
📖 Step 2 — Learning Material
This topic uses the AIM Learning Cycle to help MBBS students understand clinical disorders affecting swallowing and esophageal function by integrating Physiology, Pathology and Clinical Medicine.
1️⃣ Introduction
Swallowing is a coordinated neuromuscular process that allows safe movement of food from the mouth to the stomach. The esophagus plays a central role in transporting food through rhythmic contractions known as peristalsis. Disorders of swallowing and esophageal function can lead to difficulty eating, malnutrition, aspiration, and infection. These conditions are clinically important because they often present as dysphagia (difficulty swallowing) or odynophagia (painful swallowing). Understanding these disorders helps students recognize early symptoms and manage common clinical problems such as achalasia and esophageal candidiasis.
2️⃣ Foundation Basics
Key Definitions
- Swallowing (Deglutition): Movement of food from mouth → pharynx → esophagus → stomach
- Dysphagia: Difficulty in swallowing
- Odynophagia: Painful swallowing
- Peristalsis: Coordinated contraction pushing food forward
- Lower Esophageal Sphincter (LES): Circular muscle controlling entry into stomach
- Achalasia: Failure of LES relaxation
- Megaesophagus: Dilated esophagus due to chronic obstruction
- Esophageal Candidiasis: Fungal infection of esophageal mucosa
- Primary peristalsis: Swallow-induced wave
- Secondary peristalsis: Response to retained food
- LES tone: Resting contraction of lower esophagus
- Myenteric plexus: Controls esophageal motility
- Candida albicans: Most common fungal pathogen
3. Basic Review
Swallowing disorders arise when:
- Neural control fails
- Muscular contraction weakens
- Sphincter relaxation is impaired
- Infection damages mucosa
Result:
 Impaired food transport Pain Risk of aspiration
Impaired food transport Pain Risk of aspiration
3️⃣ Core Learning — Curriculum Coverage
1.Clinical Abnormalities of Swallowing
CORE (High-Yield Essentials)
- Dysphagia = difficulty in swallowing
- May affect oropharyngeal or esophageal phase
- Caused by neuromuscular dysfunction
- Can be structural or functional
- Leads to food retention
- Increases risk of aspiration pneumonia
- Often associated with neurological disease
- Important presenting symptom in esophageal disease
 CONCEPT EXPLAINED
CONCEPT EXPLAINED
Structure
Swallowing involves:
- Mouth
- Pharynx
- Esophagus
- Lower esophageal sphincter
Mechanism
Swallowing occurs in phases:
- Oral phase (voluntary)
- Pharyngeal phase (reflex)
- Esophageal phase (peristalsis)
Failure at any stage causes dysphagia.
Structure → Function
Normal peristalsis:
- Moves food downward
- Prevents reflux
- Protects airway
 IF DAMAGED
IF DAMAGED
Cause → Effect
- Nerve damage → weak muscle contraction
- Weak peristalsis → food retention
- Retained food → aspiration risk
- Aspiration → pneumonia
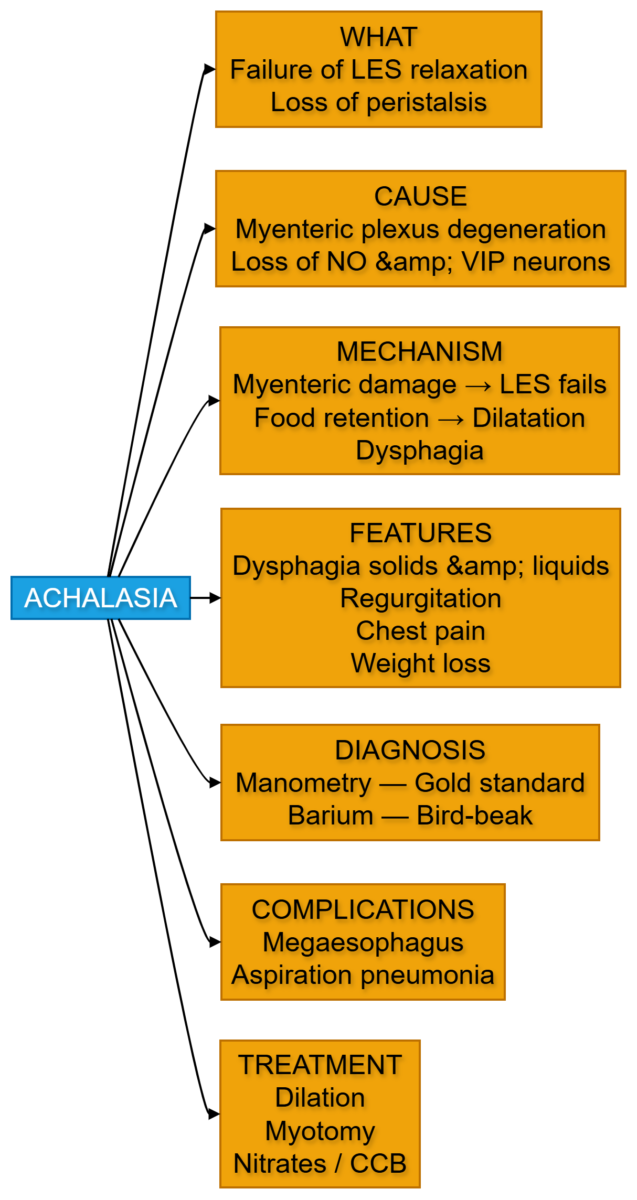
2. Achalasia
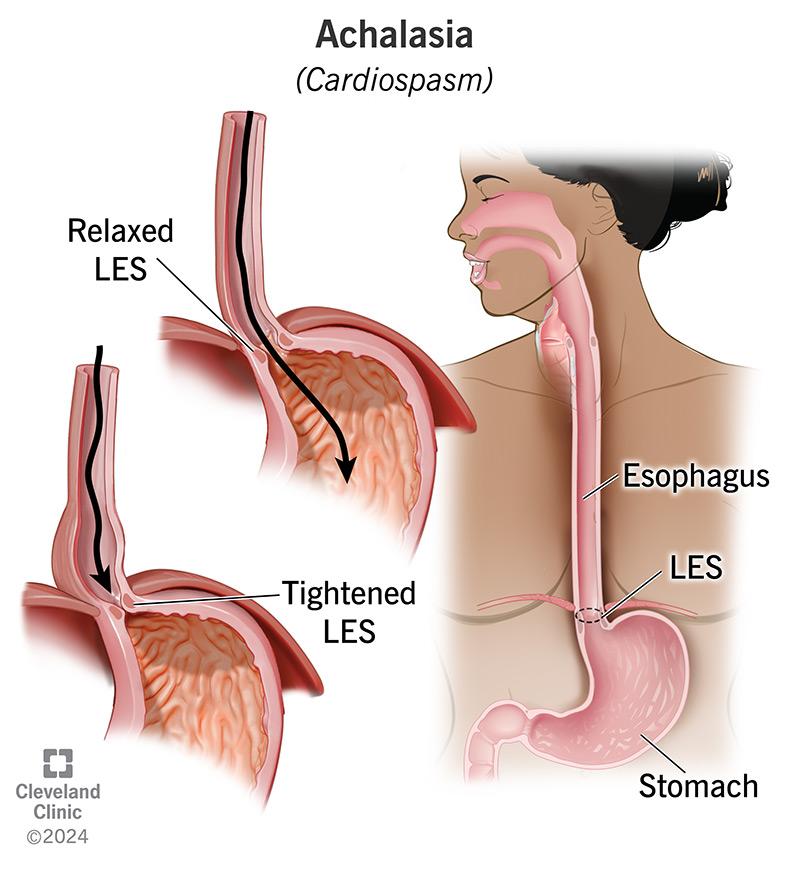
• Achalasia = failure of LES relaxation
• Caused by degeneration of myenteric plexus
• Leads to impaired peristalsis
• Food accumulates in esophagus
• Causes progressive dysphagia
• Both solids and liquids affected
• Produces regurgitation
• Diagnosed by manometry
CONCEPT EXPLAINED
Structure
Affected structures:
• Myenteric plexus
• LES muscle
• Esophageal body
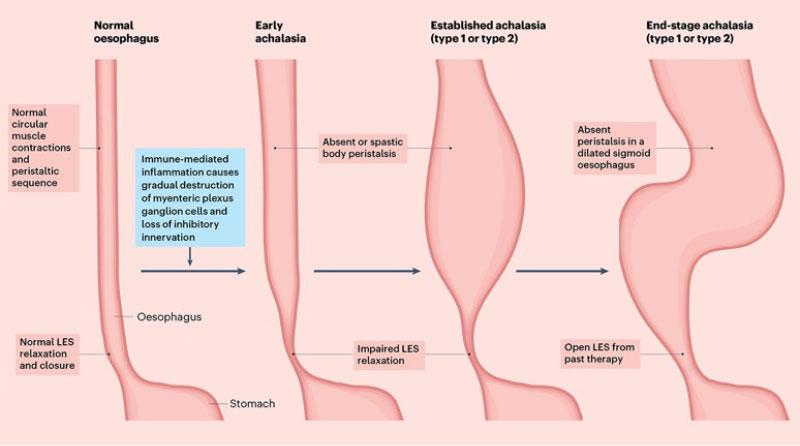
Mechanism
Stepwise:
- Neural degeneration occurs
- LES fails to relax
- Food cannot enter stomach
- Esophagus dilates
- Peristalsis weakens
Structure → Function
LES normally:
• Relaxes during swallowing
• Allows food entry
In achalasia: LES remains contracted Food accumulates
IF DAMAGED
Cause → Effect
Myenteric damage → LES failure →
Food retention → dilation → dysphagia
Concept Map 1 — Achalasia
3. Mega esophagus
- Mega esophagus = enlarged esophagus
- Usually develops after chronic achalasia
- Caused by prolonged obstruction
- Leads to muscle stretching
- Weakens esophageal wall
- Food retention worsens
- Risk of aspiration increases
- May cause weight loss
CONCEPT EXPLAINED
Structure
Affected:
- Entire esophageal tube
- Muscular wall
Mechanism
- LES obstruction persists
- Food accumulates
- Pressure increases
- Wall stretches
- Esophagus enlarges
Structure → Function
Dilated esophagus:
- Loses peristaltic power
- Cannot push food effectively
IF DAMAGED
Cause → Effect
Chronic obstruction → dilation →
Loss of motility → severe dysphagia
4. Esophageal candidiasis
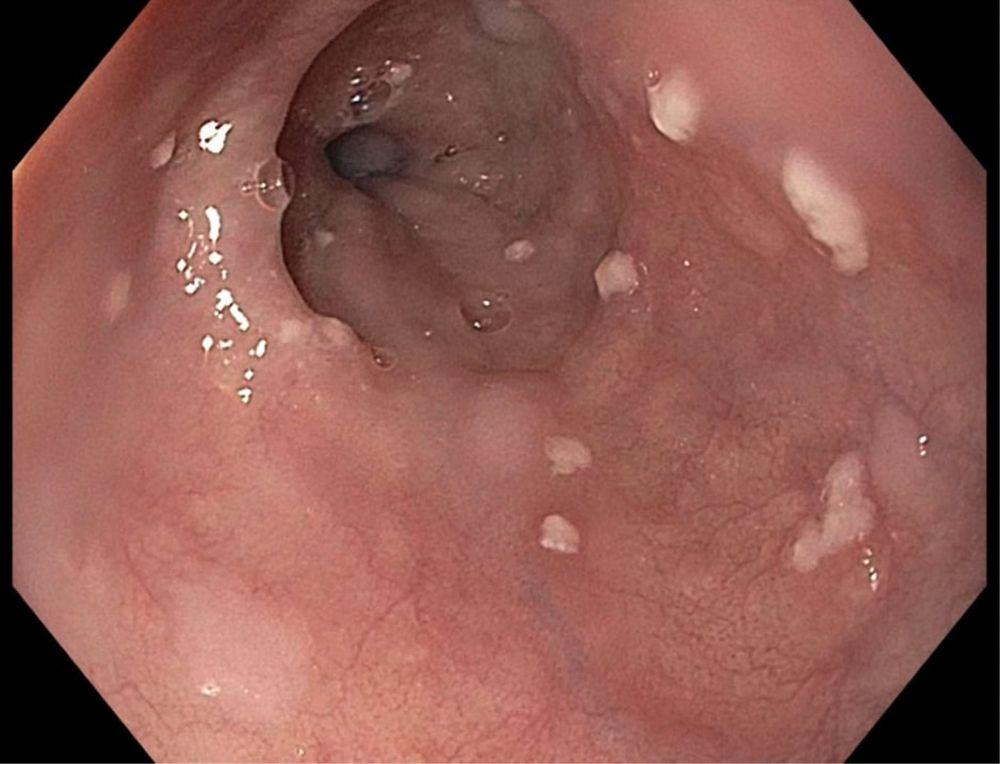
- Esophageal candidiasis = fungal infection
- Caused mainly by Candida albicans
- Occurs in immunocompromised patients
- Produces painful swallowing
- White plaques seen on mucosa
- Leads to inflammation
- Common in diabetes and HIV
- Diagnosed by endoscopy
CONCEPT EXPLAINED
Structure
Affected:
- Esophageal mucosal lining
Mechanism
- Immune system weakens
- Candida multiplies
- Fungal invasion occurs
- Inflammation develops
- Pain during swallowing occurs
Structure → Function
Damaged mucosa:
Pain Difficulty swallowing
IF DAMAGED
Cause → Effect
Fungal infection → mucosal injury →
Pain → reduced food intake
Drugs Used in Esophageal Candidiasis
CORE
- Antifungal drugs are primary treatment
- Fluconazole is first-line drug
- Itraconazole used if resistance occurs
- Amphotericin B used in severe infection
- Nystatin used for mild infection
- Therapy usually lasts 14–21 days
- Oral therapy preferred
- IV therapy used in severe cases
CONCEPT EXPLAINED
Structure
Drug targets:
Fungal cell membrane
Mechanism
Antifungals:
- Inhibit ergosterol synthesis
- Damage fungal membrane
- Cause fungal death
Structure → Function
Healthy mucosa restored →
Normal swallowing resumes
IF DAMAGED
Cause → Effect
Untreated infection → severe inflammation →
Ulceration → bleeding risk
4️⃣ Mechanism Flow
Achalasia Mechanism
- Myenteric plexus degenerates
- LES fails to relax
- Food accumulates
- Esophagus dilates
- Dysphagia develops
Esophageal Candidiasis Mechanism
- Immunity decreases
- Candida multiplies
- Mucosa inflames
- Pain occurs
- Swallowing becomes difficult
5️⃣ Functional Integration
Structure → Function → Outcome
Myenteric plexus → controls LES → allows swallowing
If damaged:
Myenteric loss → LES contraction → dysphagia
6️⃣ Clinical Correlation
Common exam-relevant conditions:
- Achalasia
- Megaesophagus
- Esophageal candidiasis
- Dysphagia
- Odynophagia
Important Signs:
- Progressive dysphagia
- Regurgitation
- Weight loss
- Painful swallowing
⭐ 7️⃣ Points to Remember
- Dysphagia is the most common symptom of esophageal disease
- Achalasia = failure of LES relaxation
- Myenteric plexus damage causes achalasia
- Chronic achalasia leads to megaesophagus
- Esophageal candidiasis occurs in immunocompromised patients
- Candida produces white mucosal plaques
- Fluconazole is first-line treatment
- Dilated esophagus loses peristalsis
- Painful swallowing suggests infection
- Untreated dysphagia may cause aspiration pneumonia.