
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Posture, locomotion and equilibrium are essential motor functions that allow the body to stand, walk, maintain balance, and keep visual fixation during movement. These functions depend on integration between the spinal cord, brainstem reticular formation, vestibular apparatus, cerebellum, motor cortex, muscles, joints and eyes. The spinal cord can generate basic reflex postural and stepping responses, but higher centers refine these movements into smooth, purposeful locomotion.
The vestibular apparatus lies in the inner ear and detects head position and head movement. It provides sensory information required for balance, posture, and stabilization of the eyes during head motion. Clinically, dysfunction of this system causes vertigo, imbalance, abnormal posture, nystagmus and unsteady gait. Therefore, this topic links neurophysiology, anatomy of the inner ear, reflex motor control and clinical neurology.
🔹 2️⃣ Foundation Concepts
Key Definitions
• Posture: The position of the body or body parts in relation to gravity and surroundings.
• Equilibrium: Maintenance of body balance during rest or movement.
• Locomotion: Coordinated movement of the body from one place to another, mainly walking.
• Positive supportive reaction: Reflex extension of the limb when pressure is applied to the foot or paw, helping the body support weight.
• Righting reflexes: Reflexes that restore normal body position when posture is disturbed.
• Cord righting reflexes: Spinal cord-mediated reflexes that help correct posture at a basic level.
• Vestibular apparatus: Sensory organ of balance located in the inner ear.
• Utricle and saccule: Otolith organs that detect static head position and linear acceleration.
• Semicircular ducts: Structures that detect angular or rotational acceleration of the head.
• Vestibulo-ocular reflex: Reflex mechanism that stabilizes gaze by moving eyes opposite to head movement.
Essential Terminology
• Static equilibrium: Balance when the head/body is still or moving linearly.
• Dynamic equilibrium: Balance during rotational movement.
• Otoliths/otoconia: Calcium carbonate crystals in utricle and saccule that help detect gravity and linear acceleration.
• Hair cells: Receptor cells of vestibular apparatus that convert mechanical movement into nerve signals.
• Endolymph: Fluid inside membranous labyrinth; movement of endolymph bends hair cells.
• Crista ampullaris: Sensory receptor in semicircular ducts.
• Macula: Sensory receptor area in utricle and saccule.
• Vestibular nuclei: Brainstem nuclei receiving vestibular input and sending outputs to spinal cord, eyes, cerebellum and cortex.
• Reticular formation: Brainstem network important in posture, tone and locomotor control.
• Pontine reticular nuclei: Facilitate extensor tone.
• Medullary reticular nuclei: Inhibit excessive extensor tone.
Basic Overview
• Posture is maintained by reflex interaction between muscles, joints, vestibular input and brainstem motor centers.
• Walking depends on spinal pattern-generating circuits but requires brainstem and cortical control for purposeful movement.
• Vestibular apparatus detects head position and movement.
• Utricle and saccule mainly detect gravity and linear acceleration.
• Semicircular ducts detect rotational acceleration.
• Vestibular signals stabilize posture through vestibulospinal pathways.
• Vestibular signals stabilize eyes through vestibulo-ocular reflex pathways.
• Failure causes vertigo, imbalance, nystagmus, falls and abnormal gait.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPT 1 — Neural Basis of Posture and Equilibrium
🧠 CORE
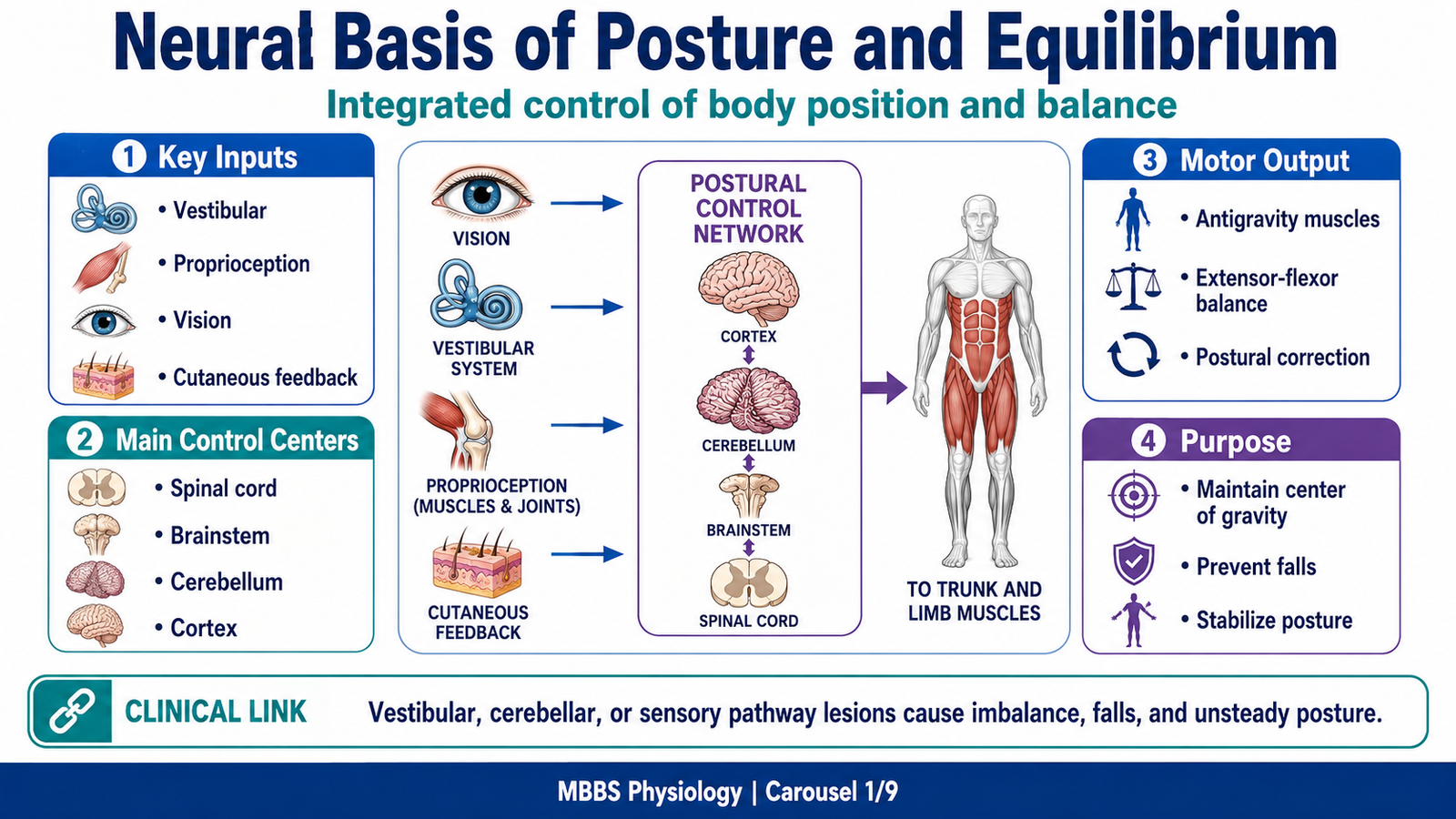
• Posture depends on continuous interaction between sensory input and motor output.
• Major sensory inputs come from vestibular apparatus, proprioceptors, vision and cutaneous receptors.
• Motor output is mainly through spinal motor neurons controlling antigravity muscles.
• Brainstem centers regulate muscle tone and postural reflexes.
• Cerebellum refines balance and coordination.
• Postural control is mostly automatic but can be influenced by conscious control.
• Maintenance of posture requires coordinated activation and inhibition of muscle groups.
🔬 CONCEPT EXPLAINED
Posture is not a fixed body position; it is a continuously adjusted motor state. Even when a person appears to stand still, the body is making constant small corrections to prevent falling. These corrections occur because gravity continuously tends to pull the body away from its center of balance. The nervous system therefore needs a mechanism that detects body position, compares it with the desired posture, and produces appropriate muscle responses.
The stimulus or initiating event for postural control is any change in body position, head position, muscle stretch, joint angle, pressure on the feet, or visual orientation. The purpose of the mechanism is to keep the center of gravity within the base of support so that the body does not fall. Sensory receptors detect the disturbance first. Proprioceptors in muscles and joints inform the spinal cord and brain about limb position. Cutaneous receptors in the soles detect pressure distribution. The vestibular apparatus detects head position and movement. Vision provides information about the body’s relation to surroundings.
These sensory signals reach spinal cord, brainstem, cerebellum and cortex. The spinal cord produces rapid reflex responses; brainstem centers regulate postural tone; cerebellum coordinates the timing and accuracy of responses; cortex contributes when posture becomes voluntary or complex. As a result, extensor and flexor muscles are activated or inhibited in a coordinated pattern.
The cause → effect relationship is simple but important: if the body sways forward, stretch and pressure receptors detect the change; this leads to activation of appropriate muscles to pull the body back. If the vestibular apparatus detects head tilt, vestibulospinal pathways adjust trunk and limb muscles. If visual input conflicts with vestibular input, balance becomes difficult.
The physiological advantage of this system is that posture is maintained automatically without constant conscious effort. This allows the brain to perform other tasks while standing, walking or looking around. If this system fails, the patient may develop unsteady posture, staggering gait, falls, vertigo or inability to maintain balance in darkness.
⚠️ CLINICAL IMPORTANCE
Damage to sensory pathways, vestibular apparatus, cerebellum or brainstem can disturb posture. A patient with vestibular dysfunction may feel spinning sensation and may fall toward the affected side. A patient with cerebellar disease may show wide-based gait and poor coordination. A patient with proprioceptive loss may depend heavily on vision and become unstable when eyes are closed.
MAJOR CONCEPT 2 — Spinal Cord Mechanisms in Posture: Positive Supportive Reaction and Cord Righting Reflexes
🧠 CORE
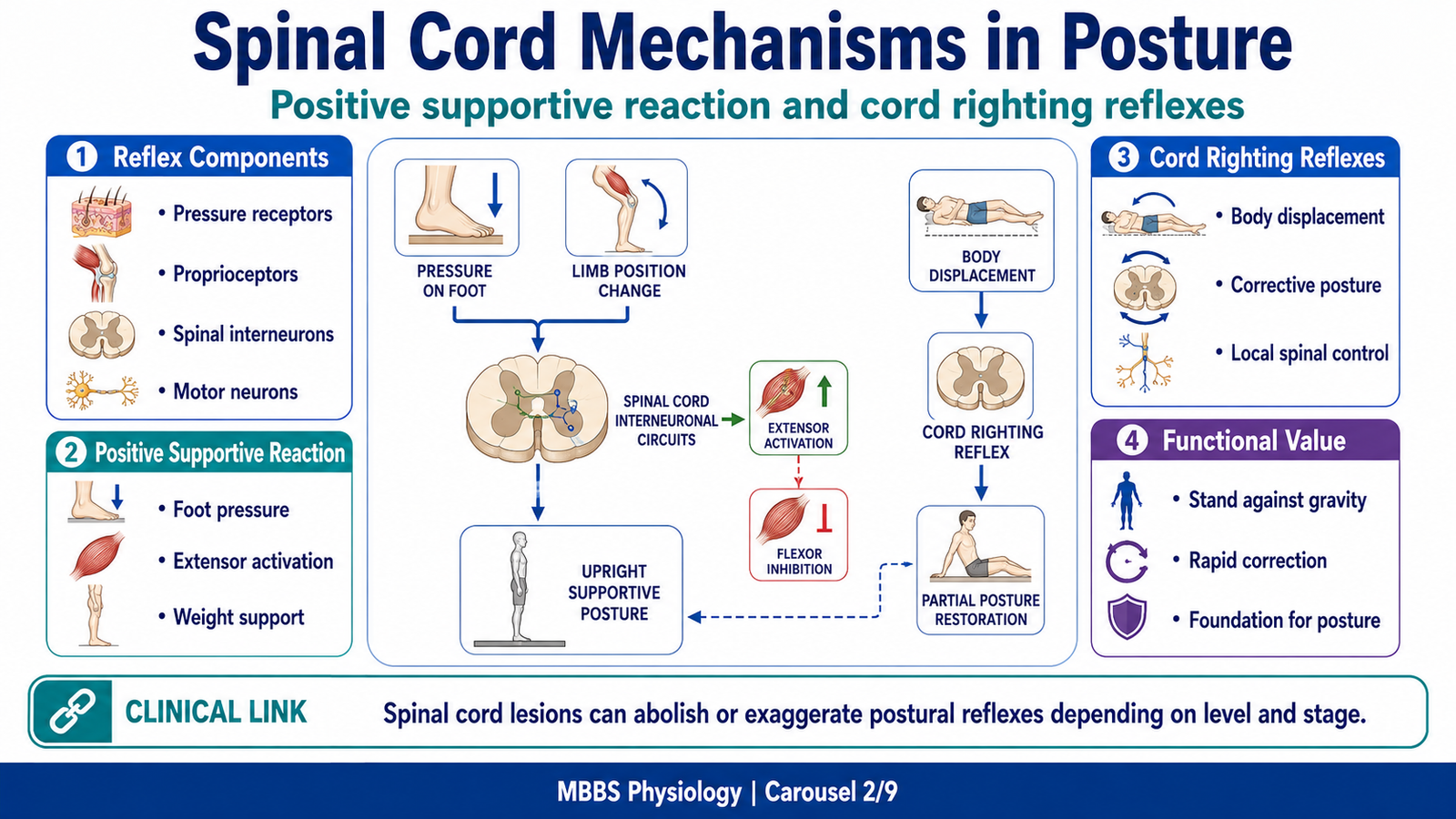
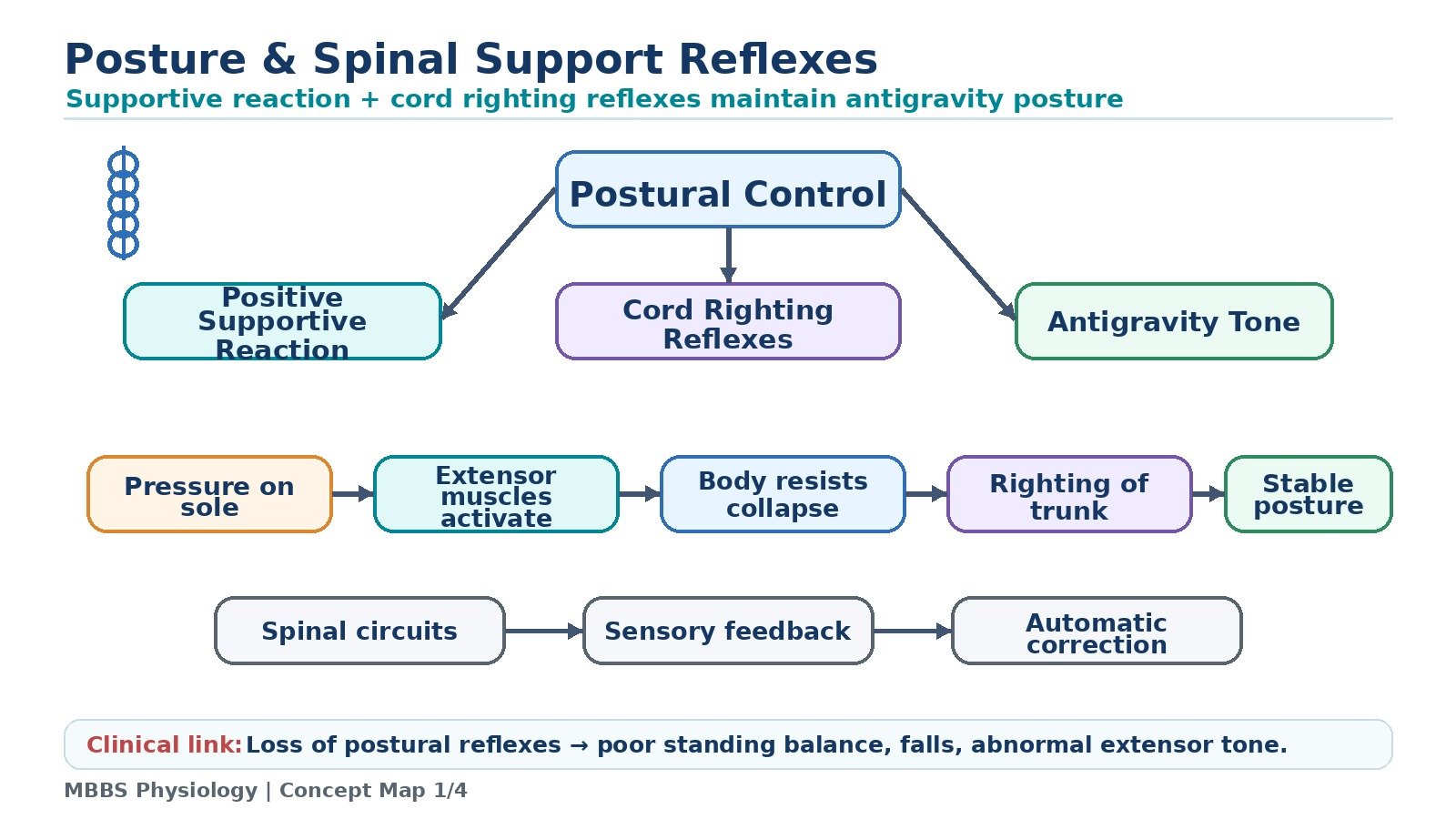
• The spinal cord can generate basic postural reflexes without direct cortical command.
• Positive supportive reaction helps limbs support body weight.
• Cord righting reflexes help restore body position after disturbance.
• These reflexes involve sensory input, spinal interneurons and motor neurons.
• Extensor muscles are especially important for antigravity support.
• Spinal reflexes provide the foundation for higher postural control.
• Brainstem and cerebellum modify spinal reflexes for smooth posture.
🔬 CONCEPT EXPLAINED
The spinal cord is not merely a pathway carrying commands from the brain to muscles. It contains local reflex circuits that can process sensory information and produce meaningful motor responses. These spinal reflexes are especially important for posture because postural correction must be fast. Waiting for conscious cortical processing would make balance slow and inefficient.
Positive Supportive Reaction
The positive supportive reaction is a reflex response in which pressure on the sole or limb causes contraction of extensor muscles, allowing the limb to support body weight. The stimulus is firm pressure applied to the foot or paw, usually combined with stretch of extensor muscles. The purpose of the mechanism is to help the body stand by increasing extensor tone when weight is placed on a limb.
The sequence begins when pressure receptors in the skin and proprioceptors in muscles and joints detect loading of the limb. These impulses enter the spinal cord through sensory afferents. Within the spinal cord, interneurons activate alpha motor neurons supplying extensor muscles. At the same time, inhibitory interneurons reduce activity in opposing flexor muscles. This produces extension at the hip, knee and ankle, allowing the limb to become firm and supportive.
The cause → effect relationship is important: pressure on the sole → sensory afferent activation → spinal interneuron processing → extensor motor neuron activation → limb extension → body weight support. The response is regulated by descending pathways from brainstem and cortex so that it is not excessive. The cerebellum also helps adjust the strength and timing of the response.
The physiological advantage is that the body automatically strengthens the supporting limb when weight is applied. This is essential during standing and walking. If this reaction is impaired, the limb may collapse under body weight. If it becomes exaggerated due to loss of inhibitory control, extensor rigidity may occur.
Cord Righting Reflexes
Cord righting reflexes are spinal-level reflex responses that help restore a disturbed body position. They are more basic than righting reflexes controlled by brainstem and vestibular systems, but they show that the spinal cord contains important postural circuitry.
The initiating event is abnormal position of the trunk or limbs. Sensory receptors detect stretch, joint displacement or pressure changes. The spinal cord then produces coordinated contraction and relaxation of muscles to restore a more stable position. For example, when body weight shifts to one side, spinal circuits can increase extensor tone on the supporting side and adjust flexor activity on the opposite side.
These reflexes exist because posture requires rapid local correction. Their control is modified by descending motor pathways. If higher brain centers are disconnected, spinal reflexes may still occur but they are poorly coordinated and not fully purposeful.
⚠️ CLINICAL IMPORTANCE
Spinal cord injury can abolish or exaggerate postural reflexes depending on the level and stage of injury. In acute spinal shock, reflexes may be absent. Later, reflexes may become exaggerated because descending inhibitory control is lost. This explains why patients with upper motor neuron lesions may show increased tone and exaggerated reflex postural responses.
MAJOR CONCEPT 3 — Stepping and Walking Movements
🧠 CORE
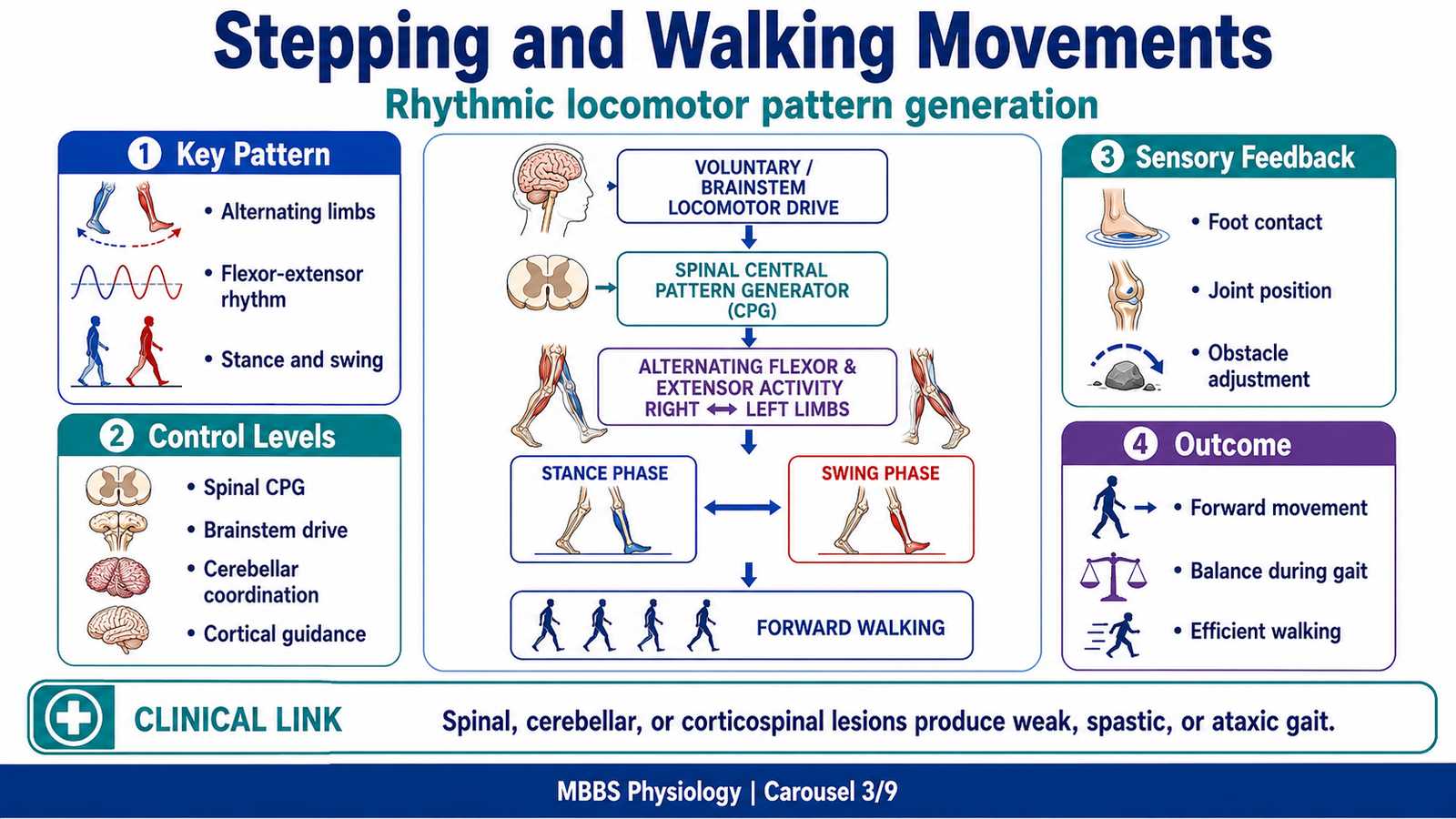
• Walking is a rhythmic alternating movement of limbs.
• Basic stepping patterns can be generated by spinal circuits.
• These circuits are called central pattern generators.
• Flexor and extensor muscles alternate during gait.
• Brainstem centers initiate and regulate locomotor rhythm.
• Cerebellum coordinates balance, timing and smoothness.
• Cortex is needed for voluntary direction, planning and adaptation.
🔬 CONCEPT EXPLAINED
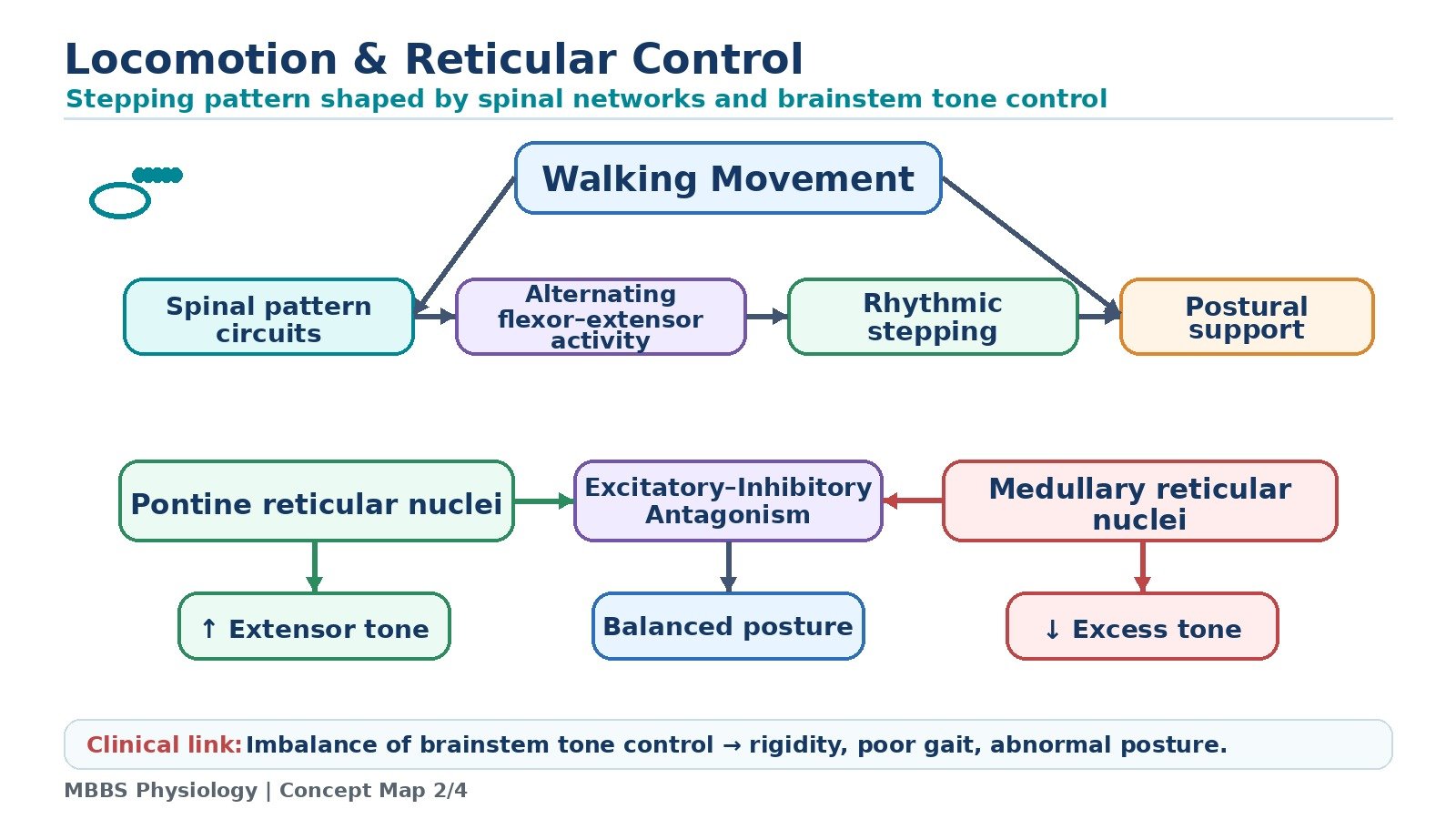
Locomotion is the process by which the body moves from one place to another. Walking appears voluntary, but much of its rhythm is automatic. Once walking begins, the nervous system does not consciously command every muscle contraction. Instead, spinal and brainstem circuits generate rhythmic alternating movements.
The stimulus or initiating event for walking may be voluntary intention from the motor cortex or automatic activation from brainstem locomotor centers. The purpose of locomotor mechanisms is to move the body forward while maintaining balance and support against gravity.
The sequence of walking involves alternating phases. During the stance phase, one limb supports body weight. Extensor muscles are active to keep the limb firm. During the swing phase, the same limb is lifted and moved forward. Flexor muscles become active, and extensor activity is reduced. Then the foot contacts the ground again, and extensor activity increases to support weight. The opposite limb performs the complementary pattern.
At spinal cord level, interneuronal circuits organize alternating flexor and extensor activity. When flexor muscles of one limb are activated, extensor muscles of the same limb are inhibited. At the same time, the opposite limb may show increased extensor activity to maintain support. This reciprocal arrangement is essential because both legs cannot be in swing phase at the same time during normal walking.
The cause → effect relationship is: intention or locomotor drive → activation of spinal pattern generators → alternating flexor-extensor activity → rhythmic stepping → forward movement. Sensory feedback from the feet, joints and muscles modifies each step. If the foot meets an obstacle, reflex circuits can increase flexion to clear the obstacle. If the ground is uneven, proprioceptive and vestibular inputs adjust posture.
The brainstem provides general locomotor drive and postural tone. The cerebellum compares intended movement with actual movement and corrects errors. The cortex is especially important for starting, stopping, changing direction, avoiding obstacles and walking in complex environments.
The physiological advantage is efficiency. Automatic rhythmic control allows walking with minimal conscious effort, while higher centers remain available for planning and environmental awareness.
⚠️ CLINICAL IMPORTANCE
Damage to spinal cord circuits can impair stepping. Damage to motor cortex or corticospinal tract may produce weakness and spastic gait. Cerebellar lesions cause ataxic gait with poor coordination. Vestibular lesions cause imbalance and deviation while walking. Parkinsonism affects automatic locomotor control and may cause shuffling gait, although detailed basal ganglia pathology belongs to later clinical teaching.
MAJOR CONCEPT 4 — Brainstem Reticular Control of Posture: Pontine and Medullary Reticular Nuclei
🧠 CORE
• Reticular formation is a brainstem network involved in posture and tone.
• Pontine reticular nuclei facilitate antigravity extensor muscles.
• Medullary reticular nuclei inhibit excessive extensor tone.
• Posture depends on balance between excitation and inhibition.
• Vestibular nuclei strongly influence extensor tone.
• Cortical and cerebellar inputs regulate reticular activity.
• Loss of balance can produce rigidity or postural instability.
🔬 CONCEPT EXPLAINED
To understand posture, it is essential to understand muscle tone. The body must maintain enough tone to stand against gravity, but not so much tone that movement becomes rigid. This balance is controlled mainly by brainstem centers, especially the reticular formation.
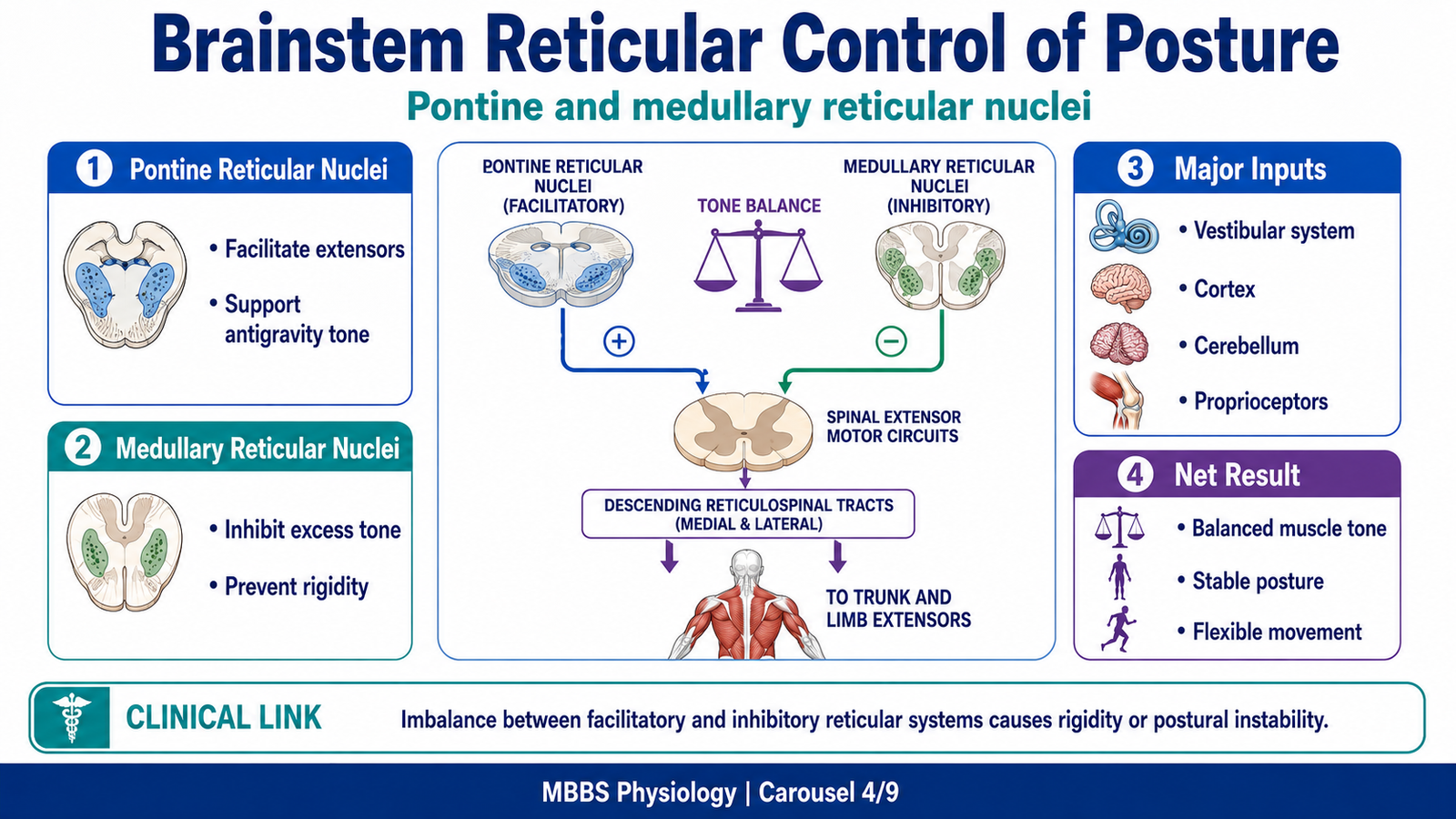
The pontine reticular nuclei have an excitatory effect on antigravity muscles, especially extensor muscles of the trunk and limbs. Their activity helps maintain standing posture. The medullary reticular nuclei have an inhibitory effect on the same antigravity system and prevent excessive rigidity. Thus posture depends on excitatory-inhibitory antagonism between these two groups.
The stimulus or initiating need for this mechanism is the constant pull of gravity on the body. The purpose is to maintain enough extensor tone for support while allowing flexible movement. Without this mechanism, the body would either collapse due to low tone or become rigid due to excessive tone.
The sequence begins with sensory information from proprioceptors, vestibular apparatus and cortex reaching brainstem centers. Pontine reticular nuclei send excitatory signals through reticulospinal tracts to spinal motor circuits that activate extensor muscles. Medullary reticular nuclei send inhibitory signals that reduce excessive activity in the same systems. The cerebellum and motor cortex regulate both centers according to body position and intended movement.
The cause → effect relationship is: increased pontine reticular drive → increased extensor tone → improved antigravity support. On the other hand, increased medullary reticular inhibition → reduced extensor tone → prevention of rigidity. Proper posture requires both systems to be balanced.
Vestibular nuclei also facilitate extensor tone through vestibulospinal tracts. This becomes important when the head position changes. For example, if the head tilts, vestibular signals adjust extensor activity to maintain body balance. Therefore, the vestibular apparatus and reticular formation work together in postural control.
The physiological advantage is controlled stability. The body can stand firmly but still move smoothly. If the excitatory system dominates abnormally, extensor rigidity may occur. If inhibitory control is excessive or excitatory pathways are damaged, posture becomes weak and unstable.
⚠️ CLINICAL IMPORTANCE
Brainstem lesions can disturb postural tone. Severe imbalance between facilitatory and inhibitory systems may produce abnormal rigidity. Loss of higher inhibitory control can exaggerate extensor tone. Clinically, abnormal posturing in neurological disease reflects disruption of brainstem and descending motor control pathways.
MAJOR CONCEPT 5 — Physiologic Anatomy of the Vestibular Apparatus
🧠 CORE
• Vestibular apparatus is located in the inner ear within the petrous temporal bone.
• It consists of utricle, saccule and three semicircular ducts.
• Utricle and saccule are otolith organs.
• Semicircular ducts detect rotational movement.
• Sensory receptors are hair cells.
• Hair cells respond to bending caused by endolymph or otolith movement.
• Vestibular nerve carries signals to vestibular nuclei and cerebellum.
🔬 CONCEPT EXPLAINED
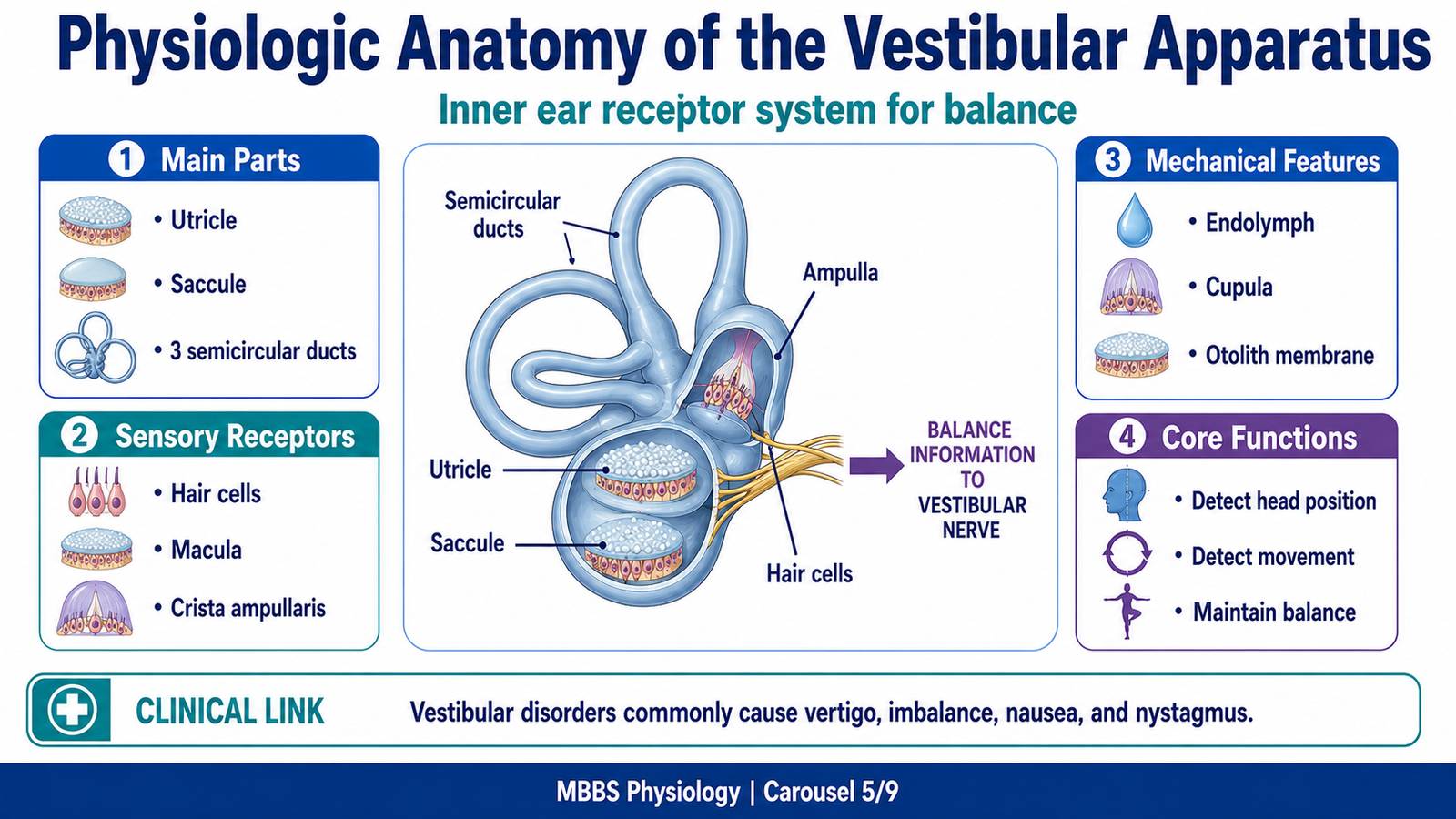
The vestibular apparatus is the sensory organ of balance. It is located in the membranous labyrinth of the inner ear. Although small in size, it provides continuous information about head position and movement. This information is essential because the head contains the eyes and brain; therefore, knowing head position is central to orientation of the whole body.
The vestibular apparatus has two major functional parts. The utricle and saccule detect static head position and linear acceleration. The semicircular ducts detect angular or rotational acceleration. Together they allow the nervous system to detect whether the head is tilted, moving forward, moving upward, rotating, or turning.
The receptor cells are hair cells. These cells have hair-like projections that bend when mechanical forces act on them. Bending in one direction increases receptor activity, while bending in the opposite direction decreases activity. This is important because the vestibular system does not simply detect movement; it detects direction of movement.
The vestibular apparatus is filled with endolymph. In semicircular ducts, movement of endolymph bends sensory structures during head rotation. In utricle and saccule, heavy otolith crystals shift in response to gravity or linear acceleration and bend hair cells. Mechanical bending is converted into electrical signals that travel through the vestibular division of the vestibulocochlear nerve.
The physiological advantage of this structure is that mechanical movement of the head is converted into precise neural information. The brain can then adjust posture, eye position and perception of balance. If the vestibular apparatus fails, the brain receives incorrect or unequal signals from the two ears, producing vertigo, nystagmus and imbalance.
⚠️ CLINICAL IMPORTANCE
Vestibular dysfunction commonly produces vertigo, nausea, imbalance and abnormal eye movements. Because vestibular apparatus is closely related to cochlea, inner ear disorders may sometimes affect both balance and hearing. However, hearing mechanisms are separate from vestibular mechanisms.
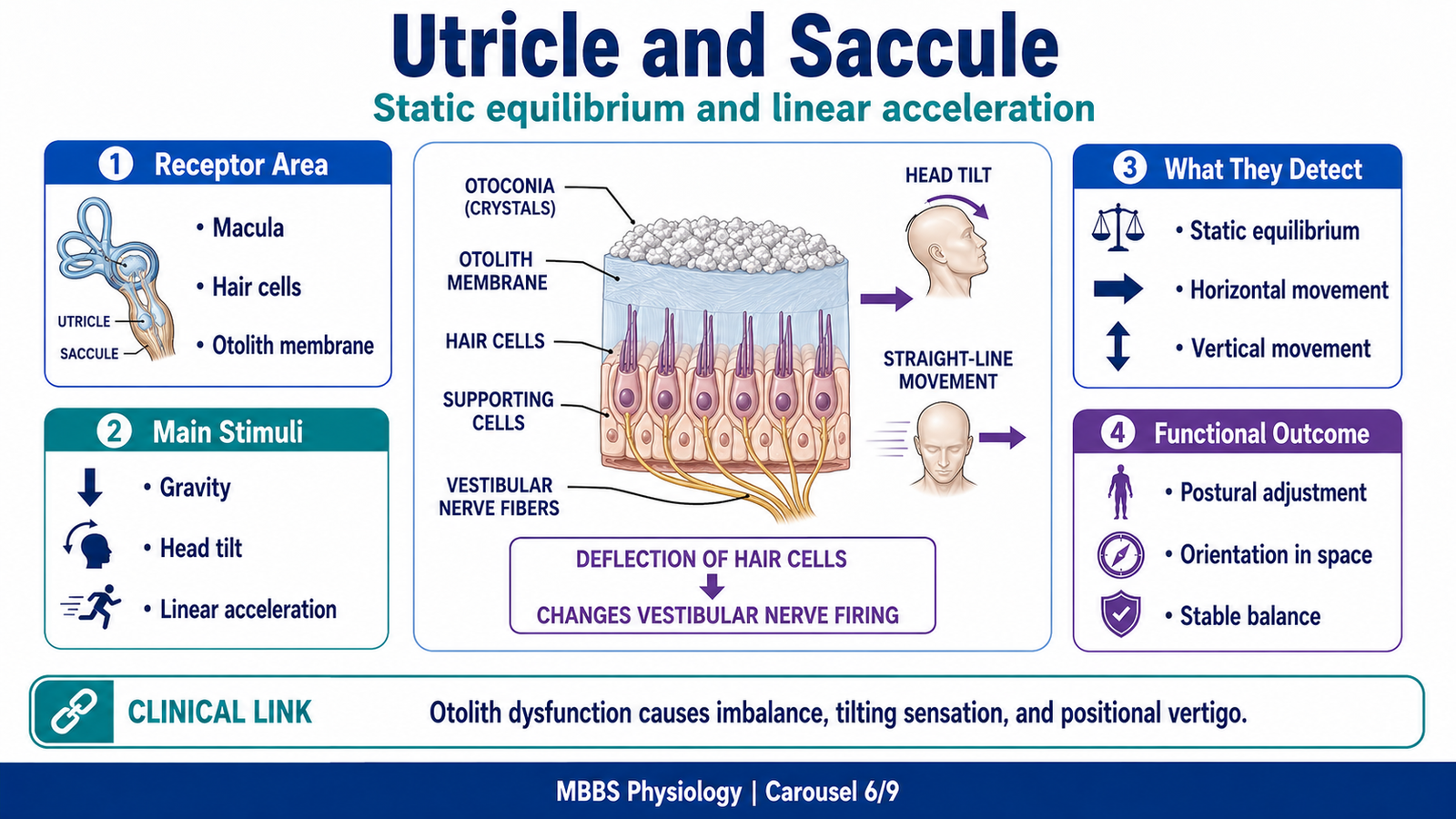
MAJOR CONCEPT 6 — Utricle and Saccule: Static Equilibrium and Linear Acceleration
🧠 CORE
• Utricle and saccule are otolith organs.
• Their sensory receptor area is called macula.
• They detect head position relative to gravity.
• They also detect linear acceleration and deceleration.
• Otoliths add weight and inertia to the gelatinous layer.
• Hair cell bending changes vestibular nerve firing.
• They are essential for static equilibrium.
🔬 CONCEPT EXPLAINED
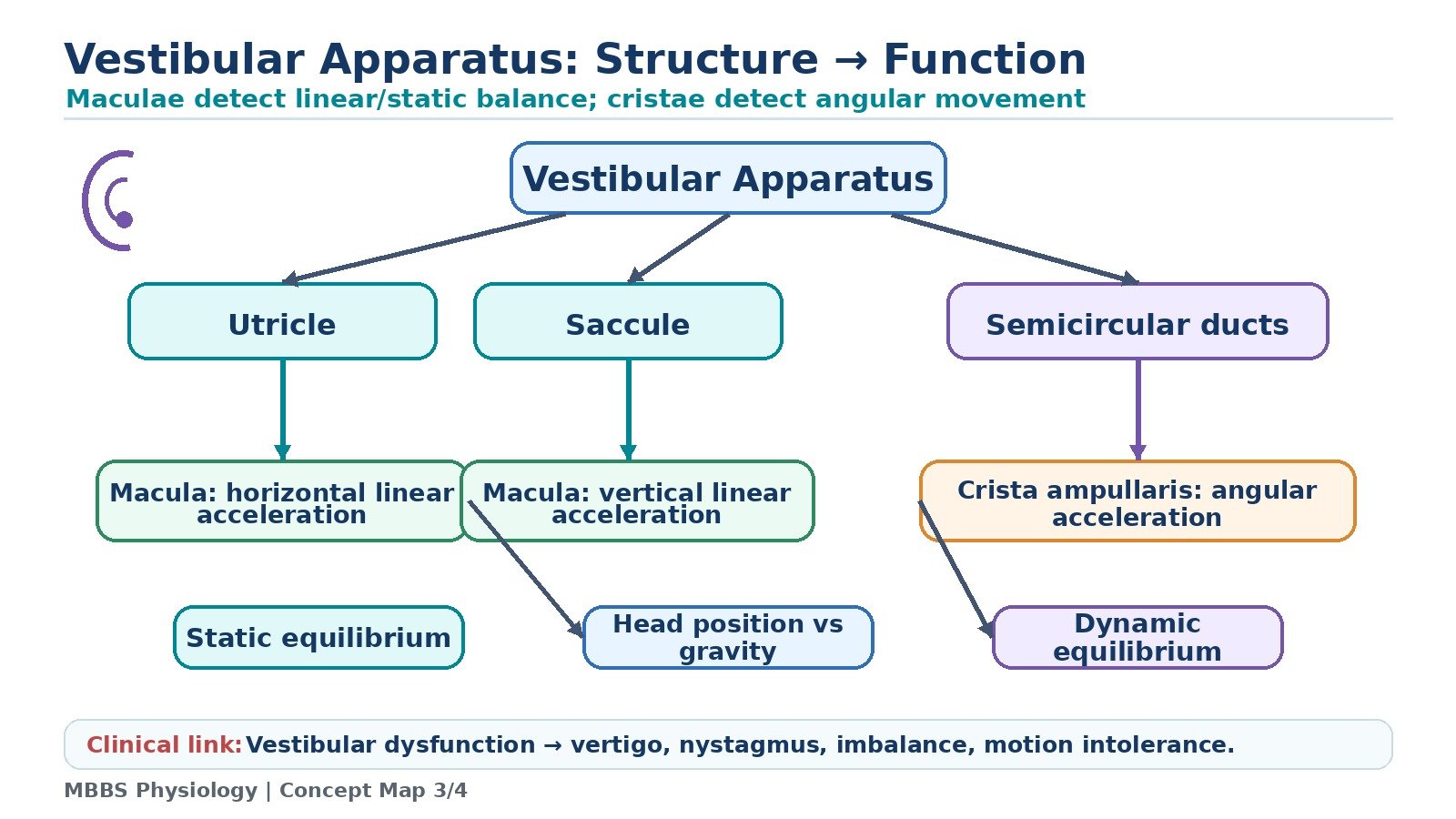
Static equilibrium refers to awareness of head position in relation to gravity, especially when the head is still or moving in a straight line. The utricle and saccule are responsible for this function. They are called otolith organs because their sensory membrane contains tiny calcium carbonate crystals called otoliths or otoconia.
The stimulus or initiating event for utricle and saccule activity is head tilt, gravity, or linear acceleration. For example, when a person tilts the head forward, starts moving in a car, or moves upward in an elevator, the otolith organs detect the change. The purpose of the mechanism is to inform the brain about head orientation and straight-line movement so that posture and eye position can be adjusted.
The sequence begins when gravity or linear acceleration causes the otolith membrane to shift. Because the otoliths are heavier than surrounding fluid, they create a dragging force on the gelatinous layer. This bends the hair cells in the macula. Bending toward the excitatory direction increases firing of vestibular nerve fibers; bending in the opposite direction decreases firing. The brain interprets this change in firing as head tilt or linear acceleration.
The utricle is especially sensitive to horizontal movements and head tilt in the horizontal plane. The saccule is more sensitive to vertical movements. Together, they provide a three-dimensional sense of static head position and linear movement.
The cause → effect relationship is: head tilt or linear acceleration → otolith membrane displacement → hair cell bending → altered vestibular nerve firing → brainstem and cerebellar processing → postural and eye adjustments.
Control and regulation occur through central interpretation. The vestibular nuclei compare input from both ears and integrate it with visual and proprioceptive information. If signals from both sides are equal and appropriate, balance is stable. If one side gives abnormal signals, the brain interprets it as movement even when the body is still.
The physiological advantage is that the body can maintain balance even with eyes closed. For example, a person can sense head tilt in darkness because utricle and saccule do not require vision.
⚠️ CLINICAL IMPORTANCE
Damage or irritation of otolith organs can disturb static equilibrium. Patients may feel tilting, floating, swaying or imbalance. Otolith dysfunction can contribute to positional vertigo. In basic MBBS terms, the key exam concept is that utricle and saccule detect static equilibrium and linear acceleration, not angular rotation.
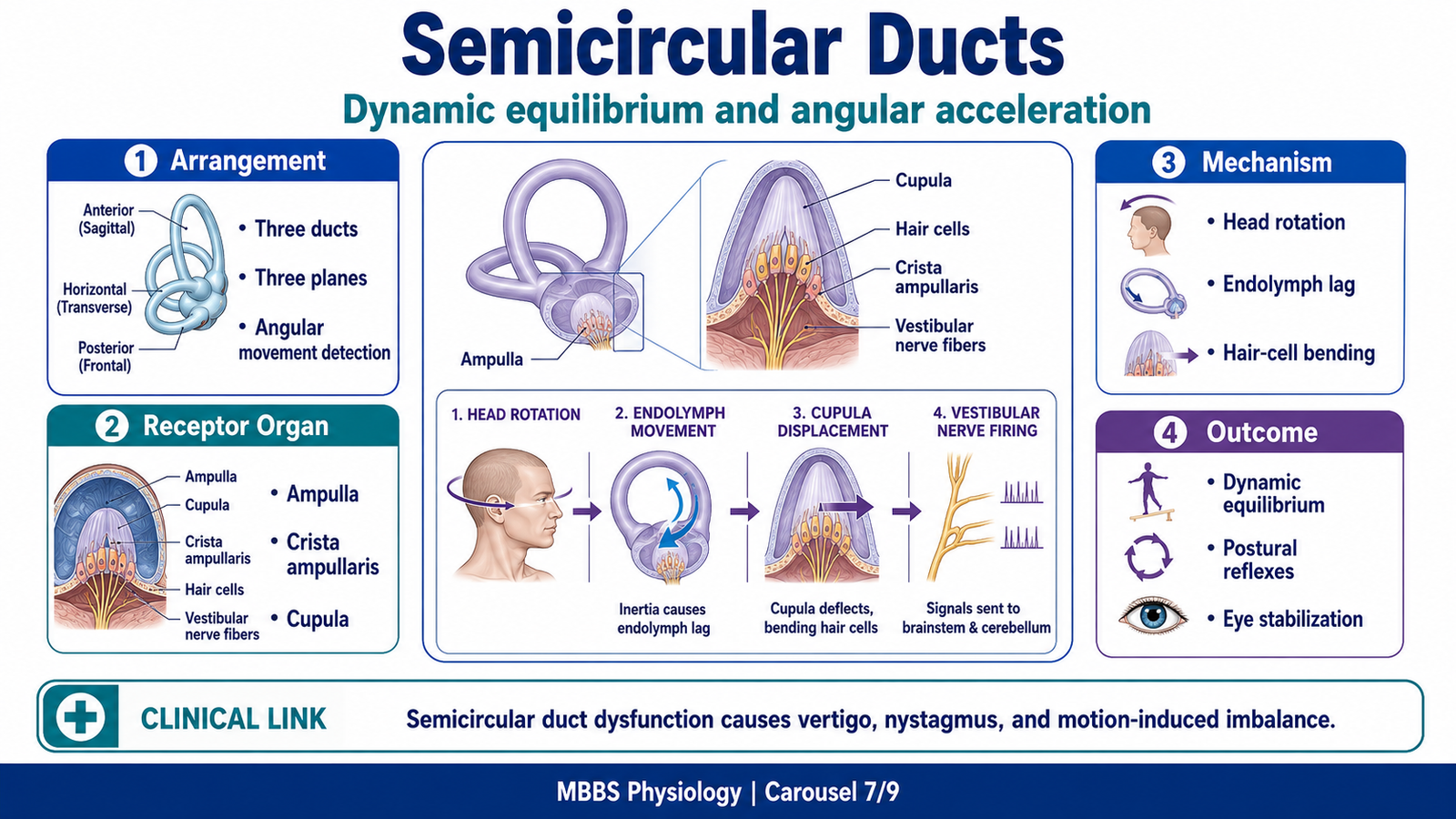
MAJOR CONCEPT 7 — Semicircular Ducts: Dynamic Equilibrium and Angular Acceleration
🧠 CORE
• There are three semicircular ducts on each side.
• They are arranged approximately at right angles to each other.
• They detect rotational or angular acceleration of the head.
• The receptor organ is crista ampullaris in the ampulla.
• Hair cells project into a gelatinous cupula.
• Endolymph movement bends the cupula during rotation.
• They are essential for dynamic equilibrium.
🔬 CONCEPT EXPLAINED
While utricle and saccule detect static position and linear movement, the semicircular ducts detect rotation of the head. This is called dynamic equilibrium because it is especially important during movement. The head can rotate in different planes, so three semicircular ducts are needed: anterior, posterior and lateral. Their arrangement at nearly right angles allows detection of rotation in all directions.
The stimulus or initiating event is angular acceleration of the head, such as turning the head to the right, nodding, or tilting sideways. The purpose of the mechanism is to detect rotational movement and allow rapid correction of posture and eye position.
The sequence begins when the head starts rotating. The bony and membranous labyrinth move with the skull, but the endolymph inside tends to lag behind because of inertia. This relative movement of endolymph pushes the cupula in the ampulla. Hair cells embedded in the cupula bend. Depending on the direction of bending, vestibular nerve firing increases or decreases.
The cause → effect relationship is: head rotation → endolymph inertia → cupula displacement → hair cell bending → altered vestibular nerve firing → vestibular nuclei activation → eye and postural reflexes.
An important concept is that semicircular ducts mainly detect changes in rotational velocity, not constant rotation. When rotation continues at a constant speed, endolymph eventually catches up, and receptor stimulation decreases. When rotation stops, endolymph continues moving briefly, causing a sensation of rotation in the opposite direction. This explains dizziness after spinning.
Control and regulation depend on paired activity between ducts on both sides. When the head turns to one side, the corresponding semicircular duct on that side is excited while the paired duct on the opposite side is inhibited. The brain reads this difference as direction of rotation.
The physiological advantage is rapid detection of head movement. This is essential because eyes and posture must be adjusted almost immediately during head rotation. If semicircular duct function is impaired, the patient may experience vertigo, imbalance and abnormal eye movements.
⚠️ CLINICAL IMPORTANCE
Semicircular duct dysfunction causes disturbed dynamic equilibrium. Patients may complain of spinning sensation, especially with head movement. Nystagmus occurs because vestibular input strongly connects with eye movement nuclei. A classic exam point is that semicircular ducts detect angular acceleration, while utricle and saccule detect static equilibrium and linear acceleration.
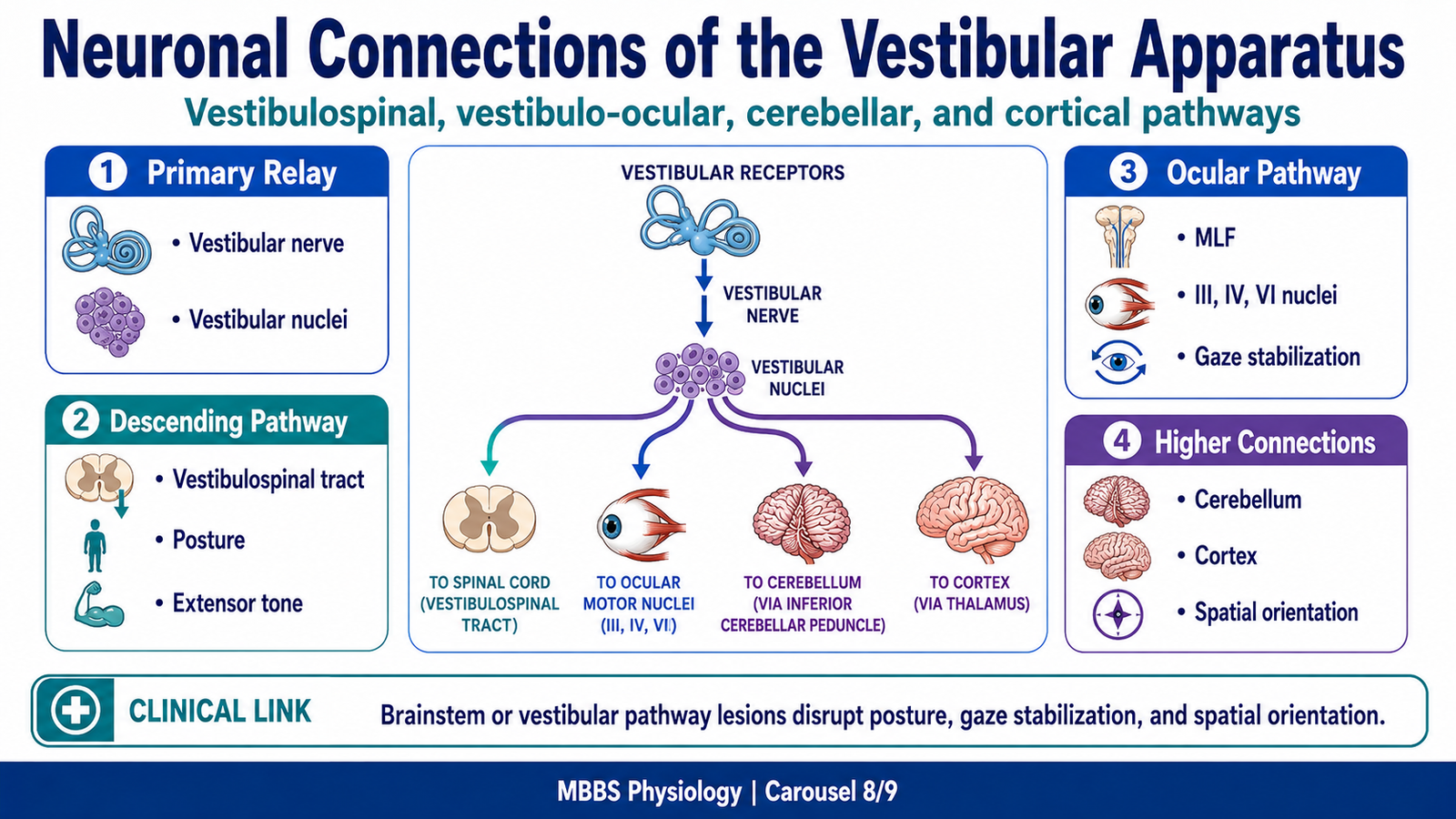
MAJOR CONCEPT 8 — Neuronal Connections of the Vestibular Apparatus
🧠 CORE
• Vestibular hair cells send signals through vestibular nerve.
• Vestibular nerve enters brainstem at pontomedullary junction.
• Main relay is vestibular nuclei.
• Vestibular nuclei connect to spinal cord, cerebellum, ocular motor nuclei and cortex.
• Vestibulospinal tracts control posture and extensor tone.
• Vestibulo-ocular pathways stabilize gaze.
• Cerebellum refines vestibular responses.
🔬 CONCEPT EXPLAINED
The vestibular apparatus is only the receptor part of the equilibrium system. Its signals must reach motor centers to produce useful responses. Therefore, vestibular neuronal connections are essential for converting head movement information into posture, eye movement and conscious perception of balance.
The stimulus begins as mechanical movement of hair cells in utricle, saccule or semicircular ducts. This changes firing in vestibular nerve fibers. The vestibular nerve carries the information to the vestibular nuclei in the brainstem. Some fibers also project directly to the cerebellum, especially areas involved in balance.
The purpose of these connections is to distribute vestibular information to all systems that need it. The spinal cord needs vestibular input to adjust body posture. The eye movement nuclei need it to stabilize gaze. The cerebellum needs it to coordinate balance. The cortex needs it for conscious awareness of head position and movement.
Vestibulospinal Connections
Vestibular nuclei send descending fibers to the spinal cord through vestibulospinal tracts. These pathways influence motor neurons controlling neck, trunk and limb muscles. Their main function is to adjust muscle tone, especially extensor tone, according to head position and movement.
The cause → effect relationship is: head tilt → vestibular receptor activation → vestibular nuclei → vestibulospinal tract → activation of appropriate antigravity muscles → correction of posture.
Vestibulo-Cerebellar Connections
The cerebellum receives vestibular information and compares it with proprioceptive and motor signals. It helps make balance responses smooth and accurate. Without cerebellar refinement, vestibular reflexes may become poorly coordinated.
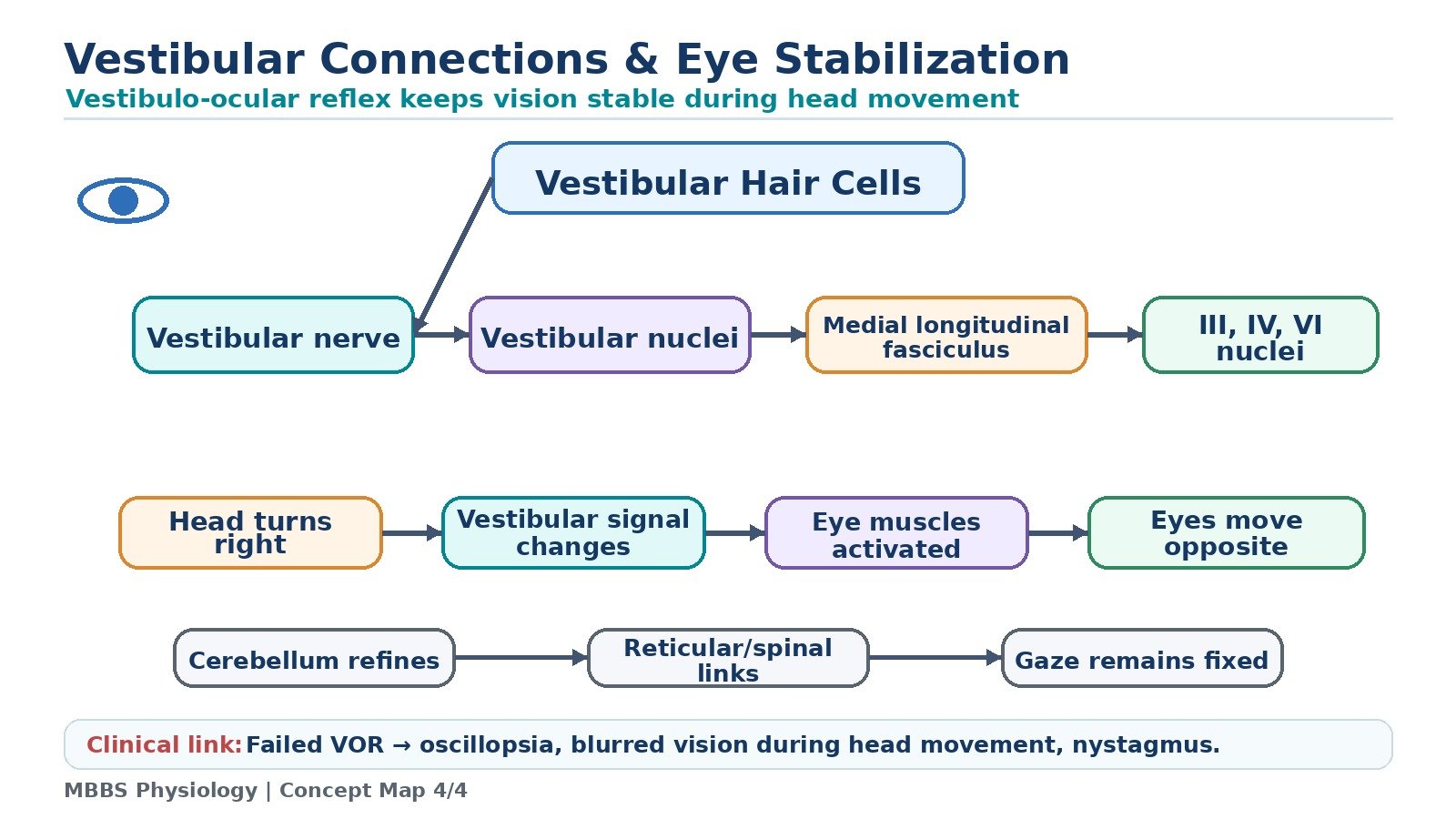
Vestibulo-Ocular Connections
Vestibular nuclei connect to the nuclei of cranial nerves III, IV and VI through pathways including the medial longitudinal fasciculus. These connections control extraocular muscles and form the basis of the vestibulo-ocular reflex.
Cortical Connections
Vestibular information also reaches higher centers, allowing conscious perception of movement and spatial orientation. This is why vestibular stimulation can produce a subjective sensation of spinning or falling.
The physiological advantage of this network is integration. A single head movement produces coordinated responses in posture, eye position and perception. If the connections fail, the receptors may detect movement, but the body cannot respond properly.
⚠️ CLINICAL IMPORTANCE
Lesions of vestibular nuclei or pathways can produce vertigo, nystagmus, imbalance and abnormal postural reflexes. Brainstem lesions may affect vestibular connections along with other cranial nerve functions. Cerebellar involvement produces severe balance disturbance and ataxia.
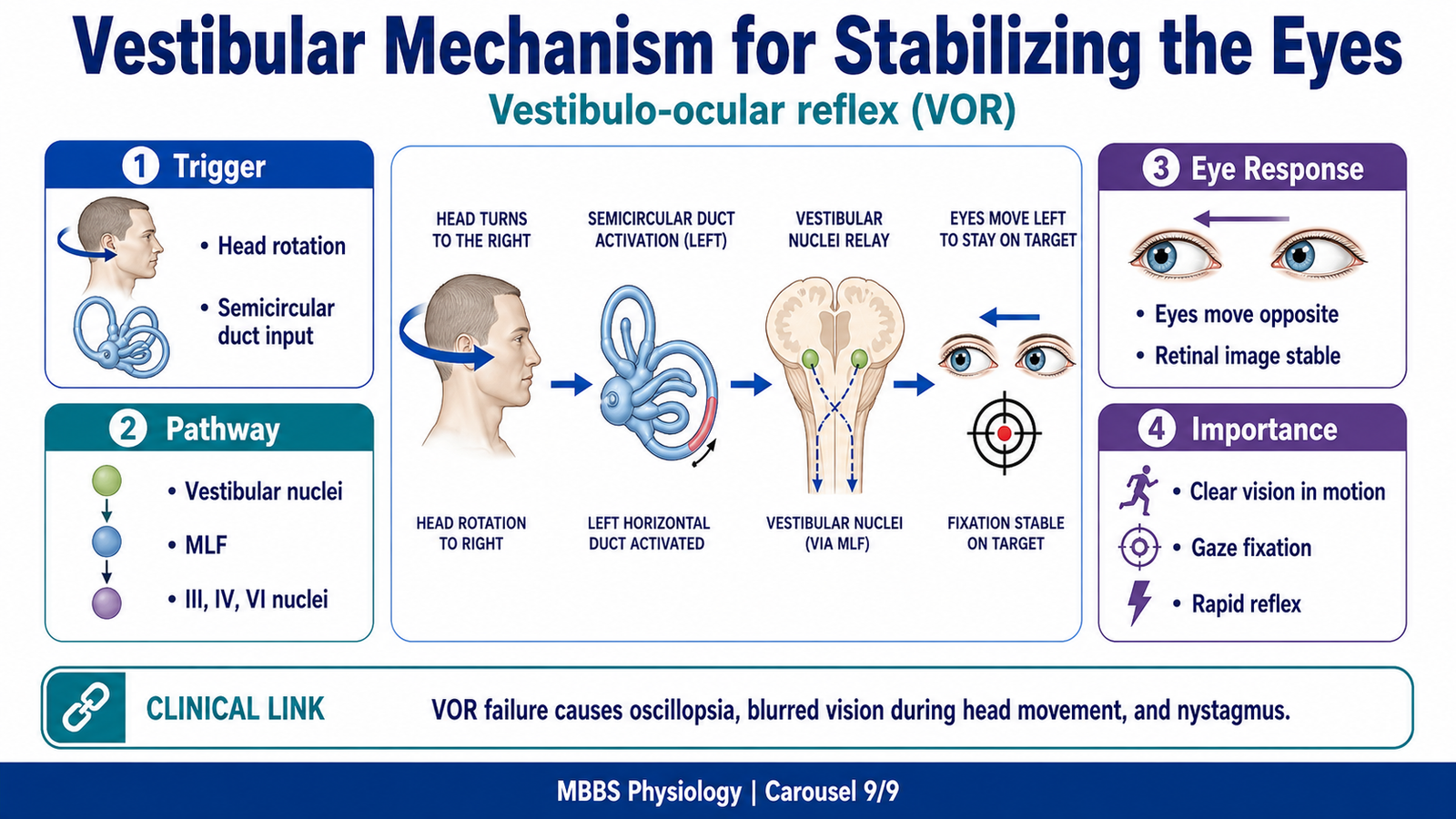
MAJOR CONCEPT 9 — Vestibular Mechanism for Stabilizing the Eyes
🧠 CORE
• Eye stabilization during head movement is achieved by vestibulo-ocular reflex.
• The reflex keeps images stable on the retina.
• Semicircular ducts detect head rotation.
• Vestibular nuclei activate ocular motor nuclei.
• Eyes move opposite to the direction of head movement.
• This reflex works rapidly and automatically.
• Failure causes blurred vision during head movement and nystagmus.
🔬 CONCEPT EXPLAINED
When the head moves, the eyes must move in the opposite direction to keep vision stable. Without this mechanism, every head movement would make the visual world appear blurred or jumpy. The vestibular system solves this problem through the vestibulo-ocular reflex.
The stimulus or initiating event is head movement, especially rotation detected by semicircular ducts. The purpose of the reflex is to stabilize images on the retina during head movement. This is essential for clear vision while walking, turning the head or moving rapidly.
The sequence begins when the head turns, for example to the right. The right horizontal semicircular duct is stimulated, while the left paired duct is relatively inhibited. This difference in vestibular nerve firing reaches the vestibular nuclei. From there, signals pass to ocular motor nuclei controlling the extraocular muscles. The eyes are moved to the left, opposite the head movement. As a result, the visual image remains fixed on the retina.
The cause → effect relationship is: head turns right → right semicircular duct excitation → vestibular nuclei activation → ocular motor nuclei stimulation → eyes move left → visual fixation maintained.
This reflex is extremely fast because it does not require conscious visual processing. It is mainly controlled at brainstem level, though cerebellum helps calibrate its accuracy. The reflex also works in darkness because it depends on vestibular input, not visual input.
The physiological advantage is stable vision during movement. For example, a person can walk while keeping eyes fixed on an object. If the vestibulo-ocular reflex is impaired, the patient may experience blurred vision during head movement, oscillopsia, vertigo or nystagmus.
Nystagmus occurs when vestibular imbalance drives rhythmic eye movement. There is usually a slow phase caused by vestibular tone imbalance and a fast corrective phase generated by central mechanisms. At MBBS level, the important point is that abnormal vestibular input can produce involuntary rhythmic eye movements.
⚠️ CLINICAL IMPORTANCE
Vestibulo-ocular reflex testing is important in clinical neurology and ENT. Abnormal eye movements can indicate vestibular dysfunction or brainstem involvement. Patients with vestibular disease may complain that the environment appears to move when they turn their head.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
The spinal cord contains interneuronal circuits that can produce rapid reflex responses. This structure allows the body to generate basic supportive and corrective postural reflexes without waiting for conscious command. The outcome is fast postural adjustment.
The reticular formation is widely connected with cortex, cerebellum, vestibular nuclei and spinal cord. This structure allows it to regulate overall muscle tone. The outcome is balanced antigravity support without excessive rigidity.
The vestibular apparatus is located in the inner ear and contains mechanically sensitive hair cells. This structure allows head movement and position to be converted into neural signals. The outcome is awareness of head position and rapid postural correction.
The utricle and saccule contain otolith crystals over hair cells. Their structure makes them sensitive to gravity and linear acceleration. The outcome is static equilibrium and detection of straight-line movement.
The semicircular ducts are arranged in three planes and contain endolymph and cupula-based receptors. Their structure makes them sensitive to angular acceleration. The outcome is dynamic equilibrium and detection of head rotation.
The vestibular nuclei act as integration centers. They connect vestibular receptors with spinal cord, cerebellum, ocular motor nuclei and cortex. The outcome is coordinated balance, posture, eye movement and perception.
The vestibulo-ocular pathway connects vestibular nuclei with ocular motor nuclei. This structure allows eyes to move opposite the head movement. The outcome is stable vision during motion.
🩺 5️⃣ Clinical Correlation
1. Vertigo
Vertigo is a false sensation of spinning or movement. It usually occurs when vestibular signals from the two sides are unequal. The brain interprets this asymmetry as head movement even when the person is still. This produces dizziness, nausea, imbalance and sometimes nystagmus.
2. Nystagmus
Nystagmus is involuntary rhythmic eye movement. Vestibular imbalance can drive abnormal signals to ocular motor nuclei. The result is slow eye drift followed by fast corrective movement. It is an important clinical sign of vestibular or brainstem dysfunction.
3. Ataxic Gait
Ataxic gait occurs when balance and coordination are disturbed, commonly due to cerebellar or vestibular dysfunction. The patient may walk with a broad base and irregular steps. The mechanism is failure to coordinate postural correction with limb movement.
4. Postural Instability
Postural instability may occur due to vestibular dysfunction, proprioceptive loss, cerebellar disease or brainstem pathway lesions. The underlying mechanism is failure to detect body position or failure to generate proper corrective motor output.
5. Abnormal Extensor Tone
If pontine facilitatory influences dominate or inhibitory control is lost, extensor tone may become excessive. This can contribute to rigidity and abnormal posturing. If extensor tone is insufficient, the patient may be unable to stand properly.
6. Blurring of Vision During Head Movement
If vestibulo-ocular reflex is impaired, eyes cannot move appropriately opposite to head movement. The image slips on the retina, causing blurred vision or oscillopsia during movement.
📌 6️⃣ Summary Points
- Posture depends on integration of vestibular, proprioceptive, visual and cutaneous inputs.
- Positive supportive reaction helps the limb support body weight by increasing extensor tone.
- Cord righting reflexes are basic spinal mechanisms that help restore posture.
- Walking depends on spinal rhythmic circuits, brainstem drive, cerebellar coordination and cortical control.
- Pontine reticular nuclei facilitate extensor tone; medullary reticular nuclei inhibit excessive extensor tone.
- Vestibular apparatus is located in the inner ear and consists of utricle, saccule and semicircular ducts.
- Utricle and saccule detect static equilibrium and linear acceleration.
- Semicircular ducts detect angular acceleration and dynamic equilibrium.
- Vestibular nuclei connect with spinal cord, cerebellum, ocular motor nuclei and cortex.
- Vestibulospinal pathways help maintain posture and antigravity tone.
- Vestibulo-ocular reflex stabilizes gaze by moving eyes opposite to head movement.
- Vestibular dysfunction commonly causes vertigo, imbalance, nystagmus and unsteady gait.