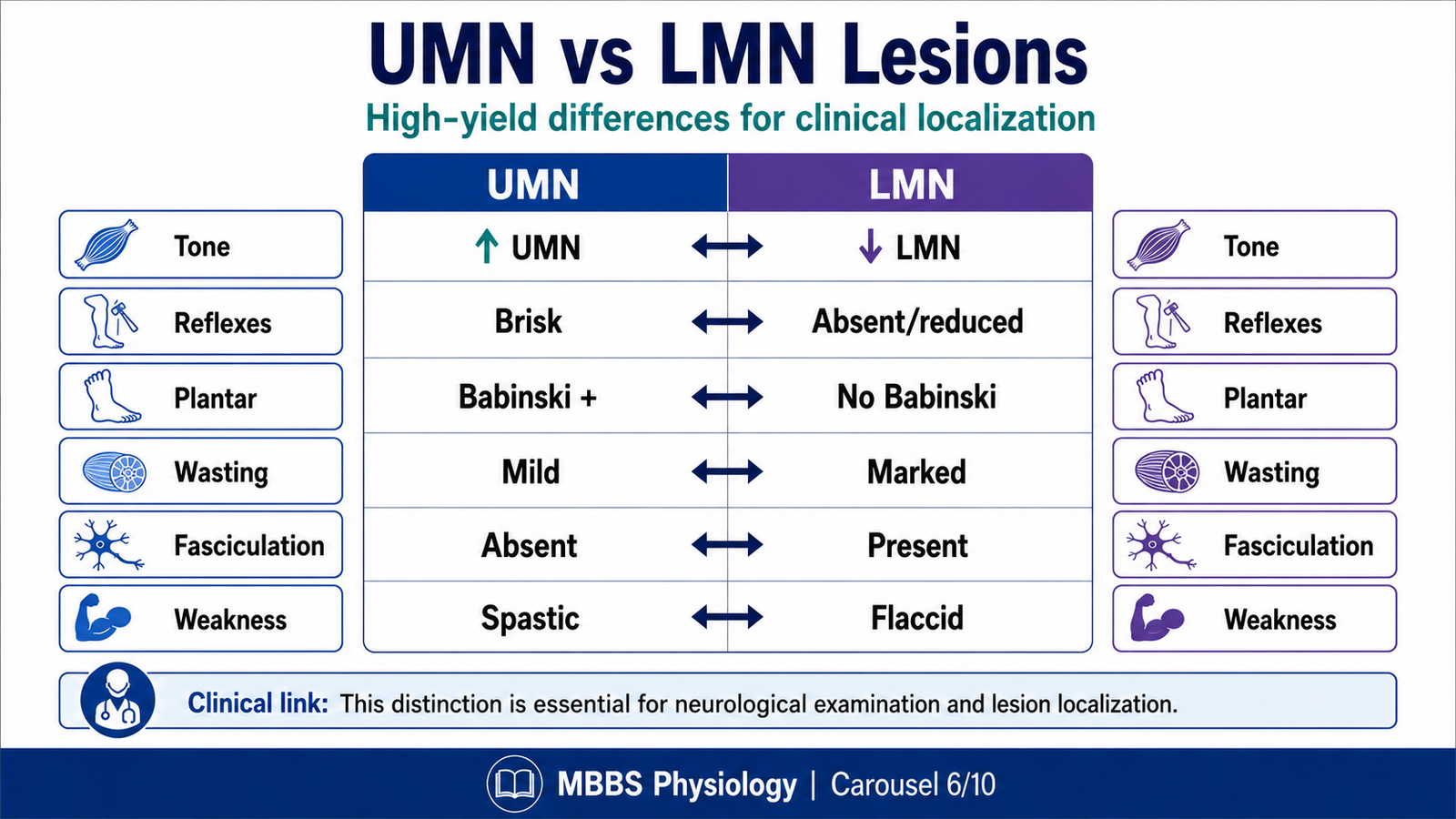
MAJOR CONCEPT 6 — Difference Between UMN and LMN Lesions
🧠 CORE
• UMN lesion affects descending control; LMN lesion affects final motor output.
• UMN lesion causes spastic weakness; LMN lesion causes flaccid weakness.
• UMN lesion causes hyperreflexia; LMN lesion causes hyporeflexia.
• UMN lesion produces Babinski sign; LMN lesion does not.
• UMN wasting is mild; LMN wasting is marked.
• Fasciculations are typical of LMN lesions.
• Lesion localization depends on combining motor, reflex, and sensory findings.
🔬 CONCEPT EXPLAINED
The difference between UMN and LMN lesions is based on the level of damage in the motor system. If the lesion is above the anterior horn cell, the lower motor neuron remains present but loses proper descending control. This produces the UMN pattern. If the lesion damages the anterior horn cell or peripheral motor pathway, the muscle loses its direct supply. This produces the LMN pattern.
In UMN lesions, weakness occurs because voluntary commands cannot descend normally. However, spinal reflex circuits remain intact and become overactive because inhibitory control is lost. Therefore, tone and reflexes increase.
In LMN lesions, weakness occurs because the final pathway to the muscle is interrupted. Since the reflex arc itself is damaged, tone and reflexes decrease. Muscle also wastes significantly because of denervation.
This difference is clinically powerful. For example, a patient with paraplegia due to spinal cord compression may initially show flaccid weakness due to spinal shock. Later, UMN signs appear below the lesion. However, at the level of cord damage, anterior horn cells or roots may be damaged, producing LMN signs in specific muscles.
⚠️ CLINICAL IMPORTANCE
High-Yield Comparison
| Feature | UMN Lesion | LMN Lesion |
|---|---|---|
| Site of lesion | Above anterior horn cell | Anterior horn cell, root, nerve, motor unit |
| Weakness | Present | Present |
| Tone | Increased after acute phase | Decreased |
| Reflexes | Increased | Decreased or absent |
| Plantar response | Extensor Babinski | Flexor or absent |
| Wasting | Mild disuse wasting | Marked denervation wasting |
| Fasciculations | Absent | Present |
| Clonus | May be present | Absent |
| Distribution | Often groups of muscles | Specific muscles supplied by damaged LMN |
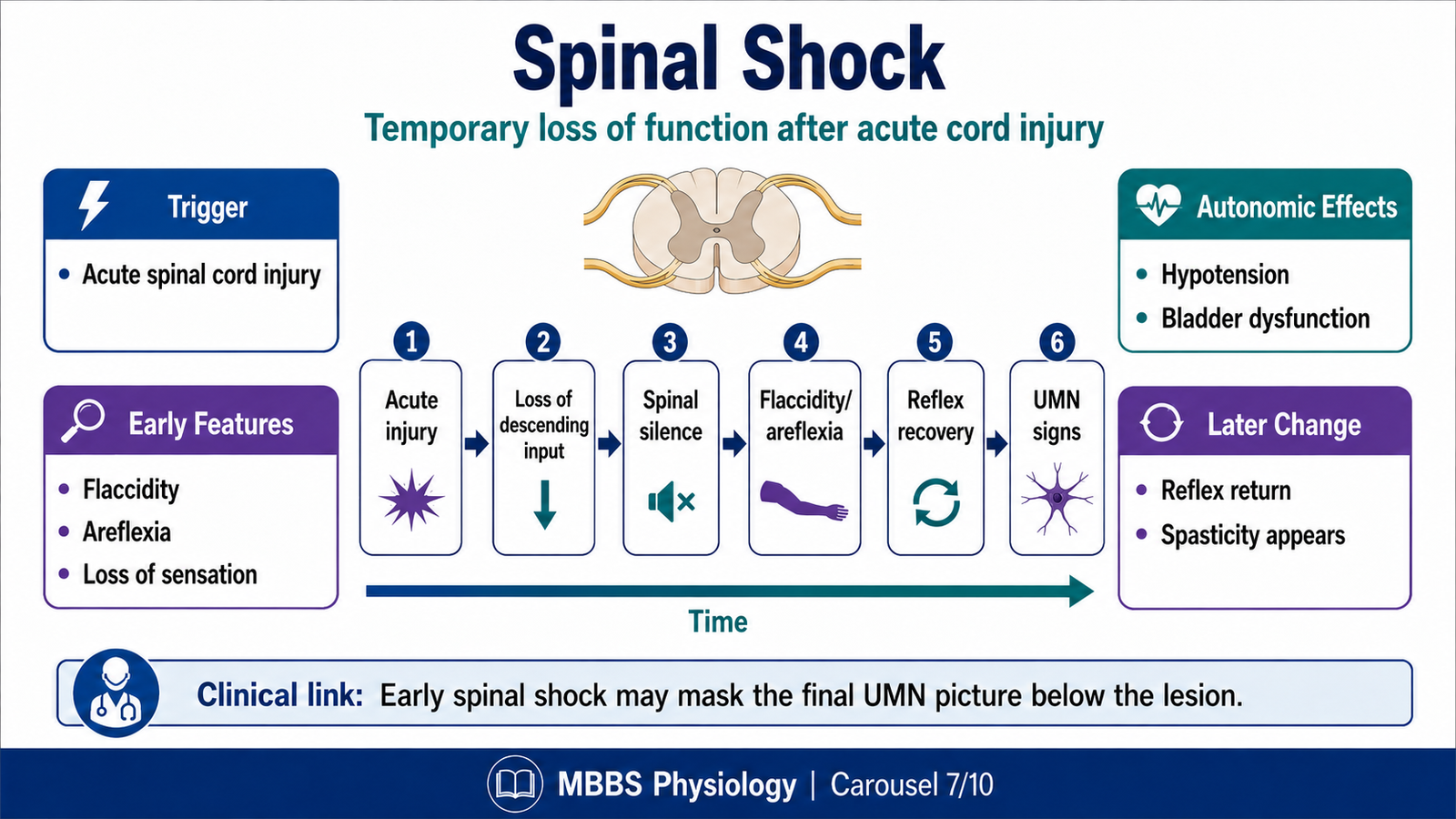
MAJOR CONCEPT 7 — Spinal Shock
🧠 CORE
• Spinal shock occurs after acute severe spinal cord injury.
• It causes temporary loss of motor, sensory, reflex, and autonomic function below the lesion.
• Muscles below the lesion become flaccid initially.
• Deep tendon reflexes are absent during the early phase.
• Autonomic dysfunction may cause hypotension and bladder involvement.
• Reflexes gradually return over days to weeks.
• Later, UMN signs usually develop below the lesion.
🔬 CONCEPT EXPLAINED
Spinal shock is a temporary physiological state that follows sudden severe injury to the spinal cord. It occurs because spinal neurons below the lesion suddenly lose descending excitatory and inhibitory influences from the brain. This sudden loss makes the spinal cord circuits temporarily inactive.
In the early phase, muscles below the lesion become flaccid. Reflexes disappear because spinal reflex circuits are not functioning properly. Sensation and voluntary movement below the lesion are also lost depending on the severity of cord injury. Autonomic functions may be disturbed, causing problems such as low blood pressure, loss of sweating, and bladder dysfunction.
The important point is that spinal shock is not the same as permanent cord destruction. It is a temporary loss of function of spinal cord segments below the lesion. Over time, spinal neurons regain excitability. Reflexes begin to return, often starting with simple reflexes. Later, because normal descending control is absent, reflexes may become exaggerated and spasticity develops.
This explains a common clinical sequence: immediately after spinal cord injury, the patient may show LMN-like flaccidity below the lesion. After spinal shock resolves, the same patient develops UMN signs below the lesion.
⚠️ CLINICAL IMPORTANCE
Spinal shock can mask the final neurological picture of spinal cord injury. Therefore, early flaccidity after trauma does not necessarily mean LMN lesion. Repeated neurological examination is required as reflexes recover.
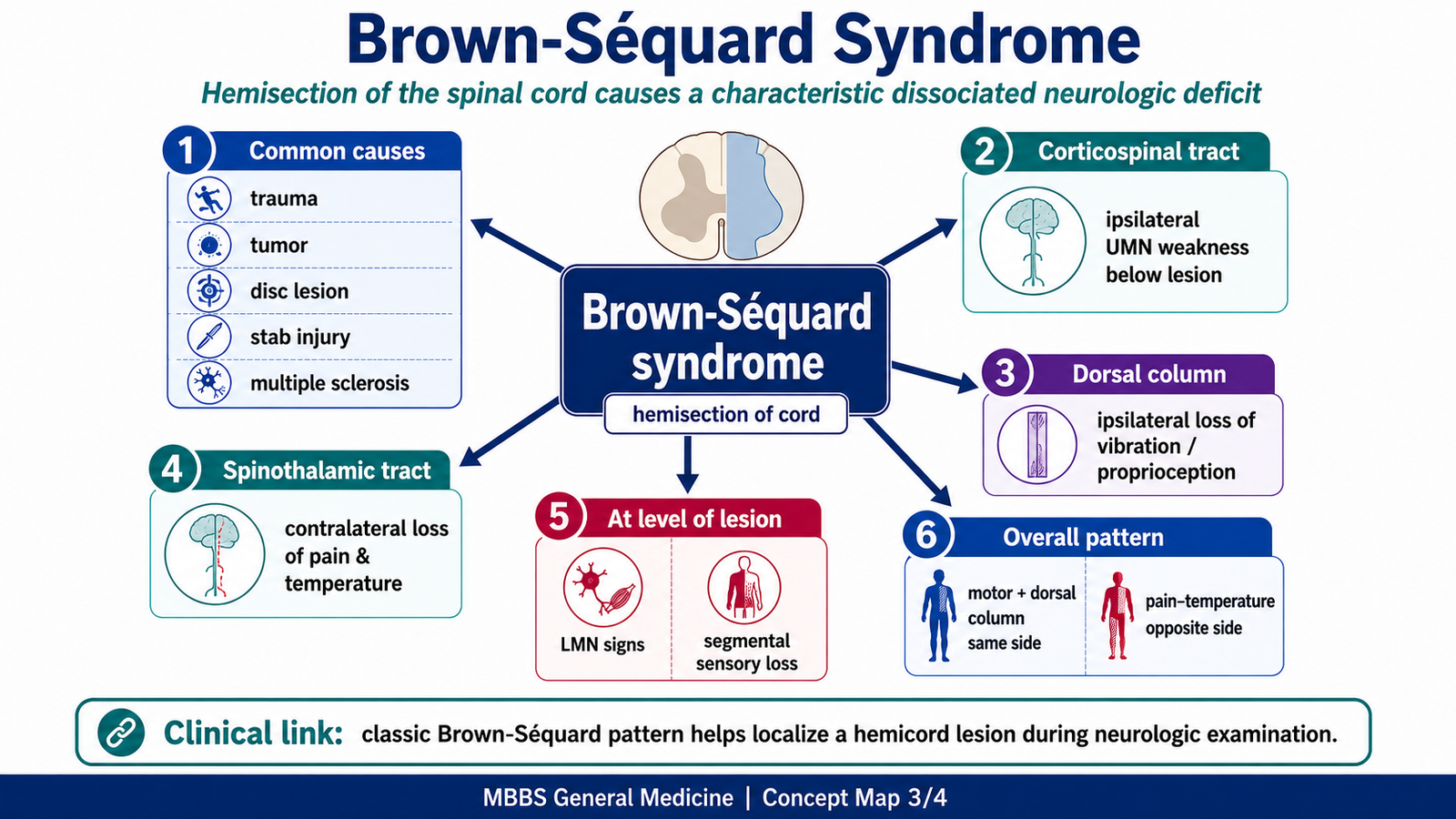
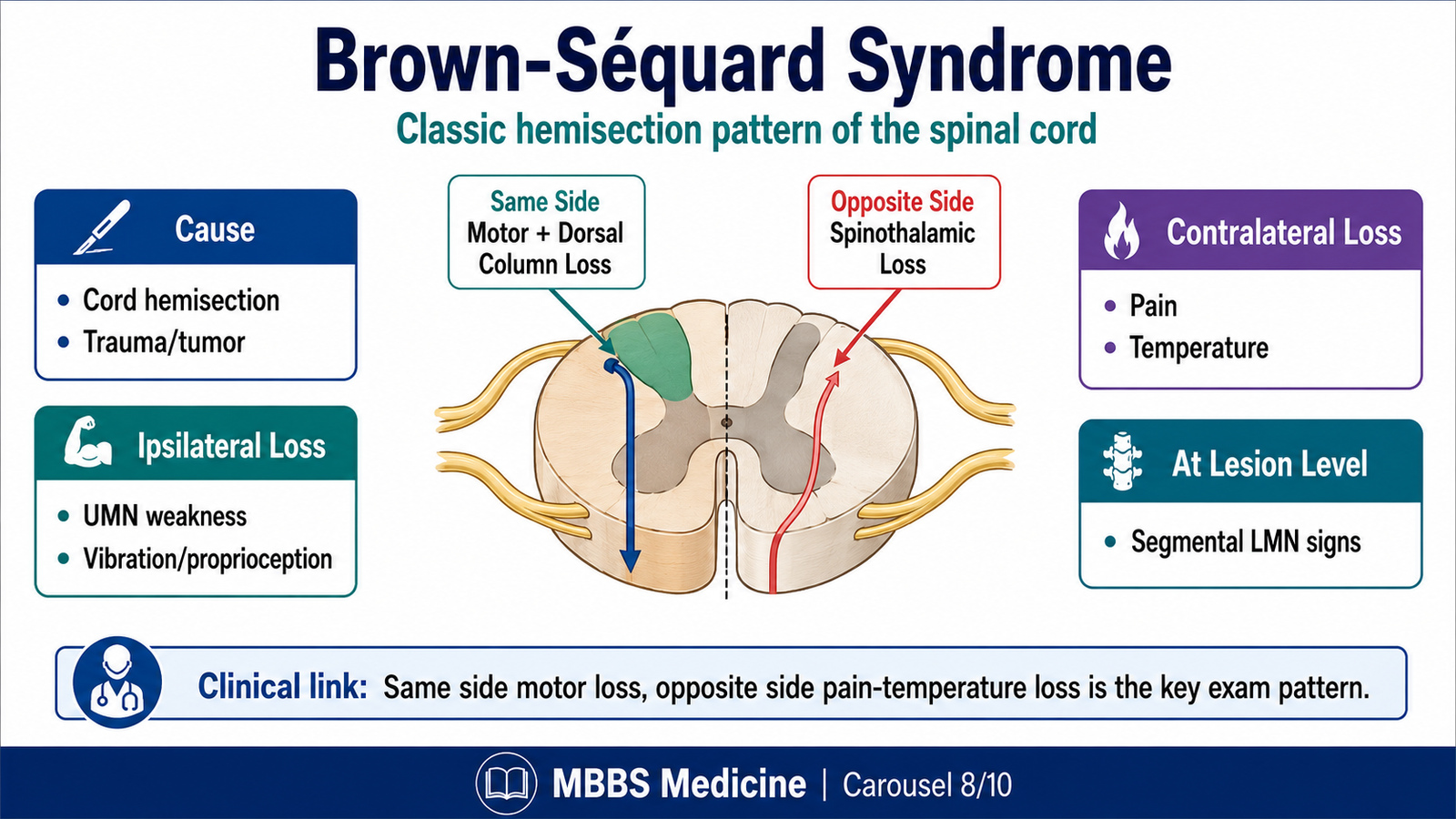
MAJOR CONCEPT 8 — Brown-Séquard Syndrome
🧠 CORE
• Brown-Séquard syndrome results from hemisection of the spinal cord.
• It causes ipsilateral UMN weakness below the lesion.
• It causes ipsilateral loss of proprioception, vibration, and fine touch below the lesion.
• It causes contralateral loss of pain and temperature below the lesion.
• LMN signs may occur at the level of lesion.
• Segmental sensory loss may occur at the lesion level.
• It is commonly due to penetrating trauma, tumors, disc disease, or demyelination.
🔬 CONCEPT EXPLAINED
Brown-Séquard syndrome is a classic example of how spinal tract anatomy explains clinical signs. It occurs when one half of the spinal cord is damaged. Because different sensory and motor pathways cross at different levels, the pattern of loss is highly characteristic.
The corticospinal tract has already crossed in the medulla before entering the spinal cord. Therefore, damage to the right corticospinal tract in the spinal cord produces right-sided UMN weakness below the lesion. This weakness later becomes spastic with hyperreflexia.
The dorsal column pathway carries proprioception, vibration, and fine touch. These fibers ascend on the same side of the spinal cord and cross later in the medulla. Therefore, hemisection of the spinal cord causes ipsilateral loss of proprioception, vibration, and fine touch below the lesion.
Pain and temperature fibers behave differently. They enter the spinal cord, synapse, and then cross to the opposite side within one or two spinal segments through the anterior white commissure. They then ascend in the spinothalamic tract. Therefore, damage to one side of the cord causes contralateral loss of pain and temperature below the lesion, usually beginning slightly below the level of injury.
At the exact level of lesion, anterior horn cells or nerve roots may be damaged. This can produce LMN signs in muscles supplied by that segment. Segmental sensory loss may also occur at the level of damage.
⚠️ CLINICAL IMPORTANCE
Brown-Séquard syndrome is an exam-favorite because it tests tract anatomy and clinical localization. The key rule is:
Same side: motor weakness and dorsal column loss.
Opposite side: pain and temperature loss.
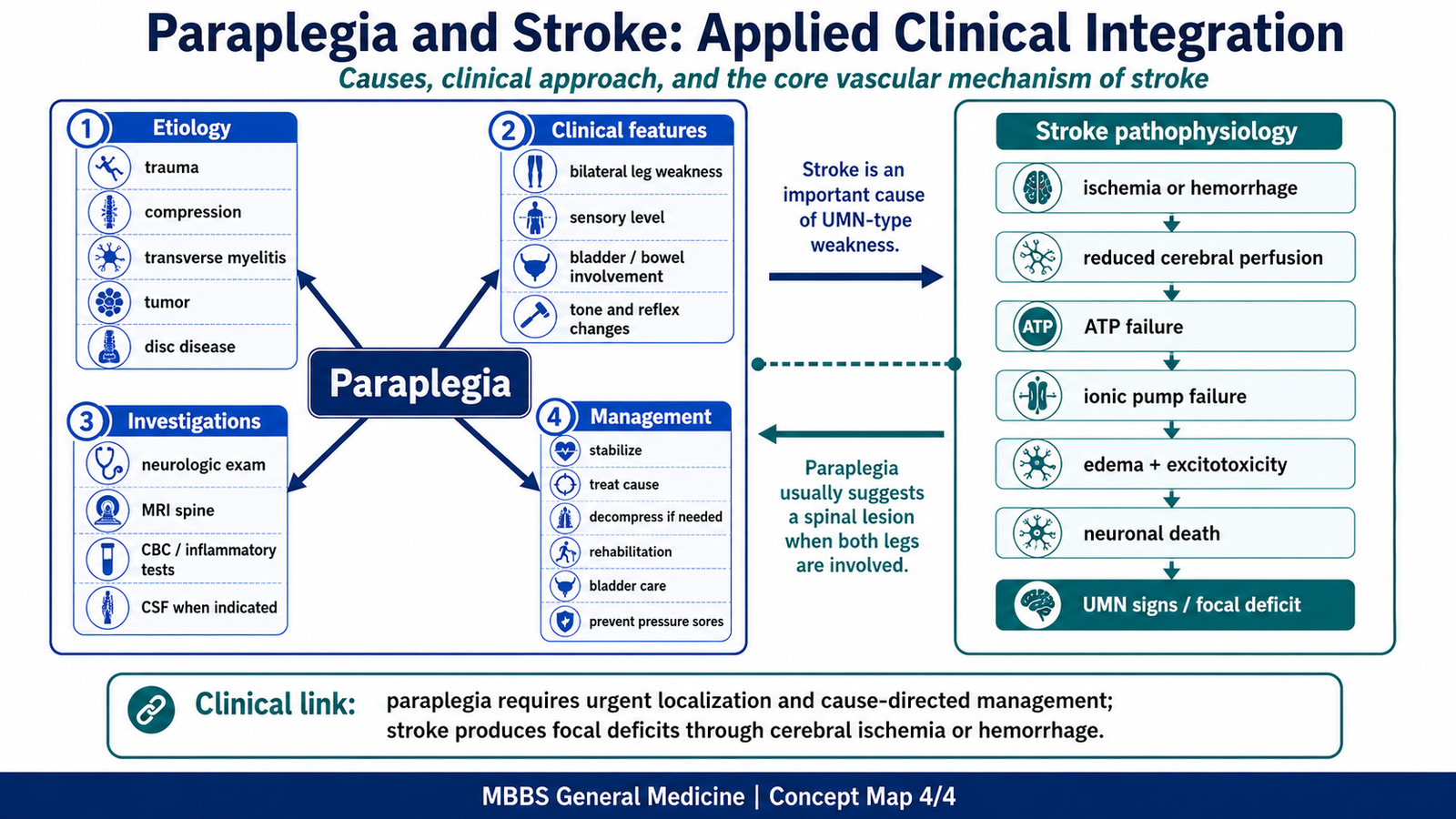
MAJOR CONCEPT 9 — Paraplegia
🧠 CORE
• Paraplegia means weakness or paralysis of both lower limbs.
• It commonly results from spinal cord disease below the cervical enlargement.
• Causes include trauma, compression, infection, inflammation, vascular lesions, congenital disorders, and degenerative disease.
• Clinical features include weakness, sensory loss, reflex changes, bladder and bowel dysfunction.
• Examination should identify UMN or LMN pattern and sensory level.
• Investigations aim to localize cause and level of lesion.
• Management depends on cause, severity, and urgency.
🔬 CONCEPT EXPLAINED
Paraplegia occurs when motor control of both lower limbs is impaired. The lesion may be in the spinal cord, brain, peripheral nerves, or muscles, but in clinical neurology, paraplegia commonly suggests spinal cord involvement. The level and nature of lesion determine the clinical picture.
If the spinal cord is compressed or damaged above the lumbar enlargement, lower limbs develop UMN signs after the acute phase. These include spasticity, hyperreflexia, extensor plantar response, and weakness. If the lesion affects the conus medullaris, cauda equina, anterior horn cells, or peripheral nerves, LMN signs may dominate, including flaccidity, reduced reflexes, and wasting.
Sensory findings are very important. A clear sensory level on the trunk strongly suggests spinal cord disease. Bladder and bowel involvement also support spinal cord or cauda equina pathology. Pain may suggest compression, infection, trauma, or malignancy.
Etiology is broad. Trauma can fracture or dislocate vertebrae and injure the cord. Tumors, abscesses, disc prolapse, or tuberculosis of spine may compress the cord. Inflammatory conditions such as transverse myelitis can damage cord tissue. Vascular lesions may cause spinal cord infarction. Congenital or degenerative conditions may also produce progressive weakness.
Investigation begins with careful neurological examination. MRI spine is the most important imaging test for suspected spinal cord compression because it shows cord, vertebrae, discs, tumors, abscesses, and inflammation. X-ray or CT may be useful in trauma or bony disease. Blood tests may detect infection, inflammation, metabolic causes, or malignancy. CSF examination may be needed in inflammatory or infective causes when safe.
Management depends on the cause. Acute cord compression is a neurological emergency because prolonged compression may cause irreversible damage. Treatment may include immobilization in trauma, urgent decompression, corticosteroids in selected inflammatory or compressive conditions, antibiotics for infection, antituberculous therapy for spinal tuberculosis, anticoagulation or vascular care in vascular causes, and rehabilitation. Supportive care includes bladder care, prevention of pressure sores, physiotherapy, prevention of contractures, and psychological support.
⚠️ CLINICAL IMPORTANCE
In paraplegia, the key clinical task is localization. Students should ask: Is it UMN or LMN? Is there a sensory level? Is bladder involved? Is onset acute or gradual? Is there pain or fever? These questions guide diagnosis and urgency.
MAJOR CONCEPT 10 — Pathophysiology of Stroke
🧠 CORE
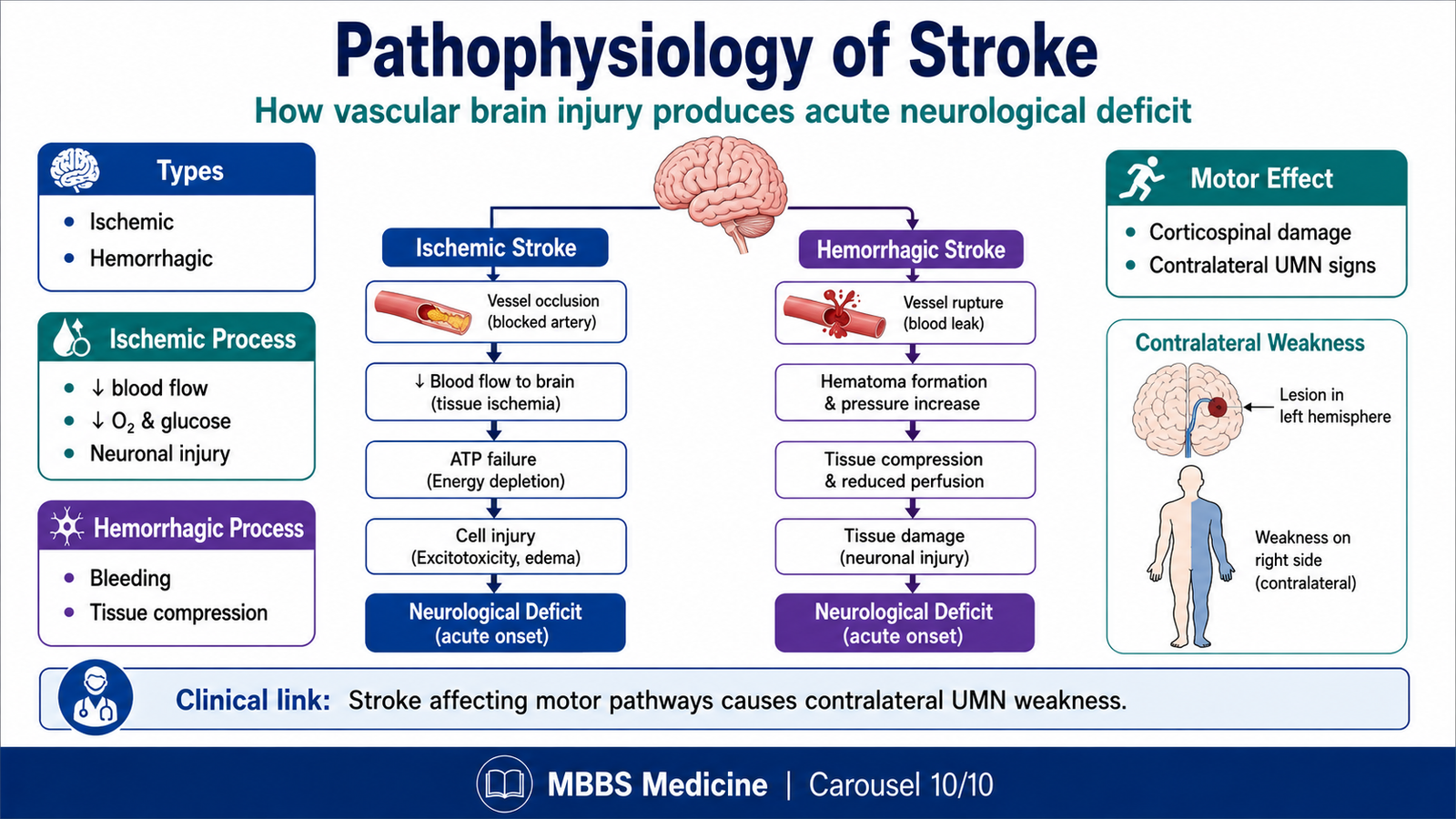
• Stroke is an acute neurological deficit due to vascular injury to the brain.
• It may be ischemic or hemorrhagic.
• Ischemic stroke results from blockage of cerebral blood flow.
• Hemorrhagic stroke results from bleeding into brain tissue or surrounding spaces.
• Neurons are highly sensitive to oxygen and glucose deprivation.
• Stroke may cause UMN signs because descending motor pathways are damaged.
• Clinical features depend on the vascular territory involved.
🔬 CONCEPT EXPLAINED
Although this topic focuses mainly on spinal cord lesions, stroke is included because it is a major cause of upper motor neuron signs. Stroke occurs when blood supply to a part of the brain is suddenly interrupted or when a blood vessel ruptures. Brain tissue requires continuous oxygen and glucose delivery because neurons have high metabolic demand and limited energy storage.
In ischemic stroke, a cerebral artery becomes blocked by thrombosis or embolism. Reduced blood flow decreases oxygen and glucose delivery. As ATP production falls, ion pumps fail. Sodium and water enter neurons, causing cellular swelling. Calcium enters cells and activates damaging enzymes. Excitatory neurotransmitters such as glutamate increase, causing excitotoxic injury. If blood flow is not restored, neurons die.
In hemorrhagic stroke, bleeding damages brain tissue directly and increases pressure within the skull. The expanding hematoma compresses surrounding tissue and may reduce blood flow to nearby areas. This causes neurological deficit both by tissue destruction and pressure effects.
When stroke involves the motor cortex, internal capsule, or corticospinal pathway, the patient develops UMN signs on the opposite side of the body. This occurs because corticospinal fibers cross in the medulla. A lesion in the left cerebral hemisphere therefore commonly causes right-sided weakness.
⚠️ CLINICAL IMPORTANCE
Stroke is important in this topic because it produces UMN signs above the spinal cord. Unlike spinal cord lesions, stroke often affects face and upper limb along with lower limb and may be associated with speech, vision, or cortical deficits depending on the area involved.
⚙️ 4️⃣ Functional Flow
Spinal cord lesions are best understood through the relationship:
Structure → Function → Outcome
The corticospinal tract is a descending motor pathway. Its structure allows the brain to control voluntary movement. When it is damaged, voluntary movement becomes weak and UMN signs appear.
The anterior horn cell is the lower motor neuron. Its function is to directly activate skeletal muscle. When it is damaged, the muscle loses motor supply, producing flaccid weakness, wasting, and reduced reflexes.
The muscle spindle is a stretch receptor. Its function is to detect muscle length and maintain tone through reflex activity. When spindle input or reflex arcs fail, tone decreases. When descending inhibition fails, reflex tone becomes excessive.
The dorsal column carries proprioception, vibration, and fine touch on the same side of the spinal cord. When it is damaged in Brown-Séquard syndrome, ipsilateral loss of these sensations occurs.
The spinothalamic tract carries pain and temperature after crossing in the spinal cord. When one side of the cord is damaged, pain and temperature are lost on the opposite side below the lesion.
The spinal cord also contains autonomic pathways. When these are damaged, bladder, bowel, blood pressure, and sexual function may be affected. This is why paraplegia is not only a motor disorder but a whole neurological syndrome.
Thus, spinal cord disease affects movement, tone, reflexes, sensation, posture, and autonomic function because all these systems are anatomically and physiologically integrated within the cord.
🩺 5️⃣ Clinical Correlation
1. Upper Motor Neuron Lesion
UMN lesions occur in stroke, spinal cord compression, multiple sclerosis, and traumatic cord injury. The patient develops weakness with increased tone, exaggerated reflexes, clonus, and Babinski sign. The mechanism is loss of descending control over spinal reflex circuits.
2. Lower Motor Neuron Lesion
LMN lesions occur in peripheral nerve injury, poliomyelitis, radiculopathy, anterior horn cell disease, and cauda equina lesions. The patient develops flaccid weakness, reduced reflexes, marked wasting, and fasciculations because the final motor pathway is damaged.
3. Spinal Shock
After acute spinal cord injury, the patient initially shows flaccidity and absent reflexes below the lesion. This can mimic LMN disease, but it is temporary. Later, reflexes return and UMN signs appear below the lesion.
4. Brown-Séquard Syndrome
A patient with hemisection of the cord shows ipsilateral UMN weakness and dorsal column sensory loss with contralateral pain and temperature loss. It is commonly caused by penetrating trauma, tumors, disc prolapse, or demyelinating disease.
5. Paraplegia
Paraplegia may result from trauma, spinal cord compression, transverse myelitis, spinal tuberculosis, tumors, vascular lesions, or degenerative disease. Important clinical features include bilateral lower limb weakness, sensory level, bladder and bowel dysfunction, altered reflexes, and tone changes. MRI spine is the key investigation when spinal cord disease is suspected.
6. Stroke
Stroke can produce UMN signs when it affects the motor cortex, internal capsule, or corticospinal tract. Unlike spinal cord lesions, stroke may also cause facial weakness, aphasia, visual field defects, or cortical signs depending on the involved brain region.
📌 6️⃣ Summary Points
- Muscle tone is maintained mainly by the stretch reflex and regulated by descending pathways.
- Normal tone requires muscle spindles, Ia afferents, alpha motor neurons, gamma motor neurons, and intact spinal circuits.
- UMN lesions cause weakness with spasticity, hyperreflexia, clonus, and Babinski sign.
- LMN lesions cause weakness with flaccidity, hyporeflexia, wasting, and fasciculations.
- Spinal shock initially causes flaccidity and absent reflexes below acute cord injury.
- After spinal shock resolves, UMN signs usually appear below the level of spinal cord lesion.
- Brown-Séquard syndrome causes ipsilateral motor and dorsal column loss with contralateral pain and temperature loss.
- A sensory level strongly suggests spinal cord involvement.
- Paraplegia is not only motor weakness; bladder, bowel, sensory, reflex, and tone changes must also be assessed.
- MRI spine is the most important investigation for suspected spinal cord compression.
- Stroke produces UMN signs when motor cortex, internal capsule, or corticospinal pathways are involved.
- At the level of a spinal cord lesion, LMN signs may occur; below the lesion, UMN signs may appear after spinal shock resolves.