
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
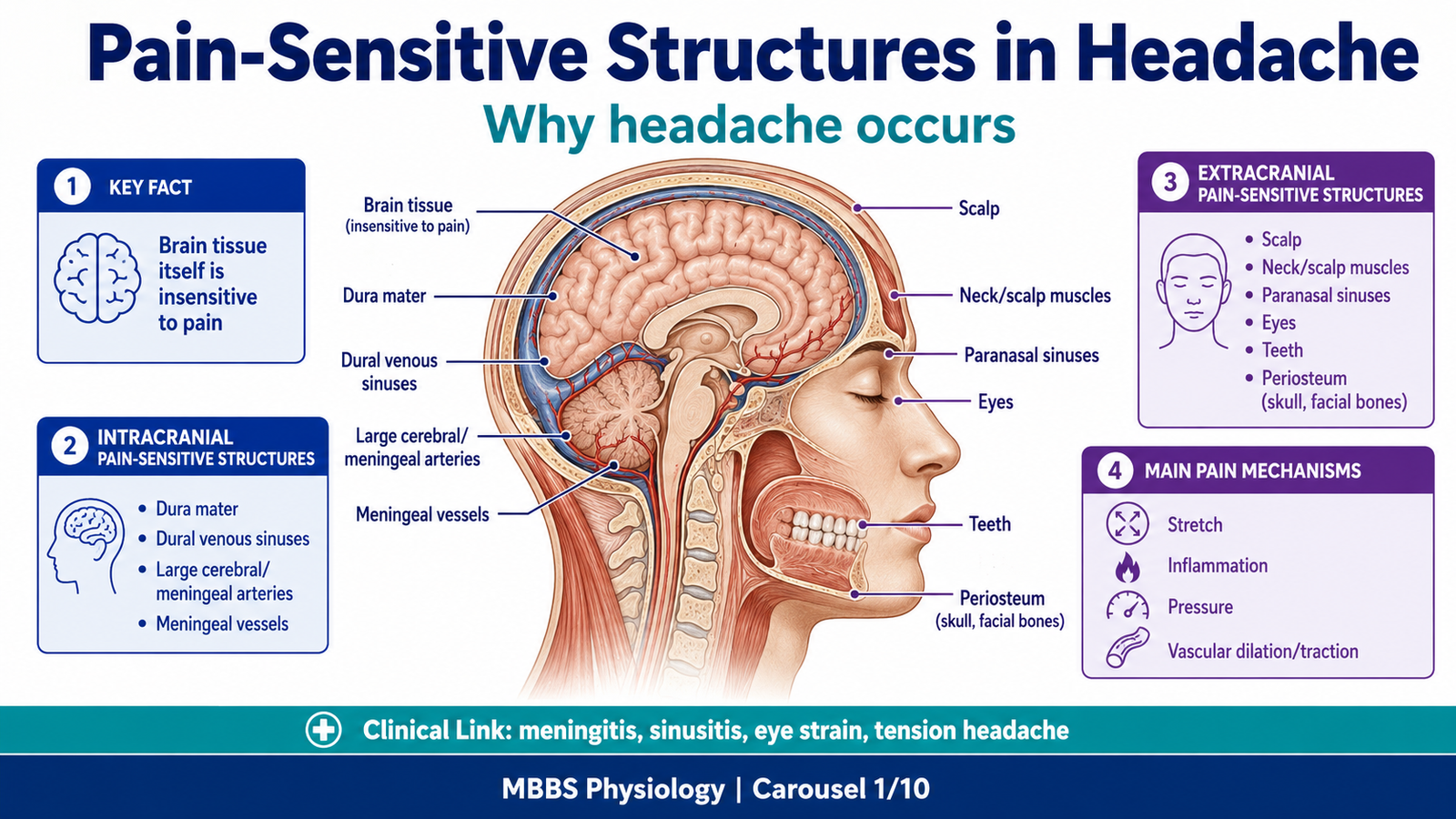
Headache is one of the most common clinical symptoms and is closely related to the physiology of pain pathways. Although the brain tissue itself is insensitive to pain, many structures around the brain, such as meninges, dural venous sinuses, cerebral blood vessels, scalp, muscles, eyes, nose, and teeth, are pain-sensitive. To understand headache, students must first understand pain receptors, pain transmission pathways, referred pain, thermal sensation, and natural analgesic systems of the body. This topic integrates anatomy of dural venous sinuses with physiology of pain and thermal pathways, and biochemistry of prostaglandins. Clinically, this helps explain why meningitis, migraine, sinusitis, dental disease, and muscle tension can all present as headache.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Pain: An unpleasant sensory and emotional experience associated with actual or potential tissue damage.
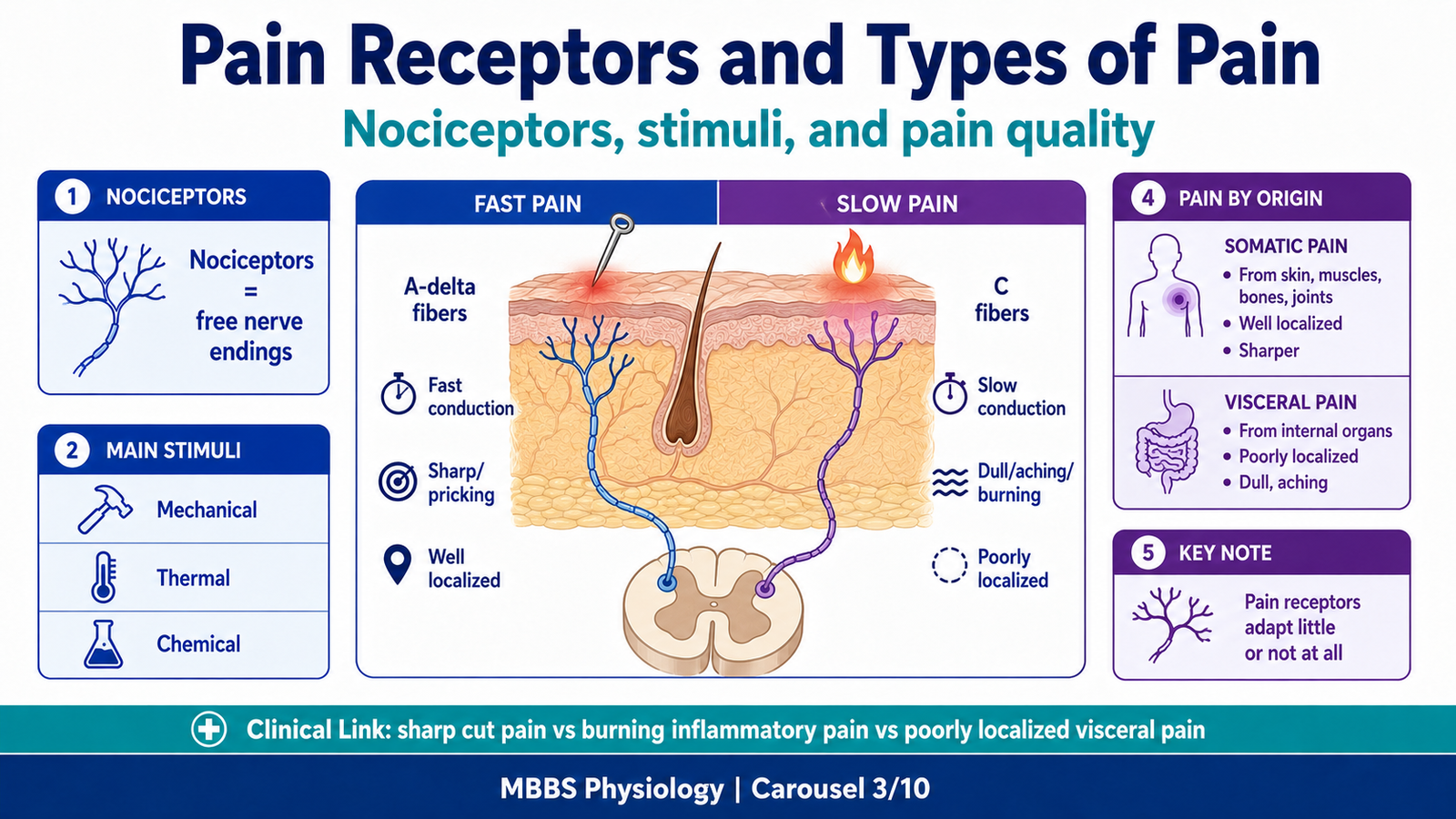
- Nociceptors: Free nerve endings that detect painful stimuli.
- Fast pain: Sharp, localized pain transmitted mainly by A-delta fibers.
- Slow pain: Dull, aching, burning pain transmitted mainly by C fibers.
- Analgesia: Suppression or reduction of pain sensation without loss of consciousness.
- Hyperalgesia: Increased sensitivity to painful stimuli.
- Primary hyperalgesia: Increased pain sensitivity at the site of tissue injury.
- Secondary hyperalgesia: Increased pain sensitivity in surrounding uninjured tissues.
- Referred pain: Pain felt at a site different from the actual source of injury.
- Prostaglandins: Lipid-derived inflammatory mediators that sensitize pain receptors.
- Thermal receptors: Sensory receptors that detect cold and warm temperatures.
Essential Terminology
- Dura mater: Tough outer meningeal covering of the brain.
- Dural venous sinuses: Endothelial-lined venous channels between layers of cranial dura mater.
- Spinothalamic tract: Major ascending pathway for pain, temperature, and crude touch.
- Substantia gelatinosa: Area in dorsal horn involved in modulation of pain.
- Periaqueductal gray: Midbrain region involved in descending pain suppression.
- Endorphins and enkephalins: Endogenous opioid peptides that suppress pain.
Basic Overview
- Pain begins when nociceptors are stimulated by mechanical, thermal, or chemical injury.
- Pain impulses enter the spinal cord through dorsal roots and ascend mainly through the anterolateral system.
- The brain interprets pain according to site, intensity, quality, and emotional meaning.
- The body also has pain-suppressing systems that reduce pain transmission.
- Headache occurs when pain-sensitive intracranial or extracranial structures are stimulated.
- Prostaglandins do not directly cause all pain but strongly increase pain sensitivity during inflammation.
🔹 3️⃣ Core Learning — Curriculum Coverage
1 — Pain-Sensitive Structures in Headache
🧠 CORE
- Brain parenchyma itself is insensitive to pain.
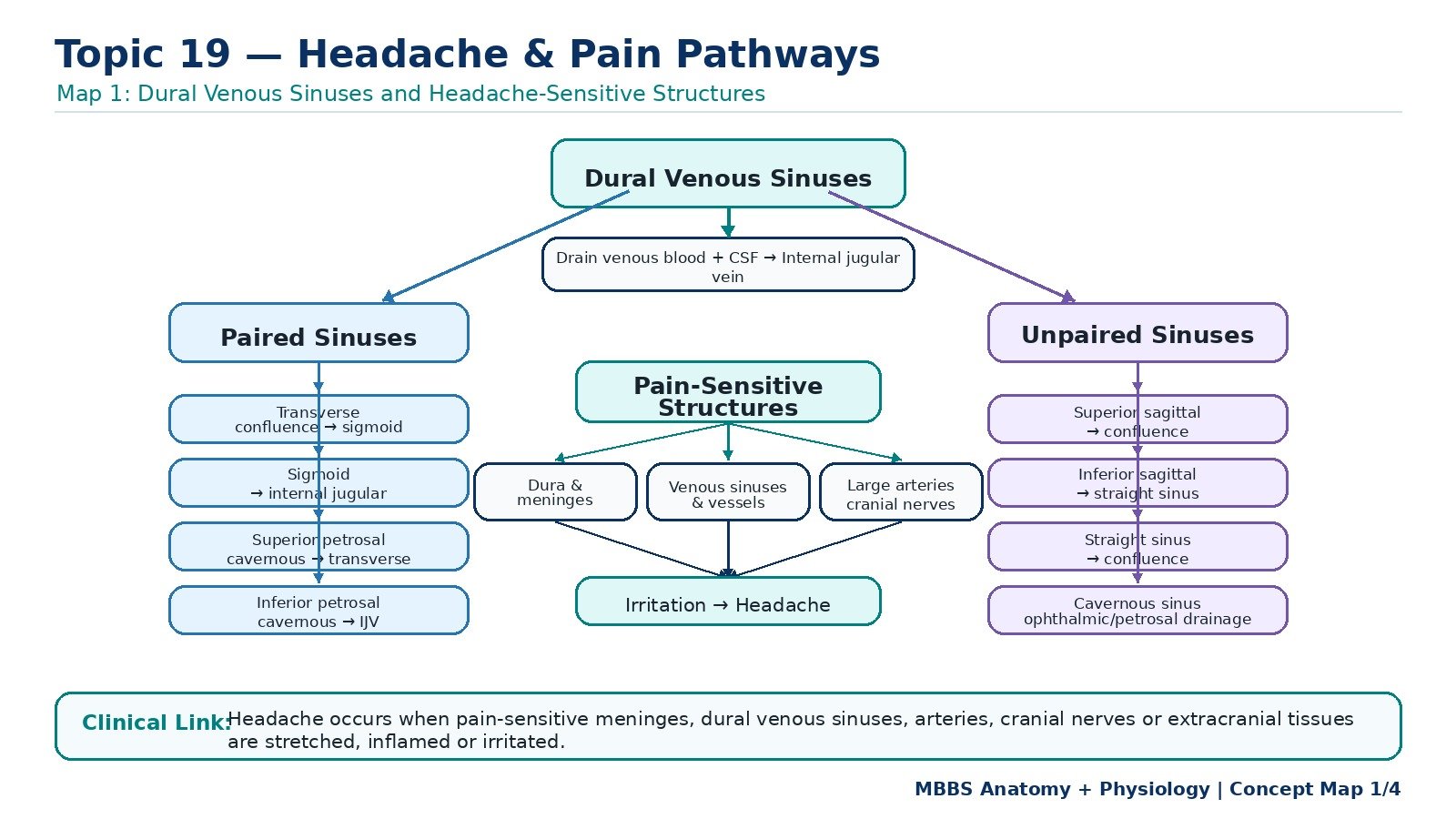
- Pain-sensitive intracranial structures include dura mater, dural venous sinuses, large cerebral arteries, and meningeal vessels.
- Pain-sensitive extracranial structures include scalp, muscles, periosteum, eyes, nose, teeth, sinuses, and cervical tissues.
- Headache results when these structures are stretched, inflamed, compressed, or irritated.
- Intracranial and extracranial pain may be referred to different areas of the head.
- Understanding headache requires linking anatomy with pain pathways.
- Different types of headache reflect different underlying pain mechanisms.
🔬 CONCEPT EXPLAINED
To understand headache, the most important principle is that the brain substance itself does not feel pain. Cutting or stimulating brain tissue does not usually produce pain because neurons of the brain parenchyma lack pain receptors. However, the structures surrounding and supporting the brain are richly supplied with pain-sensitive nerve endings.
The dura mater, dural venous sinuses, and large intracranial blood vessels are particularly important in headache. When these structures are stretched, inflamed, displaced, or compressed, nociceptors are activated. For example, stretching of meningeal vessels may contribute to vascular headache, while inflammation of meninges causes severe headache in meningitis.
Extracranial structures are also common sources of headache. These include the scalp, facial muscles, cervical muscles, nasal sinuses, teeth, eyes, and periosteum of the skull. This is why sinusitis, eye strain, dental infection, and muscle tension can all produce headache.
Therefore, headache is not simply “pain in the brain.” It is usually pain arising from pain-sensitive cranial and extracranial structures, transmitted through cranial nerves and upper cervical nerves, and interpreted by the brain as pain in the head.
⚠️ CLINICAL IMPORTANCE
Headache becomes clinically important because its location and character may suggest the structure involved. Meningeal irritation produces severe generalized headache with neck stiffness. Sinus inflammation causes facial or frontal headache. Eye strain may cause orbital or frontal headache. Tension in scalp and neck muscles commonly produces dull bilateral headache.
2 — Dural Venous Sinuses: Anatomy and Drainage
🧠 CORE
- Dural venous sinuses are venous channels located between layers of dura mater.
- They drain venous blood from the brain, meninges, skull, and orbit.
- They also receive cerebrospinal fluid through arachnoid granulations.
- Sinuses are classified as paired and unpaired.
- They ultimately drain mainly into the internal jugular veins.
- Dural venous sinuses are clinically important because thrombosis, infection, or raised pressure can produce headache.
- Their walls are rigid because they are formed by dura mater and do not collapse easily.
🔬 CONCEPT EXPLAINED
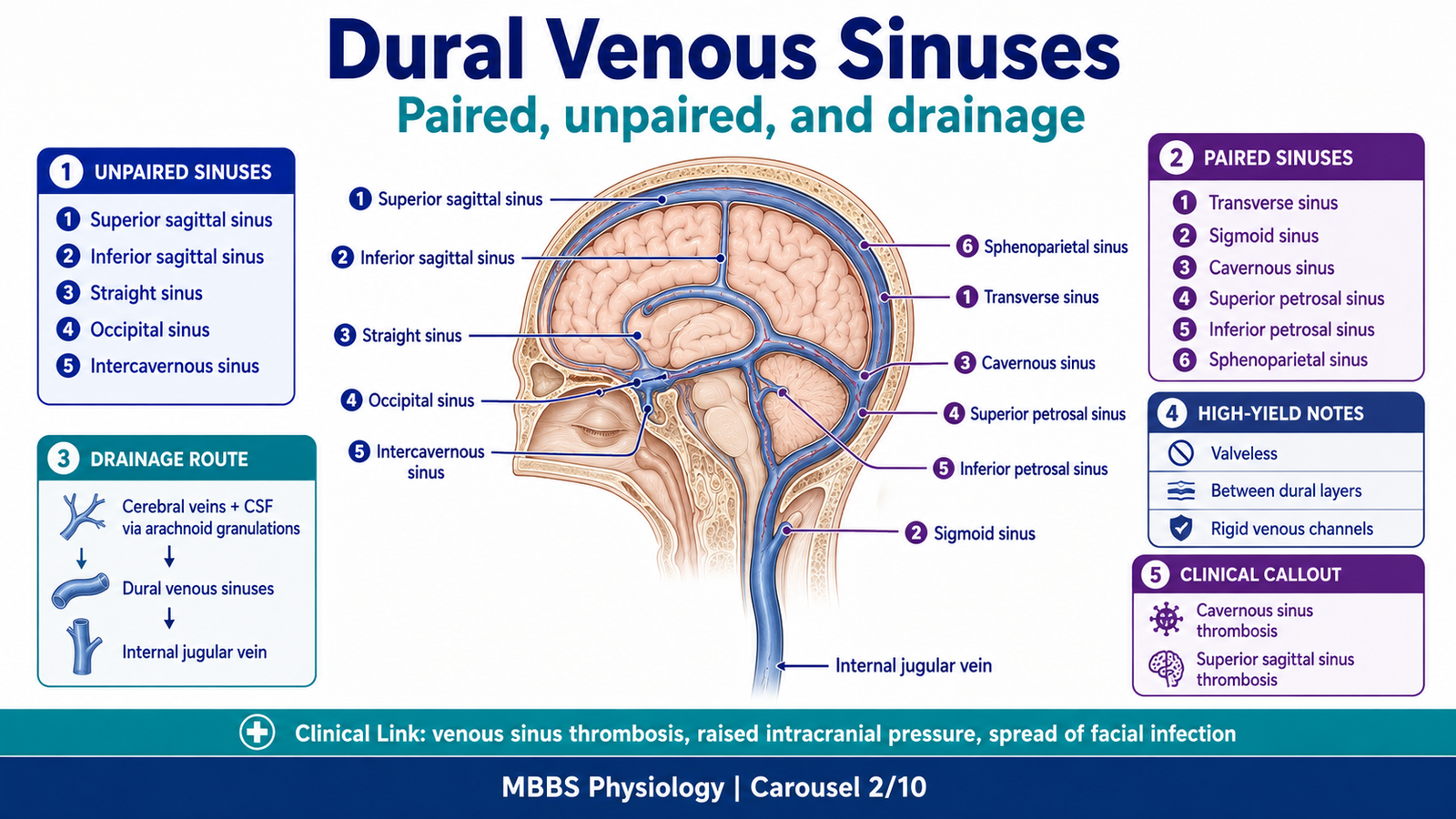
The cranial dura mater has two layers: an outer periosteal layer and an inner meningeal layer. At certain places, these layers separate and form endothelial-lined venous channels called dural venous sinuses. Unlike ordinary veins, these sinuses do not have valves and their walls are supported by tough dura, so they remain open even when venous pressure changes.
The dural venous sinuses drain blood from cerebral veins and also receive cerebrospinal fluid through arachnoid granulations, especially into the superior sagittal sinus. This means they are important not only for venous drainage but also for maintaining CSF circulation and intracranial pressure.
Because the dura and sinuses are pain-sensitive, distension, thrombosis, infection, or inflammation of these sinuses can cause headache. Their connections with facial and scalp veins also explain how infection from the face, nose, or scalp may spread intracranially.
Unpaired Dural Venous Sinuses
Superior sagittal sinus lies in the upper attached margin of falx cerebri. It begins near the crista galli and runs backward to the confluence of sinuses. It receives superior cerebral veins, diploic veins, emissary veins, and CSF through arachnoid granulations. It usually drains into the right transverse sinus.
Inferior sagittal sinus lies in the lower free margin of falx cerebri. It runs backward and joins the great cerebral vein to form the straight sinus.
Straight sinus lies at the junction of falx cerebri and tentorium cerebelli. It receives the inferior sagittal sinus and great cerebral vein, and drains into the confluence of sinuses, often toward the left transverse sinus.
Occipital sinus lies in the attached margin of falx cerebelli. It communicates with the confluence of sinuses and venous plexuses around the foramen magnum.
Intercavernous sinuses connect the two cavernous sinuses around the pituitary gland. They form venous channels anterior and posterior to the hypophysis.
Paired Dural Venous Sinuses
Transverse sinuses begin at the confluence of sinuses and run laterally in the attached margin of tentorium cerebelli. Each continues as a sigmoid sinus.
Sigmoid sinuses are S-shaped sinuses that continue from transverse sinuses and pass through the jugular foramina to become the internal jugular veins.
Cavernous sinuses lie on either side of the body of sphenoid bone. They receive ophthalmic veins and superficial middle cerebral veins and drain into superior and inferior petrosal sinuses. They are clinically important because the internal carotid artery and cranial nerves III, IV, V1, V2, and VI are related to them.
Superior petrosal sinuses lie along the upper border of petrous temporal bone. They drain cavernous sinus into transverse or sigmoid sinus.
Inferior petrosal sinuses lie in the groove between petrous temporal bone and occipital bone. They drain cavernous sinus directly into the internal jugular vein.
Sphenoparietal sinuses run along the lesser wing of sphenoid and drain into the cavernous sinus.
⚠️ CLINICAL IMPORTANCE
Cavernous sinus thrombosis is an important exam concept. Infection from the danger area of the face can spread through valveless facial and ophthalmic veins to the cavernous sinus. This may produce severe headache, fever, eye swelling, ophthalmoplegia, and cranial nerve involvement. Superior sagittal sinus thrombosis may cause headache, raised intracranial pressure, seizures, or neurological deficits.
3 — Pain Receptors and Stimuli Causing Pain
🧠 CORE
- Pain receptors are called nociceptors.
- They are free nerve endings found in skin, muscles, joints, periosteum, blood vessels, meninges, and viscera.
- They respond to mechanical, thermal, and chemical stimuli.
- Pain receptors do not adapt easily; persistent injury continues to produce pain.
- Tissue damage releases chemicals that stimulate or sensitize nociceptors.
- Pain protects the body by forcing withdrawal, rest, and avoidance of further injury.
- Excessive pain may become harmful and disabling.
🔬 CONCEPT EXPLAINED
Pain begins at nociceptors, which are free nerve endings specialized for detecting tissue injury. These receptors are widely distributed in the body, especially in the skin and protective tissues. They are also present in deep structures such as muscles, joints, periosteum, blood vessel walls, and meninges.
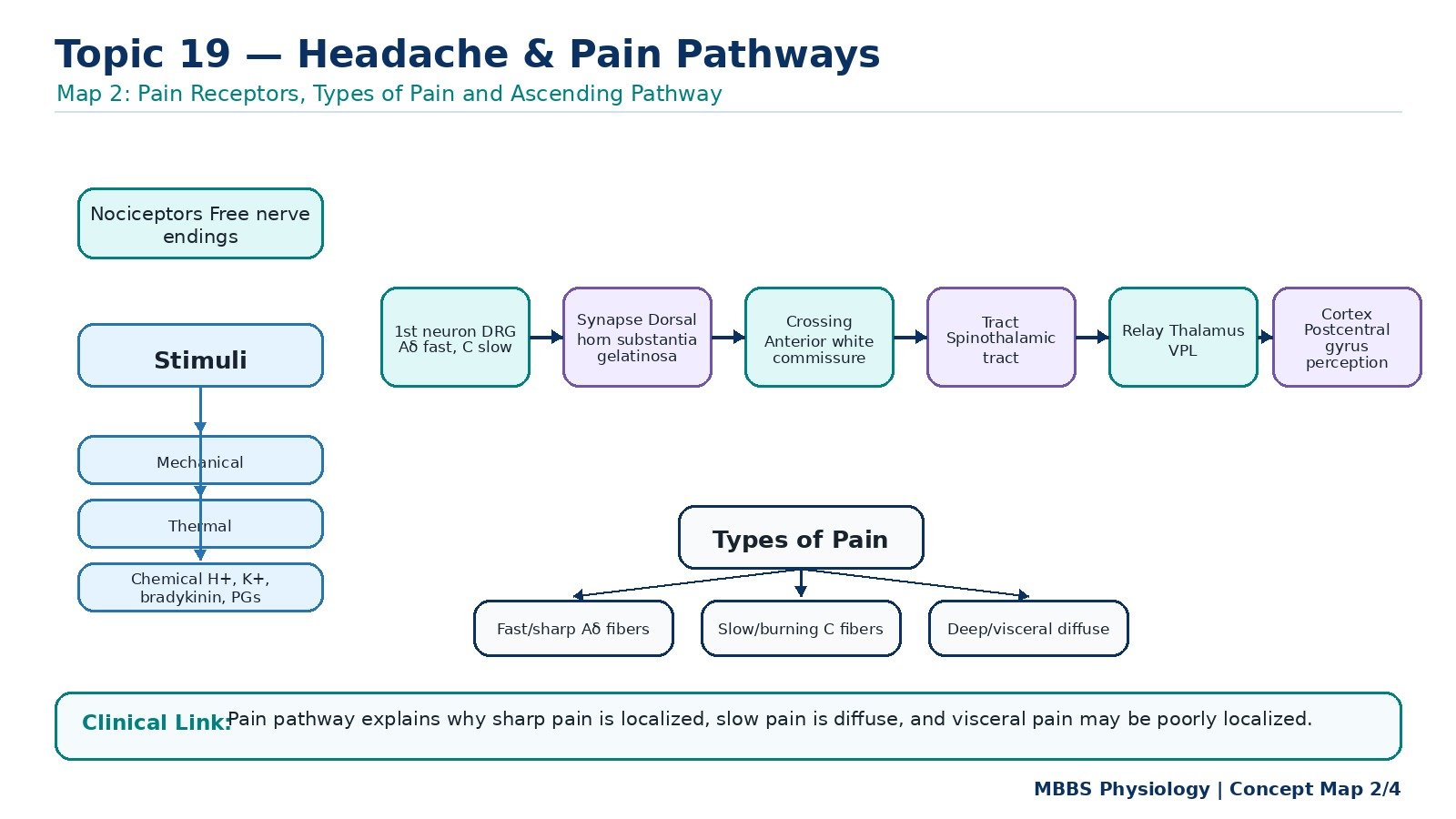
Pain receptors are stimulated by three major types of stimuli. Mechanical stimuli include cutting, crushing, pressure, stretching, or tearing of tissues. Thermal stimuli include extreme heat or cold that can damage tissue. Chemical stimuli include substances released from damaged or inflamed tissues, such as bradykinin, prostaglandins, histamine, potassium ions, acids, and substance P.
A key feature of pain receptors is that they adapt very little or not at all. This is biologically useful because pain should continue as long as tissue damage continues. For example, if a tissue remains inflamed or compressed, continued pain warns the person to protect that area.
Pain therefore exists as a protective mechanism. It alerts the body to injury, produces withdrawal reflexes, limits movement, and encourages healing. However, if pain becomes excessive or chronic, it may lose its protective value and become a disease problem itself.
⚠️ CLINICAL IMPORTANCE
Inflammation increases pain because inflammatory mediators sensitize nociceptors. This is why an inflamed area becomes tender and painful even with mild touch or movement. Analgesic drugs such as NSAIDs reduce pain partly by decreasing prostaglandin formation.
4 — Types of Pain
🧠 CORE
- Pain may be classified as fast pain and slow pain.
- Fast pain is sharp, well localized, and carried by A-delta fibers.
- Slow pain is dull, aching, burning, poorly localized, and carried by C fibers.
- Pain may also be somatic or visceral.
- Somatic pain arises from skin, muscles, joints, and body wall.
- Visceral pain arises from internal organs and is often poorly localized.
- Headache may involve vascular, meningeal, muscular, neural, or referred pain mechanisms.
🔬 CONCEPT EXPLAINED
Pain is not a single sensation. The body experiences different qualities of pain depending on the type of stimulus, receptor, nerve fiber, and central pathway involved.
Fast pain occurs quickly after injury. It is sharp, pricking, or cutting in character and is usually well localized. This type of pain is transmitted by A-delta fibers, which are thinly myelinated and conduct impulses relatively rapidly. Fast pain helps the body respond immediately to harmful stimuli, such as withdrawing the hand from a sharp object.
Slow pain begins after a delay and is dull, aching, throbbing, or burning. It is transmitted by C fibers, which are unmyelinated and conduct slowly. Slow pain is often associated with tissue destruction, inflammation, or deep injury. It is more unpleasant and emotionally disturbing than fast pain.
Pain may also be classified by origin. Somatic pain arises from skin, muscles, joints, bones, or body wall. Superficial somatic pain is usually well localized, while deep somatic pain may be dull and aching. Visceral pain arises from internal organs and is often poorly localized because visceral afferents are fewer and converge with somatic pathways.
In headache, the type of pain depends on the structure involved. Vascular distension may cause throbbing pain, muscle contraction may cause dull tight pain, meningeal irritation may cause severe diffuse pain, and sinus disease may cause localized facial or frontal pain.
⚠️ CLINICAL IMPORTANCE
The character of headache helps identify mechanism. A throbbing headache suggests vascular involvement. A tight band-like headache suggests muscle tension. Severe headache with neck stiffness suggests meningeal irritation. Facial pain worsened by bending forward suggests sinus involvement.
5 — Detailed Pain Pathway
🧠 CORE
- Pain impulses enter the spinal cord through dorsal roots.
- First-order neurons have cell bodies in dorsal root ganglia or sensory cranial nerve ganglia.
- Second-order neurons are located mainly in the dorsal horn.
- Pain fibers cross to the opposite side of the spinal cord.
- They ascend in the anterolateral/spinothalamic tract.
- Third-order neurons are located in the thalamus.
- Final perception occurs in cerebral cortex, especially somatosensory cortex.
- Emotional response to pain involves limbic and reticular systems.
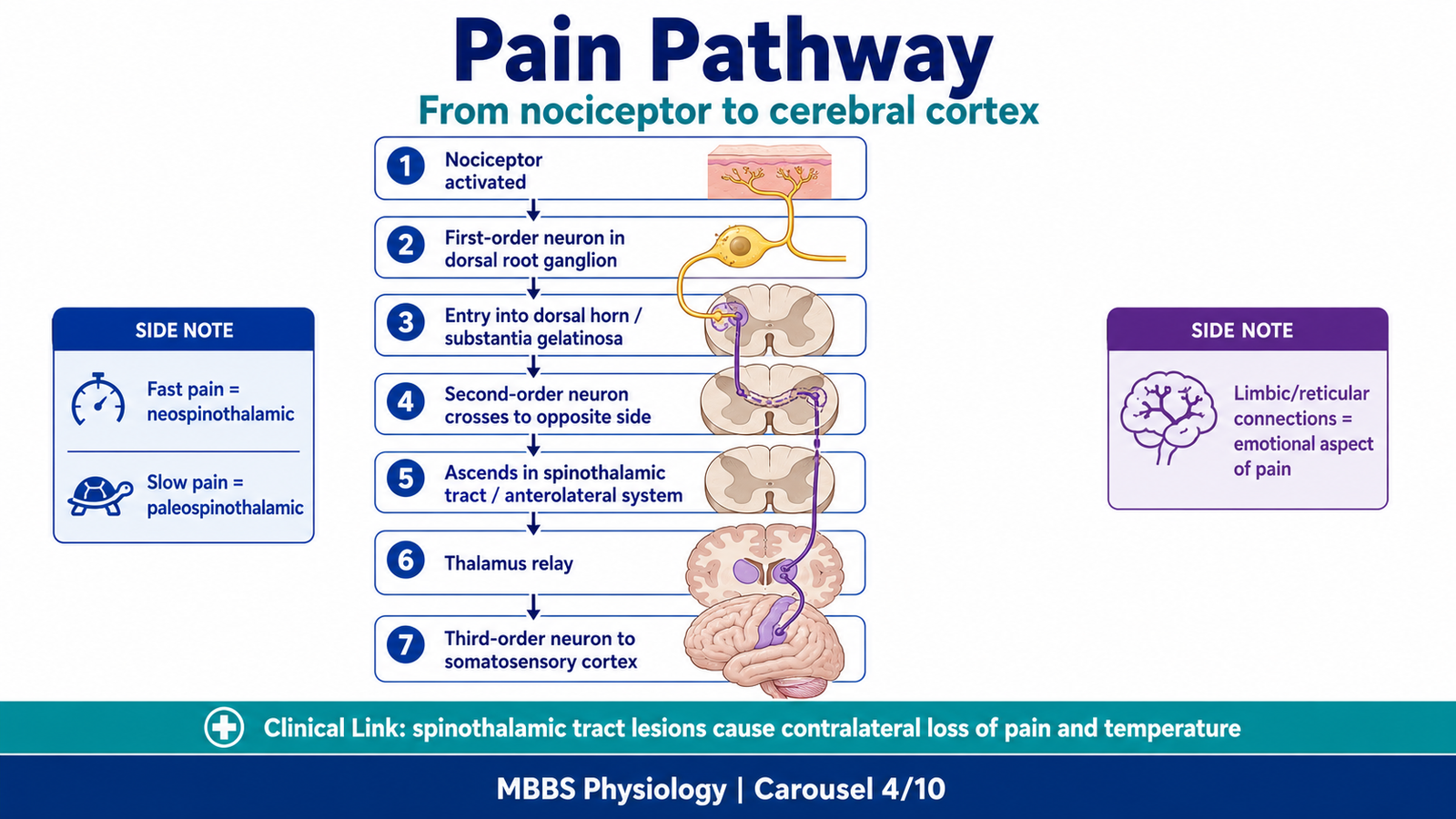
🔬 CONCEPT EXPLAINED
The pain pathway begins when nociceptors are stimulated by tissue injury. The impulse travels through peripheral sensory fibers to the cell body of the first-order neuron, located in the dorsal root ganglion for spinal nerves or sensory ganglia of cranial nerves for head and face.
The central processes of these neurons enter the spinal cord through the dorsal root and synapse in the dorsal horn. Important areas include lamina I, lamina II, also called substantia gelatinosa, and lamina V. Here the first-order neuron communicates with the second-order neuron.
The second-order neuron crosses to the opposite side of the spinal cord through the anterior white commissure. It then ascends in the anterolateral system, especially the spinothalamic tract. This crossing explains why damage to one side of the spinal cord can affect pain and temperature sensation on the opposite side of the body below the lesion.
The ascending fibers reach the thalamus, especially the ventral posterolateral nucleus for body pain and ventral posteromedial nucleus for facial pain. From the thalamus, third-order neurons project to the somatosensory cortex, where pain is localized and interpreted.
Pain is not only a sensory experience. Collaterals also reach the reticular formation and limbic system, which produce arousal, attention, emotional distress, and autonomic responses. This is why pain can cause anxiety, sweating, tachycardia, and behavioral changes.
Fast Pain Pathway
Fast pain travels mainly through A-delta fibers. It enters the dorsal horn, crosses, and ascends rapidly in the neospinothalamic tract to the thalamus and somatosensory cortex. This pathway allows accurate localization of sharp pain.
Slow Pain Pathway
Slow pain travels mainly through C fibers. It synapses more diffusely in the dorsal horn and ascends through paleospinothalamic pathways. It projects to the thalamus, reticular formation, limbic areas, and cortex. This explains why slow pain is poorly localized and emotionally unpleasant.
⚠️ CLINICAL IMPORTANCE
Lesions of the spinothalamic tract cause loss of pain and temperature sensation on the opposite side of the body. In headache, pain from the face and anterior head is commonly transmitted through the trigeminal nerve, while pain from the posterior head and upper neck may involve upper cervical nerves.
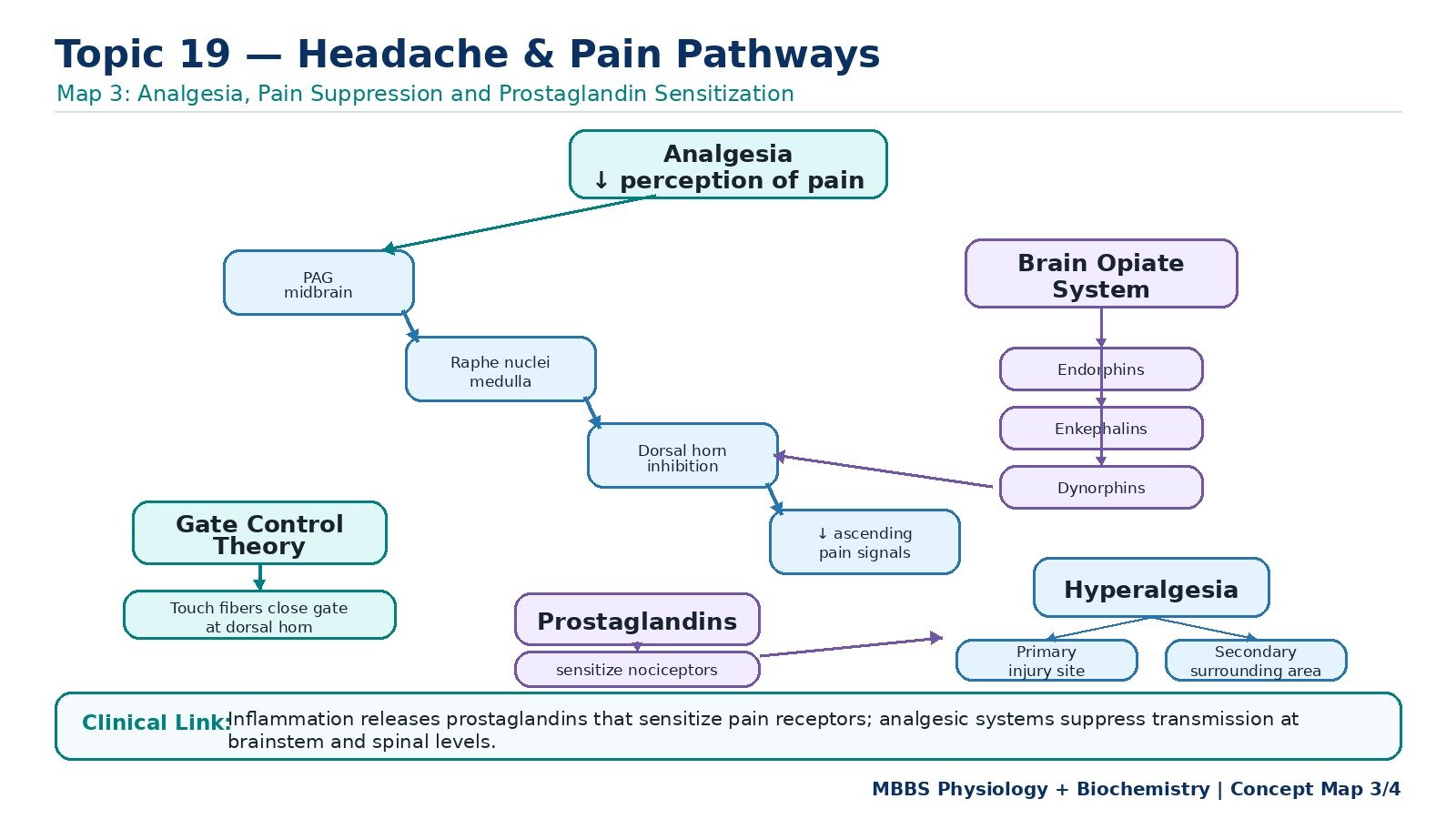
6 — Analgesia and Pain Suppression System
🧠 CORE
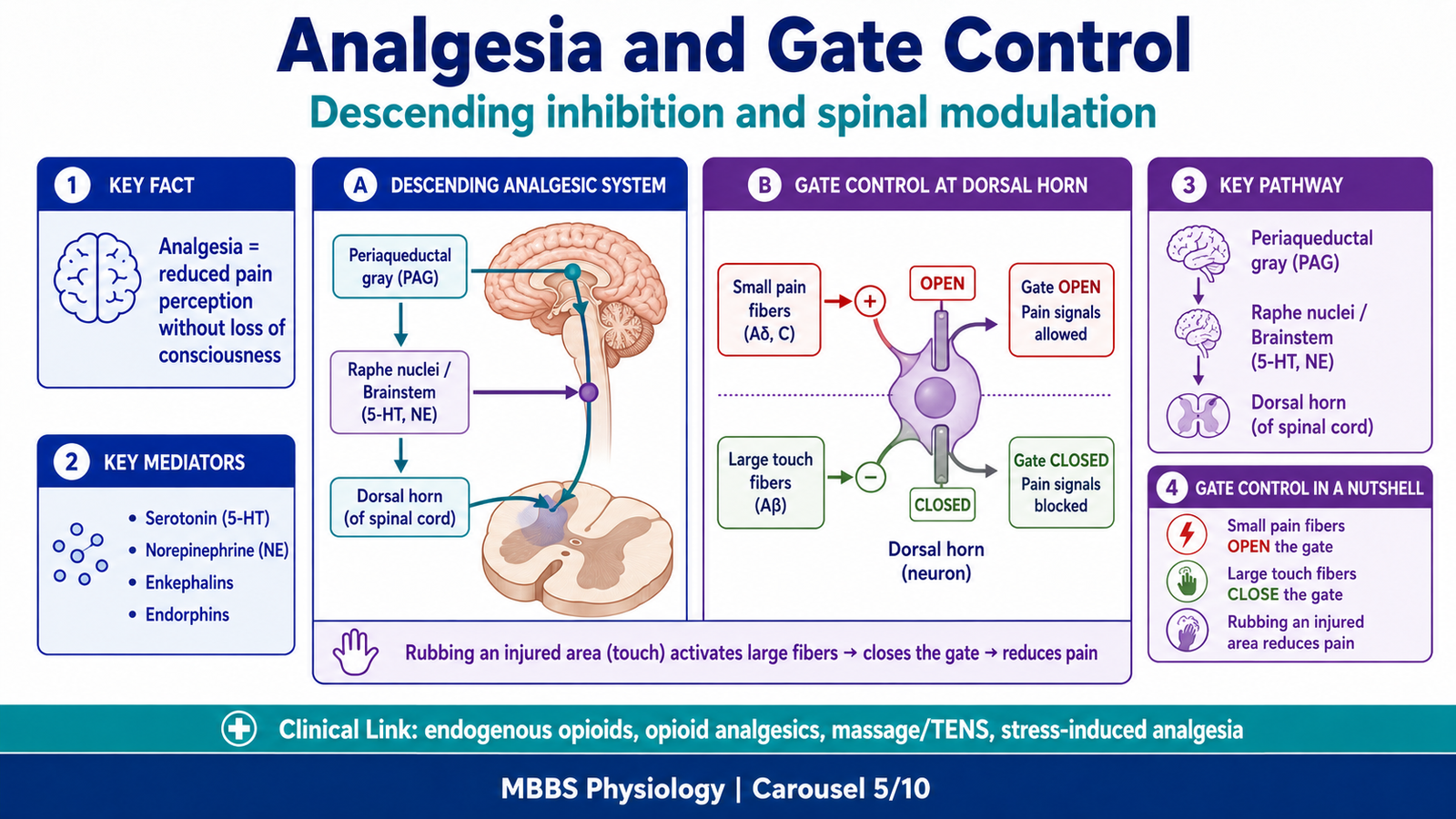
- Analgesia means reduction or absence of pain sensation.
- The body has a natural descending pain suppression system.
- Important areas include periaqueductal gray, raphe nuclei, and dorsal horn.
- Neurotransmitters involved include serotonin, norepinephrine, enkephalins, endorphins, and dynorphins.
- Pain suppression acts by inhibiting transmission at the dorsal horn.
- The brain opiate system uses endogenous opioid peptides.
- This system explains stress-induced analgesia and the action of opioid drugs.
🔬 CONCEPT EXPLAINED
Pain is not simply transmitted passively from the body to the brain. The nervous system has powerful mechanisms to suppress pain. This is important because constant pain transmission would interfere with survival, movement, and attention. During emergencies, the body may temporarily reduce pain so that a person can escape danger.
The descending pain suppression system begins mainly in the periaqueductal gray area of the midbrain. Neurons from this region project to the raphe nuclei in the medulla and other brainstem centers. From there, descending fibers travel down the spinal cord and end in the dorsal horn, especially around the substantia gelatinosa.
At the dorsal horn, descending fibers inhibit pain transmission from primary afferent neurons to second-order neurons. This inhibition occurs partly through release of serotonin, norepinephrine, and endogenous opioid peptides such as enkephalins. These substances reduce neurotransmitter release from pain fibers and decrease excitability of second-order pain neurons.
The brain opiate system consists of naturally occurring opioid peptides, including endorphins, enkephalins, and dynorphins. These substances bind to opioid receptors and suppress pain transmission. Opioid drugs such as morphine produce analgesia because they act on similar receptors.
Therefore, analgesia can occur naturally through descending inhibition or pharmacologically through analgesic drugs. The body’s analgesic system does not remove the injury; it reduces the perception and transmission of pain.
⚠️ CLINICAL IMPORTANCE
Stress-induced analgesia occurs when a person feels little pain during acute danger but experiences pain later. Opioid analgesics act by enhancing opioid receptor activity but can cause dependence and respiratory depression, which are beyond the main scope of this first-year learning level.
7 — Gate Control Theory of Pain
🧠 CORE
- Gate control theory explains modulation of pain at the spinal cord level.
- The “gate” is mainly in the dorsal horn, especially substantia gelatinosa.
- Large touch fibers can inhibit pain transmission.
- Small pain fibers tend to open the gate and enhance pain transmission.
- Rubbing an injured area reduces pain by activating touch fibers.
- This theory explains some effects of massage, pressure, and transcutaneous electrical stimulation.
- It shows that pain can be modified before reaching the brain.
🔬 CONCEPT EXPLAINED
The gate control theory states that pain transmission can be increased or decreased at the level of the spinal cord. The dorsal horn acts like a gate that controls how much pain information passes upward to the brain.
Small pain fibers, especially A-delta and C fibers, carry nociceptive impulses into the dorsal horn. These impulses excite second-order pain neurons and open the gate, allowing pain to ascend.
Large sensory fibers, such as A-beta fibers carrying touch and pressure, activate inhibitory interneurons in the substantia gelatinosa. These interneurons reduce the activity of second-order pain neurons. As a result, less pain information ascends to the brain.
This explains why rubbing or pressing an injured area reduces pain. For example, after hitting the elbow, a person instinctively rubs the area. Touch and pressure impulses activate large fibers, which partially close the spinal pain gate.
⚠️ CLINICAL IMPORTANCE
Gate control theory is clinically relevant in massage, physiotherapy, and transcutaneous electrical nerve stimulation. It also explains why non-painful sensory input can reduce pain perception.
8 — Hyperalgesia: Primary and Secondary
🧠 CORE
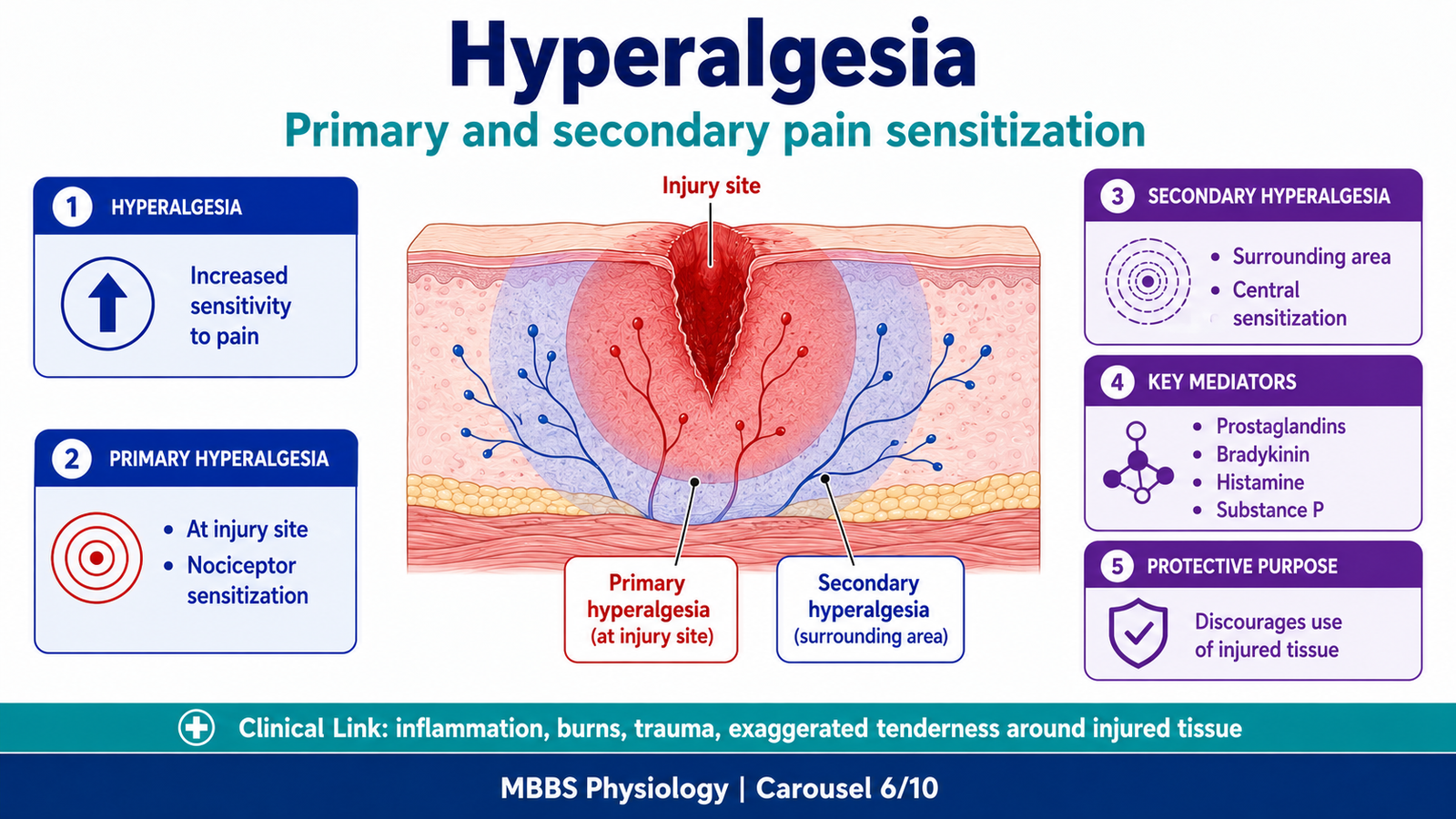
- Hyperalgesia means increased sensitivity to painful stimuli.
- Primary hyperalgesia occurs at the injured area.
- Secondary hyperalgesia occurs in surrounding uninjured tissue.
- Primary hyperalgesia is mainly due to sensitization of nociceptors.
- Secondary hyperalgesia is mainly due to central sensitization in spinal cord pathways.
- Inflammatory mediators such as prostaglandins contribute to hyperalgesia.
- Hyperalgesia protects injured tissue but may also increase suffering.
🔬 CONCEPT EXPLAINED
When tissue is injured, the painful area often becomes unusually sensitive. A stimulus that normally causes mild pain may become extremely painful. This is called hyperalgesia.
Primary hyperalgesia occurs at the site of injury. It is mainly caused by local chemical mediators released from damaged cells and inflammatory cells. These mediators include prostaglandins, bradykinin, histamine, potassium ions, and substance P. They lower the threshold of nociceptors, so the receptors fire more easily. As a result, the injured area becomes tender and painful.
Secondary hyperalgesia occurs in the surrounding uninjured tissue. Here the problem is not mainly at the peripheral receptor. Instead, repeated pain impulses increase the excitability of neurons in the dorsal horn and central pain pathways. This is called central sensitization. Because spinal neurons become more responsive, pain may spread beyond the injured area.
The purpose of hyperalgesia is protective. It discourages movement and pressure on injured tissue, allowing healing. However, excessive hyperalgesia can cause unnecessary pain and disability.
⚠️ CLINICAL IMPORTANCE
Primary hyperalgesia is common around inflamed or injured tissue. Secondary hyperalgesia explains why pain may spread beyond the exact area of injury. This is important in burns, trauma, inflammation, and chronic pain states.
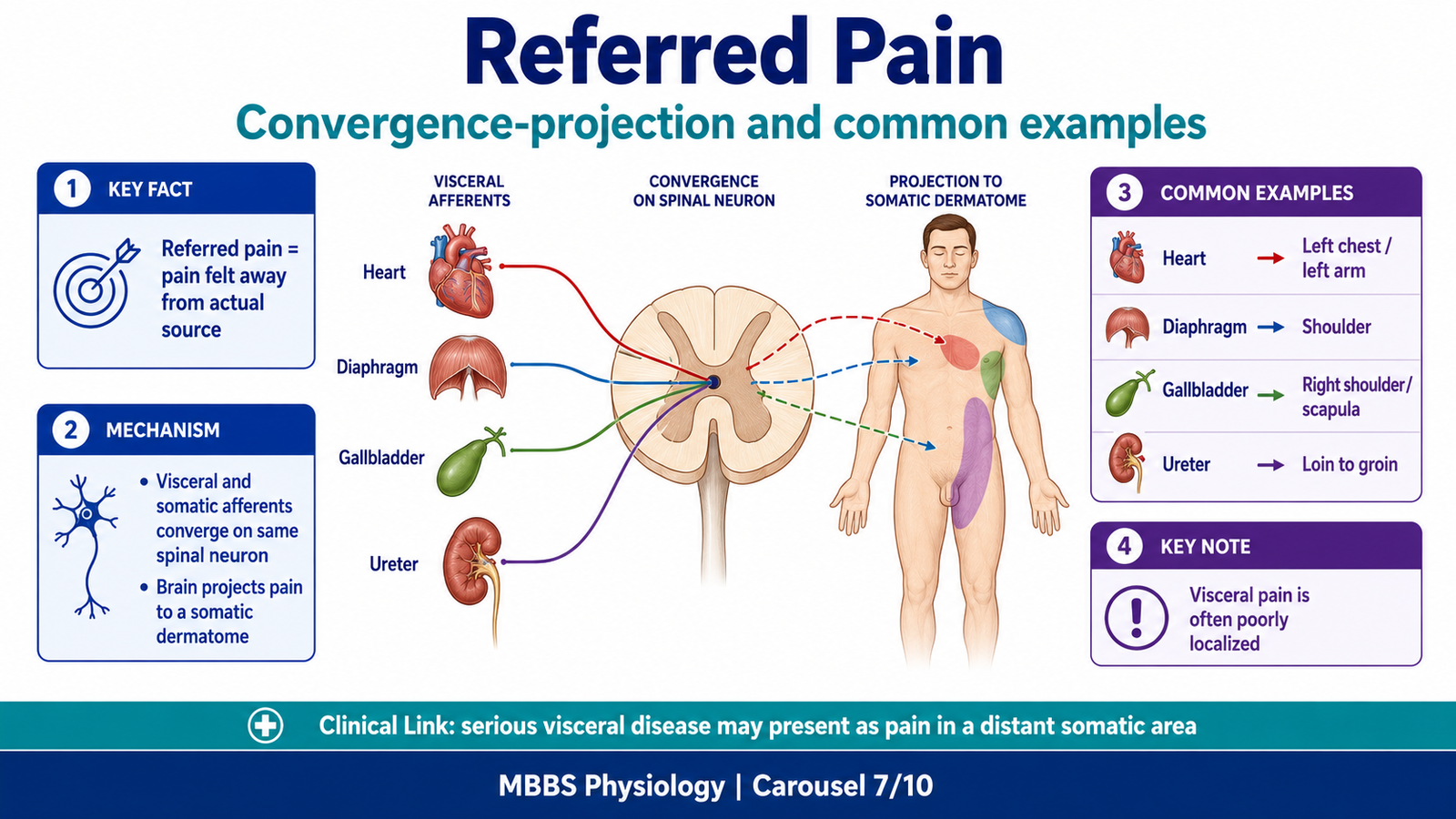
9 — Referred Pain and Its Mechanism
🧠 CORE
- Referred pain is pain felt away from its actual source.
- It commonly occurs with visceral pain.
- Visceral and somatic afferents may enter the same spinal cord segments.
- The brain misinterprets visceral pain as coming from a somatic area.
- This is called convergence-projection mechanism.
- Referred pain follows dermatomal patterns.
- Clinical examples include cardiac pain felt in left arm and diaphragmatic irritation felt in shoulder.
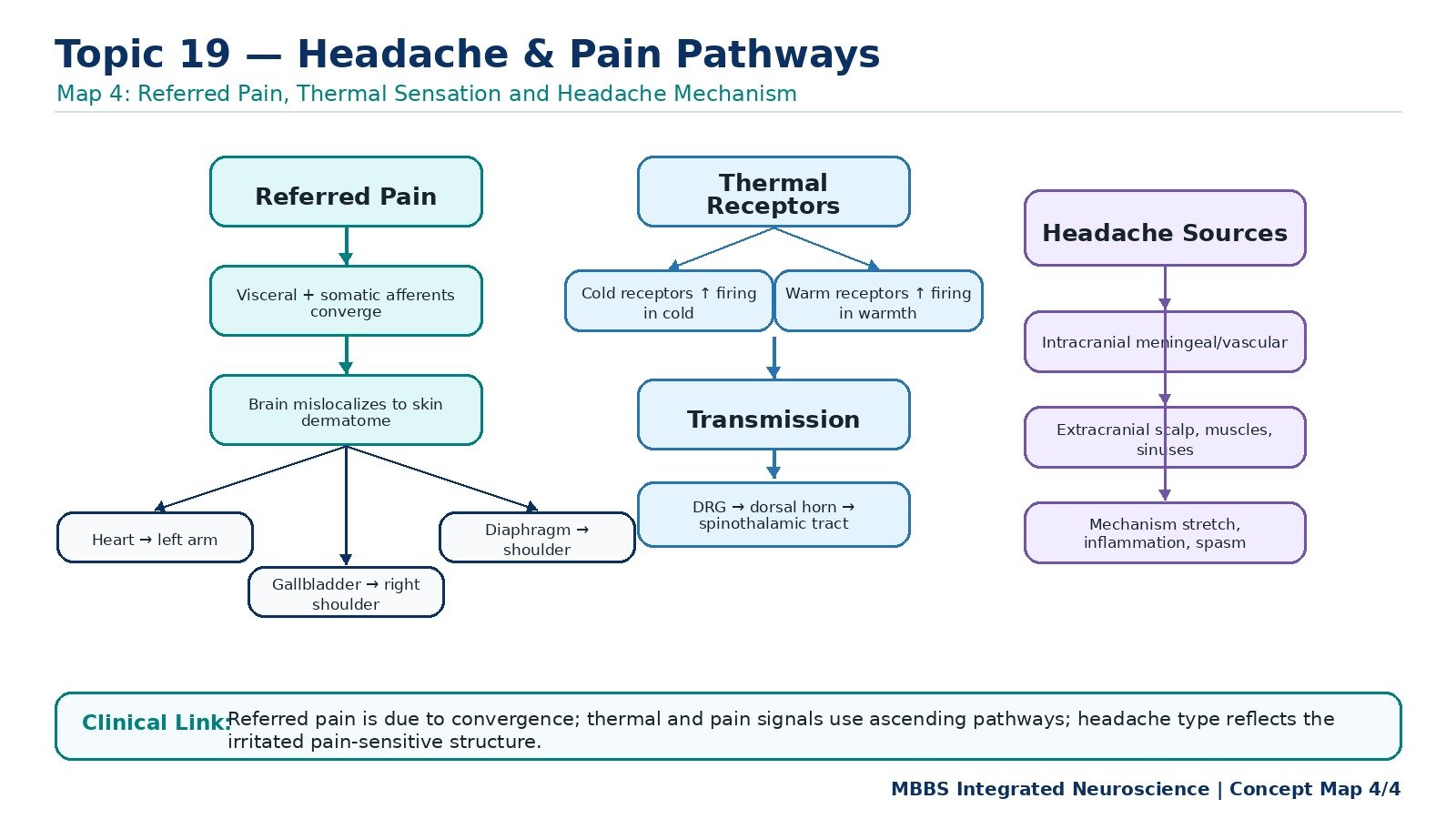
🔬 CONCEPT EXPLAINED
Referred pain occurs when pain arising from one structure is felt in another area of the body. This usually happens because visceral organs and somatic body regions share common spinal cord segments.
The most accepted explanation is the convergence-projection theory. Visceral pain fibers and somatic pain fibers converge on the same second-order neurons in the spinal cord. The brain is more accustomed to receiving pain from skin and muscles than from internal organs. Therefore, when visceral pain impulses activate the shared pathway, the brain incorrectly projects the pain to the somatic region supplied by the same spinal segment.
For example, pain from the heart enters spinal cord segments T1–T5. These segments also receive sensory fibers from the left chest and medial side of the left arm. As a result, cardiac pain may be felt in the chest, left shoulder, or left arm.
Referred pain is clinically important because the site of pain may not be the actual site of disease. A patient with gallbladder irritation may feel pain in the right shoulder. Diaphragmatic irritation may also refer pain to the shoulder because the diaphragm is supplied by the phrenic nerve from C3–C5, the same segments that supply the shoulder region.
Causes of Referred Pain
Referred pain may occur due to:
- Convergence of visceral and somatic afferents on the same spinal neurons.
- Embryological origin of organs and body wall from related segments.
- Poor localization of visceral pain by the brain.
- Shared spinal cord segments between deep structures and superficial dermatomes.
- Irritation of nerves that supply both deep and superficial regions.
Clinical Examples
- Heart ischemia → pain in chest, left shoulder, left arm, jaw.
- Diaphragmatic irritation → shoulder pain.
- Gallbladder disease → right shoulder or right scapular pain.
- Ureteric colic → loin to groin pain.
- Sinusitis → frontal or facial headache.
- Dental disease → referred facial or head pain.
⚠️ CLINICAL IMPORTANCE
Referred pain is a high-yield clinical concept because serious disease may present as pain in a distant area. In headache, pain from sinuses, teeth, cervical muscles, eyes, or meninges may be perceived in specific regions of the head.
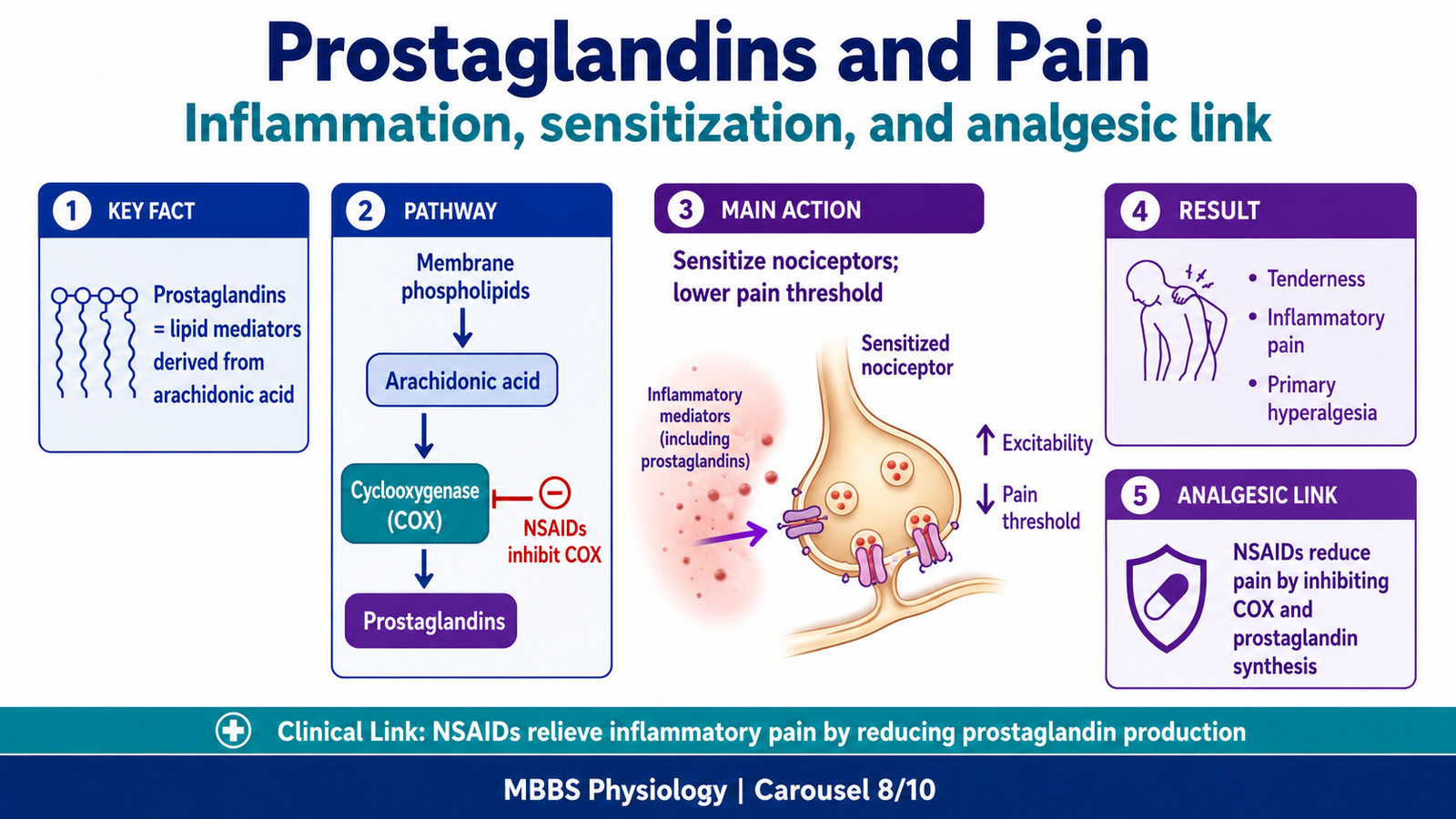
10 — Prostaglandins and Pain
🧠 CORE
- Prostaglandins are lipid-derived chemical mediators.
- They are formed from arachidonic acid in cell membranes.
- They are produced during tissue injury and inflammation.
- Prostaglandins sensitize nociceptors to other pain-producing chemicals.
- They contribute to tenderness, hyperalgesia, fever, and inflammatory pain.
- NSAIDs reduce pain by inhibiting prostaglandin synthesis.
- Prostaglandins link biochemistry with clinical pain mechanisms.
🔬 CONCEPT EXPLAINED
Prostaglandins are locally acting lipid mediators derived from arachidonic acid, a fatty acid present in cell membrane phospholipids. When tissue is injured or inflamed, arachidonic acid is released and converted into prostaglandins through cyclooxygenase enzymes.
Prostaglandins do not always directly produce strong pain by themselves. Their major role is to sensitize pain receptors. This means they lower the threshold of nociceptors so that other painful stimuli, such as bradykinin, pressure, heat, or chemical irritation, produce stronger pain.
This mechanism is very important in inflammation. In an inflamed area, prostaglandins make nociceptors more excitable. Therefore, even mild touch, pressure, or movement may become painful. This contributes to tenderness and primary hyperalgesia.
The role of prostaglandins also explains the mechanism of common analgesic drugs. NSAIDs inhibit cyclooxygenase enzymes and reduce prostaglandin synthesis. As prostaglandin levels fall, nociceptor sensitization decreases, and pain is reduced.
⚠️ CLINICAL IMPORTANCE
The mechanistic link between inflammation and pain is largely due to chemical mediators such as prostaglandins. This is why inflammatory headache, muscle pain, sinus pain, and tissue injury may improve with NSAIDs.
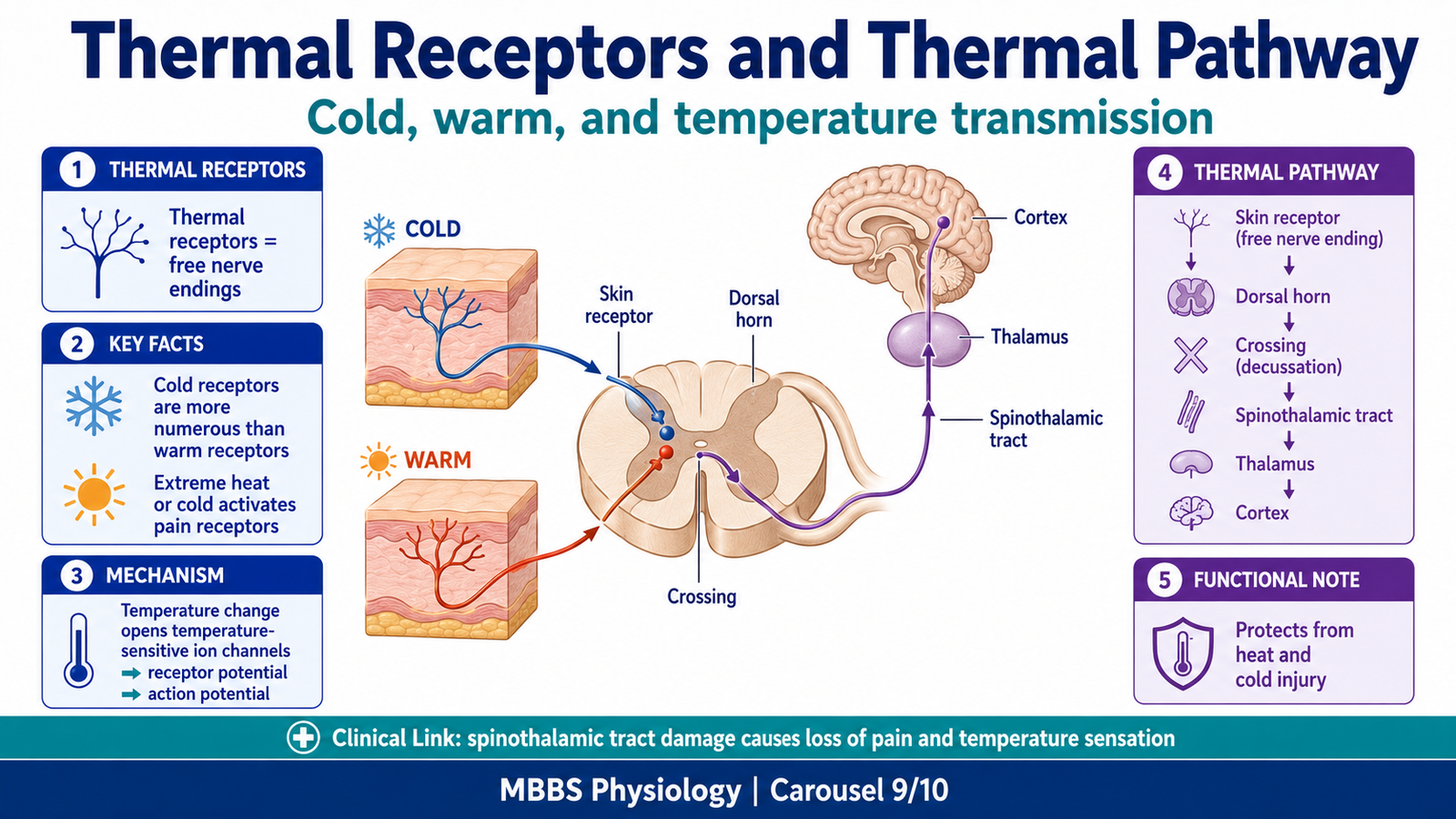
11 — Thermal Receptors and Thermal Sensation
🧠 CORE
- Thermal receptors detect cold and warmth.
- Cold receptors are more numerous than warm receptors.
- Thermal receptors are free nerve endings.
- Cold is mainly carried by A-delta and C fibers.
- Warmth is mainly carried by C fibers.
- Extreme heat or cold can stimulate pain receptors.
- Thermal signals ascend mainly through the spinothalamic pathway.
- Thermal sensation protects the body from temperature injury.
🔬 CONCEPT EXPLAINED
Thermal sensation allows the body to detect environmental temperature and protect tissues from thermal injury. The skin contains separate receptors for cold and warmth. These receptors are free nerve endings that respond to changes in temperature.
Cold receptors are more numerous and respond to cooling of the skin. They are most active during moderate cooling. Warm receptors respond to warming of the skin. If temperature becomes extreme, especially above damaging levels or below freezing levels, pain receptors are activated instead of ordinary thermal receptors. This is why very hot and very cold stimuli can both feel painful.
The mechanism of stimulation depends on temperature-induced changes in receptor membrane permeability and ion channel activity. When temperature changes, specific temperature-sensitive ion channels open or close, generating receptor potentials. If the receptor potential reaches threshold, action potentials are produced in sensory fibers.
Thermal impulses enter the spinal cord through dorsal roots, synapse in the dorsal horn, cross to the opposite side, and ascend in the anterolateral system, especially the spinothalamic tract. They reach the thalamus and then the somatosensory cortex, where the temperature sensation is consciously perceived.
Thermal sensation has great survival value. It allows withdrawal from harmful heat or cold, guides behavior, and helps maintain body temperature.
⚠️ CLINICAL IMPORTANCE
Damage to the spinothalamic tract may cause loss of pain and temperature sensation on the opposite side of the body. Loss of thermal sensation increases the risk of burns or cold injury.
12 — Headache: Intracranial and Extracranial Causes with Mechanisms
🧠 CORE
- Headache occurs due to stimulation of pain-sensitive structures.
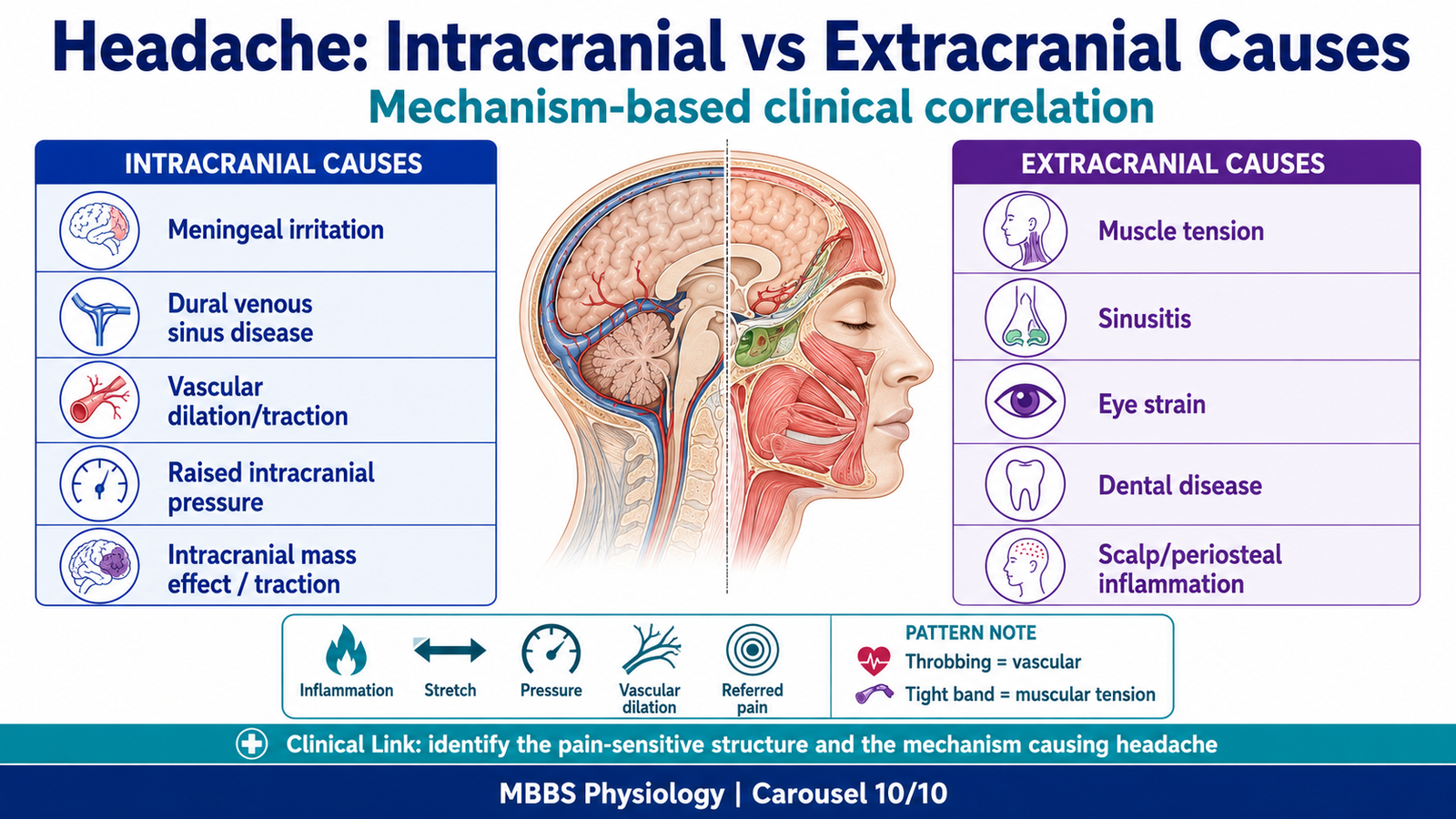
- Intracranial causes include meningeal irritation, vascular distension, venous sinus disease, raised intracranial pressure, and traction on vessels.
- Extracranial causes include muscle tension, sinusitis, dental disease, eye strain, scalp inflammation, and cervical problems.
- Pain mechanism may be vascular, inflammatory, muscular, compressive, or referred.
- Headache location depends on nerve supply and referred pain patterns.
- Prostaglandins and inflammatory mediators increase pain sensitivity.
- Headache assessment requires mechanism-based thinking.
🔬 CONCEPT EXPLAINED
Headache can be understood by asking one question: which pain-sensitive structure is being stimulated, and by what mechanism?
Intracranial headache occurs when structures inside the skull that contain nociceptors are affected. Meningeal inflammation, as in meningitis, activates pain receptors in the dura and meninges. Stretching or dilation of intracranial arteries may produce throbbing headache. Venous sinus thrombosis can cause headache by venous congestion, inflammation, and raised intracranial pressure. Increased intracranial pressure may stretch dura and blood vessels, producing diffuse headache.
Extracranial headache arises from structures outside the skull. Tension headache commonly results from contraction or strain of scalp and neck muscles. Sinusitis causes headache because inflamed sinus mucosa releases inflammatory mediators and pressure changes stimulate sensory nerves. Dental disease can refer pain to the face or head through branches of the trigeminal nerve. Eye strain can cause frontal or orbital headache due to overuse of ocular and periocular structures.
The mechanism of headache may therefore be inflammatory, vascular, muscular, compressive, or referred. For example, a throbbing headache suggests vascular pulsation; a dull tight headache suggests muscle tension; severe headache with fever and neck stiffness suggests meningeal irritation; facial pain with nasal symptoms suggests sinus disease.
Causes of Intracranial Headache
- Meningeal irritation, such as meningitis or subarachnoid irritation.
- Dilation or traction of large cerebral arteries.
- Dural venous sinus thrombosis or congestion.
- Raised intracranial pressure stretching dura or vessels.
- Intracranial mass effect causing traction on pain-sensitive structures.
- Inflammation involving meninges or vascular structures.
Causes of Extracranial Headache
- Scalp and neck muscle tension.
- Sinusitis.
- Dental disease.
- Eye strain or glaucoma-related pain.
- Scalp inflammation or trauma.
- Cervical joint or muscle disorders.
- Facial nerve or trigeminal sensory irritation.
⚠️ CLINICAL IMPORTANCE
Headache should be correlated with its mechanism. Meningeal headache is due to irritation of pain-sensitive meninges. Sinus headache is due to inflammation and pressure in paranasal sinuses. Tension headache is due to muscle contraction and local pain receptor activation. Vascular headache is related to distension or irritation of blood vessels.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
| Structure / Component | Function | Outcome |
|---|---|---|
| Nociceptors | Detect tissue injury | Pain warning signal begins |
| A-delta fibers | Rapid pain transmission | Sharp, localized fast pain |
| C fibers | Slow pain transmission | Dull, aching, burning pain |
| Dorsal horn | First central relay for pain | Pain can be transmitted or inhibited |
| Spinothalamic tract | Carries pain and temperature | Conscious perception of pain and thermal sensation |
| Thalamus | Sensory relay | Pain signal distributed to cortex |
| Somatosensory cortex | Localization and interpretation | Person identifies site and intensity of pain |
| Limbic system | Emotional response | Pain becomes unpleasant and distressing |
| Periaqueductal gray | Starts descending inhibition | Natural analgesia |
| Substantia gelatinosa | Modulates pain gate | Pain may increase or decrease |
| Dural venous sinuses | Drain venous blood and CSF | Sinus disease may cause headache |
| Prostaglandins | Sensitize nociceptors | Inflammatory pain and hyperalgesia |
| Thermal receptors | Detect warm and cold | Protection from heat and cold injury |
The anatomical arrangement of pain pathways explains clinical symptoms. Pain receptors detect injury, spinal pathways transmit the signal, cortical areas identify the pain, and descending systems control its intensity. In headache, dural sinuses, meninges, blood vessels, muscles, sinuses, eyes, and teeth provide the structural source of pain. Prostaglandins and inflammatory mediators increase receptor sensitivity, making pain stronger. Therefore, headache is best understood as an integrated result of structure, chemical mediators, nerve pathways, and brain interpretation.
🩺 5️⃣ Clinical Correlation
1. Meningitis Headache
Meningitis causes inflammation of meninges. The meninges are pain-sensitive, so inflammatory mediators stimulate nociceptors. This produces severe headache, often associated with fever, neck stiffness, and photophobia. The mechanism is meningeal irritation and inflammatory sensitization.
2. Migraine-Type Vascular Headache
Vascular headache is related to changes in cranial blood vessels and activation of trigeminal pain pathways. Dilation or irritation of meningeal vessels may activate nociceptors and produce throbbing pain. Chemical mediators can increase sensitivity of vascular pain receptors.
3. Sinus Headache
Sinusitis causes inflammation of paranasal sinus mucosa. Swelling, pressure changes, and prostaglandin-mediated sensitization stimulate sensory fibers. Pain may be felt in frontal, maxillary, or facial regions depending on the sinus involved.
4. Tension Headache
Tension headache is commonly related to sustained contraction or strain of scalp and neck muscles. Muscle ischemia, local chemical changes, and stimulation of pain receptors produce dull, tight, band-like headache.
5. Dental Referred Pain
Dental disease can produce pain referred to the face, jaw, or head because sensory fibers travel through branches of the trigeminal nerve. The brain may interpret pain as coming from nearby craniofacial areas.
6. Cavernous Sinus Thrombosis
Infection from the danger area of the face may spread to the cavernous sinus through valveless veins. This can cause severe headache, fever, eye swelling, and cranial nerve involvement because important nerves and the internal carotid artery are related to the cavernous sinus.
7. Raised Intracranial Pressure
Raised intracranial pressure stretches pain-sensitive dura, vessels, and venous sinuses. This may cause diffuse headache, often worse with coughing, straining, or lying down. The pain mechanism is mechanical stretching of intracranial pain-sensitive structures.
8. Hyperalgesia in Inflammation
Inflamed tissue becomes tender because prostaglandins and other mediators lower nociceptor threshold. This causes primary hyperalgesia at the site of injury. Repeated pain input can also produce secondary hyperalgesia in surrounding tissues.
📌 6️⃣ Summary Points
- Brain tissue itself is insensitive to pain, but dura, dural venous sinuses, meningeal vessels, scalp, muscles, sinuses, eyes, and teeth are pain-sensitive.
- Dural venous sinuses are endothelial-lined channels between dural layers and drain blood mainly into internal jugular veins.
- Superior sagittal sinus receives CSF through arachnoid granulations and is important in venous drainage and CSF absorption.
- Pain receptors are free nerve endings called nociceptors and respond to mechanical, thermal, and chemical stimuli.
- Fast pain is sharp and localized through A-delta fibers; slow pain is dull and poorly localized through C fibers.
- Pain and temperature ascend mainly through the spinothalamic tract after crossing in the spinal cord.
- Analgesia is produced naturally by descending pain suppression pathways involving periaqueductal gray, raphe nuclei, dorsal horn, and endogenous opioids.
- Gate control theory explains why rubbing an injured area reduces pain through activation of large touch fibers.
- Primary hyperalgesia occurs at the injury site due to nociceptor sensitization; secondary hyperalgesia occurs around the injury due to central sensitization.
- Referred pain occurs because visceral and somatic afferents converge on the same spinal neurons.
- Prostaglandins are lipid mediators derived from arachidonic acid and sensitize nociceptors during inflammation.
- Headache should always be interpreted by identifying the pain-sensitive structure involved and the mechanism causing its stimulation.