
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Peptic ulcer disease and pancreatic disorders are among the most common gastrointestinal conditions encountered in clinical practice. These diseases primarily affect the stomach, duodenum, and pancreas, organs responsible for digestion and protection of the gastrointestinal mucosa. Understanding how gastric acid, mucosal defense, inflammation, and pancreatic enzymes interact is essential for diagnosing and managing these disorders. Conditions such as peptic ulcer disease, GERD, gastric cancer, and acute pancreatitis are clinically important due to their complications like bleeding, perforation, and systemic inflammation. Pharmacological therapy plays a major role in treatment by reducing acid secretion and protecting mucosa. This topic integrates pathology, pharmacology, and clinical medicine to help students understand disease mechanisms and management logically.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Peptic Ulcer Disease (PUD): A break in gastric or duodenal mucosa caused by acid-pepsin digestion.
- GERD (Gastroesophageal Reflux Disease): Backflow of gastric contents into esophagus causing mucosal injury.
- Acute Pancreatitis: Acute inflammation of pancreas due to premature activation of pancreatic enzymes.
- Gastric Cancer: Malignant tumor arising from gastric epithelium.
- Gastric Lavage: Procedure used to wash stomach contents for diagnosis or treatment.
- Anti-ulcer Drugs: Medications that reduce gastric acidity or protect gastric mucosa.
Essential Terminology
- HCl: Gastric acid secreted by parietal cells
- Pepsin: Protein-digesting enzyme
- Mucosal Barrier: Protective layer preventing acid injury
- Helicobacter pylori: Bacteria associated with peptic ulcers
- LES: Lower esophageal sphincter
- Trypsin: Pancreatic enzyme causing tissue digestion
Basic Overview
- Gastric mucosa is protected by mucus, bicarbonate, and blood supply.
- Ulcers occur when acid exceeds mucosal protection.
- Pancreatitis occurs when digestive enzymes activate inside pancreas.
- Anti-ulcer drugs reduce acid or enhance protection.
- Early recognition prevents complications like bleeding or perforation.
🔹 3️⃣ Core Learning — Curriculum Coverage
PEPTIC ULCER DISEASE
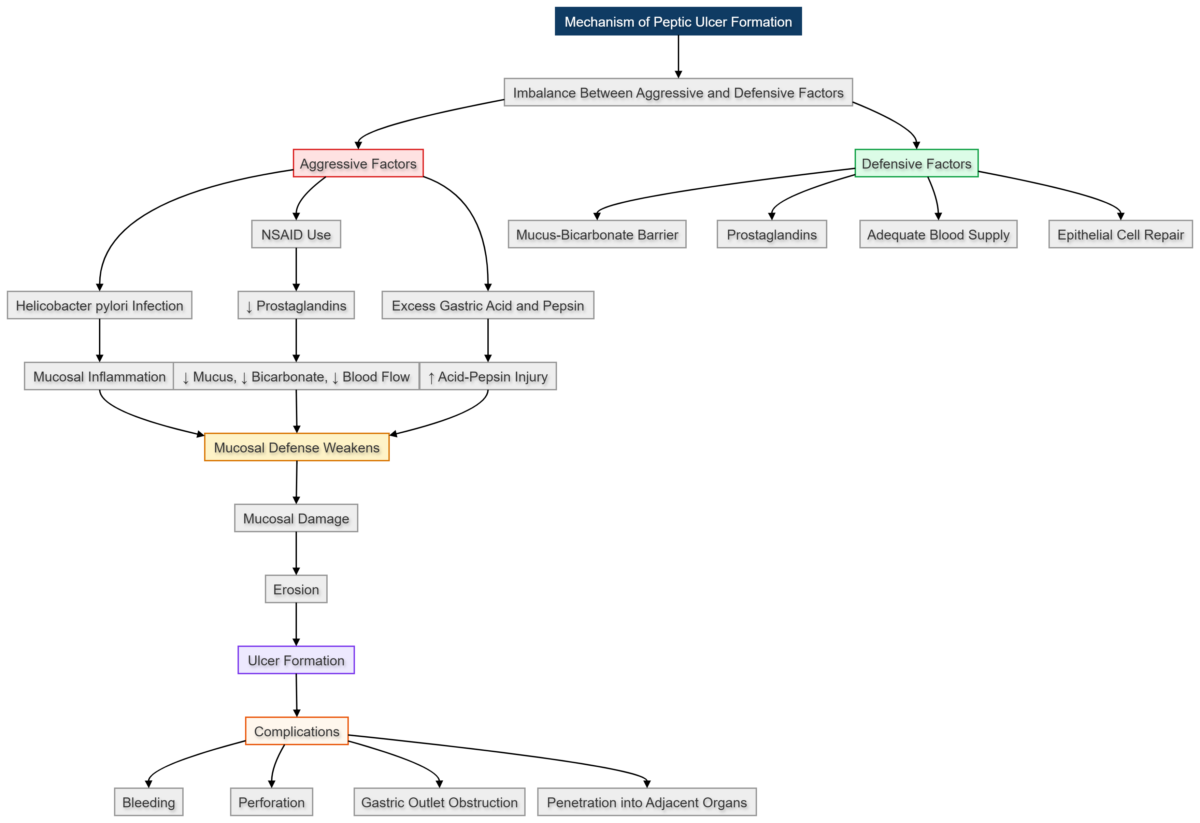
Mechanism of Peptic Ulcer Formation
🧠 CORE
- Peptic ulcer is erosion of gastric or duodenal mucosa.
- Caused by imbalance between acid secretion and mucosal defense.
- Major causes:
- Helicobacter pylori infection
- NSAID use
- Excess acid secretion
- Common sites:
- Duodenum (most common)
- Gastric antrum
- Pepsin and acid digest mucosal tissue.
- Reduced mucus protection increases injury risk.
🔬 CONCEPT EXPLAINED
The stomach produces hydrochloric acid and pepsin for digestion. Normally, the mucosal barrier protects the stomach lining using mucus and bicarbonate secretion. Helicobacter pylori damages mucosal cells and reduces bicarbonate secretion, weakening protection. NSAIDs reduce prostaglandin synthesis, leading to decreased mucus production and reduced blood flow. As protection weakens, acid penetrates mucosa, causing tissue destruction and ulcer formation.
Structure → Function
- Parietal cells → Acid secretion
- Mucous cells → Protection
- Failure of balance → Ulcer formation
⚠️ IF DAMAGED
Cause → Effect:
- H. pylori infection → Mucosal inflammation → Ulcer formation
- NSAID use → Reduced prostaglandins → Loss of protection
- Excess acid → Tissue erosion → Ulcer
Stages of Peptic Ulcer
🧠 CORE
- Ulcers develop in progressive stages.
- Stages include:
- Inflammation
- Erosion
- Ulceration
- Healing or fibrosis
- Tissue damage increases gradually.
- Chronic ulcers may develop scar tissue.
- Healing occurs with reduced acid exposure.
🔬 CONCEPT EXPLAINED
Initially, inflammation begins in superficial mucosa. Continued acid exposure leads to erosion of mucosal layers. As damage deepens, ulcers penetrate muscular layers. During healing, fibrosis forms scar tissue, which may distort gastric structure.
⚠️ IF DAMAGED
- Repeated injury → Chronic ulcer
- Fibrosis → Gastric outlet obstruction
- Deep penetration → Bleeding or perforation
Complications of Peptic Ulcer
🧠 CORE
Major complications include:
- Hemorrhage (most common)
- Perforation
- Gastric outlet obstruction
- Penetration into adjacent organs
- Peritonitis
- Chronic pain
🔬 CONCEPT EXPLAINED
Deep ulcers erode blood vessels causing bleeding. If the ulcer perforates through the stomach wall, gastric contents enter the peritoneal cavity causing peritonitis. Scar formation near pylorus leads to narrowing and obstruction of food passage.
⚠️ IF DAMAGED
- Vessel erosion → Hematemesis or melena
- Wall perforation → Acute abdomen
- Pyloric narrowing → Persistent vomiting
GERD (Gastroesophageal Reflux Disease)
🧠 CORE
- GERD occurs due to reflux of gastric acid into esophagus.
- Caused by:
- Weak LES
- Hiatal hernia
- Increased abdominal pressure
- Leads to esophageal inflammation.
- Symptoms include:
- Heartburn
- Regurgitation
- Chest discomfort
🔬 CONCEPT EXPLAINED
Lower esophageal sphincter normally prevents reflux. When LES tone decreases, gastric acid flows backward into esophagus. Unlike stomach, esophageal mucosa lacks strong protective mucus, leading to mucosal injury.
⚠️ IF DAMAGED
- Chronic reflux → Esophagitis
- Repeated injury → Barrett esophagus
- Long-term damage → Cancer risk
Gastric Cancer
🧠 CORE
- Malignant tumor of stomach mucosa.
- Associated with:
- Chronic gastritis
- H. pylori infection
- Smoking
- Diet factors
- Common symptoms:
- Weight loss
- Loss of appetite
- Lump in abdomen
🔬 CONCEPT EXPLAINED
Long-term inflammation damages mucosal DNA, causing uncontrolled cell growth. Tumors invade surrounding tissues and spread to lymph nodes.
⚠️ IF DAMAGED
- Tumor growth → Gastric obstruction
- Metastasis → Systemic disease
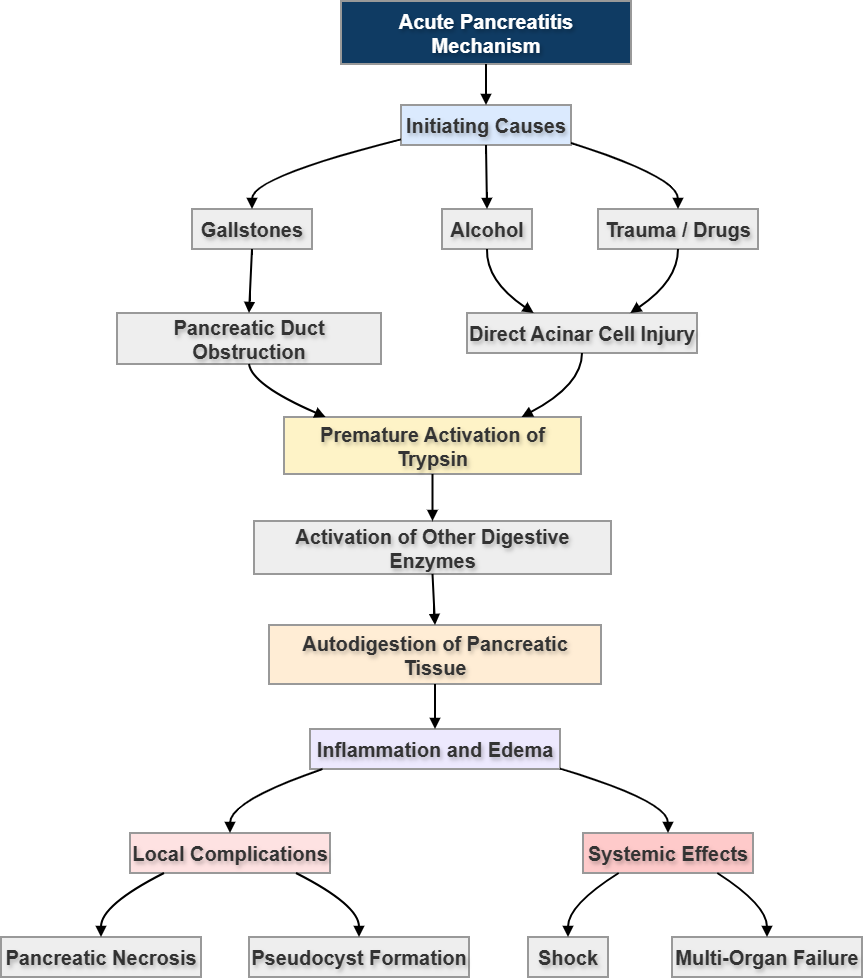
Acute Pancreatitis
🧠 CORE
- Acute inflammation of pancreas.
- Caused by:
- Gallstones
- Alcohol
- Trauma
- Hyperlipidemia
- Characterized by:
- Severe abdominal pain
- Enzyme activation
- Trypsin activation causes tissue destruction.
🔬 CONCEPT EXPLAINED
Normally pancreatic enzymes are inactive until reaching intestine. In pancreatitis, premature activation of trypsin occurs inside pancreas. Activated enzymes digest pancreatic tissue causing inflammation and edema.
⚠️ IF DAMAGED
- Enzyme leakage → Tissue destruction
- Severe inflammation → Shock
- Necrosis → Organ failure
Classification of Anti-Ulcer Drugs
🧠 CORE
Major classes:
- Proton pump inhibitors (PPIs)
- H2 receptor blockers
- Antacids
- Mucosal protectants
- Prostaglandin analogues
- Antibiotics (H. pylori treatment)
🔬 CONCEPT EXPLAINED
Each drug class targets acid secretion or mucosal protection. PPIs block H+/K+ ATPase pump reducing acid production. H2 blockers reduce histamine-induced acid release. Antacids neutralize existing acid.
⚠️ IF DAMAGED
- Excess acid → Ulcer persistence
- Drug failure → Complications
Mechanism of Anti-Ulcer Drugs
🧠 CORE
- PPIs block final acid secretion step.
- H2 blockers reduce histamine stimulation.
- Antacids neutralize acid.
- Prostaglandins increase mucus secretion.
- Antibiotics eliminate H. pylori.
🔬 CONCEPT EXPLAINED
Drugs work at different stages of acid production. PPIs act directly on proton pumps. H2 blockers act on histamine receptors. Protective agents strengthen mucosal barrier.
⚠️ IF DAMAGED
- Inadequate therapy → Chronic ulcer
- Improper drug use → Recurrence
Gastric Lavage
🧠 CORE
- Procedure used to wash stomach contents.
- Indications:
- Poison ingestion
- Drug overdose
- Contraindications:
- Corrosive poisoning
- Esophageal injury
- Sampling used for laboratory analysis.
🔬 CONCEPT EXPLAINED
A tube is inserted into stomach to remove contents. This reduces toxin absorption and allows sample collection for diagnosis.
⚠️ IF DAMAGED
- Improper technique → Aspiration
- Contraindicated use → Tissue injury
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
- Gastric mucosa → Protection from acid → Ulcer prevention
- LES → Prevent reflux → Protect esophagus
- Pancreas → Enzyme secretion → Digestion
- Failure of protection → Disease formation
🩺 5️⃣ Clinical Correlation
Common exam-relevant conditions:
- Peptic ulcer disease
- GERD
- Acute pancreatitis
- Gastric carcinoma
- Gastric outlet obstruction
- Bleeding ulcer
Clinical signs:
- Hematemesis
- Melena
- Epigastric pain
- Vomiting
- Weight loss
📌 6️⃣ Summary Points
- H. pylori and NSAIDs are major causes of peptic ulcers.
- PPIs are most effective anti-ulcer drugs.
- Bleeding is the most common complication of ulcers.
- Perforation causes sudden severe abdominal pain.
- GERD occurs due to weak LES.
- Acute pancreatitis results from enzyme activation inside pancreas.
- Gallstones and alcohol are major pancreatitis causes.
- Gastric lavage is contraindicated in corrosive poisoning.
- Chronic ulcers may cause gastric outlet obstruction.
- Early diagnosis prevents severe complications.