
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The liver, gall bladder, and biliary tree develop from the foregut endoderm during early embryonic life. These organs play a vital role in digestion, metabolism, bile formation, and detoxification. The liver is the largest gland in the body, while the gall bladder stores bile and the biliary tree conducts bile to the intestine. Understanding their development explains many congenital anomalies such as biliary atresia, gall bladder agenesis, and accessory hepatic ducts. This topic is clinically important because developmental defects often present as neonatal jaundice, biliary obstruction, or digestive dysfunction.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Hepatic diverticulum — An endodermal outgrowth from the foregut that forms liver and biliary system.
- Foregut — The anterior portion of primitive gut tube that gives rise to liver, pancreas, and biliary structures.
- Biliary tree — System of ducts carrying bile from liver to duodenum.
- Hepatoblasts — Primitive liver cells derived from hepatic diverticulum.
- Septum transversum — Mesodermal structure that contributes to liver stroma and diaphragm.
Essential Terminology
- Endoderm → Forms epithelial components.
- Mesoderm → Forms connective tissue and blood vessels.
- Vitelline veins → Important in formation of hepatic sinusoids.
- Bile canaliculi → Microscopic channels carrying bile between hepatocytes.
- Extrahepatic bile ducts → Ducts outside liver connecting to intestine.
Basic Overview
- Liver, gall bladder, and biliary tree originate from hepatic diverticulum.
- Development begins around 4th week of intrauterine life.
- Structures arise from foregut endoderm.
- Interaction with septum transversum mesoderm is essential.
- Biliary system establishes connection with duodenum.
🔹 3️⃣ Core Learning — Curriculum Coverage
A. Development of Liver
🧠 CORE
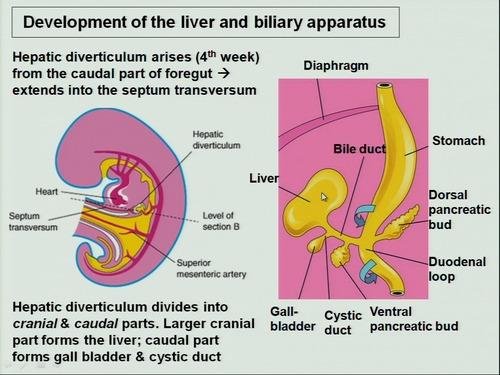
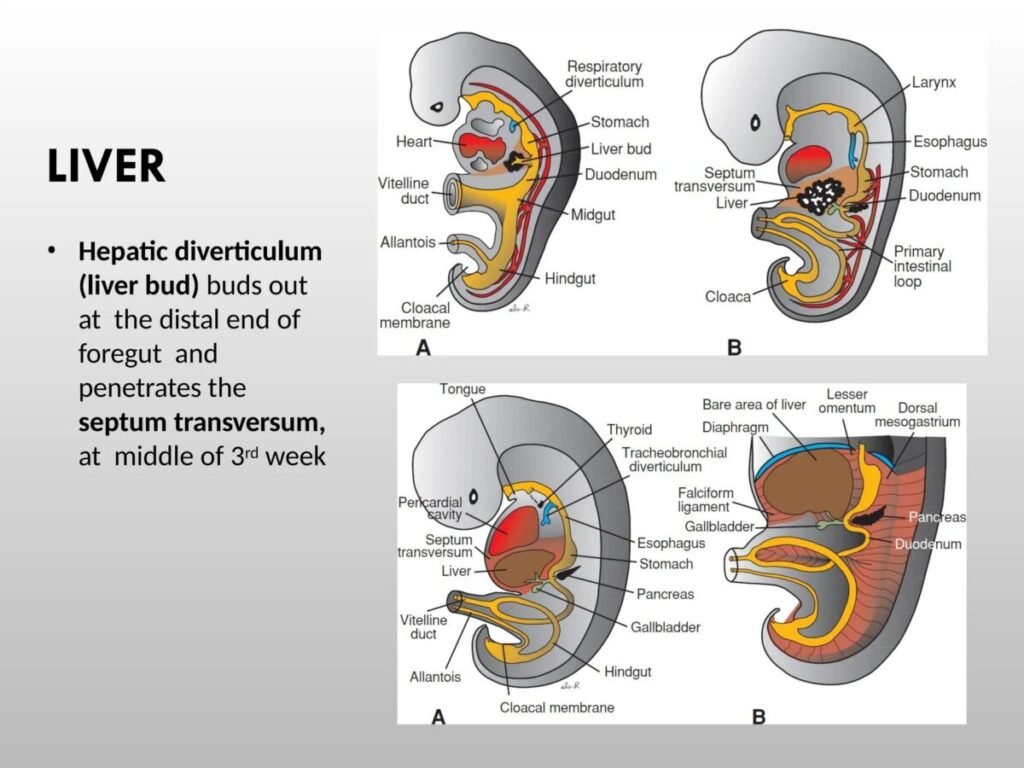
- Liver develops from hepatic diverticulum.
- Appears during 4th week of development.
- Originates from ventral wall of foregut (duodenum).
- Divided into:
- Cranial part → Liver parenchyma
- Caudal part → Gall bladder and cystic duct
- Hepatic cells derived from endoderm.
- Connective tissue derived from septum transversum mesoderm.
- Vitelline veins form hepatic sinusoids.
- Liver functions as hematopoietic organ in fetus.
🔬 CONCEPT EXPLAINED
Structure
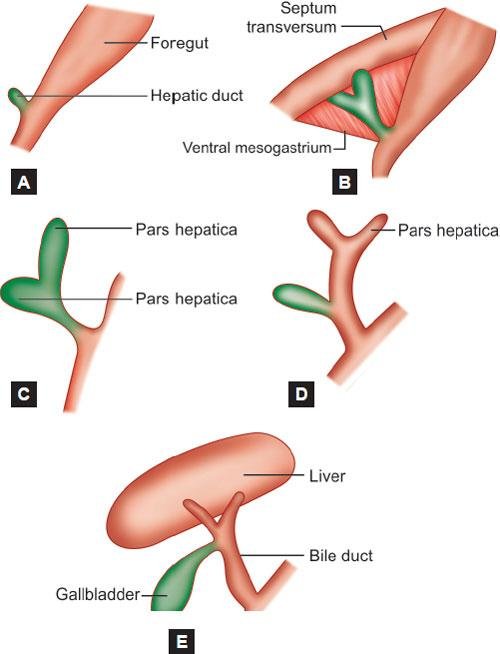
During the 4th week, an outgrowth called the hepatic diverticulum arises from the ventral foregut. This diverticulum grows into the septum transversum, which provides supportive mesenchyme.
The cranial part of the diverticulum enlarges and divides into cords of cells called hepatoblasts. These cells form:
- Hepatocytes
- Bile canaliculi
- Hepatic cords
Meanwhile, vitelline veins passing through liver tissue break into networks forming hepatic sinusoids, allowing blood flow through the developing liver.
Mechanism
- Hepatic diverticulum forms from foregut endoderm.
- Diverticulum grows into septum transversum.
- Hepatic cords develop and branch.
- Vitelline veins fragment → hepatic sinusoids.
- Liver enlarges rapidly.
- Hematopoiesis begins in fetal liver.
Structure → Function
- Hepatic cords → form hepatocytes → bile secretion.
- Sinusoids → allow blood filtration.
- Septum transversum → provides connective tissue support.
⚠️ IF DAMAGED
Cause → Effect
- Failure of hepatic diverticulum development → Liver agenesis (rare)
- Poor sinusoid formation → Abnormal liver circulation
- Impaired liver growth → Reduced fetal hematopoiesis
B. Development of Gall Bladder
🧠 CORE
- Gall bladder develops from caudal part of hepatic diverticulum.
- Appears during 4th week.
- Derived from endoderm.
- Cystic duct forms from narrow connection.
- Gall bladder lumen temporarily closes.
- Recanalization restores lumen.
- Bile storage function begins after birth.
🔬 CONCEPT EXPLAINED
Structure
The caudal portion of hepatic diverticulum becomes the gall bladder primordium. This portion elongates and forms a sac-like structure.
The narrow connection between gall bladder and bile duct becomes the cystic duct.
Initially, the gall bladder lumen is obliterated due to epithelial proliferation. Later, it recanalizes, restoring the cavity.
Mechanism
- Caudal hepatic diverticulum enlarges.
- Gall bladder bud forms.
- Lumen temporarily closes.
- Recanalization restores cavity.
- Gall bladder connects to biliary tree.
Structure → Function
- Gall bladder sac → bile storage.
- Cystic duct → bile passage.
- Recanalization → allows bile flow.
⚠️ IF DAMAGED
Cause → Effect
- Failure of gall bladder formation → Gall bladder agenesis
- Failure of recanalization → Gall bladder atresia
- Abnormal cystic duct formation → Biliary obstruction
C. Development of Biliary Tree
🧠 CORE
- Biliary ducts arise from hepatic diverticulum stalk.
- Derived from endoderm.
- Intrahepatic ducts form from hepatic cords.
- Extrahepatic ducts form from diverticulum stalk.
- Common bile duct connects to duodenum.
- Recanalization required for lumen formation.
- Ducts carry bile to intestine.
🔬 CONCEPT EXPLAINED
Structure
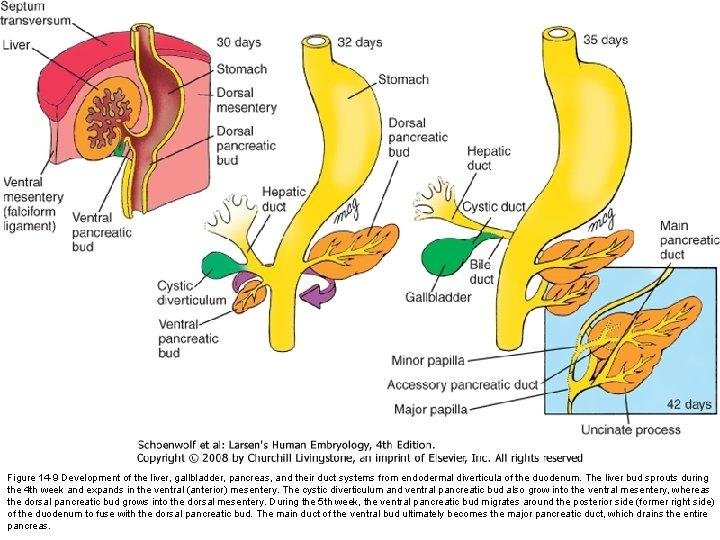
As hepatic diverticulum grows, the connecting stalk becomes the common bile duct.
Branching of hepatic cords forms intrahepatic bile ducts. These ducts join extrahepatic ducts to form a complete biliary pathway.
The bile duct opens into the duodenum, establishing digestive continuity.
Mechanism
- Hepatic diverticulum forms.
- Stalk becomes bile duct.
- Branching forms intrahepatic ducts.
- Extrahepatic ducts develop.
- Lumen recanalizes.
Structure → Function
- Biliary ducts → transport bile.
- Common bile duct → delivers bile to intestine.
- Branching pattern → distributes bile.
⚠️ IF DAMAGED
Cause → Effect
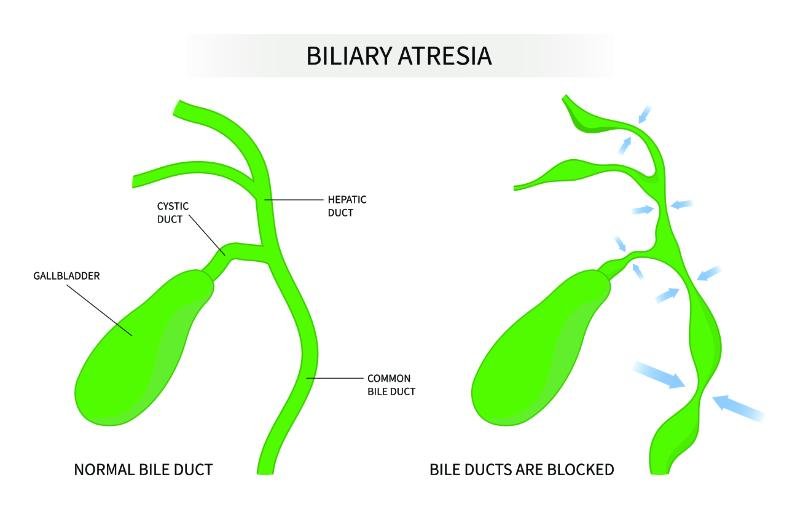
- Failure of recanalization → Biliary atresia
- Narrow ducts → Biliary stenosis
- Abnormal branching → Accessory bile ducts
D. Developmental Anomalies of Liver
🧠 CORE
- Liver anomalies occur due to abnormal growth.
- May involve size, position, or structure.
- Accessory lobes may form.
- Lobulation defects possible.
- Rare cases of liver agenesis occur.
- Blood supply defects affect liver growth.
🔬 CONCEPT EXPLAINED
Structure
Accessory hepatic tissue may arise from excess branching of hepatic cords. Lobulation abnormalities occur when growth patterns vary.
Rarely, incomplete development leads to small liver or missing liver tissue.
Mechanism
- Excess hepatic budding → accessory lobes.
- Reduced growth → hypoplastic liver.
- Vascular defects → impaired liver development.
Structure → Function
- Accessory lobes → usually asymptomatic.
- Reduced liver tissue → decreased metabolic capacity.
⚠️ IF DAMAGED
Cause → Effect
- Hypoplastic liver → reduced metabolic function.
- Accessory liver tissue → risk of torsion.
- Vascular defects → impaired blood flow.
E. Developmental Anomalies of Biliary Tree
🧠 CORE
- Most common anomaly → Biliary atresia.
- Caused by failure of duct recanalization.
- Accessory ducts may form.
- Abnormal duct connections possible.
- Gall bladder anomalies associated.
- Leads to bile flow obstruction.
🔬 CONCEPT EXPLAINED
Structure
Failure of bile duct formation or recanalization results in narrowed or absent ducts. This obstructs bile flow from liver to intestine.
Accessory ducts form due to abnormal branching patterns.
Mechanism
- Failure of recanalization.
- Duct remains closed.
- Bile accumulates.
- Liver damage occurs.
Structure → Function
- Obstructed ducts → bile retention.
- Bile retention → liver injury.
- Progressive obstruction → cirrhosis.
⚠️ IF DAMAGED
Cause → Effect
- Biliary atresia → neonatal jaundice.
- Accessory ducts → bile leakage during surgery.
- Duct stenosis → obstructive jaundice.
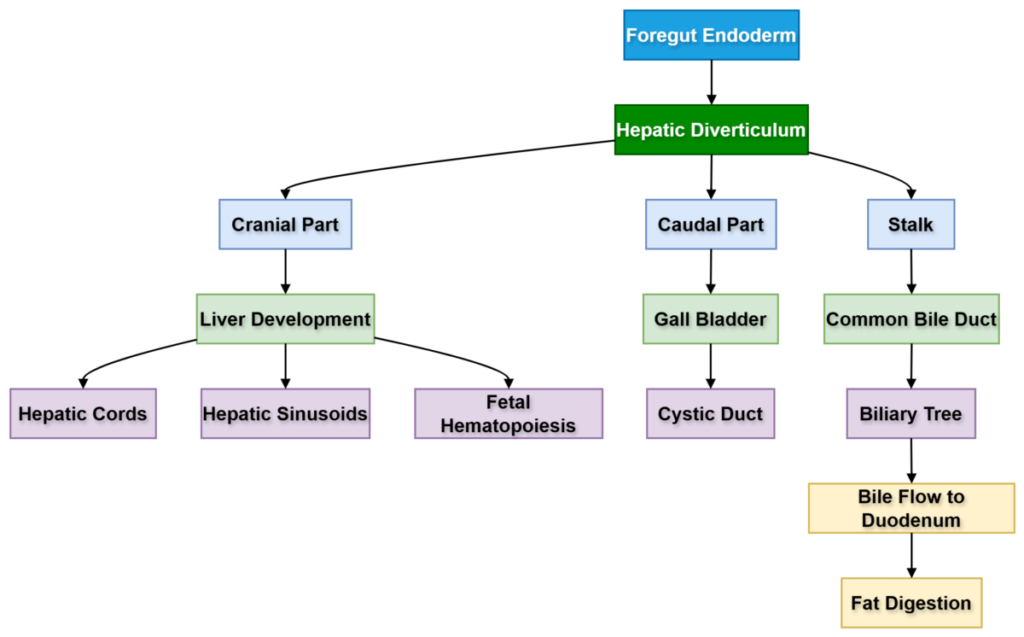
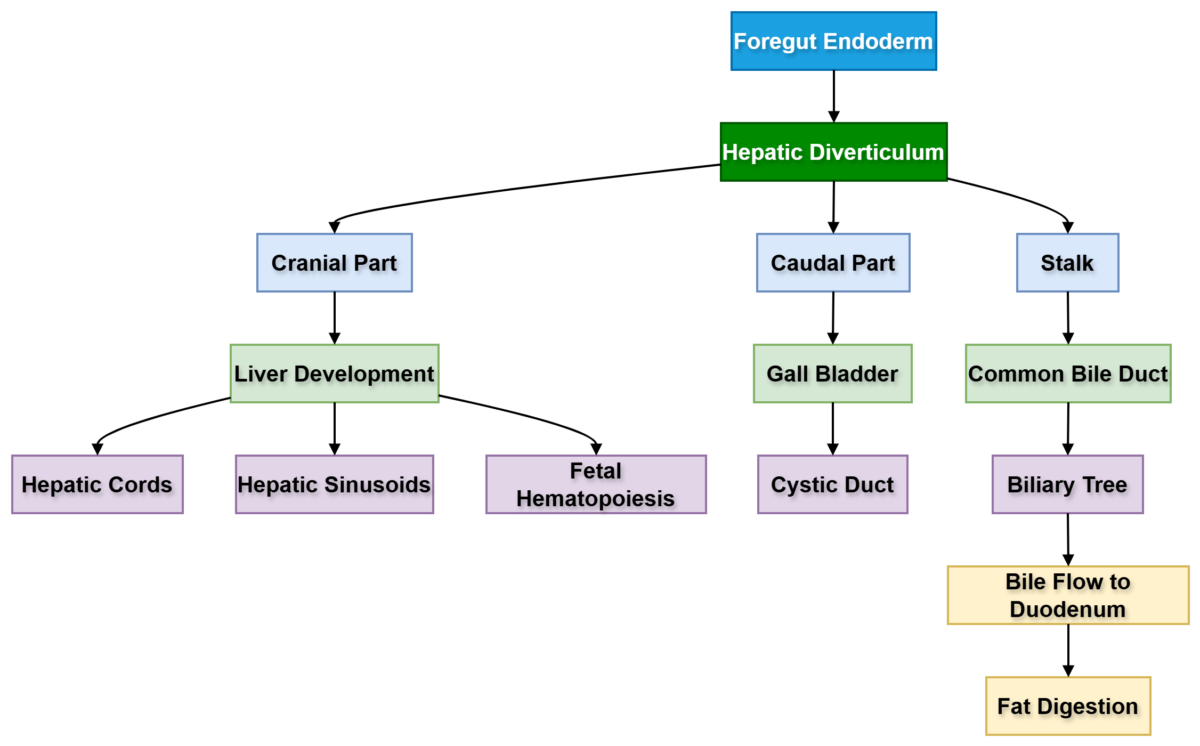
Concept Map — Hepatobiliary Development
⚙️ 4️⃣ Functional Flow
Development of Hepatobiliary System
- Foregut endoderm forms hepatic diverticulum.
- Diverticulum grows into septum transversum.
- Cranial part forms liver.
- Caudal part forms gall bladder.
- Stalk forms bile ducts.
- Hepatic cords branch.
- Vitelline veins form sinusoids.
- Biliary ducts recanalize.
- System connects to duodenum.
🩺 5️⃣ Clinical Correlation
Common clinical conditions:
- Biliary atresia
- Most important neonatal biliary disorder.
- Causes persistent neonatal jaundice.
- Accessory hepatic ducts
- Important during gall bladder surgery.
- Gall bladder agenesis
- Rare congenital anomaly.
- Congenital hepatic cysts
- Due to abnormal bile duct development.
📌 6️⃣ Summary Points
- Liver develops from hepatic diverticulum.
- Development begins in 4th week.
- Cranial part → Liver
- Caudal part → Gall bladder
- Stalk → Bile ducts
- Vitelline veins → Hepatic sinusoids
- Liver acts as fetal hematopoietic organ.
- Recanalization is essential for duct formation.
- Biliary atresia causes neonatal jaundice.
- Gall bladder arises from caudal diverticulum.