
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Digestion and absorption are essential biochemical and physiological processes by which food is broken down into absorbable molecules and delivered to body tissues. These processes mainly occur in the gastrointestinal tract, especially the small intestine, with major support from pancreatic secretions, bile, intestinal enzymes, and absorptive epithelial cells. Pancreatic enzymes digest carbohydrates, proteins, and fats, while bicarbonate neutralizes acidic chyme entering the duodenum. Absorbed nutrients are then used for energy production, tissue repair, growth, and metabolic homeostasis. Failure of digestion or absorption may lead to malnutrition, anemia, weight loss, diarrhea, and vitamin or mineral deficiencies. Understanding this topic is clinically important for conditions such as pancreatic insufficiency, celiac disease, iron deficiency anemia, vitamin B12 deficiency, and protein-energy malnutrition.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Digestion: Breakdown of large food molecules into smaller absorbable units.
- Absorption: Movement of digested nutrients from intestinal lumen into blood or lymph.
- Pancreatic juice: Alkaline digestive secretion containing enzymes and bicarbonate.
- Bicarbonate: Alkaline ion that neutralizes gastric acid in the duodenum.
- Micelles: Bile salt–fat complexes that help fat absorption.
- Chylomicrons: Lipoprotein particles that transport absorbed dietary fats through lymph.
- Basal Metabolic Rate (BMR): Minimum energy required to maintain basic body functions at rest.
- Protein-energy malnutrition: Deficiency of protein and energy intake causing growth failure, wasting, or edema.
- Adipose tissue homeostasis: Balance between fat storage and fat mobilization according to energy needs.
Essential Terminology
- Amylase: Enzyme that digests carbohydrates.
- Lipase: Enzyme that digests fats.
- Proteases: Enzymes that digest proteins.
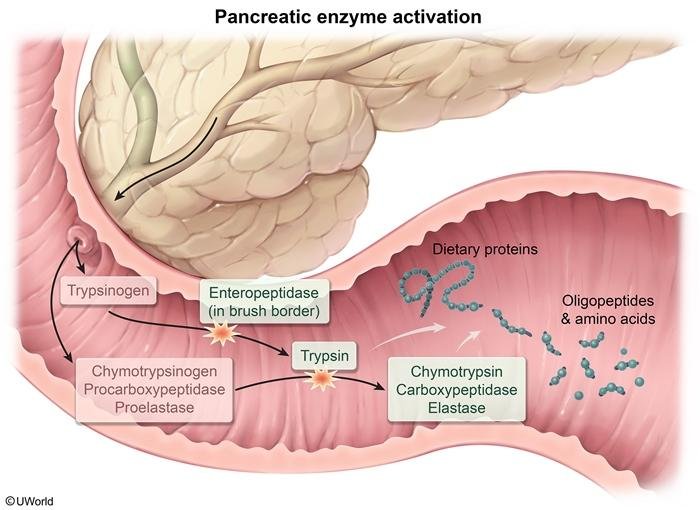
- Trypsinogen: Inactive precursor of trypsin.
- Enteropeptidase: Intestinal enzyme that activates trypsinogen.
- Intrinsic factor: Gastric protein needed for vitamin B12 absorption.
- Folate: Vitamin needed for DNA synthesis and red blood cell formation.
- Iron: Mineral required for hemoglobin synthesis.
- Anabolism: Building of body molecules.
- Catabolism: Breakdown of molecules to release energy.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. Pancreatic Secretions & Digestive Mechanisms
1.1: Composition of Pancreatic Secretions
🧠 CORE
- Pancreatic secretion is an alkaline digestive fluid released into the duodenum.
- It contains digestive enzymes and bicarbonate-rich fluid.
- Enzymes are mainly secreted by pancreatic acinar cells.
- Bicarbonate is mainly secreted by ductal epithelial cells.
- Major enzymes include amylase, lipase, trypsinogen, chymotrypsinogen, procarboxypeptidase, and nucleases.
- Bicarbonate neutralizes acidic chyme from the stomach.
- Pancreatic enzymes digest carbohydrates, fats, proteins, and nucleic acids.
- Pancreatic secretion works best in an alkaline pH.
- It is controlled mainly by secretin, cholecystokinin, and vagal stimulation.
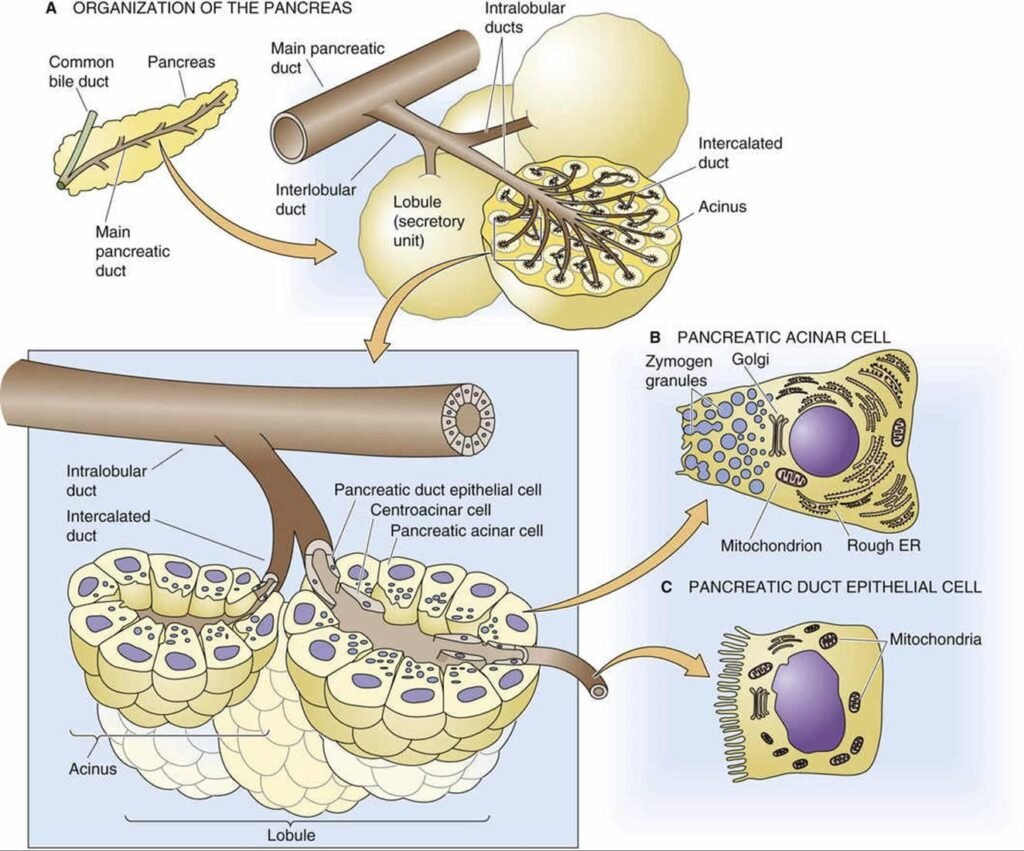
🔬 CONCEPT EXPLAINED
The pancreas has two major functional parts. The acinar cells produce enzyme-rich secretion, while the duct cells produce bicarbonate-rich watery secretion.
When acidic chyme enters the duodenum, the pancreas releases alkaline juice. This neutralizes gastric acid and creates a suitable pH for pancreatic enzymes.
Structure → Function:
- Acinar cells → enzyme production → digestion of nutrients.
- Duct cells → bicarbonate secretion → neutralization of acid.
- Pancreatic duct → delivers secretion into duodenum.
⚠️ IF DAMAGED
Pancreatic damage → reduced enzyme secretion → poor digestion of fats, proteins, and carbohydrates.
Poor fat digestion → steatorrhea → bulky, foul-smelling stools and weight loss.
Reduced bicarbonate → acidic duodenal environment → enzyme inactivation and mucosal irritation.
1.2: Mechanism of Pancreatic Enzyme Secretion
🧠 CORE
- Pancreatic enzymes are produced mainly by acinar cells.
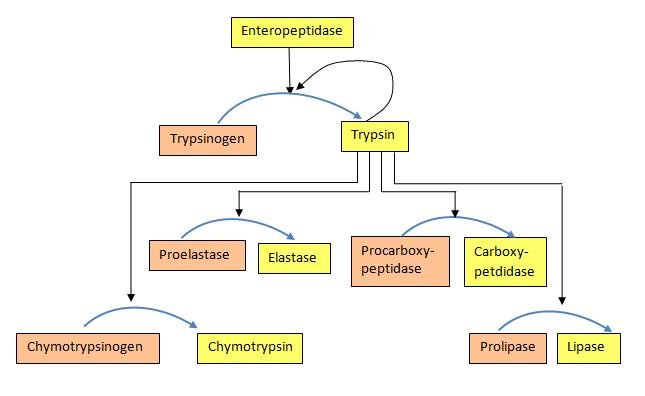
- Many protein-digesting enzymes are secreted as inactive zymogens.
- Trypsinogen is converted into trypsin by enteropeptidase.
- Trypsin activates other pancreatic protease precursors.
- Amylase and lipase are secreted in active forms.
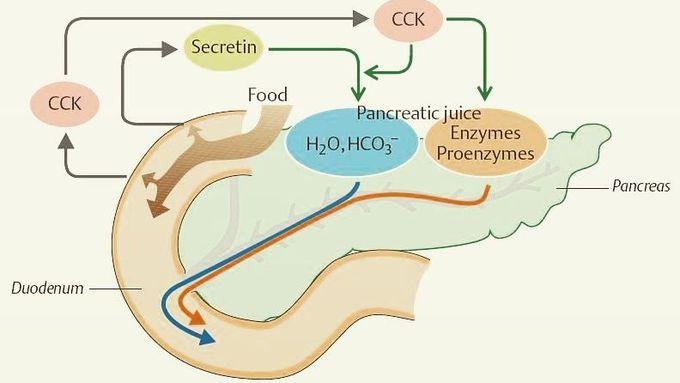
- Cholecystokinin strongly stimulates enzyme secretion.
- Vagal stimulation also increases enzyme secretion.
- Enzyme secretion increases after food enters the duodenum.
- Zymogen secretion protects the pancreas from self-digestion.
🔬 CONCEPT EXPLAINED
Food in the duodenum stimulates release of cholecystokinin (CCK) from intestinal mucosa. CCK acts on pancreatic acinar cells and causes enzyme-rich secretion.
Proteolytic enzymes are dangerous if active inside the pancreas. Therefore, they are secreted in inactive forms such as trypsinogen and chymotrypsinogen. In the duodenum, enteropeptidase activates trypsinogen into trypsin. Trypsin then activates other proteases.
This is a protective biochemical mechanism.
⚠️ IF DAMAGED
Premature activation of pancreatic enzymes inside the pancreas → autodigestion → acute pancreatitis.
Reduced enzyme secretion → maldigestion → diarrhea, weight loss, and nutritional deficiency.
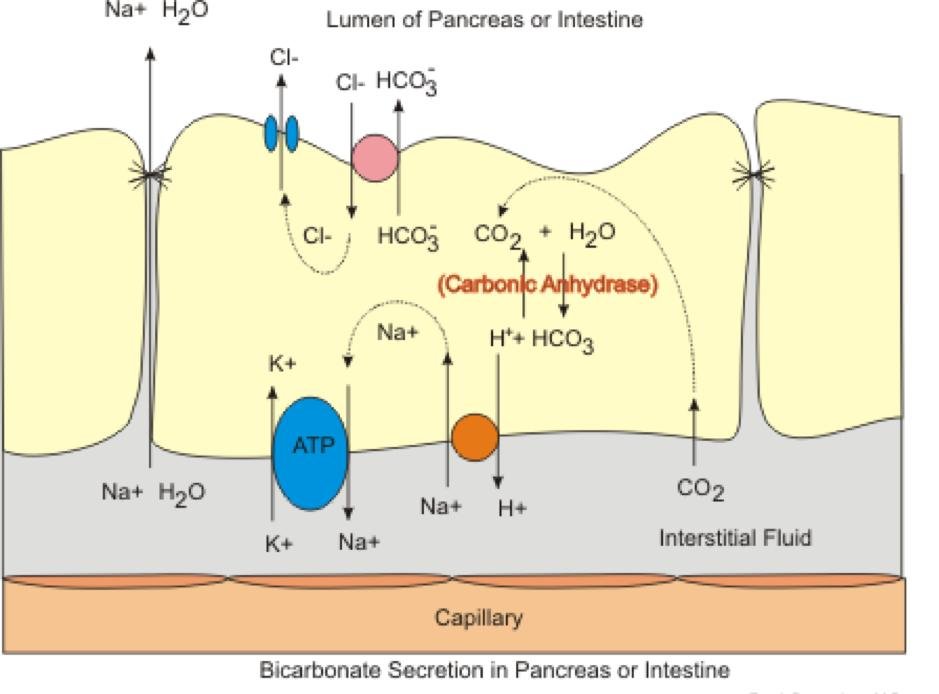
1.3: Mechanism of Synthesis of Bicarbonates
🧠 CORE
- Bicarbonate is secreted mainly by pancreatic duct cells.
- It neutralizes acidic chyme entering the duodenum.
- Secretin is the major hormone stimulating bicarbonate secretion.
- Carbon dioxide and water form carbonic acid inside duct cells.
- Carbonic acid dissociates into hydrogen ions and bicarbonate.
- Bicarbonate is transported into duct lumen.
- Hydrogen ions move into blood in exchange for sodium.
- Water follows electrolytes, forming alkaline pancreatic juice.
- Bicarbonate protects duodenal mucosa and optimizes enzyme activity.
🔬 CONCEPT EXPLAINED
When acidic chyme enters the duodenum, intestinal cells release secretin. Secretin stimulates pancreatic duct cells to secrete bicarbonate.
Inside duct cells:
- CO₂ combines with water.
- Carbonic acid is formed.
- Carbonic acid splits into H⁺ and HCO₃⁻.
- Bicarbonate enters pancreatic duct.
- Alkaline pancreatic juice reaches the duodenum.
This creates an alkaline environment for pancreatic enzymes.
⚠️ IF DAMAGED
Reduced bicarbonate secretion → duodenal acidity persists.
Persistent acidity → pancreatic enzymes fail to work properly → impaired digestion.
Acid injury may also damage duodenal mucosa.
2. Digestion of Nutrients
2.1: Digestion of Fats
🧠 CORE
- Dietary fats are mainly triglycerides.
- Fat digestion occurs mainly in the small intestine.
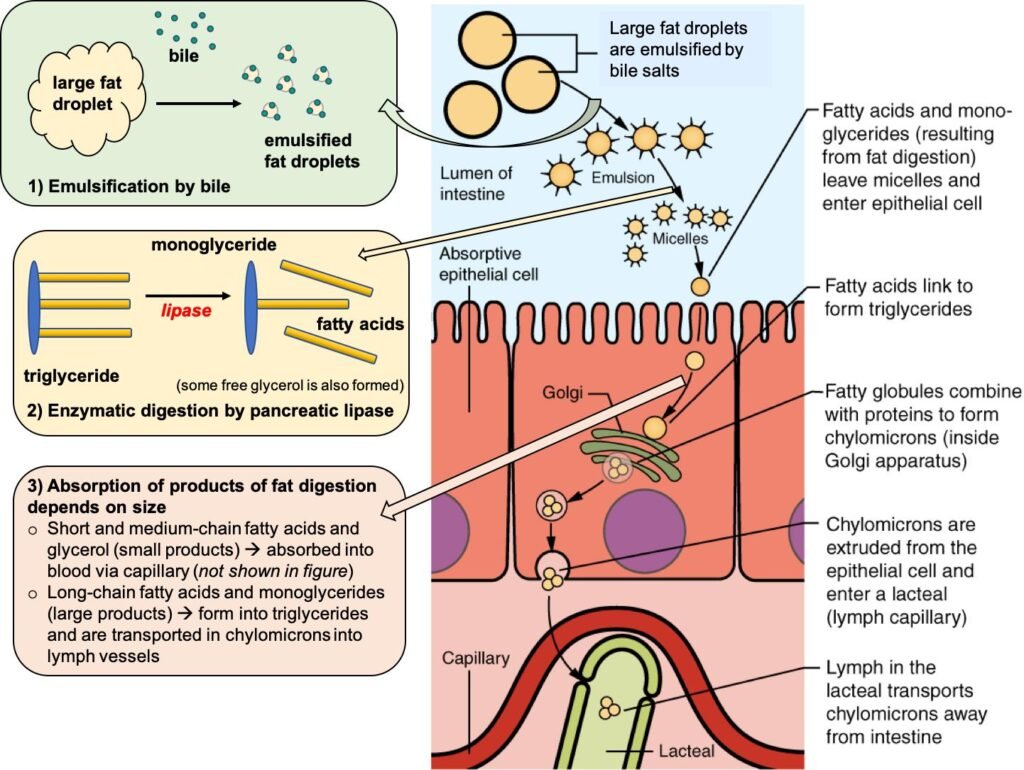
- Bile salts emulsify large fat droplets.
- Pancreatic lipase digests triglycerides.
- Products include free fatty acids and monoglycerides.
- Micelles help transport lipid digestion products to intestinal cells.
- Fat digestion requires bile, pancreatic lipase, and alkaline pH.
- Fat-soluble vitamins are absorbed along with dietary fats.
🔬 CONCEPT EXPLAINED
Fat is water-insoluble, so it cannot mix easily with intestinal fluid. Bile salts break large fat globules into smaller droplets. This process is called emulsification.
Pancreatic lipase then acts on triglycerides and breaks them into monoglycerides and fatty acids. These products combine with bile salts to form micelles, which deliver fat molecules to the intestinal absorptive surface.
⚠️ IF DAMAGED
Lack of bile or pancreatic lipase → fat maldigestion.
Fat maldigestion → steatorrhea, weight loss, and deficiency of vitamins A, D, E, and K.
2.2: Digestion of Proteins
🧠 CORE
- Protein digestion begins in the stomach and continues in the small intestine.
- Pancreatic proteases are essential for protein digestion.
- Proteases are secreted as inactive zymogens.
- Trypsinogen is activated by enteropeptidase.
- Trypsin activates other proteases.
- Proteins are broken into peptides and amino acids.
- Brush border enzymes further digest small peptides.
- Amino acids and small peptides are absorbed by enterocytes.
🔬 CONCEPT EXPLAINED
Proteins are large molecules that must be broken down before absorption. Pancreatic proteases such as trypsin, chymotrypsin, and carboxypeptidase break proteins into smaller peptides.
Brush border enzymes on intestinal epithelial cells further break peptides into amino acids and small peptides. These are then absorbed into portal blood.
⚠️ IF DAMAGED
Reduced protease activity → impaired protein digestion.
This may cause poor growth, muscle wasting, hypoalbuminemia, and nutritional deficiency.
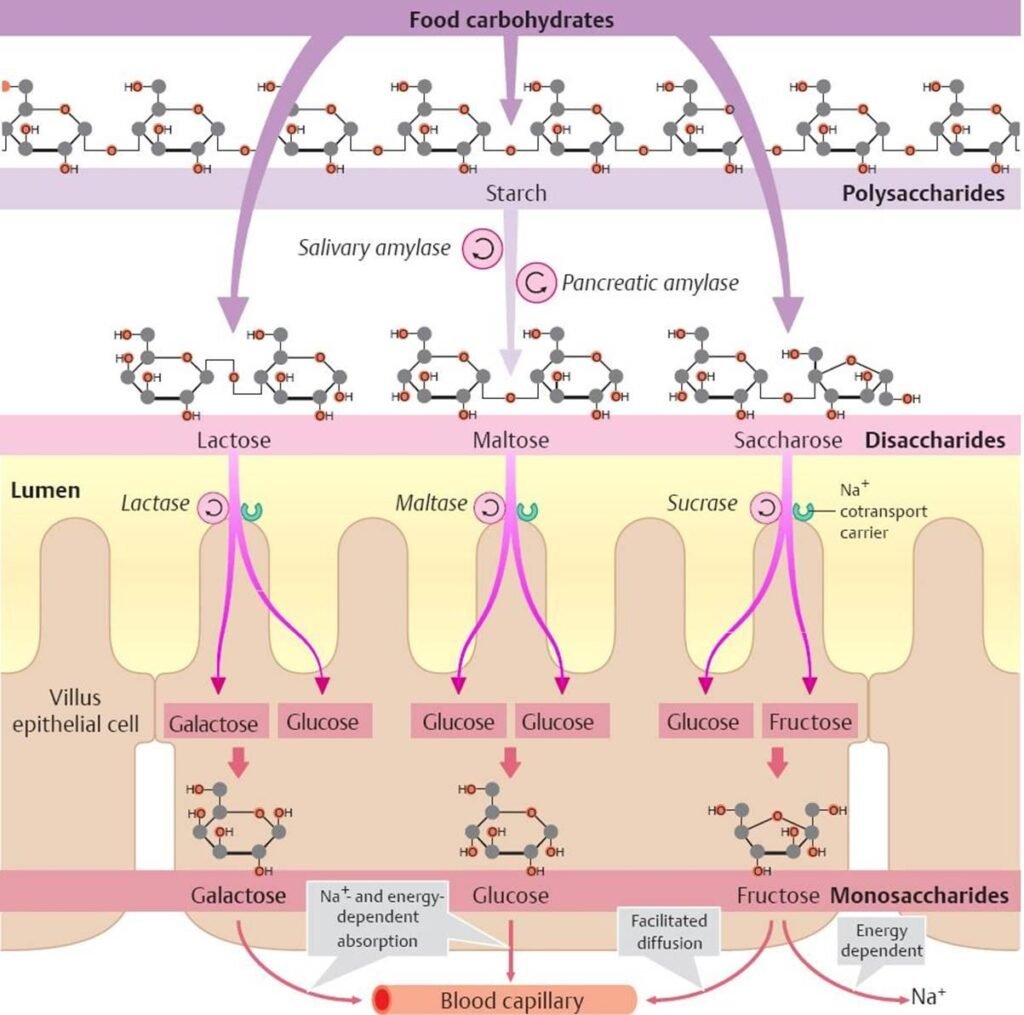
2.3: Digestion of Carbohydrates
🧠 CORE
- Carbohydrate digestion begins in the mouth and continues in the small intestine.
- Pancreatic amylase digests starch.
- Starch is broken into maltose, maltotriose, and dextrins.
- Brush border enzymes complete carbohydrate digestion.
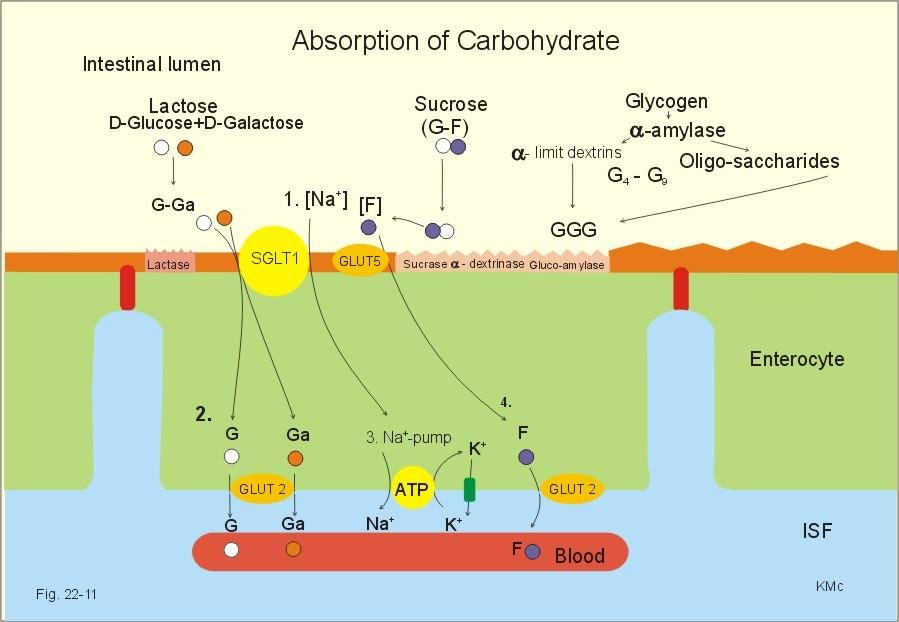
- Final products are glucose, galactose, and fructose.
- Only monosaccharides are absorbed.
- Glucose is the major energy source for many tissues.
- Carbohydrate digestion depends on enzyme activity at intestinal surface.
🔬 CONCEPT EXPLAINED
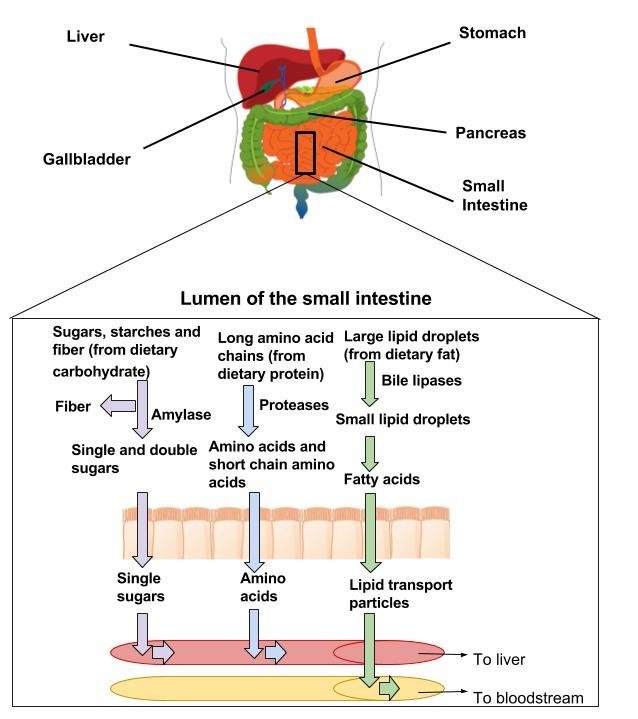
Dietary carbohydrates are mainly starch, disaccharides, and some fiber. Pancreatic amylase breaks starch into smaller carbohydrate units.
Brush border enzymes such as maltase, sucrase, and lactase convert these into monosaccharides. These monosaccharides are then absorbed into blood.
⚠️ IF DAMAGED
Brush border enzyme deficiency → carbohydrate malabsorption.
Example: lactase deficiency → lactose intolerance → bloating, abdominal cramps, and diarrhea.
3. Absorption of Nutrients
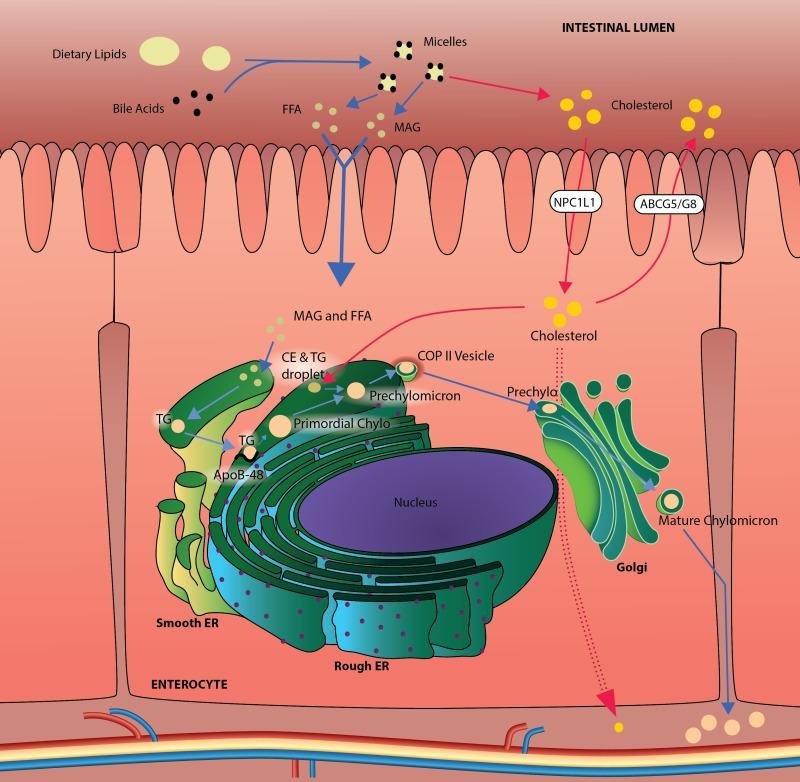
3.1: Absorption of Fats
🧠 CORE
- Fat absorption occurs mainly in the small intestine.
- Micelles deliver fatty acids and monoglycerides to enterocytes.
- Lipids enter intestinal epithelial cells.
- Inside enterocytes, triglycerides are reformed.
- Triglycerides combine with proteins to form chylomicrons.
- Chylomicrons enter lymphatic lacteals.
- They later reach blood circulation.
- Short-chain fatty acids may enter portal blood directly.
🔬 CONCEPT EXPLAINED
Fat digestion products are carried by micelles to the intestinal brush border. Fatty acids and monoglycerides enter enterocytes, where they are reassembled into triglycerides.
These triglycerides are packed into chylomicrons. Because chylomicrons are large, they enter lymphatic vessels called lacteals rather than directly entering blood capillaries.
⚠️ IF DAMAGED
Fat absorption failure → steatorrhea.
Long-term fat malabsorption → deficiency of fat-soluble vitamins A, D, E, and K.
3.2: Absorption of Proteins
🧠 CORE
- Proteins are absorbed mainly as amino acids and small peptides.
- Absorption occurs in the small intestine.
- Amino acids use specific transport systems.
- Some transport is sodium-dependent.
- Small peptides may be absorbed and digested inside enterocytes.
- Absorbed amino acids enter portal blood.
- They are transported to the liver.
- Amino acids are used for protein synthesis and energy when needed.
🔬 CONCEPT EXPLAINED
After digestion, amino acids and small peptides move across enterocytes by carrier-mediated transport. Many amino acid transporters depend on sodium gradients.
Once absorbed, amino acids enter portal circulation and reach the liver. The liver regulates their use for protein synthesis, metabolism, or energy production.
⚠️ IF DAMAGED
Protein absorption failure → reduced amino acid availability.
This may cause muscle wasting, poor healing, immune weakness, and growth failure.
3.3: Absorption of Carbohydrates
🧠 CORE
- Carbohydrates are absorbed as monosaccharides.
- Glucose and galactose are absorbed by sodium-dependent transport.
- Fructose is absorbed by facilitated diffusion.
- Monosaccharides leave enterocytes into portal blood.
- The liver receives absorbed carbohydrates first.
- Glucose is used for ATP production.
- Excess glucose may be stored as glycogen or converted to fat.
- Efficient absorption depends on healthy intestinal mucosa.
🔬 CONCEPT EXPLAINED
Only monosaccharides can be absorbed. Glucose and galactose enter enterocytes along with sodium using specific transporters. Fructose uses facilitated diffusion.
After entering enterocytes, monosaccharides pass into portal blood and reach the liver. The liver maintains blood glucose balance.
⚠️ IF DAMAGED
Carbohydrate malabsorption → osmotic diarrhea.
Unabsorbed carbohydrates are fermented by intestinal bacteria → gas, bloating, and abdominal discomfort.
4. Absorption of Vitamins & Minerals
4.1: Absorption of Iron
🧠 CORE
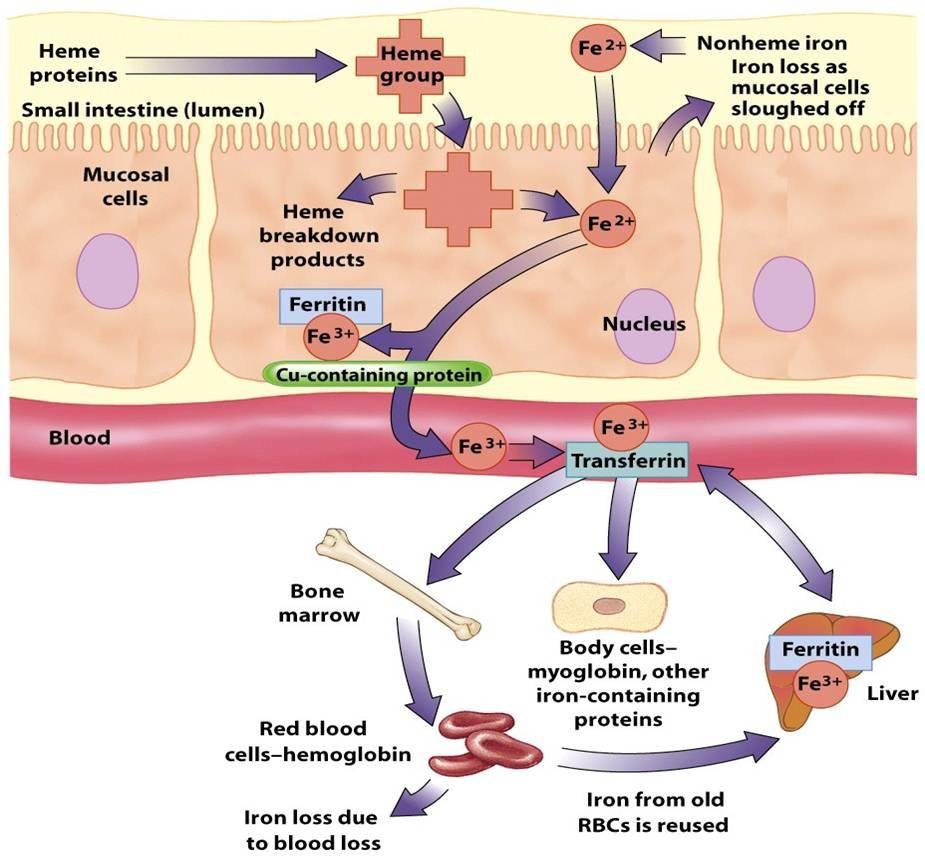
- Iron is mainly absorbed in the duodenum and upper jejunum.
- Dietary iron exists as heme and non-heme iron.
- Heme iron is better absorbed.
- Vitamin C enhances non-heme iron absorption.
- Iron is transported inside enterocytes.
- It may be stored as ferritin or transported in blood.
- Transferrin carries iron in plasma.
- Iron is essential for hemoglobin synthesis.
- Iron absorption increases when body iron stores are low.
🔬 CONCEPT EXPLAINED
Iron absorption is tightly regulated because the body has limited ability to excrete excess iron. Enterocytes absorb iron and either store it as ferritin or release it into blood.
In blood, iron binds to transferrin and is transported mainly to bone marrow for hemoglobin synthesis.
⚠️ IF DAMAGED
Reduced iron absorption → iron deficiency anemia.
Clinical effects include pallor, fatigue, weakness, shortness of breath, and poor concentration.
4.2: Absorption of Vitamin B12
🧠 CORE
- Vitamin B12 is needed for DNA synthesis and nerve function.
- It is obtained from animal-source foods.
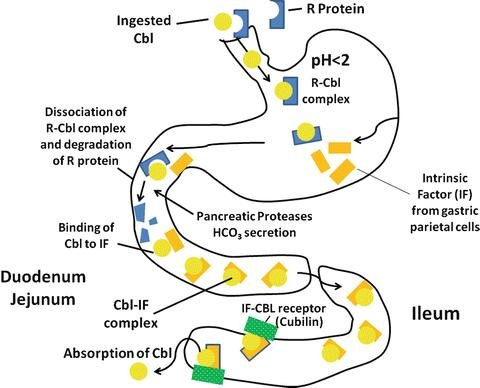
- B12 binds intrinsic factor from stomach parietal cells.
- B12-intrinsic factor complex is absorbed in terminal ileum.
- B12 deficiency causes megaloblastic anemia.
- It may also cause neurological symptoms.
- Absorption requires stomach, pancreas, and terminal ileum function.
- Long-term deficiency may cause irreversible nerve damage.
🔬 CONCEPT EXPLAINED
Vitamin B12 from food is released during digestion. It eventually binds to intrinsic factor, which is produced by gastric parietal cells.
The B12-intrinsic factor complex travels to the terminal ileum, where it binds to receptors and is absorbed.
⚠️ IF DAMAGED
Intrinsic factor deficiency or terminal ileum disease → B12 malabsorption.
B12 deficiency → megaloblastic anemia plus neurological problems such as numbness, tingling, and gait disturbance.
4.3: Absorption of Folate
🧠 CORE
- Folate is needed for DNA synthesis.
- It is important for rapidly dividing cells.
- Folate is mainly absorbed in the proximal small intestine.
- Deficiency affects red blood cell formation.
- Folate deficiency causes megaloblastic anemia.
- Unlike B12 deficiency, folate deficiency usually does not cause neurological damage.
- Folate requirement increases during pregnancy.
- Folate is important for fetal neural tube development.
🔬 CONCEPT EXPLAINED
Folate from diet is absorbed mainly in the proximal small intestine. It participates in one-carbon transfer reactions needed for DNA synthesis.
Cells with rapid turnover, especially bone marrow cells, are highly affected by folate deficiency.
⚠️ IF DAMAGED
Folate deficiency → impaired DNA synthesis → megaloblastic anemia.
In pregnancy, folate deficiency increases risk of neural tube defects in fetus.
5. Energy Metabolism & Nutritional Requirements
5.1: Daily Energy Requirement
🧠 CORE
- Daily energy requirement is the energy needed to maintain body functions and activity.
- It includes BMR, physical activity, and thermic effect of food.
- Energy is measured in kilocalories.
- Carbohydrates and proteins provide about 4 kcal/g.
- Fats provide about 9 kcal/g.
- Energy needs vary with age, sex, body size, activity, pregnancy, and illness.
- Energy balance maintains body weight.
- Excess energy intake leads to fat storage.
- Low energy intake leads to weight loss and malnutrition.
🔬 CONCEPT EXPLAINED
The body needs continuous energy for basal functions such as breathing, circulation, ion transport, temperature regulation, and cellular metabolism.
Daily energy requirement is not the same for everyone. A physically active person, growing child, pregnant woman, or febrile patient has higher energy needs.
⚠️ IF DAMAGED
Energy deficiency → weight loss, fatigue, poor immunity, and growth failure.
Chronic excess energy intake → obesity, insulin resistance, and metabolic disease.
5.2: Basal Metabolic Rate (BMR)
🧠 CORE
- BMR is the minimum energy expenditure at rest.
- It supports vital functions such as respiration, circulation, and temperature maintenance.
- It is measured under resting, fasting, and thermoneutral conditions.
- Major contributors include liver, brain, heart, kidneys, and skeletal muscle.
- Thyroid hormones strongly influence BMR.
- BMR is higher in children and lower in elderly people.
- It is affected by body size, lean body mass, hormones, fever, and nutrition.
- BMR forms the largest part of daily energy expenditure.
🔬 CONCEPT EXPLAINED
Even at complete rest, the body continuously uses ATP. Cells maintain ion gradients, synthesize essential molecules, pump blood, breathe, and regulate temperature.
Organs with high metabolic activity consume more energy. Thyroid hormones increase cellular metabolism and oxygen consumption, so they increase BMR.
⚠️ IF DAMAGED
Very low BMR may cause weight gain, fatigue, cold intolerance, and slow metabolism.
Very high BMR may cause weight loss, heat intolerance, sweating, and increased appetite.
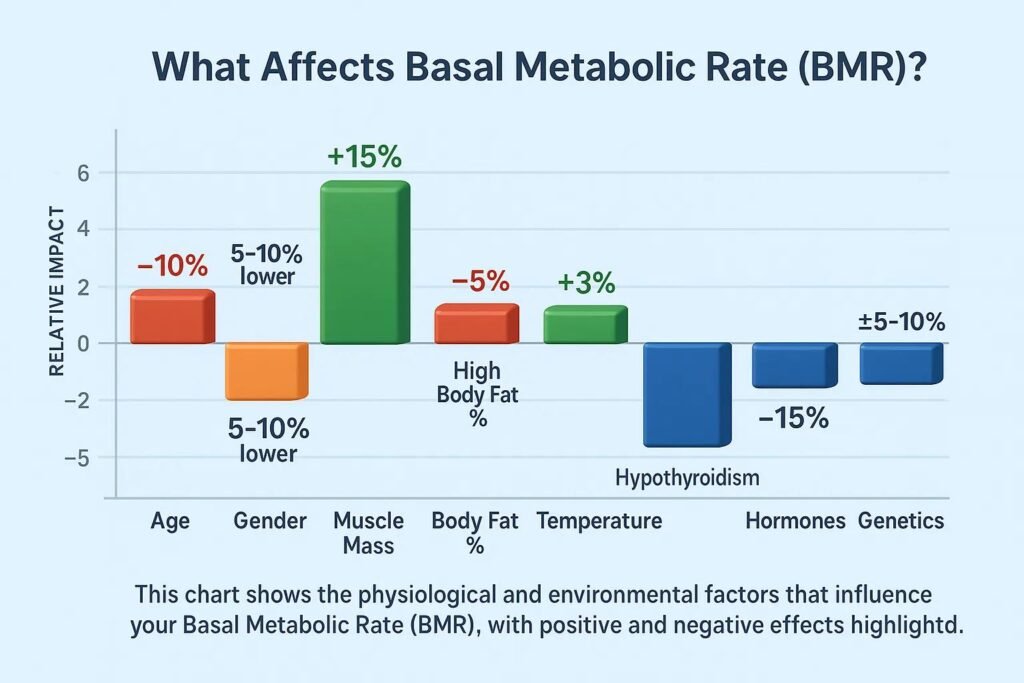
5.3: Causes of High and Low BMR
🧠 CORE
- BMR increases in hyperthyroidism.
- Fever increases BMR.
- Growth, pregnancy, and lactation increase energy demand.
- Stress hormones may increase metabolic rate.
- BMR decreases in hypothyroidism.
- Starvation reduces BMR as an adaptive mechanism.
- Aging usually lowers BMR.
- Loss of muscle mass reduces BMR.
- Malnutrition decreases metabolic activity.
🔬 CONCEPT EXPLAINED
BMR changes according to hormonal status and body energy needs. Thyroid hormones increase metabolic enzyme activity and oxygen use. Fever increases cellular reactions and energy consumption.
During starvation, the body lowers BMR to conserve energy. This protects survival but reduces activity, growth, and reproductive function.
⚠️ IF DAMAGED
High BMR → excessive energy use → weight loss and muscle wasting.
Low BMR → reduced energy use → weight gain tendency, lethargy, and cold intolerance.
5.4: Daily Requirement of Vitamins
🧠 CORE
- Vitamins are required in small amounts for normal metabolism.
- They do not provide energy directly.
- Many act as coenzymes.
- Fat-soluble vitamins are A, D, E, and K.
- Water-soluble vitamins include B-complex and vitamin C.
- Deficiency causes specific clinical syndromes.
- Excess fat-soluble vitamins may accumulate and become toxic.
- Requirements increase in growth, pregnancy, illness, and malnutrition.
- Balanced diet usually provides adequate vitamins.
🔬 CONCEPT EXPLAINED
Vitamins support enzyme function, growth, immunity, blood formation, antioxidant defense, and bone health.
Water-soluble vitamins are not stored in large amounts, so regular intake is required. Fat-soluble vitamins are stored in liver and adipose tissue.
⚠️ IF DAMAGED
Vitamin deficiency → impaired metabolism and organ dysfunction.
Examples:
- Vitamin D deficiency → rickets or osteomalacia.
- Vitamin K deficiency → bleeding tendency.
- Vitamin C deficiency → poor wound healing and bleeding gums.
- B-complex deficiency → anemia, neuropathy, or dermatitis.
5.5: Mineral Requirements
🧠 CORE
- Minerals are inorganic nutrients required for body function.
- Major minerals include calcium, phosphorus, sodium, potassium, chloride, and magnesium.
- Trace elements include iron, zinc, iodine, copper, selenium, and fluoride.
- Calcium and phosphorus are important for bones and teeth.
- Sodium and potassium maintain fluid balance and nerve function.
- Iodine is required for thyroid hormone synthesis.
- Iron is needed for hemoglobin.
- Zinc supports growth, immunity, and wound healing.
- Mineral imbalance may affect nerves, muscles, blood, and bones.
🔬 CONCEPT EXPLAINED
Minerals act as structural components, electrolytes, enzyme cofactors, and functional parts of hormones and proteins.
For example, calcium supports bone strength and muscle contraction, while iodine supports thyroid hormone synthesis and therefore metabolic rate.
⚠️ IF DAMAGED
Mineral deficiency → functional failure.
Examples:
- Iron deficiency → anemia.
- Iodine deficiency → goiter and hypothyroidism.
- Calcium deficiency → bone weakness and muscle irritability.
- Zinc deficiency → poor wound healing and growth delay.
6. Nutritional Disorders & Metabolic Homeostasis
6.1: Protein-Energy Malnutrition
🧠 CORE
- Protein-energy malnutrition results from inadequate intake of protein, energy, or both.
- It commonly affects children but may occur at any age.
- Marasmus is mainly severe energy deficiency.
- Kwashiorkor is mainly protein deficiency with edema.
- PEM causes growth failure and muscle wasting.
- It weakens immunity.
- It delays wound healing.
- It may cause anemia, diarrhea, and infections.
- It is clinically important in public health and pediatrics.
🔬 CONCEPT EXPLAINED
Protein and energy are required for growth, tissue repair, enzyme synthesis, immune function, and plasma protein production.
In severe energy deficiency, the body uses fat and muscle stores for energy, causing wasting. In protein deficiency, albumin synthesis falls, reducing plasma oncotic pressure and causing edema.
⚠️ IF DAMAGED
Low protein intake → low albumin → reduced oncotic pressure → edema.
Low energy intake → fat and muscle breakdown → severe wasting and weakness.
Poor immunity → recurrent infections.
6.2: Adipose Tissue Homeostasis
🧠 CORE
- Adipose tissue stores energy as triglycerides.
- It releases fatty acids during fasting.
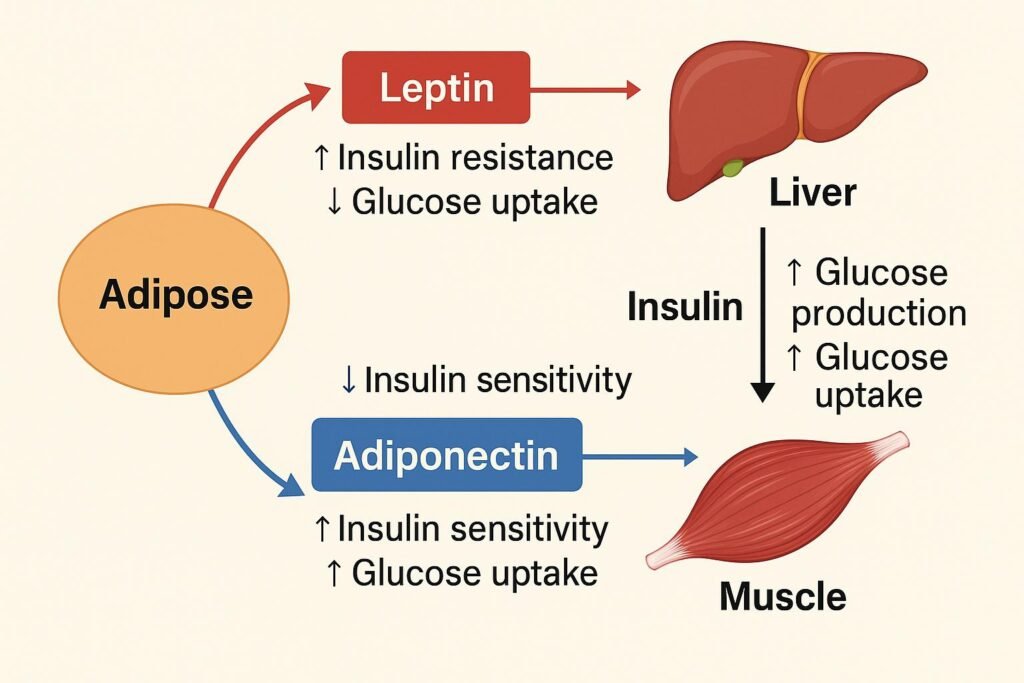
- It acts as an endocrine organ.
- Insulin promotes fat storage.
- Glucagon and catecholamines promote fat breakdown.
- Adipose tissue secretes adipokines such as leptin.
- Leptin signals energy stores to the brain.
- Balance between storage and mobilization maintains energy homeostasis.
- Dysfunction contributes to obesity and metabolic disease.
🔬 CONCEPT EXPLAINED
Adipose tissue is not only a fat storage site. It actively regulates metabolism.
After meals, insulin promotes glucose uptake and fat storage. During fasting, hormonal signals stimulate lipolysis, releasing fatty acids for energy.
Structure → Function:
- Adipocytes → triglyceride storage.
- Blood supply → transport of fatty acids and hormones.
- Adipokines → communication with brain, liver, and muscles.
⚠️ IF DAMAGED
Excess adipose tissue → insulin resistance, inflammation, fatty liver, and metabolic syndrome.
Very low adipose stores → poor energy reserve, hormonal disturbance, and weakness.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Pancreas
- Acinar cells → secrete enzymes → digestion of proteins, fats, and carbohydrates.
- Duct cells → secrete bicarbonate → neutralize acid and protect duodenum.
- Outcome: Efficient digestion in alkaline intestinal environment.
Small Intestinal Mucosa
- Villi and microvilli → increase surface area → improve absorption.
- Brush border enzymes → complete digestion → absorbable final products.
- Outcome: Nutrients enter blood or lymph efficiently.
Liver
- Portal blood supply → receives absorbed nutrients → metabolic processing.
- Outcome: Blood glucose, amino acids, vitamins, and minerals are regulated.
Lymphatics
- Lacteals → absorb chylomicrons → transport dietary fats.
- Outcome: Large lipid particles bypass portal blood initially and enter systemic circulation via lymph.
Adipose Tissue
- Adipocytes → store triglycerides → energy reserve.
- Hormone-sensitive lipolysis → releases fatty acids during fasting.
- Outcome: Maintains energy supply between meals.
🩺 5️⃣ Clinical Correlation
1. Pancreatic Insufficiency
- Reduced pancreatic enzyme secretion.
- Causes maldigestion, especially of fats.
- Features include steatorrhea, weight loss, and fat-soluble vitamin deficiency.
2. Acute Pancreatitis
- Premature activation of pancreatic enzymes inside pancreas.
- Causes pancreatic autodigestion.
- Presents with severe abdominal pain and raised pancreatic enzymes.
3. Lactose Intolerance
- Due to lactase deficiency.
- Lactose remains undigested in intestine.
- Causes bloating, cramps, flatulence, and osmotic diarrhea.
4. Iron Deficiency Anemia
- Commonly due to poor intake, blood loss, or reduced absorption.
- Causes microcytic hypochromic anemia.
- Features include pallor, fatigue, and weakness.
5. Vitamin B12 Deficiency
- May occur due to intrinsic factor deficiency or terminal ileum disease.
- Causes megaloblastic anemia.
- Neurological symptoms may occur.
6. Folate Deficiency
- Causes megaloblastic anemia.
- Important in pregnancy because deficiency increases risk of neural tube defects.
- No typical neurological damage unlike B12 deficiency.
7. Protein-Energy Malnutrition
- Marasmus: severe wasting due to energy deficiency.
- Kwashiorkor: edema due to protein deficiency and low albumin.
- Causes poor immunity, growth failure, and recurrent infections.
8. Obesity and Adipose Dysfunction
- Excess adipose tissue causes metabolic imbalance.
- Associated with insulin resistance, fatty liver, and metabolic syndrome.
📌 6️⃣ Summary Points
- Pancreatic acinar cells secrete digestive enzymes; duct cells secrete bicarbonate.
- Secretin mainly stimulates bicarbonate secretion.
- CCK mainly stimulates pancreatic enzyme secretion.
- Proteolytic enzymes are secreted as inactive zymogens to prevent pancreatic autodigestion.
- Enteropeptidase converts trypsinogen into trypsin.
- Bile salts emulsify fats and help micelle formation.
- Fat is absorbed through lymph mainly as chylomicrons.
- Carbohydrates are absorbed only as monosaccharides.
- Vitamin B12 requires intrinsic factor and terminal ileum for absorption.
- Iron is mainly absorbed in the duodenum and is transported by transferrin.
- BMR is strongly influenced by thyroid hormones and lean body mass.
- Protein-energy malnutrition causes wasting, edema, poor immunity, and growth failure.