
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Higher cortical functions are the advanced functions of the cerebral cortex that allow a person to think, understand language, speak, remember, learn, behave appropriately, and respond emotionally to the environment.
These functions are mainly performed by the cerebral association areas, especially in the frontal, parietal, temporal, and occipital lobes. Unlike primary sensory or motor areas, association areas do not simply receive sensation or produce movement; they interpret, integrate, plan, and give meaning to information.
Speech and language depend on specialized cortical areas, mainly Broca’s area and Wernicke’s area, along with auditory, visual, motor, and association pathways. Damage to these areas produces different types of aphasia.
Memory depends on synaptic changes in the cerebral cortex and limbic structures, especially the hippocampus. Emotional behavior, motivation, fear, reward, autonomic responses, and endocrine control are closely linked to the limbic system and hypothalamus.
Clinically, this topic is important because strokes, trauma, tumors, neurodegenerative disease, and psychiatric disorders may disturb speech, memory, emotions, behavior, and autonomic/endocrine functions.
🔹 2️⃣ Foundation Concepts
Key Definitions
• Higher cortical functions: Advanced brain functions such as language, speech, memory, learning, reasoning, emotion, behavior, and consciousness.
• Association areas: Cortical areas that integrate information from multiple sensory and motor regions to produce meaningful perception, thought, planning, and behavior.
• Speech: The motor expression of language through coordinated movements of respiratory, laryngeal, pharyngeal, oral, and facial muscles.
• Language: A system of symbols used for communication, including spoken, written, heard, and read language.
• Broca’s area: Motor speech area located mainly in the dominant frontal lobe; responsible for planning and production of speech.
• Wernicke’s area: Sensory language area located in the dominant posterior temporal region; responsible for understanding spoken and written language.
• Aphasia: Loss or disturbance of language function due to brain lesion, usually in the dominant cerebral hemisphere.
• Memory: Storage and recall of information in the nervous system.
• Synaptic facilitation: Increased efficiency of synaptic transmission, forming the basis of learning and memory.
• Synaptic inhibition: Reduction of synaptic activity, important for filtering unnecessary information.
• Memory consolidation: Process by which short-term memory is converted into stable long-term memory.
• Limbic system: A functional ring of cortical and subcortical structures involved in emotion, motivation, memory, reward, autonomic responses, and behavior.
• Hypothalamus: Major regulatory center connecting limbic, autonomic, and endocrine systems.
🔹 3️⃣ Core Learning — Curriculum Coverage
1 — Functional Organization of Cerebral Cortex and Association Areas
🧠 CORE
• Cerebral cortex has primary sensory, primary motor, and association areas.
• Primary areas receive or produce simple functions.
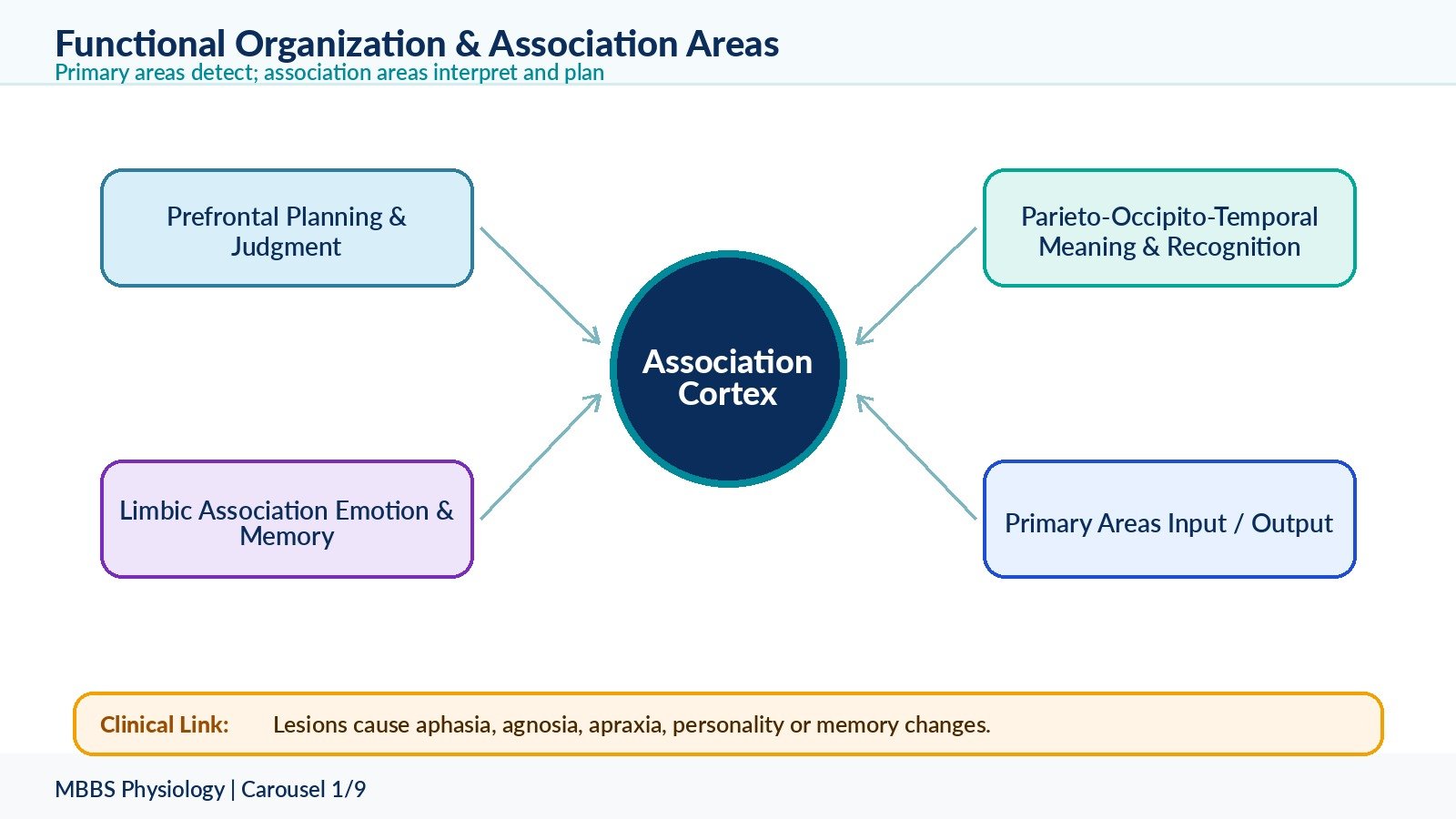
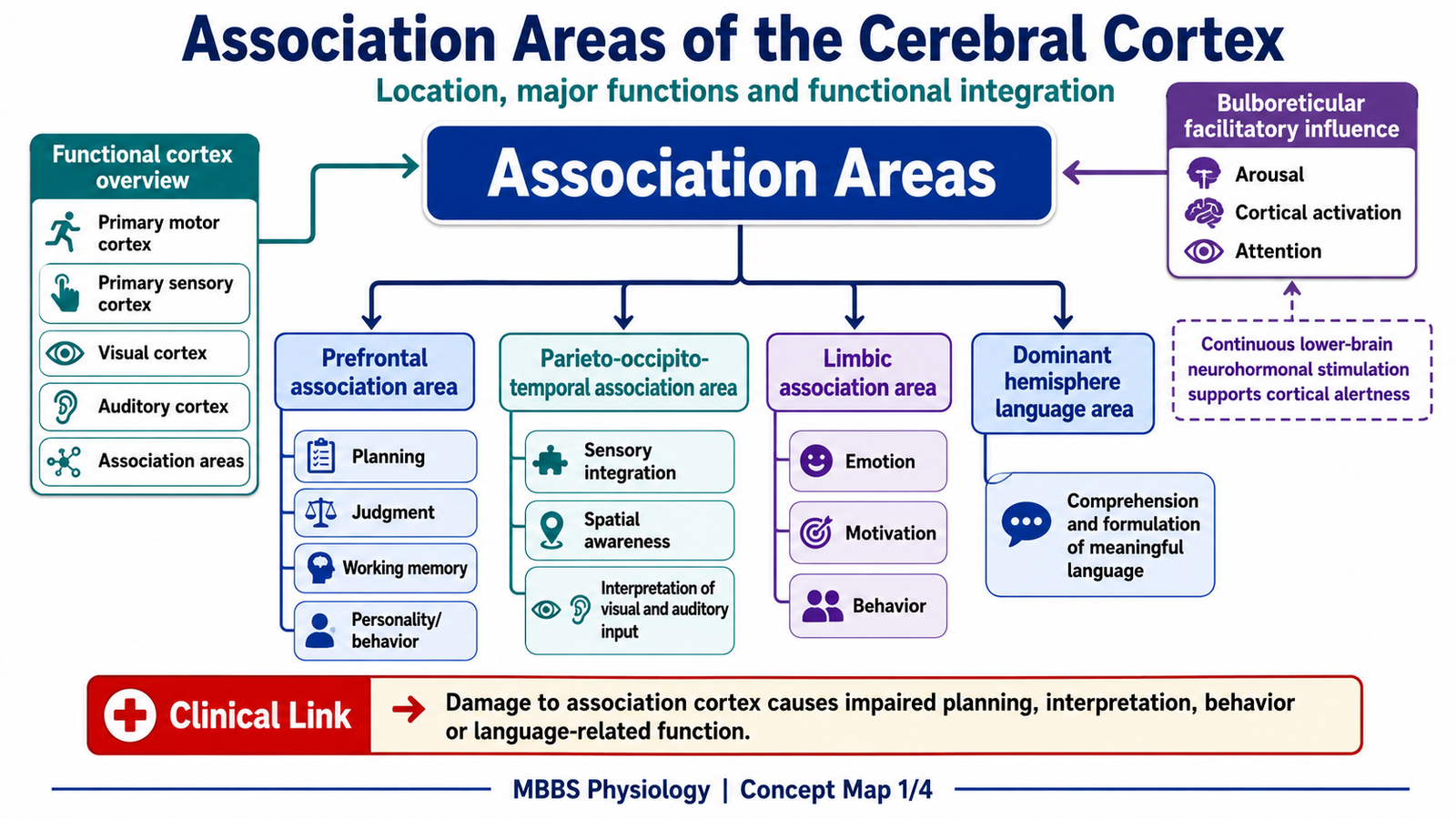
• Association areas interpret, integrate, plan, and give meaning.
• Major association areas include prefrontal, parieto-occipito-temporal, and limbic association areas.
• Most higher cortical functions depend on communication between multiple cortical areas.
• Association areas are especially well developed in humans.
• Damage causes complex deficits such as aphasia, agnosia, apraxia, personality change, and memory disturbance.
🔬 CONCEPT EXPLAINED
The cerebral cortex is not only a surface for receiving sensations and producing voluntary movements. It is also the main organ of interpretation, planning, decision-making, language, memory, and personality. To understand higher cortical functions, first separate the cortex into primary areas and association areas.
Primary sensory areas receive basic sensory information. For example, the primary visual cortex receives visual impulses, and the primary auditory cortex receives sound impulses. Primary motor cortex sends commands for voluntary movement. However, seeing light or hearing sound alone does not create understanding. Meaning is produced when information is processed by association areas.
Association areas receive inputs from multiple cortical and subcortical regions. Their purpose is to combine different types of information and produce meaningful responses. For example, when a student sees a written word, the visual cortex detects the letters, but association areas interpret the word, relate it to memory, and connect it to language areas so that it can be read aloud or understood.
The major association areas are:
1. Prefrontal association area
This lies anterior to the premotor cortex in the frontal lobe. It is responsible for planning, judgment, decision-making, social behavior, working memory, personality, and control of emotional responses.
2. Parieto-occipito-temporal association area
This lies at the junction of parietal, occipital, and temporal lobes. It integrates somatic sensation, vision, and hearing. It is important for language comprehension, spatial orientation, body awareness, object recognition, and reading.
3. Limbic association area
This is located mainly on the medial and inferior surfaces of the cerebral hemispheres. It is related to emotion, motivation, memory, and behavior.
The physiological advantage of association areas is that they allow the brain to move beyond reflexes and simple responses. They allow interpretation, learning, communication, anticipation, and socially appropriate behavior. If association areas fail, primary sensation or movement may remain intact, but the person loses meaning, planning, expression, recognition, or appropriate behavior.
⚠️ CLINICAL IMPORTANCE
Damage to association areas does not usually cause simple paralysis or loss of basic sensation alone. Instead, it causes complex functional problems. A patient may see an object but fail to recognize it, hear words but fail to understand them, or move muscles normally but fail to perform a learned action. These are important clinical clues for cortical lesions.
2 — Language and Speech: Definition, Classification, and Cortical Control
🧠 CORE
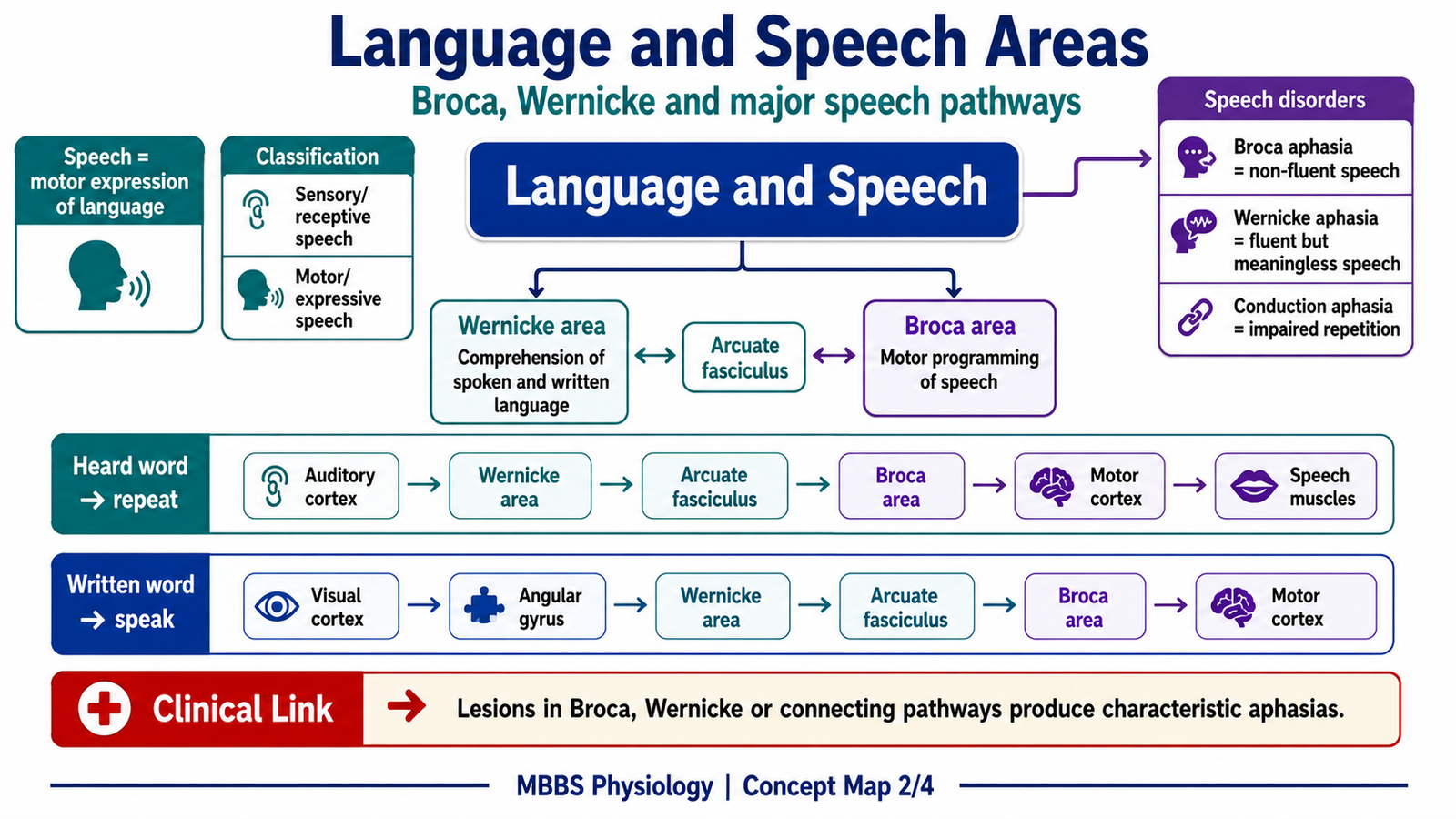
• Language is symbolic communication; speech is its motor expression.
• Speech requires sensory comprehension, cortical planning, and motor execution.
• Dominant hemisphere usually controls language; in most people this is the left hemisphere.
• Wernicke’s area understands language.
• Broca’s area plans motor speech.
• Motor cortex activates speech muscles.
• Auditory and visual association areas help in heard and written language.
• Aphasia results from cortical language area damage.
🔬 CONCEPT EXPLAINED
Language and speech are closely related but not identical. Language is the system by which meaning is encoded and understood. It includes spoken words, written words, reading, writing, and symbols. Speech is the motor act by which language is expressed through sound.
Speech may be classified functionally into:
1. Spontaneous speech
This is self-generated speech arising from thought and intention.
2. Repetition speech
This occurs when a heard or read word is repeated.
3. Comprehension speech function
This involves understanding spoken or written language.
4. Expressive speech function
This involves converting thoughts into spoken words through Broca’s area and motor pathways.
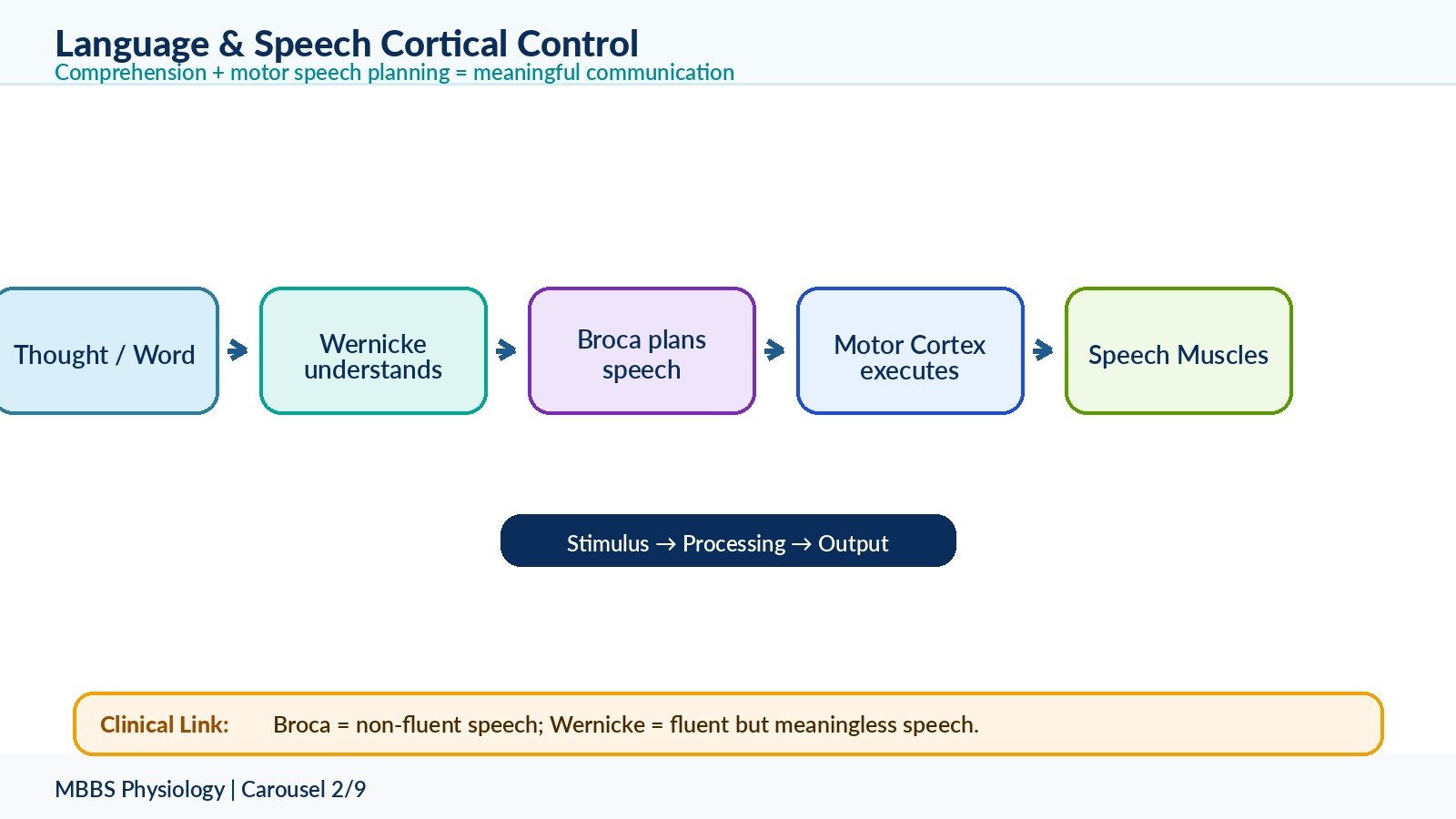
Speech requires a continuous physiological sequence. First, a stimulus enters the brain, such as a heard word or written word. Then sensory areas detect the stimulus. Association areas interpret its meaning. Wernicke’s area understands the language content. Broca’s area converts this understood language into a motor speech plan. Finally, the motor cortex activates muscles of the larynx, tongue, lips, palate, pharynx, and respiratory system.
The purpose of this organization is to separate understanding from motor production, while still allowing both to work together. This gives humans the ability to understand language, think in words, speak voluntarily, repeat words, read aloud, and communicate complex ideas.
Broca’s Area and Its Function
Broca’s area is located in the inferior frontal gyrus of the dominant hemisphere, usually the left hemisphere. It lies close to the motor cortex controlling the face, lips, tongue, and larynx. Its main function is to organize the motor pattern required for speech.
Broca’s area does not simply move the speech muscles. Instead, it arranges the sequence of motor commands required to produce meaningful words. This is important because speech requires precise timing of breathing, vocal cord vibration, tongue movement, lip movement, and articulation.
If Broca’s area is damaged, the patient understands language relatively well but cannot produce fluent speech. Speech becomes slow, effortful, broken, and non-fluent. This is called Broca’s aphasia or motor aphasia.
Wernicke’s Area and Its Function
Wernicke’s area is located in the posterior part of the superior temporal gyrus of the dominant hemisphere, near the auditory association cortex. It is responsible for comprehension of spoken and written language.
Wernicke’s area attaches meaning to words. When a person hears a word, auditory impulses first reach the primary auditory cortex. Then Wernicke’s area interprets the word and connects it with stored memory and meaning.
If Wernicke’s area is damaged, the patient can speak fluently but the speech lacks meaning. The patient also cannot properly understand spoken or written language. This is called Wernicke’s aphasia or sensory aphasia.
⚠️ CLINICAL IMPORTANCE
The difference between Broca’s and Wernicke’s aphasia is frequently tested.
In Broca’s aphasia, comprehension is relatively preserved, but speech production is impaired. The patient knows what they want to say but cannot express it fluently.
In Wernicke’s aphasia, speech is fluent but meaningless, and comprehension is poor. The patient may not realize that their speech is abnormal.
3 — Speech Pathways for Heard and Written Words
🧠 CORE
• Speech pathways connect sensory input, language comprehension, motor planning, and speech muscles.
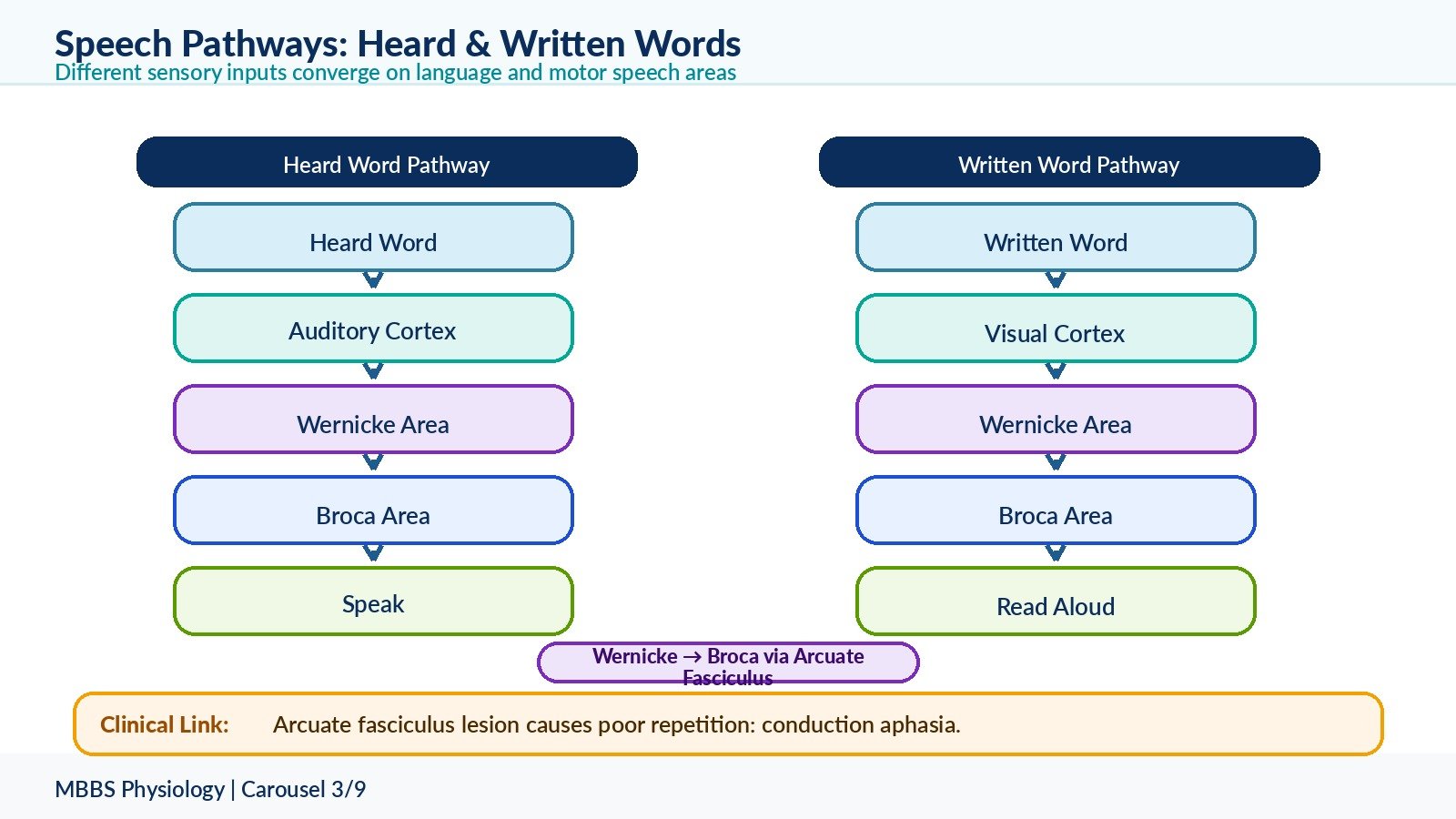
• Heard words first reach auditory cortex.
• Written words first reach visual cortex.
• Wernicke’s area provides comprehension.
• Broca’s area prepares speech motor program.
• Arcuate fasciculus connects Wernicke’s area to Broca’s area.
• Motor cortex executes speech through corticobulbar pathways.
• Lesions at different points produce different aphasias.
🔬 CONCEPT EXPLAINED
Speech is not produced by one isolated cortical area. It is produced by a pathway. The type of pathway depends on the initial stimulus. A heard word and a written word enter the brain through different sensory systems, but both must eventually reach the language comprehension system and then the motor speech system.
Speech Pathway for Perceiving a Heard Word and Speaking the Same Word
The initiating stimulus is a heard word. Sound waves enter the ear and are converted into nerve impulses by the cochlea. These impulses travel through the auditory pathway to the primary auditory cortex in the temporal lobe.
The purpose of this mechanism is to allow the brain to convert sound into meaningful language and then reproduce it as speech.
The sequence is:
The primary auditory cortex detects the sound pattern. This gives awareness of sound but not full meaning. The impulse then reaches the auditory association cortex and Wernicke’s area, where the sound pattern is interpreted as a meaningful word. Once the word is understood, information passes through the arcuate fasciculus to Broca’s area. Broca’s area creates the motor plan for speaking the word. This motor plan is sent to the primary motor cortex, especially regions controlling lips, tongue, larynx, pharynx, and respiratory muscles. Motor impulses then descend through corticobulbar pathways to cranial nerve nuclei, producing coordinated speech.
Cause → effect relationship is clear: if auditory input is intact but Wernicke’s area is damaged, sound is heard but language is not understood. If Wernicke’s area is intact but Broca’s area is damaged, the word is understood but cannot be spoken fluently. If the arcuate fasciculus is damaged, comprehension and spontaneous speech may be relatively preserved, but repetition is impaired.
Speech Pathway for Perceiving a Written Word and Repeating It
The initiating stimulus is a written word. Light from the written word reaches the retina and is transmitted through the visual pathway to the primary visual cortex in the occipital lobe.
The purpose of this pathway is to convert visual symbols into language and then into spoken speech.
The sequence is:
The primary visual cortex detects the visual pattern of letters. The visual association cortex recognizes the pattern as written symbols. This information is transferred to language comprehension areas, especially through regions that connect visual association cortex with Wernicke’s area. Wernicke’s area interprets the written word and gives meaning to it. The information then passes through the arcuate fasciculus to Broca’s area. Broca’s area prepares the motor speech plan. The motor cortex then activates speech muscles to repeat the word.
The physiological advantage of this pathway is that humans can read aloud, learn from written language, and convert visual symbols into spoken communication.
Clinical Significance of Speech Pathways
Different lesions produce different clinical pictures:
• Lesion of auditory cortex may impair perception of sound.
• Lesion of Wernicke’s area impairs comprehension.
• Lesion of arcuate fasciculus impairs repetition.
• Lesion of Broca’s area impairs fluent speech production.
• Lesion of motor cortex or corticobulbar pathways may cause dysarthria rather than aphasia.
4 — Memory: Definition, Classification, and Basic Mechanism
🧠 CORE
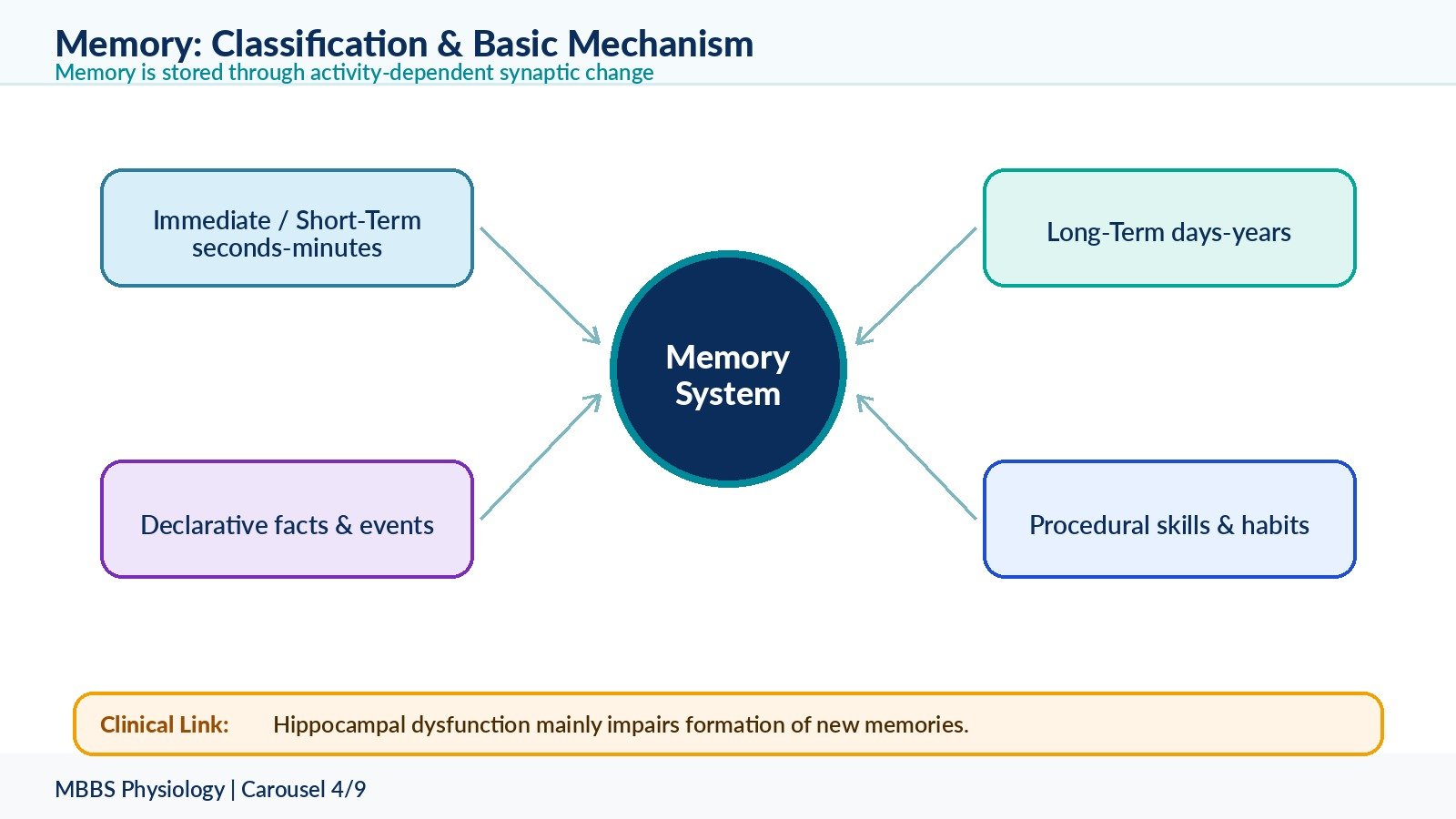
• Memory is storage and retrieval of information in the nervous system.
• It depends on changes in synaptic transmission.
• Short-term memory lasts seconds to minutes.
• Long-term memory lasts days to years.
• Working memory allows temporary manipulation of information.
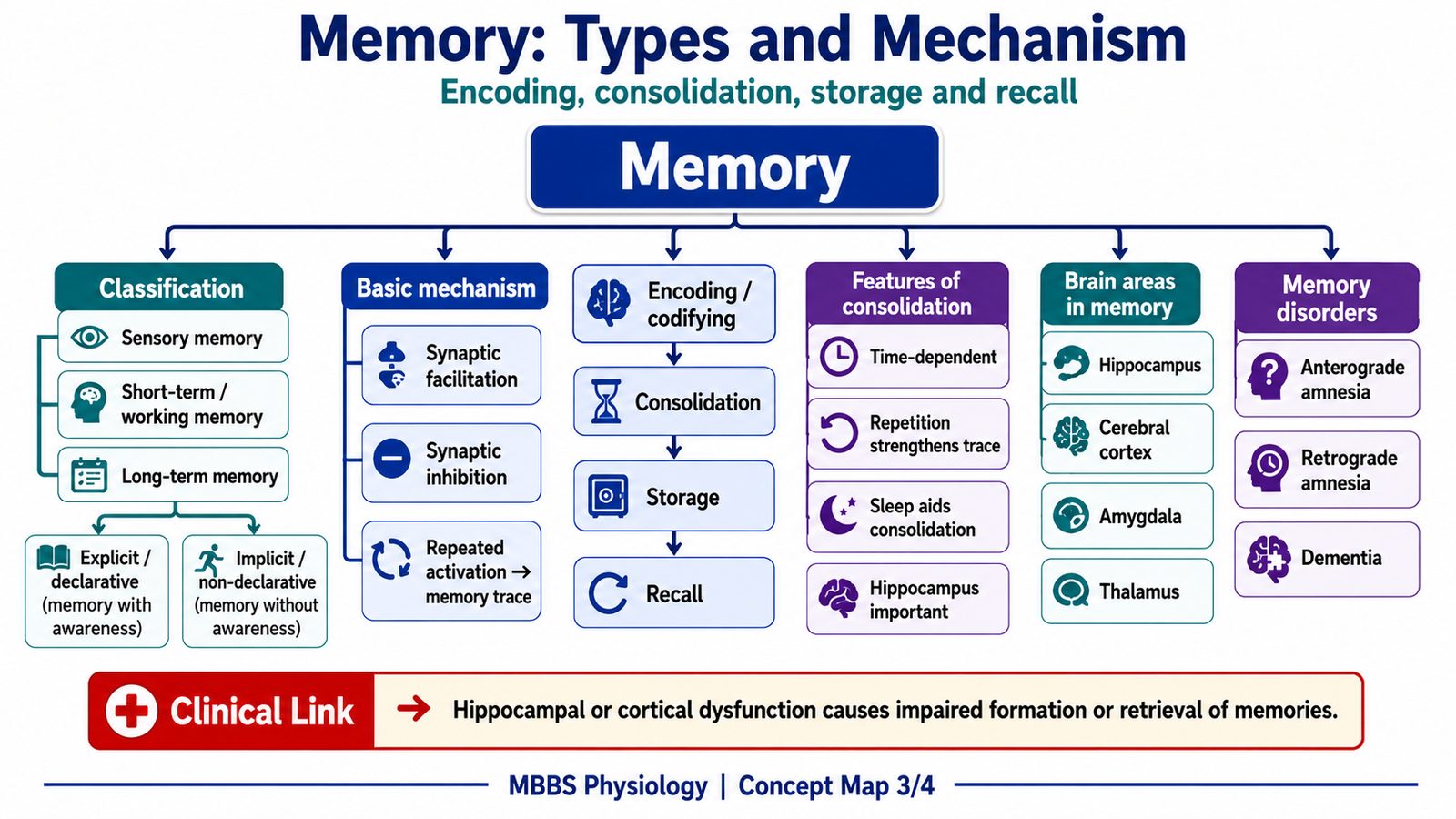
• Memory consolidation converts short-term memory into long-term memory.
• Hippocampus is essential for formation of new declarative memories.
• Cerebral cortex stores many long-term memory traces.
🔬 CONCEPT EXPLAINED
Memory is the ability of the nervous system to store information and recall it later. It is essential for learning, identity, language, behavior, clinical reasoning, and adaptation to the environment.
Memory exists because the brain must not respond to every stimulus as if it is new. The nervous system becomes more efficient when previous experience modifies future responses. Therefore, memory is a biological mechanism for learning from experience.
Memory can be classified in several ways.
Classification by Duration
1. Immediate memory
This lasts for a few seconds. It allows temporary holding of information, such as remembering a number briefly.
2. Short-term memory
This lasts seconds to minutes. It depends mainly on temporary changes in neuronal circuits and synaptic activity.
3. Intermediate long-term memory
This may last minutes to weeks. It involves chemical changes in synapses.
4. Long-term memory
This lasts days, months, or years. It requires more stable structural and biochemical changes in synapses.
Classification by Content
1. Declarative memory
This is memory of facts and events. It can be consciously recalled. It depends strongly on hippocampus and cerebral cortex.
2. Procedural memory
This is memory of skills and habits, such as riding a bicycle or writing. It involves basal ganglia, cerebellum, and motor circuits.
3. Emotional memory
This is memory linked with fear, pleasure, reward, or emotional experience. It involves amygdala and limbic system.
Basic Mechanism of Memory
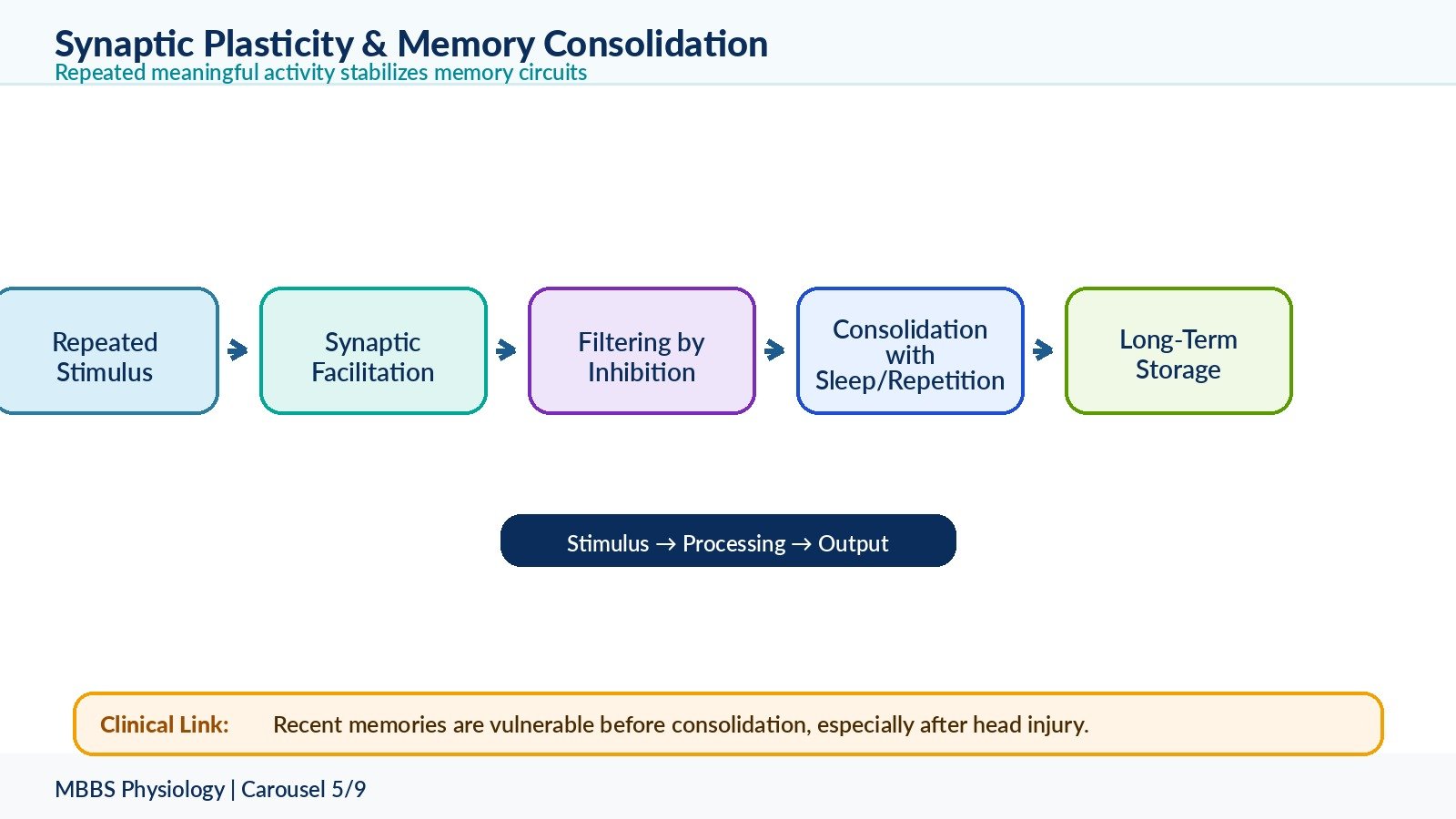
The initiating event in memory formation is repeated or meaningful stimulation of neuronal pathways. The purpose of the mechanism is to strengthen important synaptic circuits and weaken irrelevant ones.
When a stimulus repeatedly activates a neuronal pathway, synaptic transmission becomes more efficient. This occurs through increased neurotransmitter release, increased receptor sensitivity, altered ion channel activity, and sometimes formation of new synaptic connections. As a result, the same pathway becomes easier to activate in the future. This is the basis of learning.
The cause → effect relationship is:
Repeated meaningful stimulus → repeated neuronal firing → synaptic modification → easier future transmission → memory formation.
The control of memory depends on attention, emotional importance, repetition, sleep, hippocampal processing, and neuromodulators such as acetylcholine, dopamine, norepinephrine, and serotonin.
The physiological advantage is selective storage. The brain does not store everything equally; it stores what is repeated, emotionally important, useful, or strongly attended to.
⚠️ CLINICAL IMPORTANCE
Memory disorders may occur due to hippocampal damage, cortical degeneration, thiamine deficiency, head injury, stroke, or neurodegenerative disease. In early hippocampal dysfunction, formation of new memories is commonly affected more than old memories.
5 — Synaptic Facilitation, Synaptic Inhibition, and Memory Consolidation
🧠 CORE
• Memory depends on plasticity of synapses.
• Synaptic facilitation increases transmission through a pathway.
• Synaptic inhibition reduces unnecessary or competing signals.
• Consolidation stabilizes memory into long-term storage.
• Repetition strengthens consolidation.
• Emotional arousal can enhance memory.
• Sleep helps memory consolidation.
• Hippocampus organizes new declarative memory before long-term cortical storage.
🔬 CONCEPT EXPLAINED
The nervous system is plastic. This means synapses can change their strength according to use. Memory is not stored like a file in one location. Instead, it is represented by altered patterns of synaptic activity across neuronal networks.
Synaptic Facilitation
The initiating event is repeated activation of a synapse. The purpose is to make important pathways easier to activate in the future.
When a presynaptic neuron repeatedly stimulates a postsynaptic neuron, calcium entry into the presynaptic terminal may increase neurotransmitter release. Postsynaptic receptors may also become more responsive. In longer-lasting memory, protein synthesis and structural changes may occur, including increased synaptic contacts.
Cause → effect relationship:
Repeated stimulation → increased synaptic efficiency → stronger postsynaptic response → easier recall or learned response.
This mechanism is important because learning requires strengthening of meaningful connections. For example, repeated study of a concept strengthens the neuronal circuits related to that concept.
Synaptic Inhibition
Synaptic inhibition is not simply the opposite of learning. It is also necessary for proper learning. The initiating event may be activation of inhibitory interneurons or weakening of irrelevant pathways.
The purpose is to prevent excessive excitation and suppress unnecessary information. If every stimulus were stored equally, the brain would become overloaded. Inhibition allows filtering, focus, and selection.
Cause → effect relationship:
Irrelevant or competing signals → inhibitory modulation → reduced synaptic transmission → improved signal clarity.
This improves memory accuracy by allowing important signals to stand out from background noise.
Consolidation of Memory
Memory consolidation is the process by which temporary memory becomes stable long-term memory. The initiating event is meaningful learning or repeated activation of neuronal circuits.
The purpose of consolidation is to convert unstable short-term synaptic activity into more durable synaptic and structural changes.
The sequence is:
A new experience activates sensory and association cortices. If attention and importance are sufficient, the hippocampus helps organize the information. Repeated reactivation of the circuit strengthens synaptic connections. Chemical changes occur first, followed by structural changes in long-term memory. Over time, memory becomes more independent of the hippocampus and more distributed in the cerebral cortex.
Important features of consolidation include:
• It requires time.
• It is improved by repetition.
• It is strengthened by attention and emotional significance.
• It is supported by sleep.
• It may be disturbed by head injury, seizures, drugs, or severe metabolic disturbance.
• Newly formed memories are more vulnerable than older memories.
Codifying of New Memories
Codifying means organizing new information into meaningful patterns. The brain does not store isolated facts efficiently. It stores information better when it is linked with previous knowledge, emotion, context, and meaning.
For example, a student remembers Broca’s aphasia better when it is linked with frontal lobe location, non-fluent speech, preserved comprehension, and motor speech planning.
⚠️ CLINICAL IMPORTANCE
A blow to the head may erase memory of events just before injury because recent memories were not yet consolidated. This is called retrograde amnesia for recent events. Older memories are usually more resistant because they are more widely stored in cortical networks.
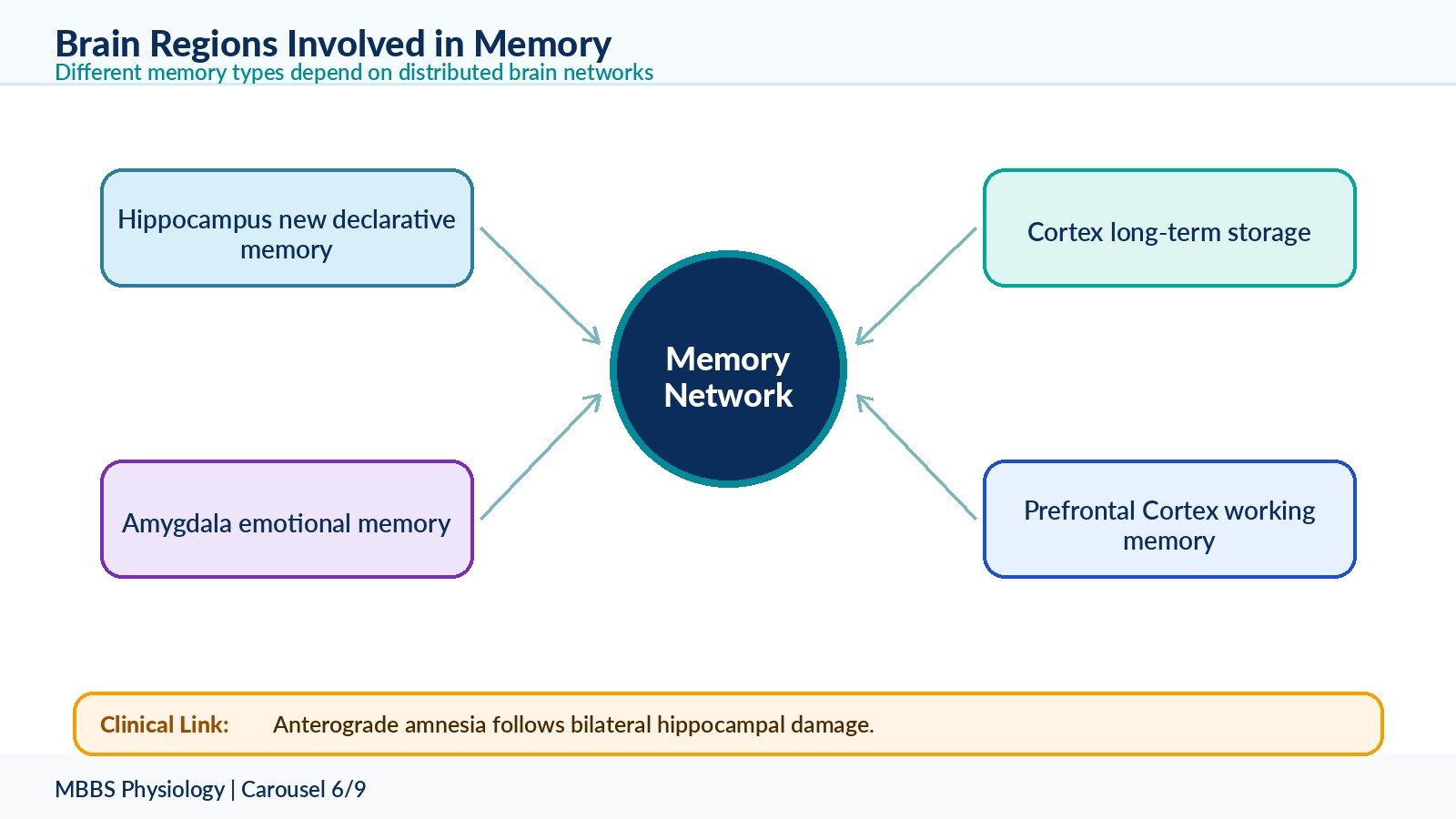
6 — Brain Regions Involved in Memory
🧠 CORE
• Hippocampus is essential for new declarative memory formation.
• Cerebral cortex stores long-term memory traces.
• Amygdala adds emotional significance to memory.
• Prefrontal cortex supports working memory and planning.
• Thalamus participates in memory circuits.
• Basal ganglia and cerebellum support procedural memory.
• Nucleus accumbens links reward and motivation with learning.
• Damage causes different patterns of memory disorder.
🔬 CONCEPT EXPLAINED
Memory is distributed. No single brain structure stores all memory. Different parts of the brain participate according to the type of memory.
Hippocampus
The hippocampus lies in the medial temporal lobe and is part of the limbic system. Its main role is formation of new declarative memories. It helps convert short-term memory into long-term memory.
The initiating event is new information that needs to be stored. The hippocampus receives processed information from association cortices. It organizes this information, links it with context, and helps transfer it into long-term cortical storage.
If the hippocampus is damaged bilaterally, the patient may be unable to form new long-term declarative memories. This is called anterograde amnesia. Old memories may remain relatively preserved because they are already stored in cortical networks.
Cerebral Cortex
The cerebral cortex is important for long-term storage of memory. Different memories are stored in relation to the cortical areas involved in their original processing. Visual memories are related to visual association areas, auditory memories to auditory association areas, and language memories to language association areas.
Amygdala
The amygdala attaches emotional value to memory. Fearful or emotionally strong events are remembered more clearly because amygdala activation enhances memory consolidation through limbic and neurohormonal mechanisms.
Prefrontal Cortex
The prefrontal cortex supports working memory, attention, planning, decision-making, and behavioral control. It allows temporary holding and manipulation of information, such as solving a problem or planning an answer.
Basal Ganglia and Cerebellum
These structures are important for procedural memory. Skills and habits are learned through repeated practice and stored in motor circuits involving basal ganglia, cerebellum, and motor cortex.
⚠️ CLINICAL IMPORTANCE
Hippocampal dysfunction causes difficulty forming new memories. Cortical dysfunction may cause loss of stored knowledge. Amygdala dysfunction may disturb emotional learning. Prefrontal dysfunction may cause poor judgment, poor working memory, impulsivity, and personality change.
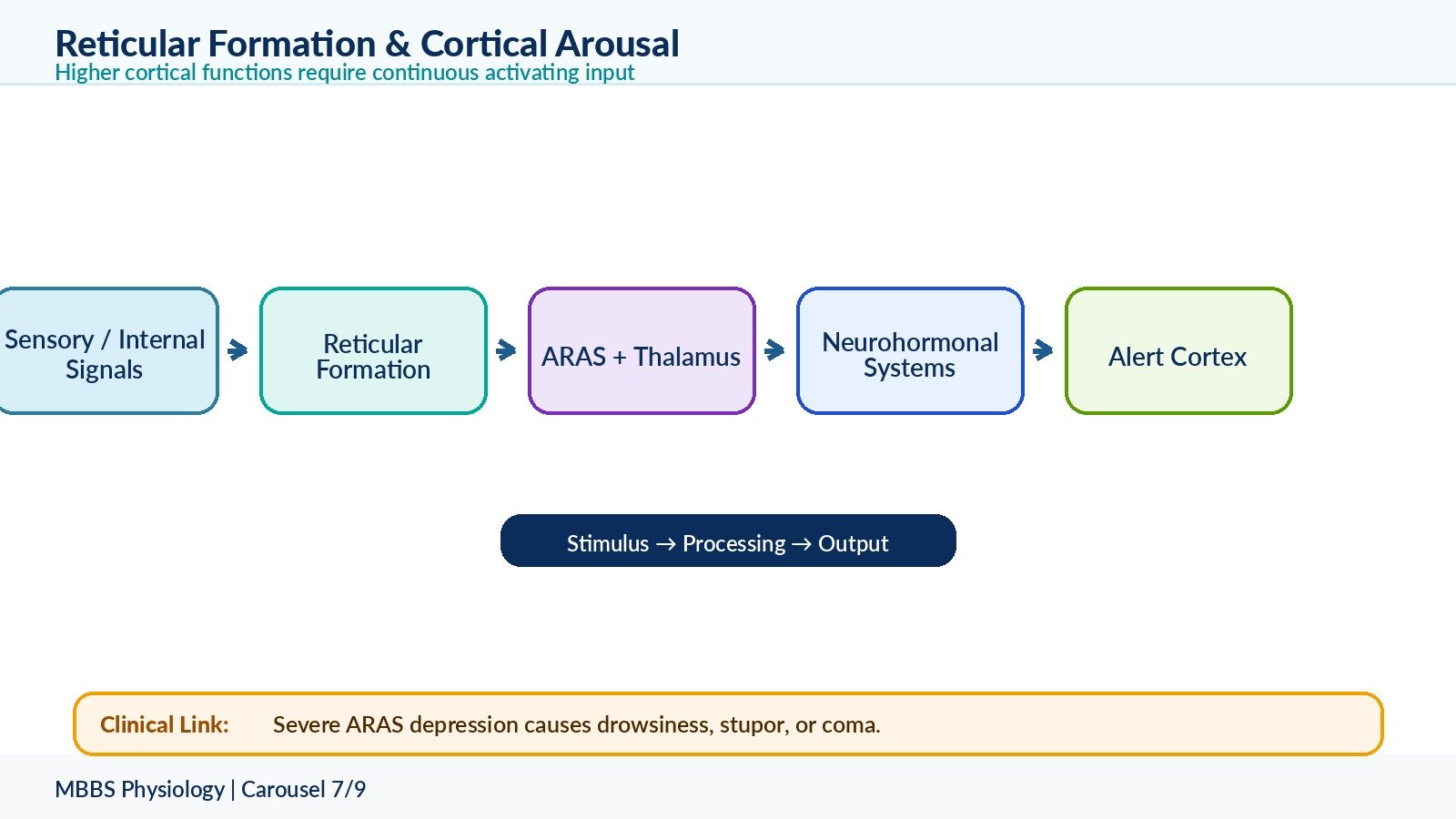
7 — Reticular Formation, Bulboreticular Facilitatory Area, and Neurohormonal Activation of Cortex
🧠 CORE
• Reticular formation regulates arousal and consciousness.
• Bulboreticular facilitatory area stimulates higher brain centers.
• Ascending reticular activating system keeps cortex alert.
• Neurohormonal systems provide continuous cortical activation.
• Acetylcholine, norepinephrine, dopamine, serotonin, and histamine influence attention and behavior.
• Cortical function needs continuous subcortical stimulation.
• Reduced activation causes drowsiness, coma, or impaired cognition.
🔬 CONCEPT EXPLAINED
Higher cortical functions require an awake and alert cerebral cortex. The cortex cannot think, speak, learn, or remember effectively unless it receives continuous activating input from lower brain centers.
The bulboreticular facilitatory area is located in the brainstem reticular formation. Its function is to maintain cortical excitability and wakefulness. It sends activating signals upward through the thalamus and other pathways to the cerebral cortex.
The initiating event may be sensory input, internal body signals, emotional stimuli, or circadian arousal mechanisms. The purpose is to keep the cortex sufficiently active to respond to the environment.
The sequence is:
Sensory or internal activating signals stimulate the brainstem reticular formation. The bulboreticular facilitatory area sends impulses upward. These impulses activate thalamic and cortical neurons. Neurohormonal systems release modulators such as acetylcholine, norepinephrine, dopamine, serotonin, and histamine. These chemicals adjust alertness, attention, motivation, mood, and learning.
The cause → effect relationship is:
Reticular activation → cortical arousal → attention and awareness → effective higher cortical function.
If this system is depressed, cortical activity decreases. The person becomes sleepy, confused, stuporous, or comatose depending on severity.
Continuous Stimulation from Lower Brain by Neurohormonal Systems
The brain uses several diffuse neurohormonal systems to regulate cortical tone:
• Noradrenergic system: arises mainly from locus coeruleus; increases alertness and attention.
• Serotonergic system: arises mainly from raphe nuclei; influences mood, sleep, and pain modulation.
• Dopaminergic system: involved in motivation, reward, movement, and cognition.
• Cholinergic system: important for attention, learning, and memory.
• Histaminergic system: promotes wakefulness.
These systems do not carry precise sensory information. Instead, they adjust the functional state of the cortex.
⚠️ CLINICAL IMPORTANCE
Damage to the brainstem reticular activating system can cause coma. Disturbance of cholinergic systems is associated with impaired attention and memory. Dopaminergic dysfunction contributes to disorders of movement, motivation, and reward.
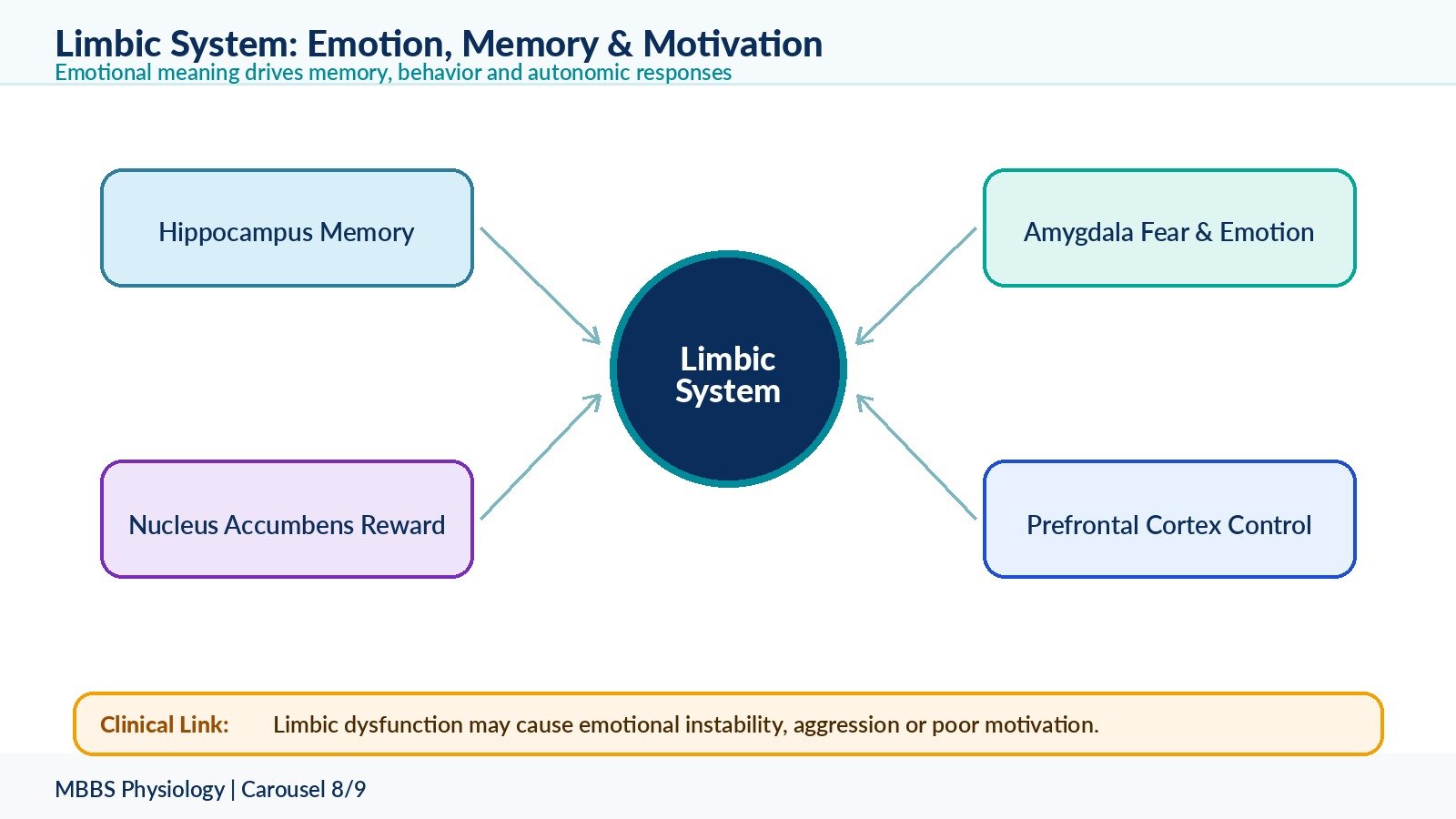
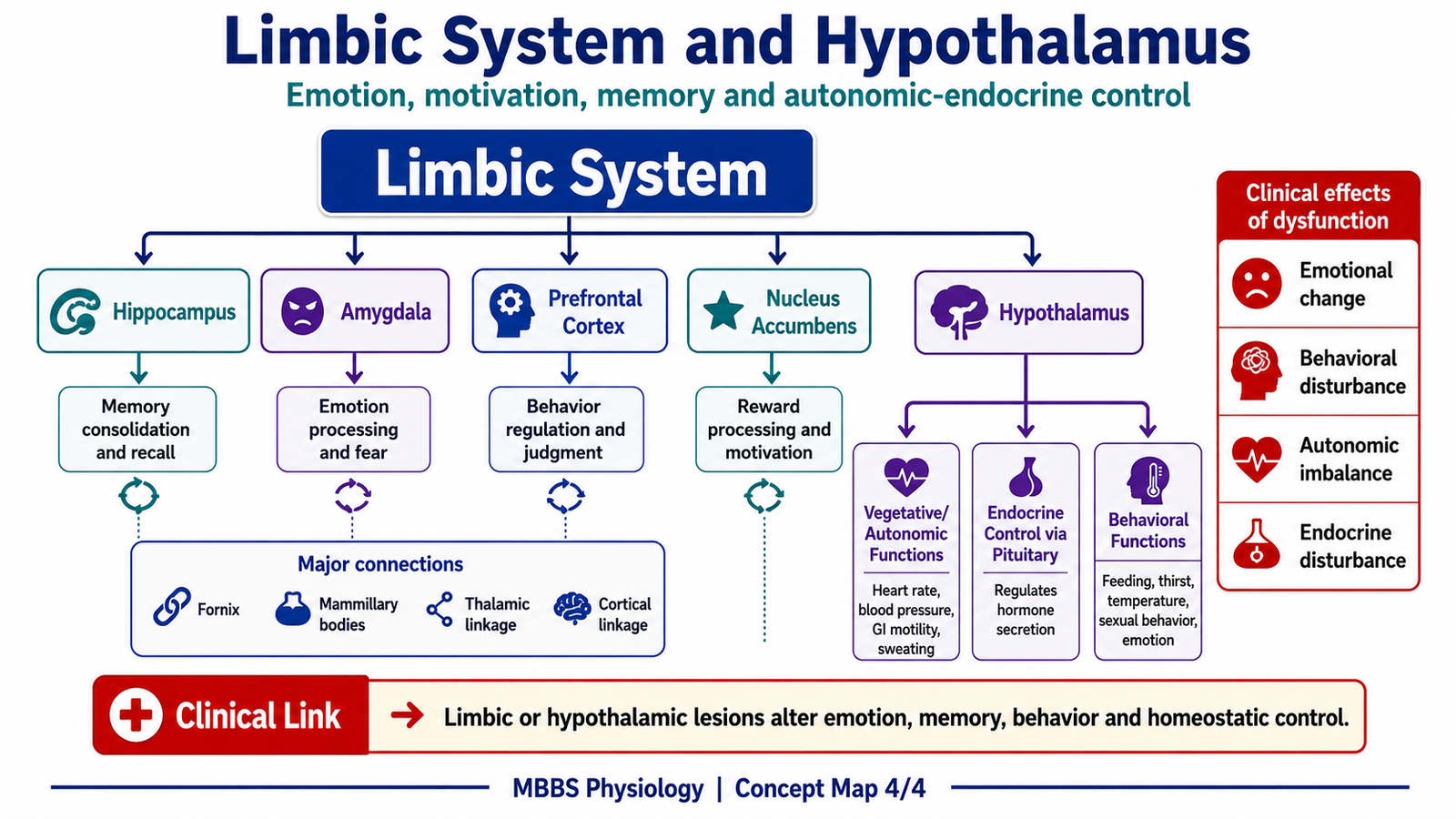
8 — Limbic System: Components, Connections, and Functions
🧠 CORE
• Limbic system links emotion, memory, motivation, and autonomic responses.
• Principal components include hippocampus, amygdala, prefrontal cortex, and nucleus accumbens.
• It has strong connections with hypothalamus.
• Hippocampus is important for memory.
• Amygdala is important for fear, aggression, and emotional learning.
• Nucleus accumbens is important for reward and motivation.
• Prefrontal cortex regulates emotional behavior.
• Limbic dysfunction causes emotional and behavioral changes.
🔬 CONCEPT EXPLAINED
The limbic system is a functional network of cortical and subcortical structures that gives emotional meaning to experience and links emotion with memory, motivation, autonomic responses, and endocrine responses.
The reason this system exists is that survival depends not only on sensation and movement but also on motivation and emotion. Hunger, fear, pleasure, anger, attachment, reward, and memory all influence behavior.
Principal Components
Hippocampus
The hippocampus is involved in memory formation, especially declarative memory and spatial memory.
Amygdala
The amygdala evaluates emotional significance, especially fear, threat, aggression, and emotional learning.
Prefrontal cortex
The prefrontal cortex controls judgment, impulse control, planning, and socially appropriate emotional expression.
Nucleus accumbens
The nucleus accumbens is part of the reward pathway. It links dopamine, motivation, pleasure, reinforcement, and habit formation.
Other related limbic structures include cingulate gyrus, parahippocampal gyrus, septal nuclei, mammillary bodies, fornix, and parts of thalamus and hypothalamus.
Pathways Connecting Components of Limbic System
Limbic structures are interconnected through important pathways:
• Fornix: connects hippocampus with mammillary bodies and septal areas.
• Mammillothalamic tract: connects mammillary bodies to anterior thalamic nuclei.
• Cingulum: connects cingulate gyrus with parahippocampal regions.
• Amygdaloid pathways: connect amygdala with hypothalamus, prefrontal cortex, and brainstem.
• Reward pathway: dopaminergic pathway from ventral tegmental area to nucleus accumbens and prefrontal cortex.
These pathways allow emotional experiences to influence memory, autonomic activity, endocrine response, and behavior.
Functions of Limbic System
The limbic system performs several integrated functions:
• Emotional behavior such as fear, anger, pleasure, and affection.
• Motivation for survival behaviors such as feeding, reproduction, and defense.
• Memory formation, especially through hippocampus.
• Emotional coloring of memory through amygdala.
• Reward and reinforcement through nucleus accumbens.
• Autonomic responses through hypothalamic connections.
• Endocrine responses through hypothalamic-pituitary control.
• Behavioral regulation through prefrontal cortex.
Anatomy of Memory and Emotion in Relation to Limbic System
Memory and emotion are strongly linked. A neutral event may be forgotten quickly, but an emotionally charged event is remembered better. This occurs because the amygdala enhances memory consolidation through its connections with the hippocampus and hypothalamus.
For example, fear activates the amygdala. The amygdala stimulates hypothalamic and autonomic responses such as increased heart rate, sweating, and stress hormone release. At the same time, it strengthens hippocampal memory of the event. This allows the person to avoid similar danger in the future.
⚠️ CLINICAL IMPORTANCE
Limbic dysfunction may produce emotional instability, aggression, loss of fear, poor motivation, addiction-related behavior, memory impairment, or abnormal autonomic/endocrine responses. These should be understood at basic mechanism level in 2nd-year MBBS.
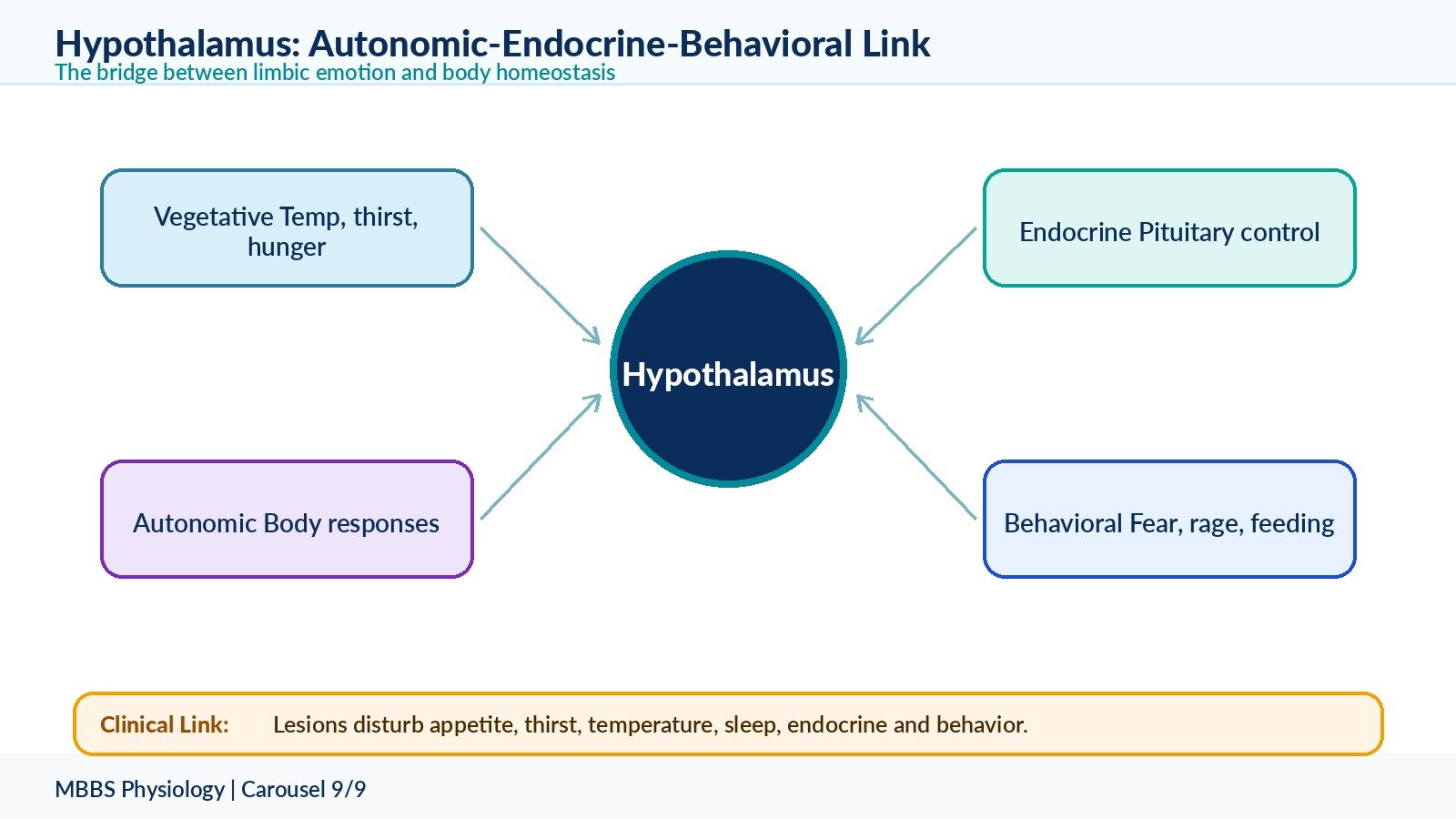
9 — Hypothalamus: Connections and Vegetative, Endocrine, and Behavioral Functions
🧠 CORE
• Hypothalamus links nervous system with endocrine and autonomic systems.
• It connects with limbic system, brainstem, thalamus, cortex, and pituitary gland.
• It regulates temperature, hunger, thirst, sleep, autonomic activity, and emotions.
• It controls anterior pituitary through releasing/inhibiting hormones.
• It controls posterior pituitary through ADH and oxytocin pathways.
• It participates in behavioral responses such as rage, fear, feeding, and sexual behavior.
• Limbic-hypothalamic pathways convert emotion into body responses.
• Dysfunction causes vegetative, endocrine, and behavioral disturbances.
🔬 CONCEPT EXPLAINED
The hypothalamus is a small but powerful regulatory region located below the thalamus and around the third ventricle. It is the major integration center for autonomic, endocrine, vegetative, and emotional responses.
Its purpose is to maintain internal homeostasis and convert emotional states into bodily responses. When a person feels fear, the hypothalamus helps produce tachycardia, sweating, increased blood pressure, and stress hormone responses. When body water is low, it stimulates thirst and ADH secretion. When body temperature changes, it activates heat loss or heat production mechanisms.
Connections of Hypothalamus with Different Areas of Brain
The hypothalamus connects with:
• Limbic system: especially amygdala and hippocampus, for emotion and memory-related autonomic responses.
• Brainstem autonomic centers: for cardiovascular, respiratory, gastrointestinal, and pupillary responses.
• Pituitary gland: for endocrine control.
• Thalamus and cerebral cortex: for awareness and behavioral expression.
• Reticular formation: for arousal and sleep-wake regulation.
• Spinal cord autonomic neurons: for sympathetic and parasympathetic output.
These connections allow the hypothalamus to act as the bridge between emotion, autonomic function, endocrine secretion, and behavior.
Vegetative Functions of Hypothalamus
Vegetative functions are basic survival functions.
The hypothalamus regulates:
• Body temperature
• Hunger and satiety
• Thirst and water balance
• Sleep-wake rhythm
• Autonomic nervous system activity
• Gastrointestinal activity
• Cardiovascular responses
• Sexual and reproductive behavior
For example, when plasma osmolality rises, hypothalamic osmoreceptors are stimulated. This causes thirst and ADH release. The result is increased water intake and water conservation by kidneys. The functional outcome is restoration of body fluid balance.
Endocrine Functions of Hypothalamus
The hypothalamus controls the pituitary gland.
For the anterior pituitary, hypothalamic releasing and inhibiting hormones enter the hypophyseal portal circulation. These regulate secretion of hormones such as TSH, ACTH, GH, FSH, LH, and prolactin.
For the posterior pituitary, hypothalamic neurons synthesize ADH and oxytocin. These hormones travel down axons to the posterior pituitary and are released into blood.
The cause → effect relationship is:
Hypothalamic neural/endocrine signal → pituitary hormone change → target gland response → homeostatic effect.
Behavioral Functions of Hypothalamus
The hypothalamus contributes to behavior because it is strongly connected with the limbic system. It participates in feeding behavior, drinking behavior, sexual behavior, fear, rage, pleasure, and defensive responses.
The hypothalamus does not create complex personality by itself, but it provides the autonomic and endocrine background for emotional behavior. The prefrontal cortex helps regulate these responses so that behavior remains socially appropriate.
⚠️ CLINICAL IMPORTANCE
Hypothalamic dysfunction may cause abnormal appetite, obesity or weight loss, temperature dysregulation, diabetes insipidus, sleep disturbance, endocrine abnormalities, and emotional or behavioral changes. For 2nd-year MBBS, the key is to understand the mechanism rather than detailed disease management.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure | Main Function | Functional Outcome |
|---|---|---|
| Prefrontal association cortex | Planning, judgment, working memory, behavior control | Organized thought, personality, decision-making |
| Parieto-occipito-temporal association area | Integration of visual, auditory, and somatic input | Language comprehension, spatial awareness, recognition |
| Broca’s area | Motor planning of speech | Fluent meaningful speech production |
| Wernicke’s area | Language comprehension | Understanding spoken and written language |
| Arcuate fasciculus | Connects Wernicke’s and Broca’s areas | Repetition and coordinated language expression |
| Hippocampus | Formation of new declarative memory | Learning of facts and events |
| Amygdala | Emotional significance and fear learning | Emotional memory and behavioral response |
| Nucleus accumbens | Reward and motivation | Reinforcement, pleasure, goal-directed behavior |
| Hypothalamus | Autonomic and endocrine integration | Homeostasis and emotional body responses |
| Reticular formation | Cortical arousal | Wakefulness, attention, consciousness |
Higher cortical function is therefore not produced by one isolated area. A student hears a question, understands it through auditory and language association areas, recalls information through hippocampal-cortical memory circuits, plans an answer through prefrontal cortex, and speaks using Broca’s area, motor cortex, and speech muscles. Emotional confidence, anxiety, motivation, and autonomic responses are influenced by limbic system and hypothalamus.
🩺 5️⃣ Clinical Correlation
1. Broca’s Aphasia
Broca’s aphasia occurs due to damage to Broca’s area in the dominant frontal lobe.
The patient understands language relatively well but cannot produce fluent speech. Speech is slow, effortful, and broken. The mechanism is failure of motor planning for speech, not paralysis of speech muscles alone.
Exam point: Non-fluent speech with relatively preserved comprehension suggests Broca’s aphasia.
2. Wernicke’s Aphasia
Wernicke’s aphasia occurs due to damage to Wernicke’s area in the dominant posterior temporal region.
The patient speaks fluently, but the speech is meaningless or inappropriate. Comprehension is poor. The mechanism is failure of language understanding.
Exam point: Fluent but meaningless speech with poor comprehension suggests Wernicke’s aphasia.
3. Conduction Aphasia
Conduction aphasia occurs due to damage to the arcuate fasciculus.
The patient may understand language and produce spontaneous speech, but repetition is impaired. The mechanism is disconnection between comprehension area and motor speech planning area.
Exam point: Poor repetition with relatively preserved comprehension suggests conduction aphasia.
4. Memory Disorder Due to Hippocampal Dysfunction
Hippocampal damage affects formation of new declarative memories.
The patient may remember old events but cannot form new long-term memories. This is because old memories are stored widely in cortex, while new memory formation requires hippocampal processing.
Exam point: Inability to form new memories is anterograde amnesia.
5. Cortical Dysfunction and Memory Loss
Cortical degeneration may disturb stored long-term memories, language, recognition, and judgment. This occurs because long-term memory traces are distributed across cortical association areas.
Exam point: Widespread cortical disease affects multiple higher functions, not only memory.
6. Limbic Dysfunction and Emotional Behavior
Amygdala or limbic dysfunction may cause abnormal fear, aggression, emotional instability, poor motivation, or inappropriate emotional responses.
The mechanism is disturbance of emotional evaluation and its connection with hypothalamic autonomic/endocrine output.
7. Hypothalamic Dysfunction
Hypothalamic lesions may cause disturbances of appetite, thirst, temperature regulation, sleep, autonomic function, endocrine function, and behavior.
The mechanism is failure of integration between body signals, limbic emotions, autonomic output, and pituitary endocrine control.
📌 6️⃣ Summary Points
- Association areas give meaning to sensory input and plan complex behavior.
- The prefrontal cortex is important for judgment, planning, working memory, personality, and behavioral control.
- Wernicke’s area understands language; Broca’s area produces motor speech plan.
- Heard word repetition pathway: auditory cortex → Wernicke’s area → arcuate fasciculus → Broca’s area → motor cortex.
- Written word reading pathway: visual cortex → visual association cortex → Wernicke’s area → Broca’s area → motor cortex.
- Broca’s aphasia is non-fluent speech with relatively preserved comprehension.
- Wernicke’s aphasia is fluent but meaningless speech with poor comprehension.
- Memory is mainly based on synaptic plasticity, especially synaptic facilitation and consolidation.
- Hippocampus is essential for formation of new declarative memories.
- Amygdala gives emotional importance to memory and behavior.
- Reticular formation maintains cortical arousal and consciousness.
- Hypothalamus connects limbic system with autonomic and endocrine responses.