
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
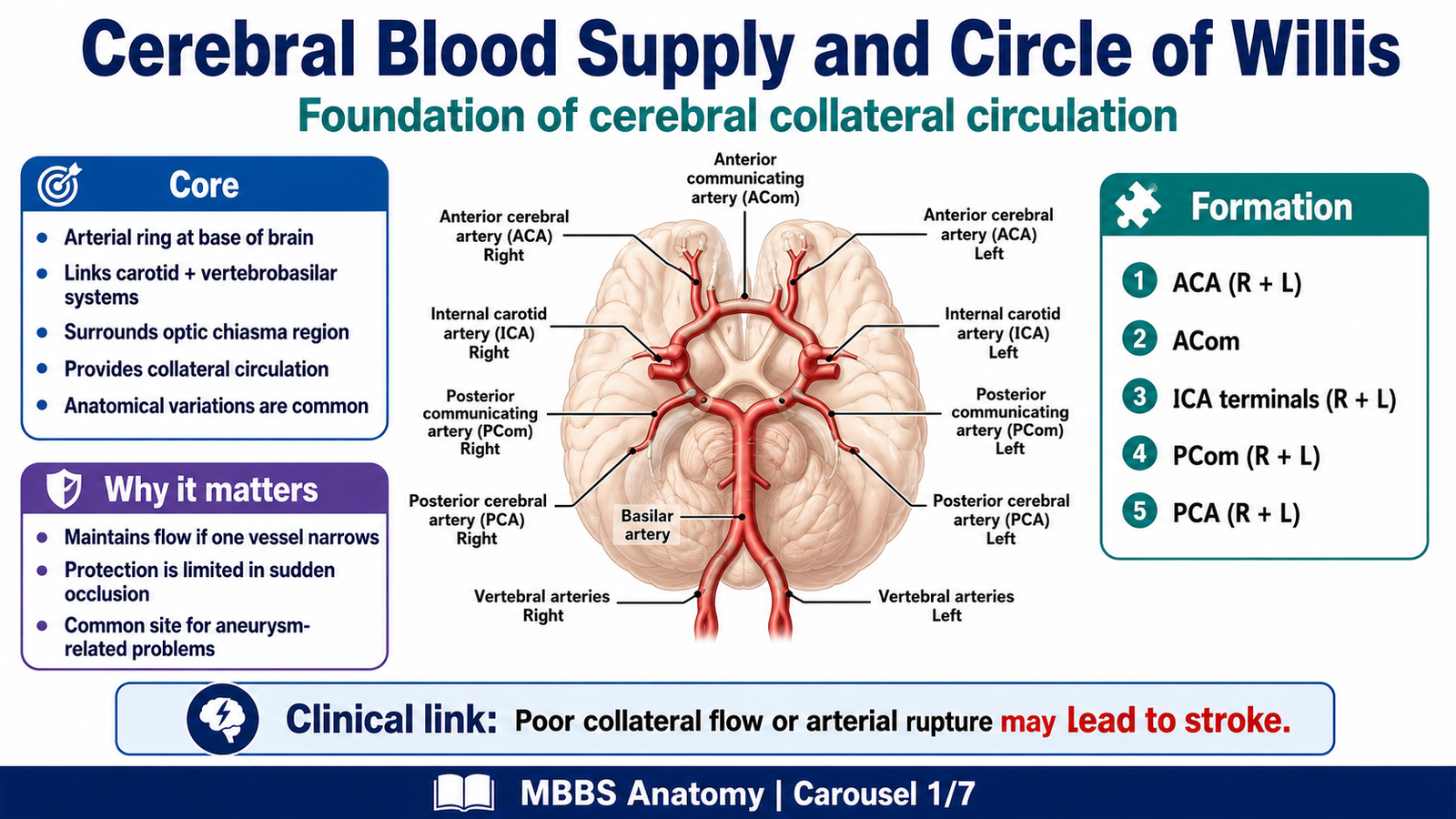
Stroke is one of the most important causes of sudden neurological disability and death. In 2nd Year MBBS, this topic is mainly studied through neuroanatomy, especially the arterial supply of the brain and the Circle of Willis. The Circle of Willis is located at the base of the brain, around the optic chiasma, infundibulum, and interpeduncular fossa. It connects the internal carotid and vertebrobasilar arterial systems.
Clinically, stroke becomes important because blockage or rupture of cerebral vessels can damage the motor cortex, internal capsule, or corticospinal tract, leading to hemiplegia, which means paralysis of one side of the body. Understanding vascular territories helps students explain why a patient may develop weakness of the face, arm, or leg depending on the site of arterial involvement. This topic also integrates risk factors, prevention, clinical features, investigations, and basic differentiation between ischemic and hemorrhagic stroke.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Stroke: Sudden onset of focal neurological deficit due to interruption of blood supply to part of the brain or bleeding into brain tissue.
- Cerebrovascular disease: Disease affecting blood vessels supplying the brain.
- Ischemic stroke: Stroke due to blockage of an artery causing reduced blood flow and infarction.
- Hemorrhagic stroke: Stroke due to rupture of a blood vessel causing bleeding into brain tissue or around the brain.
- Hemiplegia: Complete paralysis of one side of the body.
- Hemiparesis: Weakness of one side of the body.
- Circle of Willis: Arterial anastomotic circle at the base of the brain connecting anterior and posterior cerebral circulations.
- Vascular territory: Area of brain supplied by a specific artery.
- Collateral circulation: Alternative pathway of blood flow when a main artery is narrowed or blocked.
Essential Terminology
- Internal carotid artery: Major artery supplying anterior circulation of brain.
- Vertebral arteries: Arteries that unite to form basilar artery and supply posterior circulation.
- Anterior cerebral artery: Supplies medial surface of cerebral hemisphere.
- Middle cerebral artery: Supplies lateral surface of cerebral hemisphere.
- Posterior cerebral artery: Supplies occipital lobe and inferior temporal lobe.
- Anterior communicating artery: Connects right and left anterior cerebral arteries.
- Posterior communicating artery: Connects internal carotid artery with posterior cerebral artery.
- Corticospinal tract: Major descending motor pathway for voluntary movement.
- Upper motor neuron lesion: Lesion affecting motor cortex or descending motor pathways before anterior horn cell.
Basic Overview
- The brain needs continuous oxygen and glucose supply.
- Cerebral arteries supply specific anatomical regions.
- The Circle of Willis provides a potential collateral pathway.
- Stroke occurs when cerebral blood flow is blocked or bleeding damages brain tissue.
- Hemiplegia commonly results from lesions of motor cortex, internal capsule, or corticospinal tract.
- Prevention focuses on controlling risk factors such as hypertension, diabetes, smoking, obesity, and dyslipidemia.
🔹 3️⃣ Core Learning — Curriculum Coverage
A. Cerebral Blood Supply and Formation of Circle of Willis
🧠 CORE
- The Circle of Willis is an arterial circle located at the base of the brain.
- It connects the internal carotid system with the vertebrobasilar system.
- It is formed by anterior cerebral arteries, anterior communicating artery, internal carotid arteries, posterior communicating arteries, and posterior cerebral arteries.
- It surrounds important basal structures such as the optic chiasma, infundibulum, and interpeduncular region.
- Its main anatomical importance is collateral circulation.
- Its clinical importance is seen in stroke, aneurysm, and vascular territory lesions.
- Although it provides collateral potential, it may not completely prevent stroke if blockage is sudden or severe.
🔬 CONCEPT EXPLAINED
To understand stroke anatomically, students must first understand how blood reaches the brain. The brain receives arterial supply from two major systems: the internal carotid arteries anteriorly and the vertebral arteries posteriorly. The internal carotid arteries enter the cranial cavity and mainly supply the anterior and middle parts of the cerebral hemispheres. The vertebral arteries enter through the foramen magnum, unite to form the basilar artery, and supply the brainstem, cerebellum, occipital lobes, and inferior temporal regions.
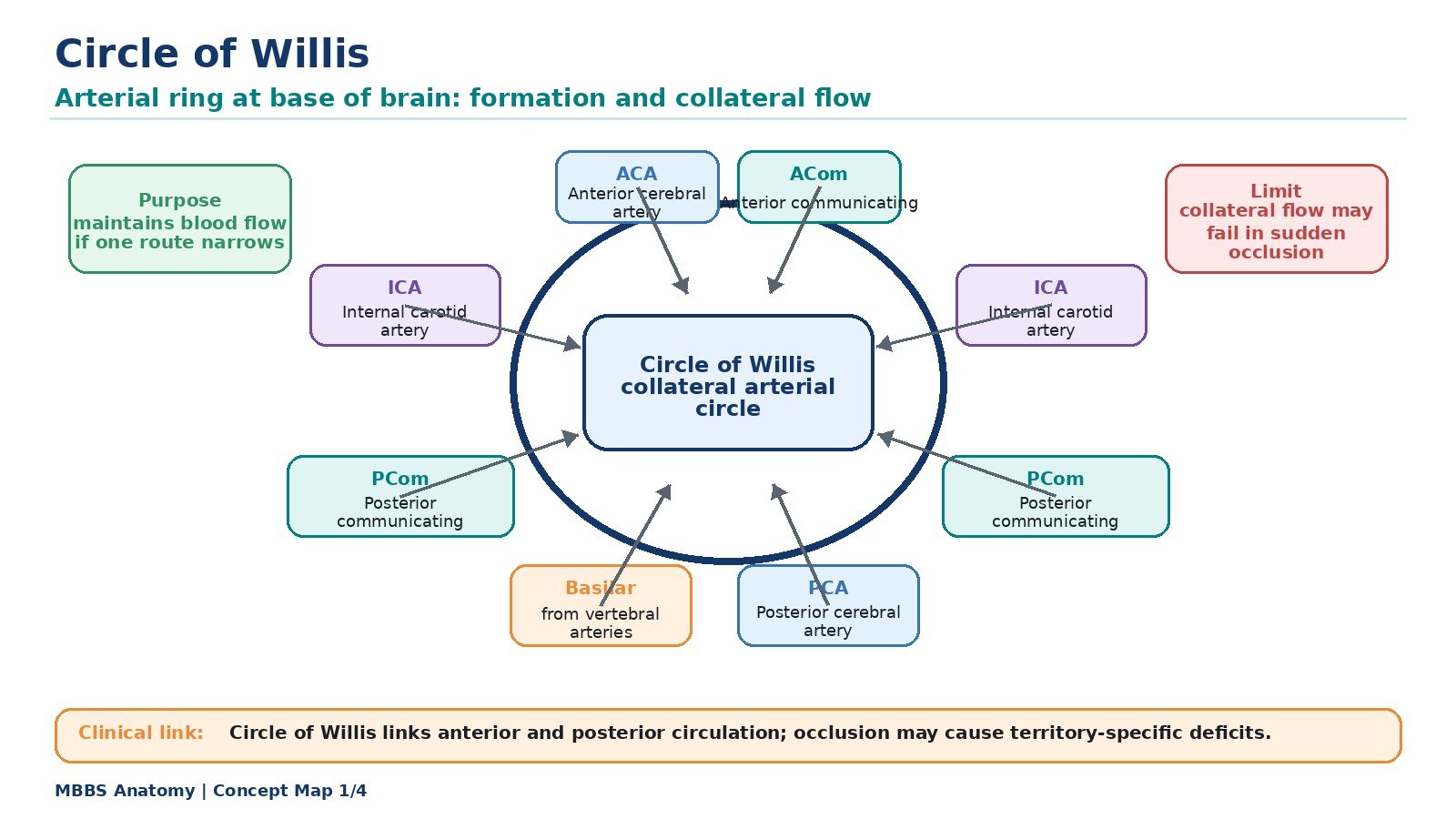
At the base of the brain, these two arterial systems are connected by the Circle of Willis. This circle is not just a structural arrangement; it exists to provide a possible alternative route for blood flow. If one major artery becomes narrowed gradually, blood may pass through communicating arteries to maintain perfusion of the threatened area. Therefore, the Circle of Willis acts as an anatomical safety mechanism.
Formation of Circle of Willis
The Circle of Willis is formed by:
- Anterior cerebral artery on each side
- Anterior communicating artery
- Terminal part of internal carotid artery on each side
- Posterior communicating artery on each side
- Posterior cerebral artery on each side
The anterior communicating artery connects the two anterior cerebral arteries. The posterior communicating arteries connect the internal carotid arteries with the posterior cerebral arteries. In this way, the anterior circulation and posterior circulation become linked.
The Circle of Willis exists because the brain is highly dependent on uninterrupted blood supply. Neurons cannot store oxygen or glucose for long periods. Therefore, even a short interruption in blood supply can cause neuronal dysfunction. However, the circle is not always complete or equally developed in every person. Anatomical variations are common. Because of this, collateral circulation may be inadequate in some patients, making them more vulnerable to stroke.
⚠️ CLINICAL IMPORTANCE
Failure of blood supply through the cerebral arteries can produce stroke. If collateral circulation through the Circle of Willis is sufficient, symptoms may be reduced. If collateral circulation is poor or the blockage is sudden, brain tissue becomes ischemic and neurological deficit appears. Aneurysms commonly occur near arterial branching points of the Circle of Willis and may rupture, causing hemorrhagic stroke or subarachnoid hemorrhage.
B. Major Cerebral Arteries and Vascular Territories
🧠 CORE
- The anterior cerebral artery supplies mainly the medial surface of the cerebral hemisphere.
- The middle cerebral artery supplies most of the lateral surface of the cerebral hemisphere.
- The posterior cerebral artery supplies the occipital lobe and inferior temporal region.
- Motor deficits depend on which cortical motor area or pathway is affected.
- The middle cerebral artery is commonly involved in stroke.
- The internal capsule is a compact motor pathway area and small lesions here can cause dense hemiplegia.
- Vascular territory localization is essential for understanding clinical stroke signs.
🔬 CONCEPT EXPLAINED
The cerebral cortex is supplied by different arteries, and each artery supplies a specific territory. This anatomical arrangement explains why different strokes produce different clinical patterns.
The anterior cerebral artery (ACA) passes forward and medially. It supplies the medial surface of the frontal and parietal lobes. This region contains the cortical representation of the opposite lower limb in the motor and sensory homunculus. Therefore, an ACA stroke commonly affects the opposite leg more than the arm or face.
The middle cerebral artery (MCA) is the largest branch of the internal carotid artery and travels laterally into the lateral sulcus. It supplies the lateral surface of the cerebral hemisphere. This region contains the motor and sensory representation of the face and upper limb. Therefore, an MCA stroke commonly causes weakness of the opposite face and arm more than the leg. Because the MCA also supplies language areas in the dominant hemisphere, its stroke may cause aphasia. This is why MCA stroke is one of the most clinically important stroke patterns.
The posterior cerebral artery (PCA) arises from the basilar artery and supplies the occipital lobe and inferior temporal region. Since the occipital lobe contains the visual cortex, PCA stroke may cause visual field defects.
A very important anatomical point is the internal capsule. Although it is not a cortical surface territory, it contains tightly packed descending motor fibers, including corticospinal and corticobulbar fibers. A small vascular lesion here can produce severe contralateral hemiplegia because many motor fibers are concentrated in a small area.
Vascular Territory and Motor Deficit
- ACA lesion: Contralateral leg weakness more than arm.
- MCA lesion: Contralateral face and arm weakness more than leg.
- Internal capsule lesion: Dense contralateral hemiplegia involving face, arm, and leg.
- Brainstem lesion: May produce crossed signs due to involvement of cranial nerve nuclei and long tracts.
- PCA lesion: Mainly visual defects rather than pure motor hemiplegia.
⚠️ CLINICAL IMPORTANCE
Vascular territory localization helps doctors predict the site of stroke from clinical signs. For example, sudden right-sided face and arm weakness with speech difficulty suggests a left MCA territory stroke. Sudden weakness of the opposite leg suggests ACA involvement. Dense hemiplegia involving the entire opposite side suggests internal capsule involvement.
C. Cortical Motor Pathway, Corticospinal Tract and Hemiplegia
🧠 CORE
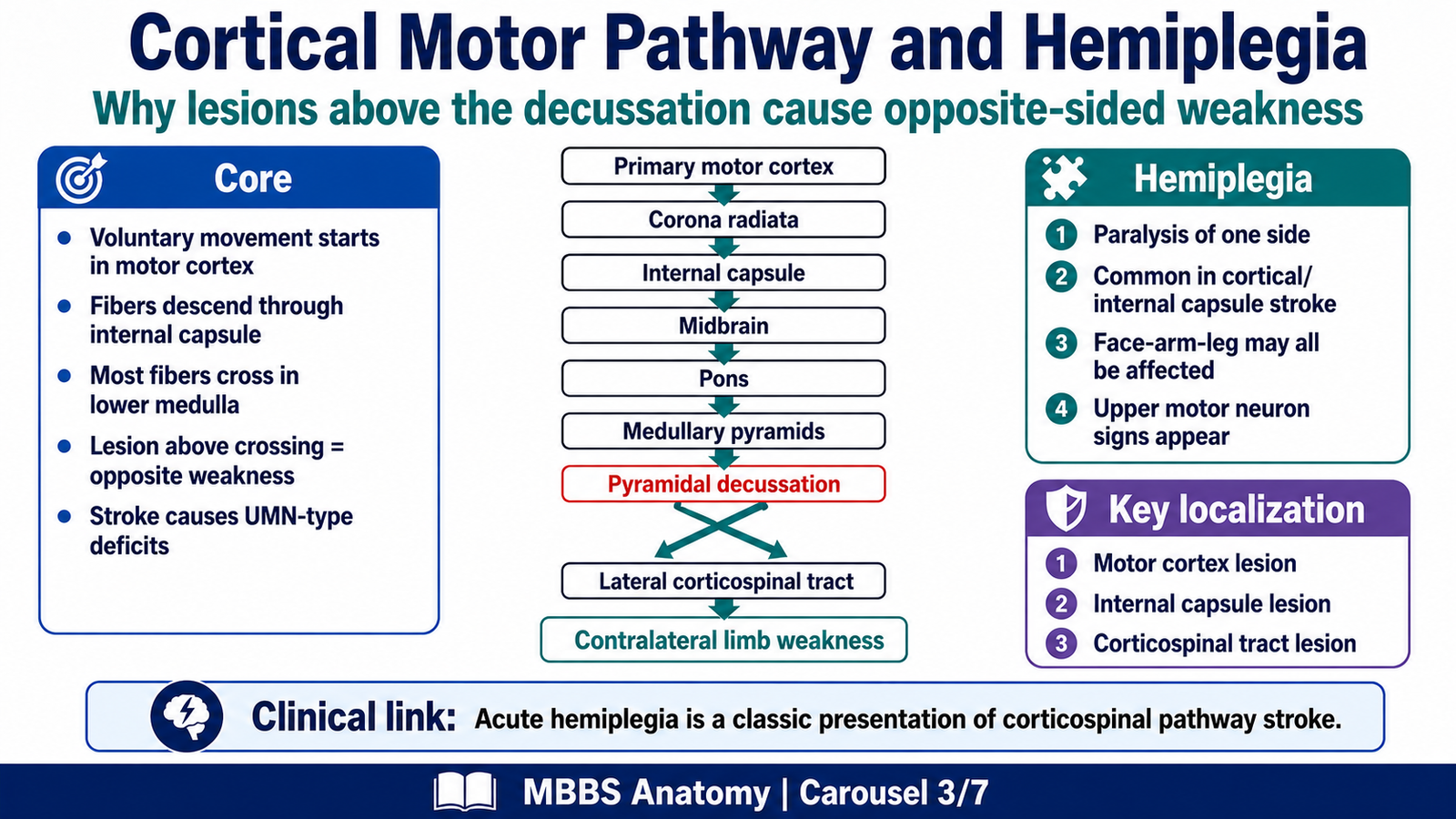
- Voluntary movement begins mainly in the primary motor cortex.
- Motor fibers descend through corona radiata and internal capsule.
- Fibers continue through midbrain, pons, medulla, and spinal cord as corticospinal tract.
- Most corticospinal fibers cross in the lower medulla at pyramidal decussation.
- Lesion above the decussation causes weakness on the opposite side.
- Stroke commonly causes upper motor neuron type weakness.
- Hemiplegia is a major clinical presentation of corticospinal tract or cortical motor pathway lesion.
🔬 CONCEPT EXPLAINED
Hemiplegia can be understood only when the motor pathway is followed from the cortex to the spinal cord. Voluntary movement starts in the primary motor cortex, located in the precentral gyrus of the frontal lobe. The motor cortex is arranged as a motor homunculus. The lower limb is represented medially, while the face and upper limb are represented more laterally.
From the cortex, motor fibers descend through the corona radiata and then become tightly packed in the internal capsule. This is why internal capsule lesions are so serious. A small stroke in this region may interrupt many descending motor fibers at once.
The fibers then pass through the cerebral peduncle of the midbrain, basis pontis of the pons, and pyramids of the medulla. At the lower medulla, most corticospinal fibers cross to the opposite side in the pyramidal decussation. After crossing, they descend in the lateral corticospinal tract of the spinal cord and influence lower motor neurons.
This crossing explains the most important clinical rule:
A lesion above the pyramidal decussation causes motor weakness on the opposite side of the body. Therefore, a stroke in the left cerebral hemisphere commonly produces right-sided hemiplegia.
Upper Motor Neuron Features in Stroke
Since stroke usually affects the motor cortex, internal capsule, or descending motor fibers, it produces an upper motor neuron pattern. Features may include:
- Weakness or paralysis of opposite side
- Increased tone after the acute phase
- Exaggerated deep tendon reflexes
- Positive Babinski sign
- Loss of fine voluntary movement
- Spasticity developing later
⚠️ CLINICAL IMPORTANCE
Stroke is an important cause of acute hemiplegia. Sudden onset of weakness suggests vascular cause until proven otherwise. The exact pattern of weakness helps localize the lesion. Face and arm weakness suggests MCA territory, leg weakness suggests ACA territory, and dense face-arm-leg weakness suggests internal capsule involvement.
D. Stroke: Basic Concept, Etiology and Types
🧠 CORE
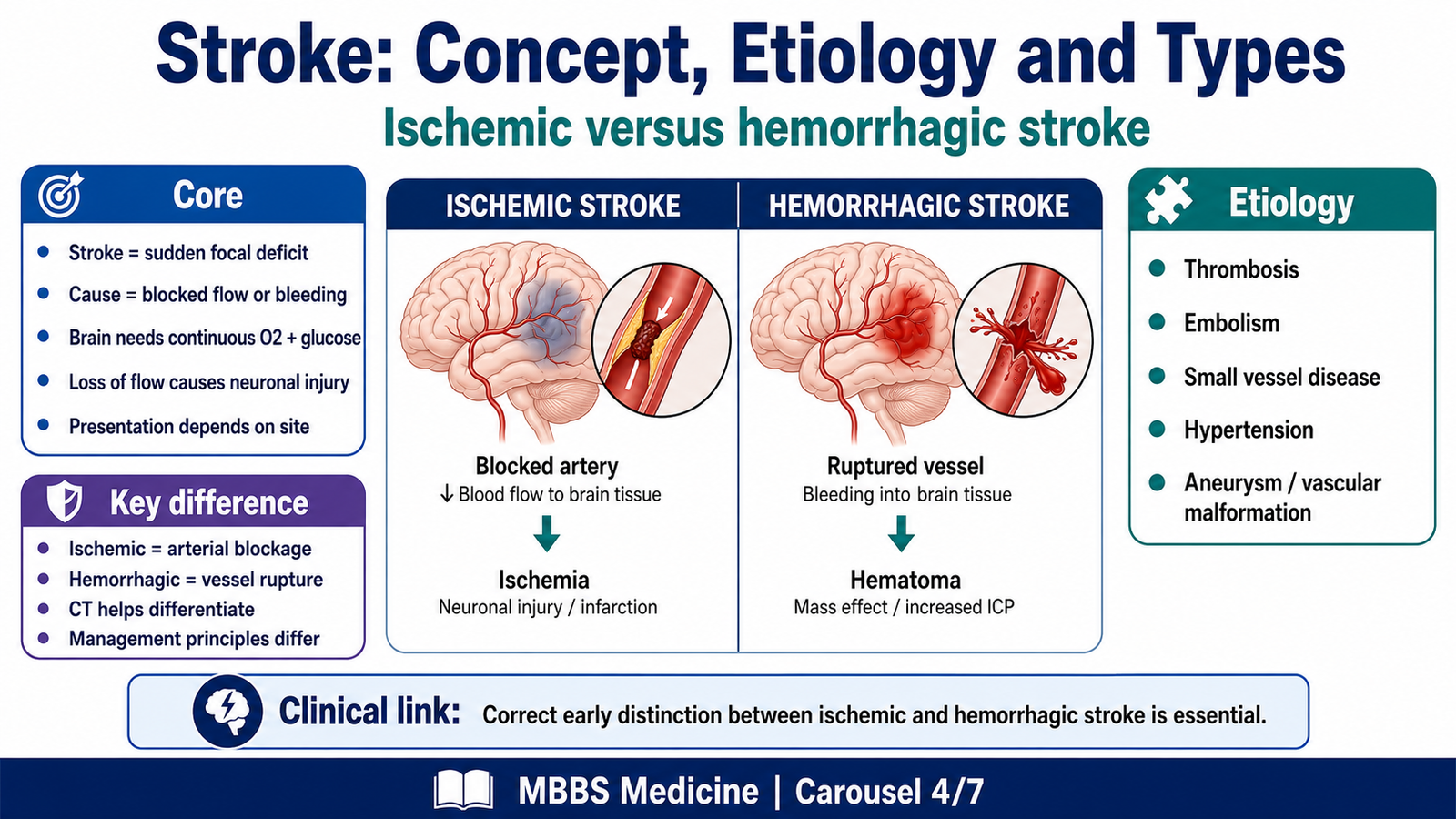
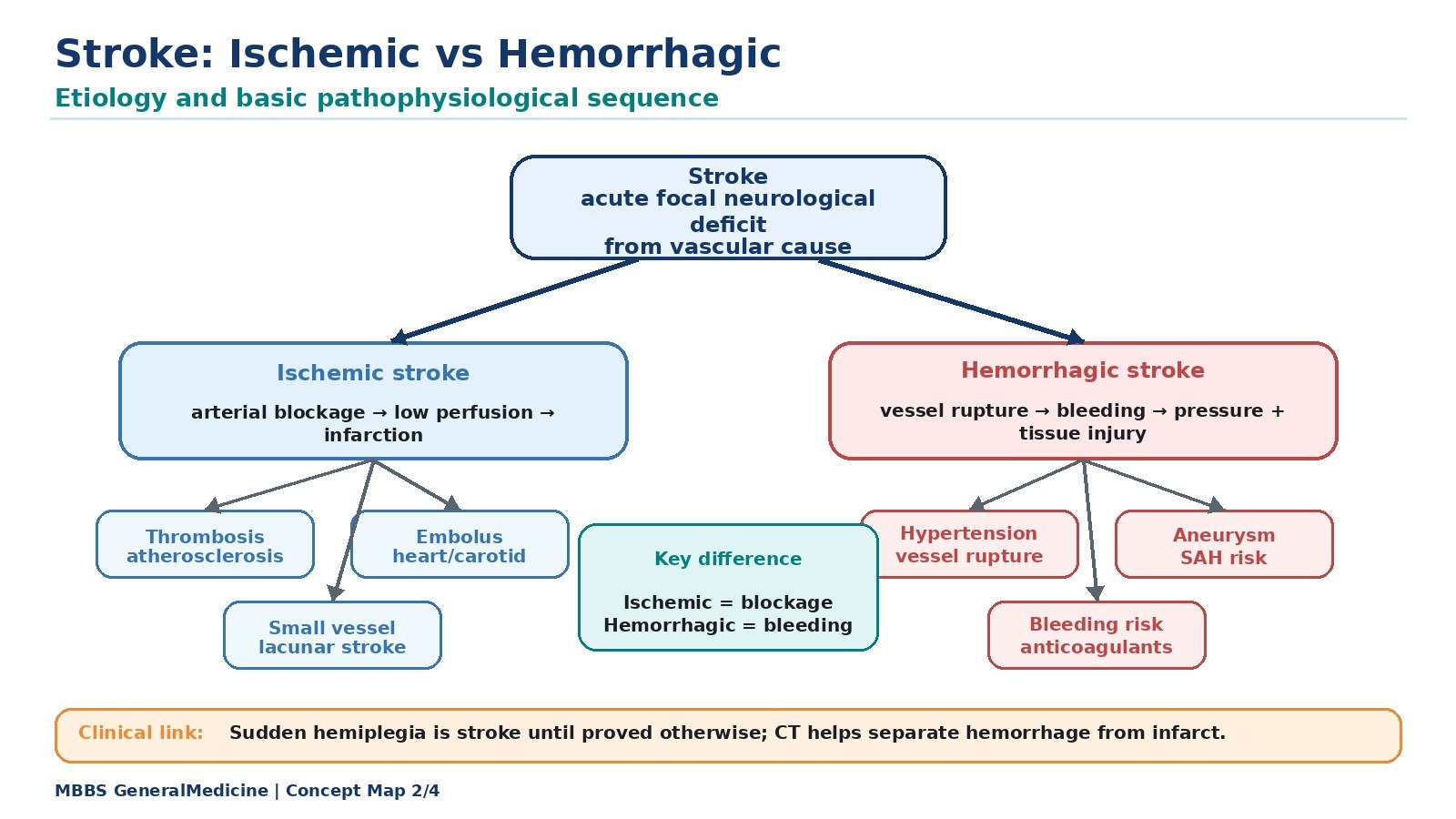
- Stroke is sudden neurological deficit due to vascular injury.
- It may be ischemic or hemorrhagic.
- Ischemic stroke is caused by arterial blockage.
- Hemorrhagic stroke is caused by vessel rupture and bleeding.
- Etiology includes thrombosis, embolism, small vessel disease, hypertension, aneurysm, and vascular malformations.
- Stroke damages neurons by reducing oxygen and glucose supply or by pressure effect of bleeding.
- Clinical features depend on the vascular territory and brain area involved.
🔬 CONCEPT EXPLAINED
Stroke occurs when a part of the brain suddenly fails to receive adequate blood supply or is damaged by bleeding. The brain has a very high metabolic demand. It needs continuous oxygen and glucose because neurons cannot function normally without them. When blood flow stops, ATP production falls. Ion pumps fail, neurons depolarize, calcium enters cells, and cell injury develops. This produces loss of function in the affected brain region.
Ischemic Stroke
Ischemic stroke occurs when an artery is blocked. The blockage may be due to:
- Thrombosis: Clot formation at the site of an atherosclerotic plaque.
- Embolism: Clot or material travels from another site, commonly heart or carotid artery, and blocks a cerebral artery.
- Small vessel disease: Narrowing of small penetrating arteries, commonly due to hypertension or diabetes.
- Hypoperfusion: Reduced blood flow due to systemic circulatory failure.
In ischemic stroke, the main problem is lack of blood supply. The affected area becomes ischemic and may progress to infarction.
Hemorrhagic Stroke
Hemorrhagic stroke occurs when a blood vessel ruptures. Blood leaks into brain tissue or around the brain. This damages the brain in two ways. First, the area supplied by the ruptured vessel may lose blood supply. Second, the collected blood compresses surrounding brain tissue and increases intracranial pressure.
Common causes include:
- Long-standing hypertension
- Ruptured aneurysm
- Arteriovenous malformation
- Bleeding disorders
- Anticoagulant use
- Head injury
Difference Between Ischemic and Hemorrhagic Stroke
| Feature | Ischemic Stroke | Hemorrhagic Stroke |
|---|---|---|
| Basic problem | Arterial blockage | Vessel rupture |
| Main mechanism | Reduced blood flow and infarction | Bleeding, pressure effect, tissue damage |
| Common cause | Thrombosis or embolism | Hypertension or aneurysm rupture |
| Onset | Sudden focal deficit | Sudden deficit, often with severe headache/vomiting |
| CT brain early | May be normal initially | Shows blood early |
| Treatment principle | Restore/prevent further blockage | Control bleeding and pressure |
⚠️ CLINICAL IMPORTANCE
Differentiating ischemic and hemorrhagic stroke is clinically essential because management differs. A patient with ischemic stroke may need antiplatelet or clot-related treatment, while hemorrhagic stroke requires bleeding control and pressure management. At MBBS 2nd year level, students should focus on the basic mechanism, cause, and clinical difference.
E. Risk Factors for Cerebrovascular Disease
🧠 CORE
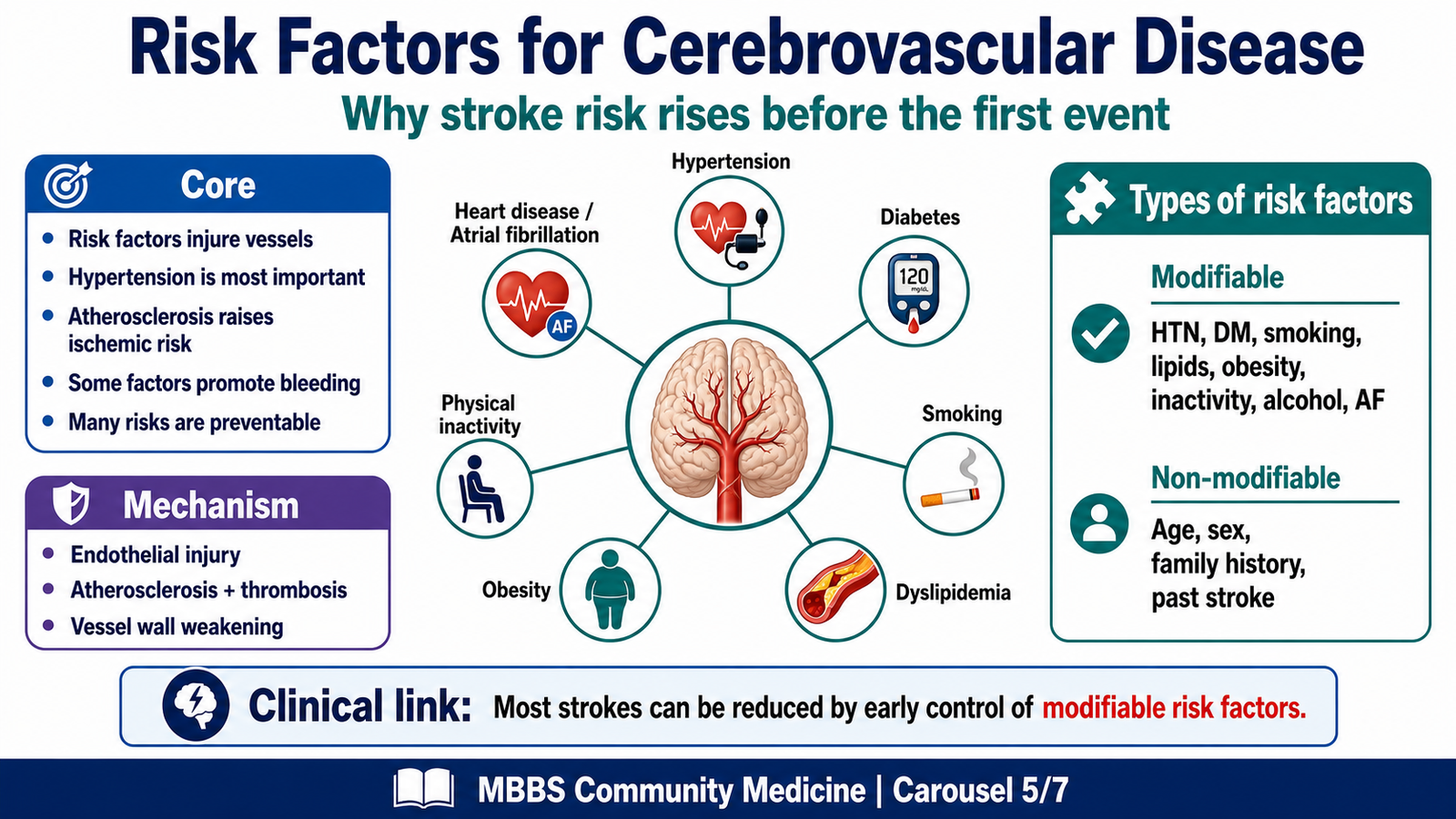
- Risk factors increase the chance of stroke and other cerebrovascular diseases.
- Some risk factors are modifiable; others are non-modifiable.
- Hypertension is the most important modifiable risk factor.
- Diabetes, smoking, dyslipidemia, obesity, and physical inactivity increase vascular injury.
- Age, sex, family history, and previous stroke are non-modifiable risks.
- Risk factors act by damaging vessel walls, increasing thrombosis, or promoting atherosclerosis.
- Prevention depends mainly on identifying and controlling modifiable risks.
🔬 CONCEPT EXPLAINED
Cerebrovascular disease does not usually appear suddenly without background risk. Most strokes occur because risk factors gradually damage arteries or increase clot formation. The most important risk factor is hypertension. High blood pressure damages the inner lining of arteries, accelerates atherosclerosis, and weakens small vessels. This can lead to both ischemic and hemorrhagic stroke.
Diabetes mellitus damages small and large blood vessels and increases atherosclerosis. Smoking causes endothelial injury, increases platelet activity, and promotes vascular narrowing. Dyslipidemia contributes to plaque formation in arteries. Obesity and physical inactivity increase hypertension, diabetes, and lipid abnormalities. Atrial fibrillation is important because it can form clots in the heart that may travel to the brain and cause embolic stroke.
Modifiable Risk Factors
- Hypertension
- Diabetes mellitus
- Smoking
- Dyslipidemia
- Obesity
- Physical inactivity
- Unhealthy diet
- Excess alcohol intake
- Atrial fibrillation and heart disease
- Poorly controlled stress and sedentary lifestyle
Non-Modifiable Risk Factors
- Increasing age
- Male sex
- Family history
- Previous stroke or transient ischemic attack
- Genetic predisposition
Community Medicine View
From a preventive medicine perspective, risk factors are important because many strokes can be prevented before they occur. Population education, screening, lifestyle modification, and early treatment of hypertension and diabetes reduce stroke burden.
⚠️ CLINICAL IMPORTANCE
In exams, students should remember that risk factors are not just lists. They cause stroke by damaging vessels, increasing atherosclerosis, increasing clot formation, or weakening vessel walls. Hypertension is especially important because it contributes to both ischemic and hemorrhagic stroke.
F. Prevention of Cerebrovascular Disease
🧠 CORE
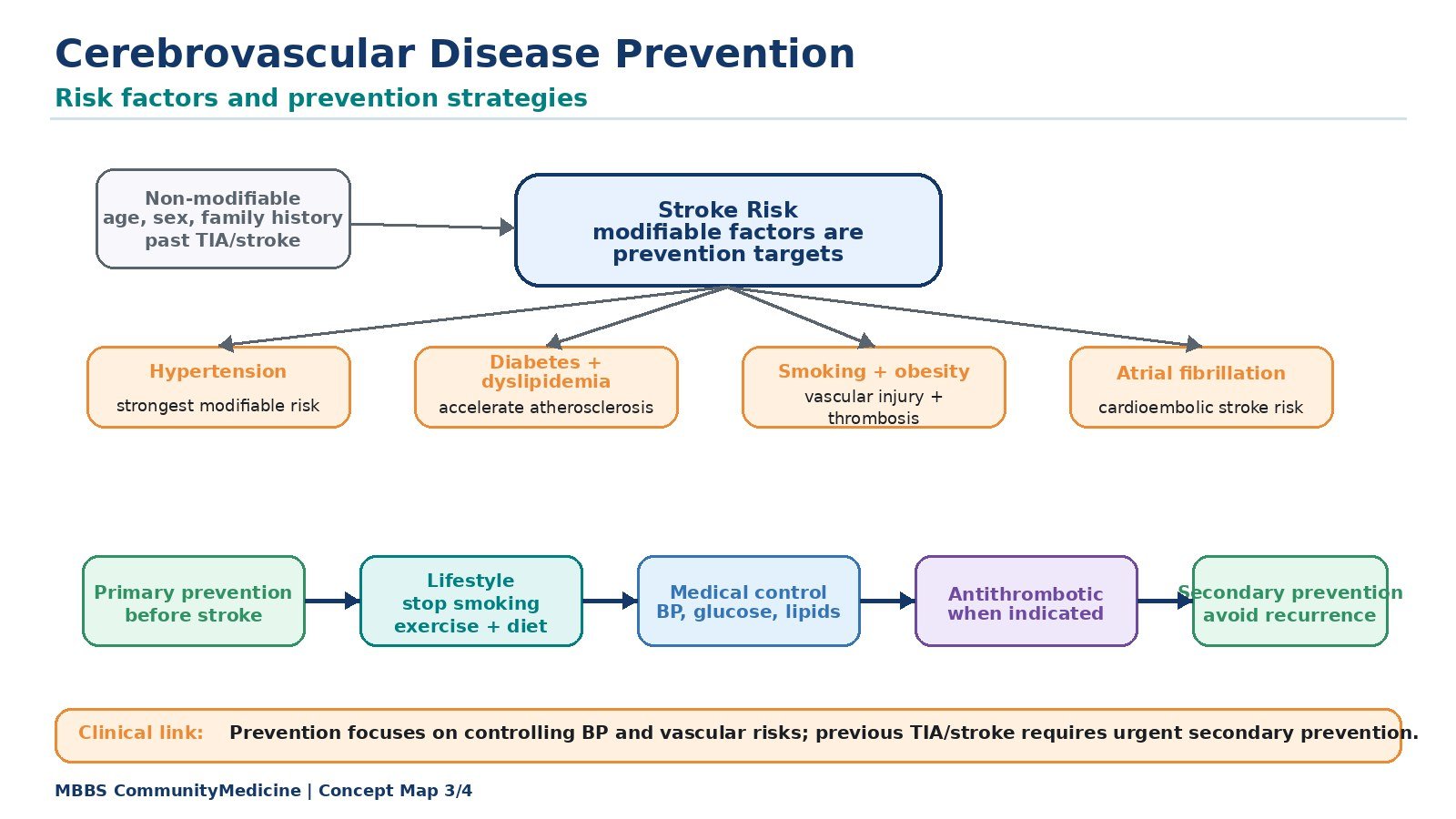
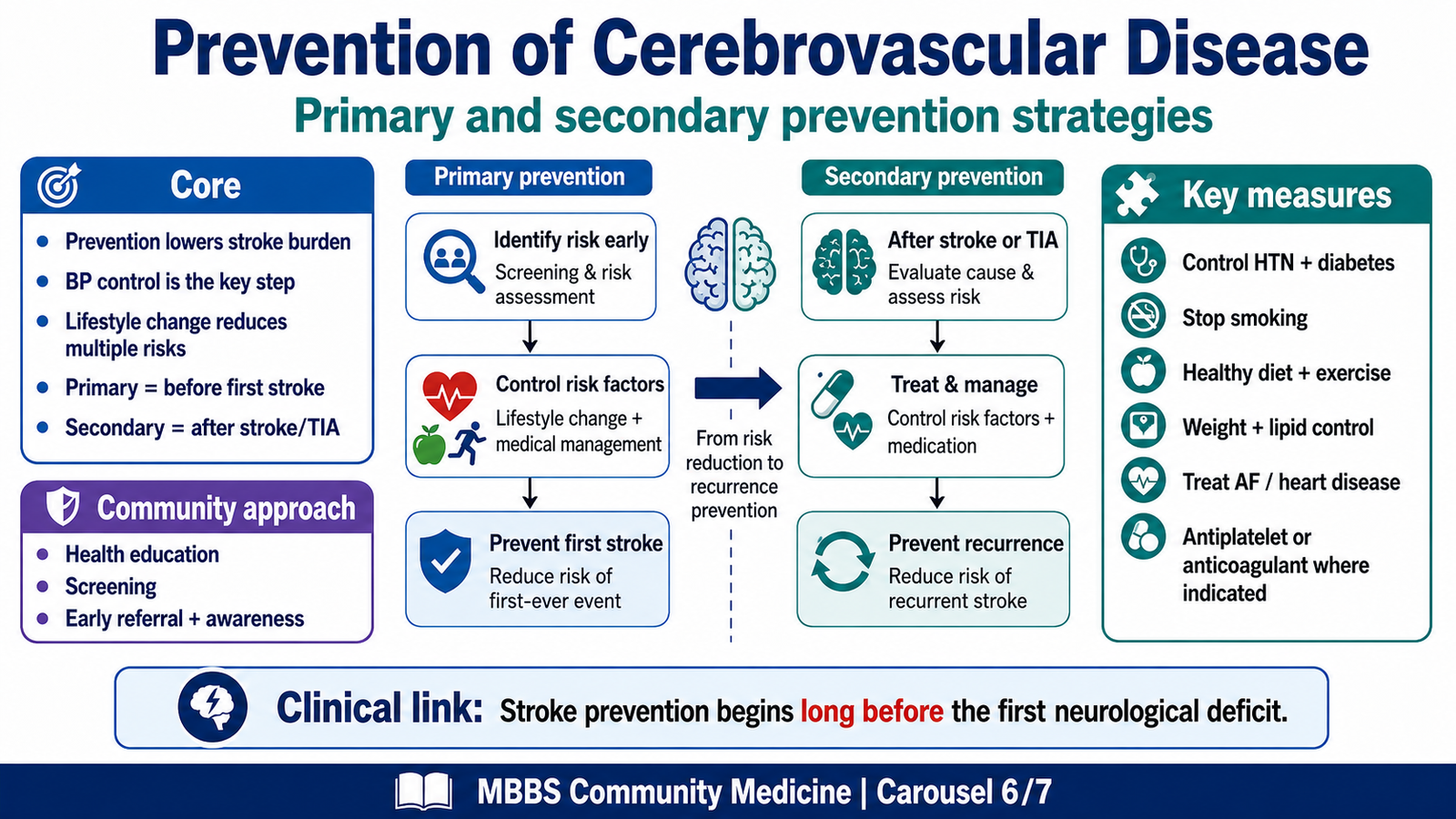
- Prevention aims to reduce stroke occurrence and recurrence.
- Primary prevention acts before the first stroke.
- Secondary prevention acts after stroke or transient ischemic attack.
- Blood pressure control is the most important preventive strategy.
- Lifestyle changes reduce multiple risk factors together.
- Community-level prevention includes screening and health education.
- Prevention is both individual and population-based.
🔬 CONCEPT EXPLAINED
Prevention of stroke is based on controlling the factors that damage cerebral blood vessels. Since stroke often results from chronic vascular injury, prevention must start before symptoms occur.
Primary Prevention
Primary prevention means preventing the first stroke. It includes:
- Screening for hypertension
- Control of diabetes
- Smoking cessation
- Healthy diet with reduced salt and saturated fat
- Regular physical activity
- Weight control
- Lipid control
- Avoiding excessive alcohol
- Detection and treatment of atrial fibrillation
- Public education about stroke warning signs
Secondary Prevention
Secondary prevention means preventing another stroke in someone who already had stroke or transient ischemic attack. It includes:
- Strict blood pressure control
- Diabetes and lipid control
- Antiplatelet therapy where indicated
- Anticoagulation in selected patients with atrial fibrillation
- Carotid artery evaluation where appropriate
- Rehabilitation and follow-up
- Lifestyle correction
Community Medicine Strategies
At community level, prevention includes health education, screening camps, risk factor surveillance, promotion of physical activity, tobacco control, dietary awareness, and early referral of suspected stroke patients. The aim is to reduce both disease incidence and disability.
⚠️ CLINICAL IMPORTANCE
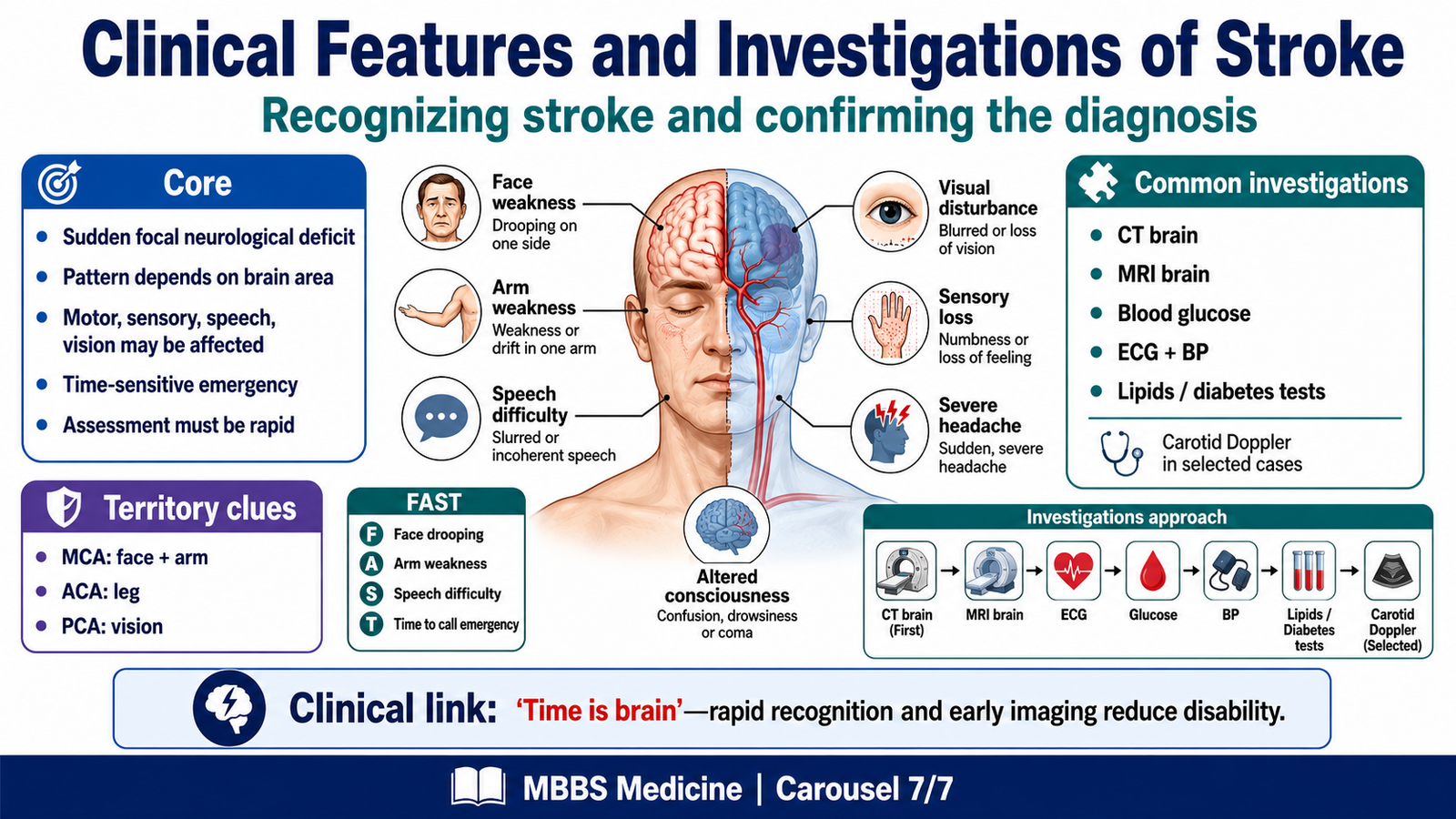
Prevention is clinically important because stroke often causes permanent disability. Recognizing warning symptoms and reaching hospital early can reduce complications. Public awareness using FAST is useful: Face drooping, Arm weakness, Speech difficulty, Time to seek emergency care.
G. Clinical Features and Investigations of Stroke
🧠 CORE
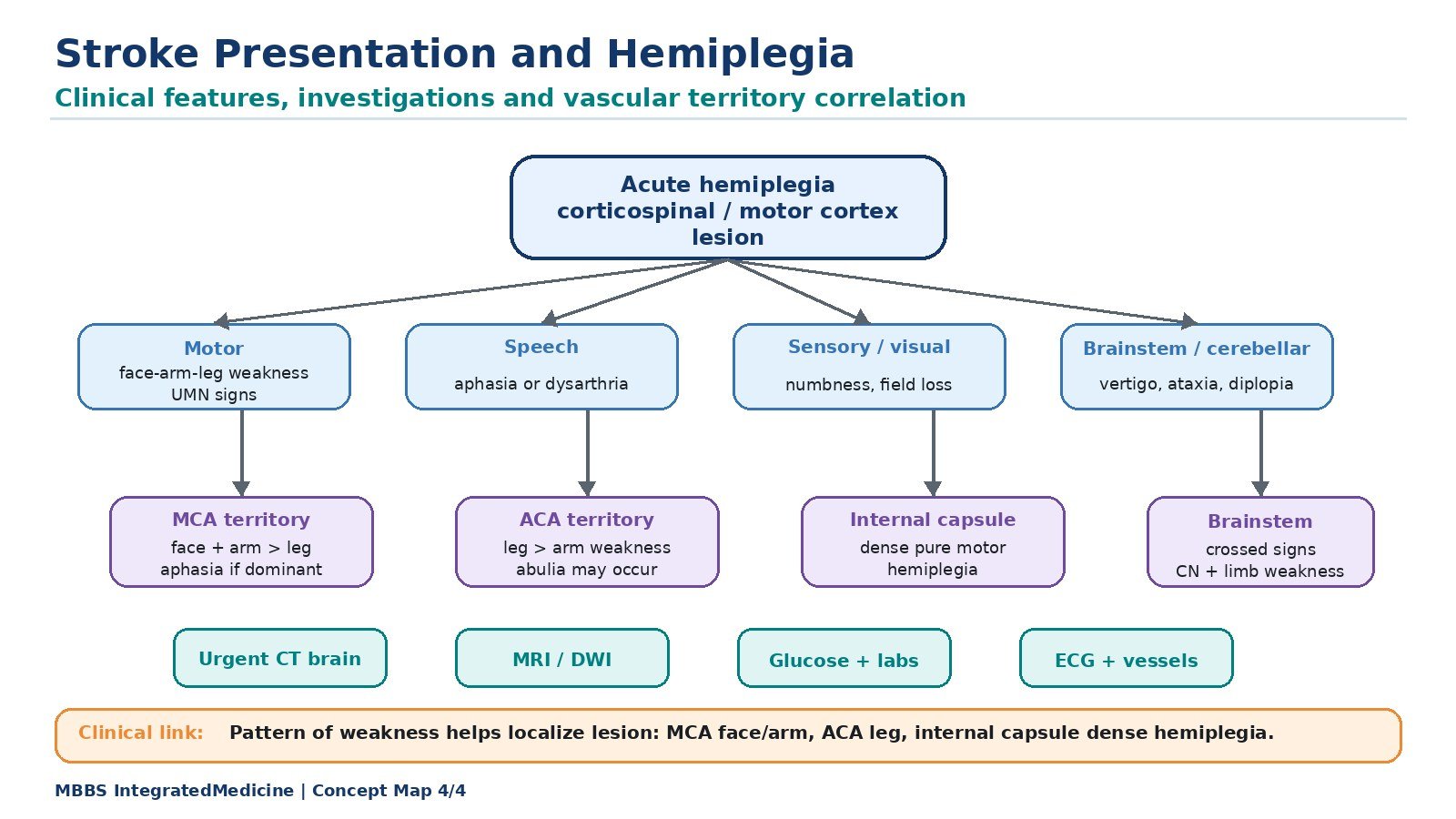
- Stroke presents with sudden focal neurological deficit.
- Features depend on the area of brain involved.
- Hemiplegia, facial weakness, speech disturbance, sensory loss, visual symptoms, and altered consciousness may occur.
- MCA stroke commonly affects face and arm.
- ACA stroke commonly affects leg.
- PCA stroke commonly affects vision.
- CT scan is commonly used first to distinguish hemorrhage from ischemia.
- Basic investigations identify cause and risk factors.
🔬 CONCEPT EXPLAINED
The clinical features of stroke reflect the function of the damaged brain area. If the motor cortex or corticospinal pathway is affected, weakness occurs. If sensory cortex is affected, sensory loss occurs. If language areas in the dominant hemisphere are affected, aphasia may occur. If visual cortex is affected, visual field defects occur.
Common Clinical Features
- Sudden weakness of one side of body
- Facial deviation or facial weakness
- Difficulty speaking or understanding speech
- Numbness or sensory loss
- Sudden visual disturbance
- Dizziness, imbalance, or ataxia
- Severe headache, especially in hemorrhagic stroke
- Vomiting or altered consciousness in severe cases
- Seizures in some patients
Clinical Features by Vascular Territory
MCA stroke:
Commonly causes contralateral face and arm weakness, sensory loss, aphasia if dominant hemisphere is involved, and neglect if non-dominant hemisphere is involved.
ACA stroke:
Commonly causes contralateral leg weakness more than arm weakness.
PCA stroke:
Commonly causes visual field defects.
Internal capsule stroke:
Can cause dense contralateral hemiplegia affecting face, arm, and leg.
Investigations of Stroke
At 2nd Year MBBS level, investigations should be understood according to purpose.
CT brain:
Used early to detect hemorrhage and differentiate hemorrhagic from ischemic stroke.
MRI brain:
More sensitive for early ischemic changes.
Blood glucose:
Hypoglycemia can mimic stroke and must be excluded.
Blood pressure measurement:
Important because hypertension is both a risk factor and acute management concern.
ECG:
Detects atrial fibrillation or cardiac cause of embolism.
Lipid profile and diabetes screening:
Identify modifiable vascular risk factors.
Carotid Doppler:
Assesses carotid narrowing in selected patients.
⚠️ CLINICAL IMPORTANCE
A stroke patient must be assessed urgently because brain tissue is time-sensitive. The phrase “time is brain” means that delay in restoring or protecting cerebral blood flow increases neuronal death and disability.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Circle of Willis
Structure: Arterial ring at the base of brain connecting internal carotid and vertebrobasilar systems.
Function: Provides collateral circulation.
Outcome: May protect brain from ischemia when arterial narrowing is gradual.
Middle Cerebral Artery
Structure: Large branch of internal carotid artery supplying lateral cerebral hemisphere.
Function: Supplies face and arm motor areas, sensory cortex, and language areas.
Outcome: MCA stroke commonly causes contralateral face-arm weakness and speech disturbance.
Anterior Cerebral Artery
Structure: Artery supplying medial cerebral hemisphere.
Function: Supplies lower limb area of motor cortex.
Outcome: ACA stroke commonly causes contralateral leg weakness.
Internal Capsule
Structure: Compact white matter pathway containing descending motor fibers.
Function: Carries motor signals from cortex to brainstem and spinal cord.
Outcome: Small lesion can cause severe contralateral hemiplegia.
Cerebral Blood Flow
Structure: Brain supplied by anterior and posterior circulations.
Function: Delivers oxygen and glucose continuously to neurons.
Outcome: Interruption causes rapid neurological dysfunction and stroke.
🩺 5️⃣ Clinical Correlation
Hemiplegia as a Presentation of Cortical Motor Pathway Lesion
Hemiplegia occurs when the motor cortex, internal capsule, brainstem motor pathway, or corticospinal tract is damaged. In stroke, this usually occurs suddenly. Because most corticospinal fibers cross in the lower medulla, lesions in the cerebral hemisphere usually cause weakness on the opposite side of the body.
Stroke as an Important Cause of Acute Hemiplegia
Acute hemiplegia should strongly suggest stroke, especially in older patients or patients with hypertension, diabetes, smoking history, or heart disease. The sudden onset helps distinguish stroke from slowly progressive causes such as tumors.
Vascular Territory and Motor Deficit
- MCA stroke: face and arm weakness more than leg.
- ACA stroke: leg weakness more than arm.
- Internal capsule stroke: dense face, arm, and leg weakness.
- PCA stroke: visual symptoms are more prominent than motor weakness.
Ischemic Versus Hemorrhagic Stroke
Ischemic stroke results from blockage of blood flow, while hemorrhagic stroke results from bleeding. Both can cause hemiplegia, but hemorrhagic stroke more commonly presents with severe headache, vomiting, reduced consciousness, or signs of raised intracranial pressure.
Prevention-Oriented Clinical Correlation
A patient with hypertension and smoking history is at high risk because both damage blood vessels. Controlling blood pressure, stopping smoking, treating diabetes, reducing lipids, and improving physical activity reduce the risk of stroke.
📌 6️⃣ Summary Points
- The Circle of Willis is located at the base of the brain and connects anterior and posterior cerebral circulations.
- It is formed by anterior cerebral arteries, anterior communicating artery, internal carotid arteries, posterior communicating arteries, and posterior cerebral arteries.
- The Circle of Willis provides potential collateral circulation but does not always prevent stroke.
- MCA stroke commonly causes contralateral face and arm weakness.
- ACA stroke commonly causes contralateral leg weakness.
- PCA stroke commonly causes visual field defects.
- Internal capsule lesions can cause dense contralateral hemiplegia because motor fibers are tightly packed.
- Ischemic stroke is due to arterial blockage; hemorrhagic stroke is due to vessel rupture.
- Hypertension is the most important modifiable risk factor for stroke.
- Stroke is an important cause of sudden hemiplegia.
- Lesions above pyramidal decussation cause opposite-sided motor weakness.
- Prevention depends on controlling blood pressure, diabetes, smoking, lipids, obesity, and physical inactivity.