
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
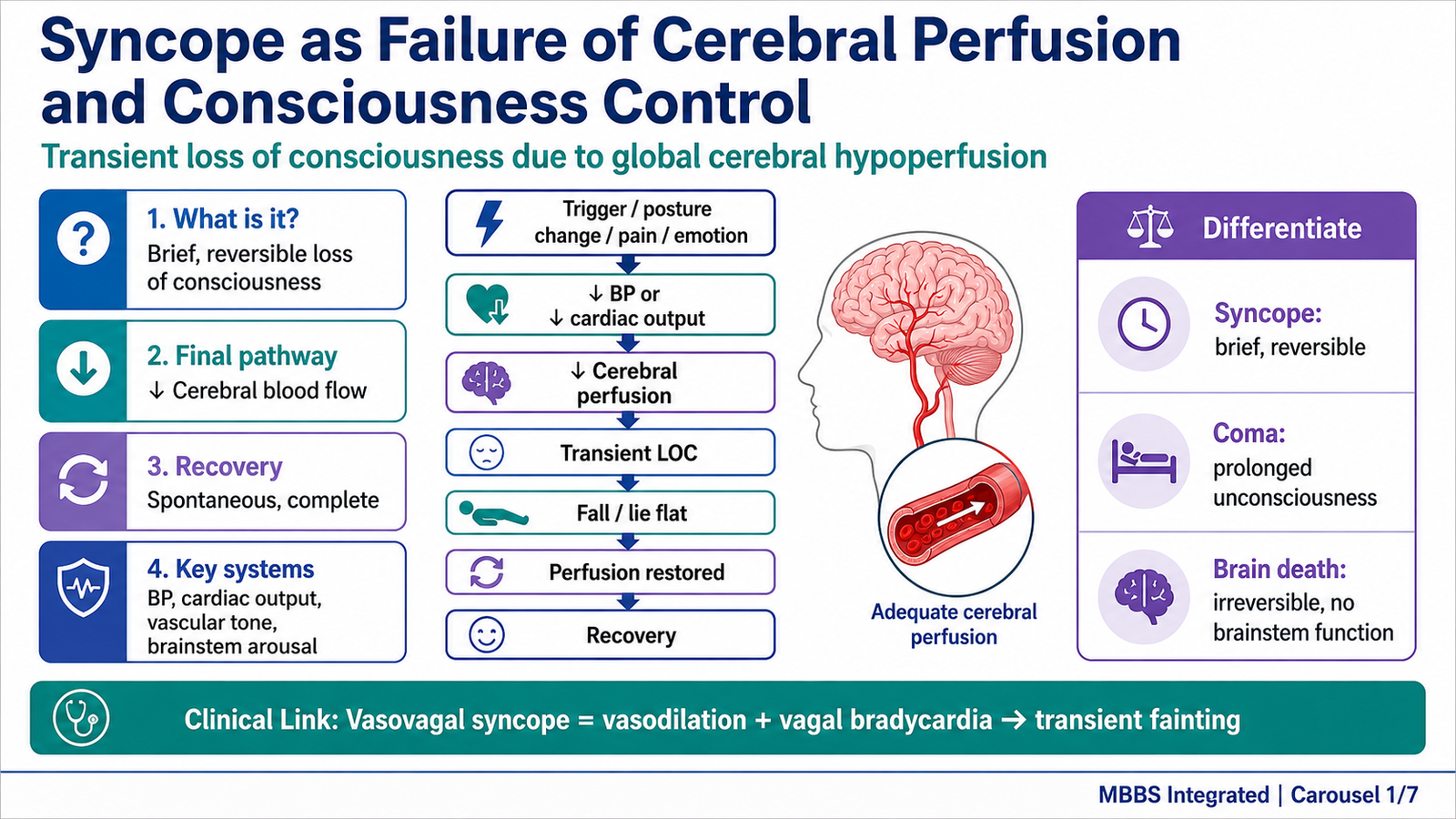
Syncope is a sudden, brief, reversible loss of consciousness caused by temporary reduction of cerebral blood flow. It is clinically important because it may arise from autonomic imbalance, vascular tone failure, cardiac causes, or brainstem arousal dysfunction. The autonomic nervous system controls heart rate, blood vessel tone, blood pressure, pupil size, bronchial tone, glandular secretion, and visceral smooth muscle activity. Therefore, drugs acting on sympathetic and parasympathetic systems can either correct autonomic dysfunction or produce dangerous adverse effects such as hypotension, bradycardia, tachycardia, and fainting.
Brain death is a different and irreversible state in which all functions of the brain, including brainstem activity, are permanently lost. In clinical and medicolegal practice, distinguishing syncope from coma and brain death is essential because syncope is reversible, coma is prolonged unconsciousness with some brain function preserved, while brain death is legally and medically equivalent to death in many jurisdictions. This topic integrates autonomic pharmacology with consciousness, vascular tone, brainstem function, and forensic certification.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Syncope: Sudden, brief loss of consciousness due to transient global cerebral hypoperfusion, followed by spontaneous recovery.
- Autonomic nervous system: Part of the nervous system controlling involuntary functions such as heart rate, vascular tone, glandular secretion, and visceral smooth muscle.
- Sympathetic nervous system: Thoracolumbar autonomic division mainly involved in “fight or flight” responses.
- Parasympathetic nervous system: Craniosacral autonomic division mainly involved in “rest and digest” functions.
- Adrenergic drugs: Drugs that act on sympathetic receptors or modify norepinephrine/adrenaline activity.
- Cholinergic drugs: Drugs that act on parasympathetic receptors or modify acetylcholine activity.
- Brainstem arousal systems: Neural networks in the reticular formation that maintain wakefulness and consciousness.
- Coma: Prolonged state of unconsciousness in which the patient cannot be aroused.
- Brain death: Irreversible loss of all brain functions, including brainstem reflexes and spontaneous respiration.
- Medicolegal certification: Official medical documentation confirming death according to accepted clinical and legal criteria.
Essential Terminology
- Adrenergic receptors: Alpha and beta receptors activated mainly by norepinephrine and adrenaline.
- Cholinergic receptors: Muscarinic and nicotinic receptors activated by acetylcholine.
- Vascular tone: Degree of contraction of blood vessel smooth muscle, important for blood pressure control.
- Baroreceptor reflex: Reflex mechanism that maintains blood pressure by adjusting heart rate and vascular tone.
- Cerebral perfusion: Blood flow to the brain.
- Brainstem reflexes: Reflexes mediated through cranial nerve nuclei in the brainstem, such as pupillary, corneal, oculocephalic, and gag reflexes.
Basic Overview
- Consciousness depends on adequate cerebral blood flow and intact brainstem arousal systems.
- Syncope occurs when cerebral perfusion temporarily falls below the level required to maintain awareness.
- Sympathetic activity usually helps maintain blood pressure by increasing heart rate, contractility, and vasoconstriction.
- Parasympathetic activity slows the heart and supports digestive and secretory functions.
- Drugs acting on these systems can either support circulation or disturb autonomic balance.
- Brain death differs from syncope because it involves irreversible loss of brain and brainstem function.
- Forensic certification of brain death has major legal importance for death declaration, organ donation, and prevention of medicolegal disputes.
🔹 3️⃣ Core Learning — Curriculum Coverage
MAJOR CONCEPTUAL HEADING 1
Syncope as Failure of Cerebral Perfusion and Consciousness Control
🧠 CORE
- Syncope is caused by transient global reduction of blood flow to the brain.
- It is usually brief and followed by complete spontaneous recovery.
- Brain perfusion depends on cardiac output, vascular tone, blood pressure, and autonomic reflexes.
- The brainstem reticular activating system is essential for maintaining wakefulness.
- Autonomic imbalance can produce hypotension or bradycardia leading to syncope.
- Syncope must be differentiated from seizure, coma, and brain death.
- It is a clinical presentation, not a final diagnosis.
🔬 CONCEPT EXPLAINED
To understand syncope, the first concept is that consciousness requires continuous blood flow to the brain. The brain has high metabolic demand and limited energy reserve, so even a short interruption in cerebral perfusion can temporarily switch off awareness. Syncope occurs when global cerebral blood flow falls suddenly, most commonly because of reduced blood pressure, reduced cardiac output, or inappropriate autonomic reflex activity.
Normally, when a person stands, gravity causes blood to pool in the lower limbs. This reduces venous return to the heart. As venous return falls, cardiac output may decrease. The body protects cerebral perfusion through the baroreceptor reflex. Baroreceptors in the carotid sinus and aortic arch detect the fall in arterial pressure and stimulate sympathetic outflow while reducing parasympathetic vagal activity. As a result, heart rate increases, cardiac contractility increases, and arterioles constrict. These responses maintain blood pressure and protect brain blood flow.
Syncope develops when this protective system fails or is overwhelmed. For example, excessive vagal discharge may slow the heart markedly, while withdrawal of sympathetic tone may cause vasodilation. Both changes reduce blood pressure. As a result, cerebral perfusion falls, the reticular activating system is under-supplied, and consciousness is briefly lost. Once the person falls to the ground, venous return improves because the brain and heart are at the same level. Cerebral perfusion is restored, and consciousness returns.
This mechanism exists as a protective circulatory adjustment. The body continuously uses autonomic reflexes to keep the brain perfused despite posture changes, emotion, pain, dehydration, or blood loss. When autonomic control is abnormal, syncope becomes a warning sign of circulatory or neural instability.
⚠️ CLINICAL IMPORTANCE
Syncope is important because it may be benign, such as vasovagal syncope, or dangerous, such as syncope due to cardiac arrhythmia. In MBBS clinical reasoning, the key point is that syncope is brief and reversible. It differs from coma because coma is prolonged unconsciousness. It differs from brain death because brain death is irreversible and includes loss of brainstem reflexes and spontaneous breathing.
MAJOR CONCEPTUAL HEADING 2
Sympathetic Nervous System and Drugs Acting on Sympathetic Pathways
🧠 CORE
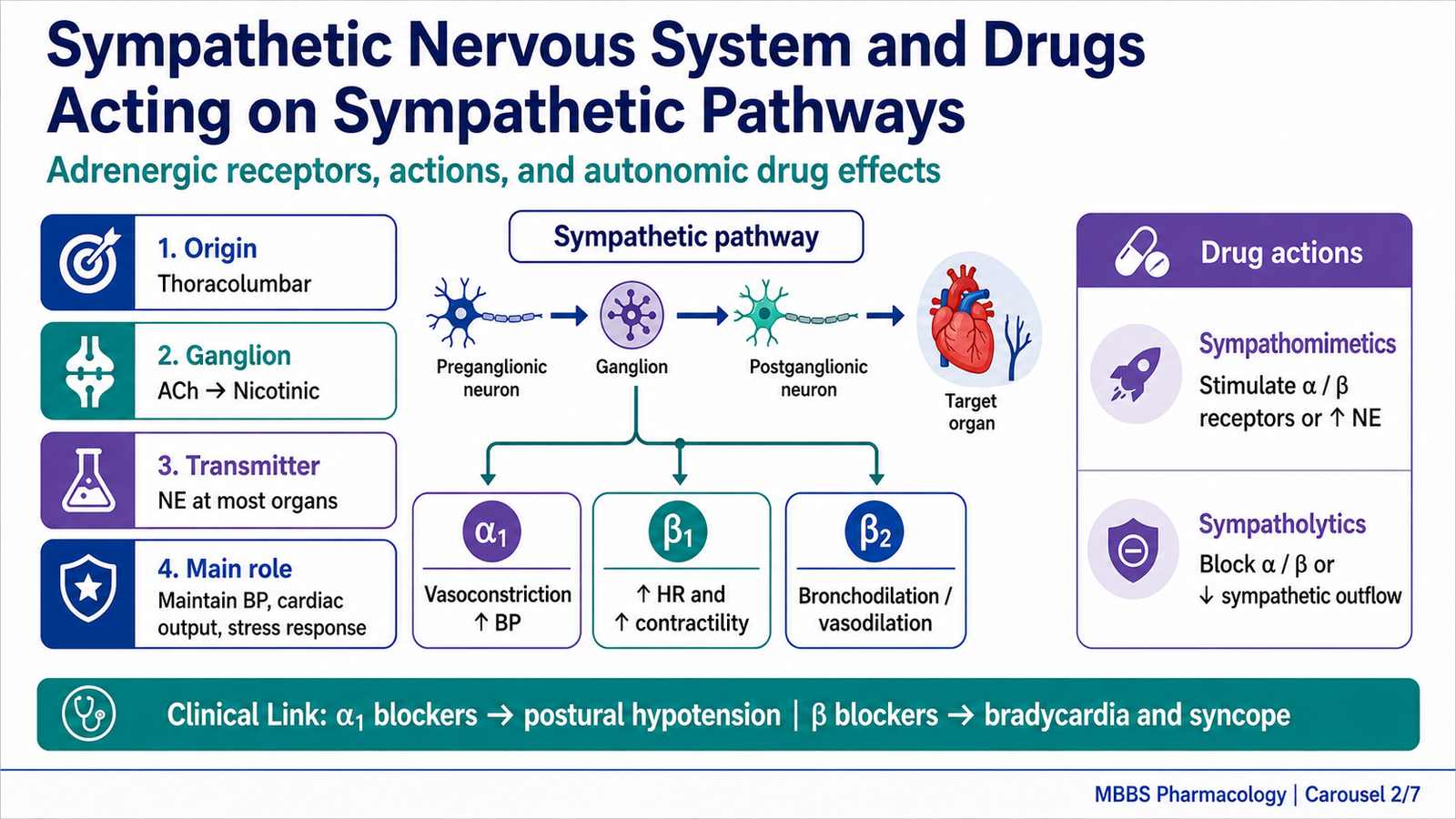
- The sympathetic nervous system maintains vascular tone, blood pressure, cardiac output, and stress responses.
- Preganglionic sympathetic neurons release acetylcholine at nicotinic receptors.
- Most postganglionic sympathetic neurons release norepinephrine.
- Sympathetic effects are mediated mainly through alpha and beta adrenergic receptors.
- Sympathomimetic drugs increase sympathetic activity.
- Sympatholytic drugs reduce sympathetic activity.
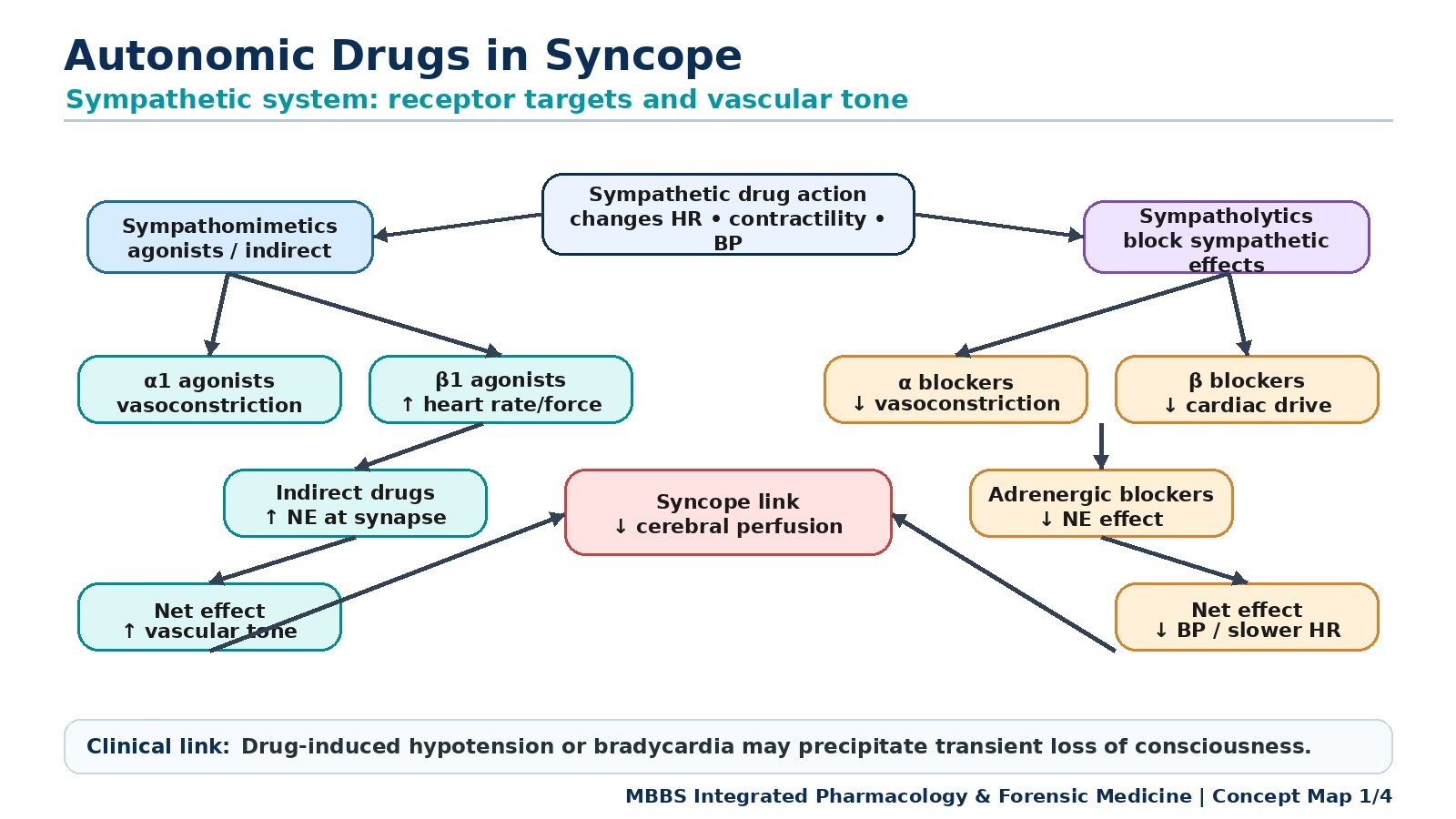
- These drugs can strongly influence syncope by altering heart rate, vascular tone, and blood pressure.
🔬 CONCEPT EXPLAINED
The sympathetic nervous system is the major autonomic system that protects blood pressure during stress, standing, exercise, pain, fear, and blood loss. It exists because the body must rapidly redistribute blood flow and maintain perfusion of vital organs, especially the brain and heart. Sympathetic activation increases heart rate, increases myocardial contractility, constricts many blood vessels, dilates bronchi, and mobilizes energy stores.
The pathway begins in the thoracolumbar spinal cord. Preganglionic neurons release acetylcholine onto nicotinic receptors in sympathetic ganglia. Postganglionic neurons usually release norepinephrine at target organs. The adrenal medulla acts like a modified sympathetic ganglion and releases adrenaline and norepinephrine into blood.
Drugs acting on the sympathetic nervous system are divided into drugs that mimic sympathetic activity and drugs that block sympathetic activity. Sympathomimetic drugs produce effects similar to norepinephrine or adrenaline. They may act directly on adrenergic receptors, indirectly by increasing norepinephrine release, or by preventing norepinephrine reuptake or metabolism. Sympatholytic drugs reduce sympathetic effects by blocking receptors, reducing neurotransmitter release, or decreasing sympathetic outflow from the central nervous system.
This becomes clinically important in syncope because vascular tone and cardiac output are major determinants of cerebral perfusion. A drug that causes vasodilation, excessive bradycardia, or reduced cardiac contractility can precipitate syncope. In contrast, a drug that increases vascular tone may help restore blood pressure in selected hypotensive states.
Mechanism of Action of Sympathomimetic Drugs
Sympathomimetic drugs work by increasing adrenergic signaling. Direct-acting sympathomimetics bind to alpha or beta receptors and activate them. For example, alpha-1 receptor stimulation causes vascular smooth muscle contraction, increasing peripheral resistance and blood pressure. Beta-1 receptor stimulation increases heart rate and contractility, increasing cardiac output. Beta-2 receptor stimulation relaxes bronchial smooth muscle and also dilates some vascular beds.
Indirect-acting sympathomimetics increase norepinephrine availability at synapses. They may promote norepinephrine release from nerve terminals, inhibit reuptake, or reduce metabolism. The final effect is increased adrenergic stimulation without necessarily binding directly to the receptor.
Mixed-acting drugs have both direct receptor stimulation and indirect norepinephrine-enhancing effects. Their final physiological outcome depends on which receptors are activated and in which tissue.
Major Receptor-Based Effects
Alpha-1 receptors are mainly present on vascular smooth muscle. When stimulated, they cause vasoconstriction. This increases peripheral resistance and helps maintain blood pressure. Excessive alpha-1 activation may cause hypertension, while alpha-1 blockade may cause postural hypotension and syncope.
Alpha-2 receptors are commonly presynaptic inhibitory receptors. When activated, they reduce norepinephrine release. Centrally acting alpha-2 agonists reduce sympathetic outflow and lower blood pressure. If blood pressure falls too much, dizziness or syncope may occur.
Beta-1 receptors are mainly found in the heart and juxtaglomerular cells of the kidney. Beta-1 stimulation increases heart rate, force of contraction, conduction velocity, and renin release. Excessive beta-1 stimulation may cause tachycardia and palpitations. Beta blockers reduce these effects and may cause bradycardia or hypotension in susceptible patients.
Beta-2 receptors are found in bronchial smooth muscle, some vascular smooth muscle, and uterine smooth muscle. Beta-2 stimulation causes bronchodilation and vasodilation in skeletal muscle vascular beds. This is useful in bronchial asthma but may produce tremor, tachycardia, or mild fall in peripheral resistance.
Mechanism of Action of Sympatholytic Drugs
Sympatholytic drugs reduce sympathetic effects. Alpha blockers prevent norepinephrine or adrenaline from activating alpha receptors. Alpha-1 blockers relax vascular smooth muscle, reducing peripheral resistance. This can lower blood pressure but may cause postural hypotension because standing requires alpha-1-mediated vasoconstriction.
Beta blockers block beta receptors. Beta-1 blockade reduces heart rate, contractility, conduction, and renin release. This decreases cardiac workload and blood pressure. However, excessive beta blockade may reduce cardiac output and produce dizziness or syncope, especially in patients with conduction defects or low baseline blood pressure.
Centrally acting sympatholytics reduce sympathetic outflow from the brainstem. They lower blood pressure by reducing peripheral vascular resistance and heart rate. Their adverse effects may include sedation, dry mouth, and hypotension.
Adrenergic neuron blockers interfere with norepinephrine storage or release. These are less commonly emphasized at undergraduate level but are important conceptually because they show that sympathetic activity can be reduced at the nerve terminal, not only at the receptor.
⚠️ CLINICAL IMPORTANCE
Sympathetic drugs are clinically important because they directly alter blood pressure and cerebral perfusion. Alpha-1 agonists increase vascular tone and may support blood pressure. Alpha-1 blockers may cause postural hypotension and syncope. Beta blockers reduce heart rate and myocardial oxygen demand but can cause bradycardia and fainting if excessive. In syncope evaluation, drug history is essential because autonomic drugs can convert a compensated circulatory state into cerebral hypoperfusion.
MAJOR CONCEPTUAL HEADING 3
Parasympathetic Nervous System and Drugs Acting on Parasympathetic Pathways
🧠 CORE
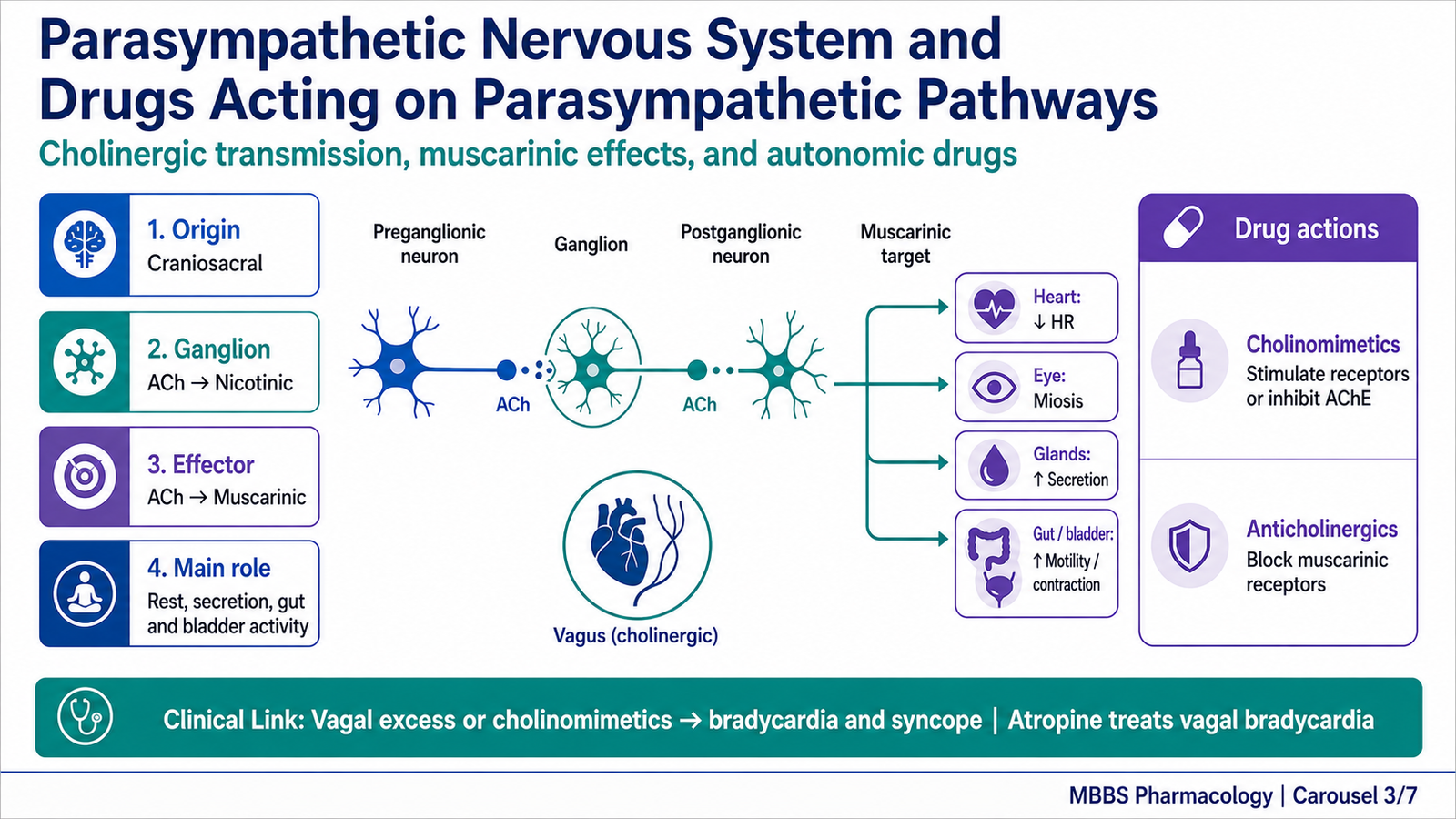
- The parasympathetic nervous system is mainly craniosacral in origin.
- It supports rest, digestion, secretion, urination, pupillary constriction, and heart rate slowing.
- Preganglionic and postganglionic parasympathetic neurons release acetylcholine.
- Acetylcholine acts on nicotinic receptors in ganglia and muscarinic receptors on effector organs.
- Cholinomimetic drugs increase parasympathetic activity.
- Anticholinergic drugs block muscarinic effects.
- Excessive parasympathetic activity can cause bradycardia, hypotension, and syncope.
🔬 CONCEPT EXPLAINED
The parasympathetic nervous system exists to conserve energy and support internal maintenance functions. It slows the heart, promotes gastrointestinal movement and secretion, contracts the bladder, constricts the pupil, and increases glandular secretion. Its major cranial component travels through cranial nerves, especially the vagus nerve, while its sacral component supplies pelvic organs.
Unlike the sympathetic system, parasympathetic ganglia are usually near or within the target organs. This allows more localized and specific control. The preganglionic neuron releases acetylcholine at nicotinic receptors in the ganglion. The postganglionic neuron also releases acetylcholine, which acts mainly on muscarinic receptors at the effector organ.
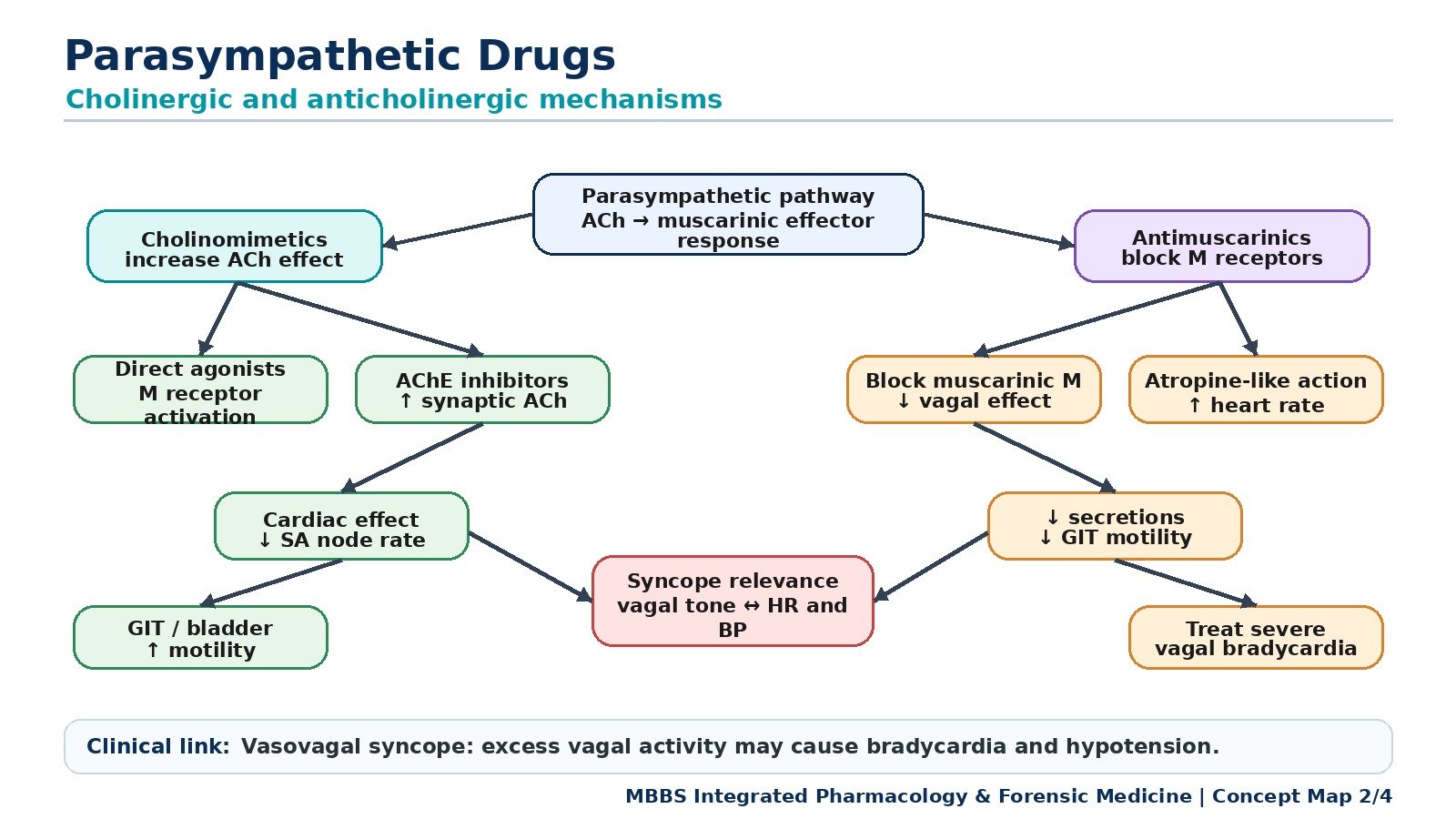
Parasympathetic drugs are important because acetylcholine has strong effects on heart rate, smooth muscle, glands, eye, and urinary bladder. Cholinomimetic drugs increase acetylcholine-like activity either by directly stimulating muscarinic receptors or by inhibiting acetylcholinesterase, the enzyme that breaks down acetylcholine. Anticholinergic drugs block muscarinic receptors and therefore reduce parasympathetic effects.
Mechanism of Action of Cholinomimetic Drugs
Cholinomimetic drugs increase cholinergic signaling. Direct-acting cholinomimetics bind to muscarinic receptors and stimulate them. This causes effects similar to parasympathetic activation: reduced heart rate, increased glandular secretion, bronchoconstriction, increased gastrointestinal motility, bladder contraction, and pupillary constriction.
Indirect-acting cholinomimetics inhibit acetylcholinesterase. Normally, acetylcholinesterase rapidly breaks down acetylcholine in synaptic clefts. When this enzyme is inhibited, acetylcholine accumulates and produces prolonged stimulation at muscarinic and nicotinic receptors. The physiological effect depends on the tissue involved. In the heart, increased muscarinic activity slows the SA node and AV node. In the gut, it increases motility. At the neuromuscular junction, it can improve transmission in conditions such as myasthenia gravis, although detailed disease management belongs to later pharmacology and medicine.
If cholinergic activity becomes excessive, muscarinic effects may become dangerous. Severe bradycardia reduces cardiac output. Increased secretions, bronchoconstriction, abdominal cramps, diarrhea, and sweating may occur. If cardiac output falls enough, cerebral perfusion decreases and syncope may result.
Mechanism of Action of Anticholinergic Drugs
Anticholinergic drugs block muscarinic receptors. By preventing acetylcholine from acting on these receptors, they reduce parasympathetic effects. In the heart, muscarinic blockade reduces vagal slowing, so heart rate may increase. In the eye, blockade causes pupillary dilation and reduced accommodation. In glands, secretion decreases, producing dry mouth. In the gut and bladder, smooth muscle activity is reduced.
Atropine is the classical muscarinic blocker. Its core concept is that it removes parasympathetic restraint. Therefore, when vagal activity is causing excessive bradycardia, atropine can increase heart rate by blocking muscarinic receptors in the heart. However, anticholinergic effects can also produce adverse effects such as urinary retention, constipation, blurred vision, dry mouth, and confusion, especially in susceptible individuals.
Parasympathetic Control of Heart Rate and Syncope
The vagus nerve provides parasympathetic input to the heart. Vagal stimulation releases acetylcholine onto muscarinic M2 receptors in the SA node and AV node. This reduces heart rate and slows conduction. This mechanism is useful because the body needs to slow the heart during rest and maintain efficient cardiac function. However, excessive vagal discharge can cause marked bradycardia or transient pauses in cardiac rhythm. As a result, cardiac output falls, cerebral perfusion decreases, and syncope may occur.
This is one mechanism behind vasovagal syncope. Emotional stress, pain, prolonged standing, dehydration, or fear may trigger reflex autonomic changes. Sympathetic tone may fall while parasympathetic tone rises. The combined effect is vasodilation plus bradycardia, leading to transient cerebral hypoperfusion.
⚠️ CLINICAL IMPORTANCE
Parasympathetic drugs are clinically important because they influence heart rate, pupil, secretions, airways, gut, and urinary bladder. Cholinomimetic excess can produce bradycardia and syncope. Anticholinergic drugs can treat excessive vagal bradycardia but may cause urinary retention, dry mouth, constipation, and blurred vision. In syncope, the parasympathetic system is especially important because vagal overactivity is a common mechanism of reflex fainting.
MAJOR CONCEPTUAL HEADING 4
Autonomic Regulation of Vascular Tone and Blood Pressure in Syncope
🧠 CORE
- Blood pressure depends on cardiac output and peripheral vascular resistance.
- Sympathetic tone maintains arteriolar and venous constriction.
- Parasympathetic control of blood vessels is limited but strongly affects heart rate.
- Baroreceptor reflex protects cerebral perfusion during posture change.
- Failure of autonomic compensation causes orthostatic hypotension.
- Autonomic drugs can either restore or impair blood pressure control.
- Cerebral hypoperfusion is the final common pathway of syncope.
🔬 CONCEPT EXPLAINED
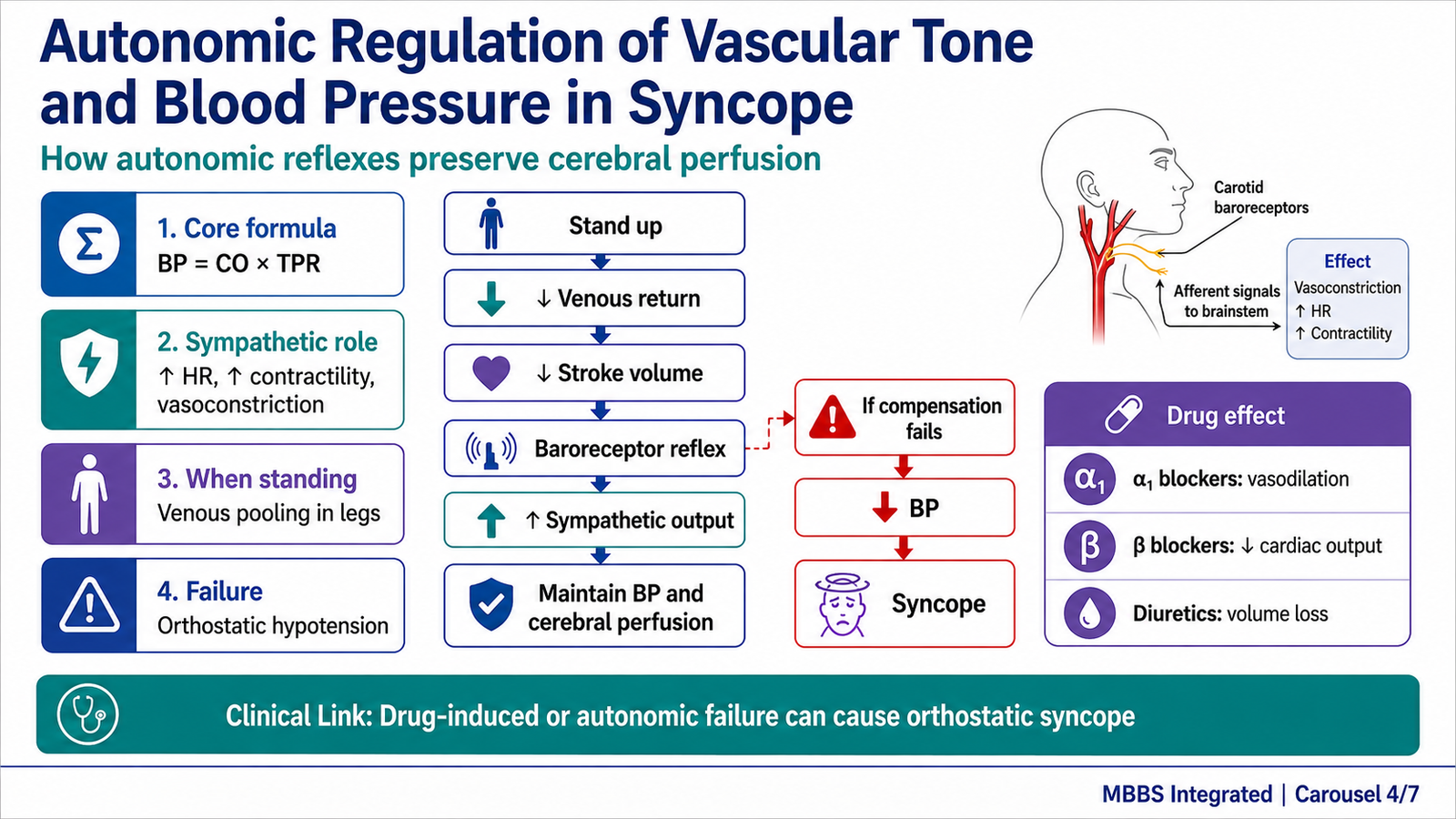
The next step is to connect autonomic pharmacology with syncope. Blood pressure is determined mainly by cardiac output and total peripheral resistance. Cardiac output depends on heart rate, myocardial contractility, and venous return. Peripheral resistance depends largely on arteriolar tone. Sympathetic activity supports both components by increasing heart rate, increasing contractility, constricting veins, and constricting arterioles.
When a person stands, venous pooling reduces venous return. If venous return falls, stroke volume decreases. The baroreceptor reflex detects this fall and increases sympathetic output. Arteriolar constriction raises peripheral resistance, venoconstriction improves venous return, and beta-1 stimulation increases cardiac output. These adjustments maintain arterial pressure and cerebral perfusion.
If this reflex fails, orthostatic hypotension occurs. The patient may feel dizziness, blurring of vision, weakness, or may faint. Drugs can contribute to this by blocking alpha-1 receptors, reducing heart rate, reducing contractility, causing diuresis, or impairing autonomic reflexes. Therefore, autonomic pharmacology is not separate from syncope; it is central to understanding why fainting occurs in many patients.
Drug Effects on Vascular Tone
Alpha-1 agonists increase vascular smooth muscle contraction. This increases peripheral resistance and blood pressure. Alpha-1 blockers prevent this vasoconstriction. While useful in some conditions, they may impair the standing response and produce postural hypotension.
Beta-1 agonists increase cardiac output by increasing heart rate and contractility. Beta blockers reduce cardiac output and renin release. They are useful in many cardiovascular conditions, but excessive beta blockade can reduce blood pressure or cause bradycardia.
Muscarinic agonists can slow the heart through vagal-like action. Muscarinic blockers can increase heart rate by removing vagal influence. Thus, both sympathetic and parasympathetic drugs can alter the same final pathway: cerebral perfusion.
⚠️ CLINICAL IMPORTANCE
The most important clinical concept is that syncope occurs when compensatory mechanisms fail to maintain blood pressure and cerebral blood flow. Drug-induced syncope is especially important in patients taking antihypertensives, alpha blockers, beta blockers, diuretics, or drugs that increase vagal tone. In exams, orthostatic hypotension and vasovagal syncope are common examples linking autonomic control with transient loss of consciousness.
MAJOR CONCEPTUAL HEADING 5
Brainstem Arousal Systems, Coma and Brain Death
🧠 CORE
- Wakefulness depends on the brainstem reticular activating system and cerebral cortex.
- Syncope temporarily suppresses consciousness due to reduced cerebral perfusion.
- Coma is prolonged unconsciousness due to brain dysfunction.
- Brain death is irreversible loss of all brain functions including brainstem function.
- Brainstem reflexes are essential in brain death assessment.
- Spontaneous respiration depends on brainstem respiratory centers.
- Loss of brainstem function is central to medicolegal certification of brain death.
🔬 CONCEPT EXPLAINED
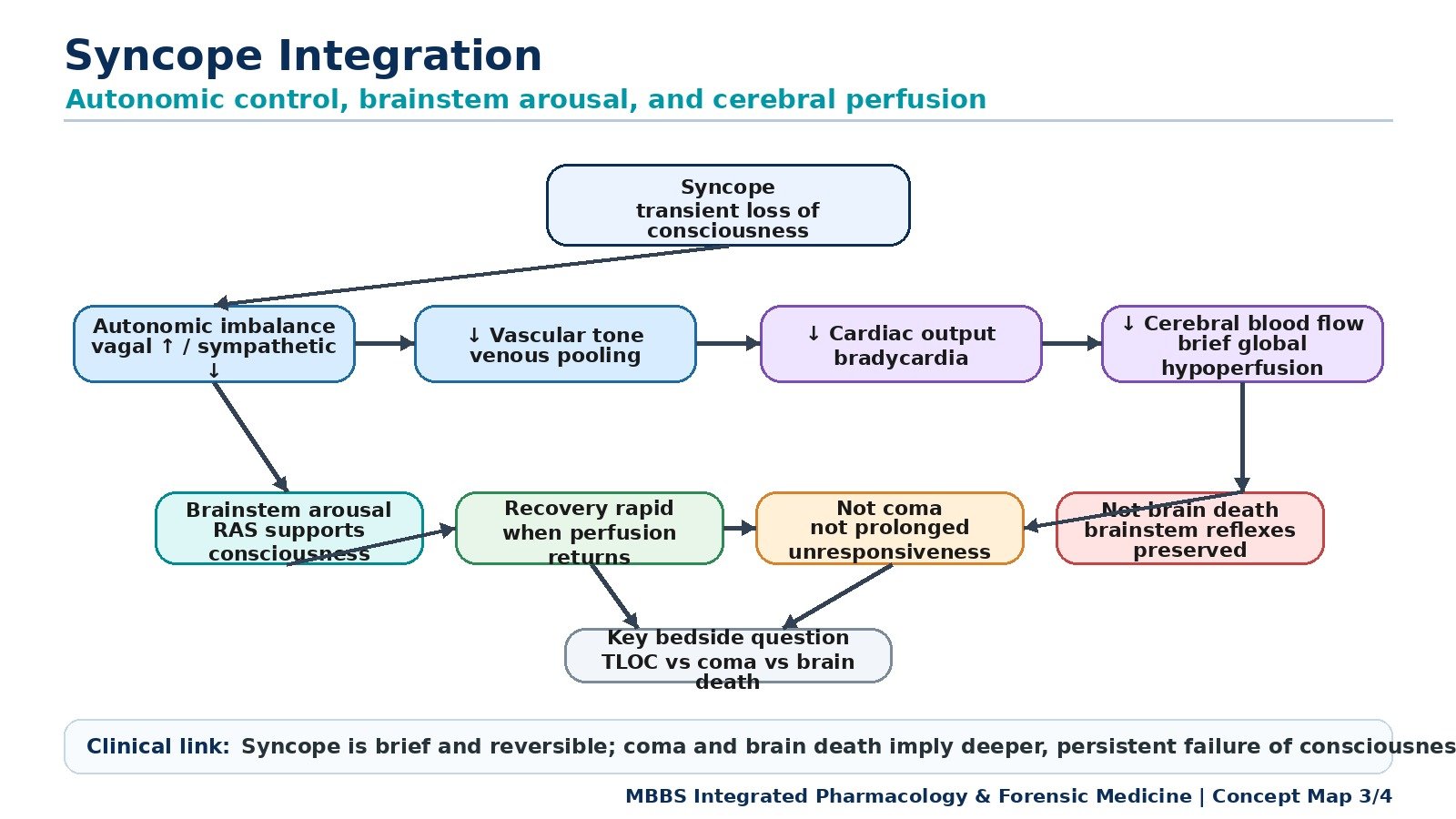
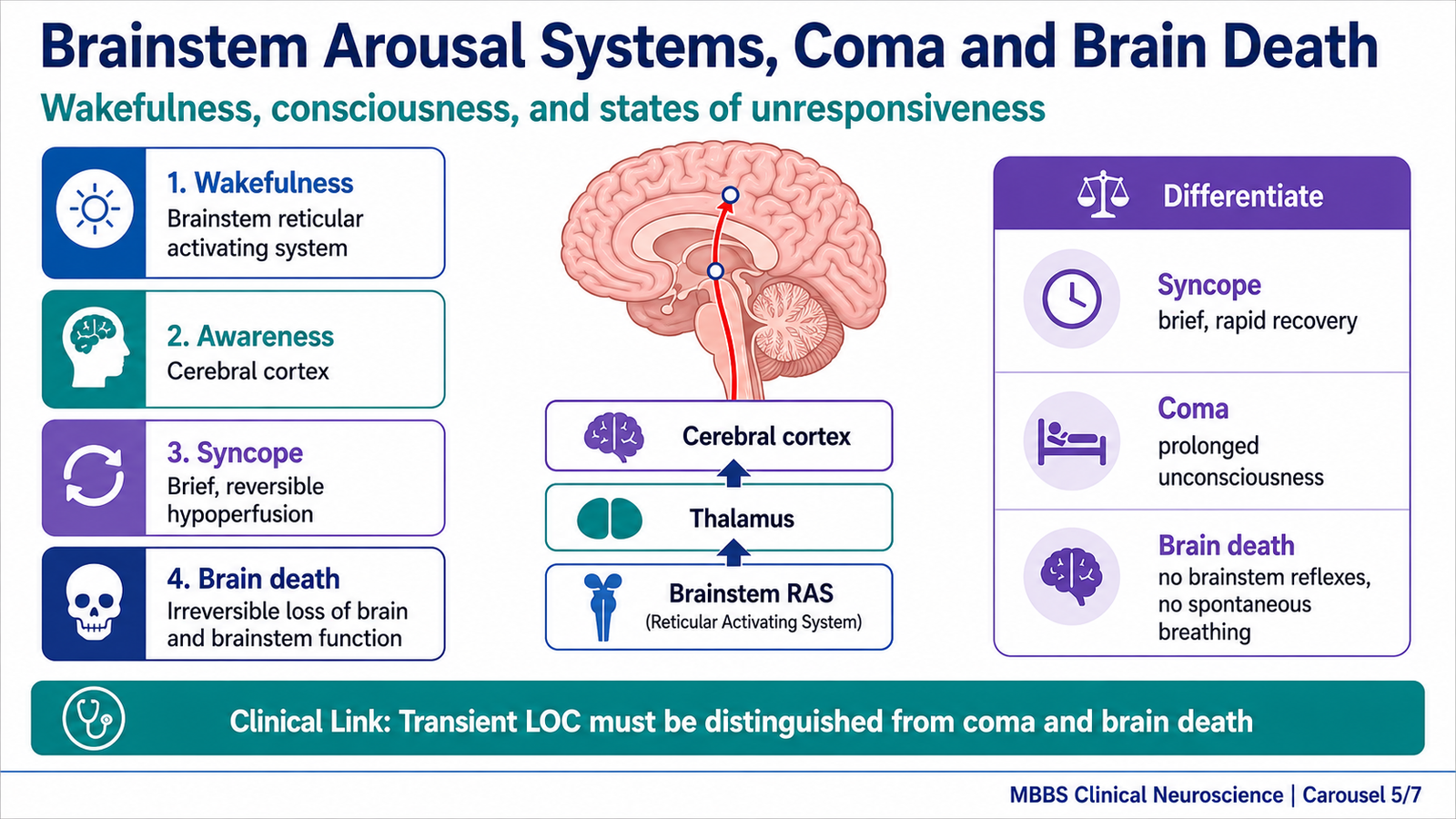
To differentiate syncope from coma and brain death, students must understand the brainstem arousal system. Consciousness has two major components: wakefulness and awareness. Wakefulness depends heavily on the ascending reticular activating system located in the brainstem reticular formation, which projects upward to the thalamus and cerebral cortex. Awareness depends mainly on cortical function.
In syncope, the brainstem and cortex are not structurally dead. They are temporarily under-perfused. When blood flow is restored, neuronal function returns and consciousness comes back. Therefore, syncope is short-lived and reversible.
Coma is different. In coma, the patient remains unconscious for a prolonged period and cannot be awakened. Coma may result from widespread cerebral dysfunction, brainstem dysfunction, metabolic causes, toxins, trauma, or raised intracranial pressure. Some brainstem reflexes may still be present depending on the cause and severity. The patient is alive, although critically ill.
Brain death is the most severe and irreversible state. It means permanent loss of all functions of the entire brain, including the brainstem. Since the brainstem controls essential reflexes and spontaneous breathing, brain death is diagnosed by showing unresponsive coma, absence of brainstem reflexes, and absence of spontaneous respiration after excluding reversible causes.
This distinction exists because clinical unconsciousness can occur at different levels of severity. A fainted patient may wake up quickly. A comatose patient is alive but deeply unconscious. A brain-dead patient has irreversible loss of brain and brainstem function and is legally considered dead in many medicolegal systems.
Differentiation of Transient Loss of Consciousness, Coma and Brain Death
Transient loss of consciousness includes syncope and some seizure-related events. In syncope, loss of consciousness is brief, posture-related or trigger-related, and recovery is spontaneous. Brainstem reflexes are preserved after recovery.
Coma is prolonged unconsciousness. The patient does not wake spontaneously within seconds or a few minutes. Brainstem reflexes may be present or impaired depending on the lesion. Spontaneous breathing may be present.
Brain death is irreversible. The patient has no consciousness, no brainstem reflexes, and no spontaneous breathing. It is not simply “deep coma”; it is death confirmed by strict clinical criteria.
⚠️ CLINICAL IMPORTANCE
The distinction between syncope, coma, and brain death is crucial. Mistaking syncope for coma may cause unnecessary panic. Mistaking coma for brain death is a serious medicolegal error. Brain death certification must be performed carefully because it has legal consequences for death declaration, withdrawal of artificial support according to law and policy, and organ donation procedures where applicable.
MAJOR CONCEPTUAL HEADING 6
Certification of Brain Death
🧠 CORE
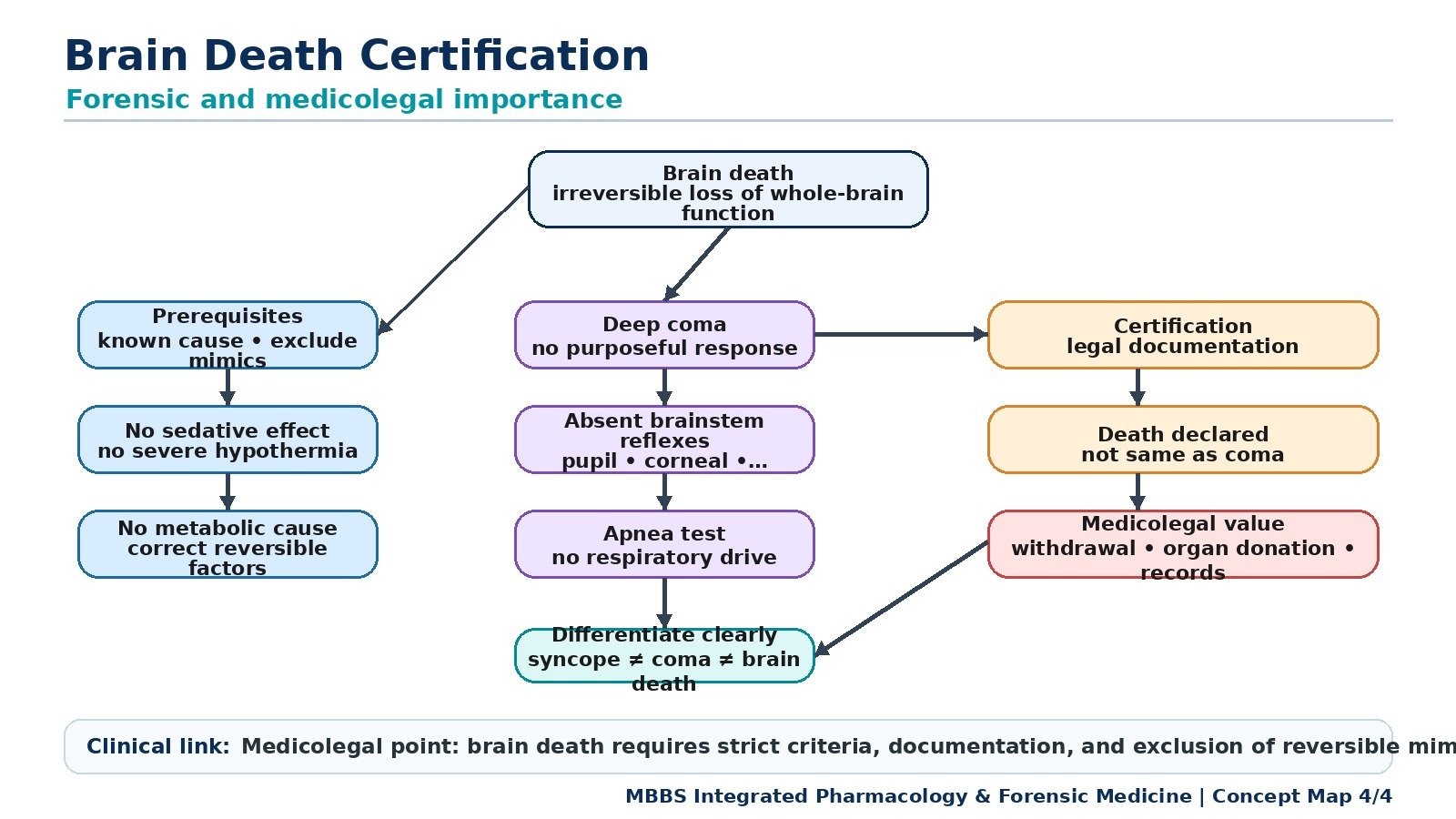
- Brain death certification confirms irreversible loss of brain and brainstem function.
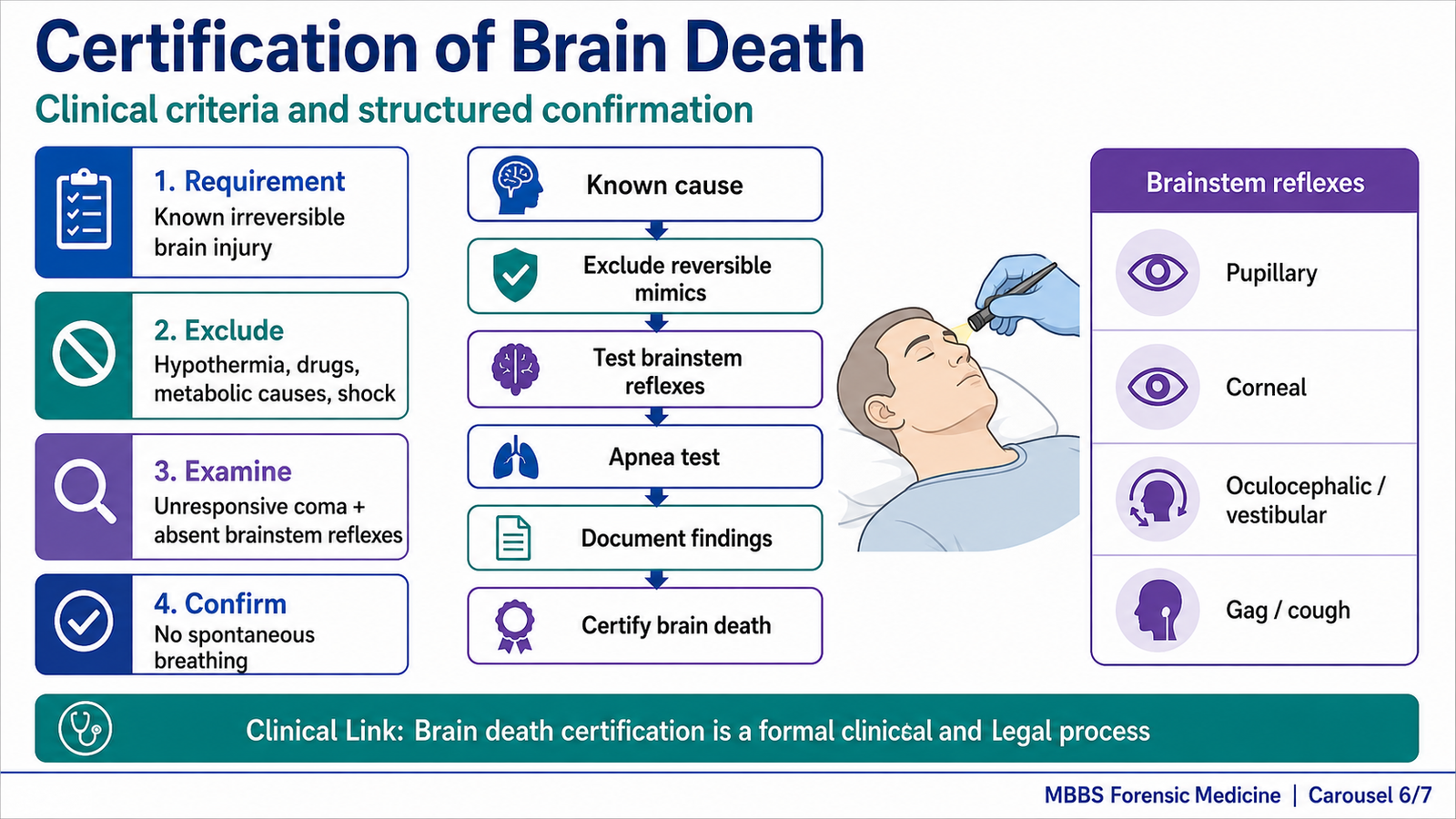
- It requires a known cause of irreversible brain injury.
- Reversible causes of coma must be excluded.
- Clinical examination demonstrates unresponsiveness and absent brainstem reflexes.
- Apnea testing assesses absence of spontaneous respiration.
- Documentation must be accurate, complete, and legally valid.
- Certification has major medicolegal importance.
🔬 CONCEPT EXPLAINED
Brain death certification is a structured medical process. It exists because modern intensive care can maintain heartbeat and circulation artificially even when the brain has permanently stopped functioning. Without clear criteria, there may be confusion between a ventilated dead patient and a deeply comatose but living patient. Certification provides medical certainty and legal clarity.
The first requirement is that the cause of brain injury must be known and sufficient to explain irreversible loss of brain function. Examples include severe traumatic brain injury, massive intracranial hemorrhage, prolonged cerebral hypoxia, or extensive brain swelling. At undergraduate level, the key concept is not detailed neurosurgical diagnosis but the principle that the cause must be established and irreversible.
Before testing brainstem function, reversible causes must be excluded. These include hypothermia, sedative or anesthetic drug effects, neuromuscular blockade, severe metabolic or endocrine disturbances, shock, and intoxication. This is important because these conditions can mimic brain death but may be reversible. A patient must not be certified brain dead if a reversible cause of absent responses is still possible.
The clinical examination assesses deep unresponsive coma and absence of brainstem reflexes. Brainstem reflexes commonly assessed include pupillary light reflex, corneal reflex, oculocephalic reflex where appropriate, oculovestibular response, gag reflex, cough reflex, and motor response to cranial nerve stimulation. The absence of these reflexes indicates failure of brainstem pathways.
The apnea test assesses whether the patient can breathe spontaneously when carbon dioxide rises. Normally, increased arterial carbon dioxide stimulates brainstem respiratory centers and triggers breathing. If carbon dioxide rises adequately and no respiratory effort occurs, this supports loss of brainstem respiratory drive. The test must be performed under controlled conditions by trained clinicians according to institutional and legal protocols.
Certification must be documented carefully. The record should include patient identity, cause of coma, exclusion of confounders, examination findings, apnea test result where performed, names and designations of certifying doctors, date and time of testing, and time of death according to local law or hospital policy.
⚠️ CLINICAL IMPORTANCE
Brain death certification is not a casual bedside opinion. It is a formal medical and legal declaration. Errors can create serious ethical, legal, and social consequences. Proper certification protects the patient, family, doctor, hospital, and legal process. It also provides clarity in organ donation pathways where legally and ethically applicable.
MAJOR CONCEPTUAL HEADING 7
Medicolegal Importance of Brain Death
🧠 CORE
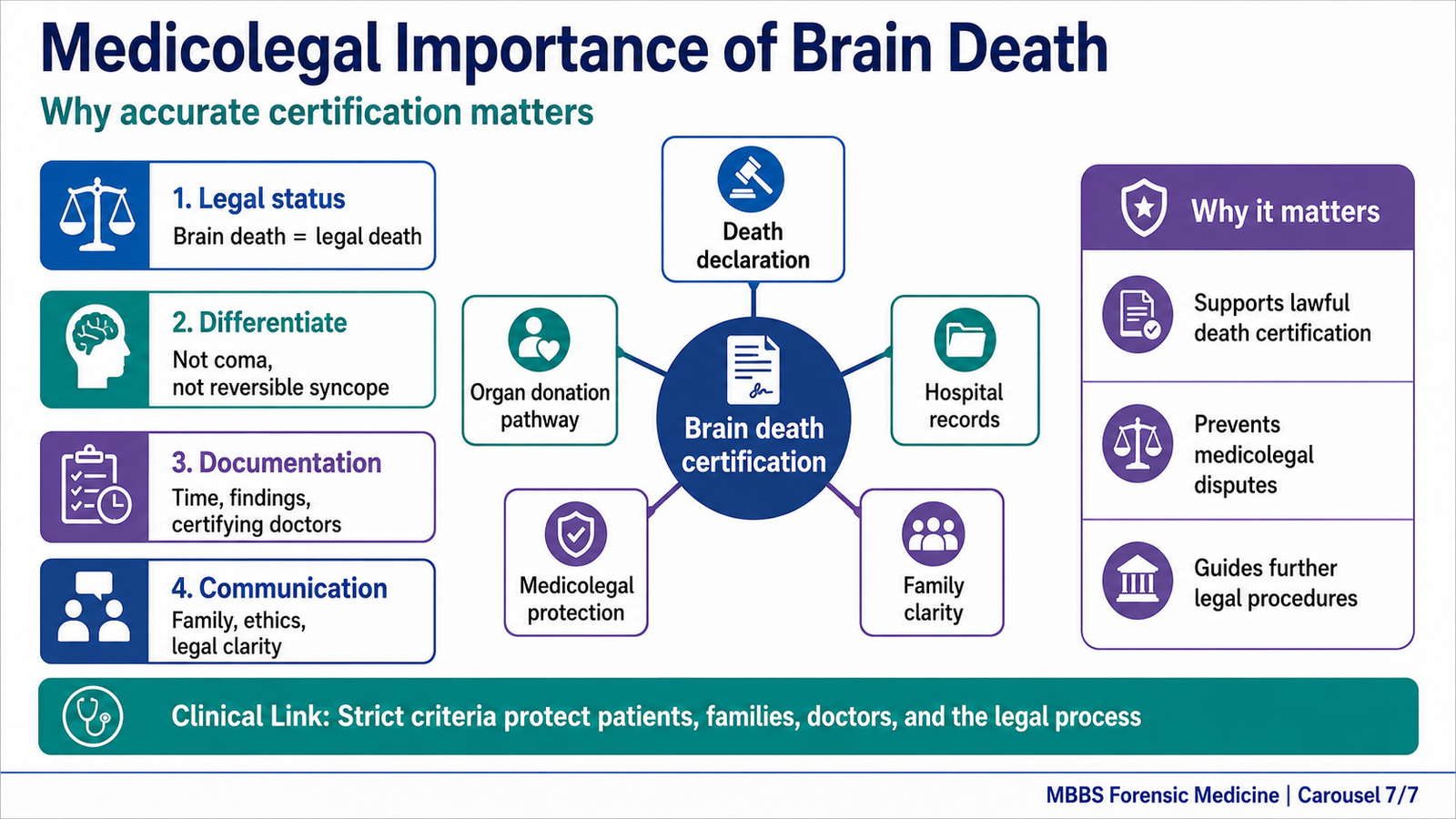
- Brain death has legal importance because it establishes death despite artificial ventilation.
- It helps distinguish death from coma or vegetative states.
- It guides documentation of time and cause of death.
- It is important for organ donation procedures where applicable.
- It protects doctors from legal disputes when properly certified.
- It requires strict adherence to recognized criteria and local law.
- It carries ethical, religious, and family communication significance.
🔬 CONCEPT EXPLAINED
The medicolegal importance of brain death arises from a modern clinical reality: machines can maintain oxygenation and circulation even after the brain has irreversibly ceased functioning. The heart may continue beating temporarily with ventilatory and circulatory support, but the person is legally dead if accepted criteria for brain death are fulfilled.
This matters because death certification affects legal identity, inheritance, insurance, criminal investigations, hospital documentation, burial processes, and organ donation. If brain death is not properly understood, families may believe that a patient is alive because the chest moves with the ventilator and the monitor shows a heartbeat. Therefore, doctors must explain that the movement is machine-generated and that the brain, including the brainstem, has irreversibly stopped functioning.
Brain death also has forensic relevance in trauma and suspected criminal cases. The cause and timing of death may become legally significant. Clear documentation is essential so that medical findings can be defended if questioned by legal authorities. In cases involving organ donation, medicolegal accuracy is especially important because organs may be retrieved only after lawful death determination and appropriate consent procedures.
The ethical principle behind brain death certification is that death must be determined by objective, reproducible, and accepted medical criteria. The doctor’s role is not only scientific but also legal and communicative. A poorly documented certification can create suspicion, conflict, or legal challenge, even if the clinical diagnosis was correct.
⚠️ CLINICAL IMPORTANCE
For MBBS students, the major exam point is that brain death is irreversible loss of brain and brainstem function and is medicolegally significant because it permits legal declaration of death under accepted criteria. It must be distinguished from coma, persistent unconsciousness, drug-induced unresponsiveness, hypothermia, and metabolic suppression.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Autonomic Nervous System
Structure: Sympathetic thoracolumbar outflow, parasympathetic craniosacral outflow, autonomic ganglia, adrenergic and cholinergic receptors.
Function: Regulates heart rate, vascular tone, blood pressure, visceral smooth muscle, glands, pupil, and bronchi.
Outcome: Maintains internal stability and protects cerebral perfusion during posture change, stress, and physiological demand.
Blood Vessels and Heart
Structure: Arteriolar smooth muscle contains adrenergic receptors; SA node and AV node receive autonomic input.
Function: Arterioles regulate peripheral resistance; heart regulates cardiac output.
Outcome: Blood pressure is maintained so that the brain receives continuous blood flow.
Brainstem Reticular Activating System
Structure: Reticular formation in the brainstem with ascending projections to thalamus and cortex.
Function: Maintains wakefulness and supports consciousness.
Outcome: Adequate perfusion maintains awareness; reduced perfusion causes syncope.
Brainstem Reflex Pathways
Structure: Cranial nerve nuclei and brainstem reflex arcs.
Function: Mediate pupillary, corneal, vestibulo-ocular, gag, cough, and respiratory responses.
Outcome: Presence of reflexes indicates functioning brainstem pathways; absence in the correct clinical context supports brain death.
Pharmacological Integration
Structure: Receptors on heart, vessels, glands, smooth muscle, and autonomic synapses.
Function: Drugs modify receptor activation or neurotransmitter availability.
Outcome: Autonomic drugs can restore blood pressure, reduce excessive heart workload, treat bronchospasm or bradycardia, but may also cause hypotension, bradycardia, tachycardia, or syncope.
Medicolegal Integration
Structure: Brain and brainstem are examined clinically through neurological reflexes and respiratory drive.
Function: Certification determines whether irreversible loss of brain function has occurred.
Outcome: Accurate brain death certification establishes legal death and prevents confusion with coma or reversible unconsciousness.
🩺 5️⃣ Clinical Correlation
Vasovagal Syncope
Vasovagal syncope occurs due to reflex autonomic imbalance. A trigger such as pain, fear, prolonged standing, or emotional stress causes withdrawal of sympathetic tone and increased vagal activity. Vasodilation lowers peripheral resistance, while bradycardia reduces cardiac output. The combined effect is reduced cerebral perfusion and brief loss of consciousness. Recovery usually occurs after lying down.
Orthostatic Hypotension
Orthostatic hypotension occurs when blood pressure falls significantly on standing. Normally, the baroreceptor reflex increases sympathetic tone to maintain blood pressure. If this reflex is impaired or blocked by drugs, venous pooling reduces venous return and cardiac output. Cerebral perfusion falls, causing dizziness or syncope. This is commonly linked with autonomic failure, dehydration, antihypertensive drugs, alpha blockers, or excessive diuresis.
Drug-Induced Syncope
Autonomic drugs may produce syncope by disturbing blood pressure or heart rate. Alpha blockers may cause vasodilation and postural hypotension. Beta blockers may cause bradycardia or reduced cardiac output. Cholinomimetic drugs may increase vagal effects and slow the heart. Centrally acting sympatholytics may reduce sympathetic tone. Therefore, drug history is an essential part of syncope assessment.
Bradycardia-Related Syncope
Excessive parasympathetic activity or drugs that slow cardiac conduction can reduce heart rate. If heart rate becomes too low, cardiac output falls. Since cerebral perfusion depends on cardiac output, the patient may develop transient loss of consciousness. This explains why severe vagal discharge or excessive beta blockade can produce fainting.
Coma
Coma is prolonged unconsciousness due to severe dysfunction of the cerebral hemispheres, brainstem, or metabolic environment. Unlike syncope, coma does not resolve rapidly just by lying down. Brainstem reflexes may still be present depending on the cause. It is not equivalent to brain death.
Brain Death
Brain death is irreversible loss of all brain function including brainstem function. The patient has no consciousness, no brainstem reflexes, and no spontaneous respiration when properly tested. It is medically and legally distinct from coma. Certification must follow accepted criteria and requires exclusion of reversible mimics.
Medicolegal Certification Error
Incorrect certification of brain death can produce serious legal and ethical consequences. If reversible causes such as sedative drugs, hypothermia, or metabolic disturbances are not excluded, a living patient may be wrongly labeled brain dead. Conversely, failure to certify true brain death may create confusion, unnecessary continuation of support, family distress, and legal uncertainty.
📌 6️⃣ Summary Points
- Syncope is brief, reversible loss of consciousness due to transient global cerebral hypoperfusion.
- The final common pathway in syncope is reduced blood flow to the brain, especially affecting the reticular activating system and cortex.
- Sympathetic activity maintains blood pressure by increasing heart rate, contractility, venous return, and arteriolar tone.
- Parasympathetic vagal activity slows the heart; excessive vagal discharge can cause bradycardia and syncope.
- Alpha-1 stimulation causes vasoconstriction, while alpha-1 blockade may cause postural hypotension.
- Beta-1 stimulation increases heart rate and contractility, while beta blockade may cause bradycardia and reduced cardiac output.
- Cholinomimetic drugs increase acetylcholine effects; excessive muscarinic cardiac action may produce bradycardia.
- Anticholinergic drugs block muscarinic receptors and reduce parasympathetic effects such as vagal slowing, secretions, gut motility, and bladder contraction.
- Syncope is reversible, coma is prolonged unconsciousness, and brain death is irreversible loss of all brain and brainstem function.
- Brain death certification requires known irreversible cause, exclusion of reversible mimics, absence of brainstem reflexes, and absence of spontaneous respiration according to accepted protocol.
- Brain death has major medicolegal importance because it establishes legal death despite artificial ventilation and possible persistent heartbeat.
- Drug history is essential in syncope because autonomic drugs can alter vascular tone, heart rate, cardiac output, and cerebral perfusion.