
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
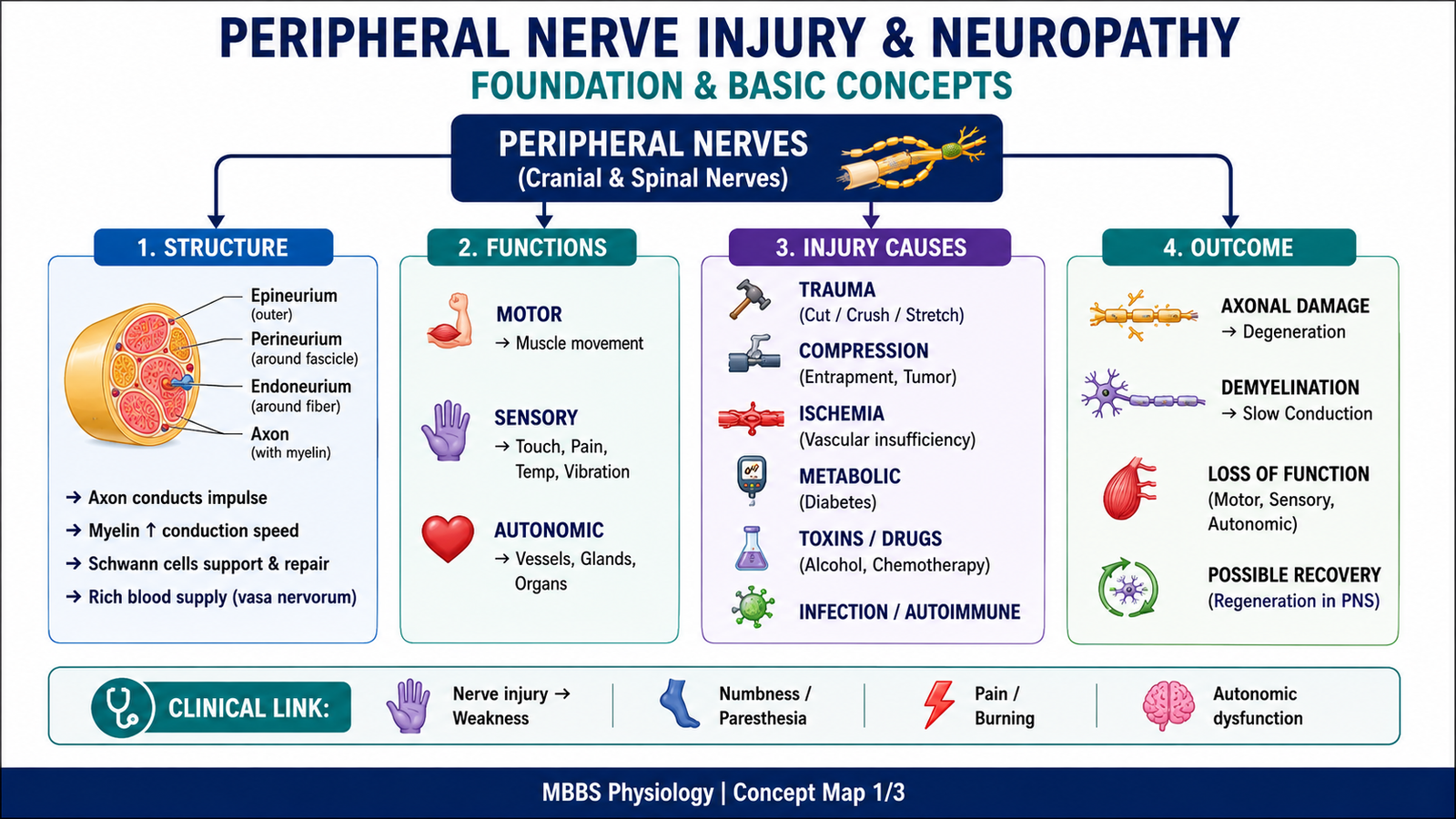
Peripheral nerves connect the central nervous system with muscles, skin, glands, blood vessels, and internal organs. They carry motor impulses from the spinal cord to skeletal muscles and sensory impulses from receptors back to the CNS. Because peripheral nerves are long, metabolically active, and exposed to trauma, compression, toxins, ischemia, and metabolic diseases, they are commonly injured.
When a peripheral nerve is damaged, the part of the axon distal to the injury loses connection with the neuronal cell body and undergoes degeneration. The proximal part may survive and attempt regeneration if the neuronal cell body remains alive and the Schwann cell pathway is preserved. This ability to regenerate is much better in the peripheral nervous system than in the central nervous system.
Clinically, peripheral nerve injury may cause weakness, sensory loss, pain, paresthesia, loss of reflexes, muscle wasting, and autonomic dysfunction. Diabetic neuropathy is one of the most important examples because chronic hyperglycemia damages peripheral nerves and produces sensory, motor, and autonomic complications.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Peripheral nerve injury: Damage to a nerve outside the brain and spinal cord, affecting motor, sensory, or autonomic fibers.
- Neuron: Functional unit of the nervous system consisting of cell body, dendrites, and axon.
- Axon: Long process of neuron that conducts impulses away from the cell body.
- Myelin sheath: Insulating covering around axons that increases speed of impulse conduction.
- Schwann cell: Glial cell of the peripheral nervous system responsible for myelination and regeneration support.
- Wallerian degeneration: Degeneration of the distal part of an axon after it is separated from the neuronal cell body.
- Chromatolysis: Microscopic reaction of neuronal cell body after axonal injury, characterized by swelling, dispersion of Nissl substance, and eccentric nucleus.
- Regeneration: Re-growth of injured axons from the proximal stump toward the target tissue.
- Peripheral neuropathy: Disease or dysfunction of peripheral nerves, usually causing sensory, motor, or autonomic symptoms.
- Diabetic neuropathy: Peripheral nerve damage caused by chronic diabetes mellitus, commonly affecting distal sensory nerves first.
Essential Terminology
- Proximal stump: Part of injured axon still connected to the neuronal cell body.
- Distal stump: Part of injured axon separated from the cell body; this part degenerates.
- Endoneurium: Connective tissue surrounding individual nerve fibers.
- Perineurium: Connective tissue surrounding a fascicle of nerve fibers.
- Epineurium: Outer connective tissue covering of an entire peripheral nerve.
- Denervation: Loss of nerve supply to a muscle, skin area, or organ.
- Paresthesia: Abnormal sensation such as tingling or pins and needles.
- Hypoesthesia: Reduced sensation.
- Neuropathic pain: Pain caused by nerve damage, often burning, shooting, or electric-like.
Basic Overview
- Peripheral nerves contain motor, sensory, and autonomic fibers.
- Axons depend on the neuronal cell body for structural proteins and metabolic support.
- When an axon is cut or severely damaged, the distal segment cannot survive independently.
- Degeneration clears damaged axon and myelin debris.
- Regeneration is possible in the peripheral nervous system because Schwann cells form guiding tubes.
- Regeneration is poor in the CNS because oligodendrocytes, glial scar formation, and inhibitory molecules prevent effective axonal regrowth.
- Diabetic neuropathy occurs due to metabolic injury, microvascular ischemia, oxidative stress, and impaired axonal function.
🔹 3️⃣ Core Learning — Curriculum Coverage
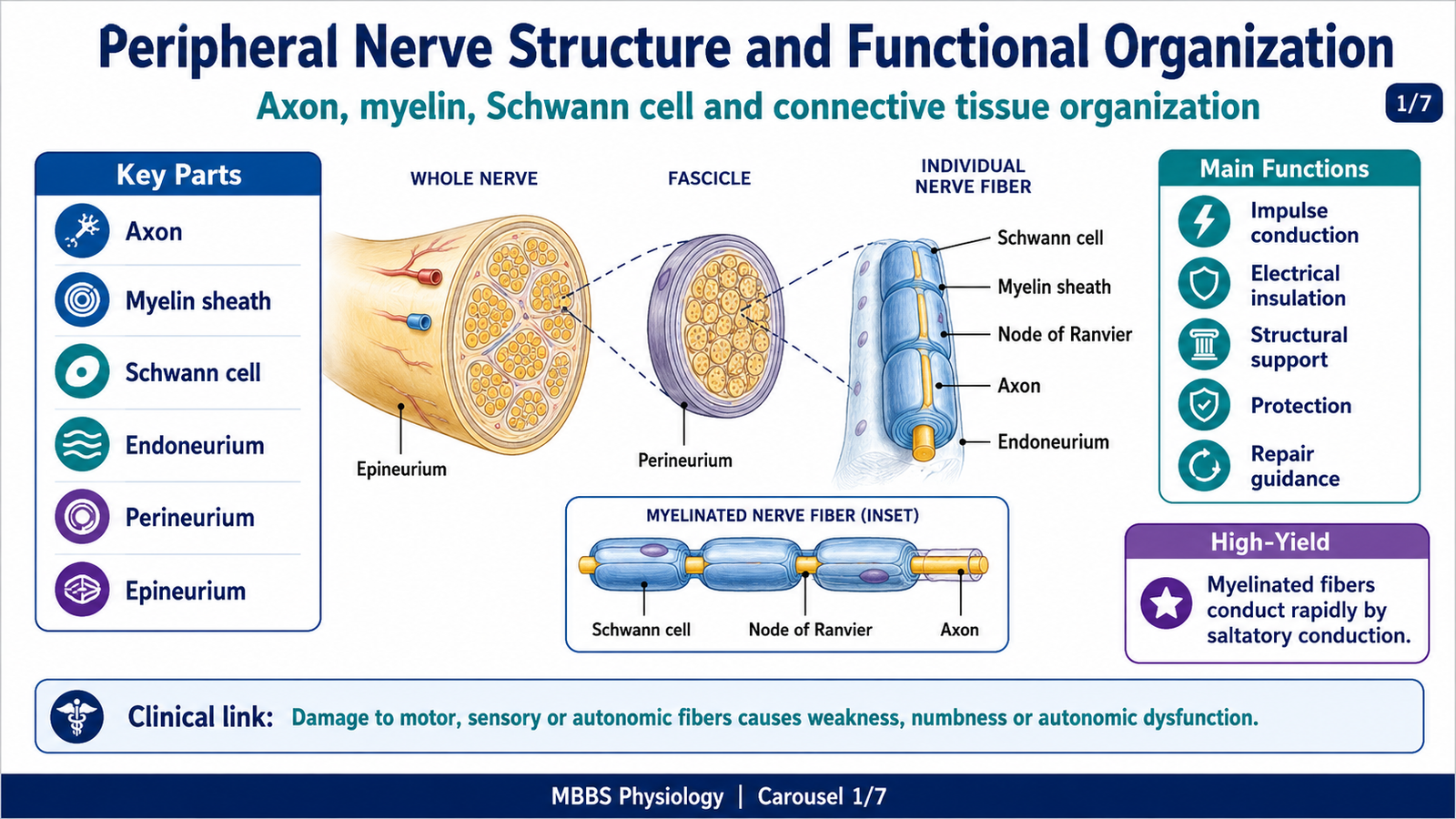
Peripheral Nerve Structure and Functional Organization
🧠 CORE
- Peripheral nerves contain axons supported by Schwann cells and connective tissue sheaths.
- Axons may be myelinated or unmyelinated.
- Myelinated fibers conduct impulses rapidly by saltatory conduction.
- Schwann cells support both myelination and regeneration in the PNS.
- Endoneurium, perineurium, and epineurium protect and organize nerve fibers.
- Blood supply to nerves is essential for axonal metabolism.
- Injury may affect motor, sensory, or autonomic fibers depending on the nerve involved.
🔬 CONCEPT EXPLAINED
To understand nerve degeneration and regeneration, students must first understand that a peripheral nerve is not just a wire-like structure. It is a living tissue made of axons, Schwann cells, connective tissue, blood vessels, and extracellular support. The axon conducts electrical impulses, but its survival depends on continuous metabolic support from the neuronal cell body. Proteins, enzymes, neurotransmitter-related substances, and structural materials move along the axon through axonal transport.
The myelin sheath is produced by Schwann cells in the peripheral nervous system. Myelin acts as an electrical insulator and allows action potentials to jump from one node of Ranvier to the next. This is called saltatory conduction. Because of this arrangement, a myelinated nerve fiber conducts impulses faster than an unmyelinated fiber. Therefore, when myelin is damaged, conduction slows or becomes blocked, even if the axon itself is not completely destroyed.
The connective tissue coverings are also functionally important. Endoneurium surrounds individual nerve fibers, perineurium organizes fibers into fascicles, and epineurium surrounds the whole nerve. These coverings protect nerve fibers and help preserve alignment after injury. If the connective tissue pathway remains intact, regenerating axons have a better chance of reaching the original target. If the nerve is completely disrupted and the pathway is lost, regeneration becomes poorly directed and functional recovery is limited.
Peripheral nerves need an adequate blood supply because axons are metabolically active. Ischemia can damage the axon and Schwann cells. This becomes clinically important in diabetes mellitus, where microvascular damage reduces nerve blood supply and contributes to neuropathy.
⚠️ CLINICAL IMPORTANCE
Damage to peripheral nerve structure causes predictable functional loss. If motor fibers are damaged, the patient develops weakness, loss of reflexes, and later muscle wasting. If sensory fibers are damaged, the patient develops numbness, tingling, burning pain, or loss of protective sensation. If autonomic fibers are damaged, sweating, vascular control, bladder function, gastrointestinal motility, or sexual function may be affected.
Causes and Patterns of Peripheral Nerve Degeneration
🧠 CORE
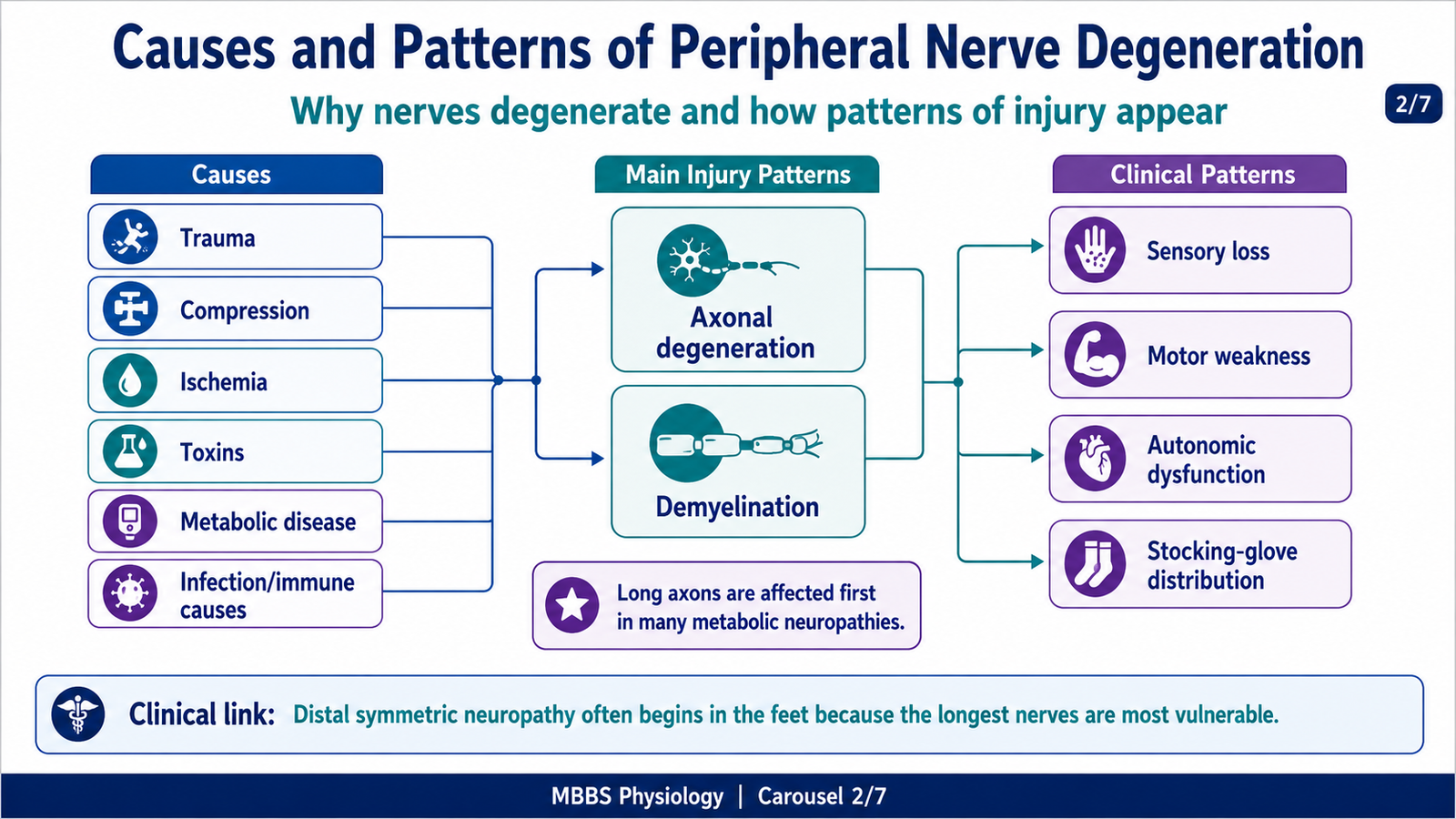
- Nerve degeneration occurs when axons or myelin are damaged.
- Common causes include trauma, compression, ischemia, toxins, metabolic disease, infection, and autoimmune injury.
- Axonal degeneration mainly damages the axon and secondarily affects myelin.
- Demyelination mainly damages myelin and slows conduction.
- Severe axonal injury produces Wallerian degeneration distal to the lesion.
- Chronic diseases such as diabetes commonly produce length-dependent neuropathy.
- The clinical pattern depends on which fibers are affected: motor, sensory, autonomic, or mixed.
🔬 CONCEPT EXPLAINED
Peripheral nerve degeneration means structural and functional breakdown of nerve fibers. The initiating event may be mechanical injury, compression, ischemia, metabolic disturbance, inflammation, toxic exposure, or inherited abnormality. The purpose of degeneration is not beneficial in itself, but it is a biological response that removes damaged axon and myelin so that repair can begin. In peripheral nerves, this removal phase is important because debris must be cleared before regenerating axons can grow through the injured segment.
In traumatic nerve injury, the axon may be crushed, stretched, or cut. If the axon remains continuous and only myelin is affected, conduction may recover quickly after remyelination. If the axon is interrupted, the distal part loses connection with the neuronal cell body. Since the cell body supplies essential proteins and metabolic material, the distal axon cannot maintain itself. This leads to Wallerian degeneration.
Compression injury causes degeneration because pressure reduces local blood flow and mechanically distorts nerve fibers. Mild compression may first damage myelin, causing conduction block. Severe or prolonged compression damages axons, leading to slower and less complete recovery. This explains why early relief of compression can prevent permanent deficit.
Ischemic injury occurs when the blood supply to the nerve is reduced. Nerve fibers require oxygen and glucose for impulse conduction and axonal transport. Reduced blood flow impairs ATP production, disrupts ion gradients, and damages axonal function. In diabetes, microvascular disease produces chronic low-grade ischemia, making distal nerves especially vulnerable.
Toxic and metabolic causes damage nerves by interfering with axonal metabolism, mitochondrial function, cytoskeletal transport, or myelin maintenance. Long axons are affected first because they have greater metabolic demand and depend heavily on long-distance axonal transport. Therefore, many neuropathies begin in the feet before the hands.
⚠️ CLINICAL IMPORTANCE
The cause and pattern of degeneration determine symptoms. Axonal neuropathy usually causes reduced amplitude of nerve impulses and often produces weakness or sensory loss. Demyelinating neuropathy mainly slows conduction and may cause weakness with relatively preserved axon early on. Length-dependent neuropathy produces a “stocking-glove” pattern because the longest nerves are affected first.
Wallerian Degeneration
🧠 CORE
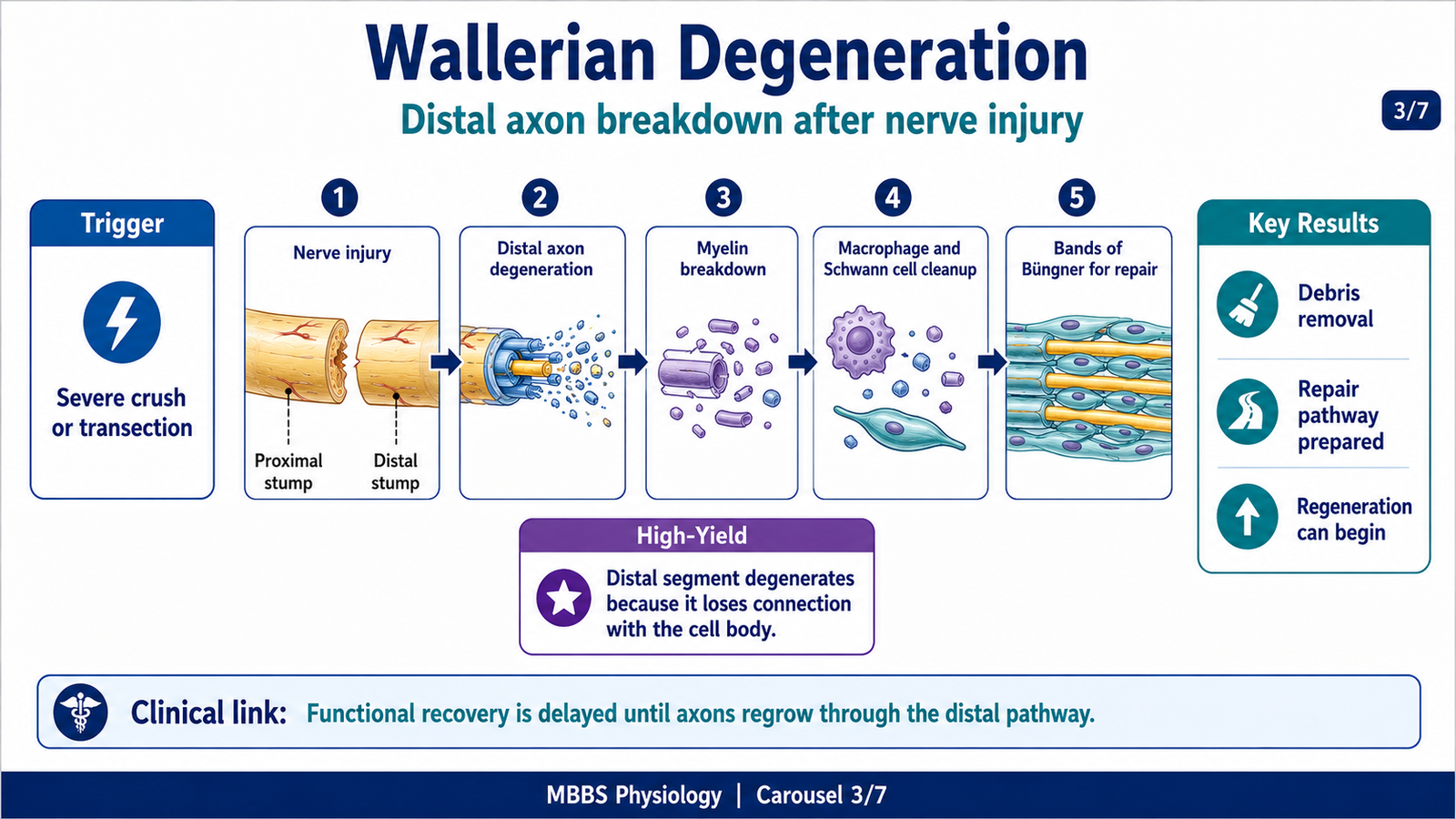
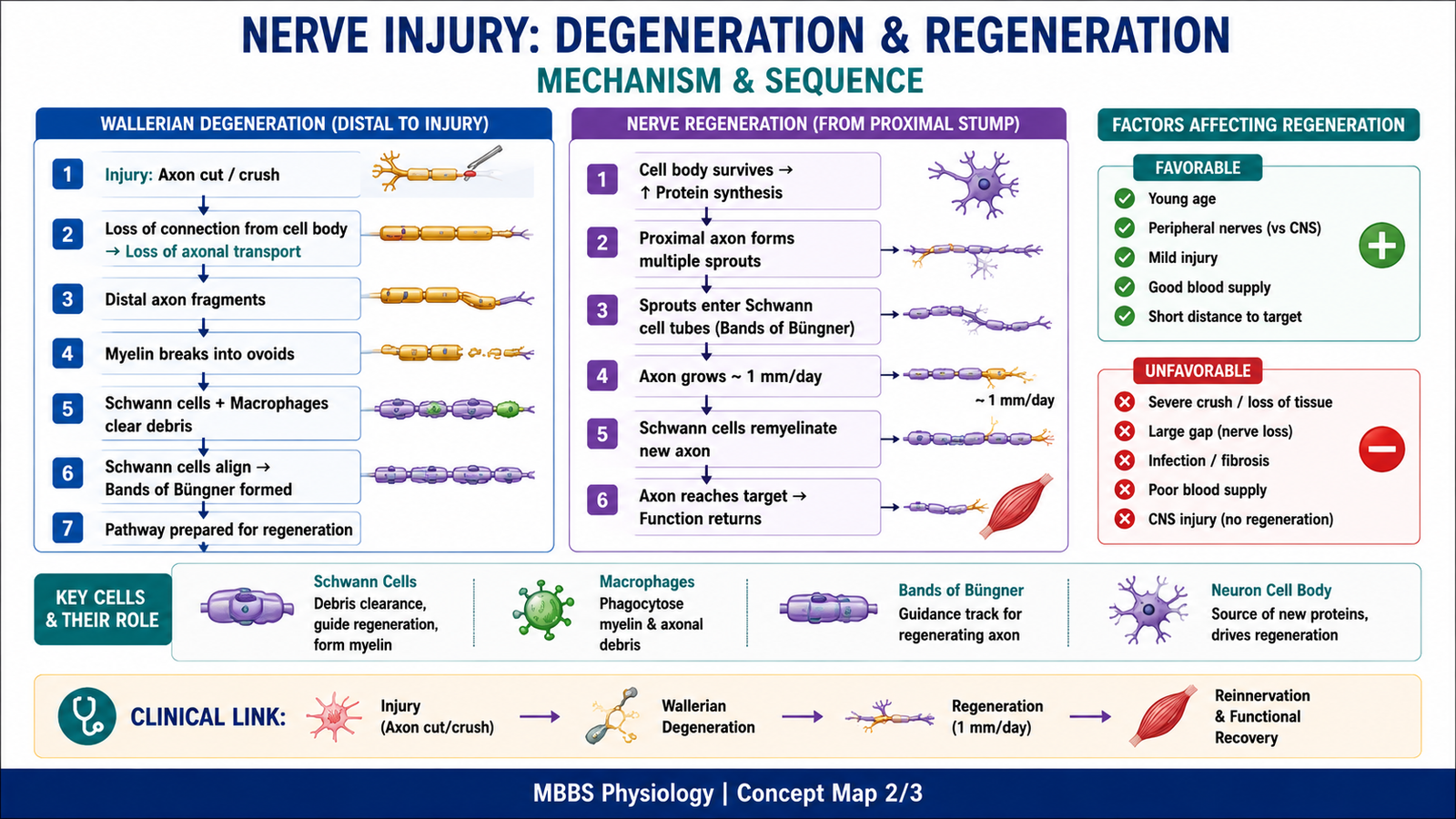
- Wallerian degeneration is degeneration of the distal axon after separation from the neuronal cell body.
- It occurs after severe axonal injury such as nerve transection or crush.
- The distal axon and myelin sheath break down.
- Schwann cells and macrophages remove debris.
- Schwann cells form regeneration tubes called bands of Büngner.
- The proximal axon forms sprouts that may grow into the Schwann cell tubes.
- Successful regeneration depends on preserved endoneurial pathway and survival of neuronal cell body.
🔬 CONCEPT EXPLAINED
Wallerian degeneration begins when an axon is cut or severely damaged. The stimulus or initiating event is loss of continuity between the distal axon and the neuronal cell body. The neuronal cell body normally provides structural proteins, enzymes, and metabolic support through axonal transport. Once the distal axon is separated, this supply stops. As a result, the distal axon cannot maintain its cytoskeleton, membrane integrity, or myelin relationship, so it degenerates.
The purpose of Wallerian degeneration is to remove the nonfunctional distal axon and damaged myelin so that the pathway can be prepared for possible regeneration. Although degeneration sounds harmful, in the peripheral nervous system it is also part of the repair process. Damaged axon and myelin debris would physically and chemically obstruct new axonal growth if they remained in place.
The sequence begins with fragmentation of the distal axon. The axonal cytoskeleton breaks down, and the myelin sheath separates into small segments called myelin ovoids. Schwann cells lose their myelinating arrangement and become active repair cells. Macrophages enter the area and, together with Schwann cells, phagocytose axonal and myelin debris. This clearing process creates a clean pathway for new growth.
At the same time, the proximal stump reacts to injury. The part of the proximal axon near the injury may degenerate backward for a short distance. If the cell body survives, the remaining proximal axon forms multiple growth sprouts. These sprouts search for a pathway. Schwann cells in the distal nerve stump proliferate and align longitudinally, forming bands of Büngner. These Schwann cell tubes guide regenerating axons toward the original target organ.
Control and regulation depend mainly on Schwann cell activity, macrophage-mediated clearance, local growth factors, and survival response of the neuronal cell body. Schwann cells produce supportive molecules and create a permissive environment for axonal growth. Macrophages clear inhibitory debris. The neuronal cell body increases protein synthesis to support regeneration.
The functional outcome depends on whether the regenerating axon enters the correct endoneurial tube and reaches the proper target. If a motor axon reaches its original muscle, motor function may recover. If it fails to reach the target, muscle remains denervated and atrophies. If axons grow incorrectly, abnormal sensation, poor motor control, or painful neuroma may occur.
The physiological advantage of Wallerian degeneration in the PNS is that it converts a damaged nerve segment into a repair pathway. It removes debris and allows Schwann cells to guide regeneration. This is why peripheral nerves can recover better than CNS tracts.
⚠️ CLINICAL IMPORTANCE
Wallerian degeneration explains why symptoms after nerve transection persist until regeneration occurs. A patient may lose movement or sensation immediately after injury because conduction is interrupted. Recovery is slow because axons must regrow from the proximal stump toward the target. If the nerve gap is large, the endoneurial pathway is destroyed, or the target muscle remains denervated too long, recovery becomes incomplete.
Microscopic Appearance of Degenerating Neurons and Nerve Fibers
🧠 CORE
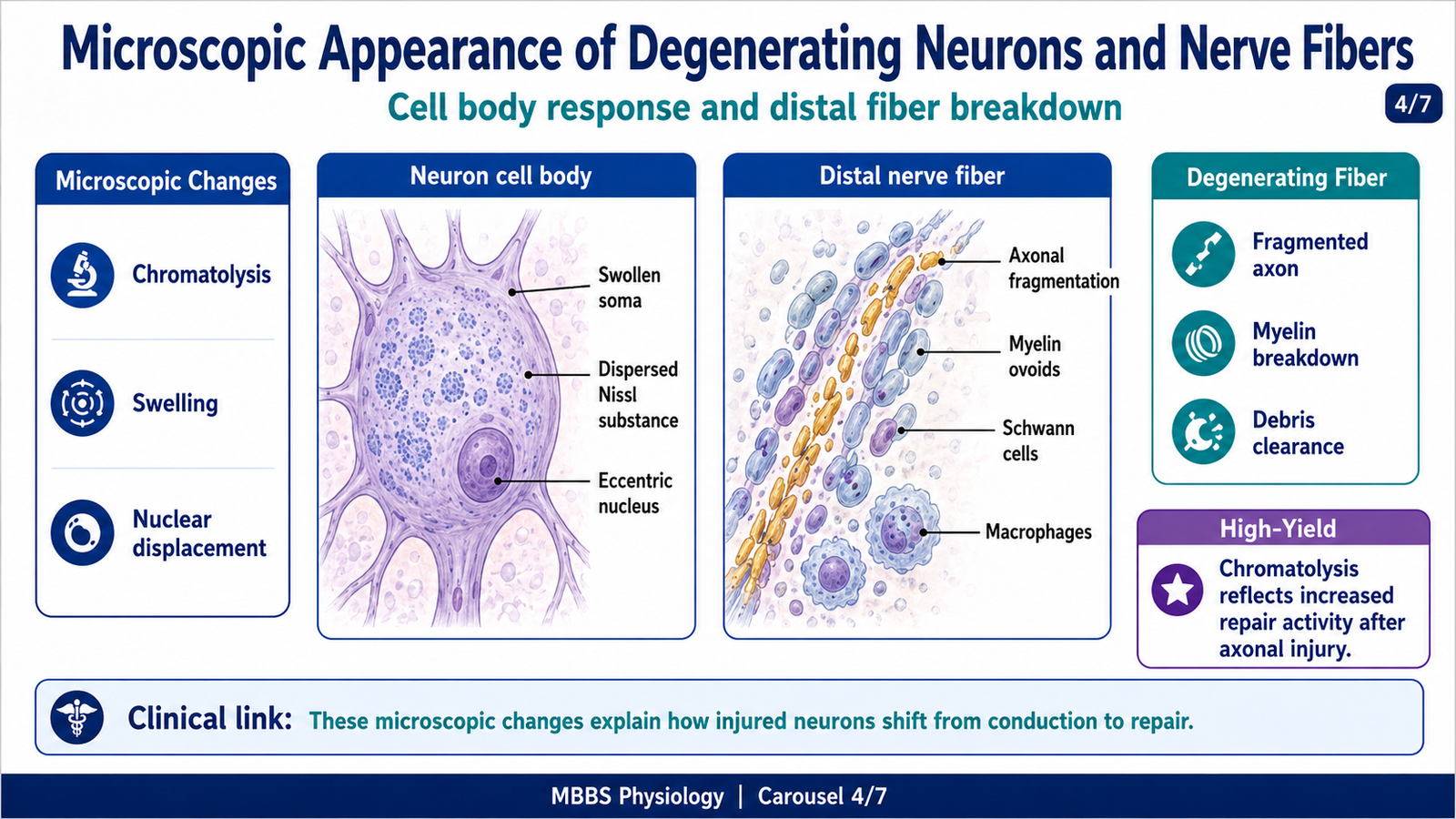
- Axonal injury produces changes in both the neuron cell body and injured nerve fiber.
- The neuronal cell body may show chromatolysis.
- Chromatolysis includes swelling of cell body, dispersion of Nissl substance, and eccentric nucleus.
- Distal axon fragments after separation from the cell body.
- Myelin breaks into ovoid fragments.
- Schwann cells proliferate and macrophages remove debris.
- Microscopic changes reflect increased repair activity and structural breakdown.
🔬 CONCEPT EXPLAINED
When a peripheral axon is injured, the neuron does not remain unchanged. The cell body must shift from its normal impulse-conducting role toward a repair and protein-synthesis role. The initiating event is axonal damage, especially when the injury is severe enough to interrupt axonal transport. The neuronal cell body senses this injury because normal communication between axon and soma is disturbed.
The major microscopic reaction of the cell body is chromatolysis. In chromatolysis, the cell body becomes swollen, the Nissl substance disperses, and the nucleus moves to an eccentric position. Nissl substance represents rough endoplasmic reticulum, which is involved in protein synthesis. Its dispersion does not mean the neuron is inactive; rather, it reflects reorganization of the cell body for increased production of proteins needed for repair and axonal growth.
The cause-effect relationship is important: axonal injury increases the demand for repair proteins; therefore, the cell body enlarges and reorganizes its synthetic machinery. If the injury is not too close to the cell body and the neuron survives, this reaction supports regeneration. If injury is very severe or close to the cell body, the neuron may die and regeneration cannot occur.
In the distal stump, the axon undergoes fragmentation because it has lost metabolic support from the cell body. The myelin sheath also breaks down into segments. Schwann cells detach from myelin, proliferate, and participate in debris clearance. Macrophages enter the area and remove remaining axonal and myelin debris. Microscopically, the degenerating nerve shows fragmented axons, myelin ovoids, proliferating Schwann cells, and inflammatory cleanup cells.
The functional outcome of these microscopic changes is preparation for regeneration. The cell body increases repair capacity, while the distal nerve stump is cleared and reorganized into a guiding pathway. If this process is effective, axonal sprouts can grow. If it fails, the nerve remains nonfunctional.
⚠️ CLINICAL IMPORTANCE
Chromatolysis indicates neuronal response to axonal injury. In peripheral nerve injury, it may be reversible if the neuron survives and regeneration succeeds. Persistent denervation leads to muscle wasting, loss of function, and poor recovery. Therefore, microscopic changes are not just histological facts; they explain the biological basis of clinical recovery or permanent deficit.
Nerve Regeneration in PNS and CNS
🧠 CORE
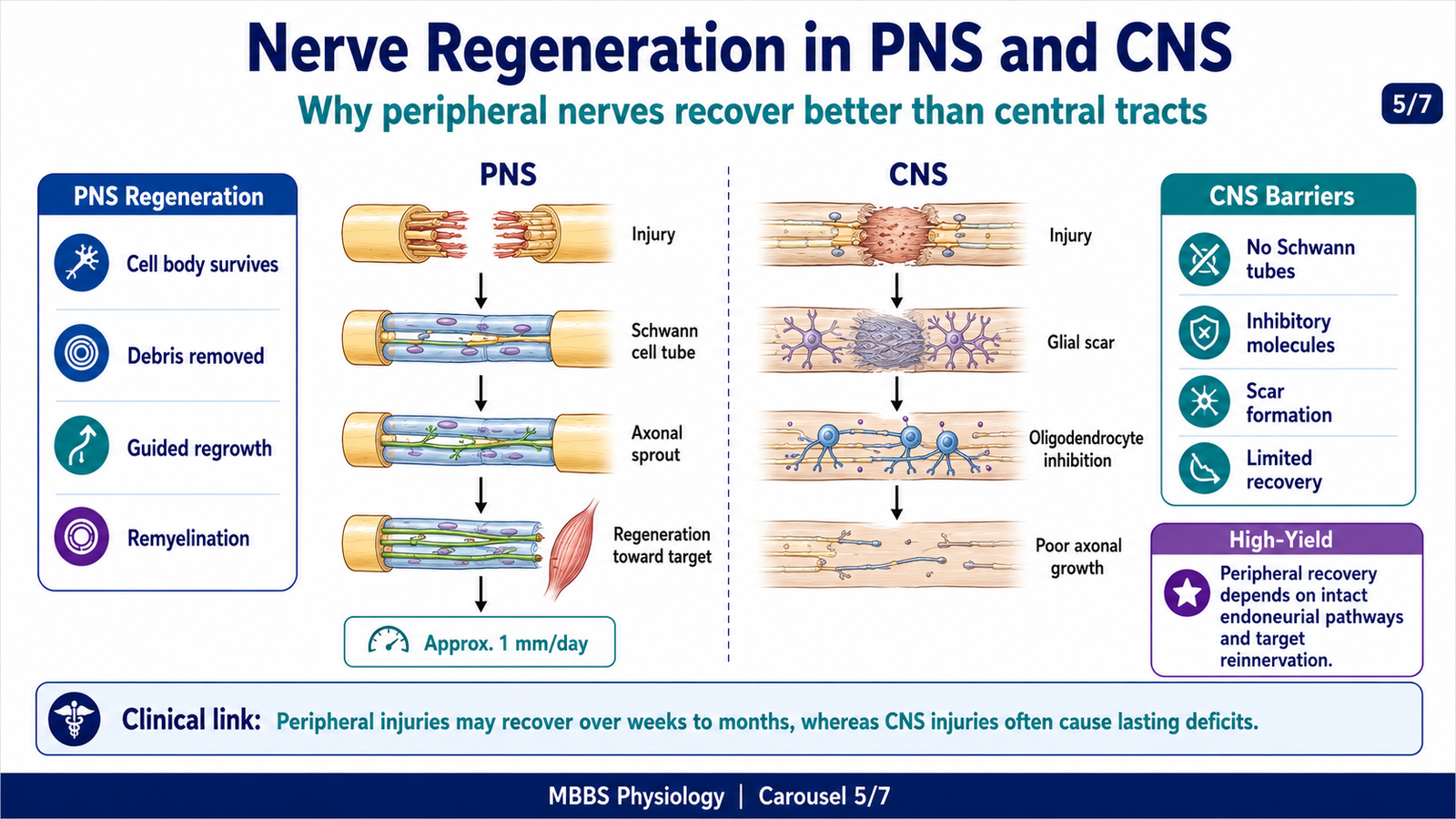
- Peripheral nerve regeneration is possible if the cell body survives and Schwann cell tubes remain intact.
- Regenerating axons grow from the proximal stump.
- Schwann cells guide axonal growth in the PNS.
- Typical peripheral axonal regeneration occurs at about 1 mm/day after regeneration begins.
- Functional recovery may require weeks to months depending on distance from target.
- CNS regeneration is very limited because oligodendrocytes, glial scar, and inhibitory molecules prevent effective regrowth.
- Recovery in CNS depends more on plasticity than true long-distance axonal regeneration.
🔬 CONCEPT EXPLAINED
Regeneration begins after degeneration has cleared the distal pathway. The initiating event is survival of the proximal neuron after axonal injury. If the cell body remains alive, it changes into a growth state. The purpose of regeneration is to restore connection between the neuron and its target tissue, such as muscle, skin receptor, or autonomic structure.
In the peripheral nervous system, regeneration follows a logical sequence. First, Wallerian degeneration removes the distal axon and myelin debris. Then Schwann cells proliferate and align inside the remaining endoneurial tubes. These Schwann cells form bands of Büngner, which act as biological guide channels. The proximal stump produces multiple axonal sprouts. Some sprouts enter the Schwann cell tubes and grow distally. Sprouts that fail to enter a proper pathway degenerate. Sprouts that successfully enter the pathway continue growing toward the target.
The growth rate in peripheral nerves is commonly about 1 mm/day after the growth pathway is established. Therefore, the duration required for recovery depends on the distance between the injury and the target tissue. If a nerve injury is close to a muscle, recovery may occur in weeks. If the injury is far from the target, such as a proximal limb nerve injury, recovery may take months. This is why distal recovery after proximal nerve injuries is slow.
Control and regulation of regeneration depend on Schwann cells, growth factors, extracellular matrix, macrophage activity, and neuronal protein synthesis. Schwann cells are central because they create a permissive pathway, support axonal growth, and later remyelinate the regenerated axon. Macrophages help by clearing debris that would otherwise block regeneration. The neuronal cell body must maintain increased protein synthesis to supply the growing axon.
The functional outcome of successful regeneration is partial or complete restoration of sensory, motor, or autonomic function. However, regenerated fibers may not become exactly normal. Myelin may be thinner, internodal distance may be shorter, and conduction velocity may remain reduced. If regenerating motor axons reach the wrong muscles or sensory axons reach abnormal skin areas, recovery may be imperfect.
The physiological advantage of PNS regeneration is preservation of function after injury. Without regeneration, every peripheral nerve injury would cause permanent loss. Schwann cell guidance allows the body to repair some nerve damage.
CNS regeneration is very different. In the brain and spinal cord, damaged axons usually do not regenerate effectively over long distances. The initiating injury may be trauma, ischemia, demyelination, or compression, but the CNS environment is not permissive for regrowth. Oligodendrocyte-associated inhibitory molecules, glial scar formation, lack of Schwann cell tubes, and complex CNS circuitry prevent effective axonal reconnection. Therefore, the duration required for true functional axonal regeneration inside the CNS is practically absent or extremely limited. Clinical recovery after CNS injury usually depends more on reduction of edema, remyelination in some conditions, synaptic plasticity, and compensation by other pathways rather than true long-distance regeneration.
⚠️ CLINICAL IMPORTANCE
Peripheral nerve injury may recover if axonal regeneration reaches the target in time. However, prolonged denervation causes irreversible muscle atrophy and fibrosis, reducing recovery even if the axon later reaches the muscle. CNS injury, such as spinal cord tract damage, usually causes permanent deficits because true regeneration is poor.
Etiology and Types of Peripheral Neuropathies
🧠 CORE
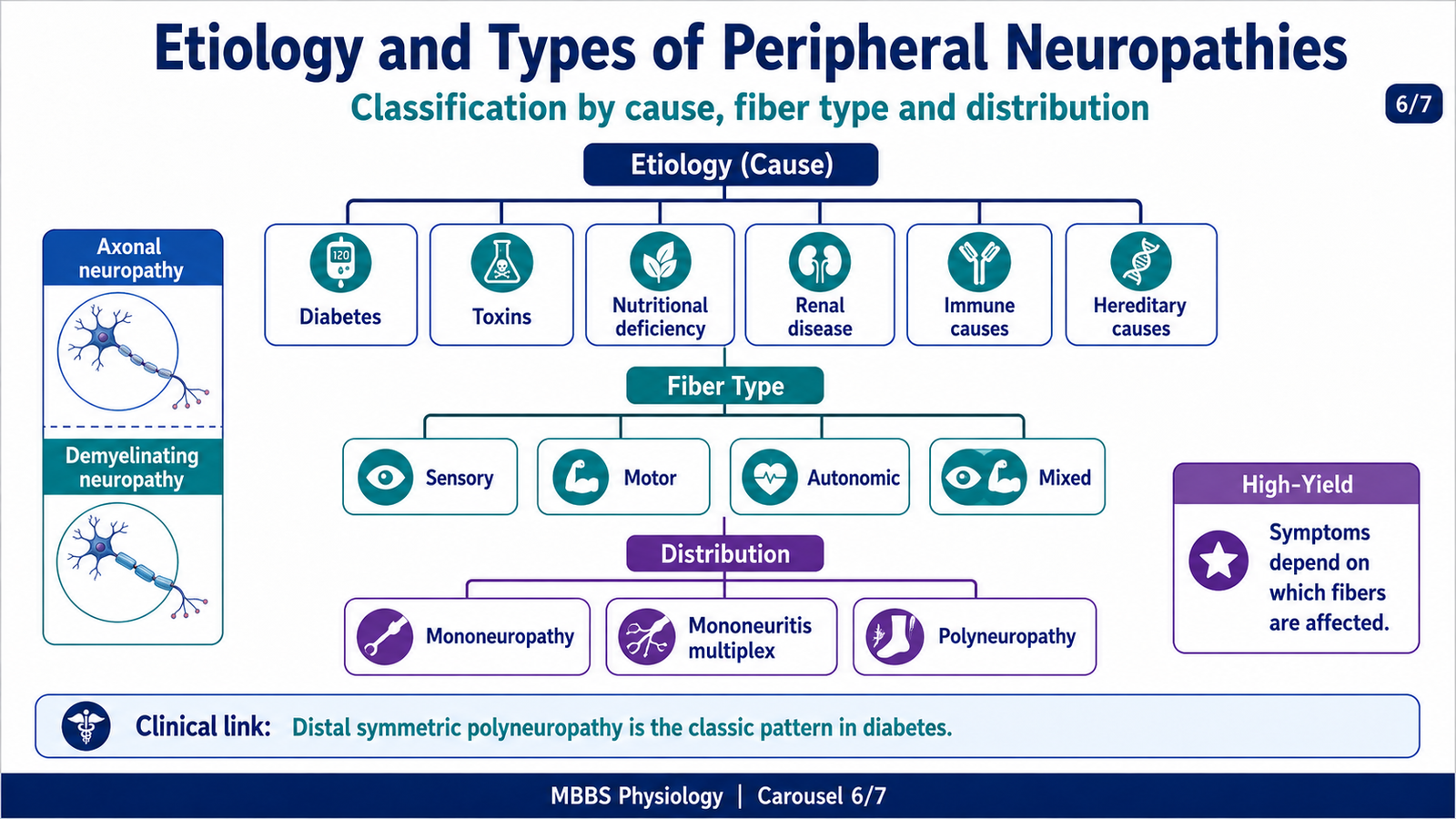
- Peripheral neuropathy means dysfunction of peripheral nerves.
- It may be sensory, motor, autonomic, or mixed.
- It may affect one nerve, many individual nerves, or many nerves symmetrically.
- Common causes include diabetes, toxins, nutritional deficiency, renal disease, autoimmune disease, infections, and hereditary disorders.
- Axonal neuropathy damages the axon.
- Demyelinating neuropathy damages myelin.
- Symptoms depend on fiber type and distribution.
🔬 CONCEPT EXPLAINED
Peripheral neuropathy develops when peripheral nerves lose normal structure or function. The initiating event may be metabolic, toxic, inflammatory, ischemic, compressive, hereditary, or infectious. The body needs peripheral nerves for sensation, movement, reflexes, autonomic regulation, and protective responses. When these nerves fail, the patient loses communication between the CNS and the body tissues.
Neuropathies can be classified by the type of fiber involved. Sensory neuropathy affects sensory fibers and produces numbness, tingling, burning pain, reduced vibration sense, reduced proprioception, or loss of pain and temperature sensation. Motor neuropathy affects motor fibers and produces weakness, reduced reflexes, cramps, fasciculations, and muscle wasting. Autonomic neuropathy affects autonomic fibers and may cause postural hypotension, abnormal sweating, gastrointestinal motility problems, bladder dysfunction, and sexual dysfunction. Mixed neuropathy affects more than one fiber type and is common in systemic diseases.
Neuropathies can also be classified by distribution. Mononeuropathy affects a single nerve, such as median nerve compression in carpal tunnel syndrome. Mononeuritis multiplex affects multiple individual nerves in an asymmetric pattern, often due to vasculitis or ischemic injury. Polyneuropathy affects many peripheral nerves, usually symmetrically and often distally. Diabetic neuropathy commonly presents as distal symmetric polyneuropathy.
Another important classification is axonal versus demyelinating neuropathy. In axonal neuropathy, the main injury is to the axon. Since the axon is the conducting core, loss of axons reduces the strength of nerve signals and produces sensory loss or weakness. Long axons are affected first, so symptoms begin in the feet. In demyelinating neuropathy, the myelin sheath is primarily damaged. Because myelin is essential for rapid conduction, demyelination slows nerve conduction and may produce conduction block. If demyelination is severe or prolonged, secondary axonal damage may occur.
⚠️ CLINICAL IMPORTANCE
Clinical presentation depends on which fibers are affected. Loss of sensory fibers may cause painless injuries because the patient cannot feel trauma. Motor involvement causes weakness and wasting. Autonomic involvement may cause postural dizziness, constipation, diarrhea, urinary problems, or erectile dysfunction. In exams, students should connect symptoms to fiber type and distribution rather than memorize neuropathy names only.
Diabetic Neuropathy
🧠 CORE
- Diabetic neuropathy is nerve damage caused by chronic diabetes mellitus.
- It commonly presents as distal symmetric sensory polyneuropathy.
- Long nerves of the feet are affected first.
- Mechanisms include hyperglycemia-induced metabolic injury, oxidative stress, microvascular ischemia, and impaired axonal transport.
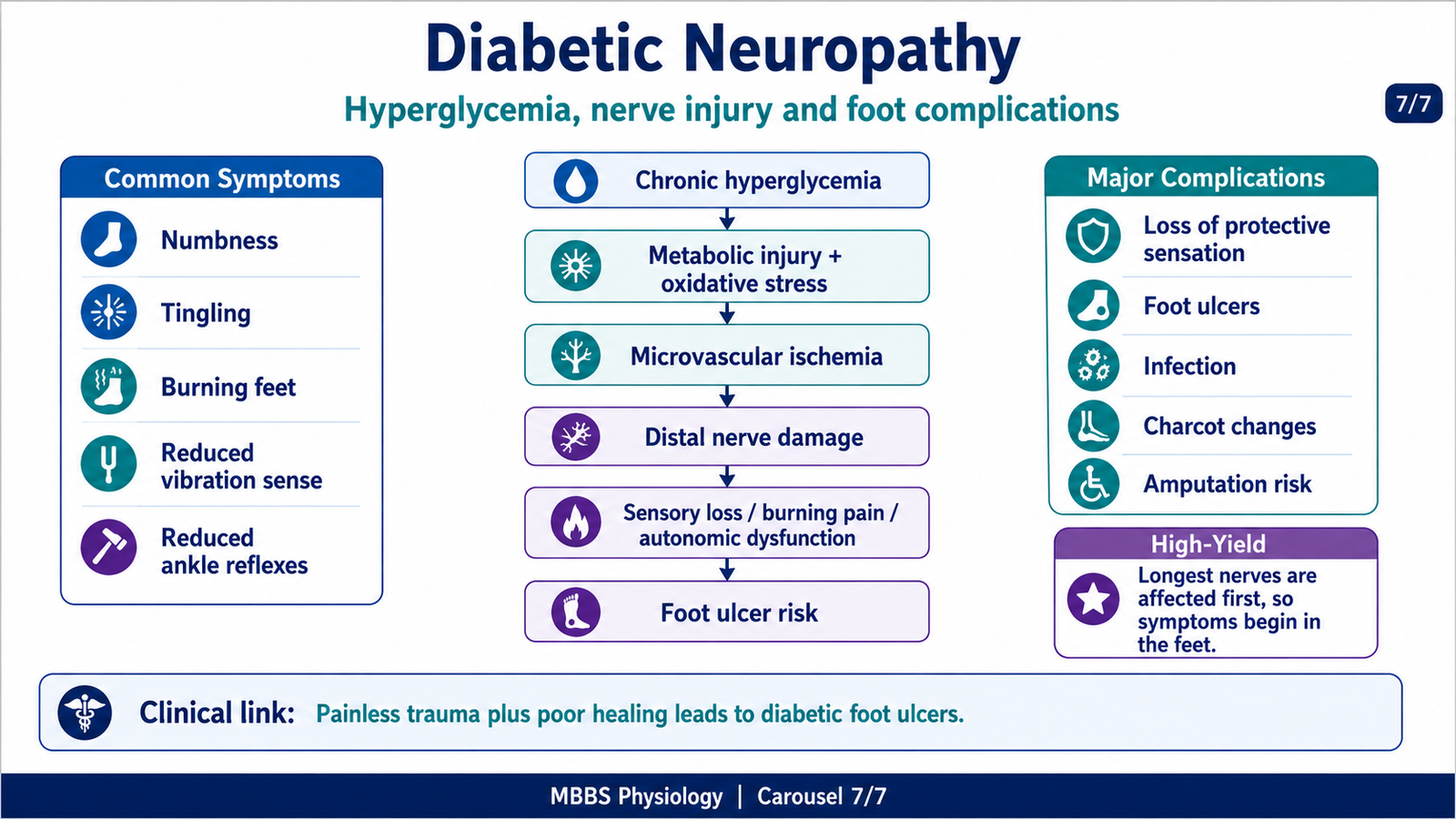
- Sensory symptoms include numbness, burning pain, tingling, and loss of protective sensation.
- Motor involvement may cause weakness and wasting in advanced disease.
- Autonomic neuropathy may affect cardiovascular, gastrointestinal, urinary, sweating, and sexual functions.
- Major complications include foot ulcers, infections, deformity, and amputation risk.
🔬 CONCEPT EXPLAINED
Diabetic neuropathy begins with chronic hyperglycemia. The initiating event is prolonged elevation of blood glucose, which exposes peripheral nerves and their blood vessels to metabolic stress. The purpose of normal glucose regulation is to provide energy without damaging tissues. When glucose remains chronically high, excess glucose enters alternative metabolic pathways, increases oxidative stress, damages small blood vessels, and impairs neuronal metabolism.
The sequence starts with persistent hyperglycemia causing increased intracellular glucose in nerve cells and Schwann cells. This leads to formation of sorbitol through the polyol pathway, oxidative stress, advanced glycation end-products, and disturbed cellular metabolism. These changes reduce normal axonal transport and damage Schwann cell function. At the same time, diabetes damages small blood vessels supplying nerves. Microvascular disease reduces oxygen delivery, producing chronic nerve ischemia. Therefore, diabetic neuropathy is both metabolic and ischemic.
The cause-effect relationship is clinically important. Hyperglycemia damages nerve metabolism and microcirculation; damaged metabolism and ischemia impair axonal function; impaired axonal function first affects the longest nerves; therefore, symptoms begin in the toes and feet. As disease progresses, symptoms ascend upward in a stocking distribution and may later involve the hands in a glove pattern.
Control and regulation depend mainly on blood glucose control, vascular health, and neuronal repair capacity. If hyperglycemia continues, nerve injury progresses. If glucose control improves early, progression may slow. However, established axonal loss may not fully reverse because damaged long axons regenerate slowly and may not completely recover.
The functional outcome of diabetic neuropathy is loss of normal sensory, motor, and autonomic communication. Sensory fiber damage causes numbness, tingling, burning pain, or loss of pain and temperature sensation. Loss of protective sensation is dangerous because the patient may not feel minor trauma, tight shoes, burns, or ulcers. Motor fiber damage weakens small foot muscles, contributing to deformity and abnormal pressure points. Autonomic fiber damage reduces sweating and alters blood flow, causing dry cracked skin and poor healing.
The physiological advantage of intact peripheral sensation is protection. Pain, pressure, and temperature warn the body about injury. In diabetic neuropathy, this protective system fails. As a result, small injuries may progress to ulcers, infections, gangrene, and amputation risk.
⚠️ CLINICAL IMPORTANCE
Diabetic neuropathy commonly presents with burning feet, numbness, tingling, reduced vibration sense, reduced ankle reflexes, and loss of protective sensation. Complications include foot ulcers, infection, Charcot joint, falls due to sensory loss, autonomic dysfunction, and increased risk of amputation. For MBBS exams, the key concept is: chronic hyperglycemia → metabolic injury + microvascular ischemia → distal axonal dysfunction → stocking-glove sensory loss → painless injury and foot ulceration.

⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Peripheral Nerve Structure → Fast and Accurate Communication
Peripheral nerves contain axons, myelin, Schwann cells, and connective tissue sheaths. Axons conduct impulses, myelin increases conduction speed, Schwann cells support and repair fibers, and connective tissue preserves nerve architecture. Therefore, normal structure allows rapid motor control, accurate sensation, reflex activity, and autonomic regulation.
Schwann Cells → Regeneration → Functional Recovery
Schwann cells are not only myelin-forming cells. After injury, they become repair cells. They remove debris, proliferate, produce growth-supporting factors, and form guiding tubes. Therefore, Schwann cells explain why peripheral nerves can regenerate better than CNS tracts.
Axonal Transport → Neuronal Survival → Distal Nerve Integrity
The distal axon depends on the neuronal cell body for proteins and metabolic support. If axonal continuity is lost, the distal segment degenerates. Therefore, Wallerian degeneration is the direct structural consequence of interrupted axonal transport.
Blood Supply → Nerve Metabolism → Neuropathy Risk
Peripheral nerves require oxygen and nutrients. If blood supply is compromised, nerve metabolism fails. In diabetes, microvascular disease reduces nerve perfusion, producing chronic ischemic damage. Therefore, vascular injury is an important cause of neuropathy.
Sensory Fibers → Protective Sensation → Prevention of Injury
Pain, pressure, vibration, and temperature sensation protect the body. When diabetic neuropathy damages sensory fibers, the patient may not feel trauma. Therefore, painless ulcers can develop, especially in the feet.
🩺 5️⃣ Clinical Correlation
Peripheral Nerve Injury
Peripheral nerve injury may occur due to trauma, fractures, compression, laceration, injections, tumors, or prolonged pressure. If motor fibers are damaged, the patient develops weakness and loss of reflexes. If sensory fibers are damaged, numbness, tingling, or pain occurs. If autonomic fibers are involved, sweating and vascular control may be altered.
The severity of injury determines recovery. Mild myelin injury may recover quickly. Axonal injury requires Wallerian degeneration and regeneration, so recovery is slow. Complete nerve transection has poor recovery unless the nerve ends are aligned because regenerating axons need a pathway.
Foot Drop as an Example of Motor Nerve Dysfunction
Foot drop occurs when dorsiflexion of the foot is weak, commonly due to injury of the common peroneal nerve or its branches. The patient cannot lift the front of the foot properly while walking. As a result, the toes may drag on the ground, and the patient develops a high-stepping gait. This illustrates the principle that motor nerve injury causes weakness in muscles supplied by that nerve.
Diabetic Distal Symmetric Polyneuropathy
This is the commonest pattern of diabetic neuropathy. It begins in the toes and feet because the longest nerves are most vulnerable. Symptoms include burning pain, numbness, tingling, reduced vibration sense, reduced ankle reflexes, and loss of protective sensation. The major danger is that the patient may develop painless injuries and ulcers.
Diabetic Autonomic Neuropathy
Autonomic fiber damage may cause postural hypotension, resting tachycardia, gastroparesis, constipation, diarrhea, bladder dysfunction, erectile dysfunction, and abnormal sweating. The underlying mechanism is failure of autonomic control of blood vessels, heart, gastrointestinal tract, bladder, and glands.
Clinical Complications of Diabetic Neuropathy
Diabetic neuropathy can lead to foot ulcers because sensory loss prevents pain warning. Motor neuropathy may cause foot muscle imbalance and deformity, increasing pressure points. Autonomic neuropathy reduces sweating, causing dry cracked skin. Microvascular disease reduces healing. Together, these factors increase risk of infection, gangrene, and amputation.
📌 6️⃣ Summary Points
- Peripheral nerves regenerate better than CNS tracts because Schwann cells form guiding pathways.
- Wallerian degeneration affects the distal axon after separation from the neuronal cell body.
- Distal axon degenerates because it loses axonal transport and metabolic support.
- Chromatolysis shows neuronal cell body response to axonal injury: swelling, dispersed Nissl substance, and eccentric nucleus.
- Peripheral axonal regeneration occurs at about 1 mm/day after regeneration begins.
- Recovery duration depends on distance from injury site to target organ.
- CNS regeneration is poor because of inhibitory molecules, glial scar, and lack of Schwann cell tubes.
- Axonal neuropathy mainly reduces nerve signal strength; demyelinating neuropathy mainly slows conduction.
- Diabetic neuropathy is due to metabolic injury plus microvascular ischemia.
- Diabetic neuropathy commonly begins in feet because the longest nerves are affected first.
- Loss of protective sensation in diabetes leads to painless trauma, ulcers, infection, and amputation risk.
- Always relate neuropathy symptoms to fiber type: sensory, motor, or autonomic.