
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
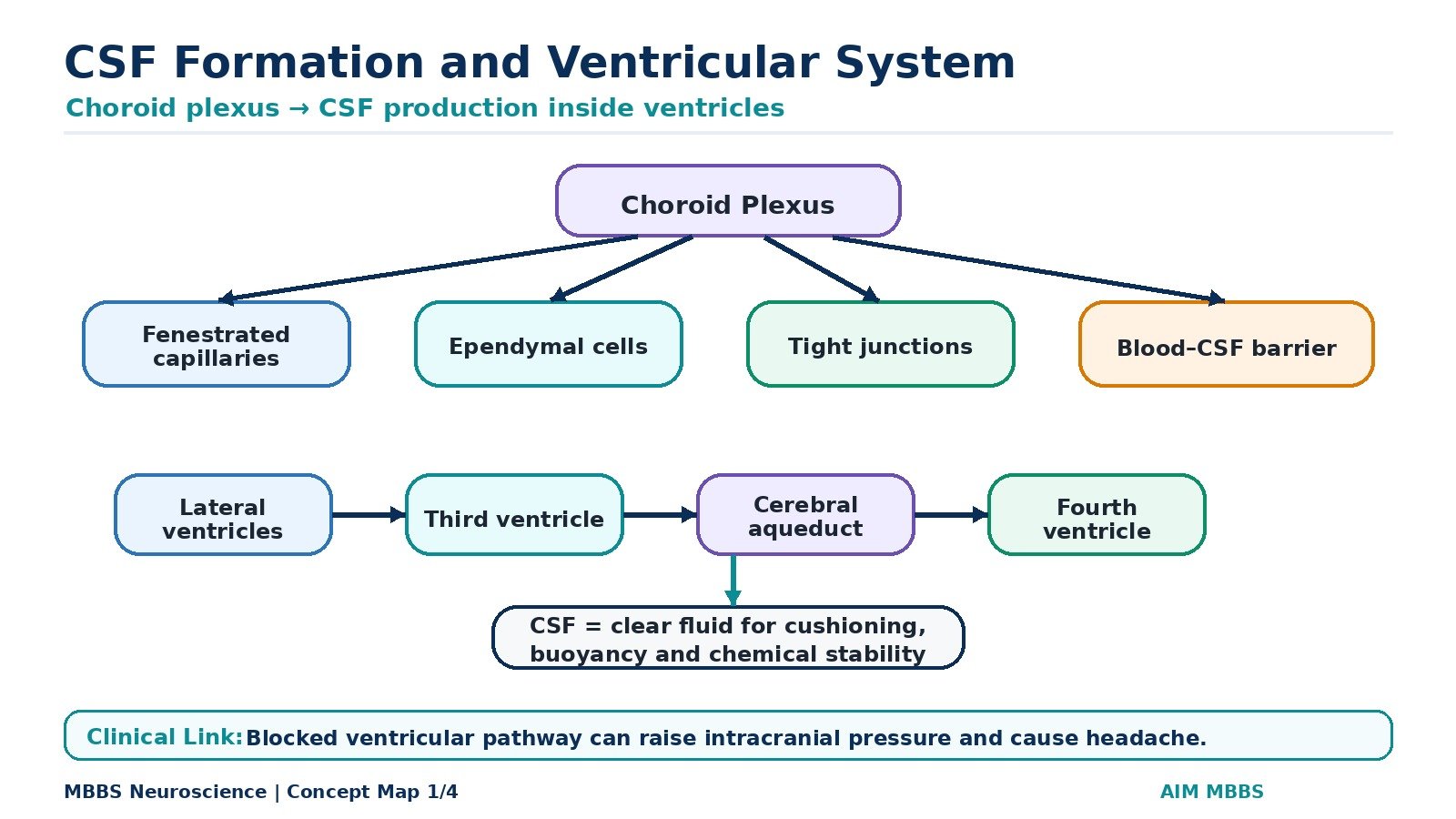
Cerebrospinal fluid, or CSF, is a clear fluid that surrounds and supports the brain and spinal cord. It is produced mainly by the choroid plexus inside the ventricles of the brain and circulates through the ventricular system, subarachnoid space, and around the spinal cord.
This topic is important because CSF maintains a stable environment for neurons, protects the brain from mechanical injury, helps remove metabolic waste, and reflects biochemical changes occurring in the central nervous system.
The ventricular system forms the internal CSF pathway of the brain, while the blood–brain barrier and blood–CSF barrier regulate what substances can enter the nervous tissue and CSF.
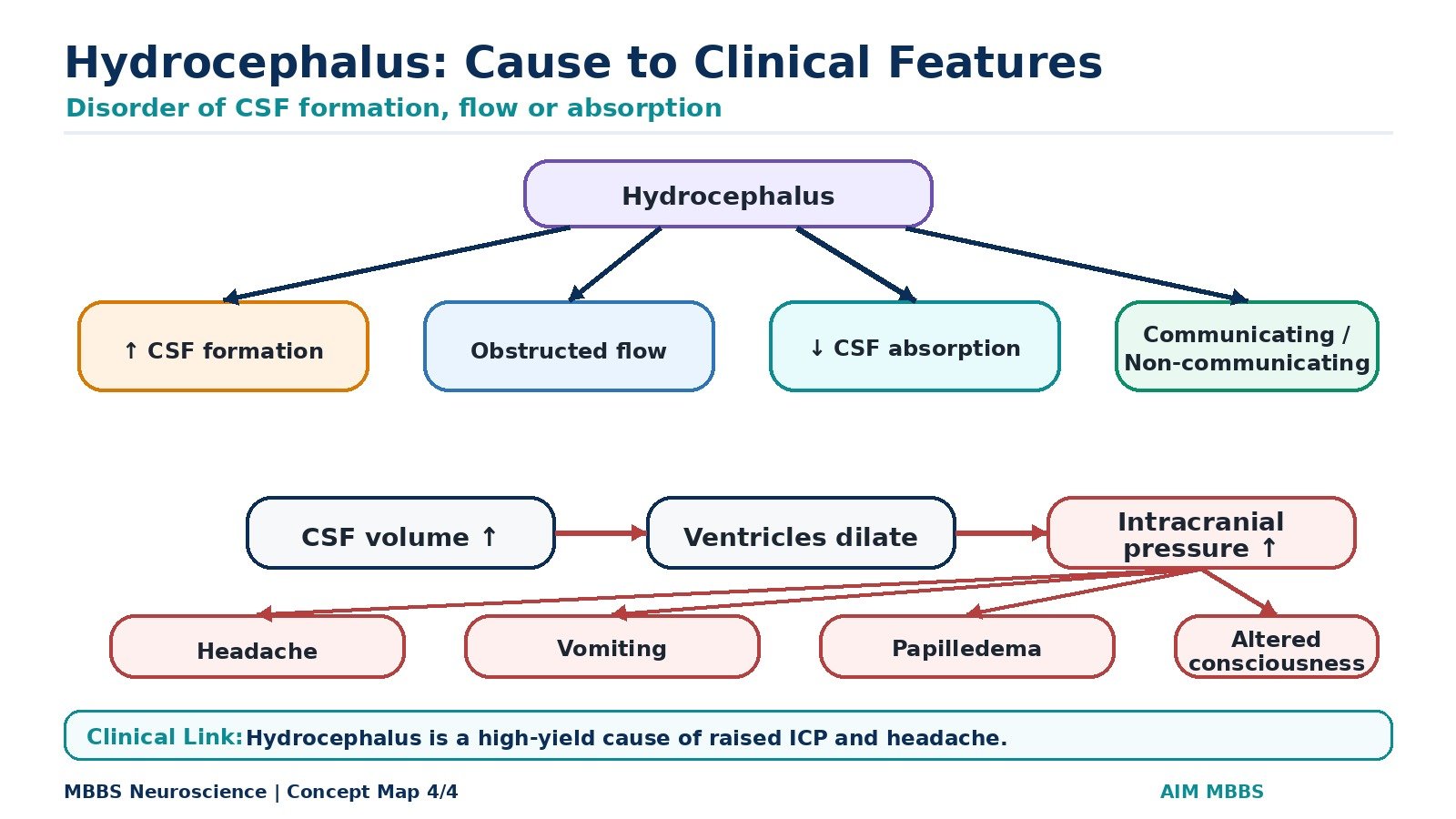
Clinically, disturbance of CSF formation, flow, or absorption can lead to hydrocephalus and raised intracranial pressure. Raised intracranial pressure is an important cause of headache and may produce vomiting, papilledema, altered consciousness, and neurological signs.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Cerebrospinal fluid (CSF): Clear, colorless fluid present in the ventricles, subarachnoid space, and central canal of spinal cord.
- Ventricular system: Interconnected cavities inside the brain through which CSF circulates.
- Choroid plexus: Highly vascular structure covered by specialized ependymal cells responsible for CSF formation.
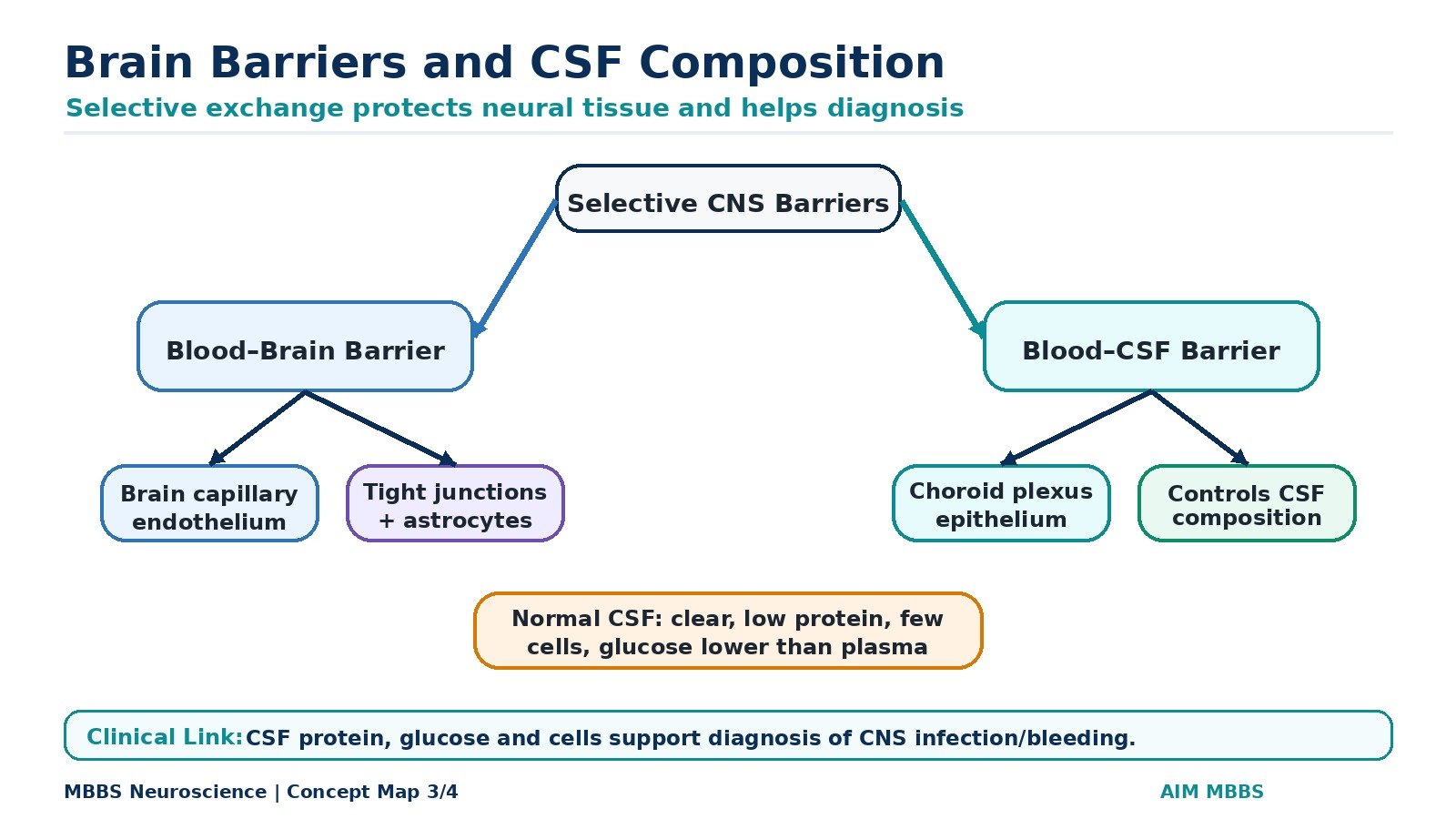
- Blood–brain barrier (BBB): Barrier between blood and brain extracellular fluid that protects neurons from harmful substances.
- Blood–CSF barrier: Barrier between blood and CSF formed mainly at the choroid plexus epithelium.
- Hydrocephalus: Abnormal accumulation of CSF due to increased formation, obstruction to flow, or impaired absorption.
- Raised intracranial pressure (ICP): Increased pressure inside the cranial cavity due to increased brain volume, blood volume, or CSF volume.
Essential Terminology
- Lateral ventricles: Paired ventricles present in cerebral hemispheres.
- Third ventricle: Midline cavity in the diencephalon.
- Cerebral aqueduct: Narrow canal connecting third and fourth ventricles.
- Fourth ventricle: Cavity between brainstem and cerebellum.
- Foramina of Monro: Connect lateral ventricles with third ventricle.
- Foramen of Magendie: Median opening from fourth ventricle to subarachnoid space.
- Foramina of Luschka: Lateral openings from fourth ventricle to subarachnoid space.
- Arachnoid villi/granulations: Structures through which CSF is absorbed into venous blood.
Basic Overview
- CSF is formed mainly by the choroid plexus.
- CSF flows from ventricles into the subarachnoid space.
- CSF is absorbed mainly through arachnoid villi into dural venous sinuses.
- The BBB protects brain tissue from toxins and large molecules.
- The blood–CSF barrier regulates the composition of CSF.
- CSF composition is clinically useful in meningitis, hemorrhage, and other CNS disorders.
- Hydrocephalus occurs when CSF production, flow, or absorption becomes abnormal.
🔹 3️⃣ Core Learning — Curriculum Coverage
1 — Ventricular System and Anatomical Pathway of CSF
🧠 CORE
- The ventricular system is a series of interconnected cavities inside the brain.
- It consists of two lateral ventricles, third ventricle, cerebral aqueduct, and fourth ventricle.
- CSF is formed mainly inside ventricles by the choroid plexus.
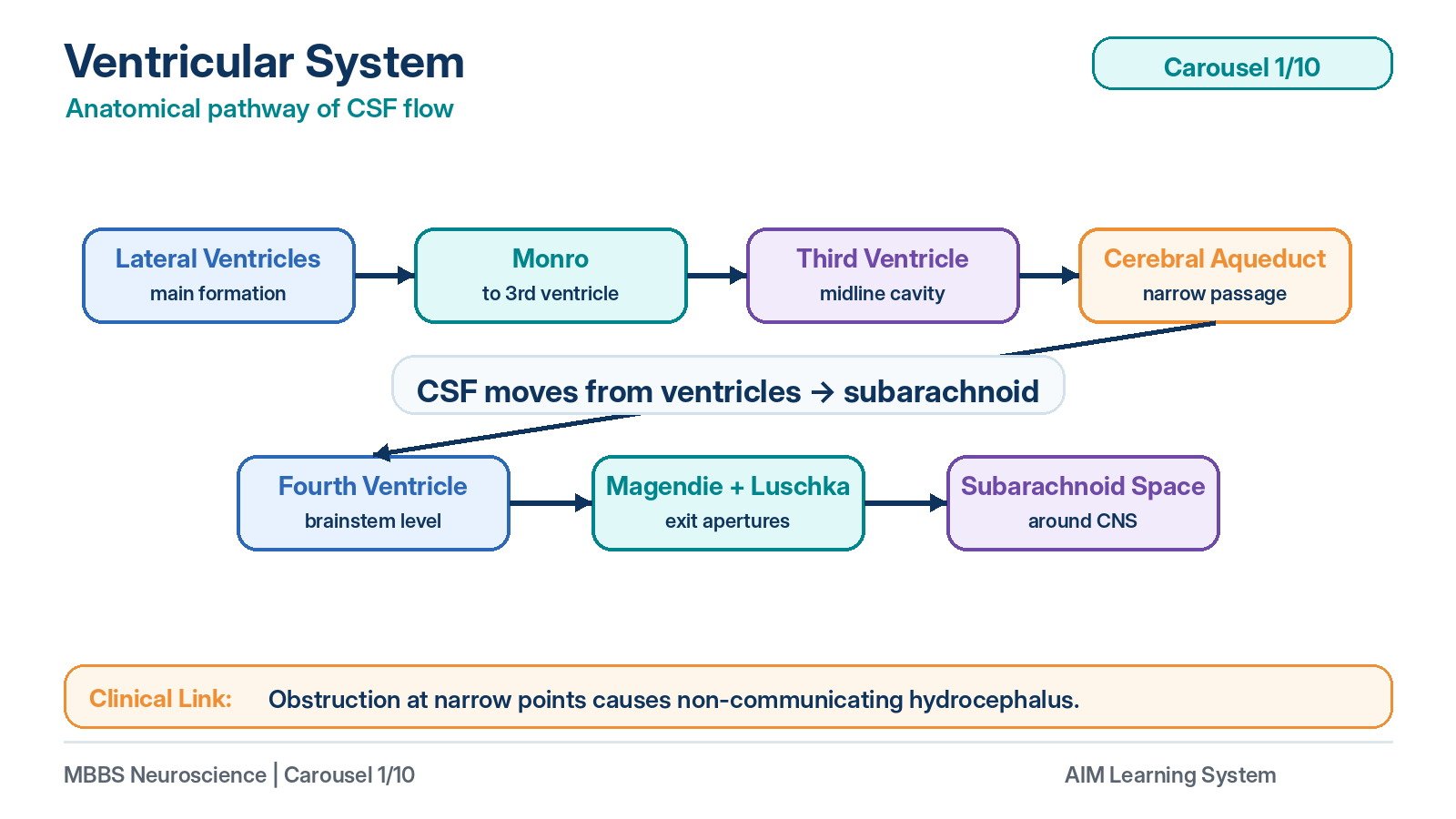
- CSF flows from lateral ventricles to third ventricle through foramina of Monro.
- From the third ventricle, CSF passes through the cerebral aqueduct to the fourth ventricle.
- CSF leaves the fourth ventricle through the median and lateral apertures.
- It then circulates in the subarachnoid space around brain and spinal cord.
- Narrow points such as the cerebral aqueduct are common sites of obstruction.
🔬 CONCEPT EXPLAINED
To understand CSF physiology, first understand its anatomical pathway. The brain contains internal cavities called ventricles, which are lined by ependymal cells and filled with CSF. These ventricles are not isolated spaces; they are connected in a continuous pathway that allows CSF to move from its site of formation to its site of absorption.
CSF is produced mainly in the lateral ventricles, where choroid plexus is abundant. From each lateral ventricle, CSF passes through the interventricular foramen of Monro into the third ventricle. The third ventricle lies in the midline between the two halves of the diencephalon. From here, CSF flows through the cerebral aqueduct of Sylvius, a narrow canal in the midbrain, into the fourth ventricle.
The fourth ventricle lies between the brainstem anteriorly and cerebellum posteriorly. From the fourth ventricle, CSF exits into the subarachnoid space through one median aperture, called the foramen of Magendie, and two lateral apertures, called the foramina of Luschka. After entering the subarachnoid space, CSF circulates around the brain and spinal cord.
This anatomical arrangement is clinically important because obstruction at any point blocks CSF movement. For example, obstruction of the cerebral aqueduct prevents CSF from leaving the third and lateral ventricles. As a result, CSF accumulates above the obstruction, causing ventricular dilatation and hydrocephalus.
⚠️ CLINICAL IMPORTANCE
Obstruction within the ventricular system causes non-communicating hydrocephalus. Common obstruction sites include the cerebral aqueduct and outlets of the fourth ventricle. Because the skull is rigid, accumulation of CSF increases intracranial pressure, which can produce headache, vomiting, papilledema, and altered consciousness.
2 — Structure of Choroid Plexus and Formation of CSF
🧠 CORE
- The choroid plexus is a vascular structure present in ventricles.
- It is formed by capillaries covered by specialized ependymal cells.
- It is the main site of CSF production.
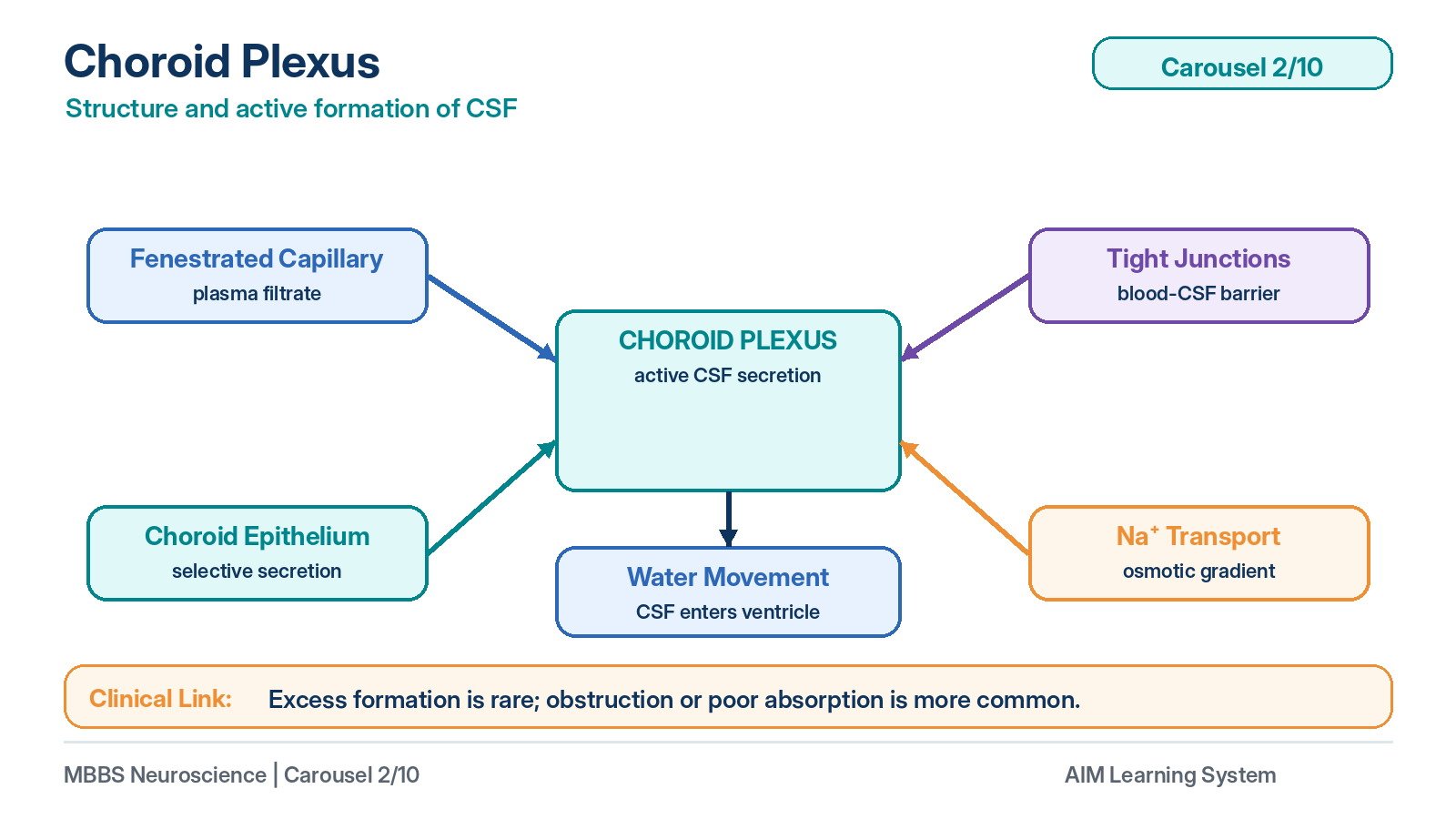
- Its capillaries are fenestrated, allowing plasma filtration.
- Tight junctions between choroid epithelial cells form the blood–CSF barrier.
- CSF formation is an active secretory process, not simple filtration only.
- Sodium transport is central to CSF formation.
- Water follows osmotic gradients into the ventricles.
🔬 CONCEPT EXPLAINED
The choroid plexus is the major anatomical and physiological structure responsible for CSF formation. It projects into the ventricles as vascular folds covered by modified ependymal cells called choroid epithelial cells. Under these cells lie rich capillary networks. These capillaries are fenestrated, meaning they allow many plasma components to pass out of the blood easily. However, the final entry of substances into CSF is controlled by the choroid epithelial cells.
CSF formation begins when plasma is filtered from choroid plexus capillaries into the connective tissue core of the choroid plexus. However, this filtrate does not become CSF directly. It must pass through the choroid epithelial cells, which actively regulate its composition. These epithelial cells contain transport systems that move sodium ions into the ventricular cavity. Chloride and bicarbonate also contribute to osmotic balance. As sodium and other solutes move into the ventricular cavity, water follows by osmosis, producing CSF.
Therefore, CSF formation is mainly an active secretory process. This is important because the body does not simply allow plasma to leak into the ventricles. Instead, it creates a special fluid with low protein content, controlled electrolyte composition, and a stable chemical environment suitable for brain function.
The choroid plexus also forms the blood–CSF barrier. Although choroid capillaries are leaky, tight junctions between choroid epithelial cells prevent free movement of substances from blood into CSF. This means the final composition of CSF is carefully regulated.
⚠️ CLINICAL IMPORTANCE
Excessive CSF formation is a rare cause of hydrocephalus, but it may occur in choroid plexus tumors. More commonly, hydrocephalus occurs due to obstruction of CSF flow or impaired absorption. The choroid plexus is also clinically important because infection, inflammation, or hemorrhage can alter CSF composition.
3 — Normal Flow and Absorption of CSF
🧠 CORE
- CSF flows from lateral ventricles to third ventricle, fourth ventricle, and subarachnoid space.
- CSF circulates around the brain and spinal cord.
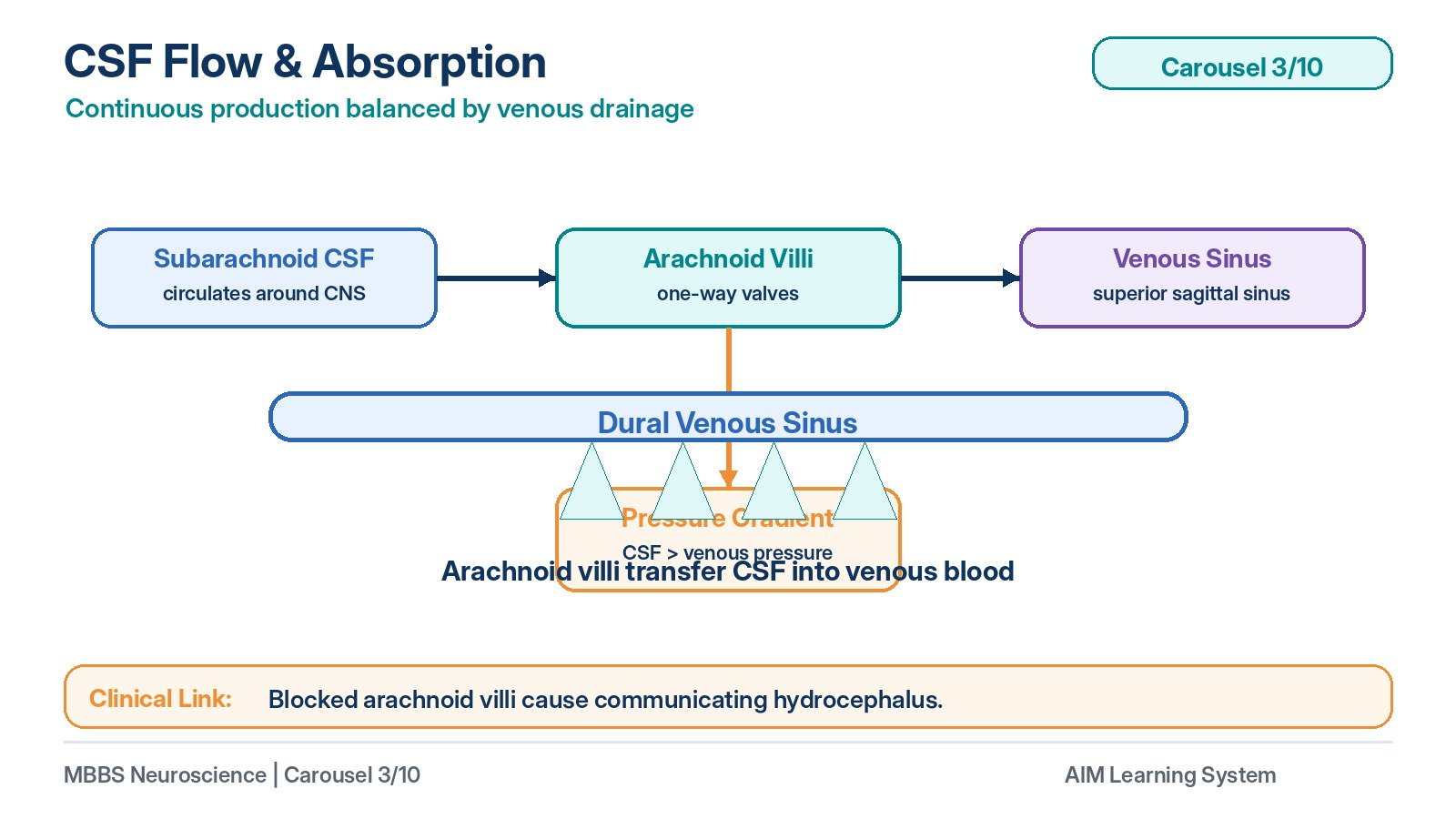
- CSF is absorbed mainly through arachnoid villi and granulations.
- Absorption occurs into dural venous sinuses, especially the superior sagittal sinus.
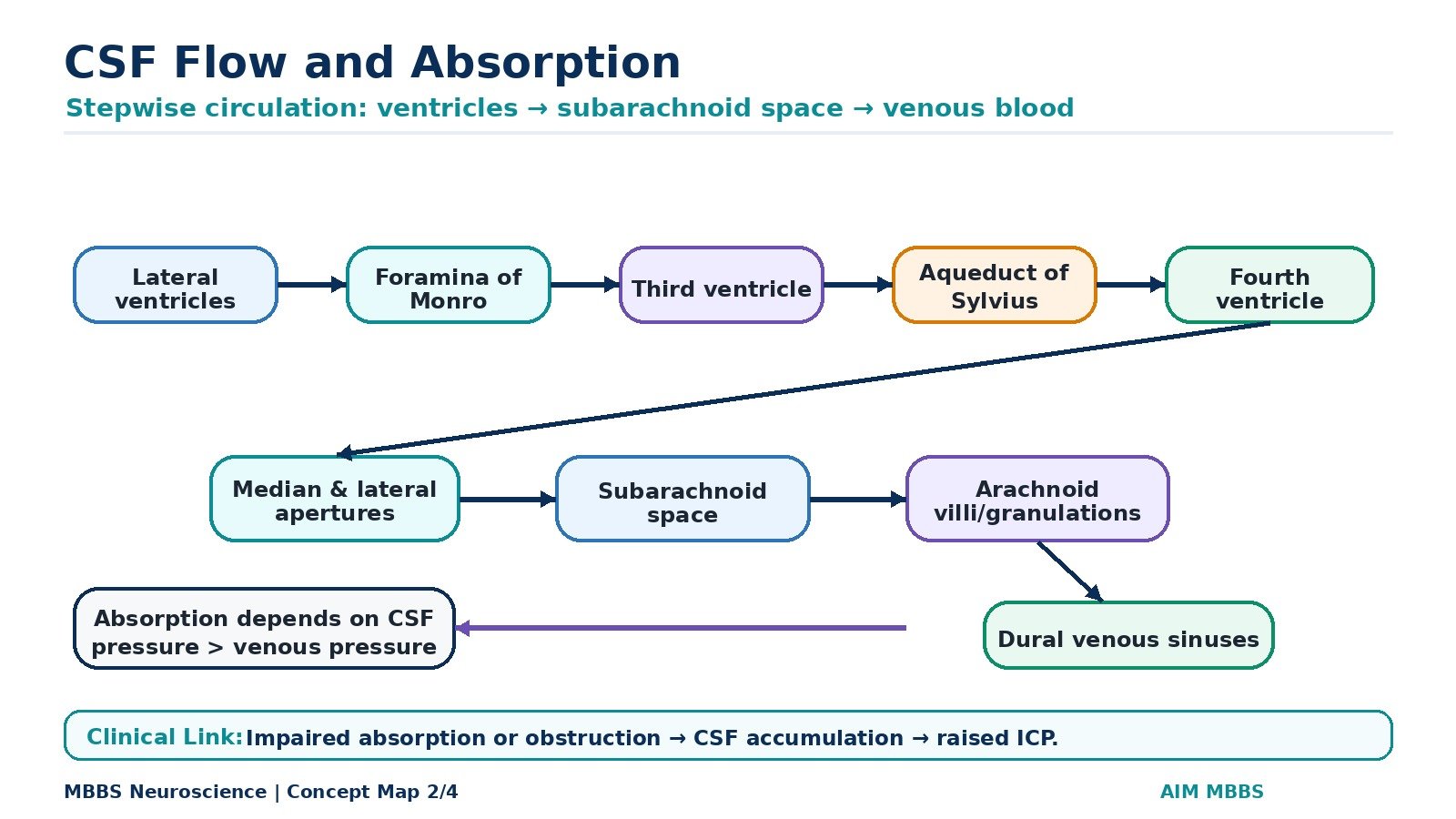
- CSF absorption depends on pressure gradient between CSF and venous blood.
- CSF is continuously produced and continuously absorbed.
- Balance between formation and absorption maintains normal CSF volume and pressure.
- Failure of absorption causes communicating hydrocephalus.
🔬 CONCEPT EXPLAINED
After CSF is produced in the ventricles, it must circulate and then return to the bloodstream. This circulation is essential because CSF is continuously formed. If it were produced without absorption, intracranial pressure would rise rapidly.
The flow begins in the lateral ventricles, passes through the foramina of Monro into the third ventricle, then through the cerebral aqueduct into the fourth ventricle. From the fourth ventricle, CSF exits through the foramina of Magendie and Luschka into the subarachnoid space. Once in the subarachnoid space, CSF surrounds the brain and spinal cord. This gives the central nervous system buoyancy and mechanical protection.
CSF is absorbed mainly through arachnoid villi and arachnoid granulations. These are projections of arachnoid mater into dural venous sinuses, especially the superior sagittal sinus. They act like one-way valves. When CSF pressure is higher than venous pressure, CSF passes into venous blood. If venous pressure becomes high, or if arachnoid villi are blocked by fibrosis, blood, or inflammation, CSF absorption decreases.
This pressure-dependent absorption is physiologically useful. It allows CSF drainage to increase when CSF pressure rises, helping maintain normal intracranial pressure. However, if absorption mechanisms fail, CSF accumulates throughout the ventricular and subarachnoid system.
⚠️ CLINICAL IMPORTANCE
Failure of CSF absorption causes communicating hydrocephalus because the ventricles still communicate with the subarachnoid space, but CSF cannot be absorbed properly. This may occur after meningitis or subarachnoid hemorrhage due to blockage or scarring of arachnoid villi.
4 — Functions of CSF
🧠 CORE
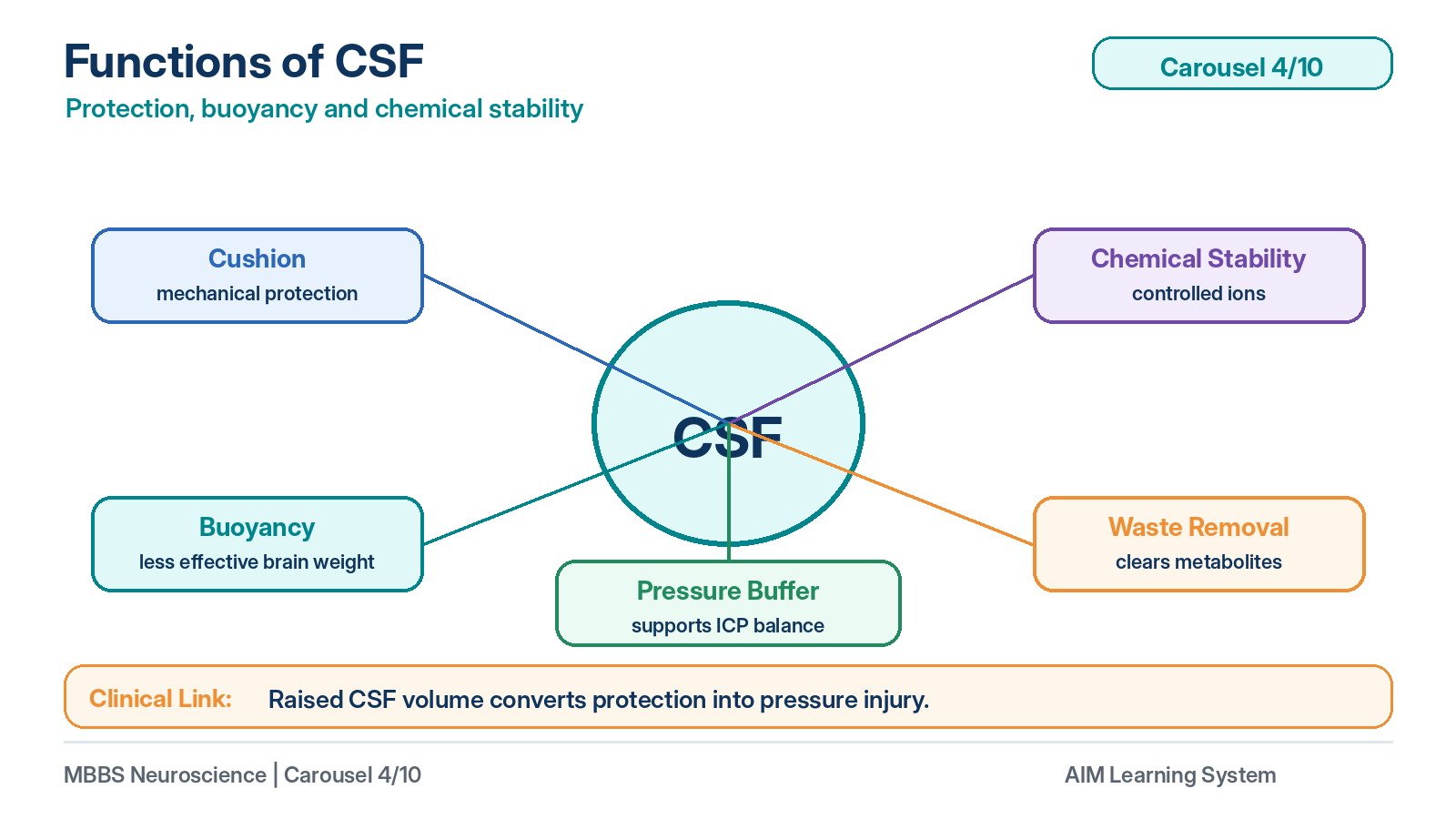
- CSF provides mechanical protection to the brain and spinal cord.
- It gives buoyancy to the brain and reduces effective brain weight.
- It maintains a stable extracellular environment for neurons.
- It helps remove metabolic waste products.
- It transports some signaling molecules.
- It acts as a buffer against sudden changes in intracranial volume.
- It supports normal neuronal excitability by controlling ionic environment.
- Abnormal CSF pressure or composition can disturb brain function.
🔬 CONCEPT EXPLAINED
CSF exists because the brain requires both protection and chemical stability. The brain is soft and delicate, and it is enclosed in a rigid skull. CSF surrounds the brain and spinal cord and acts as a fluid cushion. During minor movements or impacts, CSF reduces direct mechanical stress on nervous tissue.
Another important function is buoyancy. Although the brain has a significant actual weight, when suspended in CSF its effective weight is greatly reduced. This prevents compression of vessels and nerves at the base of the brain.
CSF also contributes to chemical homeostasis. Neurons are extremely sensitive to changes in potassium, hydrogen ions, glucose, and other substances. CSF provides a controlled environment around the CNS. Because its composition is regulated by the choroid plexus and barriers, it helps maintain proper neuronal excitability.
CSF also assists in removal of metabolic waste. Since the brain has high metabolic activity, waste products must be cleared efficiently. CSF circulation helps carry these substances away from nervous tissue toward venous drainage pathways.
⚠️ CLINICAL IMPORTANCE
When CSF pressure rises, the protective role of CSF becomes harmful because the rigid skull cannot expand. Increased CSF volume compresses brain tissue and blood vessels, leading to headache, vomiting, papilledema, and possible neurological deterioration.
5 — Regulation of Cerebral Blood Flow
🧠 CORE
- Cerebral blood flow supplies oxygen and glucose to neurons.
- Brain tissue has high metabolic demand and little energy reserve.
- Cerebral blood flow is tightly regulated.
- Major regulators include carbon dioxide, hydrogen ions, oxygen, and local metabolic activity.
- Increased CO₂ causes cerebral vasodilation.
- Decreased CO₂ causes cerebral vasoconstriction.
- Cerebral autoregulation maintains stable blood flow despite moderate changes in blood pressure.
- Failure of regulation can cause ischemia or raised intracranial pressure.
🔬 CONCEPT EXPLAINED
The brain depends almost completely on continuous blood flow because neurons have high oxygen and glucose requirements and very limited energy stores. Therefore, regulation of cerebral blood flow is essential for survival of nervous tissue.
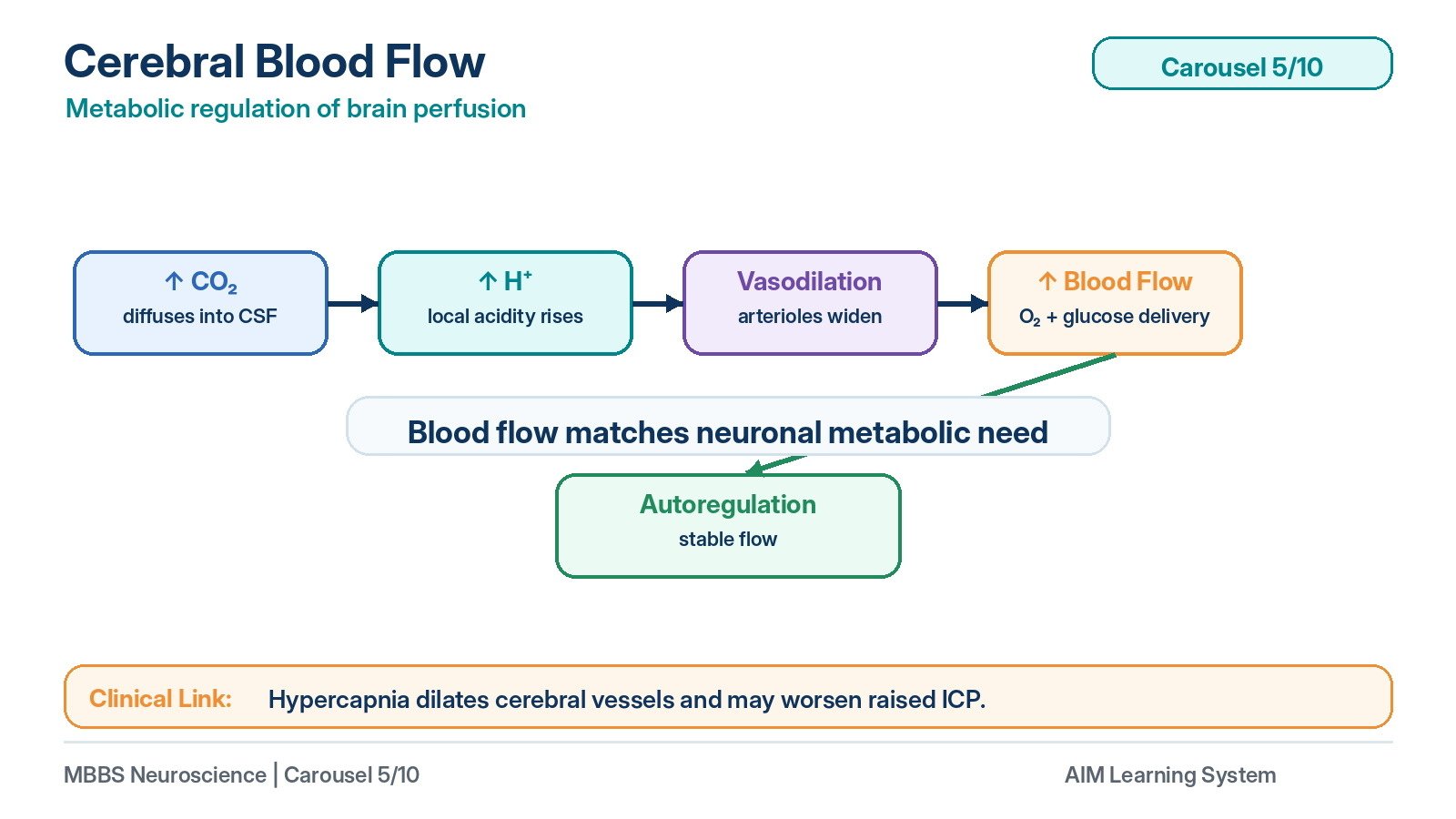
The most important regulator of cerebral blood flow is carbon dioxide. When arterial CO₂ increases, it diffuses into brain extracellular fluid and CSF. There it combines with water to form carbonic acid, which dissociates into hydrogen ions and bicarbonate. Increased hydrogen ion concentration causes cerebral arterioles to dilate. This increases blood flow and helps remove excess CO₂.
Therefore, the cause-effect relationship is:
Increased CO₂ → increased H⁺ in brain fluid → cerebral vasodilation → increased cerebral blood flow → removal of CO₂.
When CO₂ decreases, hydrogen ion concentration falls, cerebral vessels constrict, and cerebral blood flow decreases. This is why excessive hyperventilation can reduce cerebral blood flow and may cause dizziness or faintness.
Oxygen also affects cerebral blood flow, but mainly when oxygen levels fall significantly. Severe hypoxia causes vasodilation to increase blood supply to the brain. Local metabolic activity also regulates blood flow. Active brain regions produce more CO₂, hydrogen ions, adenosine, and other metabolites, which increase local blood flow.
Cerebral autoregulation maintains blood flow despite moderate changes in systemic blood pressure. If arterial pressure rises, cerebral arterioles constrict; if pressure falls, they dilate. This protects the brain from both ischemia and excessive pressure.
⚠️ CLINICAL IMPORTANCE
Failure of cerebral blood flow regulation may cause ischemic injury or increased intracranial pressure. Hypercapnia dilates cerebral vessels and can increase intracranial blood volume, worsening raised ICP. Severe hypotension may overcome autoregulation and reduce brain perfusion.
6 — Blood–Brain Barrier
🧠 CORE
- The blood–brain barrier separates blood from brain extracellular fluid.
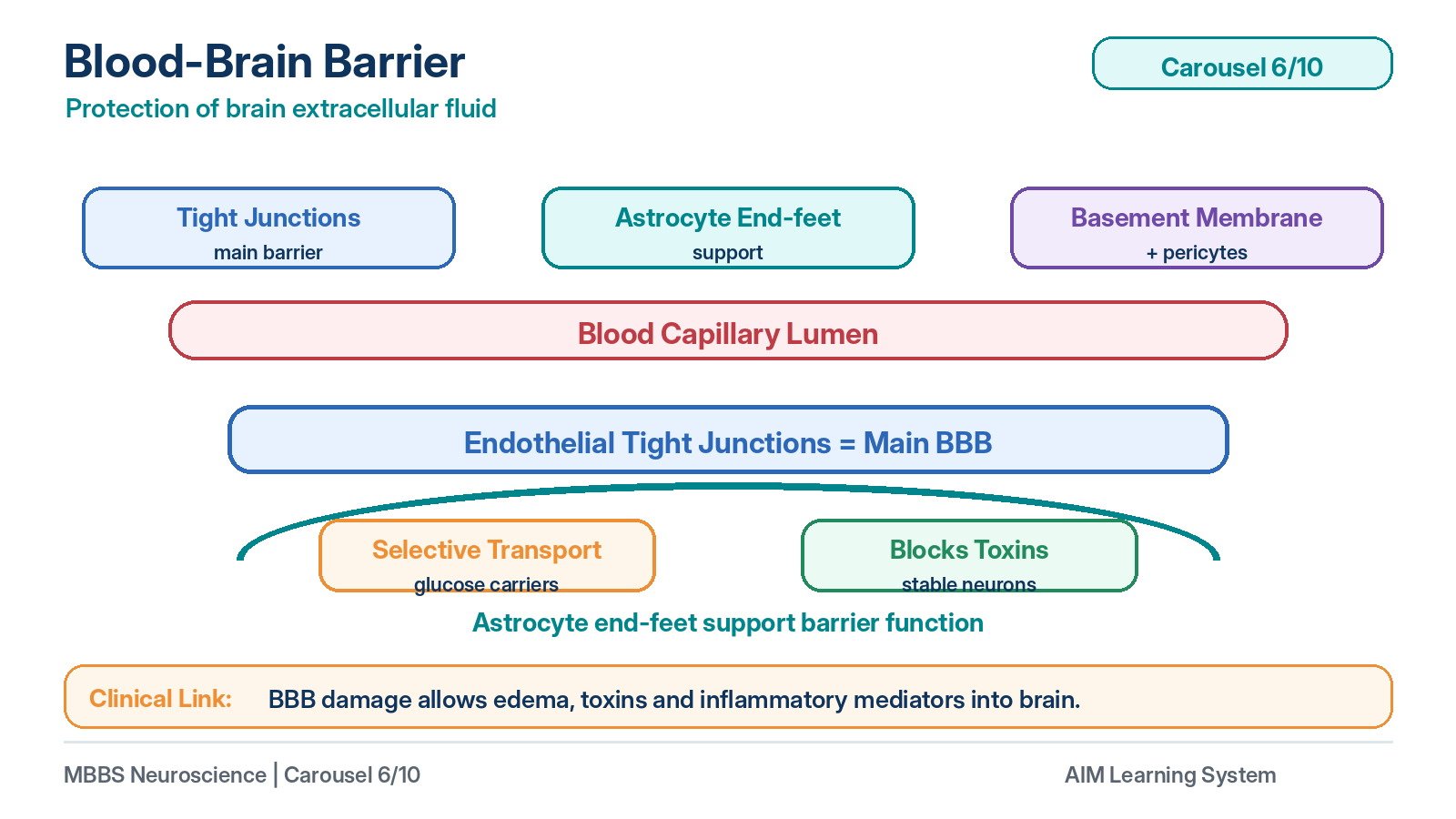
- It is formed mainly by tight junctions between brain capillary endothelial cells.
- Astrocyte end-feet support BBB function.
- Basement membrane and pericytes also contribute.
- It restricts entry of toxins, proteins, and many drugs.
- Lipid-soluble substances cross more easily.
- Glucose crosses by specific transporters.
- BBB maintains stable neuronal environment.
🔬 CONCEPT EXPLAINED
The blood–brain barrier is a protective barrier between circulating blood and the extracellular fluid of the brain. It exists because neurons are highly sensitive cells. Small changes in ionic composition, toxins, or neurotransmitter-like substances in blood can disturb neuronal excitability.
The structural basis of the BBB is the tight junctions between endothelial cells of brain capillaries. In most body capillaries, substances can pass more freely between endothelial cells. In brain capillaries, tight junctions seal these gaps and force substances to pass through endothelial cells rather than between them.
Astrocyte end-feet surround capillaries and help maintain the special properties of the endothelial cells. Pericytes and the basement membrane also support barrier integrity. Because of this arrangement, large molecules, plasma proteins, many toxins, and many drugs cannot easily enter the brain.
However, the BBB is not a complete wall. The brain still needs nutrients. Glucose crosses through specific glucose transporters, and oxygen and carbon dioxide cross because they are lipid-soluble gases. Lipid-soluble drugs can cross more easily than water-soluble drugs.
The physiological advantage of the BBB is protection and stability. It prevents sudden changes in plasma composition from directly affecting neurons. This is essential because abnormal extracellular potassium or hydrogen ion concentration can alter action potentials and synaptic transmission.
⚠️ CLINICAL IMPORTANCE
Inflammation, infection, trauma, tumors, or ischemia can disrupt the BBB. When the BBB becomes leaky, proteins and fluid may enter brain tissue, causing cerebral edema. The BBB is also important pharmacologically because many drugs cannot easily reach the brain.
7 — Blood–CSF Barrier
🧠 CORE
- The blood–CSF barrier is mainly present at the choroid plexus.
- It separates blood from CSF.
- Choroid plexus capillaries are fenestrated.
- Tight junctions between choroid epithelial cells form the true barrier.
- It controls entry of substances into CSF.
- It helps maintain low CSF protein content.
- It contributes to the special biochemical composition of CSF.
- It differs structurally from the blood–brain barrier.
🔬 CONCEPT EXPLAINED
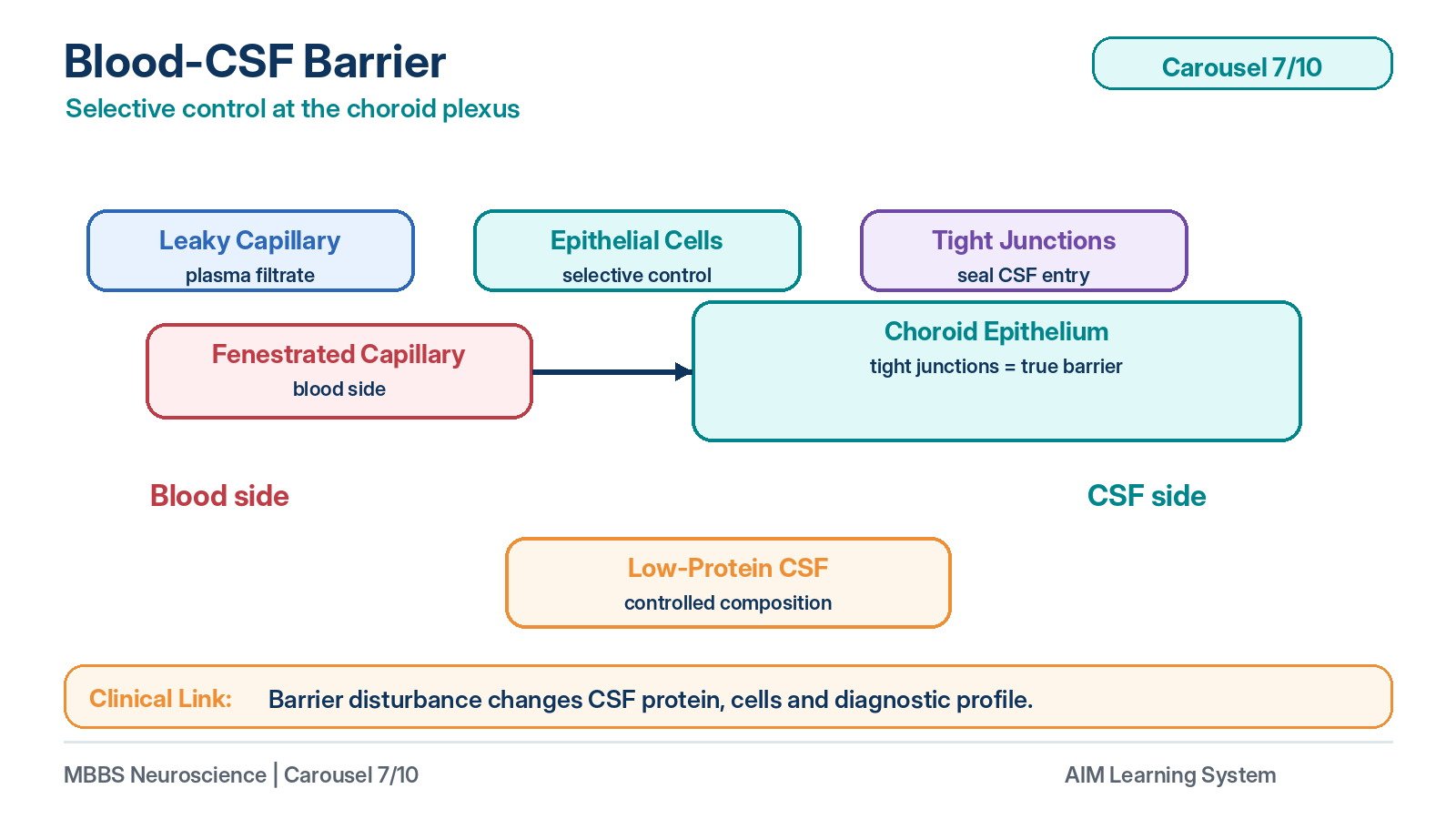
The blood–CSF barrier controls exchange between blood and CSF. It is mainly formed by the epithelial cells of the choroid plexus. Although capillaries inside the choroid plexus are fenestrated and allow plasma components to leave the blood, these substances still cannot freely enter the CSF because the choroid epithelial cells are joined by tight junctions.
This means that the barrier is not at the capillary endothelium, as in the BBB, but at the level of the choroid epithelial cells. These cells selectively transport ions, water, and nutrients into the ventricular cavity while restricting proteins and harmful substances.
The blood–CSF barrier is essential because CSF must remain chemically different from plasma. CSF has much lower protein concentration than plasma and a carefully regulated ionic composition. This controlled environment is important for normal neuronal function.
⚠️ CLINICAL IMPORTANCE
Damage to the blood–CSF barrier may alter CSF composition. Increased CSF protein, inflammatory cells, or blood pigments can indicate disease. Therefore, CSF analysis is clinically useful in CNS infections, hemorrhage, and inflammatory disorders.
8 — Biochemical Composition of CSF
🧠 CORE
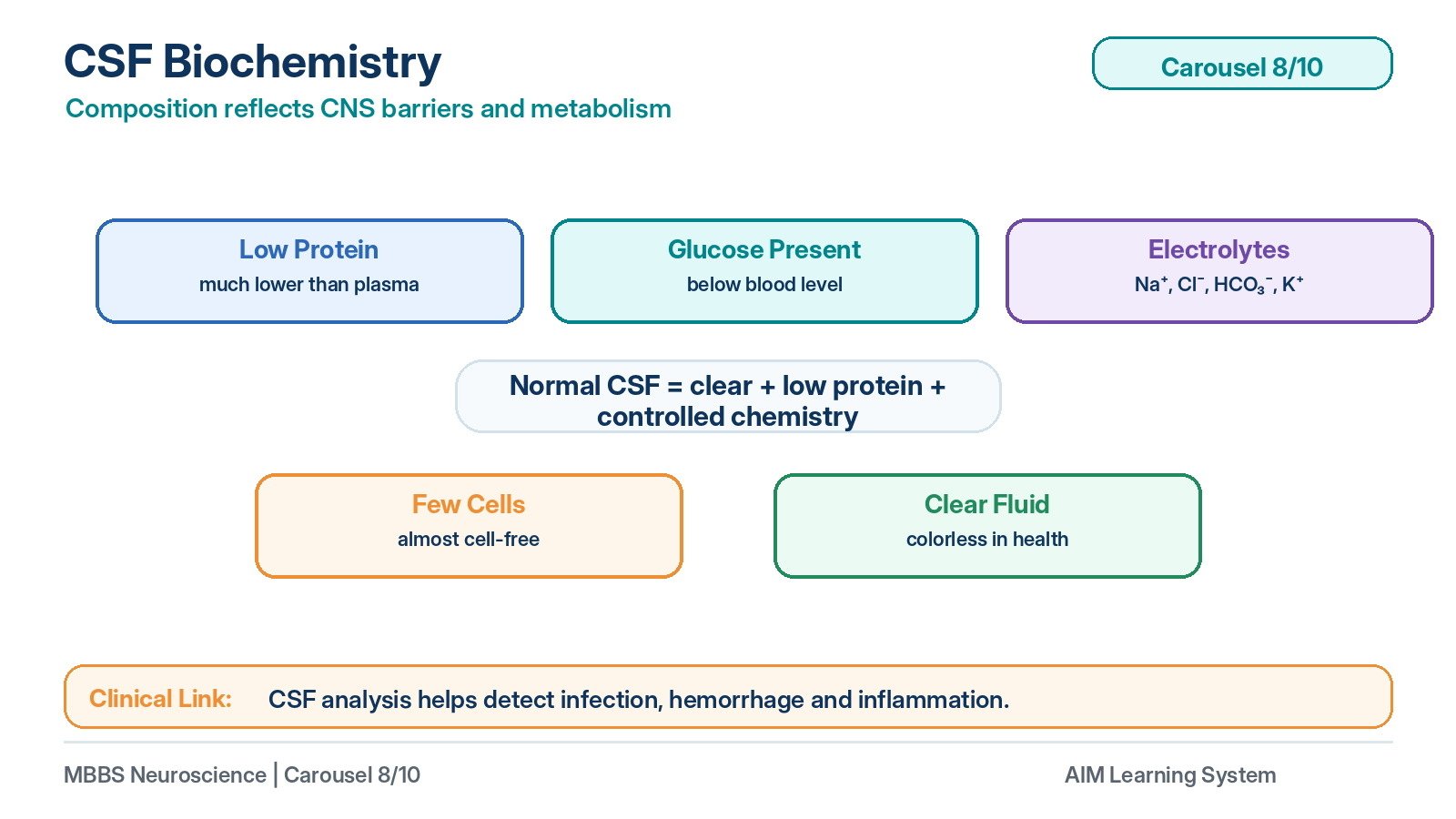
- CSF is clear and colorless under normal conditions.
- It has very low protein compared with plasma.
- It contains glucose, usually lower than blood glucose.
- It contains electrolytes such as sodium, chloride, bicarbonate, calcium, magnesium, and potassium.
- Normal CSF has very few cells.
- CSF composition reflects CNS metabolism and barrier function.
- Changes in CSF composition help diagnose CNS disease.
- Biochemical stability of CSF supports neuronal function.
🔬 CONCEPT EXPLAINED
CSF is not simply diluted plasma. Its composition is actively regulated by the choroid plexus and CNS barriers. Compared with plasma, CSF has much lower protein because large plasma proteins do not easily cross the blood–CSF barrier. This low protein content keeps CSF clear and reduces unnecessary osmotic and inflammatory effects around the CNS.
CSF contains glucose because neurons and glial cells require continuous energy supply. CSF glucose is normally lower than blood glucose because it enters from blood through regulated transport and is used by CNS cells. A marked fall in CSF glucose may occur in conditions where microorganisms or inflammatory cells consume glucose, such as bacterial meningitis. At 2nd-year level, the key point is that CSF glucose reflects both blood glucose and CNS pathological processes.
Electrolytes in CSF are important because neuronal excitability depends on ionic gradients. Sodium, potassium, calcium, chloride, and bicarbonate concentrations influence membrane potential, synaptic activity, and acid-base balance around neurons. The choroid plexus and barriers maintain these levels within a narrow range.
Normally, CSF contains very few cells. An increased white cell count suggests inflammation or infection, while red blood cells may suggest bleeding into the subarachnoid space or traumatic lumbar puncture.
⚠️ CLINICAL IMPORTANCE
CSF composition is important in clinical diagnosis. Increased protein, decreased glucose, increased cells, or blood in CSF can indicate CNS disease. In undergraduate MBBS, the major exam concept is that CSF analysis reflects the condition of CNS barriers, infection, hemorrhage, and inflammation.
9 — Hydrocephalus as a Disorder of CSF Formation, Flow, or Absorption
🧠 CORE
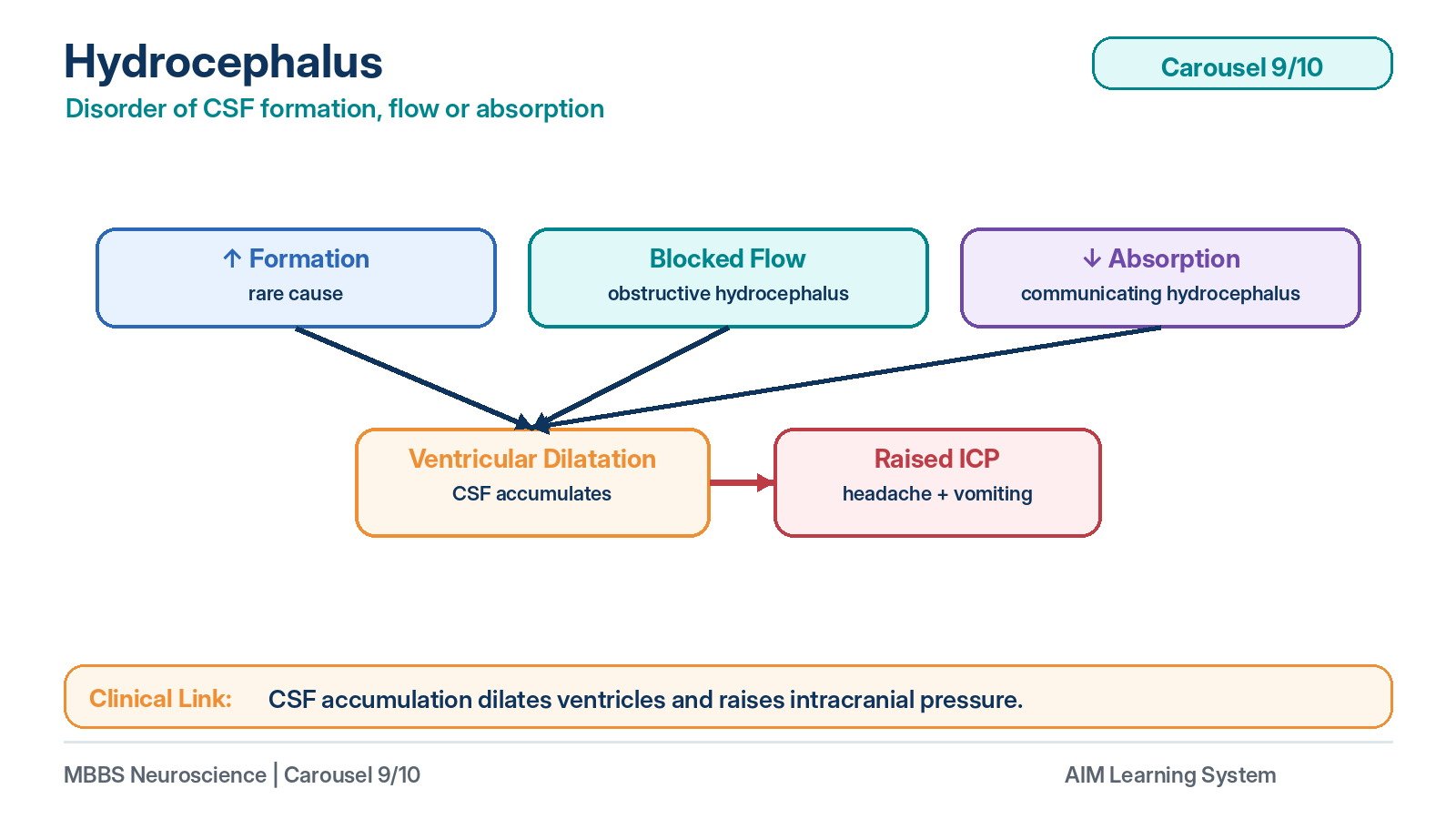
- Hydrocephalus is abnormal accumulation of CSF.
- It may result from increased CSF formation, obstruction to flow, or impaired absorption.
- Obstructive hydrocephalus occurs due to blockage within ventricular pathways.
- Communicating hydrocephalus occurs when CSF pathways communicate but absorption is impaired.
- Excess CSF increases ventricular size.
- Raised intracranial pressure occurs when CSF accumulation exceeds compensatory capacity.
- In infants, head enlargement may occur because skull sutures are not fused.
- In adults, raised ICP produces headache, vomiting, papilledema, and neurological features.
🔬 CONCEPT EXPLAINED
Hydrocephalus means abnormal accumulation of CSF inside the cranial cavity, especially within the ventricles. To understand hydrocephalus, remember that normal CSF balance depends on three processes: formation, flow, and absorption. If any one of these is disturbed, CSF volume increases.
The most common mechanism is obstruction to CSF flow. If CSF is produced normally but cannot pass through the ventricular pathway, it accumulates proximal to the obstruction. For example, obstruction of the cerebral aqueduct causes dilatation of the lateral and third ventricles because CSF cannot reach the fourth ventricle normally. This is called non-communicating or obstructive hydrocephalus.
Another mechanism is impaired absorption. In this case, CSF flows through the ventricles and reaches the subarachnoid space, but it cannot be absorbed properly through arachnoid villi. This may occur after meningitis or subarachnoid hemorrhage, where inflammation or blood products interfere with arachnoid villi. This is called communicating hydrocephalus.
Rarely, hydrocephalus may result from excessive CSF production, such as in choroid plexus tumor. However, at undergraduate level, obstruction and impaired absorption are the main mechanisms to understand.
As CSF accumulates, ventricles dilate. In infants, skull sutures are not fully fused, so head size may increase. In older children and adults, the skull cannot expand, so increased CSF volume raises intracranial pressure. This increased pressure compresses brain tissue and cerebral vessels, causing symptoms.
⚠️ CLINICAL IMPORTANCE
Hydrocephalus is clinically important because it converts a disturbance of CSF physiology into neurological dysfunction. Raised ICP causes headache due to stretching of pain-sensitive intracranial structures, especially dura and blood vessels. Vomiting may occur due to pressure effects on brainstem centers. Papilledema results from raised pressure transmitted along the optic nerve sheath.
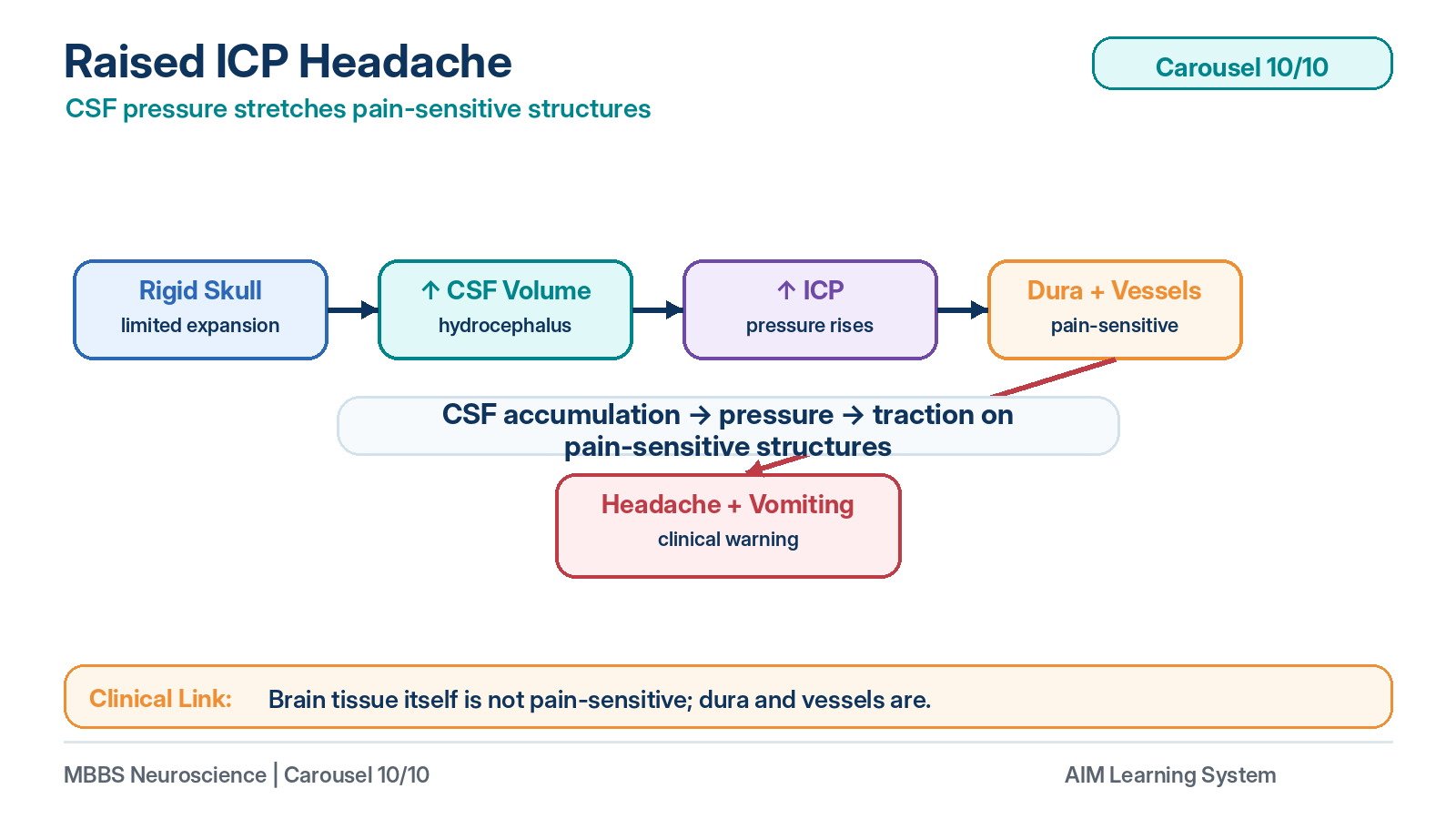
10 — Raised Intracranial Pressure as a Cause of Headache
🧠 CORE
- The skull is a rigid cavity containing brain, blood, and CSF.
- Increase in any component can raise intracranial pressure.
- CSF accumulation in hydrocephalus is an important cause of raised ICP.
- Brain parenchyma itself is not pain-sensitive.
- Pain-sensitive structures include dura mater, large vessels, and venous sinuses.
- Raised ICP causes headache by stretching or compressing pain-sensitive structures.
- Associated features may include vomiting, papilledema, and altered consciousness.
- Severe raised ICP may reduce cerebral perfusion.
🔬 CONCEPT EXPLAINED
The cranial cavity contains three main components: brain tissue, blood, and CSF. Since the skull is rigid, an increase in one component must be compensated by a decrease in another. Initially, small increases in volume may be compensated by shifting CSF or venous blood. However, once compensation fails, intracranial pressure rises rapidly.
In hydrocephalus, excess CSF increases intracranial volume. This stretches ventricular walls and increases pressure within the cranial cavity. Although brain tissue itself is not pain-sensitive, several intracranial structures are pain-sensitive, especially dura mater, large arteries, venous sinuses, and meningeal vessels. Stretching or traction on these structures produces headache.
Raised ICP can also reduce cerebral perfusion. Cerebral perfusion depends on arterial pressure being higher than intracranial pressure. If ICP rises too much, blood flow to the brain may decrease, causing altered consciousness or neurological signs.
⚠️ CLINICAL IMPORTANCE
Headache due to raised ICP is often associated with vomiting, visual symptoms due to papilledema, and worsening with situations that increase intracranial pressure. At this level, the key concept is: CSF accumulation → raised ICP → stretching of pain-sensitive structures → headache and neurological consequences.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Choroid Plexus → CSF Formation → Stable CNS Fluid Environment
The choroid plexus has fenestrated capillaries and specialized epithelial cells. This structure allows plasma filtration but controlled secretion into ventricles. The outcome is CSF with low protein and regulated electrolytes, suitable for neuronal function.
Ventricular System → CSF Flow → Distribution Around CNS
The ventricles form a connected pathway. This allows CSF to move from its site of formation to the subarachnoid space. The outcome is cushioning, buoyancy, waste removal, and chemical stability around the brain and spinal cord.
Arachnoid Villi → CSF Absorption → Normal Intracranial Pressure
Arachnoid villi project into venous sinuses and absorb CSF according to pressure gradients. This maintains balance between CSF formation and removal. If absorption fails, CSF accumulates and hydrocephalus develops.
Blood–Brain Barrier → Protection of Brain Tissue → Stable Neuronal Excitability
Tight junctions in brain capillary endothelium restrict harmful substances and large molecules from entering brain tissue. This maintains stable extracellular fluid composition and protects synaptic transmission.
Blood–CSF Barrier → Regulation of CSF Composition → Diagnostic Value of CSF
Tight junctions between choroid epithelial cells regulate CSF composition. When this barrier is disturbed, CSF protein, cells, or other substances may change. Therefore, CSF analysis becomes clinically useful.
CSF Biochemistry → Neuronal Function → Clinical Diagnosis
Low protein, controlled glucose, electrolytes, and few cells are normal CSF features. Changes in these values indicate disease processes such as infection, hemorrhage, or inflammation.
🩺 5️⃣ Clinical Correlation
1. Hydrocephalus
Hydrocephalus is abnormal accumulation of CSF due to increased formation, blocked flow, or reduced absorption. The most important undergraduate concept is that CSF is continuously produced, so any obstruction or absorption failure causes progressive accumulation.
Cause → Effect
CSF obstruction or absorption failure → ventricular dilatation → raised ICP → headache, vomiting, papilledema, and neurological features.
2. Obstructive Hydrocephalus
Obstructive hydrocephalus occurs when CSF flow is blocked within the ventricular system. A common site is the cerebral aqueduct because it is narrow.
Cause → Effect
Aqueduct obstruction → CSF cannot pass from third to fourth ventricle → lateral and third ventricles dilate → raised ICP.
3. Communicating Hydrocephalus
Communicating hydrocephalus occurs when ventricles communicate with the subarachnoid space, but absorption through arachnoid villi is impaired.
Cause → Effect
Meningitis or subarachnoid hemorrhage → arachnoid villi dysfunction → reduced CSF absorption → generalized CSF accumulation.
4. Raised Intracranial Pressure and Headache
Raised ICP causes headache because it stretches pain-sensitive structures such as dura mater, venous sinuses, and large blood vessels. Brain parenchyma itself is not pain-sensitive.
Important exam point:
Headache in raised ICP is due to stretching of pain-sensitive intracranial structures, not pain from brain tissue itself.
5. Importance of CSF Composition in Diagnosis
CSF analysis helps identify CNS disease. Increased protein suggests barrier damage or inflammation. Reduced glucose may suggest infection. Increased cells indicate inflammatory or infectious processes. Blood in CSF may suggest hemorrhage.
At 2nd-year level, the key focus is not detailed diagnosis or management, but understanding how abnormal CSF composition reflects disturbance of CNS barriers or pathology.
📌 6️⃣ Summary Points
- CSF is produced mainly by the choroid plexus inside the ventricles.
- CSF formation is mainly an active secretory process, not simple filtration only.
- CSF flows: lateral ventricles → foramina of Monro → third ventricle → cerebral aqueduct → fourth ventricle → Magendie/Luschka → subarachnoid space.
- CSF is absorbed mainly through arachnoid villi/granulations into dural venous sinuses.
- The blood–brain barrier is formed mainly by tight junctions between brain capillary endothelial cells.
- The blood–CSF barrier is formed mainly by tight junctions between choroid epithelial cells.
- CSF normally has low protein, controlled glucose, controlled electrolytes, and very few cells.
- Hydrocephalus occurs due to abnormal CSF formation, flow, or absorption.
- Obstruction of the cerebral aqueduct causes obstructive hydrocephalus.
- Failure of arachnoid villi absorption causes communicating hydrocephalus.
- Raised ICP causes headache by stretching pain-sensitive structures, especially dura and large vessels.
- CO₂ is a major regulator of cerebral blood flow; increased CO₂ causes cerebral vasodilation.