
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Parkinsonism is an important integrated topic because it connects biochemistry of membrane lipids, dopamine metabolism, basal ganglia function, drug mechanisms, and clinical tremor recognition.
The key disease process occurs mainly in the substantia nigra pars compacta, a midbrain structure whose dopaminergic neurons regulate movement through the basal ganglia.
Biochemically, this topic is important because neuronal membranes and myelin are rich in sphingolipids, especially sphingomyelin, which are essential for nerve stability, myelin integrity, and signal conduction.
In Parkinson’s disease, degeneration of dopaminergic neurons produces motor features such as resting tremor, rigidity, bradykinesia, and postural instability.
Pharmacology becomes clinically relevant because treatment aims to restore the functional balance between dopamine and acetylcholine in basal ganglia circuits.
Tremor is a high-yield clinical sign because cerebellar tremor and parkinsonian tremor indicate dysfunction in different motor control systems.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Parkinsonism: A clinical syndrome characterized mainly by bradykinesia, rigidity, tremor, and postural instability.
- Parkinson’s disease: A neurodegenerative disorder caused primarily by loss of dopaminergic neurons in the substantia nigra pars compacta.
- Substantia nigra: A pigmented midbrain nucleus involved in motor control through dopamine release to the striatum.
- Dopamine: A catecholamine neurotransmitter that facilitates normal movement through basal ganglia circuits.
- Sphingolipids: Complex lipids containing sphingosine as their backbone; important in neuronal membranes and myelin.
- Phosphosphingolipid / Sphingophospholipid: A sphingolipid containing phosphate; the major example is sphingomyelin.
- Sphingomyelin: A membrane lipid composed of sphingosine, fatty acid, phosphate, and choline; abundant in myelin sheaths.
- Resting tremor: Tremor present at rest and reduced during voluntary movement; typical of Parkinson’s disease.
- Intention tremor: Tremor that appears or worsens during purposeful movement; typical of cerebellar dysfunction.
Essential Terminology
- Striatum: Caudate nucleus + putamen; receives dopaminergic input from substantia nigra.
- Nigrostriatal pathway: Dopaminergic pathway from substantia nigra to striatum.
- Lewy bodies: Intracytoplasmic inclusions containing abnormal protein aggregates, classically associated with Parkinson’s disease.
- Bradykinesia: Slowness of movement.
- Rigidity: Increased resistance to passive movement.
- Akinesia: Difficulty initiating movement.
- Dyskinesia: Abnormal involuntary movements, often seen with long-term levodopa therapy.
🔹 3️⃣ Core Learning — Curriculum Coverage
1: Biochemistry of Phosphosphingolipids
🧠 CORE
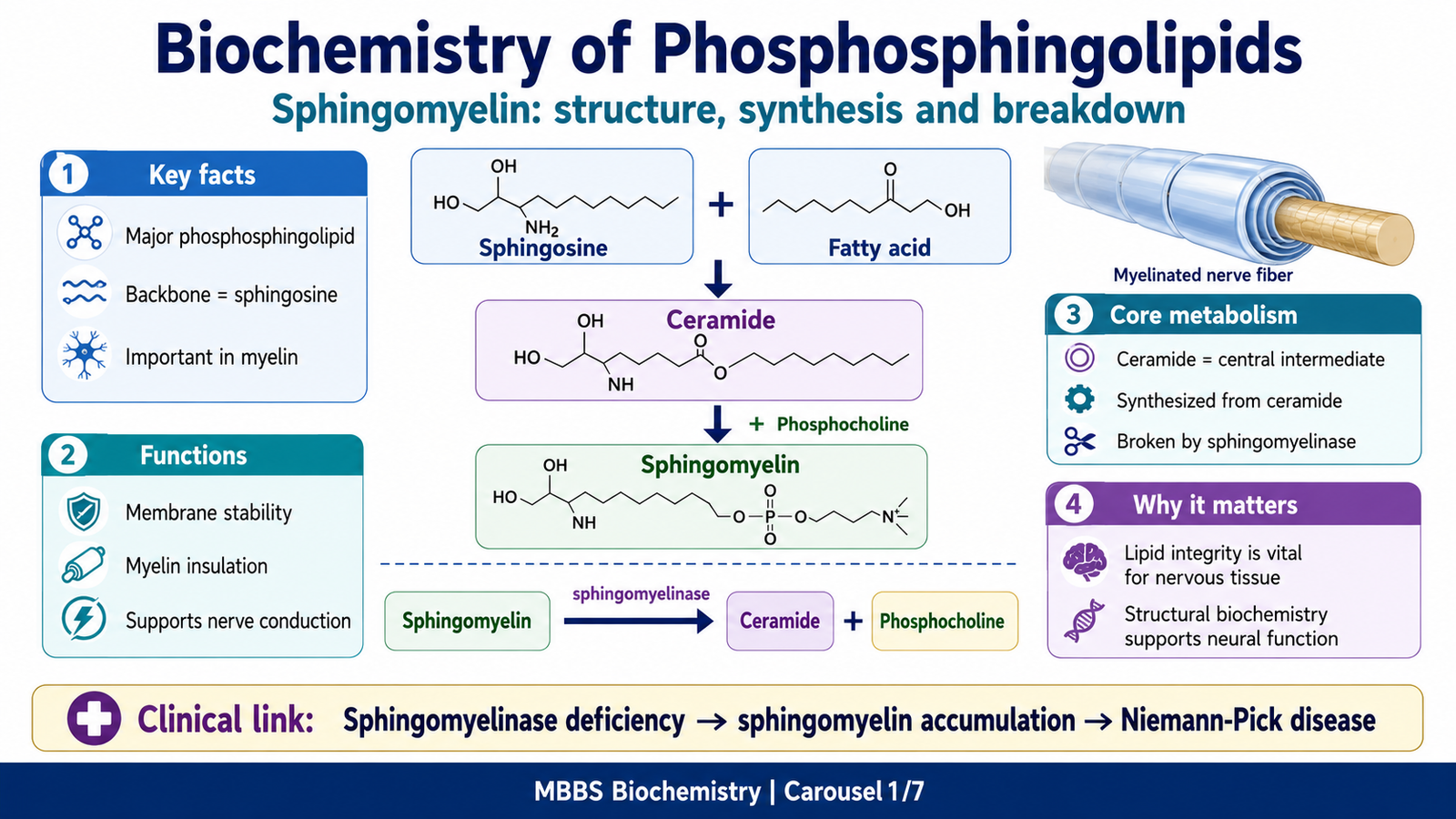
- Phosphosphingolipids are sphingolipids that contain phosphate.
- The most important phosphosphingolipid is sphingomyelin.
- Sphingomyelin is abundant in cell membranes, especially myelin sheath of nerve fibers.
- It contains sphingosine, a fatty acid, phosphate, and choline.
- It helps maintain membrane stability and insulation of nerve fibers.
- Its metabolism occurs mainly through synthesis in membranes and breakdown by sphingomyelinase.
- Defective breakdown causes sphingomyelin accumulation, classically in Niemann-Pick disease.
🔬 CONCEPT EXPLAINED
To understand phosphosphingolipids, students must first understand that neuronal function depends not only on neurotransmitters but also on the structural integrity of neuronal membranes and myelin. Neurons require stable membranes for impulse generation, synaptic transmission, axonal conduction, and protection of long nerve fibers. Sphingolipids are therefore especially important in nervous tissue.
Phosphosphingolipids are a subgroup of sphingolipids in which a phosphate-containing group is attached to the sphingosine backbone. The main biologically important phosphosphingolipid is sphingomyelin. Unlike glycerophospholipids, sphingomyelin does not contain glycerol. Instead, it contains sphingosine as its backbone. A fatty acid attaches to sphingosine to form ceramide, and then a phosphate-choline group attaches to ceramide to form sphingomyelin.
This structure gives sphingomyelin both hydrophobic and hydrophilic properties. The fatty acid and sphingosine portion form the hydrophobic region, while phosphate and choline form the polar head. As a result, sphingomyelin becomes suitable for incorporation into lipid bilayers.
The body needs sphingomyelin because it contributes to the structure of cell membranes and is especially abundant in myelin sheaths. Myelin acts like insulation around axons and allows rapid saltatory conduction of nerve impulses. Therefore, sphingomyelin is indirectly important for normal motor control, reflexes, sensation, and coordination.
Synthesis of Sphingomyelin
Sphingomyelin synthesis begins with the formation of ceramide. Ceramide is produced from sphingosine and a fatty acid. Then, phosphocholine is transferred from phosphatidylcholine to ceramide, forming sphingomyelin. This mainly occurs in cellular membranes, especially in the Golgi apparatus and plasma membrane system.
The important concept is that ceramide is the central intermediate in sphingolipid metabolism. From ceramide, the body can make sphingomyelin or other complex sphingolipids. Therefore, ceramide acts as a biochemical branch point.
Breakdown of Sphingomyelin
Sphingomyelin is degraded by the enzyme sphingomyelinase. This enzyme hydrolyzes sphingomyelin into ceramide and phosphocholine. Ceramide can then be further broken down into sphingosine and fatty acid.
If sphingomyelinase is deficient, sphingomyelin cannot be degraded properly. As a result, sphingomyelin accumulates inside lysosomes, particularly in organs rich in reticuloendothelial cells and nervous tissue. This produces Niemann-Pick disease, a lysosomal storage disorder.
Why This Matters in a Parkinsonism Topic
Although Parkinson’s disease itself is primarily a disorder of dopaminergic neuronal degeneration, the biochemical foundation of nervous tissue depends heavily on lipid-rich membranes and myelin. Phosphosphingolipids such as sphingomyelin help maintain neuronal structure and conduction. Therefore, understanding sphingolipid metabolism prepares students to understand how biochemical defects in nervous tissue can produce neurological disease.
In Parkinson’s disease, the key biochemical disturbance is not sphingomyelinase deficiency, but the functional loss of dopamine-producing neurons. Still, both sphingolipid disorders and Parkinson’s disease show an important common principle: neuronal structure and neuronal chemistry are both essential for normal nervous system function.
⚠️ CLINICAL IMPORTANCE
- Sphingomyelin is important for myelin integrity and neuronal membrane stability.
- Sphingomyelinase deficiency causes sphingomyelin accumulation.
- Accumulation of sphingomyelin causes Niemann-Pick disease, which may involve neurodegeneration.
- This reinforces the idea that lipid metabolism is essential for normal nervous system function.
- In Parkinson’s disease, neuronal dysfunction is mainly related to loss of dopaminergic neurons, not sphingomyelinase deficiency.
2: Dopamine and Basal Ganglia Function in Parkinson’s Disease
🧠 CORE
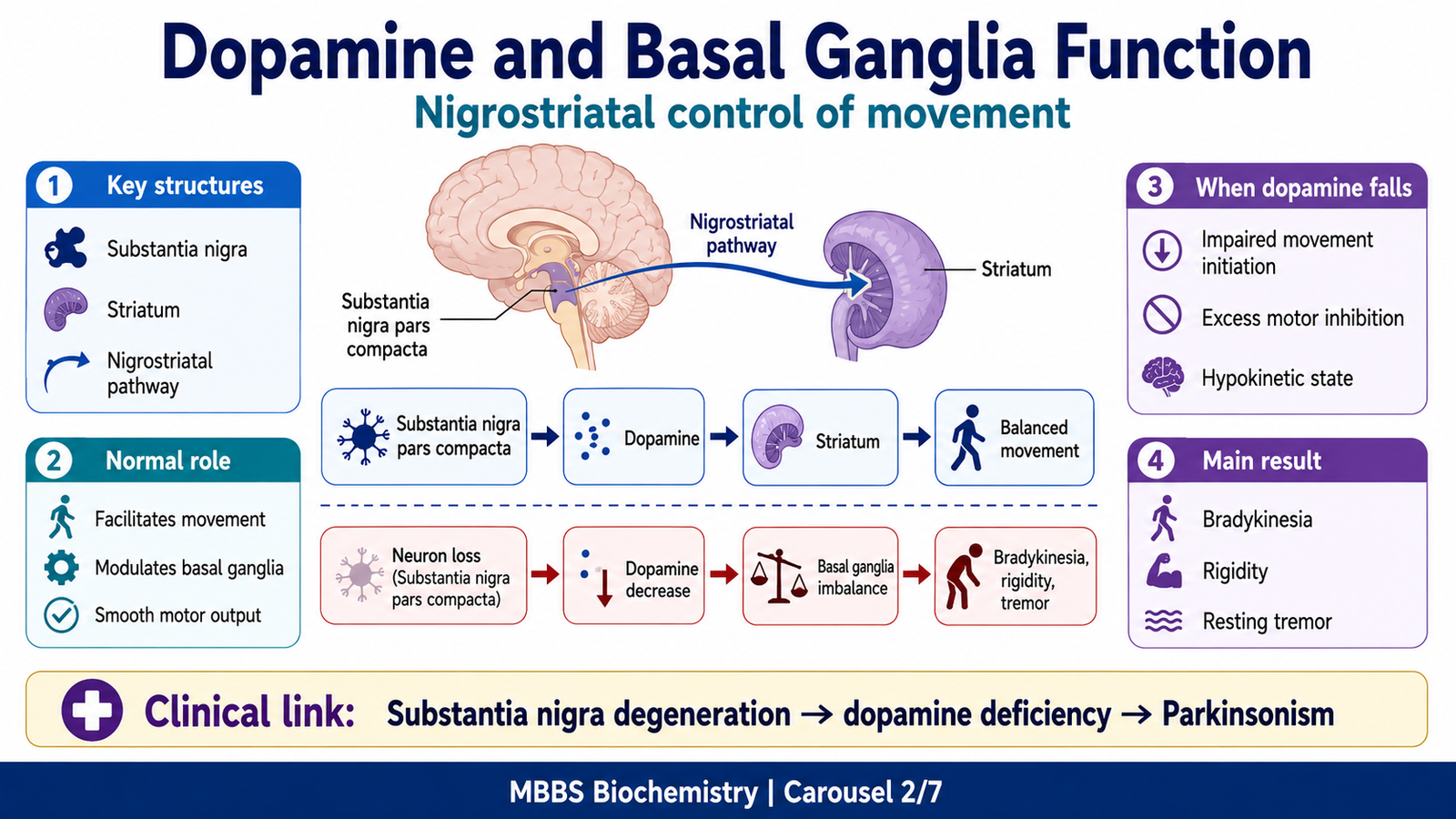
- Parkinson’s disease mainly involves degeneration of dopaminergic neurons in the substantia nigra pars compacta.
- These neurons normally project to the striatum through the nigrostriatal pathway.
- Dopamine helps facilitate desired movement and suppress unwanted motor activity.
- Loss of dopamine disturbs basal ganglia motor circuits.
- The result is bradykinesia, rigidity, resting tremor, and postural instability.
- Parkinsonian tremor is classically a resting tremor.
- The biochemical basis of treatment is restoration of dopaminergic activity.
🔬 CONCEPT EXPLAINED
Normal voluntary movement requires smooth selection and execution of motor programs. The basal ganglia do not directly contract muscles. Instead, they regulate motor cortex activity by selecting desired movements and suppressing competing unwanted movements. This control depends heavily on dopamine.
The substantia nigra pars compacta sends dopaminergic fibers to the striatum. Dopamine modifies the activity of basal ganglia pathways. In simple terms, dopamine supports movement by facilitating the direct pathway and reducing excessive inhibitory output from the basal ganglia. When dopamine is available in adequate amount, movement becomes easier to initiate and scale.
In Parkinson’s disease, dopaminergic neurons gradually degenerate. As dopamine levels fall in the striatum, the basal ganglia become excessively inhibitory toward motor output. This means the motor cortex receives less facilitation for voluntary movement. As a result, the patient develops bradykinesia and difficulty initiating movement.
Rigidity occurs because motor control becomes abnormally stiff and poorly modulated. Tremor appears because abnormal oscillatory activity develops within motor circuits. Postural instability occurs later because automatic postural reflexes are impaired.
The important clinical connection is that the location of neuronal loss explains the symptoms. Since the substantia nigra normally supports movement through dopamine, its degeneration produces hypokinetic motor features. This is why Parkinson’s disease is called a movement disorder.
⚠️ CLINICAL IMPORTANCE
- Loss of substantia nigra dopaminergic neurons reduces dopamine in the striatum.
- Reduced dopamine causes difficulty initiating and controlling movement.
- The typical motor features are bradykinesia, rigidity, resting tremor, and postural instability.
- Substantia nigra involvement is therefore central to Parkinson’s disease.
- Treatment is aimed at increasing dopaminergic activity or reducing cholinergic imbalance.
3: Pathology and Clinical Features of Parkinson’s Disease
🧠 CORE
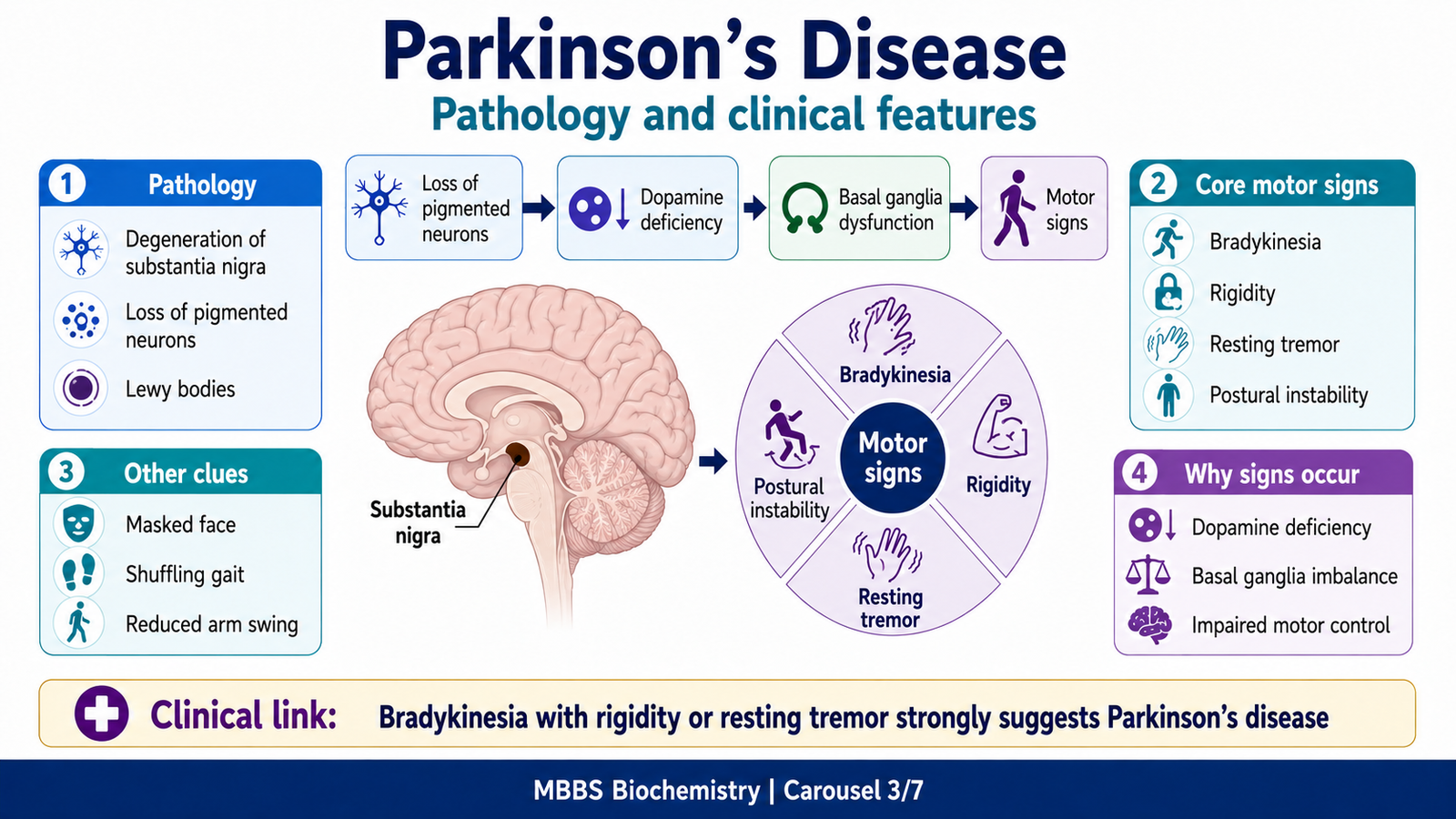
- Parkinson’s disease is a chronic progressive neurodegenerative disorder.
- The main pathology is degeneration of dopaminergic neurons in substantia nigra pars compacta.
- Loss of pigmented neurons causes pallor of the substantia nigra.
- Lewy bodies are characteristic pathological inclusions.
- Main clinical features are resting tremor, rigidity, bradykinesia, and postural instability.
- Non-motor symptoms may include mood changes, sleep problems, autonomic symptoms, and cognitive decline.
- Clinical features reflect basal ganglia dysfunction.
🔬 CONCEPT EXPLAINED
Parkinson’s disease develops when dopaminergic neurons in the substantia nigra pars compacta progressively degenerate. These neurons normally contain neuromelanin pigment, which gives the substantia nigra its dark appearance. When these neurons are lost, the substantia nigra becomes pale.
A characteristic pathological finding is the presence of Lewy bodies, which are abnormal protein aggregates inside neurons. At this undergraduate level, students should remember Lewy bodies as a pathological marker of Parkinson’s disease rather than studying detailed molecular pathology.
The clinical features arise directly from impaired basal ganglia control of movement. The most important feature is bradykinesia, which means slowness of movement. It may appear as reduced facial expression, slow walking, small handwriting, reduced arm swing, and difficulty starting movement.
Rigidity is increased muscle tone felt throughout passive movement. It may be described clinically as lead-pipe rigidity or cogwheel rigidity when tremor is superimposed.
Resting tremor is classically seen when the limb is relaxed and supported. It decreases during voluntary movement. The typical tremor is often described as “pill-rolling” because the thumb and fingers appear to move as if rolling a small object.
Postural instability usually appears later and increases the risk of falls. It reflects impaired automatic postural adjustment.
Non-motor symptoms are also important because Parkinson’s disease is not purely a motor disorder. Patients may develop constipation, depression, sleep disturbance, autonomic symptoms, reduced smell, and later cognitive impairment. However, for 2nd-year integrated learning, the main examinable focus remains the relationship between substantia nigra degeneration, dopamine deficiency, basal ganglia dysfunction, and motor features.
⚠️ CLINICAL IMPORTANCE
- Parkinson’s disease should be suspected when bradykinesia is associated with resting tremor or rigidity.
- Resting tremor points toward basal ganglia dysfunction.
- Intention tremor points more toward cerebellar dysfunction.
- The pathology explains the symptoms: substantia nigra degeneration → dopamine deficiency → basal ganglia imbalance → movement disorder.
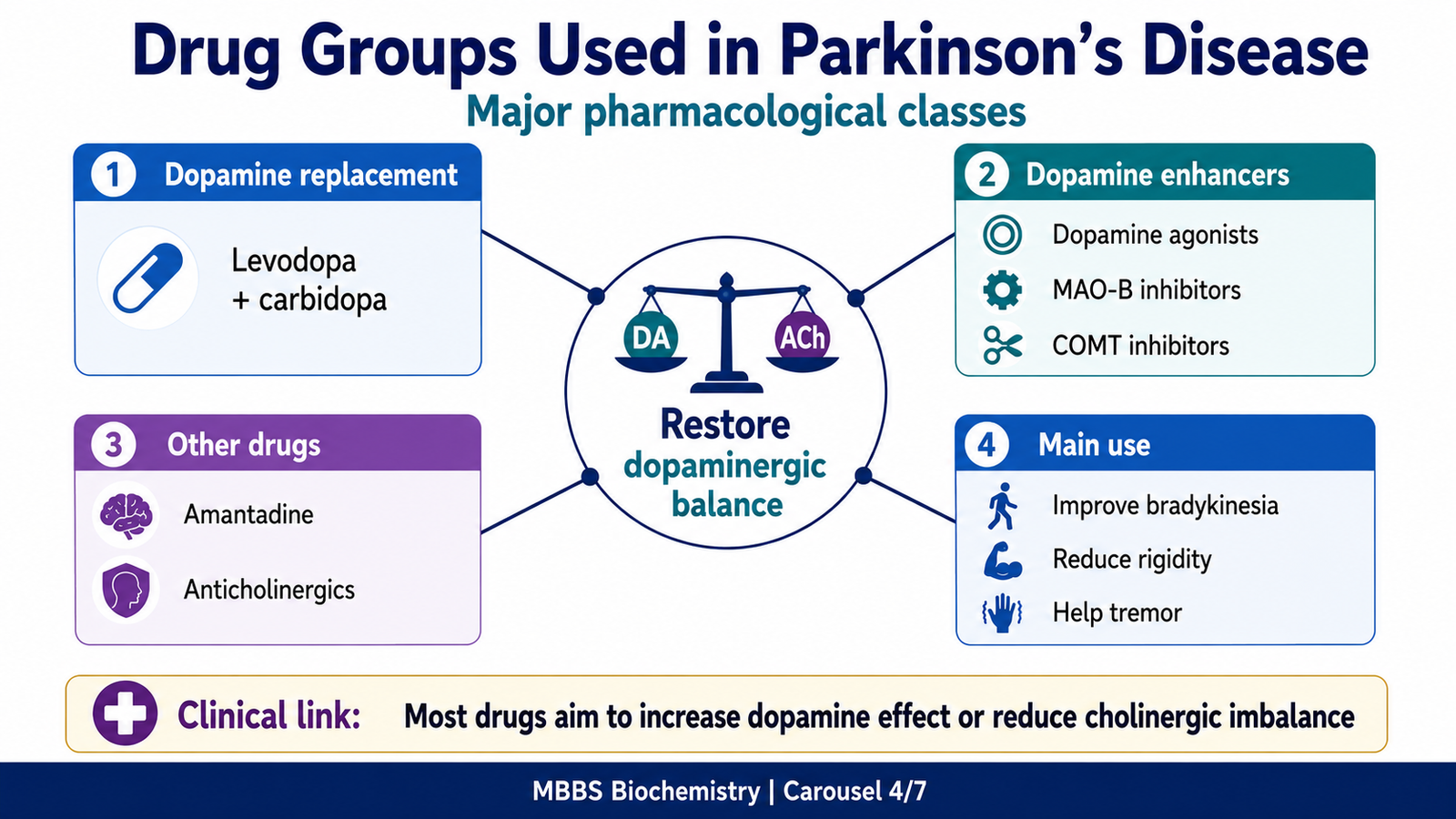
4: Pharmacological Groups Used in Parkinson’s Disease
🧠 CORE
- Parkinson’s disease drugs mainly aim to increase dopaminergic activity or reduce cholinergic overactivity.
- Major drug groups include levodopa with carbidopa, dopamine agonists, MAO-B inhibitors, COMT inhibitors, amantadine, and anticholinergics.
- Levodopa is the most effective symptomatic drug.
- Carbidopa prevents peripheral conversion of levodopa to dopamine.
- Dopamine agonists directly stimulate dopamine receptors.
- MAO-B and COMT inhibitors reduce dopamine breakdown.
- Anticholinergics are more useful for tremor than bradykinesia.
🔬 CONCEPT EXPLAINED
The pharmacological treatment of Parkinson’s disease is based on one major principle: dopamine is deficient in the basal ganglia. Therefore, treatment attempts to restore dopaminergic function or rebalance dopamine and acetylcholine activity.
Levodopa with Carbidopa
Dopamine itself cannot be given effectively because it does not cross the blood-brain barrier. Therefore, the precursor levodopa is used. Levodopa crosses the blood-brain barrier and is converted into dopamine inside the brain.
However, levodopa can also be converted into dopamine in peripheral tissues. Peripheral dopamine causes side effects such as nausea, vomiting, postural hypotension, and cardiac effects. To reduce this, levodopa is combined with carbidopa. Carbidopa inhibits peripheral dopa decarboxylase but does not cross the blood-brain barrier. Therefore, more levodopa reaches the brain and fewer peripheral side effects occur.
This combination is highly effective for improving bradykinesia and rigidity. Over time, however, patients may develop motor fluctuations and dyskinesias.
Dopamine Agonists
Dopamine agonists directly stimulate dopamine receptors in the brain. Examples include bromocriptine, pramipexole, ropinirole, and rotigotine. They do not require conversion into dopamine, so they can act directly on dopamine receptors.
These drugs may be used alone in early disease or combined with levodopa later. Their effect is usually less powerful than levodopa but may last longer. Important adverse effects include nausea, hypotension, hallucinations, sleepiness, and impulse-control problems.
MAO-B Inhibitors
Dopamine is metabolized in the brain by monoamine oxidase-B. MAO-B inhibitors such as selegiline and rasagiline reduce dopamine breakdown. As a result, dopamine remains available for a longer time in the synaptic region.
These drugs are useful in early disease or as add-on therapy to levodopa. Their effect is moderate, but they support dopaminergic activity.
COMT Inhibitors
Catechol-O-methyltransferase also participates in levodopa and dopamine metabolism. COMT inhibitors such as entacapone and tolcapone reduce levodopa breakdown. This prolongs levodopa action and helps reduce “wearing-off” symptoms.
Entacapone mainly acts peripherally and is commonly used with levodopa-carbidopa. Tolcapone can act centrally and peripherally but has greater risk of hepatotoxicity, so its use requires caution.
Amantadine
Amantadine has multiple actions. It increases dopamine release, reduces dopamine reuptake, and has NMDA receptor antagonist effects. It may help symptoms of Parkinson’s disease and is especially useful for reducing levodopa-induced dyskinesia.
Anticholinergic Drugs
In Parkinson’s disease, loss of dopamine creates a relative excess of cholinergic activity in the striatum. Anticholinergic drugs such as trihexyphenidyl and benztropine reduce this cholinergic overactivity.
These drugs are more useful for tremor and rigidity than for bradykinesia. They are usually avoided in elderly patients because they can cause confusion, dry mouth, urinary retention, constipation, and blurred vision.
⚠️ CLINICAL IMPORTANCE
- Levodopa-carbidopa is the most effective symptomatic treatment.
- Carbidopa reduces peripheral side effects and increases levodopa availability in the brain.
- Dopamine agonists directly stimulate dopamine receptors.
- MAO-B and COMT inhibitors prolong dopamine or levodopa action.
- Anticholinergics mainly help tremor but have important side effects, especially in older patients.
- Drug choice depends on symptoms, age, severity, and adverse effect profile.
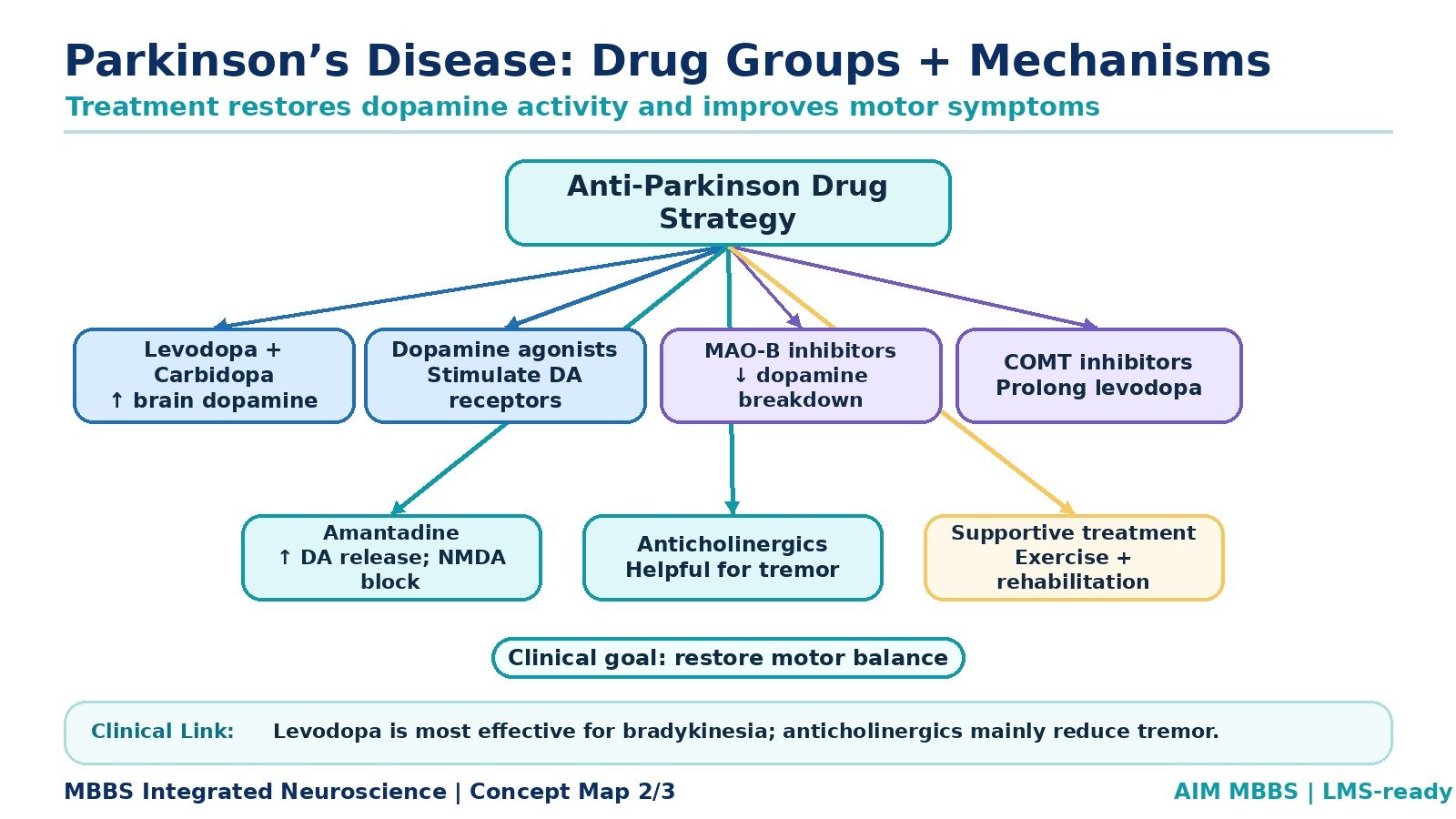
5: Mechanism of Action of Parkinson’s Disease Drugs
🧠 CORE
- Drug mechanisms are based on correcting dopamine deficiency.
- Levodopa increases dopamine synthesis in the brain.
- Carbidopa blocks peripheral levodopa conversion.
- Dopamine agonists directly activate dopamine receptors.
- MAO-B inhibitors reduce dopamine degradation in the brain.
- COMT inhibitors reduce levodopa breakdown and prolong its action.
- Anticholinergics reduce relative cholinergic overactivity.
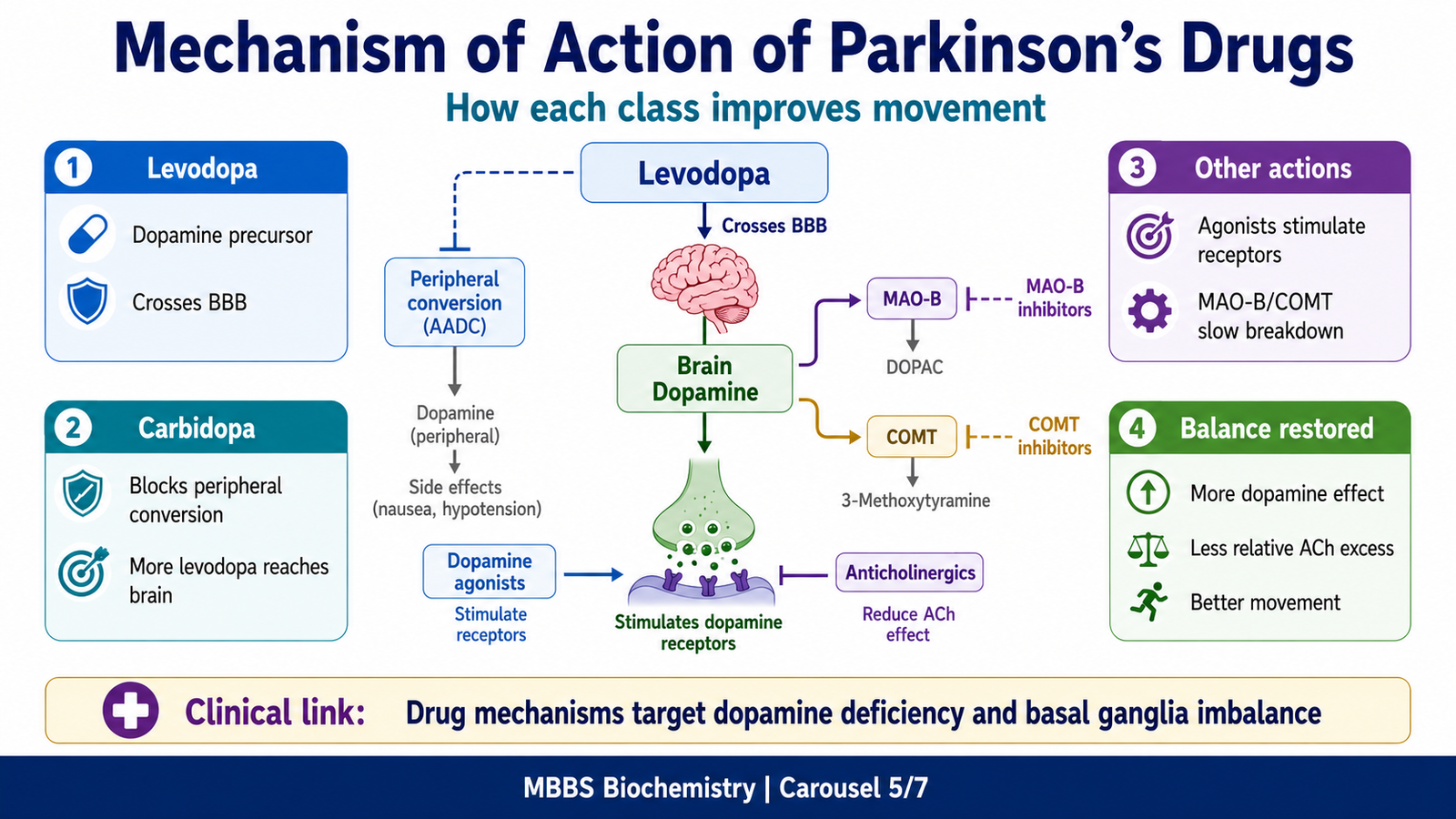
🔬 CONCEPT EXPLAINED
The mechanism of Parkinson’s drug therapy becomes easy when students connect each drug to one question: How does this drug improve dopaminergic function or reduce imbalance in the basal ganglia?
Levodopa works by replacing the missing biochemical precursor. Since dopamine cannot enter the brain efficiently, levodopa is given because it can cross the blood-brain barrier. Once inside the brain, it is converted by dopa decarboxylase into dopamine. This increases dopamine availability in the striatum and improves movement.
Carbidopa works outside the brain. It inhibits peripheral dopa decarboxylase, preventing levodopa from becoming dopamine before reaching the brain. This has two benefits: more levodopa enters the brain, and peripheral dopamine-related side effects decrease.
Dopamine agonists bypass dopamine synthesis and directly stimulate dopamine receptors. This means they can produce dopaminergic effects even when some dopamine-producing neurons are lost.
MAO-B inhibitors prevent enzymatic breakdown of dopamine in the brain. Therefore, whatever dopamine is available remains active for longer.
COMT inhibitors prevent breakdown of levodopa, especially in the periphery. This prolongs the duration of levodopa action and helps reduce wearing-off symptoms.
Anticholinergic drugs do not increase dopamine. Instead, they reduce acetylcholine activity. This is useful because dopamine deficiency creates a relative cholinergic dominance in the striatum. By reducing cholinergic influence, the functional balance between dopamine and acetylcholine improves.
Therefore, all drug groups are connected by one pharmacological principle: restore basal ganglia motor balance.
⚠️ CLINICAL IMPORTANCE
- Mechanism-based learning helps predict both therapeutic effects and adverse effects.
- Drugs increasing dopamine may improve movement but may also cause dyskinesia, hallucinations, or nausea.
- Anticholinergic drugs may reduce tremor but can cause dry mouth, urinary retention, constipation, and confusion.
- Long-term levodopa therapy may produce wearing-off and dyskinesia.
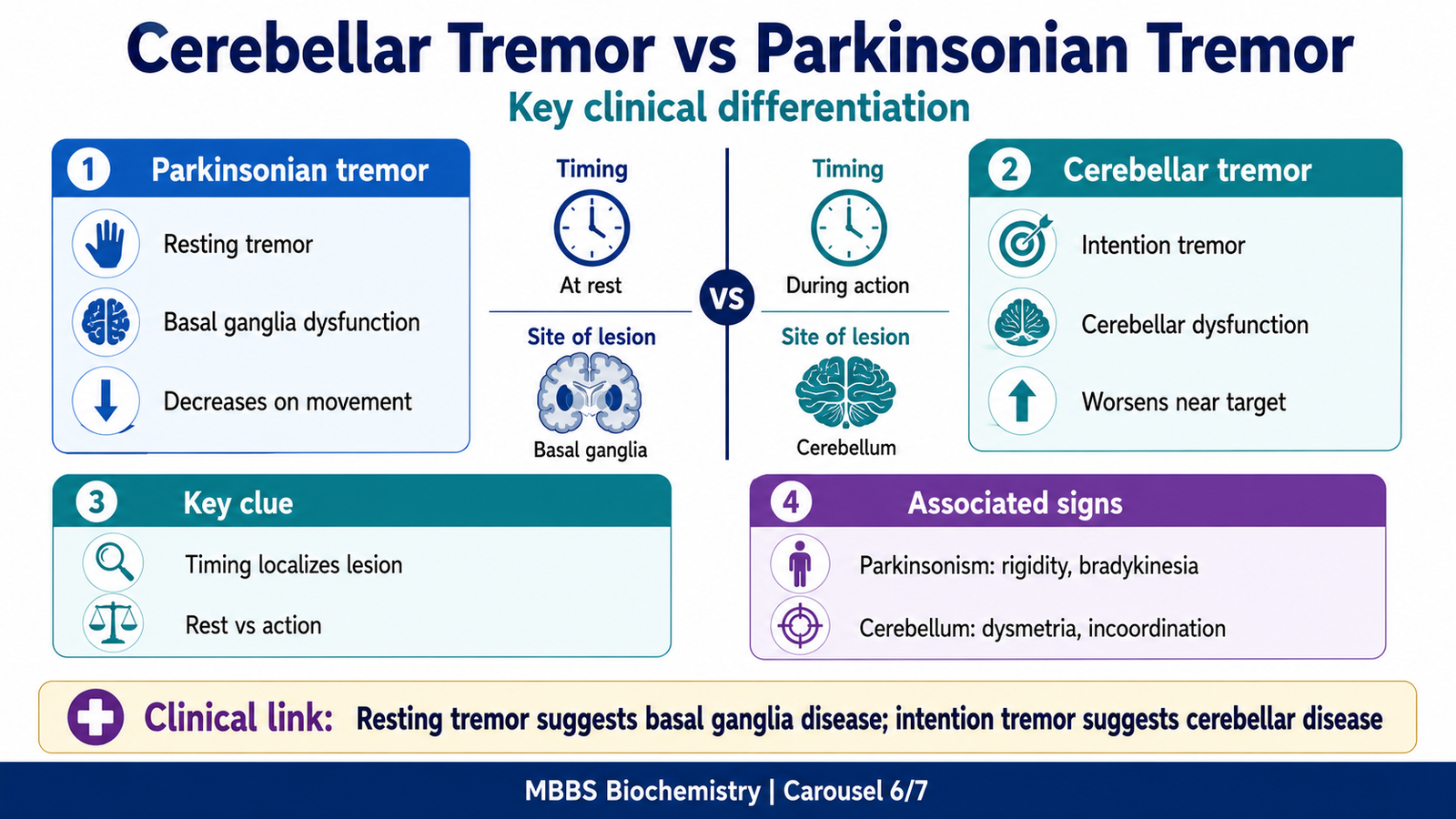
6: Tremor Integration — Cerebellar Tremor versus Parkinsonian Tremor
🧠 CORE
- Tremor is an involuntary rhythmic oscillatory movement.
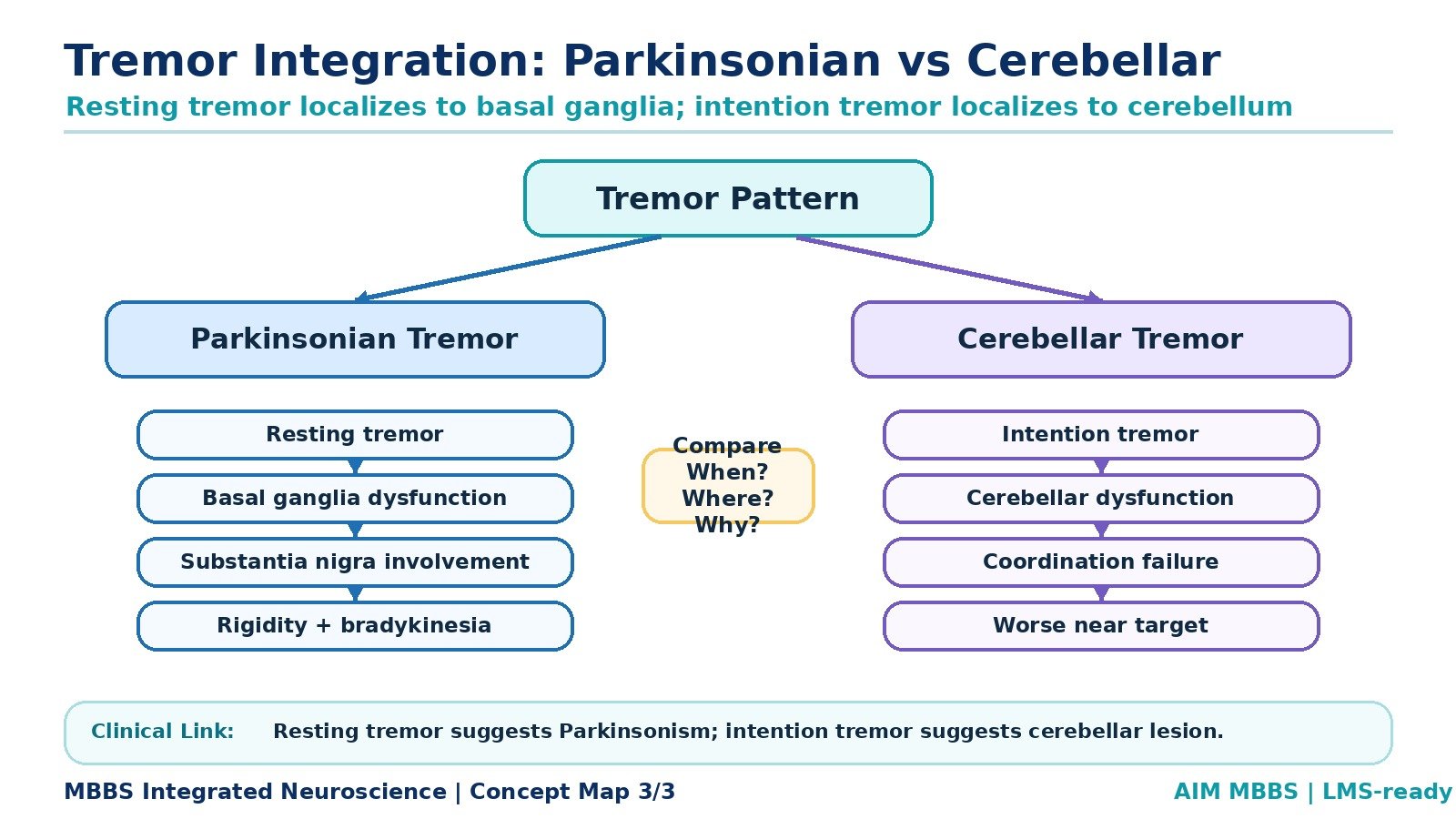
- Parkinsonian tremor is typically a resting tremor.
- Cerebellar tremor is typically an intention tremor.
- Parkinsonian tremor is related to basal ganglia dysfunction.
- Cerebellar tremor is related to coordination failure.
- Parkinsonian tremor decreases during voluntary movement.
- Cerebellar tremor worsens as the target is approached.
🔬 CONCEPT EXPLAINED
Tremor becomes clinically meaningful when it is interpreted according to when it appears. The timing of tremor helps identify the damaged motor system.
In Parkinson’s disease, the tremor is usually present when the limb is at rest. This occurs because basal ganglia circuits are abnormal even when the patient is not performing a purposeful movement. The tremor often decreases when the patient starts voluntary movement. This is why it is called a resting tremor.
Parkinsonian tremor is commonly slow and rhythmic and may involve the hands in a pill-rolling pattern. It reflects basal ganglia dysfunction due to dopamine deficiency.
Cerebellar tremor is different. The cerebellum is responsible for coordination, timing, error correction, and smooth execution of movement. When the cerebellum is damaged, the patient can initiate movement, but the movement becomes poorly coordinated. The tremor appears during purposeful movement and becomes worse as the finger approaches a target. This is called an intention tremor.
Therefore, the difference is not just descriptive; it reflects different mechanisms. Basal ganglia dysfunction produces tremor at rest because motor program regulation is abnormal. Cerebellar dysfunction produces tremor during action because coordination and correction of movement are impaired.
Comparison Table: Cerebellar Tremor and Parkinsonian Tremor
| Feature | Parkinsonian Tremor | Cerebellar Tremor |
|---|---|---|
| Type | Resting tremor | Intention tremor |
| Appears when | Limb is at rest | During voluntary movement |
| Effect of movement | Usually decreases | Worsens during movement |
| System involved | Basal ganglia | Cerebellum |
| Mechanism | Dopamine deficiency and basal ganglia circuit dysfunction | Coordination failure and impaired error correction |
| Common association | Parkinson’s disease | Cerebellar lesion |
| Clinical clue | Pill-rolling tremor | Past-pointing, dysmetria, intention tremor |
⚠️ CLINICAL IMPORTANCE
- Resting tremor suggests basal ganglia dysfunction.
- Intention tremor suggests cerebellar dysfunction.
- Parkinsonian tremor is related to substantia nigra degeneration.
- Cerebellar tremor reflects failure of coordination, not dopamine deficiency.
- This distinction is commonly tested in exams and clinically useful during neurological examination.
7: Treatment of Parkinson’s Disease — Integrated Clinical View
🧠 CORE
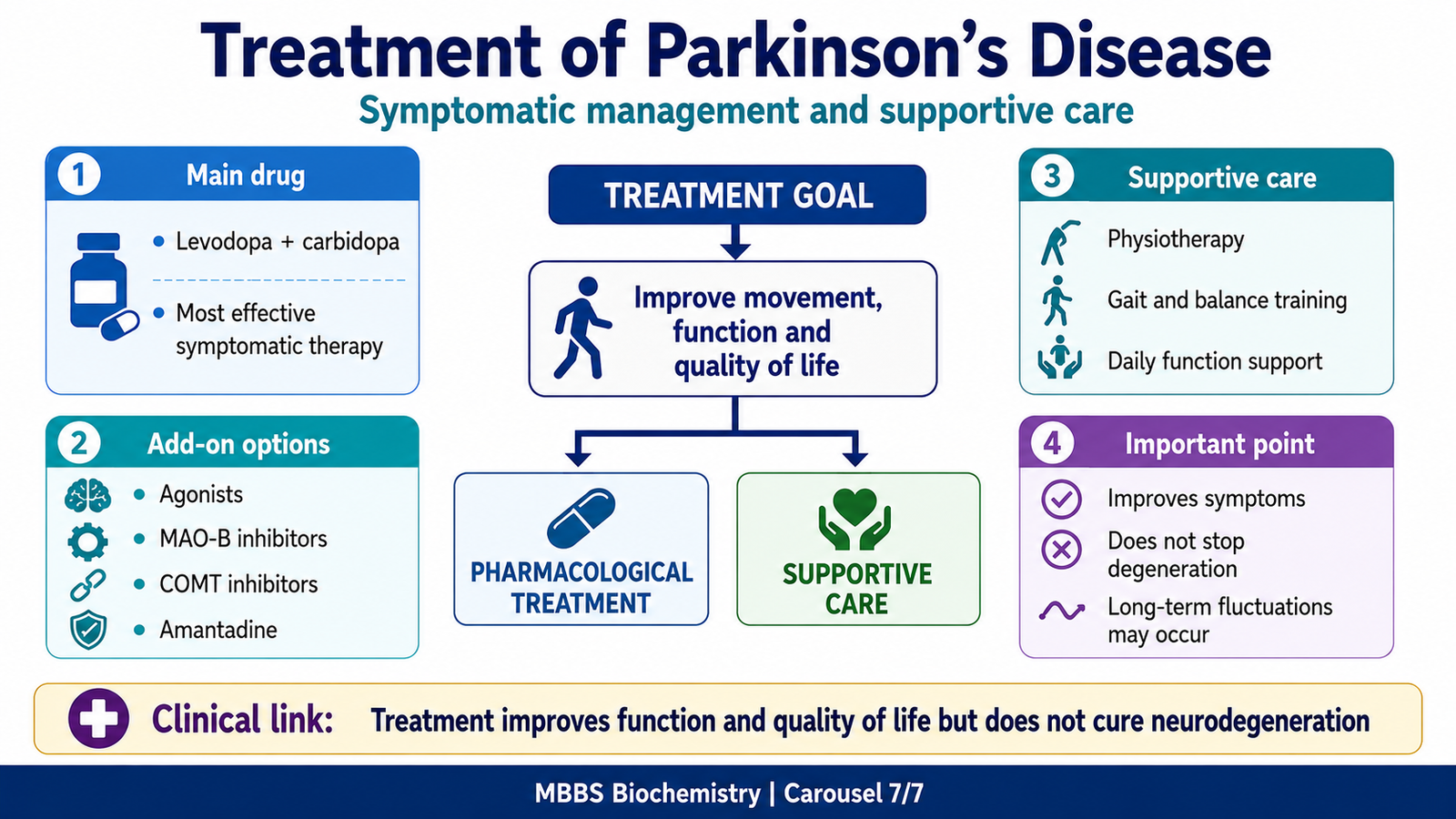
- Treatment is mainly symptomatic.
- Main aim is to improve functional movement and quality of life.
- Levodopa-carbidopa is the most effective drug therapy.
- Dopamine agonists, MAO-B inhibitors, COMT inhibitors, amantadine, and anticholinergics are used according to symptoms.
- Physiotherapy and exercise are important supportive measures.
- Advanced disease may require specialist management.
- Treatment does not completely stop neurodegeneration.
🔬 CONCEPT EXPLAINED
Treatment of Parkinson’s disease is based on the severity of symptoms, age of the patient, functional disability, and adverse effect risk. The central problem is dopamine deficiency in the basal ganglia, so most drugs aim to increase dopamine effect.
In early mild disease, drugs such as MAO-B inhibitors or dopamine agonists may be used depending on the patient profile. When symptoms interfere with daily function, levodopa-carbidopa is usually the most effective treatment.
Levodopa improves bradykinesia and rigidity strongly, but long-term use may cause motor fluctuations. Patients may experience “wearing-off,” where benefit decreases before the next dose, or dyskinesias, which are involuntary movements due to excessive dopaminergic stimulation.
Supportive treatment is also important. Physiotherapy helps maintain mobility, posture, balance, and gait. Speech therapy may help patients with soft voice or swallowing difficulty. Occupational therapy helps with daily activities.
At this level, students should understand the principle rather than detailed specialist protocols: Parkinson’s treatment improves symptoms by restoring dopaminergic function, reducing motor imbalance, and supporting daily movement.
⚠️ CLINICAL IMPORTANCE
- Parkinson’s treatment is symptomatic and individualized.
- Levodopa-carbidopa remains the most effective drug therapy.
- Long-term therapy may cause motor fluctuations and dyskinesia.
- Non-drug support is important for mobility and quality of life.
- Recognizing tremor type helps identify whether the problem is basal ganglia or cerebellar.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure / Biochemical Component | Function | Outcome if Normal | Outcome if Impaired |
|---|---|---|---|
| Sphingomyelin | Maintains membrane and myelin integrity | Stable nerve conduction | Storage disease or neurological dysfunction if metabolism fails |
| Myelin sheath | Insulates axons | Rapid impulse conduction | Slowed or impaired nerve signaling |
| Substantia nigra pars compacta | Produces dopamine | Smooth basal ganglia motor regulation | Parkinson’s disease features |
| Nigrostriatal pathway | Delivers dopamine to striatum | Facilitates movement control | Bradykinesia, rigidity, tremor |
| Striatum | Receives dopamine and regulates motor circuits | Balanced motor program selection | Abnormal movement control |
| Cerebellum | Coordinates voluntary movement | Smooth accurate movement | Intention tremor and dysmetria |
| Levodopa | Dopamine precursor | Restores dopamine synthesis | Improves Parkinsonian symptoms |
| Carbidopa | Blocks peripheral levodopa conversion | More levodopa reaches brain | Reduces peripheral adverse effects |
Integrated Explanation
The biochemical integrity of nervous tissue depends on lipids such as sphingomyelin, while functional motor control depends on neurotransmitters such as dopamine. Sphingomyelin supports neuronal membrane and myelin stability, allowing efficient conduction of impulses. Dopamine supports basal ganglia regulation of movement.
When sphingomyelin metabolism fails, lipid accumulation can damage cells. When dopaminergic neurons of the substantia nigra fail, basal ganglia circuits become imbalanced. In both situations, a biochemical disturbance produces neurological consequences.
Thus, Parkinson’s disease is best understood as a clinical movement disorder with a strong biochemical foundation: degeneration of dopamine-producing neurons causes neurotransmitter imbalance, which leads to abnormal motor output.
🩺 5️⃣ Clinical Correlation
Parkinson’s Disease
Parkinson’s disease is caused mainly by progressive loss of dopaminergic neurons in the substantia nigra pars compacta. This reduces dopamine in the striatum and disturbs basal ganglia control of movement. The patient develops bradykinesia, rigidity, resting tremor, and postural instability.
Parkinsonian Tremor
Parkinsonian tremor is a resting tremor. It appears when the limb is relaxed and decreases with voluntary movement. It reflects basal ganglia dysfunction due to dopamine deficiency.
Cerebellar Tremor
Cerebellar tremor is an intention tremor. It appears during purposeful movement and worsens near the target. It occurs because the cerebellum cannot properly coordinate and correct movement.
Niemann-Pick Disease
Niemann-Pick disease is classically associated with sphingomyelinase deficiency. Sphingomyelin accumulates in lysosomes, causing cellular dysfunction. It is important here as a biochemical example of how defective sphingolipid metabolism can affect nervous tissue.
Drug-Related Clinical Concepts
Levodopa-carbidopa improves Parkinsonian motor symptoms by increasing dopamine availability in the brain. However, long-term use may cause wearing-off and dyskinesia. Anticholinergic drugs may help tremor but can cause confusion and autonomic side effects, especially in elderly patients.
📌 6️⃣ Summary Points
- The main phosphosphingolipid is sphingomyelin.
- Sphingomyelin contains sphingosine + fatty acid + phosphate + choline.
- Ceramide is the central intermediate in sphingolipid metabolism.
- Sphingomyelin is broken down by sphingomyelinase.
- Sphingomyelinase deficiency causes Niemann-Pick disease.
- Parkinson’s disease is mainly due to degeneration of dopaminergic neurons in the substantia nigra pars compacta.
- Dopamine deficiency in the striatum causes basal ganglia motor imbalance.
- Main Parkinson’s features are bradykinesia, rigidity, resting tremor, and postural instability.
- Levodopa crosses the blood-brain barrier and is converted into dopamine.
- Carbidopa prevents peripheral conversion of levodopa and reduces peripheral side effects.
- Parkinsonian tremor is a resting tremor due to basal ganglia dysfunction.
- Cerebellar tremor is an intention tremor due to coordination failure.