
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
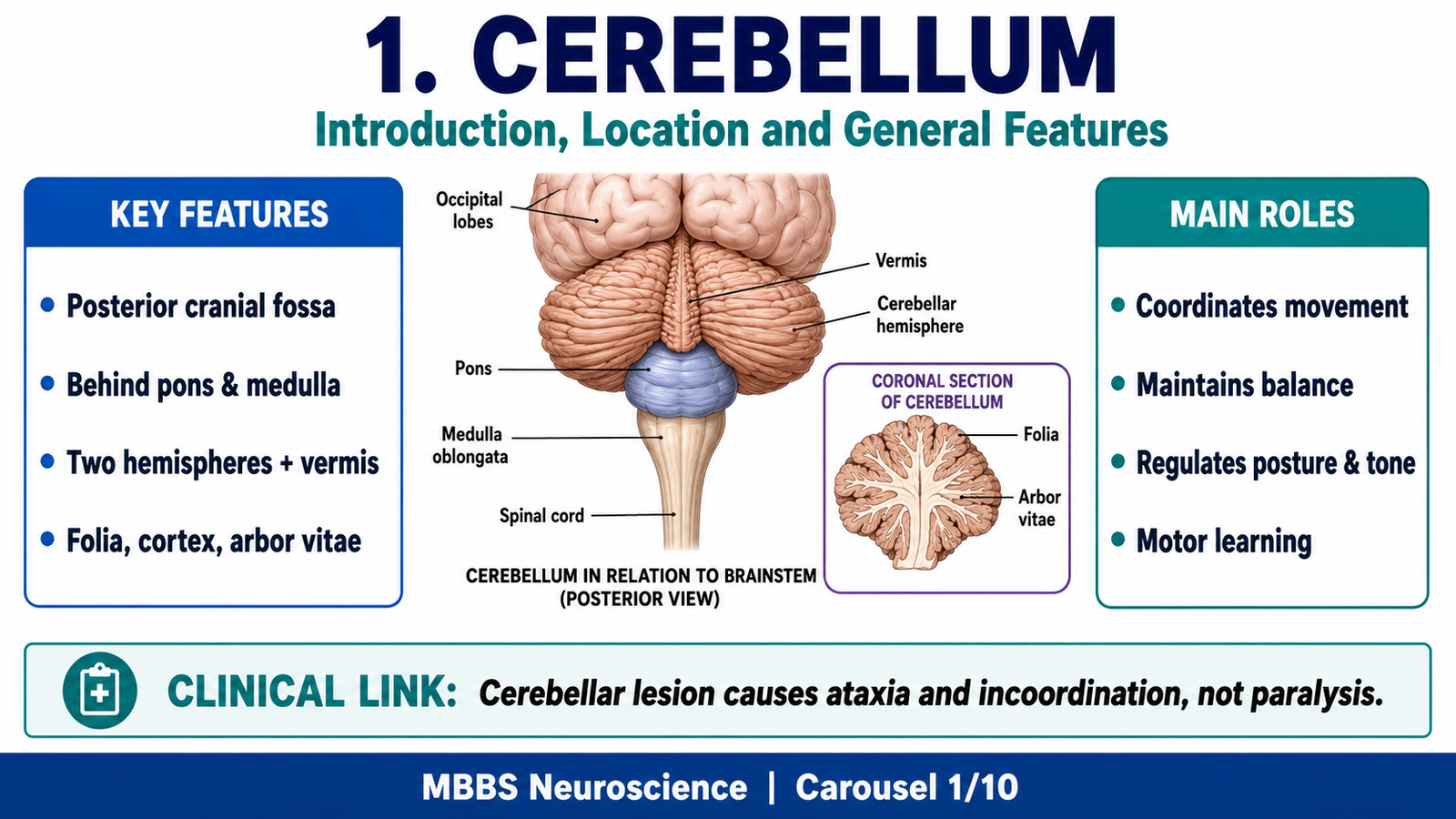
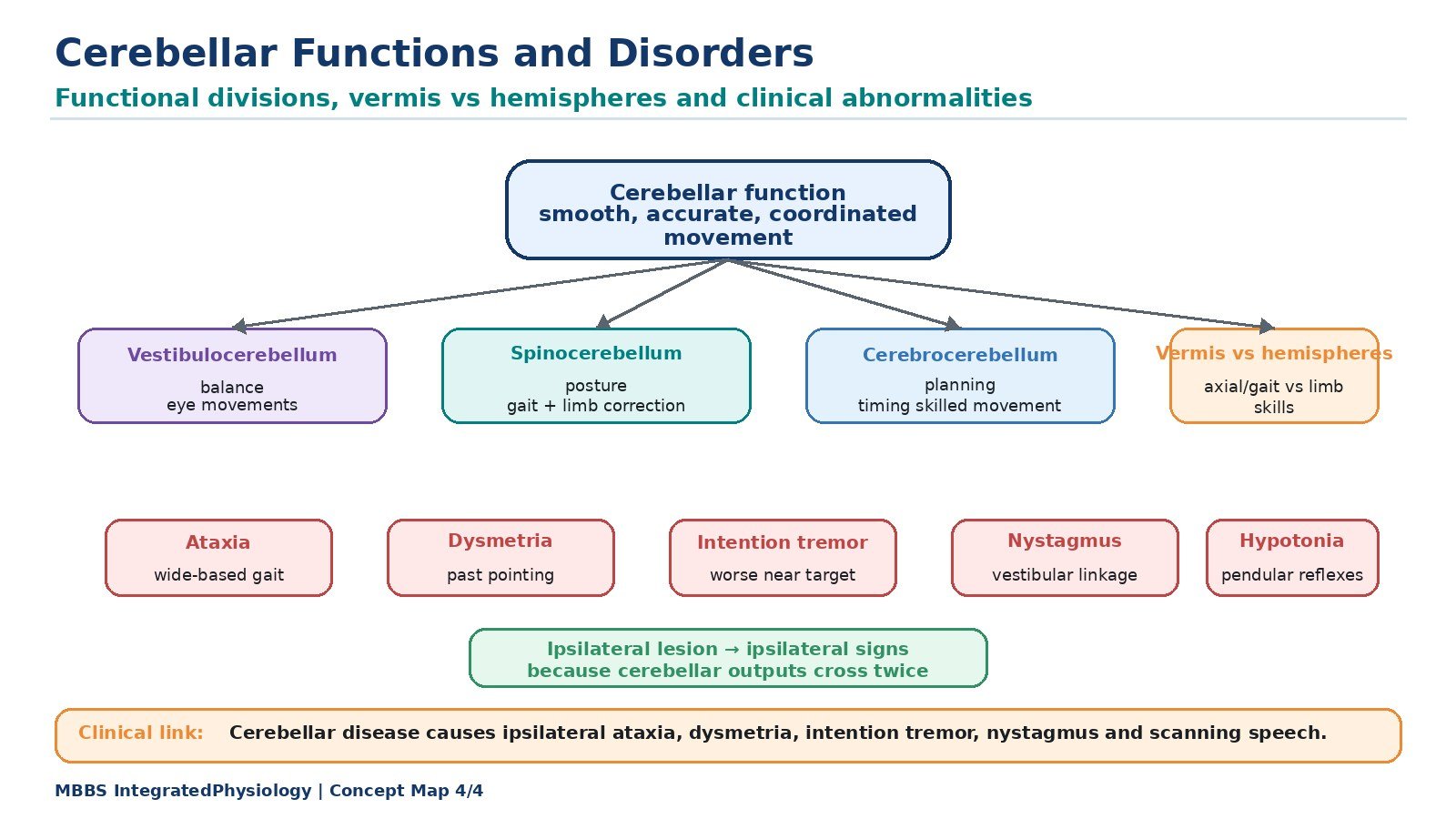
The cerebellum is a major motor coordination center of the brain located in the posterior cranial fossa, behind the pons and medulla and below the occipital lobes of the cerebrum. Although it does not initiate voluntary movement, it is essential for making movements smooth, accurate, coordinated, balanced, and properly timed. The cerebellum continuously compares intended movement with actual movement and corrects errors during motor activity. It also helps maintain posture, muscle tone, equilibrium, eye movements, and motor learning.
Clinically, cerebellar lesions produce characteristic abnormalities such as ataxia, intention tremor, dysmetria, nystagmus, hypotonia, scanning speech, and loss of balance. These signs are important because cerebellar disorders usually affect the same side of the body as the lesion, unlike many corticospinal tract lesions. Understanding cerebellar anatomy, histology, connections, and functions allows students to connect structure with clinical motor disorders.
🔹 2️⃣ Foundation Concepts
Key Definitions
• Cerebellum: A part of the hindbrain responsible for coordination, balance, posture, tone, timing of movement, and motor learning.
• Vermis: The midline part of cerebellum that mainly controls axial and proximal muscles involved in posture and gait.
• Cerebellar hemispheres: Lateral parts of cerebellum involved mainly in coordination of limb movements, especially skilled voluntary movements.
• Cerebellar cortex: Outer gray matter of the cerebellum arranged in three histological layers.
• Deep cerebellar nuclei: Gray matter nuclei inside cerebellar white matter that act as the main output stations of the cerebellum.
• Purkinje cells: Large neurons of cerebellar cortex that provide the only output from cerebellar cortex; they are inhibitory.
• Mossy fibers: Major cerebellar afferent fibers that indirectly influence Purkinje cells through granule cells.
• Climbing fibers: Afferent fibers from the inferior olivary nucleus that powerfully excite Purkinje cells.
• Vestibulocerebellum: Functional division involved in balance and eye movements.
• Spinocerebellum: Functional division involved in posture, tone, and ongoing limb movement correction.
• Cerebrocerebellum: Functional division involved in planning, timing, and coordination of skilled voluntary movements.
Essential Terminology
• Ataxia: Incoordination of voluntary movement.
• Dysmetria: Inability to judge distance or range of movement.
• Intention tremor: Tremor that appears or worsens during purposeful movement.
• Nystagmus: Rhythmic involuntary eye movements.
• Hypotonia: Reduced muscle tone.
• Past pointing: Overshooting a target during finger-nose testing.
• Dysdiadochokinesia: Difficulty performing rapid alternating movements.
• Scanning speech: Slow, irregular, broken speech due to cerebellar involvement.
Basic Overview
• The cerebellum receives information from the cerebral cortex, spinal cord, vestibular system, and brainstem.
• It compares planned motor commands with sensory feedback from actual movement.
• It sends corrective signals through deep cerebellar nuclei to motor areas of the brain and brainstem.
• Its cortex has three layers: molecular layer, Purkinje cell layer, and granular layer.
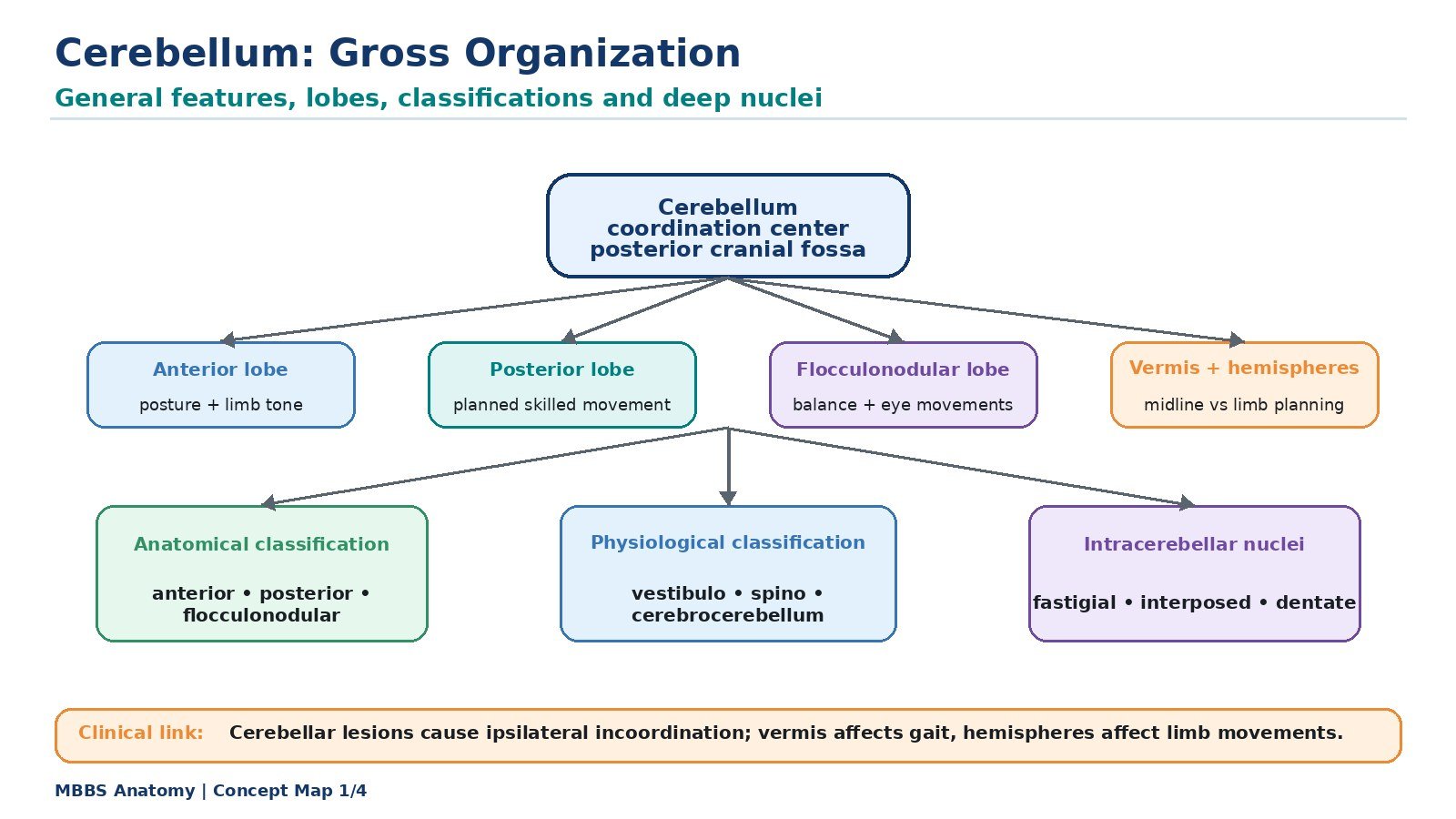
• Its major functional divisions are vestibulocerebellum, spinocerebellum, and cerebrocerebellum.
• Cerebellar lesions cause ipsilateral motor incoordination, not paralysis.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. Gross Anatomy and General Features of Cerebellum
🧠 CORE
• The cerebellum is located in the posterior cranial fossa, behind the brainstem.
• It consists of two cerebellar hemispheres connected by a midline vermis.
• Its surface is folded into narrow leaf-like folds called folia.
• The outer gray matter forms the cerebellar cortex, while inner white matter forms the arbor vitae.
• Deep cerebellar nuclei are embedded within the white matter.
• It is connected to the brainstem by three cerebellar peduncles.
• It coordinates movement, posture, tone, equilibrium, and motor learning.
🔬 CONCEPT EXPLAINED
The cerebellum is a highly folded part of the hindbrain situated below the occipital lobes and behind the pons and medulla. Its folded surface greatly increases the area of cerebellar cortex, allowing it to process large amounts of sensory and motor information. The folds of the cerebellar surface are called folia, and the white matter inside has a branching tree-like appearance called arbor vitae.
Anatomically, the cerebellum has a midline vermis and two lateral cerebellar hemispheres. This arrangement reflects its function. The vermis is more closely related to control of the trunk, posture, and gait, while the hemispheres are more involved in coordination of limb movements and skilled voluntary motor activity.
The cerebellum communicates with the rest of the nervous system through three paired bundles called cerebellar peduncles. The superior cerebellar peduncle mainly carries cerebellar outputs to the midbrain and thalamus, the middle cerebellar peduncle mainly carries inputs from the pontine nuclei, and the inferior cerebellar peduncle carries many inputs from the spinal cord, vestibular system, and medulla. Therefore, the cerebellum is anatomically placed as a monitoring and correction center between sensory feedback, brainstem motor systems, and cortical motor planning areas.
The cerebellum does not directly cause muscle contraction. Instead, it improves the quality of movement by regulating timing, force, range, and coordination. As a result, when the cerebellum is damaged, the patient is not usually paralyzed, but movements become clumsy, inaccurate, tremulous, and poorly coordinated.
⚠️ CLINICAL IMPORTANCE
Damage to cerebellar structure causes incoordination rather than weakness. A patient with cerebellar disease may have normal muscle power but cannot perform smooth purposeful movements. This is an important examination difference from corticospinal tract lesions, where weakness and spasticity are prominent.
2. Lobes and Anatomical Classification of Cerebellum
🧠 CORE
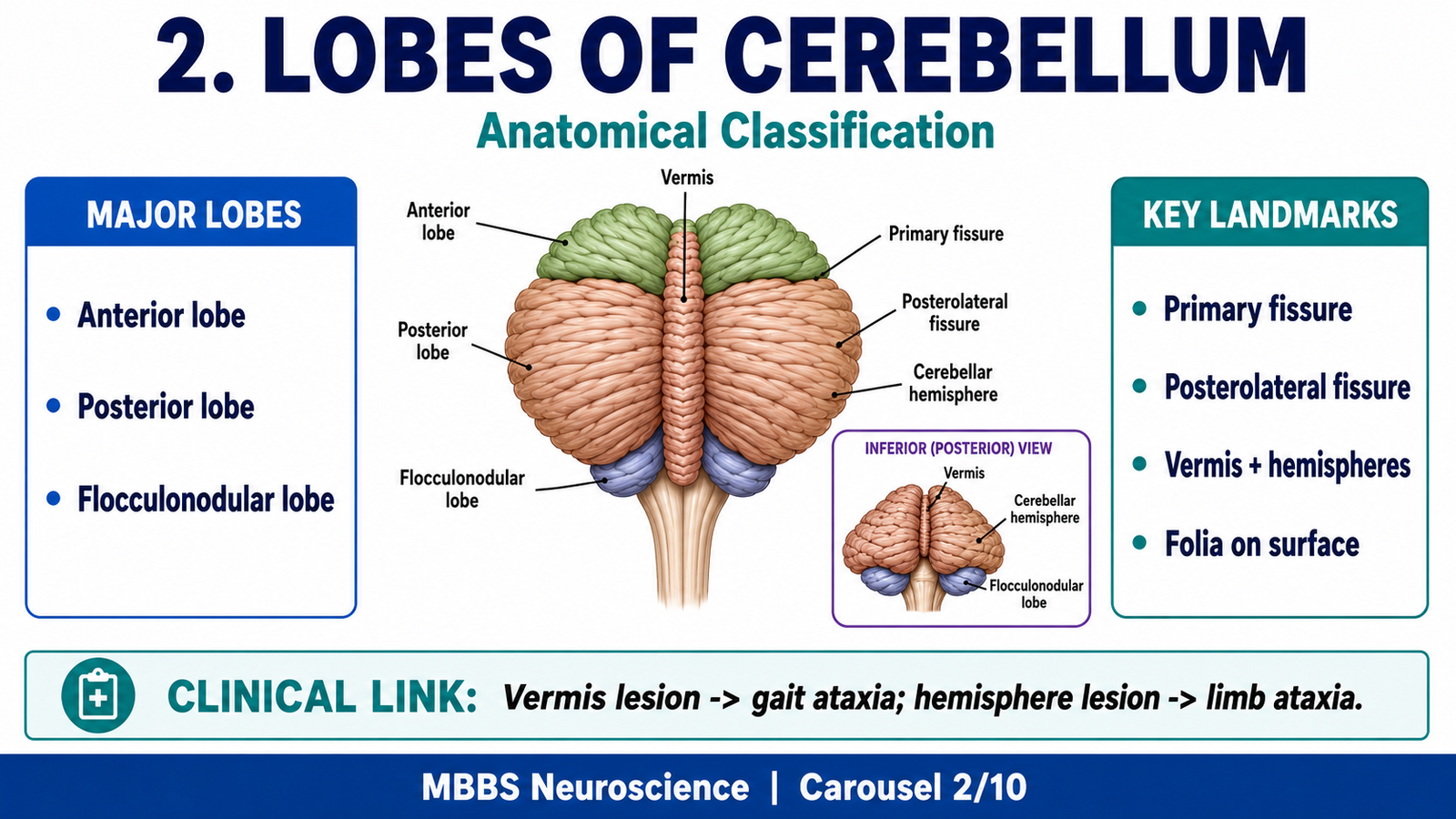
• The cerebellum is divided into anterior, posterior, and flocculonodular lobes.
• The primary fissure separates the anterior lobe from the posterior lobe.
• The posterolateral fissure separates the flocculonodular lobe from the posterior lobe.
• Anatomically, the cerebellum has vermis, intermediate zone, and lateral hemispheres.
• The anterior lobe is mainly related to spinal cord input and posture.
• The posterior lobe is mainly related to skilled voluntary motor coordination.
• The flocculonodular lobe is mainly related to vestibular function and balance.
🔬 CONCEPT EXPLAINED
To understand cerebellar function, students must first understand its lobes. The cerebellum is divided by fissures into three major lobes. The anterior lobe lies above the primary fissure and is mainly associated with control of posture, tone, and limb movement through spinal cord input. The posterior lobe lies between the primary and posterolateral fissures and is the largest part; it is especially important for planning, timing, and coordination of skilled voluntary movements. The flocculonodular lobe is the oldest part of the cerebellum and is closely related to the vestibular system, equilibrium, and eye movements.
Anatomically, the cerebellum can also be divided into the vermis, intermediate zone, and lateral hemispheres. The vermis lies in the midline and is mainly concerned with axial muscles, trunk stability, posture, and gait. The intermediate zone lies lateral to the vermis and is important for control of distal limb movements during ongoing activity. The lateral hemispheres are large in humans because skilled hand movements, planning, and coordination are highly developed.
Therefore, the anatomical organization of the cerebellum directly reflects the type of motor control being performed. Midline parts control posture and balance, while lateral parts participate in complex voluntary movement planning and correction.
⚠️ CLINICAL IMPORTANCE
Lesions of the vermis commonly cause truncal ataxia and gait disturbance. Lesions of the cerebellar hemispheres cause limb ataxia, intention tremor, dysmetria, and past pointing on the same side of the body. Lesions of the flocculonodular lobe commonly produce vertigo, nystagmus, and loss of balance.
3. Physiological Classification of Cerebellum
🧠 CORE
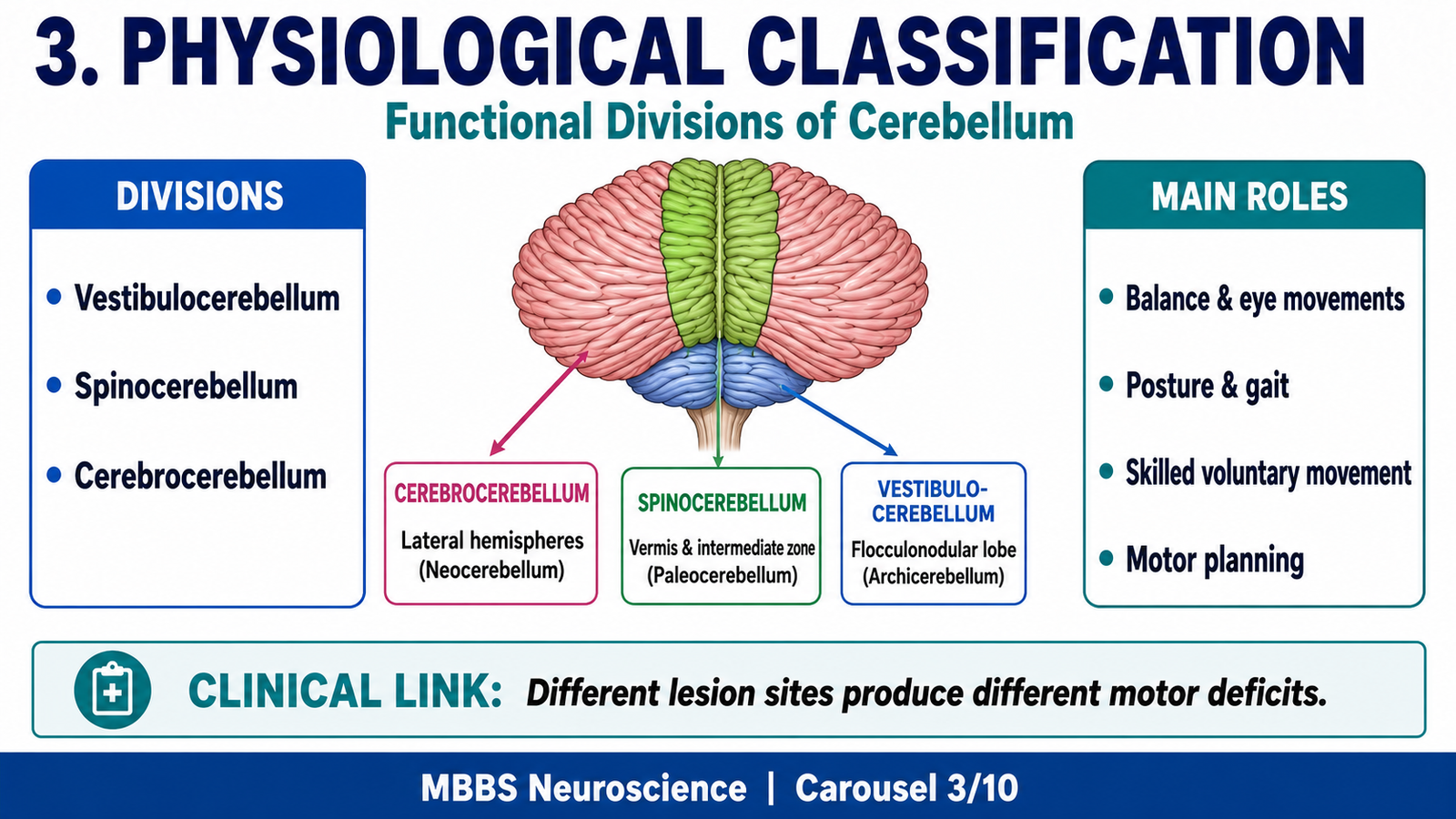
• Physiologically, the cerebellum is divided into vestibulocerebellum, spinocerebellum, and cerebrocerebellum.
• Vestibulocerebellum includes the flocculonodular lobe.
• Spinocerebellum includes vermis and intermediate zones.
• Cerebrocerebellum includes lateral cerebellar hemispheres.
• Each division receives different inputs and performs different motor functions.
• Functional classification helps explain clinical signs of cerebellar lesions.
• The three divisions work together to refine movement and maintain posture.
🔬 CONCEPT EXPLAINED
The physiological classification of cerebellum is based on function and connections rather than only visible anatomy. This classification is very important because cerebellar symptoms become easier to understand when each division is linked to its main input and output pathways.
The vestibulocerebellum mainly consists of the flocculonodular lobe. It receives input from vestibular apparatus and vestibular nuclei and is concerned with balance, equilibrium, and eye movements. It helps coordinate movements of the eyes with movements of the head so that visual fixation remains stable during motion.
The spinocerebellum consists mainly of the vermis and intermediate zone. It receives sensory information from the spinal cord about position, muscle stretch, and ongoing movement. It compares actual movement with intended movement and helps correct errors during movement. It is essential for posture, gait, tone, and smooth execution of limb movements.
The cerebrocerebellum consists mainly of the lateral cerebellar hemispheres. It receives input from the cerebral cortex through pontine nuclei. It is involved in planning, timing, sequencing, and coordination of skilled voluntary movements. This part of the cerebellum is especially important in humans because fine hand movements, speech coordination, and complex motor planning are highly developed.
Thus, physiological classification shows that the cerebellum is not a single uniform motor organ. It is a set of functionally specialized circuits that help the body maintain balance, control posture, guide ongoing movement, and plan complex motor activity.
⚠️ CLINICAL IMPORTANCE
Physiological classification explains why different cerebellar lesions produce different clinical patterns. Vestibulocerebellar lesions mainly disturb balance and eye movements. Spinocerebellar lesions disturb posture, gait, and ongoing movement correction. Cerebrocerebellar lesions disturb skilled voluntary movement, producing intention tremor, dysmetria, and decomposition of movement.
4. Intracerebellar Nuclei and Cerebellar Output Organization
🧠 CORE
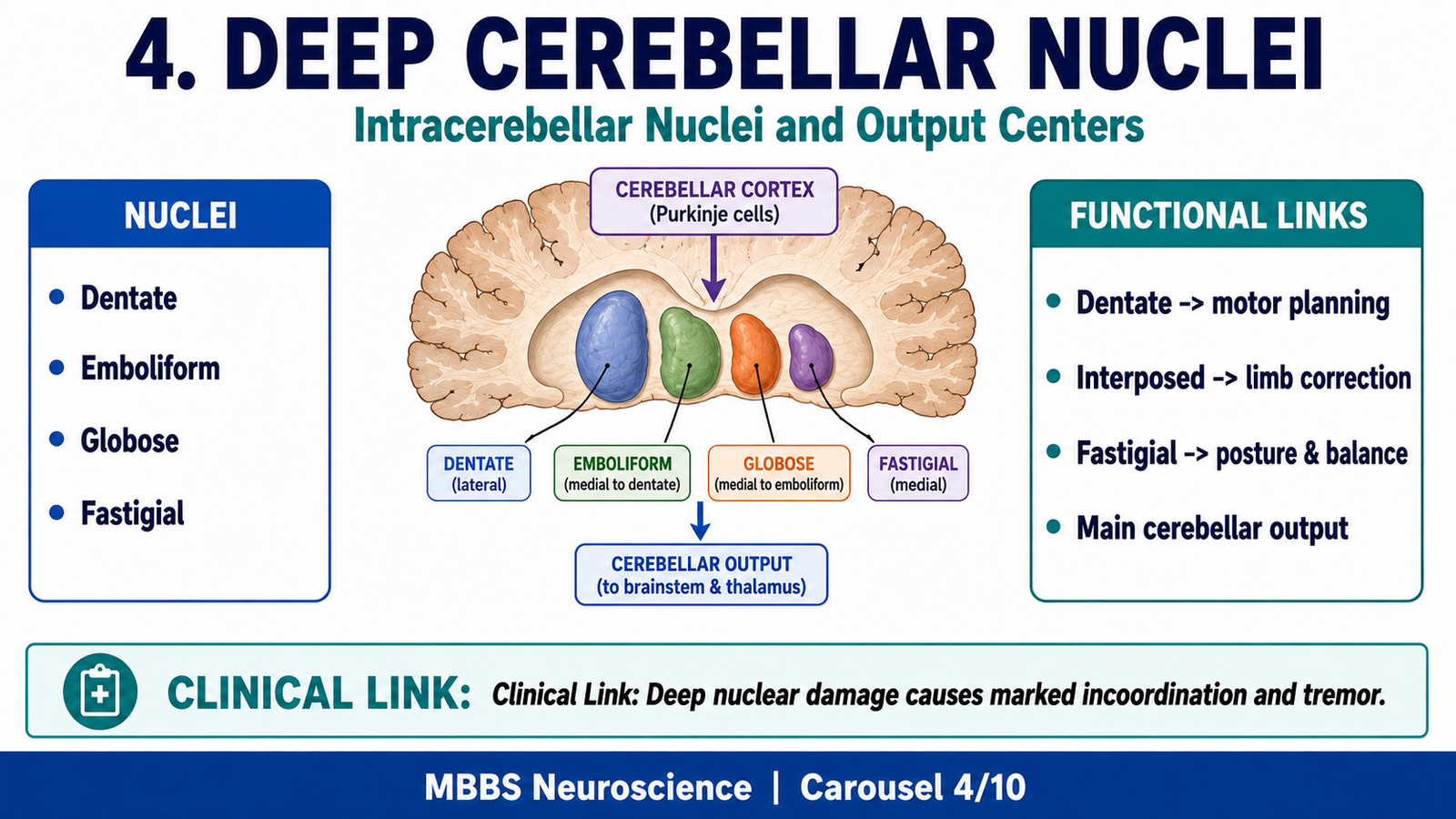
• Deep cerebellar nuclei are the main output centers of the cerebellum.
• The four paired nuclei are dentate, emboliform, globose, and fastigial nuclei.
• Emboliform and globose nuclei are collectively called interposed nuclei.
• Fastigial nucleus is related mainly to vermis and vestibular/postural control.
• Interposed nuclei are related mainly to intermediate zone and limb movement correction.
• Dentate nucleus is related mainly to lateral hemispheres and skilled voluntary movement.
• Purkinje cells inhibit deep nuclei, while mossy and climbing fiber collaterals excite them.
🔬 CONCEPT EXPLAINED
The deep cerebellar nuclei are embedded within the white matter of cerebellum. They are essential because the cerebellar cortex itself does not directly send most final motor signals to the body. Instead, cerebellar cortical processing influences the deep nuclei, and the deep nuclei send the main output signals to brainstem and cerebral motor systems.
There are four major deep nuclei arranged from lateral to medial: dentate, emboliform, globose, and fastigial. A useful memory order is: Don’t Eat Greasy Food — Dentate, Emboliform, Globose, Fastigial. The emboliform and globose nuclei together are called interposed nuclei.
The fastigial nucleus is mainly associated with the vermis and helps regulate posture, balance, axial muscles, and eye movement control through brainstem pathways. The interposed nuclei receive influence from the intermediate cerebellar zone and help correct ongoing limb movements. The dentate nucleus is the largest and is associated with the lateral hemispheres; it participates in planning, timing, and coordination of skilled voluntary movements through pathways to the thalamus and motor cortex.
A key concept is that Purkinje cells are inhibitory. They inhibit deep cerebellar nuclei. At the same time, incoming mossy and climbing fibers send excitatory collaterals to deep nuclei. Therefore, cerebellar output depends on a balance between excitatory input to deep nuclei and inhibitory control from Purkinje cells. This balance allows the cerebellum to fine-tune movement rather than simply excite or suppress muscles.
⚠️ CLINICAL IMPORTANCE
Damage to deep cerebellar nuclei disrupts cerebellar output and produces severe coordination defects. Dentate nucleus involvement affects skilled movement planning and may produce intention tremor. Fastigial involvement may produce truncal instability and balance problems.
5. Histology of Cerebellar Cortex
🧠 CORE
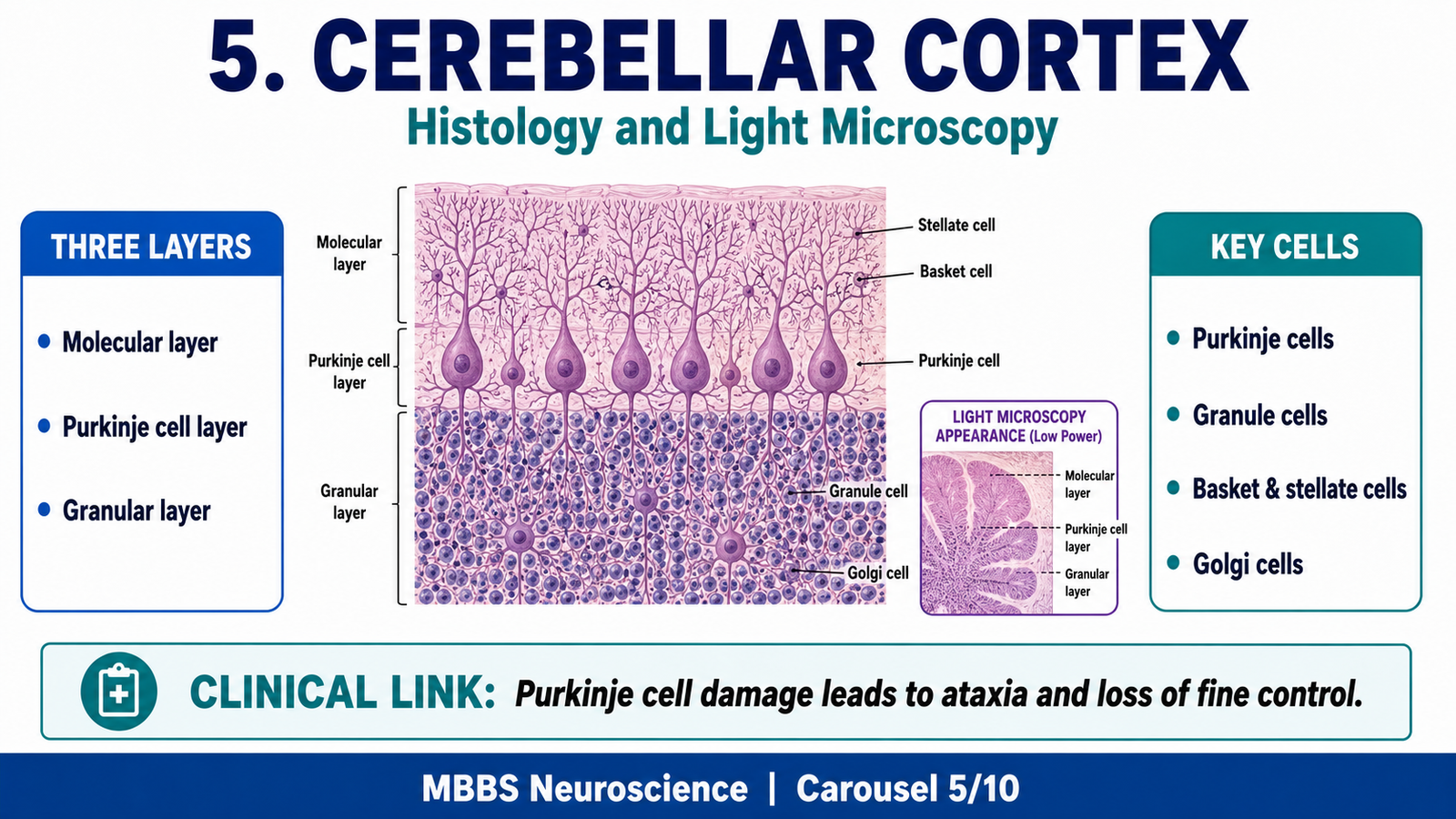
• Cerebellar cortex has three layers: molecular, Purkinje cell, and granular layers.
• The molecular layer is the outer pale layer with few cells and many synaptic connections.
• The Purkinje cell layer contains large flask-shaped Purkinje neurons in a single row.
• The granular layer is densely cellular and contains granule cells and Golgi cells.
• Purkinje cells are the only output neurons of the cerebellar cortex.
• Granule cells are excitatory and give rise to parallel fibers.
• Basket and stellate cells inhibit Purkinje cells.
🔬 CONCEPT EXPLAINED
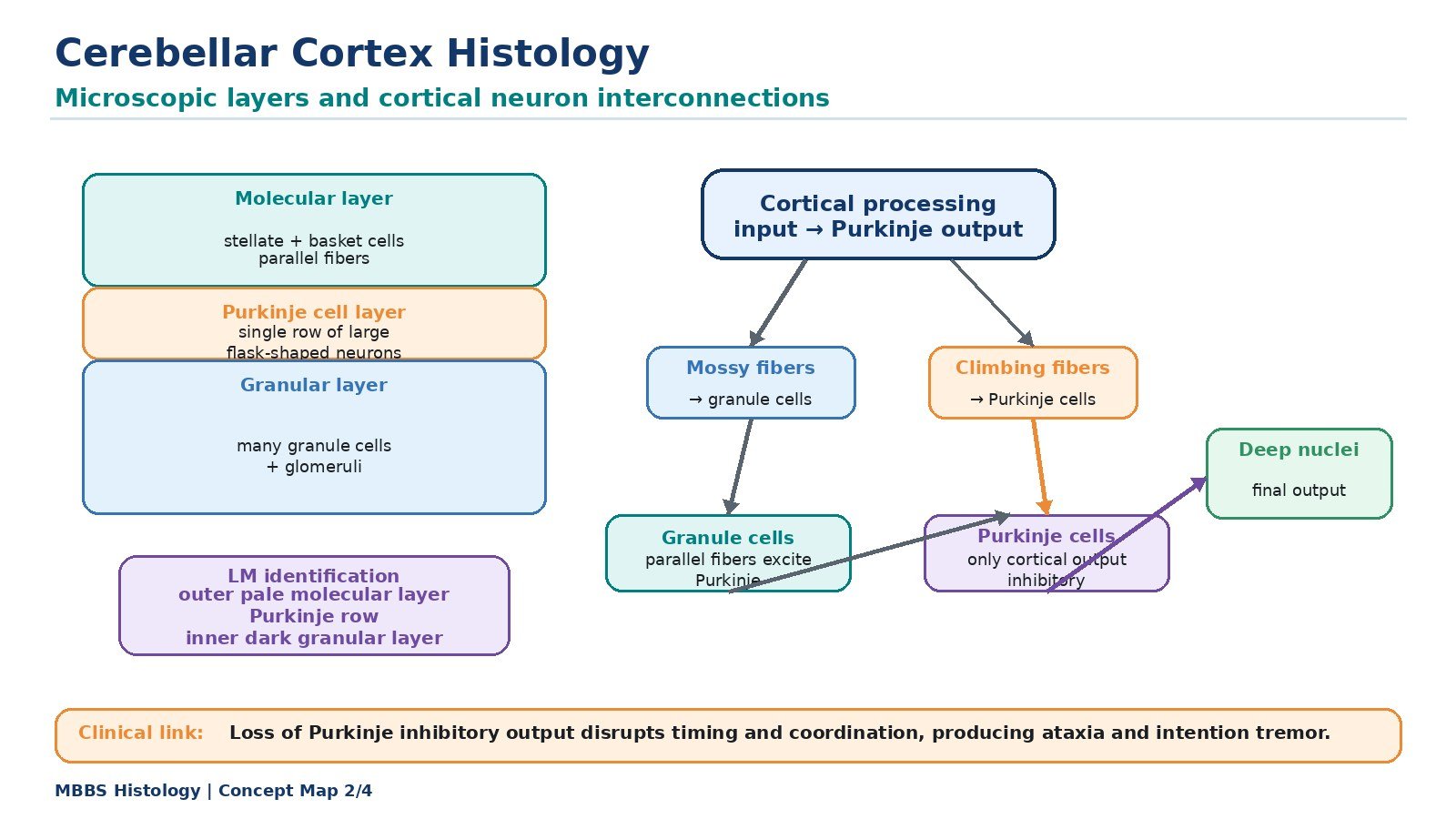
On light microscopy, the cerebellar cortex is recognized by its characteristic three-layered structure. From superficial to deep, these layers are the molecular layer, Purkinje cell layer, and granular layer. Beneath the cortex lies cerebellar white matter.
The molecular layer is the outermost layer and appears pale because it contains relatively few cell bodies. It contains dendrites of Purkinje cells, parallel fibers of granule cells, and inhibitory interneurons such as stellate and basket cells. This layer is important because many synaptic interactions occur here.
The Purkinje cell layer is the most distinctive layer. It contains a single row of large flask-shaped Purkinje cells. These cells have extensive dendritic trees extending into the molecular layer. Purkinje cells are very important because they form the only output pathway from the cerebellar cortex. Their neurotransmitter is inhibitory, mainly GABA, so they inhibit deep cerebellar nuclei and vestibular nuclei.
The granular layer is the deepest cortical layer and appears darkly stained due to numerous small granule cells. Granule cells receive input from mossy fibers and send axons upward into the molecular layer, where they divide into parallel fibers. These parallel fibers excite many Purkinje cell dendrites. Golgi cells in this layer provide inhibitory feedback regulation.
The histological arrangement of cerebellar cortex reflects its function. Inputs enter through mossy and climbing fibers, information is processed through granule cells, interneurons, and Purkinje cells, and the final cortical influence is inhibitory control of deep nuclei. This arrangement allows precise timing, filtering, and correction of motor signals.
⚠️ CLINICAL IMPORTANCE
Purkinje cell damage is clinically important because Purkinje cells regulate cerebellar output. Loss of Purkinje cell inhibition causes abnormal deep nuclear activity, leading to uncoordinated movement, tremor, and ataxia. Alcohol and some degenerative disorders can affect cerebellar cortical neurons, especially in regions involved in gait.
6. Cerebellar Afferent Fibers: Inputs to Cerebellum
🧠 CORE
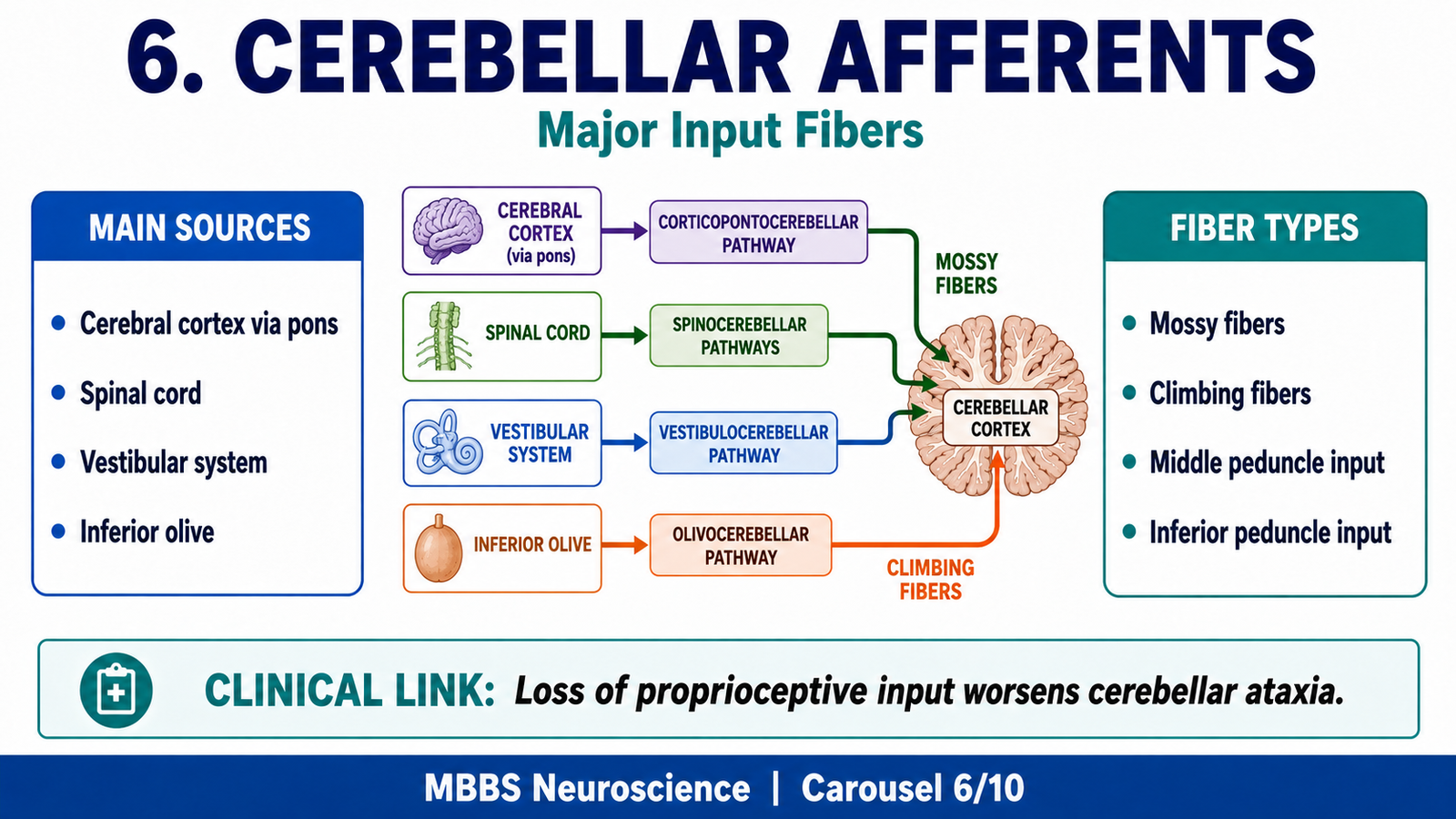
• Cerebellum receives information from cerebral cortex, spinal cord, vestibular system, and brainstem.
• Afferent fibers enter mainly through middle and inferior cerebellar peduncles.
• Mossy fibers are the major afferent type and influence Purkinje cells indirectly.
• Climbing fibers arise from the inferior olivary nucleus and strongly excite Purkinje cells.
• Vestibular inputs help balance and eye movement control.
• Spinocerebellar inputs provide unconscious proprioceptive information.
• Corticopontocerebellar inputs help coordinate planned voluntary movement.
🔬 CONCEPT EXPLAINED
The cerebellum works by receiving continuous information about both intended and actual movements. This information enters through cerebellar afferent fibers. These inputs tell the cerebellum what the cerebral cortex plans to do, what the body is actually doing, and how balance and posture are changing.
One major input pathway is the corticopontocerebellar pathway. Motor and premotor areas of the cerebral cortex send signals to pontine nuclei. Pontine fibers then cross and enter the opposite cerebellar hemisphere through the middle cerebellar peduncle. This pathway allows the cerebellum to receive a copy of planned voluntary movement. The cerebellum can then help plan timing, sequence, and accuracy before movement is fully executed.
Another important input comes from the spinal cord through spinocerebellar tracts. These pathways carry unconscious proprioceptive information from muscles, tendons, and joints. This tells the cerebellum the current position and movement of body parts. By comparing this sensory feedback with the intended motor command, the cerebellum can correct errors during ongoing movement.
The vestibular apparatus and vestibular nuclei send input mainly to the vestibulocerebellum. These inputs inform the cerebellum about head position, acceleration, and balance. This information is essential for equilibrium and coordination of eye movements with head movements.
At the cellular level, cerebellar afferents are mainly of two types: mossy fibers and climbing fibers. Mossy fibers come from many sources, including pontine nuclei, spinal cord, and vestibular nuclei. They excite granule cells, which then influence Purkinje cells through parallel fibers. Climbing fibers arise from the inferior olivary nucleus and form powerful excitatory synapses with Purkinje cells. Climbing fibers are especially important for error signals and motor learning.
Therefore, cerebellar afferents provide the sensory and motor information needed for comparison, correction, and learning.
⚠️ CLINICAL IMPORTANCE
Damage to cerebellar afferent pathways prevents the cerebellum from receiving accurate feedback. As a result, the patient may perform movements with poor timing and incorrect range. Loss of proprioceptive input can worsen ataxia because the cerebellum cannot properly compare intended and actual movement.
7. Cerebellar Efferent Fibers: Outputs from Cerebellum
🧠 CORE
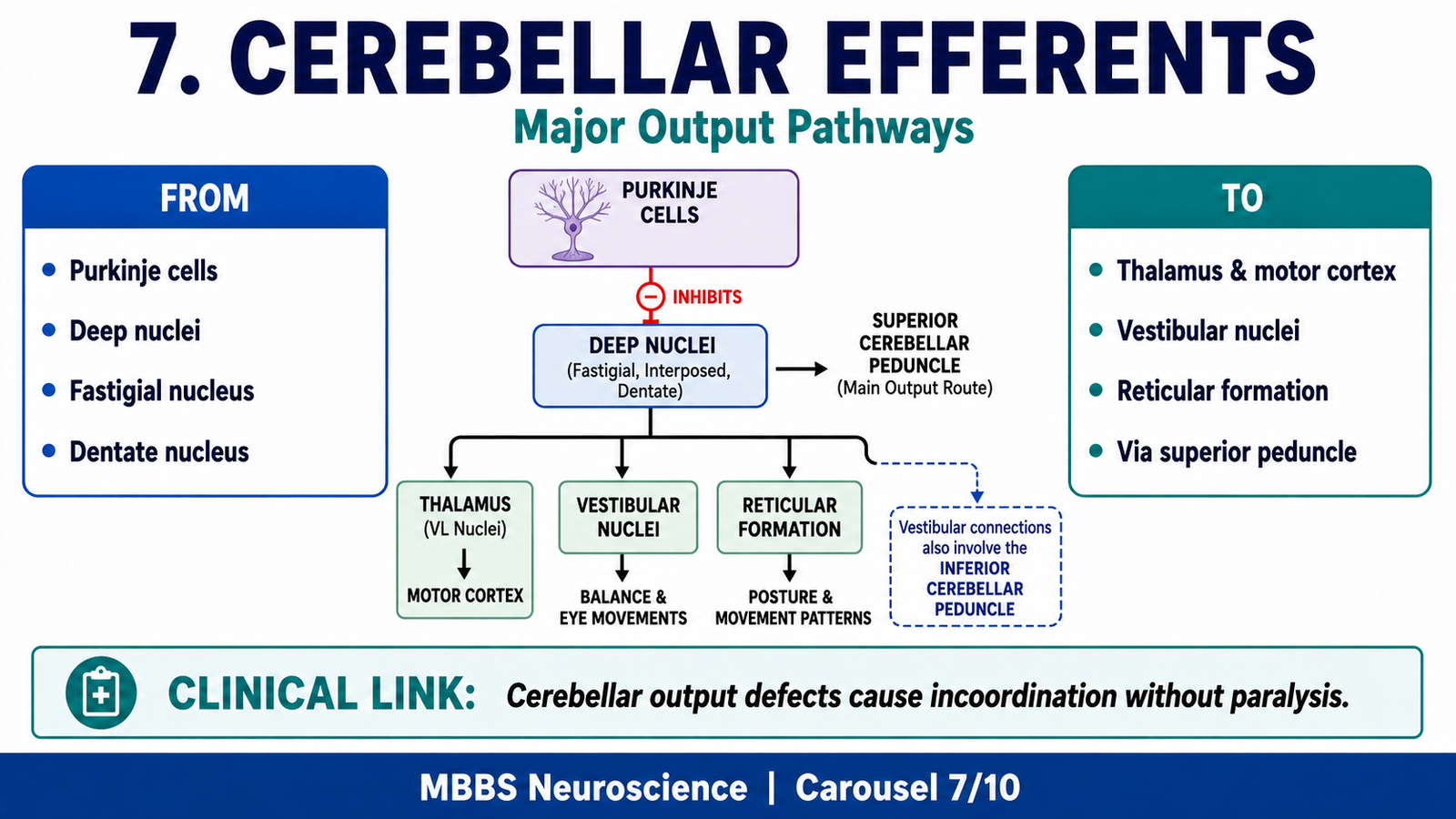
• Cerebellar outputs mainly arise from deep cerebellar nuclei.
• Purkinje cells inhibit deep nuclei and regulate their output.
• Superior cerebellar peduncle carries major outputs to thalamus and motor cortex.
• Fastigial nucleus outputs influence vestibular and reticular pathways.
• Interposed nuclei help correct ongoing limb movements.
• Dentate nucleus outputs influence motor planning through thalamus and cortex.
• Cerebellar output modifies motor activity but does not directly cause muscle contraction.
🔬 CONCEPT EXPLAINED
After processing input information, the cerebellum sends corrective signals to motor control systems. Most cerebellar output begins in the deep cerebellar nuclei, except some vestibulocerebellar outputs that may go directly from Purkinje cells to vestibular nuclei.
The fastigial nucleus sends outputs to vestibular nuclei and reticular formation. These brainstem centers influence vestibulospinal and reticulospinal tracts, which control posture, balance, and axial muscles. Therefore, fastigial output is important for standing, walking, and maintaining equilibrium.
The interposed nuclei send outputs through the superior cerebellar peduncle to motor-related brainstem and thalamic areas. These outputs help regulate ongoing limb movements. If a movement is deviating from its target, the cerebellum uses these pathways to adjust force, timing, and direction.
The dentate nucleus sends output mainly through the superior cerebellar peduncle to the contralateral thalamus, which then projects to motor and premotor cortices. This circuit allows the cerebellum to influence planning and initiation of skilled voluntary movements.
An important principle is that cerebellar output eventually influences the same side of the body. Although many cerebellar pathways cross, motor pathways may cross again before reaching muscles. This double-crossed arrangement explains why cerebellar lesions usually produce ipsilateral signs.
⚠️ CLINICAL IMPORTANCE
Because cerebellar output modifies motor programs rather than directly producing movement, cerebellar lesions cause abnormal coordination rather than paralysis. The patient may have normal strength but cannot control the accuracy and smoothness of movement.
8. Interconnections of Neurons of Cerebellar Cortex
🧠 CORE
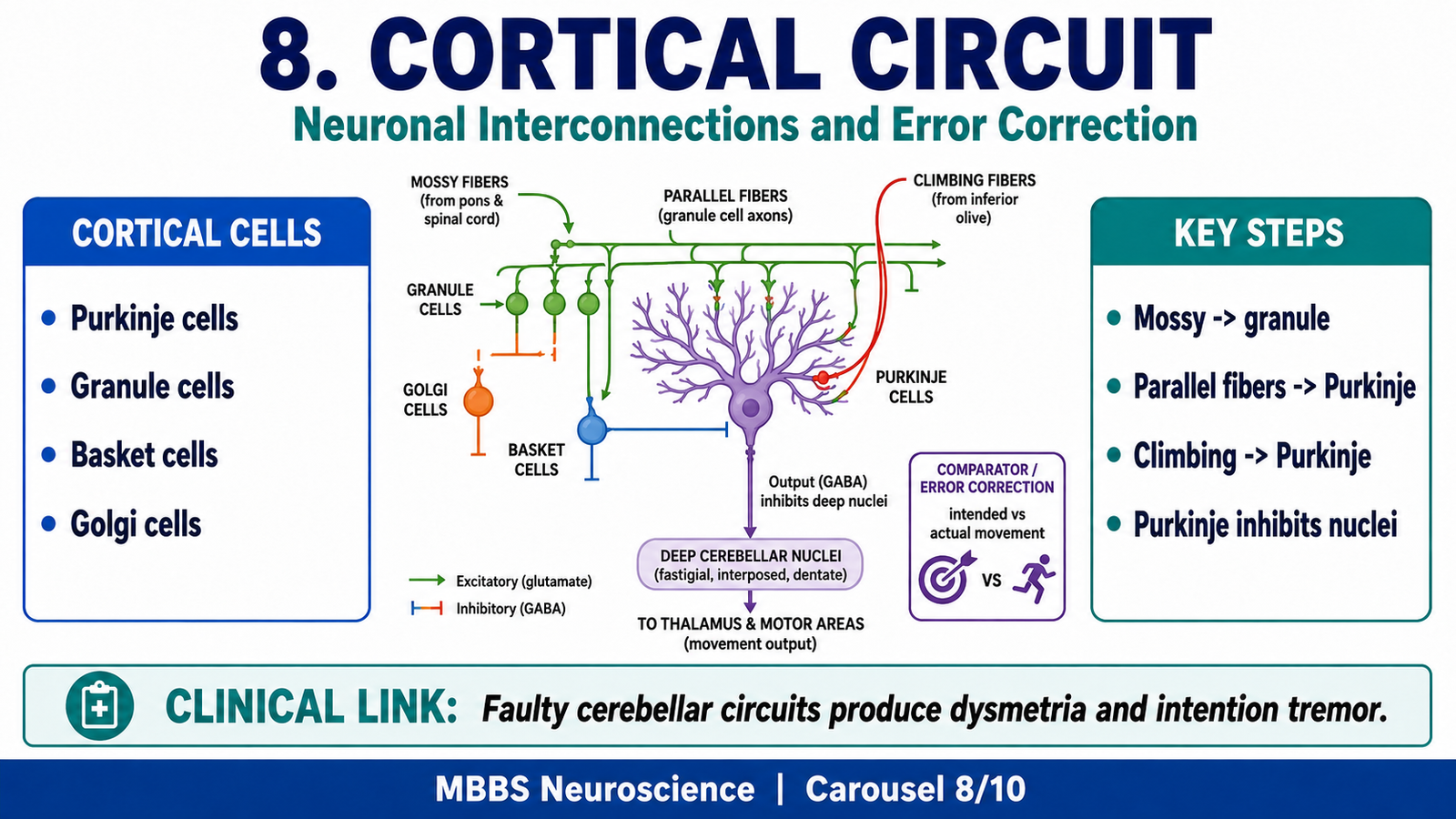
• Cerebellar cortical processing depends on Purkinje cells, granule cells, Golgi cells, basket cells, and stellate cells.
• Mossy fibers excite granule cells.
• Granule cells form parallel fibers that excite Purkinje cells.
• Climbing fibers strongly excite Purkinje cells.
• Purkinje cells inhibit deep cerebellar nuclei.
• Basket and stellate cells inhibit Purkinje cells.
• Golgi cells regulate granule cell activity through feedback inhibition.
🔬 CONCEPT EXPLAINED
The cerebellar cortex works like a highly organized processing unit. Its job is to receive large amounts of input, compare signals, detect errors, and regulate deep nuclear output.
The most important output neuron of the cerebellar cortex is the Purkinje cell. Purkinje cells receive excitatory input from parallel fibers and climbing fibers. However, their output is inhibitory. They project to deep cerebellar nuclei and reduce their activity. This inhibitory control is essential because it allows fine adjustment of cerebellar output.
Mossy fibers bring information from many sources, including spinal cord, pontine nuclei, and vestibular nuclei. They excite granule cells in the granular layer. Granule cell axons ascend to the molecular layer and split into parallel fibers, which run across Purkinje cell dendrites. This arrangement allows one mossy fiber input to influence many Purkinje cells.
Climbing fibers arise from the inferior olivary nucleus. Each climbing fiber forms strong synaptic contact with Purkinje cells. These fibers are especially important in signaling motor errors. When a movement is inaccurate, climbing fiber activity helps modify cerebellar circuits so that future movements become more accurate. This is the basis of cerebellar motor learning.
Inhibitory interneurons refine this processing. Basket cells and stellate cells inhibit Purkinje cells in the molecular layer. Golgi cells inhibit granule cells in the granular layer. These inhibitory mechanisms prevent excessive excitation and sharpen the timing and precision of cerebellar signals.
Thus, cerebellar cortex functions through a balance of excitation and inhibition. This balance allows precise control over deep nuclei and therefore precise control over movement.
⚠️ CLINICAL IMPORTANCE
If cerebellar cortical circuits fail, movement becomes poorly timed and poorly scaled. The patient overshoots or undershoots targets, develops intention tremor, and cannot perform rapid alternating movements smoothly.
9. Functional Circuits of Cerebellum
🧠 CORE
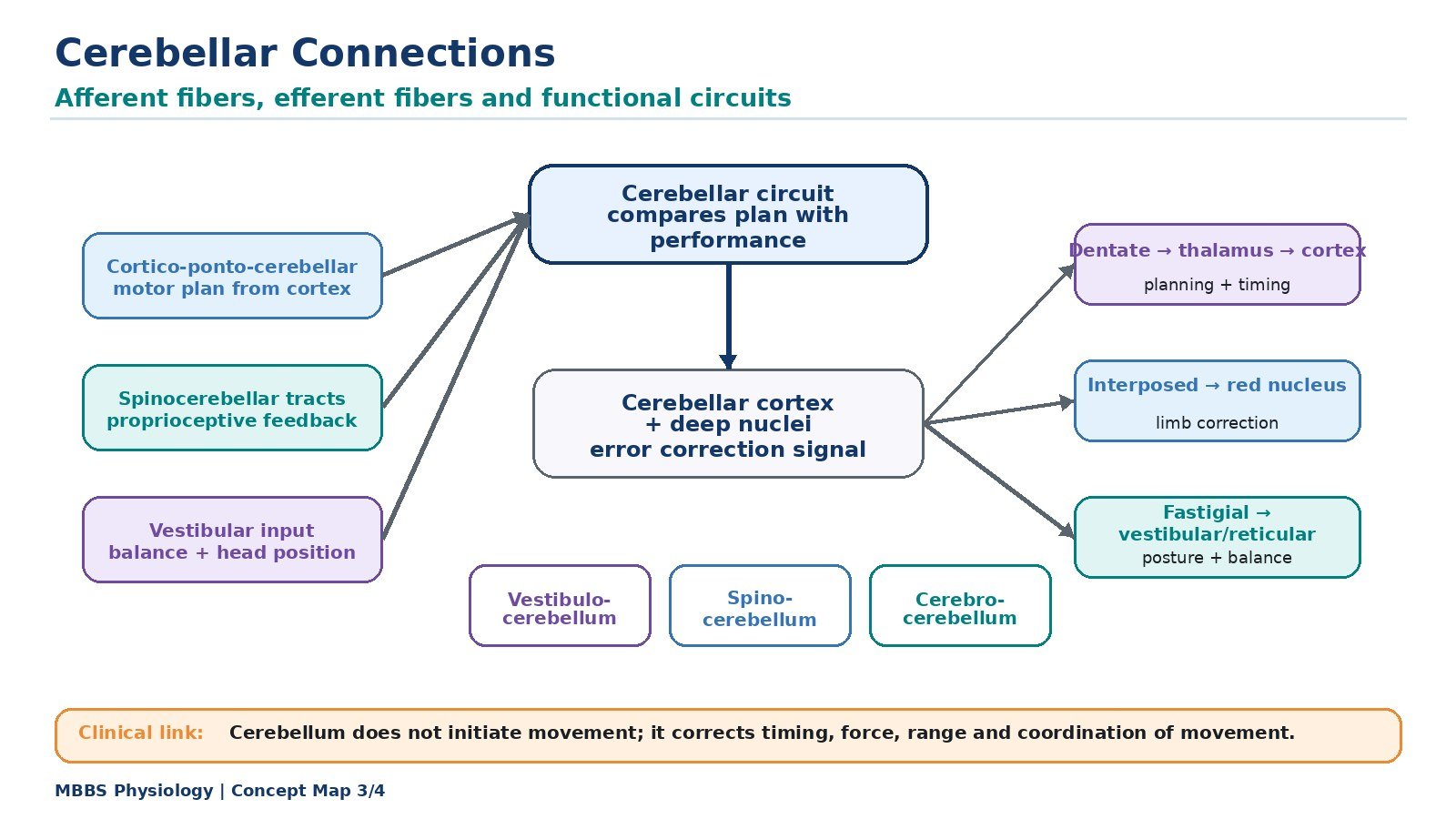
• Cerebellar circuits compare intended movement with actual movement.
• Motor plan information reaches cerebellum from cerebral cortex.
• Sensory feedback reaches cerebellum from spinal cord and vestibular system.
• Cerebellar cortex processes signals through Purkinje cells.
• Deep nuclei send corrective output to motor cortex and brainstem.
• Circuits operate continuously during posture and movement.
• These circuits are essential for motor learning and automatic correction.
🔬 CONCEPT EXPLAINED
The cerebellum functions through comparison circuits. The cerebral cortex sends a motor command to the spinal cord to produce movement. At the same time, a copy of that motor plan is sent to the cerebellum through pontine nuclei. This is called an internal copy of intended movement. The spinal cord and sensory receptors then send information about the actual movement being performed. The cerebellum compares these two streams of information.
If the intended movement and actual movement match, the cerebellum supports smooth continuation of the activity. If there is a mismatch, the cerebellum generates corrective output. These corrections pass through deep cerebellar nuclei to the thalamus, motor cortex, vestibular nuclei, reticular formation, and other motor control centers.
This mechanism is especially important during rapid movement. Many voluntary movements occur too quickly for conscious correction. The cerebellum predicts movement errors and makes rapid automatic adjustments. This predictive function allows smooth walking, accurate reaching, coordinated speech, and precise hand movements.
Motor learning also depends on cerebellar circuits. Repeated practice modifies cerebellar synapses so that movements become smoother and more automatic. For example, learning to write, play a musical instrument, or perform a clinical procedure requires cerebellar timing and error correction.
⚠️ CLINICAL IMPORTANCE
When functional circuits fail, patients lose automatic correction. Movements become irregular, jerky, delayed, and inaccurate. This explains why cerebellar patients often decompose a smooth movement into several small movements.
10. Functional Differences Between Vermis and Cerebellar Hemispheres
🧠 CORE
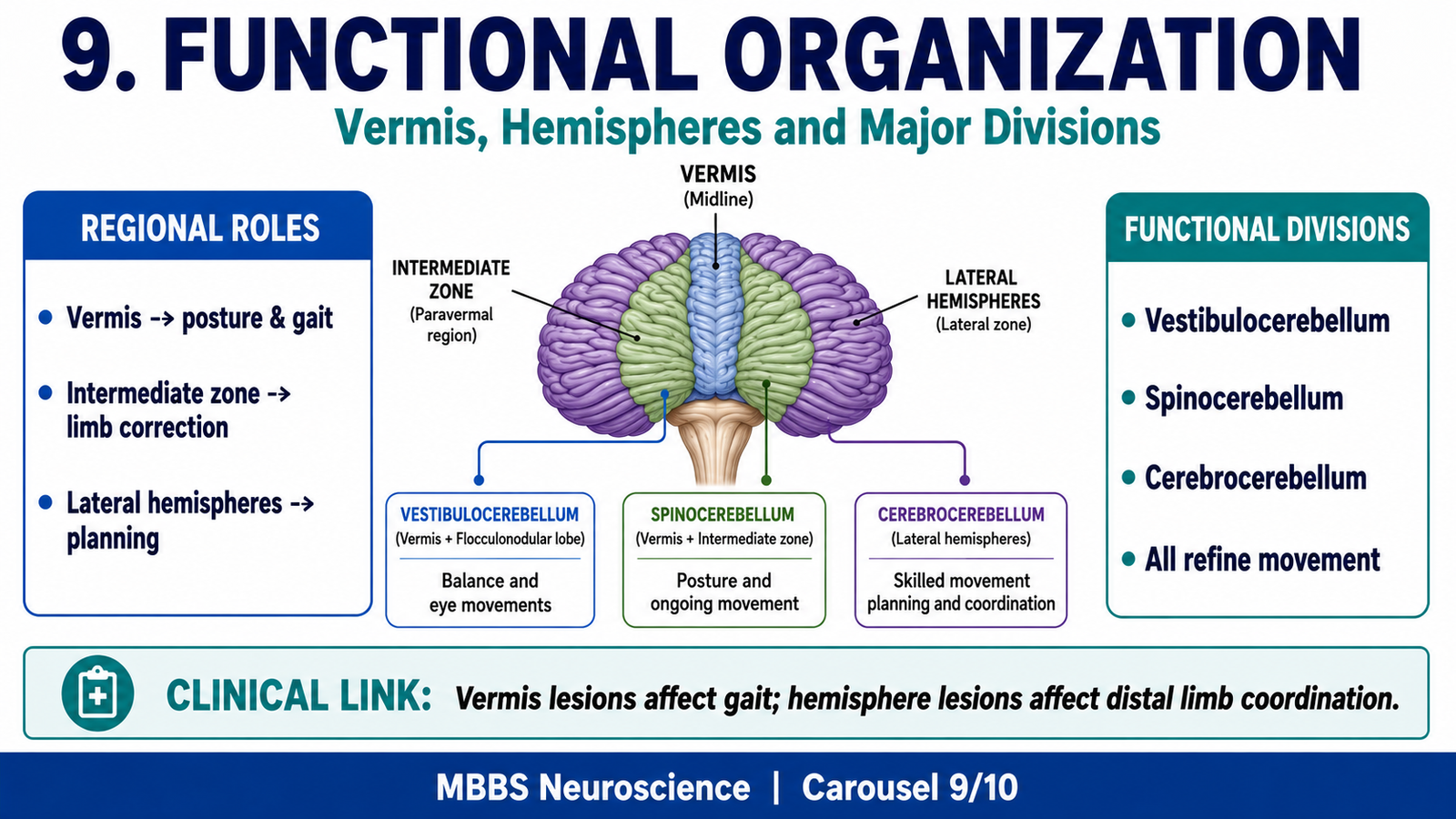
• Vermis controls axial muscles, posture, gait, and trunk stability.
• Intermediate zone controls ongoing movements of distal limbs.
• Lateral hemispheres help plan and coordinate skilled voluntary movements.
• Vermis is closely related to fastigial nucleus.
• Intermediate zone is related to interposed nuclei.
• Lateral hemispheres are related to dentate nucleus.
• Lesions produce different clinical patterns depending on the region involved.
🔬 CONCEPT EXPLAINED
The cerebellum has a medial-to-lateral functional organization. The vermis lies in the midline and controls muscles near the body axis. These include muscles of the trunk, neck, and proximal limbs. Since these muscles are essential for posture and balance, vermal lesions commonly produce truncal instability and a wide-based gait.
The intermediate zone lies lateral to the vermis and is involved in control of limb movements, especially during ongoing motion. It receives sensory feedback from the spinal cord and helps correct errors in movement as they occur. This region is important when a person reaches for an object and must adjust the movement during the action.
The lateral hemispheres are involved in planning and coordination of complex skilled movements. They communicate heavily with the cerebral cortex through pontine nuclei and thalamus. This region helps determine timing, sequence, and smooth execution of voluntary movement before and during performance.
Therefore, the cerebellum is organized according to body function. The midline region stabilizes the body; the intermediate region adjusts limb movement; the lateral region plans and coordinates skilled motor activity.
⚠️ CLINICAL IMPORTANCE
Vermis lesions cause truncal ataxia and gait imbalance. Hemisphere lesions cause ipsilateral limb ataxia, dysmetria, intention tremor, and difficulty with finger-nose testing. This regional distinction is commonly tested in MBBS examinations.
11. Functions of Vestibulocerebellum
🧠 CORE
• Vestibulocerebellum consists mainly of flocculonodular lobe.
• It receives input from vestibular apparatus and vestibular nuclei.
• It helps maintain equilibrium and balance.
• It coordinates eye movements with head movements.
• It regulates vestibulo-ocular reflexes.
• It influences vestibular nuclei and vestibulospinal tracts.
• Lesions cause nystagmus, vertigo, and imbalance.
🔬 CONCEPT EXPLAINED
The vestibulocerebellum is the oldest functional part of the cerebellum. It is closely connected with the vestibular system, which detects head position and movement. When the head moves, vestibular receptors send information to vestibular nuclei and cerebellum. The vestibulocerebellum uses this information to maintain balance and coordinate eye movements.
One of its important functions is control of the vestibulo-ocular reflex. When the head turns in one direction, the eyes must move in the opposite direction to keep vision stable. The vestibulocerebellum helps adjust this reflex so that visual fixation remains accurate.
It also influences vestibulospinal pathways, which help maintain posture and balance by adjusting extensor muscle tone. This becomes important during standing and walking because the body must continuously correct small shifts in position.
⚠️ CLINICAL IMPORTANCE
Damage to vestibulocerebellum causes vertigo, nystagmus, loss of balance, and difficulty standing or walking. Patients may stagger and have difficulty maintaining gaze during head movement.
12. Functions of Spinocerebellum
🧠 CORE
• Spinocerebellum includes vermis and intermediate cerebellar zones.
• It receives unconscious proprioceptive input from spinal cord.
• It controls posture, gait, muscle tone, and ongoing limb movements.
• Vermis mainly controls axial and proximal muscles.
• Intermediate zone controls distal limb movement correction.
• It compares intended movement with actual movement.
• Lesions cause gait ataxia, limb ataxia, hypotonia, and dysmetria.
🔬 CONCEPT EXPLAINED
The spinocerebellum receives continuous sensory feedback from muscles, tendons, and joints. This feedback tells the cerebellum what is actually happening during movement. For example, when a person walks, the spinocerebellum receives information about limb position, muscle stretch, and joint movement.
The spinocerebellum compares this actual movement information with the intended motor command. If the foot placement, limb direction, or muscle force is incorrect, cerebellar circuits send corrective signals through deep nuclei and brainstem pathways. This correction happens automatically and rapidly.
The vermis helps maintain posture and gait by controlling axial and proximal muscles. The intermediate zone helps adjust distal limb movements, such as reaching, grasping, and finger movements. This division is especially important during movements that must be continuously corrected while they are being performed.
⚠️ CLINICAL IMPORTANCE
Spinocerebellar dysfunction causes ataxic gait, hypotonia, intention tremor, dysmetria, and difficulty performing rapid alternating movements. Patients may walk with a wide base because they cannot maintain stable posture.
13. Functions of Cerebrocerebellum
🧠 CORE
• Cerebrocerebellum consists mainly of lateral cerebellar hemispheres.
• It receives input from cerebral cortex through pontine nuclei.
• It helps plan and time skilled voluntary movements.
• It coordinates sequence, force, and direction of movement.
• It is important for motor learning and learned skilled activity.
• It influences motor cortex through dentate nucleus and thalamus.
• Lesions cause intention tremor, dysmetria, and decomposition of movement.
🔬 CONCEPT EXPLAINED
The cerebrocerebellum is highly developed in humans because humans perform complex skilled voluntary movements. It receives information from the cerebral cortex through the corticopontocerebellar pathway. This information represents planned movement before or during execution.
The cerebrocerebellum helps plan the timing, sequence, and force of movement. For example, when a student writes with a pen, many small muscles must contract in a precise order and with correct force. The cerebrocerebellum helps coordinate this activity so that movement is smooth and accurate.
It also contributes to motor learning. With repeated practice, cerebellar circuits improve the accuracy and automaticity of movement. This is why skills become smoother after repetition.
The output of cerebrocerebellum passes through the dentate nucleus, superior cerebellar peduncle, thalamus, and motor cortex. Through this route, the cerebellum influences cortical motor planning.
⚠️ CLINICAL IMPORTANCE
Cerebrocerebellar lesions produce problems in skilled voluntary movement. The patient may overshoot a target, show intention tremor, break a movement into separate parts, and have difficulty with rapid alternating movements.
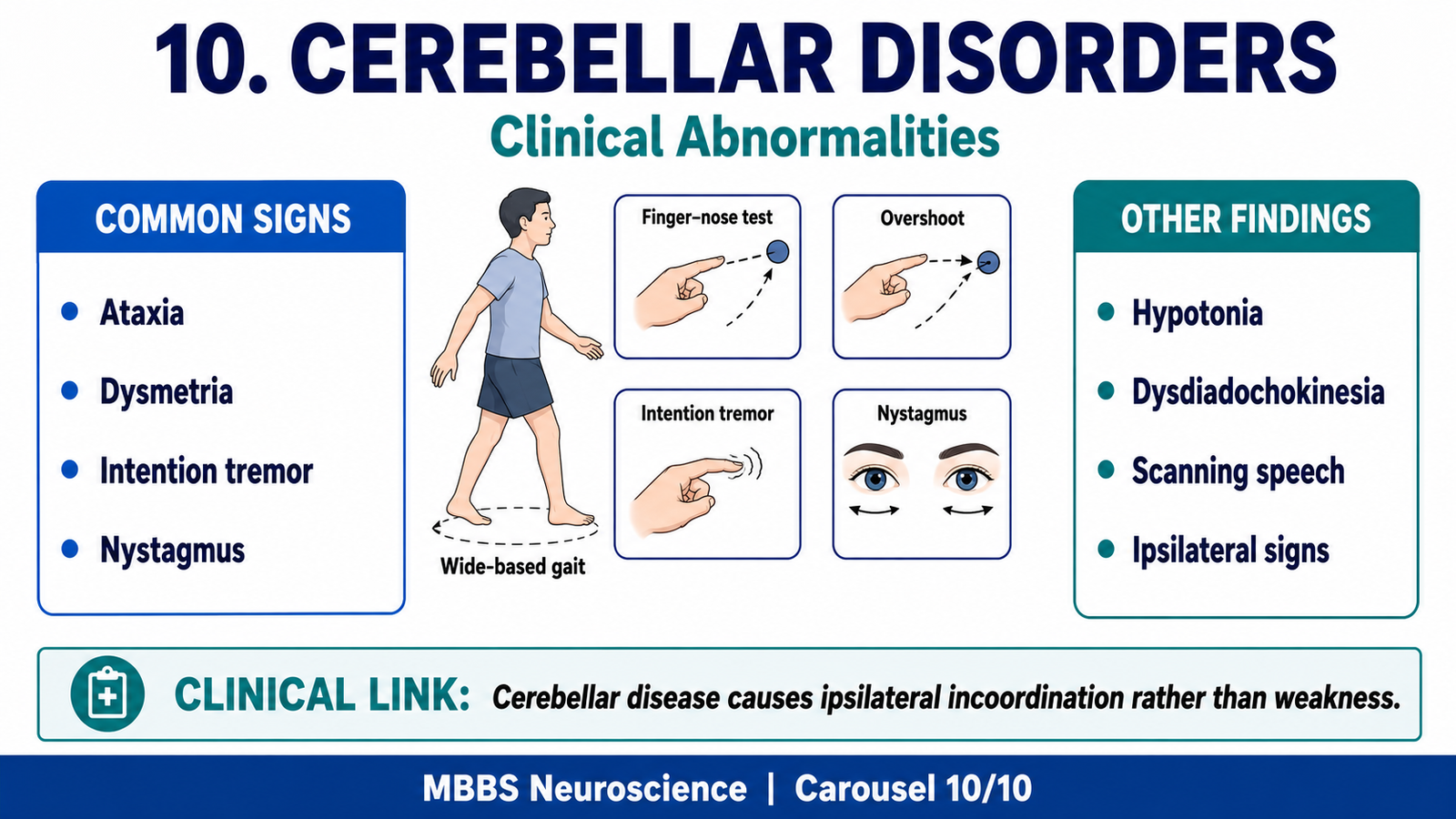
14. Clinical Abnormalities of Cerebellum
🧠 CORE
• Cerebellar lesions cause ipsilateral signs.
• Ataxia is the main feature of cerebellar dysfunction.
• Dysmetria causes overshooting or undershooting of target.
• Intention tremor worsens near the target.
• Nystagmus occurs especially with vestibulocerebellar involvement.
• Hypotonia occurs due to loss of cerebellar facilitation of muscle tone.
• Scanning speech occurs due to incoordination of speech muscles.
🔬 CONCEPT EXPLAINED
Cerebellar disease produces abnormalities of coordination rather than paralysis. Since the cerebellum normally smooths movement, its failure causes irregular and inaccurate movement. The most important clinical feature is ataxia, which means incoordination of voluntary movement.
Dysmetria occurs because the cerebellum cannot correctly judge the range of movement. The patient may overshoot or undershoot a target during finger-nose testing. Past pointing is a related sign in which the patient points beyond the intended target.
Intention tremor occurs during purposeful movement and becomes more prominent as the target is approached. This happens because the cerebellum cannot progressively correct movement errors near the target. Unlike resting tremor, intention tremor is most visible during action.
Dysdiadochokinesia is difficulty performing rapid alternating movements, such as rapidly pronating and supinating the hand. It occurs because cerebellar timing and sequencing are impaired.
Hypotonia occurs because cerebellar influence on motor pathways helps maintain normal tone. When this influence is lost, resistance to passive movement decreases.
Nystagmus occurs when vestibulocerebellar control of eye movements is impaired. The eyes show rhythmic involuntary movements because gaze stabilization is disturbed.
Scanning speech occurs due to incoordination of muscles involved in speech. Speech becomes slow, irregular, and broken into separated syllables.
A key examination concept is that cerebellar signs are usually ipsilateral. This is because cerebellar pathways often cross twice before influencing the body.
⚠️ CLINICAL IMPORTANCE
Cerebellar disorders are commonly tested through bedside signs: finger-nose test, heel-shin test, rapid alternating movements, gait examination, rebound phenomenon, speech assessment, and eye movement examination. The most important clinical concept is: cerebellar lesion = coordination problem, not primary paralysis.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Cerebellar Folia → Increased Cortical Surface Area → Large-Scale Motor Processing
The folded folia increase the surface area of cerebellar cortex. This allows the cerebellum to process huge amounts of sensory and motor information required for continuous movement correction.
Vermis → Axial Muscle Control → Stable Posture and Gait
The vermis is connected with fastigial nucleus and brainstem motor pathways. This organization allows control of trunk and proximal muscles, producing balance, posture, and coordinated walking.
Intermediate Zone → Limb Movement Correction → Accurate Ongoing Movement
The intermediate zone receives spinal feedback and influences interposed nuclei. It helps correct movements while they are happening, especially movements of limbs.
Lateral Hemispheres → Dentate Nucleus → Skilled Voluntary Movement Planning
The lateral hemispheres communicate with the cerebral cortex through pontine nuclei and thalamus. This supports planning, timing, and coordination of skilled voluntary movements.
Purkinje Cells → Inhibitory Output → Fine Control of Deep Nuclei
Purkinje cells inhibit deep cerebellar nuclei. This inhibition prevents excessive or poorly timed motor output and allows precise regulation of movement.
Granular Layer → Granule Cells and Parallel Fibers → Wide Distribution of Input
Granule cells distribute mossy fiber information widely through parallel fibers. This allows many Purkinje cells to participate in processing movement information.
Vestibulocerebellum → Vestibular Nuclei → Balance and Eye Movement Control
The flocculonodular lobe works with vestibular nuclei to maintain equilibrium and stabilize gaze during head movement.
🩺 5️⃣ Clinical Correlation
1. Cerebellar Ataxia
Cerebellar ataxia means incoordination due to cerebellar dysfunction. The patient may have normal power but cannot perform smooth and accurate movements. Gait becomes wide-based and unsteady because posture and balance correction are impaired.
2. Dysmetria and Past Pointing
Dysmetria occurs when the cerebellum cannot control the range of movement. The patient overshoots or undershoots the target. This is commonly tested by the finger-nose test.
3. Intention Tremor
Intention tremor appears during voluntary movement and worsens near the target. It occurs because the cerebellum cannot make progressive corrections during purposeful movement.
4. Dysdiadochokinesia
This is inability to perform rapid alternating movements smoothly. It occurs because cerebellar timing and sequencing of agonist and antagonist muscles are impaired.
5. Nystagmus
Nystagmus occurs especially in vestibulocerebellar lesions. The cerebellum fails to regulate vestibular control of eye movements, causing rhythmic involuntary eye oscillations.
6. Hypotonia
Cerebellar lesions can reduce muscle tone. This happens because cerebellar facilitation of motor pathways is reduced, causing decreased resistance to passive movement.
7. Scanning Speech
Speech requires precise timing of respiratory, laryngeal, and oral muscles. Cerebellar dysfunction disrupts this coordination, producing slow, irregular, broken speech.
8. Ipsilateral Cerebellar Signs
Cerebellar lesions usually produce signs on the same side of the body. This occurs because cerebellar output pathways commonly cross twice before influencing muscles.
📌 6️⃣ Summary Points
- The cerebellum coordinates movement but does not initiate voluntary movement.
- Cerebellar damage causes incoordination, not primary paralysis.
- The three anatomical lobes are anterior, posterior, and flocculonodular lobes.
- The three physiological divisions are vestibulocerebellum, spinocerebellum, and cerebrocerebellum.
- Vermis controls posture, gait, and axial muscles.
- Cerebellar hemispheres coordinate skilled voluntary limb movements.
- Deep cerebellar nuclei are dentate, emboliform, globose, and fastigial.
- Purkinje cells are the only output neurons of cerebellar cortex and are inhibitory.
- Cerebellar cortex has three layers: molecular, Purkinje cell, and granular layers.
- Mossy fibers act mainly through granule cells and parallel fibers.
- Climbing fibers arise from the inferior olivary nucleus and are important for motor error learning.
- Classic cerebellar signs include ataxia, dysmetria, intention tremor, nystagmus, hypotonia, dysdiadochokinesia, and scanning speech.