
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
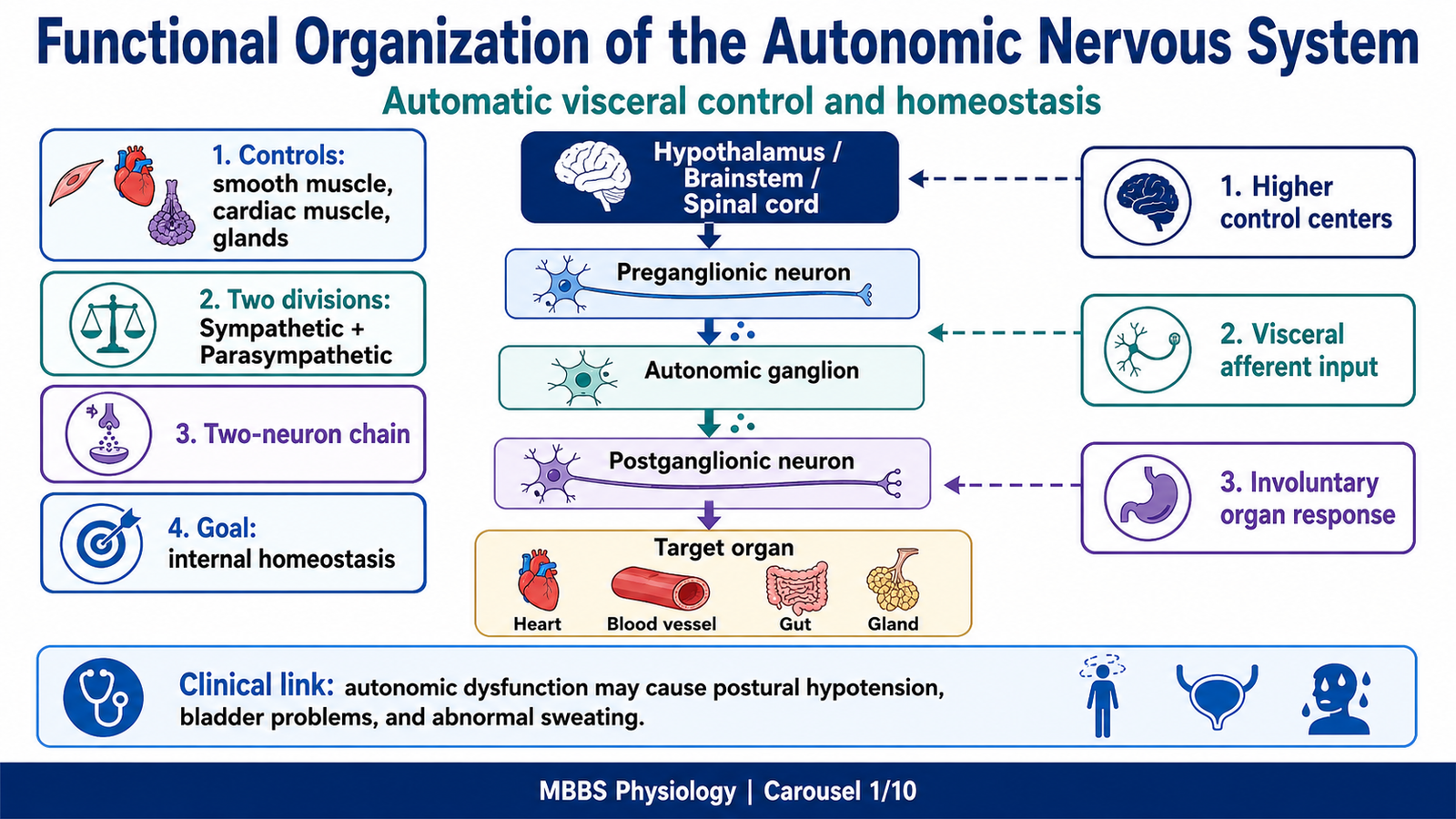
he autonomic nervous system is the part of the nervous system that controls the internal organs without requiring conscious effort. It regulates heart rate, blood pressure, respiration, digestion, sweating, pupil size, urinary bladder function, reproductive responses, and many other visceral functions.
It is located functionally between the central nervous system and visceral organs, using motor pathways that pass through autonomic ganglia before reaching target organs. The two major divisions are the sympathetic nervous system and the parasympathetic nervous system.
The sympathetic system prepares the body for stress, activity, and emergency situations, while the parasympathetic system supports rest, digestion, conservation of energy, and routine visceral maintenance. Clinically, this topic is important because autonomic dysfunction can produce postural hypotension, abnormal sweating, urinary retention, constipation, cardiac rhythm disturbances, pupillary abnormalities, and shock-like states.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Autonomic nervous system: Part of the peripheral nervous system that controls involuntary visceral functions.
- Sympathetic nervous system: Thoracolumbar division of the ANS that prepares the body for stress, exercise, fear, and emergency responses.
- Parasympathetic nervous system: Craniosacral division of the ANS that promotes rest, digestion, energy conservation, and organ-specific regulation.
- Preganglionic neuron: First autonomic neuron whose cell body lies in the CNS and whose axon reaches an autonomic ganglion.
- Postganglionic neuron: Second autonomic neuron whose cell body lies in an autonomic ganglion and whose axon reaches the target organ.
- Autonomic ganglion: Collection of neuronal cell bodies outside the CNS where preganglionic neurons synapse with postganglionic neurons.
- Visceral afferent fibers: Sensory fibers carrying information from internal organs to the CNS.
- Visceral efferent fibers: Motor fibers carrying autonomic commands from the CNS to smooth muscle, cardiac muscle, glands, and adrenal medulla.
- Autonomic tone: Continuous baseline activity of sympathetic or parasympathetic nerves that maintains normal organ function.
- Adrenal medulla: Modified sympathetic ganglion that secretes epinephrine and norepinephrine into blood.
Essential Terminology
- Thoracolumbar outflow: Sympathetic origin from T1–L2 spinal cord segments.
- Craniosacral outflow: Parasympathetic origin from cranial nerves III, VII, IX, X and sacral spinal segments S2–S4.
- Cholinergic neuron: Neuron that releases acetylcholine.
- Adrenergic neuron: Neuron that releases norepinephrine or epinephrine.
- Nicotinic receptor: Receptor found in autonomic ganglia and adrenal medulla that responds to acetylcholine.
- Muscarinic receptor: Receptor found on parasympathetic target organs and sweat glands that responds to acetylcholine.
- Alpha and beta receptors: Adrenergic receptors on sympathetic effector organs.
Basic Overview
- The ANS controls organs automatically, but it is regulated by higher centers such as the hypothalamus, brainstem, and spinal cord.
- Sympathetic and parasympathetic systems often have opposite effects on the same organ, but not always.
- The ANS uses a two-neuron chain: preganglionic neuron → ganglion → postganglionic neuron → target organ.
- Sympathetic ganglia are usually close to the spinal cord, so sympathetic preganglionic fibers are short and postganglionic fibers are long.
- Parasympathetic ganglia are usually near or inside the target organ, so parasympathetic preganglionic fibers are long and postganglionic fibers are short.
- Autonomic receptors determine the final response of the target organ.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPT 1 — Functional Organization of the Autonomic Nervous System
🧠 CORE
- The ANS controls involuntary activity of smooth muscle, cardiac muscle, glands, and adrenal medulla.
- It is divided into sympathetic and parasympathetic systems.
- Autonomic motor pathways usually contain two neurons: preganglionic and postganglionic.
- Preganglionic neurons arise from the CNS.
- Postganglionic neurons arise from autonomic ganglia.
- The hypothalamus, brainstem, and spinal cord coordinate autonomic activity.
- Autonomic responses maintain internal homeostasis during rest, stress, posture, digestion, and temperature change.
🔬 CONCEPT EXPLAINED
The autonomic nervous system exists because many body functions must continue continuously and automatically without conscious attention. Heart rate, vascular tone, digestion, sweating, urinary bladder filling, pupillary size, and glandular secretion must be adjusted every moment according to the needs of the body. If every visceral function required conscious control, survival would be impossible during sleep, exercise, fear, illness, or injury.
The basic plan of the ANS is different from the somatic motor system. In the somatic motor system, a single lower motor neuron directly supplies skeletal muscle. In the autonomic system, the CNS usually sends signals through a two-neuron chain. The first neuron, called the preganglionic neuron, begins in the brainstem or spinal cord. It synapses in an autonomic ganglion with the second neuron, called the postganglionic neuron, which then supplies the target organ.
This arrangement gives the ANS flexibility. One preganglionic neuron can influence many postganglionic neurons, especially in the sympathetic system. As a result, sympathetic responses can be widespread, such as during fear or exercise. In contrast, parasympathetic responses are often more localized and organ-specific, allowing fine control of digestion, heart rate, urinary bladder emptying, and glandular secretion.
The ANS is not completely independent. It is regulated by higher centers. The hypothalamus is the major integrating center because it links autonomic responses with temperature, hunger, thirst, emotion, endocrine function, and stress. The brainstem controls vital autonomic reflexes such as cardiovascular and respiratory reflexes. The spinal cord contains autonomic reflex circuits for sweating, vasomotor tone, micturition, defecation, and sexual reflexes.
Therefore, the ANS acts as the body’s automatic control system. It receives information from visceral organs, processes it through central autonomic centers, and sends efferent output to maintain homeostasis.
⚠️ CLINICAL IMPORTANCE
Damage to autonomic pathways can produce serious functional disturbance even when voluntary movement is normal. Autonomic dysfunction may cause postural hypotension, abnormal heart rate control, bladder dysfunction, constipation, impotence, impaired sweating, or abnormal pupillary responses. These signs are clinically important because they indicate failure of internal homeostatic regulation.
MAJOR CONCEPT 2 — Sympathetic Nervous System: Location, Level and Organization
🧠 CORE
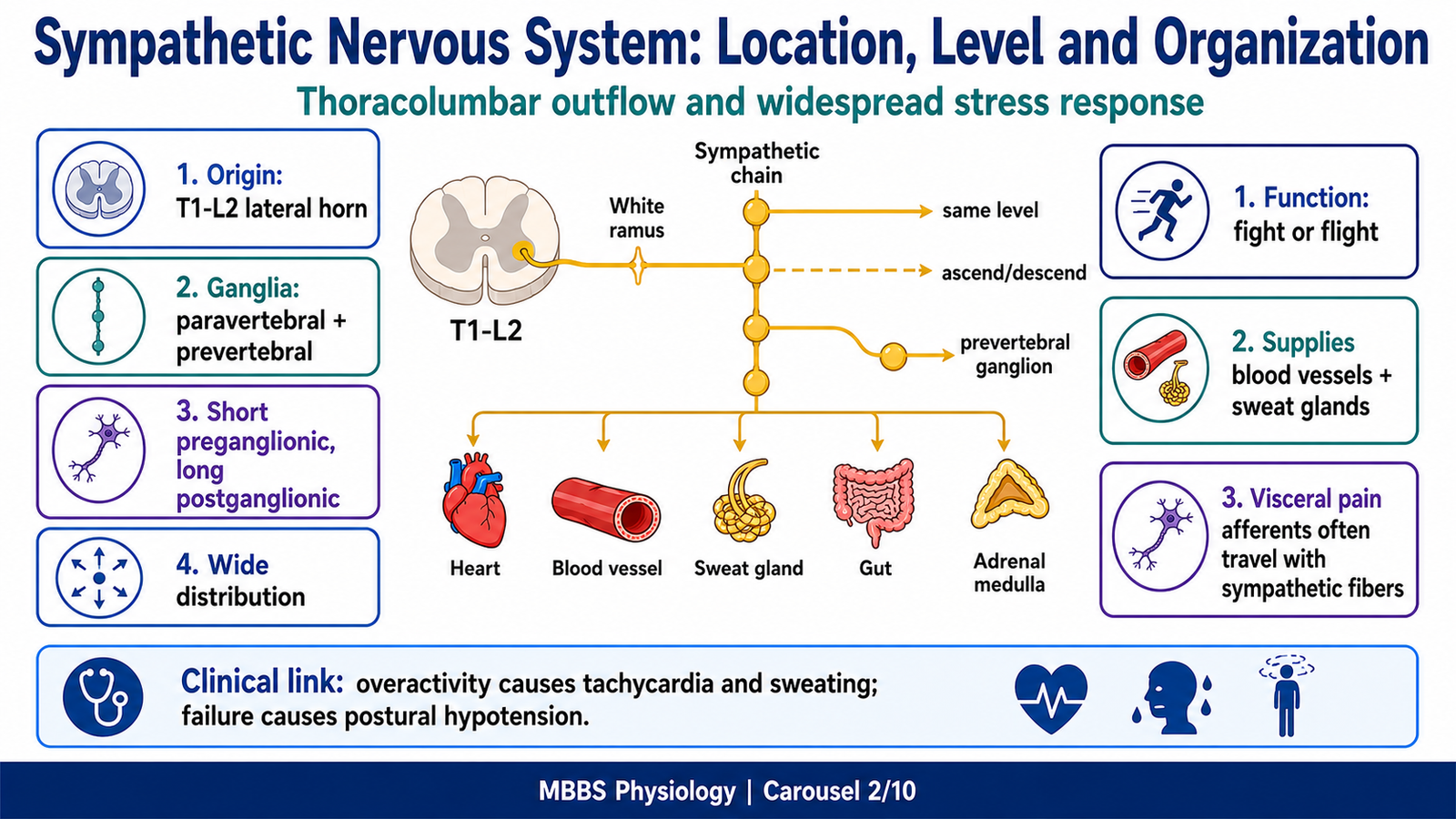
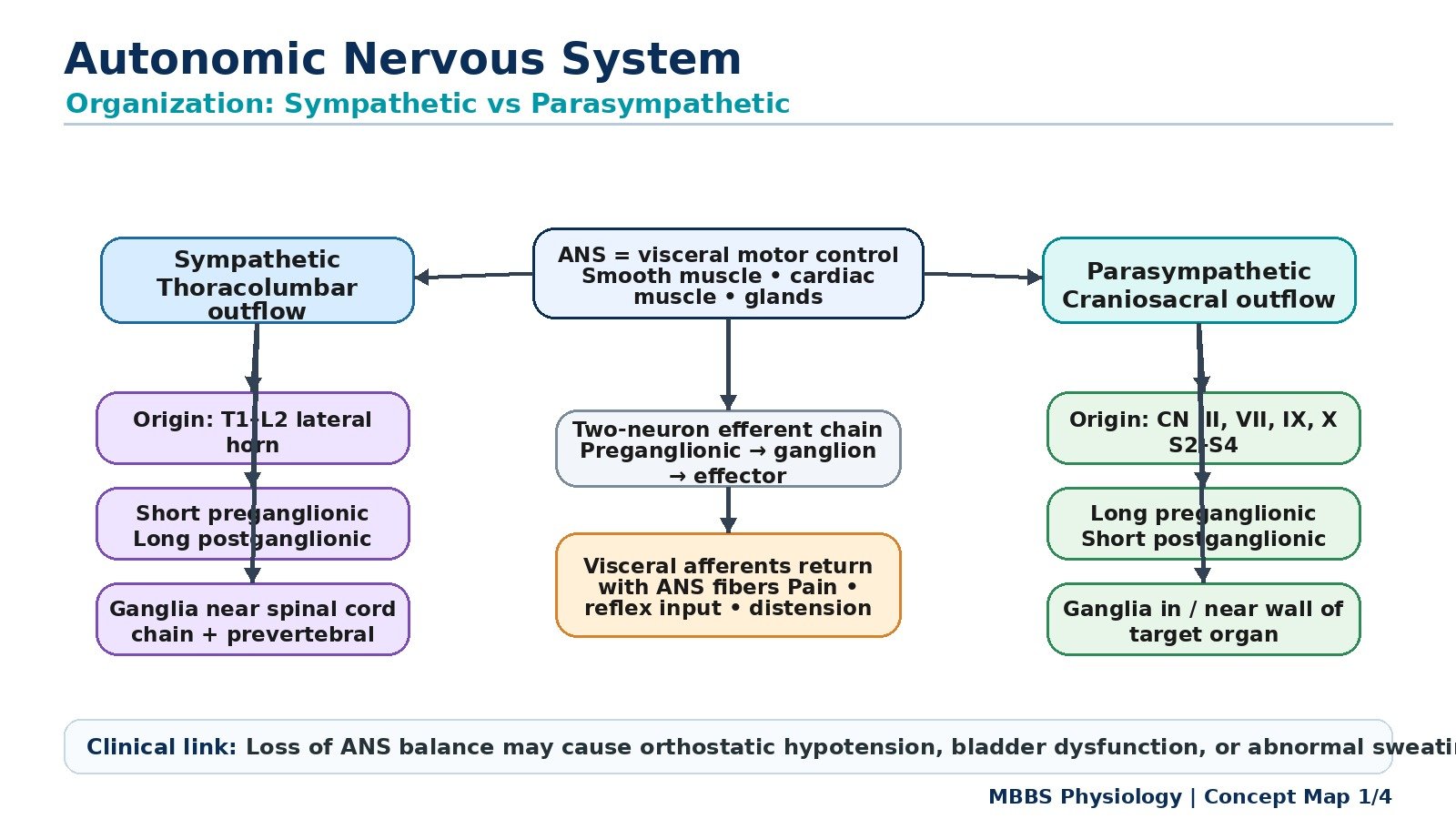
- The sympathetic nervous system is the thoracolumbar division of the ANS.
- Preganglionic sympathetic neurons arise from the lateral horn of spinal cord segments T1–L2.
- Sympathetic ganglia lie close to the vertebral column.
- Preganglionic fibers are usually short.
- Postganglionic fibers are usually long.
- Sympathetic output is widely distributed throughout the body.
- It prepares the body for stress, exercise, fear, trauma, and emergency conditions.
🔬 CONCEPT EXPLAINED
The sympathetic nervous system originates from the thoracic and upper lumbar spinal cord, specifically from T1 to L2 segments. Because of this origin, it is called the thoracolumbar outflow. The cell bodies of sympathetic preganglionic neurons are located mainly in the intermediolateral cell column, also called the lateral horn of the spinal cord.
After leaving the spinal cord, sympathetic preganglionic fibers pass through the anterior roots and spinal nerves, then enter the sympathetic chain through white rami communicantes. From here, they may synapse at the same level, ascend or descend in the sympathetic chain, or pass through without synapsing to reach prevertebral ganglia.
This arrangement is important because it allows sympathetic signals to spread widely. For example, a stress signal from the CNS can activate the heart, blood vessels, sweat glands, adrenal medulla, bronchi, pupils, and metabolic tissues at the same time. This widespread activation is suitable for the “fight or flight” response.
The sympathetic ganglia are located near the spinal cord, mainly in the paravertebral sympathetic chain or in prevertebral ganglia near major abdominal arteries. Because the ganglia are close to the CNS, sympathetic preganglionic fibers are usually short, while postganglionic fibers must travel a longer distance to reach organs; therefore, they are usually long.
The sympathetic system exists to support survival during conditions requiring increased energy, rapid circulation, oxygen delivery, and alertness. It increases heart rate, dilates bronchi, redistributes blood to skeletal muscles, mobilizes glucose and fatty acids, dilates pupils, increases sweating, and reduces digestive activity.
Distribution of Sympathetic Efferent Fibers
Sympathetic efferent fibers supply:
- Heart
- Blood vessels
- Bronchi
- Sweat glands
- Arrector pili muscles
- Pupils
- Gastrointestinal tract
- Liver
- Adrenal medulla
- Urinary bladder
- Reproductive organs
A key feature is that sympathetic fibers supply almost all blood vessels and sweat glands throughout the body. This makes sympathetic activity essential for blood pressure regulation and temperature control.
Distribution of Sympathetic Afferent Fibers
Sympathetic afferent fibers carry visceral pain and reflex information from thoracic and abdominal organs back to the spinal cord. Pain from organs such as the heart, stomach, intestine, and ureter often travels with sympathetic fibers. This explains referred pain, where visceral pain is felt in body wall regions supplied by the same spinal segments.
⚠️ CLINICAL IMPORTANCE
Excessive sympathetic activation may cause tachycardia, hypertension, sweating, tremor, anxiety-like symptoms, and palpitations. Reduced sympathetic activity may cause postural hypotension, poor vascular tone, reduced sweating, and impaired stress tolerance. Sympathetic visceral pain pathways are clinically important in myocardial infarction, renal colic, and abdominal visceral pain.
MAJOR CONCEPT 3 — Parasympathetic Nervous System: Location, Level and Organization
🧠 CORE
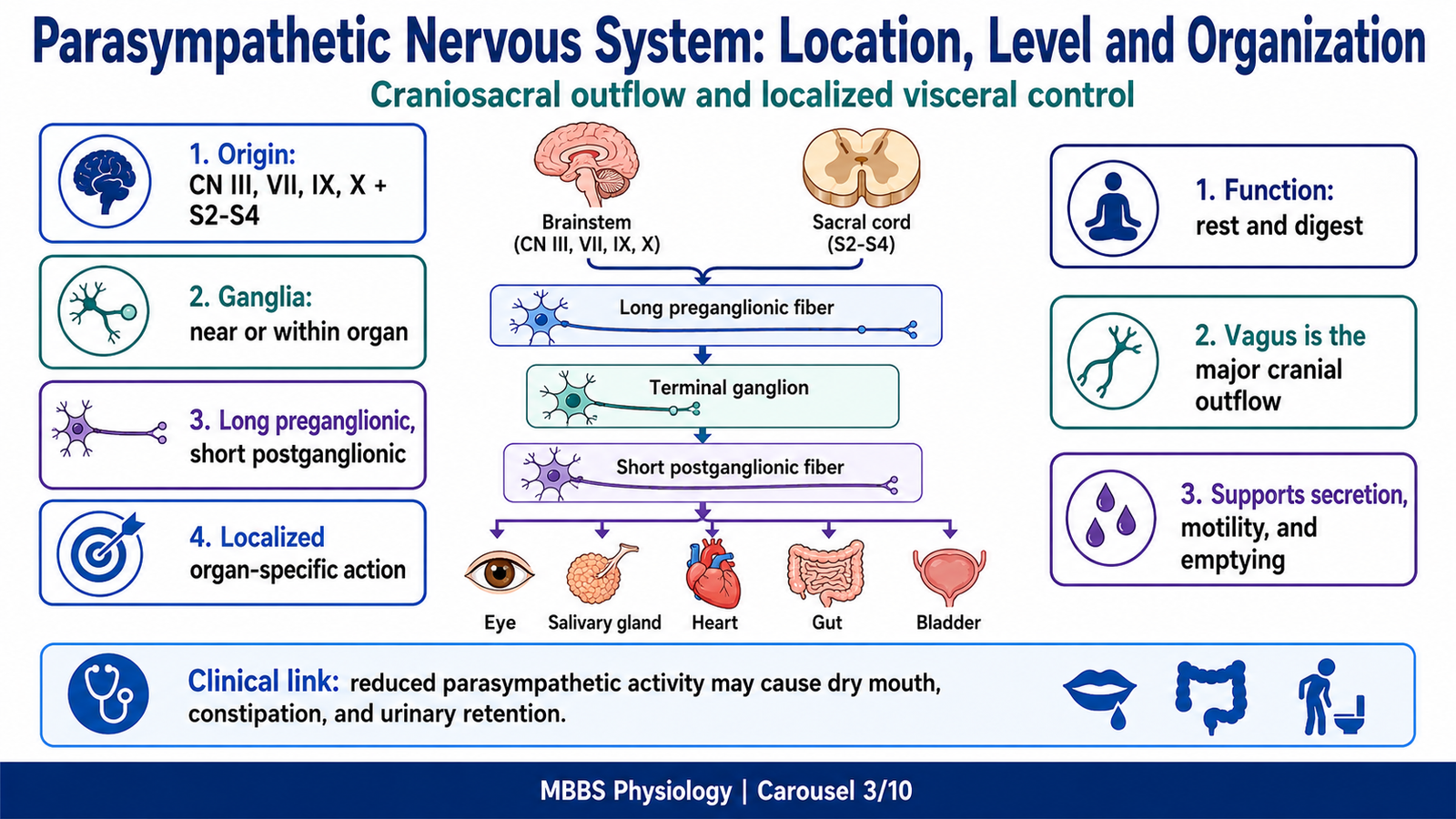
- The parasympathetic nervous system is the craniosacral division of the ANS.
- Cranial outflow travels through cranial nerves III, VII, IX, and X.
- Sacral outflow arises from S2–S4 spinal cord segments.
- Parasympathetic ganglia lie near or within target organs.
- Preganglionic fibers are long.
- Postganglionic fibers are short.
- Parasympathetic effects are usually localized and organ-specific.
- It promotes rest, digestion, secretion, storage, and elimination.
🔬 CONCEPT EXPLAINED
The parasympathetic nervous system originates from two regions: the brainstem and the sacral spinal cord. Because of this arrangement, it is called the craniosacral outflow.
The cranial parasympathetic outflow travels through cranial nerves:
- CN III: Supplies sphincter pupillae and ciliary muscle of the eye.
- CN VII: Supplies lacrimal, nasal, submandibular, and sublingual glands.
- CN IX: Supplies the parotid gland.
- CN X: Supplies thoracic and most abdominal organs, including heart, lungs, stomach, intestine, liver, pancreas, and proximal colon.
The sacral parasympathetic outflow arises from S2–S4 and supplies pelvic organs such as the distal colon, rectum, urinary bladder, and reproductive organs.
Parasympathetic ganglia are located very close to or inside the target organs. Therefore, parasympathetic preganglionic fibers are long because they must travel from the CNS almost to the organ. Postganglionic fibers are short because the ganglion lies near the target tissue.
This arrangement produces more localized control than the sympathetic system. For example, parasympathetic stimulation can increase salivary secretion without necessarily causing widespread effects throughout the whole body. Similarly, vagal activity can slow the heart while also promoting gastrointestinal motility and secretion.
The parasympathetic system exists because the body needs a mechanism for conservation, digestion, absorption, storage, and controlled elimination. It slows heart rate, constricts pupils, stimulates salivary secretion, increases gastrointestinal motility, stimulates digestive secretions, promotes bladder emptying, and supports defecation.
Distribution of Parasympathetic Efferent Fibers
Parasympathetic efferent fibers supply:
- Eye
- Lacrimal glands
- Salivary glands
- Heart
- Lungs
- Gastrointestinal tract
- Liver and pancreas
- Urinary bladder
- Rectum
- Reproductive organs
Parasympathetic supply to most blood vessels is limited, which is why vascular tone is mainly controlled by the sympathetic system.
Distribution of Parasympathetic Afferent Fibers
Parasympathetic afferent fibers carry physiological reflex information from organs to the CNS. These afferents monitor stretch, pressure, chemical changes, and organ distension. For example, vagal afferents carry information from baroreceptors, chemoreceptors, lungs, and gastrointestinal tract. Sacral afferents carry information from bladder and rectum.
⚠️ CLINICAL IMPORTANCE
Excess parasympathetic activity may produce bradycardia, excessive salivation, bronchoconstriction, abdominal cramps, diarrhea, and increased urination. Reduced parasympathetic activity may cause dry mouth, constipation, urinary retention, increased heart rate, and impaired pupillary accommodation.
MAJOR CONCEPT 4 — Comparison of Sympathetic and Parasympathetic Systems
🧠 CORE
- Sympathetic origin: T1–L2 spinal cord.
- Parasympathetic origin: cranial nerves III, VII, IX, X and S2–S4.
- Sympathetic ganglia are near the spinal cord.
- Parasympathetic ganglia are near or within target organs.
- Sympathetic preganglionic fibers are short; postganglionic fibers are long.
- Parasympathetic preganglionic fibers are long; postganglionic fibers are short.
- Both systems release acetylcholine at autonomic ganglia.
- Target organ neurotransmitters and receptors differ between the two systems.
🔬 CONCEPT EXPLAINED
The sympathetic and parasympathetic systems are both autonomic divisions, but they are organized differently because they serve different functional purposes.
The sympathetic system must often activate many organs together during stress. Therefore, its ganglia are placed near the spinal cord, and its preganglionic fibers can diverge widely. This allows rapid, coordinated body-wide activation. One preganglionic sympathetic fiber may activate many postganglionic neurons, producing widespread effects such as increased heart rate, vasoconstriction, sweating, bronchodilation, and metabolic fuel mobilization.
The parasympathetic system is designed for more precise, organ-specific regulation. Its ganglia lie near or inside target organs, so each organ can be regulated more independently. This is useful for digestion, secretion, micturition, defecation, and slowing of the heart.
Comparison Table
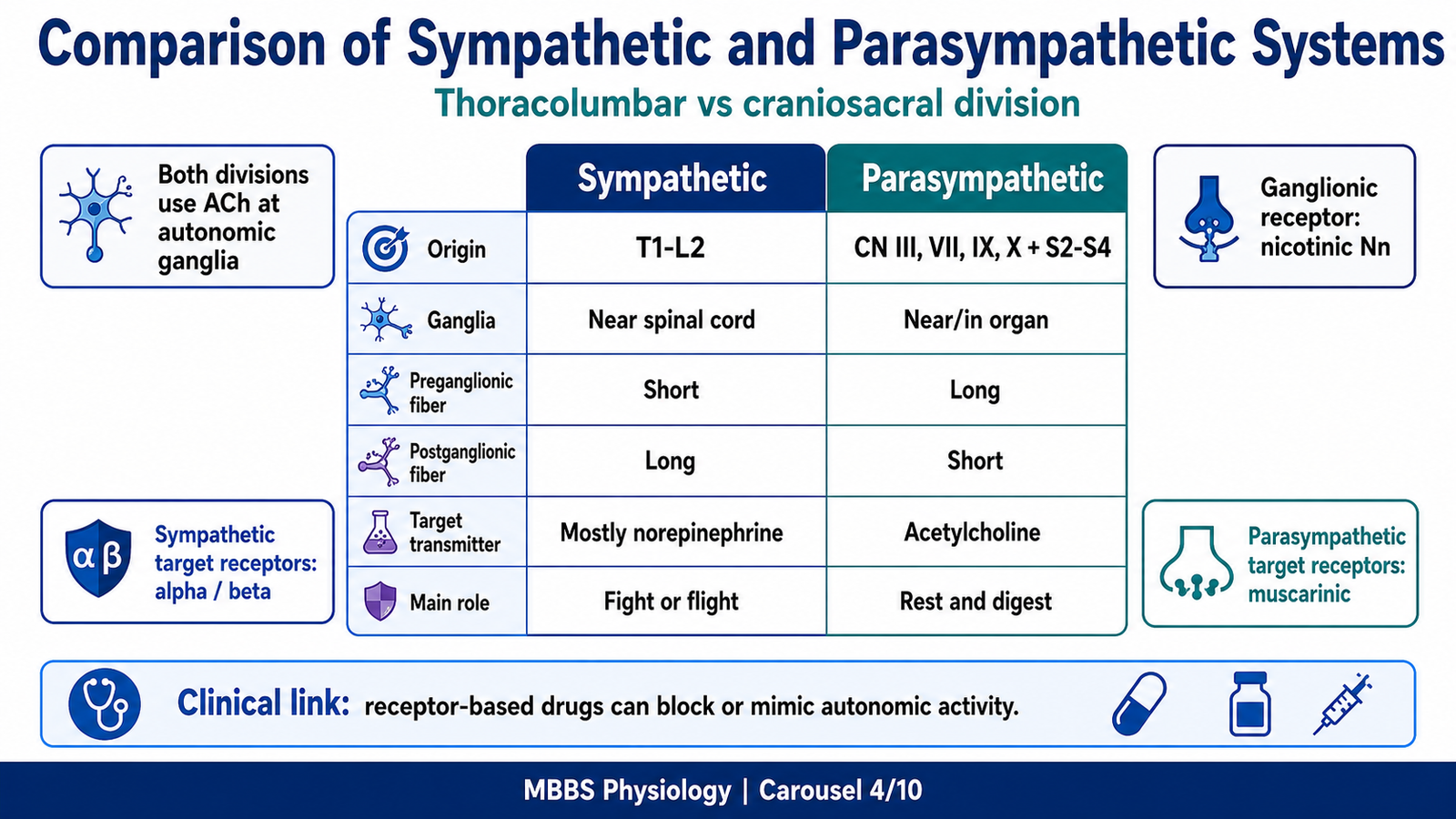
| Feature | Sympathetic Nervous System | Parasympathetic Nervous System |
|---|---|---|
| Division of origin | Thoracolumbar | Craniosacral |
| CNS origin | T1–L2 spinal cord | CN III, VII, IX, X and S2–S4 |
| Ganglia location | Near spinal cord | Near or inside target organ |
| Preganglionic fiber | Short | Long |
| Postganglionic fiber | Long | Short |
| Ganglionic neurotransmitter | Acetylcholine | Acetylcholine |
| Ganglionic receptor | Nicotinic Nn | Nicotinic Nn |
| Main target organ neurotransmitter | Mostly norepinephrine | Acetylcholine |
| Target organ receptors | Alpha and beta adrenergic receptors | Muscarinic receptors |
| Distribution | Widespread | More localized |
| General function | Fight or flight | Rest and digest |
Important Exceptions
Not all sympathetic postganglionic neurons release norepinephrine. Sympathetic fibers to most sweat glands release acetylcholine, which acts on muscarinic receptors. The adrenal medulla behaves like a modified sympathetic ganglion and releases catecholamines into blood instead of sending a postganglionic axon to a local target.
⚠️ CLINICAL IMPORTANCE
Understanding this comparison is essential for pharmacology. Drugs that block muscarinic receptors reduce parasympathetic effects and may cause dry mouth, tachycardia, constipation, urinary retention, and dilated pupils. Drugs that stimulate beta receptors may increase heart rate or dilate bronchi, while beta blockers reduce heart rate and cardiac workload.
MAJOR CONCEPT 5 — Autonomic Neurotransmitters and Receptors
🧠 CORE
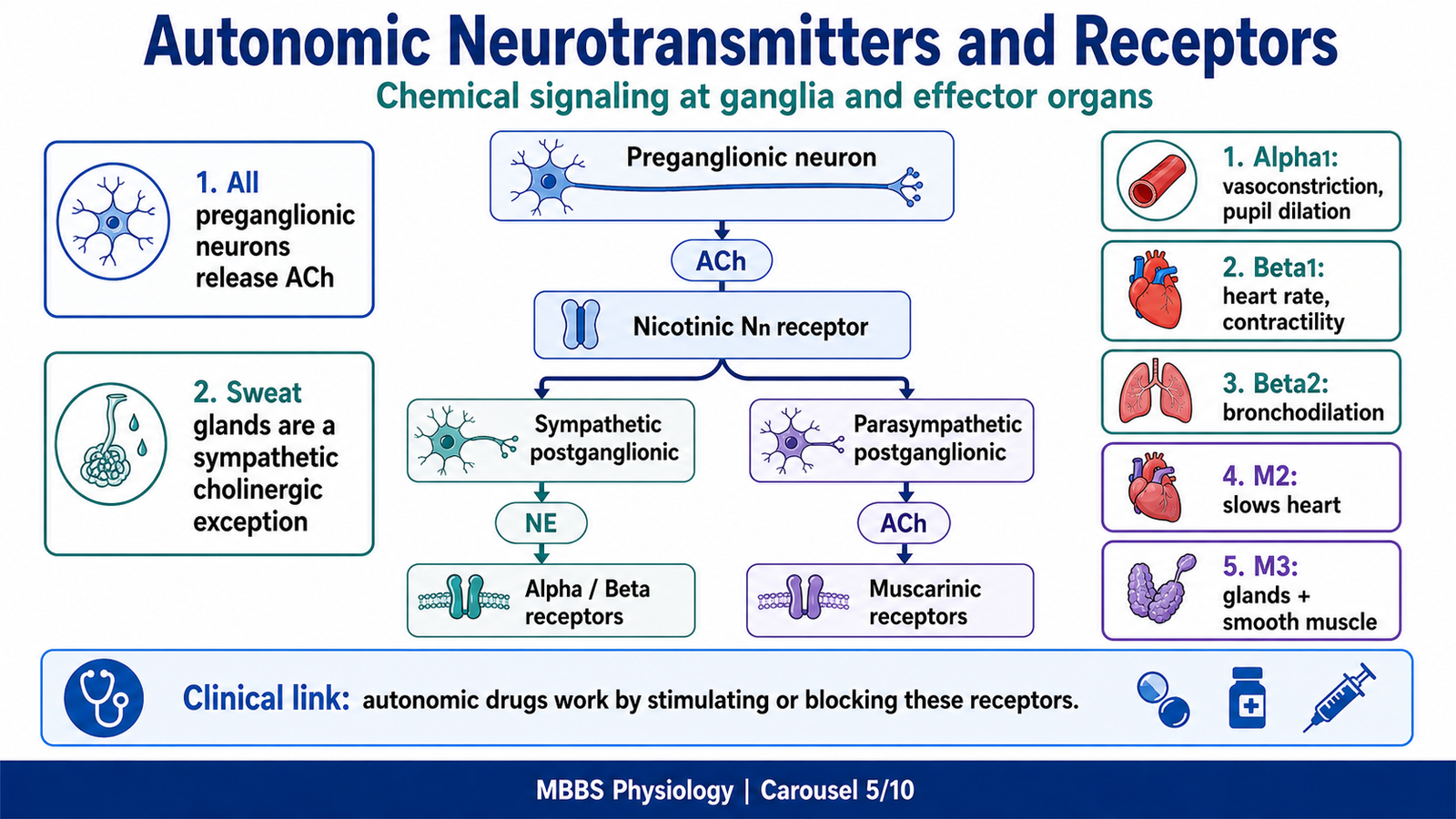
- Acetylcholine is released by all autonomic preganglionic neurons.
- Nicotinic receptors are present in autonomic ganglia.
- Most sympathetic postganglionic neurons release norepinephrine.
- Parasympathetic postganglionic neurons release acetylcholine.
- Adrenergic receptors include alpha and beta receptors.
- Muscarinic receptors mediate most parasympathetic target organ effects.
- Receptor type determines the response of the organ.
- The same neurotransmitter can produce different effects in different organs depending on receptor subtype.
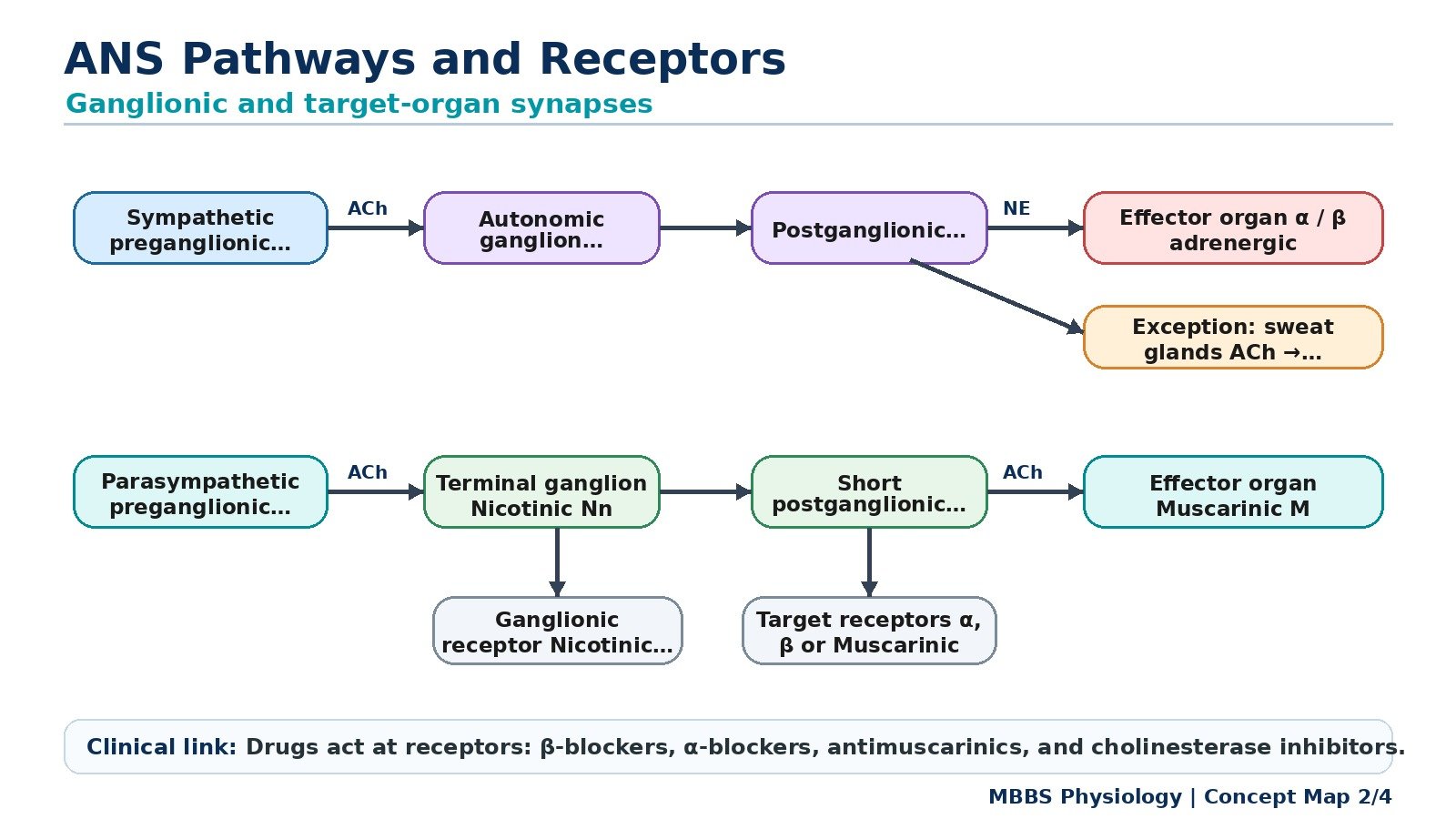
🔬 CONCEPT EXPLAINED
Autonomic function depends not only on which nerve is activated, but also on which neurotransmitter is released and which receptor is present on the target cell.
At all autonomic ganglia, both sympathetic and parasympathetic preganglionic neurons release acetylcholine. This acetylcholine acts on nicotinic neuronal receptors, also called Nn receptors, located on postganglionic neuron cell bodies. Nicotinic receptors are ion channels, so their activation produces rapid depolarization of the postganglionic neuron.
After the ganglion, the two systems differ. Most sympathetic postganglionic neurons release norepinephrine, which acts on alpha or beta adrenergic receptors on target organs. Parasympathetic postganglionic neurons release acetylcholine, which acts on muscarinic receptors.
The receptor determines the final effect. For example, sympathetic stimulation of the heart increases heart rate because cardiac cells have mainly beta-1 receptors. Sympathetic stimulation of many blood vessels causes vasoconstriction because vascular smooth muscle has mainly alpha-1 receptors. Sympathetic stimulation of bronchial smooth muscle causes bronchodilation because bronchi have beta-2 receptors.
Similarly, acetylcholine released by parasympathetic fibers slows the heart through M2 muscarinic receptors, but increases glandular secretion and smooth muscle contraction through other muscarinic receptor actions. Therefore, the same chemical messenger may produce different physiological results depending on receptor type and tissue location.
Major Receptors on Effector Organs
| Receptor | Main Location | Main Effect |
|---|---|---|
| Nicotinic Nn | Autonomic ganglia, adrenal medulla | Ganglionic transmission |
| Muscarinic M2 | Heart | Decreases heart rate and AV conduction |
| Muscarinic M3 | Glands, smooth muscle | Increases secretion, contraction of many smooth muscles |
| Alpha-1 | Blood vessels, radial muscle of iris, sphincters | Vasoconstriction, pupil dilation, sphincter contraction |
| Alpha-2 | Presynaptic nerve endings, some CNS sites | Decreases neurotransmitter release |
| Beta-1 | Heart, kidney juxtaglomerular cells | Increases heart rate, contractility, renin release |
| Beta-2 | Bronchi, some blood vessels, uterus, liver | Bronchodilation, vasodilation in skeletal muscle, relaxation, glycogenolysis |
| Beta-3 | Adipose tissue, bladder detrusor | Lipolysis, bladder relaxation |
⚠️ CLINICAL IMPORTANCE
Receptor knowledge explains drug effects and side effects. Beta-1 stimulation increases cardiac activity, while beta-1 blockade slows the heart. Alpha-1 stimulation causes vasoconstriction and raises blood pressure, while alpha-1 blockade may cause postural hypotension. Muscarinic blockade causes dry mouth, blurred vision, constipation, urinary retention, and tachycardia.
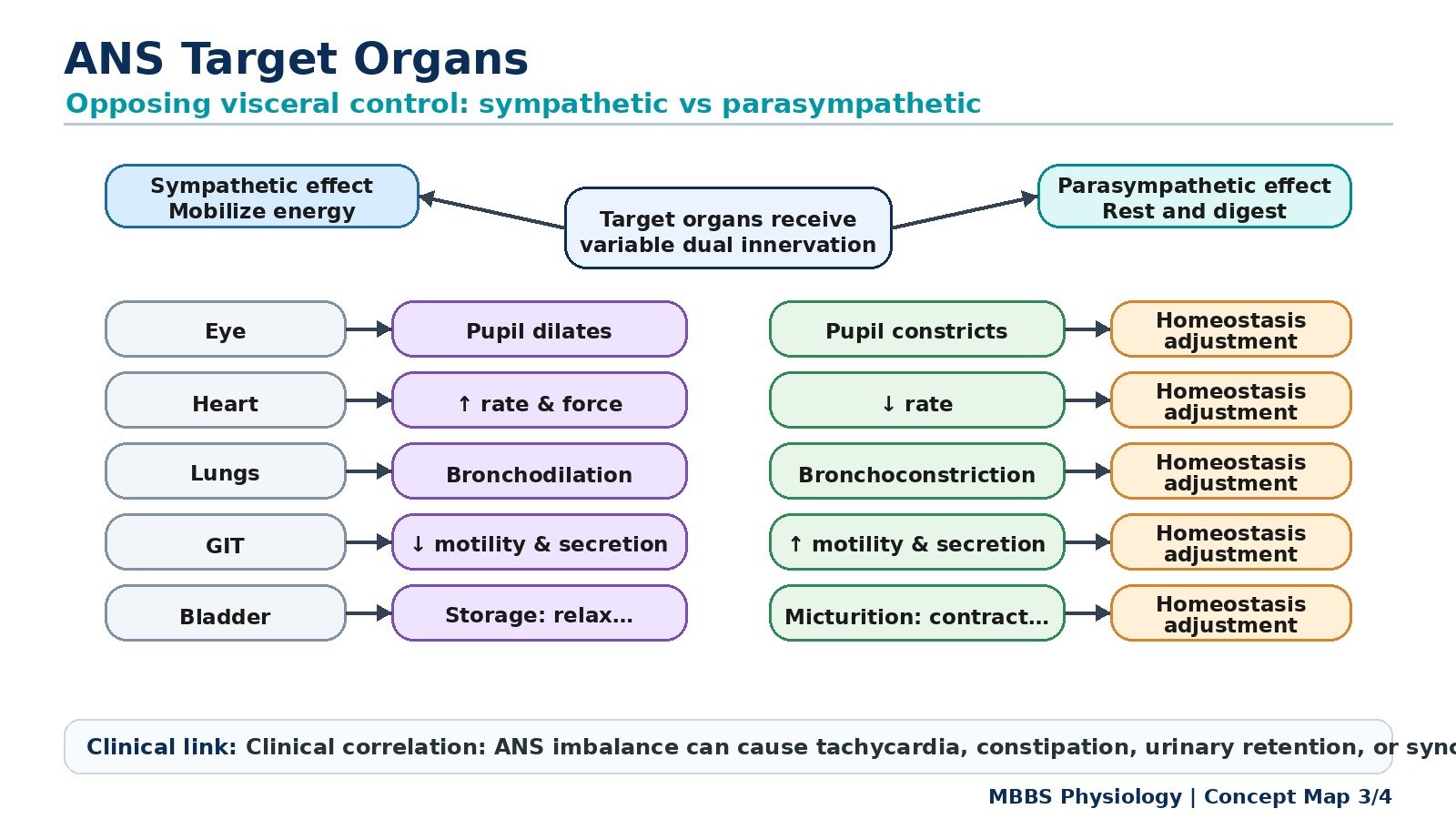
MAJOR CONCEPT 6 — Target Organs and Visceral Control
🧠 CORE
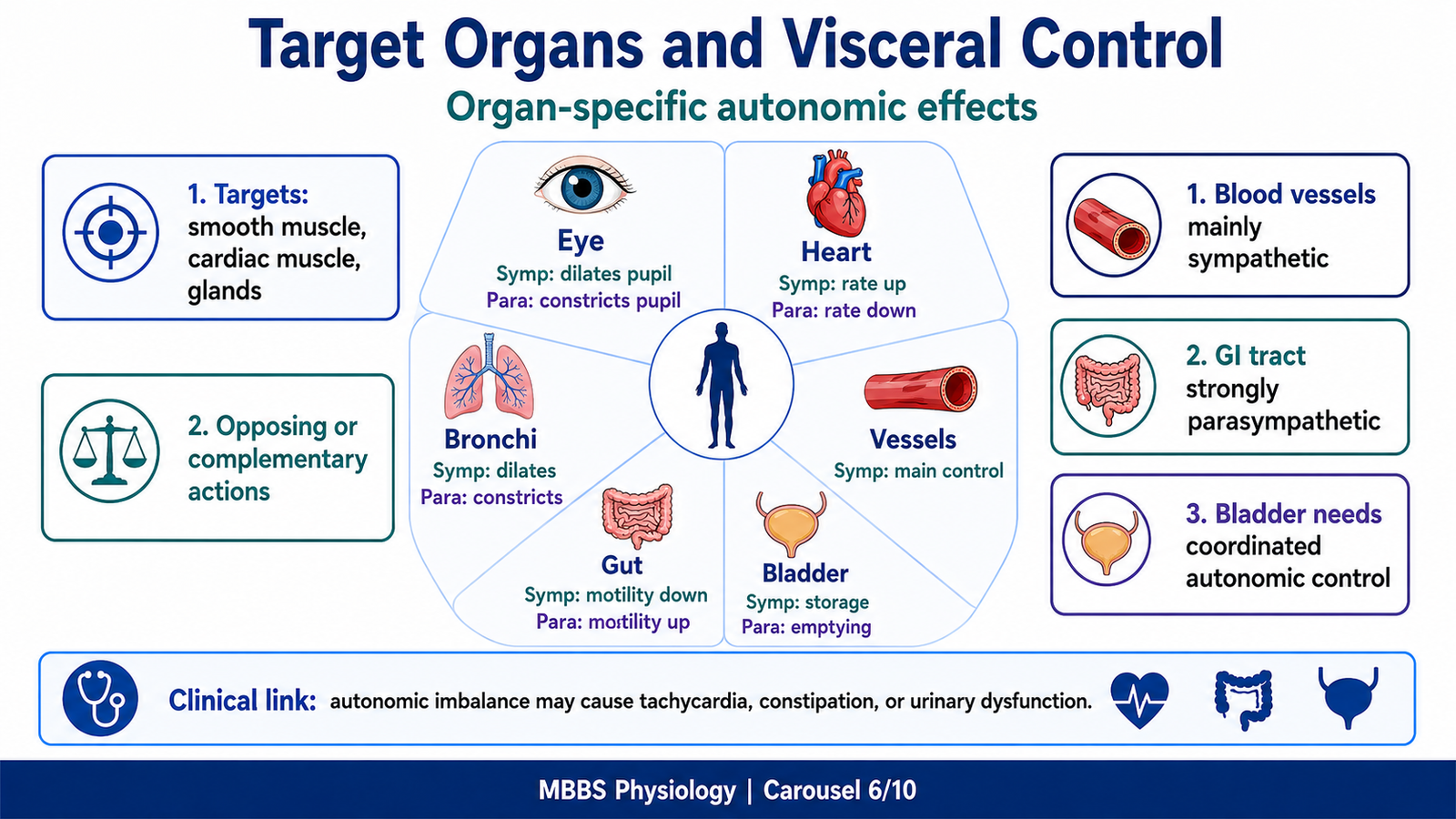
- The ANS controls cardiac muscle, smooth muscle, glands, and adrenal medulla.
- Sympathetic and parasympathetic systems may have opposite, complementary, or organ-specific effects.
- Sympathetic activity generally supports activity, stress, circulation, and energy mobilization.
- Parasympathetic activity generally supports digestion, secretion, storage, and elimination.
- Blood vessels are mainly controlled by sympathetic tone.
- The heart receives both sympathetic and parasympathetic supply.
- The gastrointestinal tract is strongly influenced by parasympathetic and enteric systems.
- Some organs receive mainly one autonomic division.
🔬 CONCEPT EXPLAINED
Target organs respond to autonomic stimulation according to their receptors, tissue structure, and functional role. The ANS does not simply “turn organs on or off.” Instead, it adjusts organ activity according to body needs.
The heart is a good example. During rest, parasympathetic vagal tone keeps the heart rate lower than its natural pacemaker rate. During exercise or stress, sympathetic stimulation increases heart rate, conduction, and contractility, allowing more blood to reach muscles and vital organs.
Blood vessels are mainly controlled by sympathetic nerves. Continuous sympathetic vasoconstrictor tone maintains arterial pressure. When sympathetic tone increases, many blood vessels constrict and blood pressure rises. When sympathetic tone decreases, vessels dilate and blood pressure falls. Parasympathetic supply to most blood vessels is minimal.
The gastrointestinal tract is mainly supported by parasympathetic activity. Parasympathetic stimulation increases motility, secretion, and digestive activity. Sympathetic stimulation reduces digestion because, during stress, blood and energy are redirected away from the gut toward skeletal muscles, heart, and brain.
The urinary bladder also shows coordinated autonomic control. During bladder filling, sympathetic activity relaxes the detrusor muscle and contracts the internal sphincter, allowing storage of urine. During micturition, parasympathetic activity contracts the detrusor and relaxes bladder outlet mechanisms, allowing emptying.
Target Organ Effects
| Organ | Sympathetic Effect | Parasympathetic Effect |
|---|---|---|
| Eye | Pupil dilation | Pupil constriction, accommodation |
| Heart | Increased rate, force, conduction | Decreased rate and AV conduction |
| Bronchi | Bronchodilation | Bronchoconstriction, secretion |
| Blood vessels | Mostly vasoconstriction | Usually little direct effect |
| Sweat glands | Increased sweating | No significant effect |
| GI tract | Decreased motility and secretion | Increased motility and secretion |
| Liver | Glycogenolysis, glucose release | Minor digestive/metabolic support |
| Pancreas | Modifies secretion | Increases digestive enzyme secretion |
| Bladder | Urine storage | Urine emptying |
| Genital organs | Ejaculation | Erection |
⚠️ CLINICAL IMPORTANCE
Autonomic imbalance produces predictable organ dysfunction. Excess sympathetic activity may cause tachycardia, hypertension, sweating, dilated pupils, constipation, and urinary retention. Excess parasympathetic activity may cause bradycardia, bronchoconstriction, abdominal cramps, diarrhea, and increased urination.
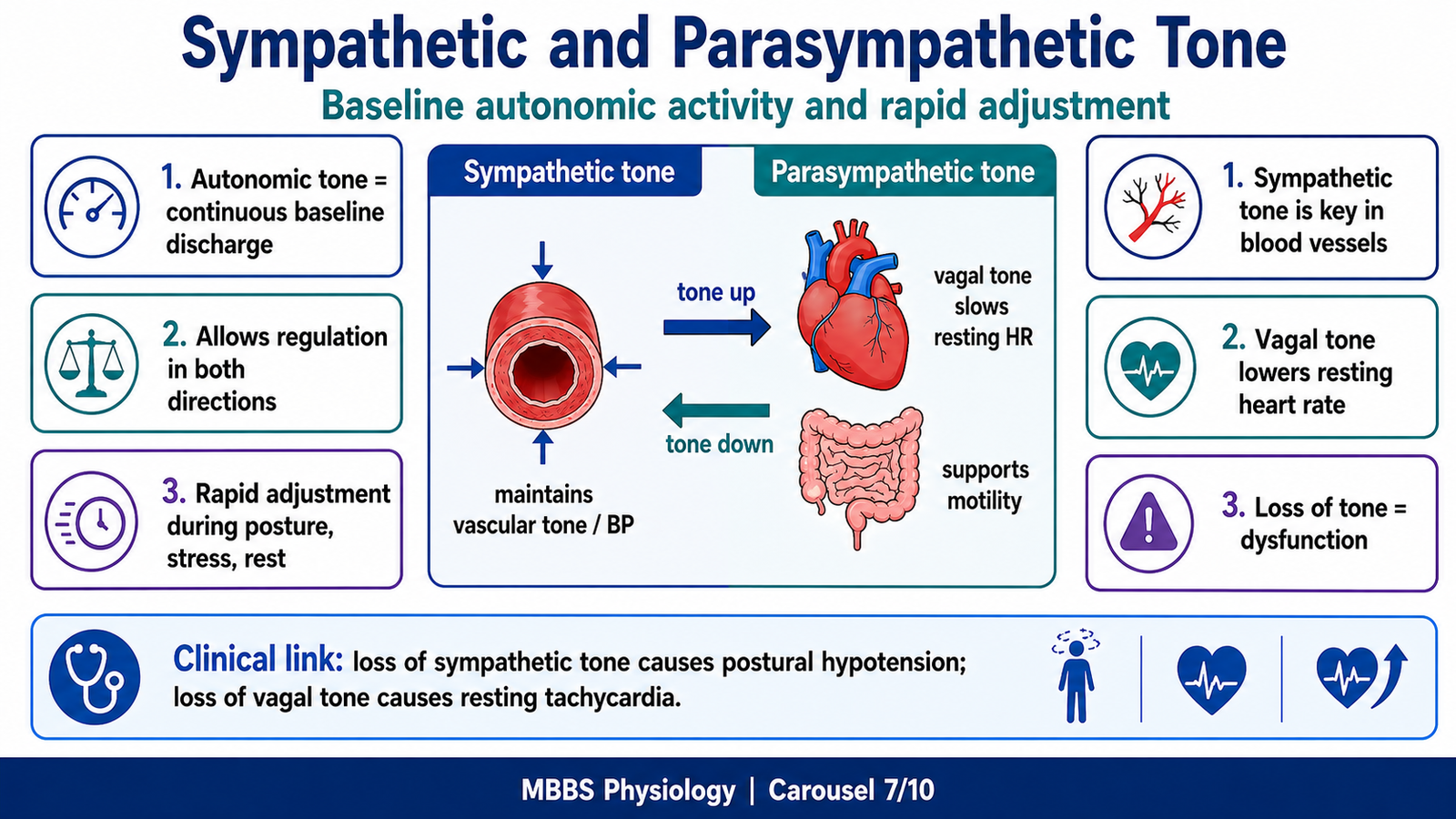
MAJOR CONCEPT 7 — Sympathetic and Parasympathetic Tone
🧠 CORE
- Autonomic tone means continuous baseline autonomic activity.
- Sympathetic tone is especially important in blood vessels.
- Parasympathetic tone is especially important in the heart and gastrointestinal tract.
- Tone allows organs to be regulated in both directions.
- Increased or decreased tone changes organ function rapidly.
- Vagal tone keeps resting heart rate below intrinsic SA node rate.
- Sympathetic vascular tone maintains blood pressure.
- Loss of tone causes major clinical dysfunction.
🔬 CONCEPT EXPLAINED
Autonomic organs are not controlled only by sudden bursts of activity. Many organs receive continuous low-level autonomic stimulation called autonomic tone. This tone is important because it allows fine adjustment.
For example, blood vessels are normally partially constricted because of continuous sympathetic tone. If the body needs to increase blood pressure, sympathetic tone increases and vessels constrict more. If the body needs to reduce vascular resistance, sympathetic tone decreases and vessels dilate. Therefore, regulation is possible in both directions.
The heart is strongly influenced by parasympathetic tone at rest. The SA node has an intrinsic firing rate that is higher than normal resting heart rate. Vagal parasympathetic tone slows the SA node, keeping resting heart rate around normal resting levels. During exercise, withdrawal of vagal tone first increases heart rate, and then sympathetic stimulation further increases it.
The gastrointestinal tract also depends on parasympathetic tone for digestive readiness. Parasympathetic activity supports motility and secretion, while sympathetic activity suppresses these processes during stress.
Mechanism of Autonomic Tone
Stimulus or initiating event:
The body continuously needs stable blood pressure, heart rate, digestion, temperature control, and organ perfusion.
Purpose:
Autonomic tone exists so that organs are not inactive at baseline. Instead, they remain partially active and can be adjusted upward or downward quickly.
Sequential events:
Central autonomic centers continuously send low-frequency impulses to autonomic neurons. These impulses maintain basal neurotransmitter release at target organs. The target organs remain in a controlled baseline state. When body needs change, central output increases or decreases.
Cause → Effect relationship:
Increased sympathetic vascular tone causes vasoconstriction and increased blood pressure. Decreased sympathetic vascular tone causes vasodilation and reduced blood pressure. Increased vagal tone slows heart rate. Decreased vagal tone increases heart rate.
Control and regulation:
Tone is regulated by baroreceptors, chemoreceptors, hypothalamus, brainstem cardiovascular centers, temperature centers, emotional centers, and local metabolic needs.
Functional outcome:
The body maintains stable internal conditions despite changes in posture, exercise, stress, temperature, and digestion.
Physiological advantage:
Tone allows rapid adjustment without needing to start from zero activity.
Clinical consequence if impaired:
Loss of sympathetic tone may cause postural hypotension and fainting. Loss of vagal tone may produce resting tachycardia. Excess tone may cause hypertension, bradycardia, or abnormal organ activity depending on the affected division.
⚠️ CLINICAL IMPORTANCE
Postural hypotension is a classic example of impaired sympathetic tone. When a person stands, gravity pulls blood into lower limbs. Normally sympathetic tone increases to constrict blood vessels and maintain blood pressure. If this response fails, cerebral blood flow falls and the person may feel dizzy or faint.
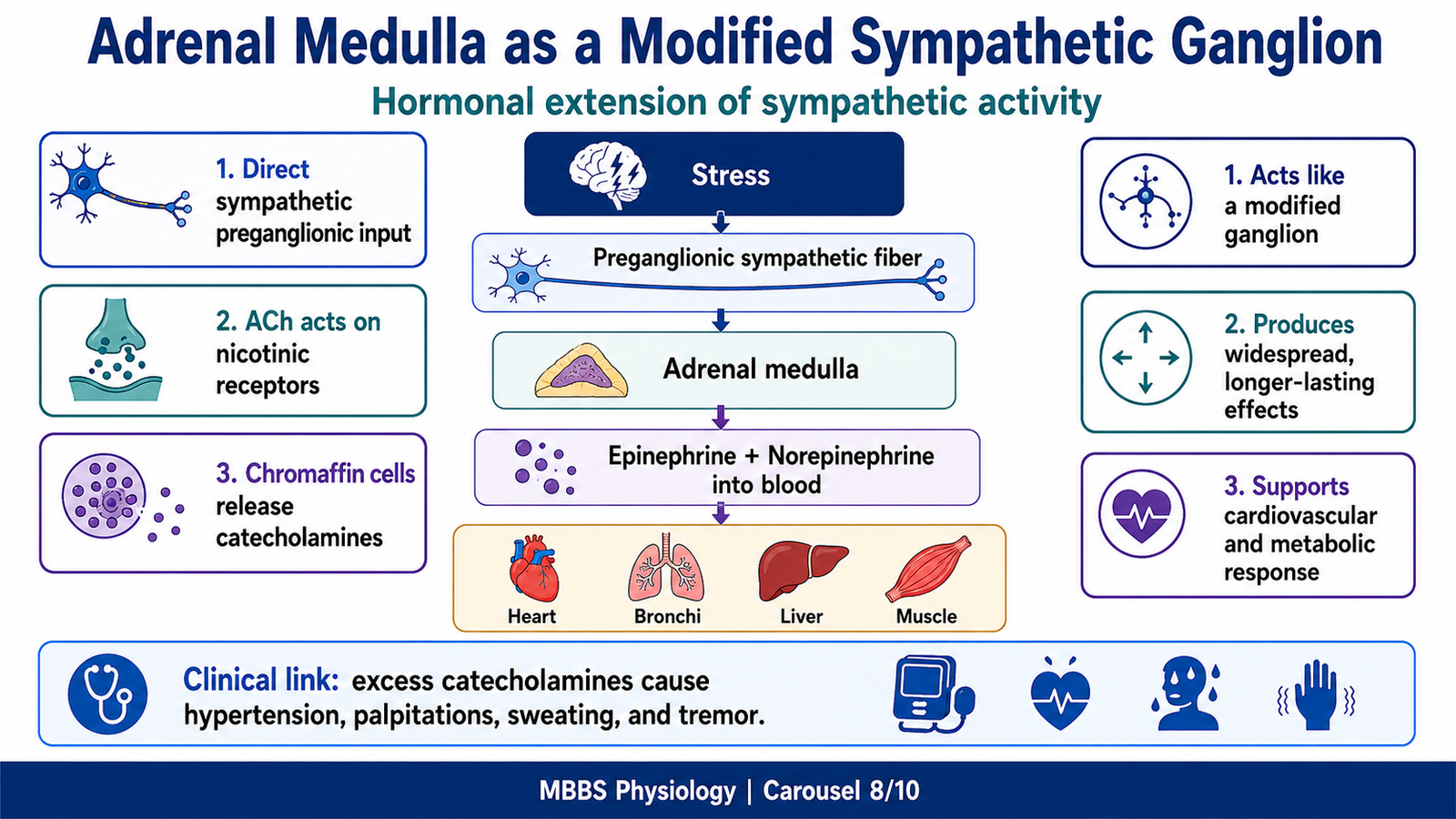
MAJOR CONCEPT 8 — Adrenal Medulla as a Modified Sympathetic Ganglion
🧠 CORE
- The adrenal medulla is functionally part of the sympathetic nervous system.
- It acts like a modified sympathetic ganglion.
- It receives sympathetic preganglionic fibers directly.
- Preganglionic fibers release acetylcholine.
- Chromaffin cells respond through nicotinic receptors.
- The adrenal medulla secretes epinephrine and norepinephrine into blood.
- Its hormonal secretion produces widespread and prolonged sympathetic effects.
- It is important in stress response and metabolic mobilization.
🔬 CONCEPT EXPLAINED
The adrenal medulla is unique because it does not send a typical postganglionic neuron to a target organ. Instead, it acts as a modified sympathetic ganglion. Sympathetic preganglionic fibers directly innervate chromaffin cells in the adrenal medulla. These chromaffin cells are embryologically and functionally similar to postganglionic sympathetic neurons.
When sympathetic preganglionic neurons are activated, they release acetylcholine onto nicotinic receptors on chromaffin cells. This stimulates chromaffin cells to release catecholamines, mainly epinephrine and some norepinephrine, directly into the bloodstream.
This mechanism exists because emergency responses must affect the whole body, not only organs directly innervated by sympathetic nerves. Circulating epinephrine reaches the heart, blood vessels, liver, skeletal muscle, adipose tissue, and bronchi. It increases cardiac output, mobilizes glucose, promotes lipolysis, dilates bronchi, and supports blood flow redistribution.
Mechanism of Adrenal Medullary Response
Stimulus or initiating event:
Stress, fear, trauma, pain, hypoglycemia, exercise, hemorrhage, or severe emotional arousal activates sympathetic centers.
Purpose:
The adrenal medulla provides a hormonal extension of the sympathetic system so that the body can generate a widespread and longer-lasting response.
Sequential physiological events:
Stress activates hypothalamic and brainstem sympathetic centers. Preganglionic sympathetic neurons fire. Acetylcholine is released onto adrenal medullary chromaffin cells. Nicotinic receptors are activated. Chromaffin cells secrete epinephrine and norepinephrine into blood. Catecholamines circulate to distant organs and activate adrenergic receptors.
Cause → Effect relationship:
Catecholamines stimulate beta-1 receptors in the heart, causing increased heart rate and contractility. They stimulate beta-2 receptors in bronchi, causing bronchodilation. They stimulate metabolic receptors in liver and adipose tissue, causing glucose and fatty acid mobilization.
Control and regulation:
Adrenal medullary output is controlled by sympathetic preganglionic activity, which is regulated by hypothalamus, brainstem, emotional centers, blood pressure status, glucose level, pain, and stress signals.
Functional outcome:
The body becomes prepared for rapid action, increased oxygen delivery, increased blood glucose availability, and improved cardiovascular performance.
Physiological advantage:
Hormonal secretion produces effects that are more widespread and longer lasting than nerve stimulation alone.
Clinical consequence if impaired:
Reduced adrenal medullary response may impair stress tolerance. Excess catecholamine secretion can cause palpitations, hypertension, sweating, tremor, headache, and anxiety-like symptoms.
⚠️ CLINICAL IMPORTANCE
Tumors of adrenal medulla can produce excess catecholamines, leading to episodic hypertension, palpitations, sweating, headache, and tremor. At undergraduate level, the key concept is that excess catecholamines exaggerate sympathetic effects.
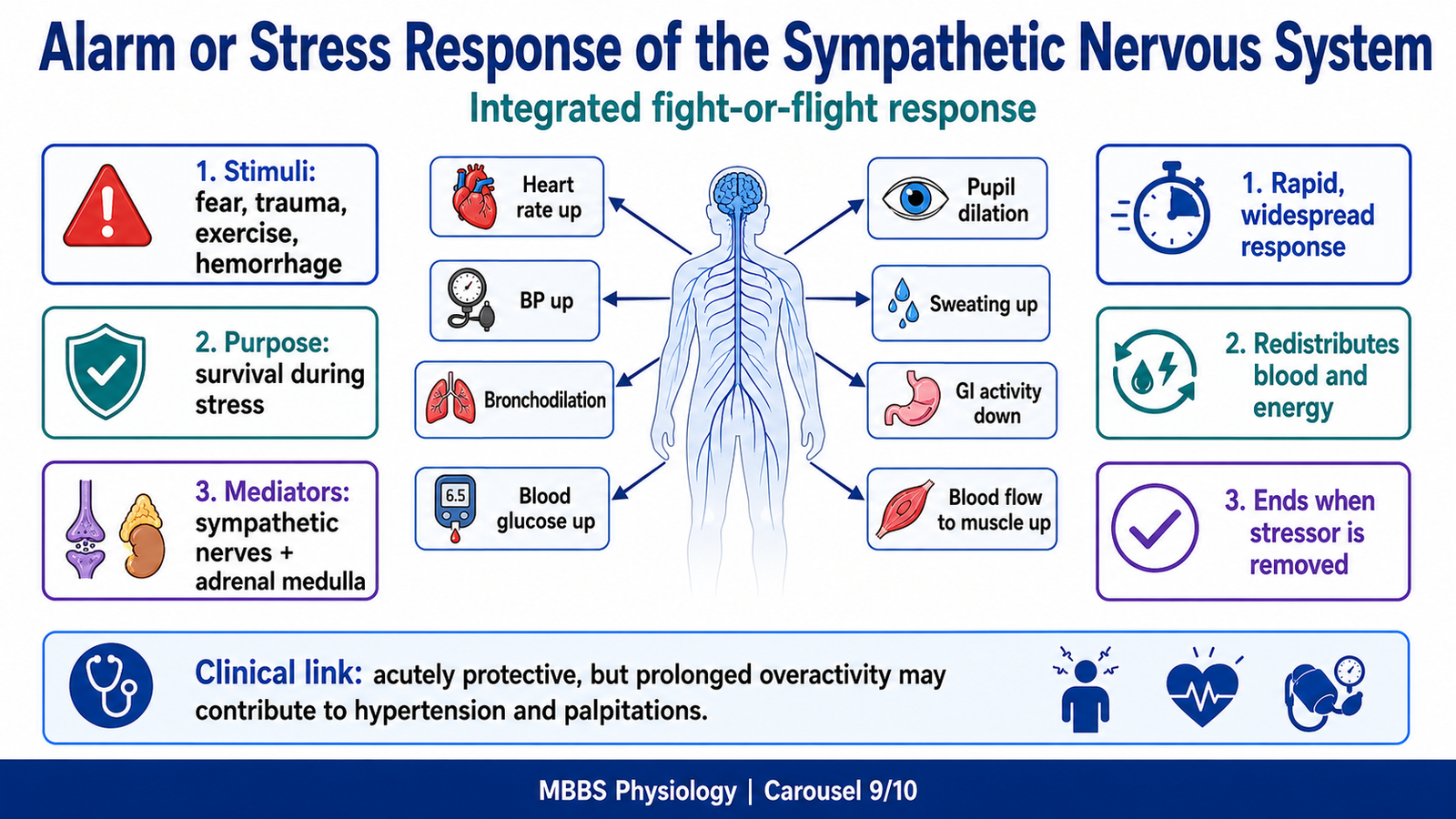
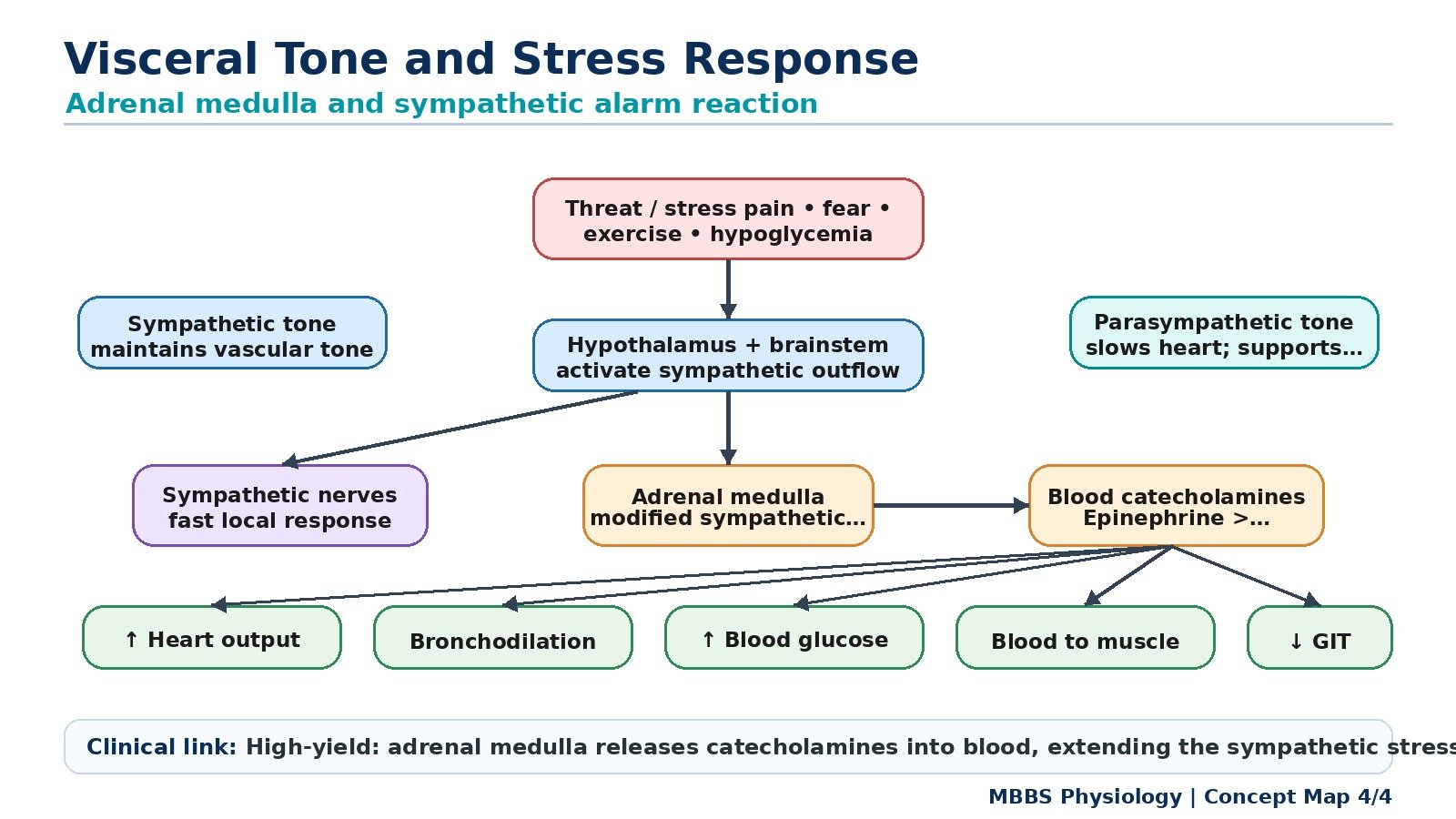
MAJOR CONCEPT 9 — Alarm or Stress Response of the Sympathetic Nervous System
🧠 CORE
- The alarm response is the body’s emergency sympathetic response.
- It prepares the body for fight, flight, injury, fear, or severe stress.
- It involves sympathetic nerves and adrenal medulla.
- Heart rate and cardiac output increase.
- Bronchi dilate to improve air entry.
- Blood is redistributed toward skeletal muscles and vital organs.
- Blood glucose and fatty acids increase.
- Digestion and urinary activity are suppressed.
🔬 CONCEPT EXPLAINED
The alarm response is one of the most important integrated functions of the sympathetic nervous system. It occurs when the brain detects danger, fear, pain, trauma, exercise, hemorrhage, or severe stress. The body must rapidly shift from a resting state to a survival state.
Mechanism of Sympathetic Alarm Response
Stimulus or initiating event:
A stressor such as fear, trauma, exercise, blood loss, pain, hypoglycemia, or emotional stress activates higher brain centers and the hypothalamus.
Purpose:
The purpose of the alarm response is to protect life by preparing the body for immediate action, maintaining blood pressure, increasing oxygen delivery, and mobilizing energy stores.
Sequential physiological events:
The hypothalamus activates sympathetic centers in the brainstem and spinal cord. Sympathetic preganglionic neurons stimulate sympathetic ganglia and adrenal medulla. Postganglionic sympathetic fibers release norepinephrine at target organs. The adrenal medulla releases epinephrine and norepinephrine into blood. These neurotransmitters and hormones act on adrenergic receptors in multiple organs.
Cause → Effect relationships:
Stimulation of beta-1 receptors in the heart increases heart rate and force of contraction, which increases cardiac output. Stimulation of alpha-1 receptors in many blood vessels causes vasoconstriction, helping maintain blood pressure. Stimulation of beta-2 receptors in bronchi causes bronchodilation, improving oxygen intake. Stimulation of liver and adipose tissue increases glucose and fatty acid availability. Reduced gastrointestinal activity conserves blood and energy for emergency organs.
Control and regulation:
The response is controlled by hypothalamus, limbic system, brainstem autonomic centers, adrenal medulla, baroreceptor reflexes, chemoreceptor reflexes, and circulating catecholamine levels. Once the stressor ends, sympathetic output decreases and parasympathetic activity helps restore resting functions.
Functional outcome:
The body becomes alert, cardiovascular performance increases, air entry improves, blood glucose rises, sweating increases, pupils dilate, and digestive activity decreases.
Physiological advantage:
The alarm response increases survival during sudden danger by ensuring that oxygen, blood flow, and energy reach the tissues most needed for action.
Clinical consequence if impaired:
If the response is inadequate, the person may fail to maintain blood pressure during stress or hemorrhage. If excessive or prolonged, it may contribute to tachycardia, hypertension, anxiety symptoms, palpitations, sweating, tremor, and metabolic strain.
⚠️ CLINICAL IMPORTANCE
The sympathetic alarm response is useful acutely but harmful if excessive or prolonged. Chronic sympathetic overactivity can increase cardiovascular workload and may contribute to hypertension and stress-related symptoms. In shock, sympathetic activation is initially compensatory because it attempts to maintain blood pressure and perfusion.
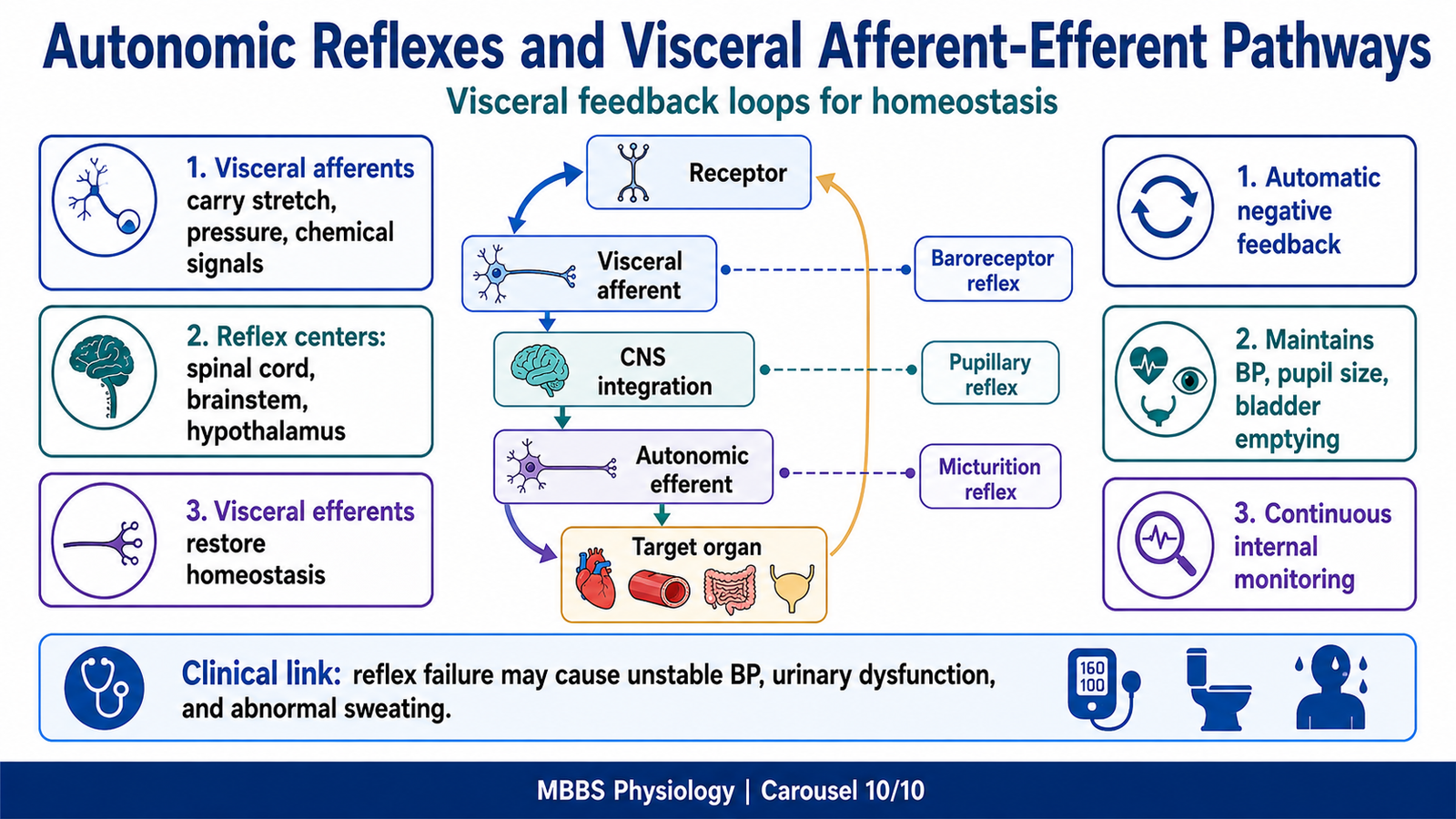
MAJOR CONCEPT 10 — Autonomic Reflexes and Visceral Afferent-Efferent Pathways
🧠 CORE
- Autonomic reflexes maintain homeostasis without conscious effort.
- Visceral afferents carry information from organs to CNS.
- Visceral efferents carry autonomic commands from CNS to organs.
- Reflex centers are present in spinal cord, brainstem, and hypothalamus.
- Baroreceptor reflex regulates blood pressure.
- Pupillary light reflex regulates pupil size.
- Micturition reflex regulates bladder emptying.
- Defecation and gastrointestinal reflexes regulate digestive function.
🔬 CONCEPT EXPLAINED
Autonomic control depends on both sensory input and motor output. Internal organs constantly send information to the CNS through visceral afferent fibers. These fibers detect stretch, pressure, chemical composition, irritation, ischemia, and organ distension. The CNS processes this information and sends autonomic efferent output back to target organs.
For example, when blood pressure rises, baroreceptors in the carotid sinus and aortic arch increase their firing. This information reaches the brainstem. The brainstem then reduces sympathetic output and increases parasympathetic vagal output to the heart. Heart rate and vascular tone decrease, bringing blood pressure back toward normal. This is a classic negative feedback autonomic reflex.
In the bladder, stretch receptors detect filling. When bladder volume becomes sufficient, afferent signals reach sacral spinal centers and higher centers. Parasympathetic efferent activity can then contract the detrusor muscle and allow micturition when socially appropriate.
Autonomic reflexes exist because internal organs need rapid automatic regulation. Conscious control is limited and delayed, so visceral afferent-efferent loops protect homeostasis continuously.
⚠️ CLINICAL IMPORTANCE
Damage to autonomic reflex pathways may cause unstable blood pressure, urinary retention or incontinence, constipation, abnormal sweating, pupillary abnormalities, and impaired cardiovascular responses to posture.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
The autonomic nervous system is structurally arranged as a two-neuron chain because visceral organs require regulated, modifiable control rather than direct voluntary activation. Preganglionic neurons connect the CNS to ganglia, while postganglionic neurons distribute signals to target organs.
In the sympathetic system, ganglia are close to the spinal cord. This structure allows one preganglionic neuron to influence many postganglionic neurons. The functional result is widespread activation, suitable for stress and emergency responses.
In the parasympathetic system, ganglia are near or within target organs. This structure allows more specific organ control. The functional result is localized regulation of digestion, secretion, cardiac slowing, bladder emptying, and defecation.
Receptors provide the final link between nerve signal and organ response. The same autonomic neurotransmitter can cause different outcomes depending on the receptor. For example, adrenergic stimulation increases heart activity through beta-1 receptors but relaxes bronchi through beta-2 receptors. Therefore:
Neural pathway structure → neurotransmitter release → receptor activation → organ response → homeostatic outcome
The adrenal medulla adds an endocrine dimension to autonomic control. Instead of sending a postganglionic axon, it releases catecholamines into blood. This produces widespread and prolonged sympathetic support during stress.
🩺 5️⃣ Clinical Correlation
1. Postural Hypotension
When a person stands, blood pools in the lower limbs. Normally sympathetic tone increases, causing vasoconstriction and maintenance of blood pressure. If sympathetic reflexes fail, blood pressure falls, cerebral perfusion decreases, and dizziness or fainting may occur.
2. Tachycardia and Palpitations
Excess sympathetic stimulation of beta-1 receptors in the heart increases heart rate and contractility. This may produce palpitations and increased cardiac workload.
3. Bronchoconstriction
Excess parasympathetic muscarinic activity in the bronchi can cause bronchoconstriction and increased secretions. This is clinically relevant in obstructive airway disease concepts.
4. Urinary Retention
Excess sympathetic activity or reduced parasympathetic activity may relax the bladder detrusor and increase outlet resistance, causing difficulty in bladder emptying.
5. Dry Mouth and Constipation
Reduced parasympathetic activity or muscarinic receptor blockade decreases salivary secretion and gastrointestinal motility. This causes dry mouth and constipation.
6. Excess Catecholamine Effects
Excess adrenal medullary catecholamine activity can cause episodic hypertension, sweating, tremor, palpitations, and headache due to exaggerated sympathetic effects.
7. Referred Visceral Pain
Pain afferents from thoracic and abdominal organs often travel with sympathetic fibers to spinal cord segments. Because somatic and visceral afferents may enter the same spinal segments, pain may be perceived in body wall regions rather than directly over the diseased organ.
📌 6️⃣ Summary Points
- The ANS controls involuntary visceral functions through sympathetic and parasympathetic divisions.
- Sympathetic outflow is thoracolumbar: T1–L2.
- Parasympathetic outflow is craniosacral: CN III, VII, IX, X and S2–S4.
- Sympathetic preganglionic fibers are usually short and postganglionic fibers are long.
- Parasympathetic preganglionic fibers are usually long and postganglionic fibers are short.
- All autonomic preganglionic neurons release acetylcholine onto nicotinic receptors.
- Most sympathetic postganglionic neurons release norepinephrine onto alpha and beta receptors.
- Parasympathetic postganglionic neurons release acetylcholine onto muscarinic receptors.
- Sweat glands are an important sympathetic exception because they receive cholinergic sympathetic fibers.
- Sympathetic tone maintains vascular tone and blood pressure.
- Parasympathetic vagal tone keeps resting heart rate lower than the intrinsic SA node rate.
- The adrenal medulla is a modified sympathetic ganglion that releases catecholamines into blood.