
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The appendix and abdominal vessels are important structures involved in gastrointestinal function, blood supply, venous drainage, and immune defense. The appendix is a narrow diverticulum attached to the cecum and is clinically important because appendicitis is one of the most common surgical emergencies. The abdominal aorta and its branches supply oxygenated blood to abdominal organs, while the inferior vena cava returns venous blood to the heart. Lymphatic drainage of abdominal organs plays a major role in immunity, absorption of fats, and spread of infections or malignancies. Understanding the arrangement of abdominal vessels helps students explain ischemia, portal circulation, surgical anatomy, and radiological findings. These structures are located mainly in the posterior abdominal wall and mesenteries. Their design demonstrates strong structure–function relationships essential for maintaining abdominal organ viability.
🔹 2️⃣ Foundation Concepts
Key Definitions
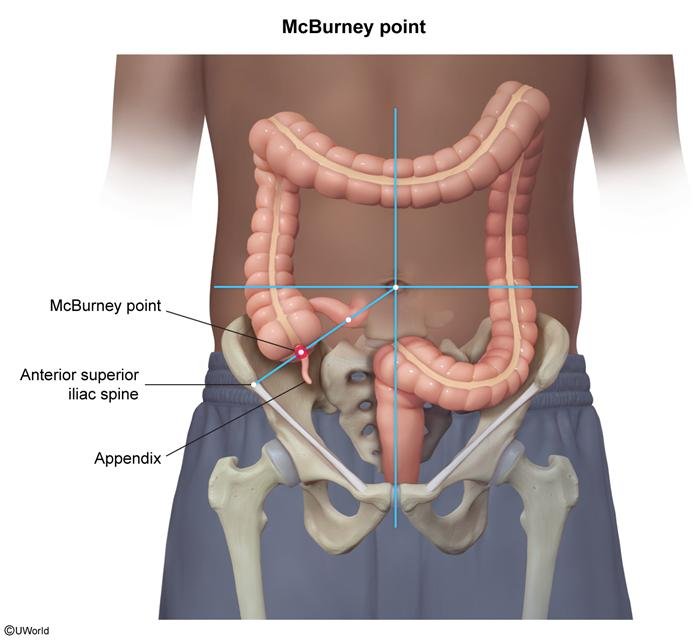
- Appendix: Narrow worm-like tubular diverticulum attached to cecum.
- Mesoappendix: Peritoneal fold connecting appendix to ileum and cecum.
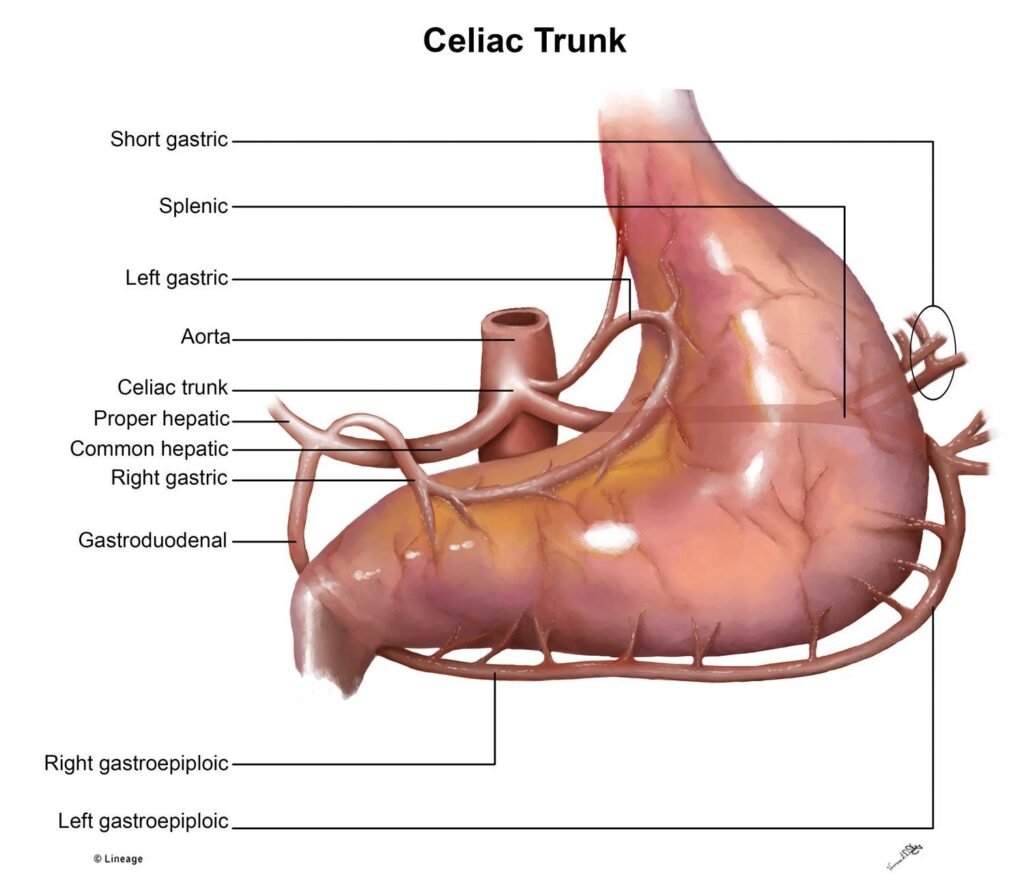
- Celiac trunk: First major unpaired branch of abdominal aorta supplying foregut.
- Superior mesenteric artery (SMA): Supplies midgut structures.
- Inferior mesenteric artery (IMA): Supplies hindgut structures.
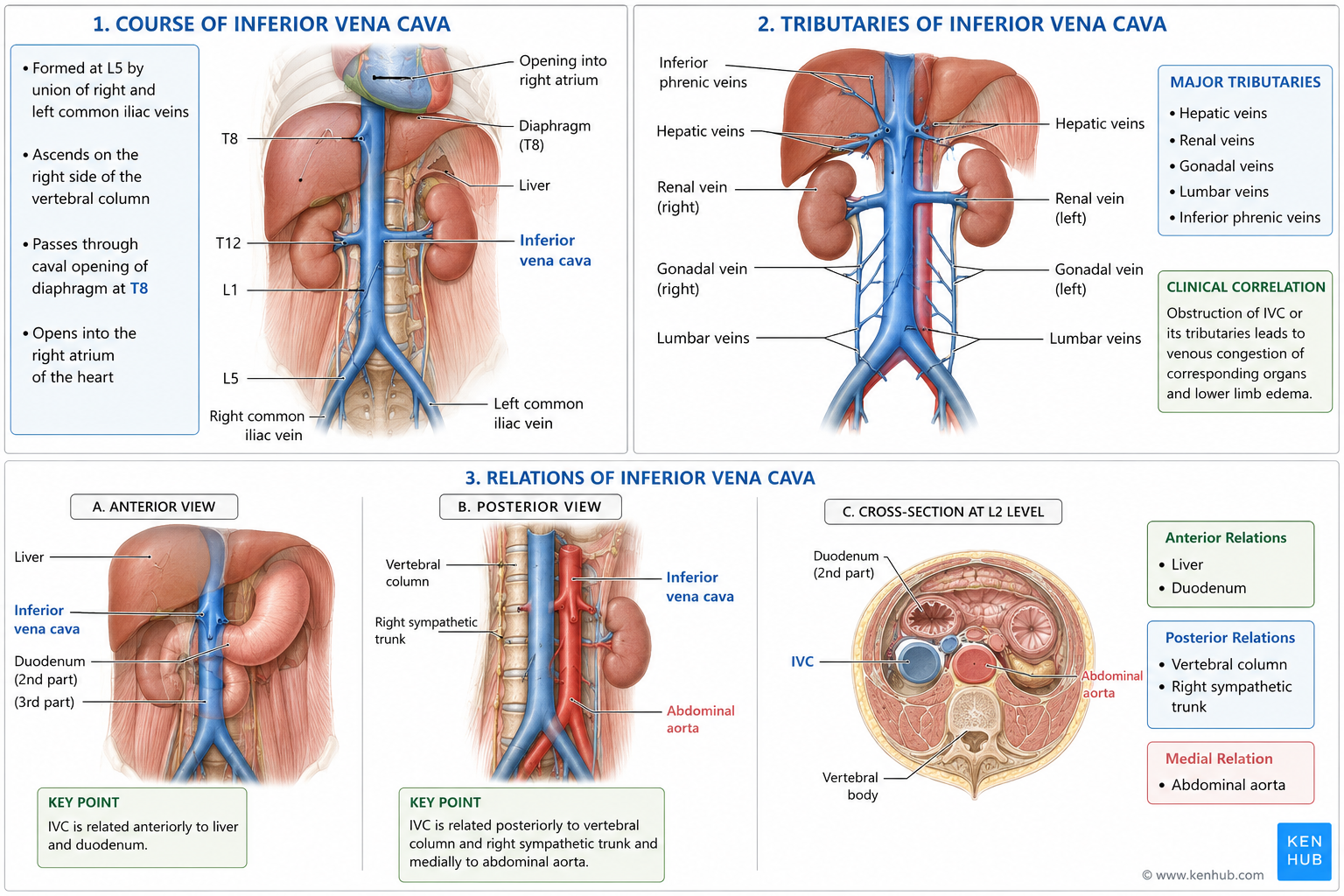
- Inferior vena cava (IVC): Largest abdominal vein returning blood to right atrium.
- Cisterna chyli: Dilated lymphatic sac receiving intestinal and lumbar lymph.
- Lymphatic drainage: Movement of tissue fluid through lymphatic vessels into venous circulation.
Essential Terminology
- Foregut: Esophagus to proximal duodenum.
- Midgut: Distal duodenum to proximal 2/3 transverse colon.
- Hindgut: Distal 1/3 transverse colon to upper anal canal.
- Tributary: Smaller vessel draining into larger vessel.
- Anastomosis: Communication between blood vessels.
- Retroperitoneal: Located posterior to peritoneum.
Basic Overview
- Appendix arises from posteromedial wall of cecum.
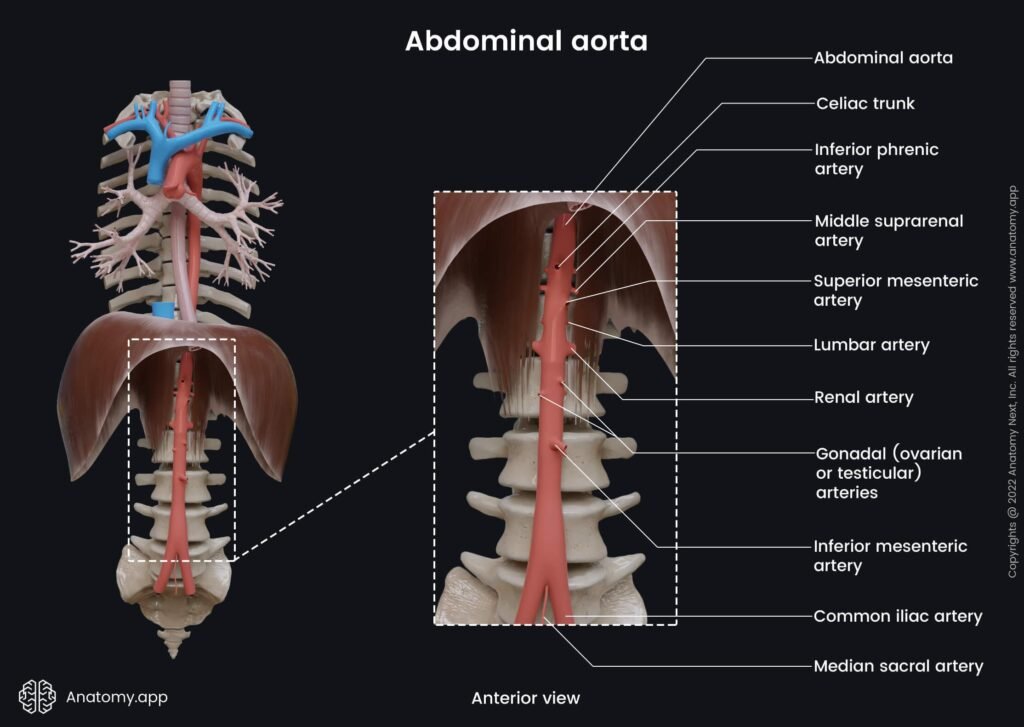
- Abdominal aorta begins at T12 and ends at L4.
- Major unpaired branches:
- Celiac trunk
- SMA
- IMA
- IVC forms at L5.
- Cisterna chyli is part of lymphatic drainage pathway.
- Abdominal lymphatics accompany arteries.
🔹 3️⃣ Core Learning — Curriculum Coverage
Branches of Abdominal Aorta
🧠 CORE
- Begins at T12.
- Ends at L4.
- Divides into common iliac arteries.
- Major unpaired branches:
- Celiac trunk
- SMA
- IMA.
- Paired branches:
- Renal arteries
- Gonadal arteries
- Inferior phrenic arteries.
🔬 CONCEPT EXPLAINED
The abdominal aorta supplies oxygenated blood to abdominal organs and posterior abdominal wall.
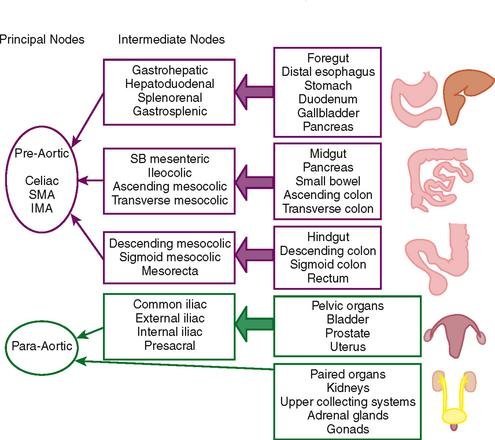
Unpaired branches supply gastrointestinal tract according to embryological divisions:
- Foregut
- Midgut
- Hindgut.
Structure → Function
- Central large artery → High-volume blood flow.
- Multiple branches → Organ-specific supply.
⚠️ IF DAMAGED
- Aortic aneurysm → Risk of rupture.
- Arterial blockage → Intestinal ischemia.
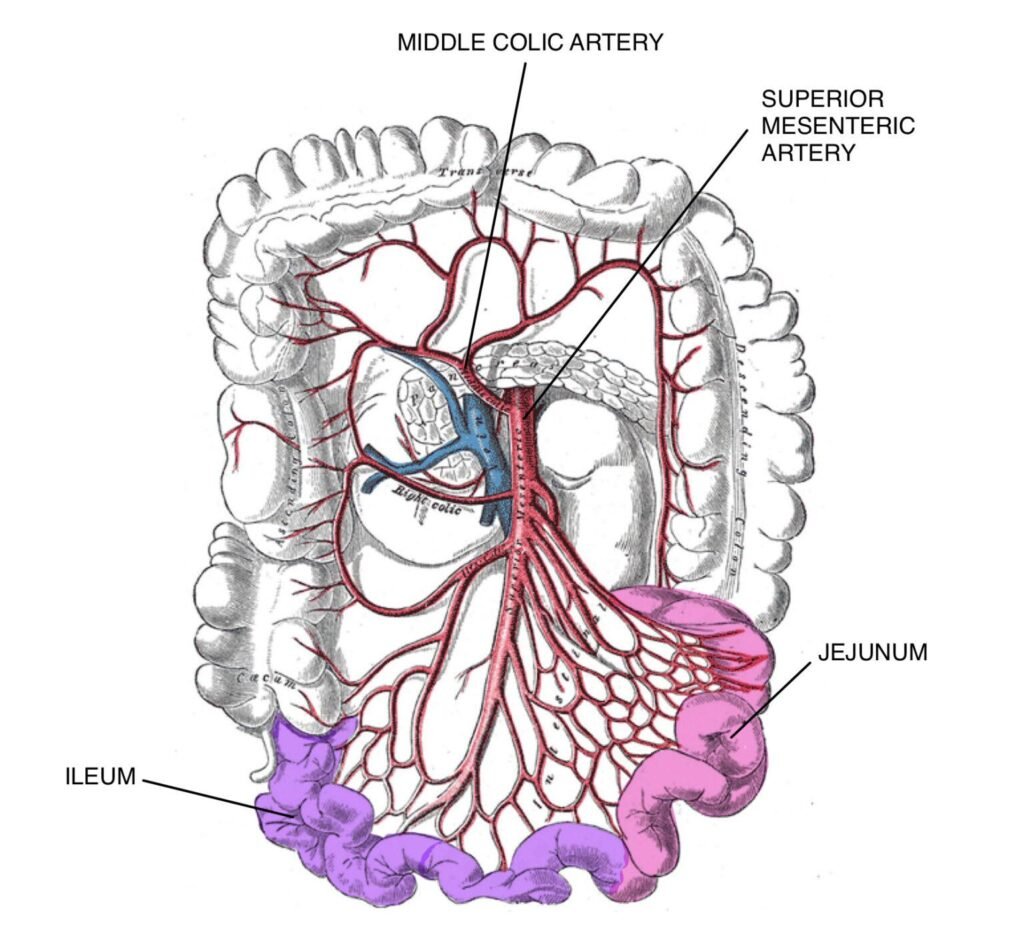
Superior Mesenteric Artery (SMA) — Course and Distribution
🧠 CORE
- Second unpaired branch of abdominal aorta.
- Arises at L1 vertebral level.
- Origin lies inferior to celiac trunk.
- Passes anterior to:
- Left renal vein
- Third part of duodenum.
- Enters root of mesentery.
- Descends downward and to the right.
- Main artery of midgut.
- Gives intestinal and colic branches.
Major Structures Supplied
- Distal duodenum
- Jejunum
- Ileum
- Cecum
- Appendix
- Ascending colon
- Proximal 2/3 transverse colon.
🔬 CONCEPT EXPLAINED
The superior mesenteric artery arises from the anterior surface of the abdominal aorta at the L1 level. After originating below the celiac trunk, it descends anterior to the left renal vein and third part of the duodenum before entering the mesentery.
Inside the mesentery, the SMA gives numerous branches to the small intestine and proximal large intestine. These branches form arterial arcades and vasa recta that maintain continuous blood supply during intestinal movement.
The SMA supplies midgut-derived organs which are highly active in digestion and nutrient absorption. Therefore, these organs require rich and continuous arterial supply.
Structure → Function
- Long mobile course → Reaches extensive midgut structures.
- Mesenteric position → Allows branches to move with intestines.
- Multiple arterial branches → Maintains continuous intestinal perfusion.
- Rich blood supply → Supports digestion and nutrient absorption.
⚠️ IF DAMAGED
Cause → Effect
- SMA obstruction → Reduced intestinal blood supply.
- Mesenteric ischemia → Severe abdominal pain.
- Prolonged ischemia → Bowel necrosis.
- Reduced intestinal perfusion → Malabsorption.
- Complete arterial occlusion → Intestinal infarction and gangrene.
Cisterna Chyli
🧠 CORE
- Dilated lymphatic sac.
- Located at L1–L2.
- Posterior to right crus of diaphragm.
- Receives:
- Intestinal trunk
- Lumbar trunks.
- Continues as thoracic duct.
🔬 CONCEPT EXPLAINED
The cisterna chyli collects lipid-rich lymph (chyle) from intestines and lower body.
Structure → Function
- Dilated sac → Temporary lymph reservoir.
- Continuation into thoracic duct → Returns lymph to venous circulation.
⚠️ IF DAMAGED
- Lymph leakage.
- Chylous ascites.
Lymphatic Drainage of Abdominal Organs
🧠 CORE
- Lymph follows arteries.
- Drains into pre-aortic lymph nodes.
- Major groups:
- Celiac nodes
- Superior mesenteric nodes
- Inferior mesenteric nodes.
- Ultimately drains into cisterna chyli.
🔬 CONCEPT EXPLAINED
Lymphatics remove excess tissue fluid, transport fats, and support immunity.
Organs drain according to arterial supply and embryological origin.
Structure → Function
- Lymph vessels near arteries → Efficient drainage.
- Nodes filter pathogens and malignant cells.
⚠️ IF DAMAGED
- Lymphedema.
- Spread of abdominal malignancy.
- Impaired fat absorption.
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| Appendix lymphoid tissue | Immune surveillance | Gut immune defense |
| SMA branches | Supply small intestine | Nutrient absorption |
| IMA branches | Supply distal colon | Water absorption |
| IVC | Venous return | Maintains circulation |
| Cisterna chyli | Collects lymph | Fat transport and immunity |
🩺 5️⃣ Clinical Correlation
Acute Appendicitis
- Most common surgical emergency.
- Pain shifts from umbilical region to right iliac fossa.
- May cause perforation.
Mesenteric Ischemia
- Reduced SMA blood flow.
- Severe abdominal pain.
- Bowel necrosis may occur.
Abdominal Aortic Aneurysm
- Dilatation of abdominal aorta.
- Risk of fatal rupture.
IVC Obstruction
- Causes lower limb edema.
- Venous congestion develops.
Chylous Ascites
- Leakage of lymph into peritoneal cavity.
- Occurs after lymphatic injury.
📌 6️⃣ Summary Points
- Appendix arises from posteromedial wall of cecum.
- Appendicular artery is an end artery.
- McBurney’s point is important in appendicitis.
- Celiac trunk supplies foregut.
- SMA supplies midgut.
- IMA supplies hindgut.
- IVC forms at L5.
- Cisterna chyli is origin of thoracic duct.
- Lymphatics generally follow arteries.
- Mesenteric ischemia is a surgical emergency.
- Retrocecal appendix may produce atypical symptoms.
- Lymph nodes filter pathogens and malignant cells.