
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The liver and pancreas are essential digestive organs that work together to process food, absorb nutrients, and maintain metabolic balance.
The pancreas lies retroperitoneally behind the stomach and secretes enzymes and bicarbonate into the duodenum.
The liver lies in the right upper abdomen beneath the diaphragm and receives blood from both the portal vein and hepatic artery.
Bile produced by the liver helps in fat digestion and excretion of bilirubin.
This topic is clinically important because disorders such as jaundice, pancreatitis, hepatitis, cirrhosis, and gallstones are common in medical practice.
Understanding liver blood flow, bile secretion, pancreatic secretion, and bilirubin metabolism helps students connect physiology with clinical disease.
🔹 2️⃣ Foundation Concepts
Key Definitions
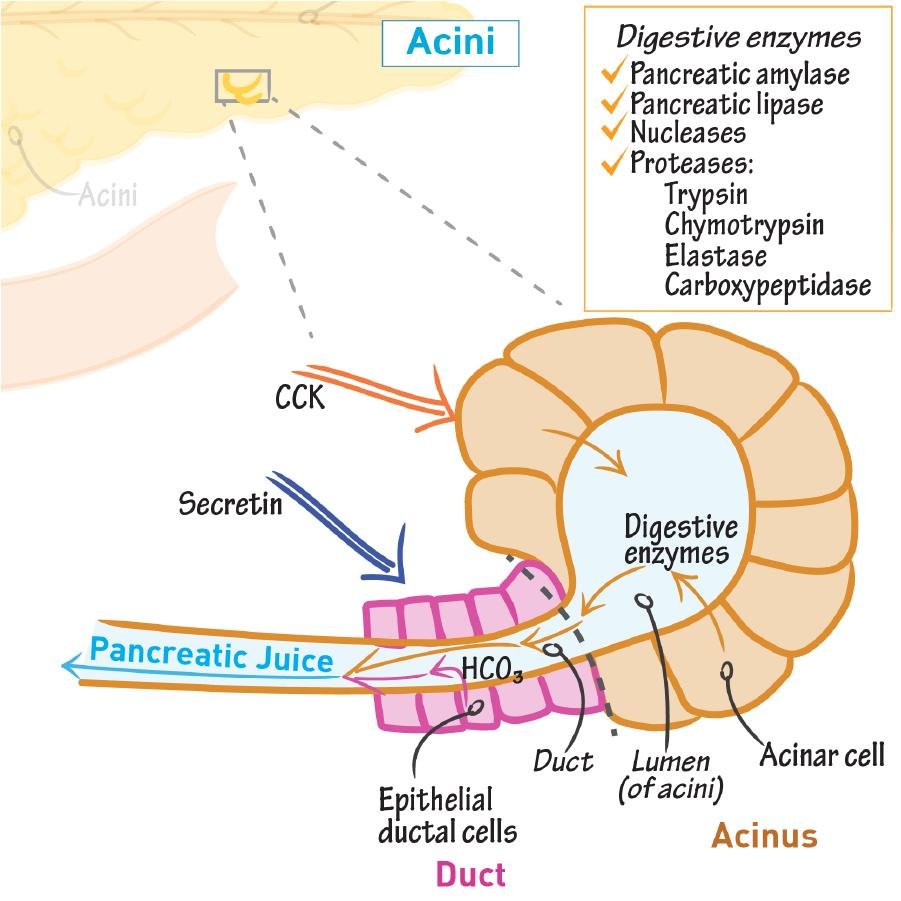
• Pancreatic secretion: Digestive fluid produced by the pancreas containing enzymes and bicarbonate.
• Acini: Exocrine pancreatic cells that secrete digestive enzymes.
• Duct cells: Pancreatic cells that secrete bicarbonate-rich fluid.
• Bile: Green-yellow fluid produced by hepatocytes that helps in fat digestion and waste excretion.
• Bile salts: Components of bile that emulsify fats and help fat absorption.
• Hepatocyte: Main functional cell of the liver.
• Portal vein: Vessel carrying nutrient-rich blood from the gut to the liver.
• Bilirubin: Yellow pigment formed from hemoglobin breakdown.
• Conjugation: Process in the liver that makes bilirubin water-soluble.
• Jaundice: Yellow discoloration due to increased bilirubin in blood.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. Role of Pancreatic Secretions in Digestion
🧠 CORE
• Pancreatic secretion is essential for digestion of carbohydrates, proteins, and fats.
• It contains digestive enzymes and bicarbonate-rich fluid.
• Acinar cells secrete enzymes.
• Duct cells secrete bicarbonate and water.
• Pancreatic amylase digests carbohydrates.
• Trypsin, chymotrypsin, and carboxypeptidase digest proteins.
• Pancreatic lipase digests fats.
• Bicarbonate neutralizes acidic chyme entering the duodenum.
• Enzymes work best in alkaline pH.
• Pancreatic secretion protects duodenal mucosa from acid damage.
🔬 CONCEPT EXPLAINED
The pancreas has an exocrine part that releases digestive juice into the duodenum. This juice contains enzymes for food breakdown and bicarbonate for neutralizing gastric acid.
When acidic chyme enters the duodenum from the stomach, pancreatic bicarbonate raises the pH. This creates a suitable alkaline environment for pancreatic enzymes.
Structure → Function:
Acini are enzyme-secreting units, while ducts add bicarbonate-rich fluid. Together, they produce a complete digestive secretion.
⚠️ IF DAMAGED
Cause → Effect:
• Pancreatic damage → reduced enzyme secretion → maldigestion
• Reduced lipase → fat malabsorption → steatorrhea
• Reduced bicarbonate → acidic duodenal contents → poor enzyme activity
• Severe pancreatic dysfunction → weight loss and nutritional deficiency
2. Phases of Pancreatic Secretion
🧠 CORE
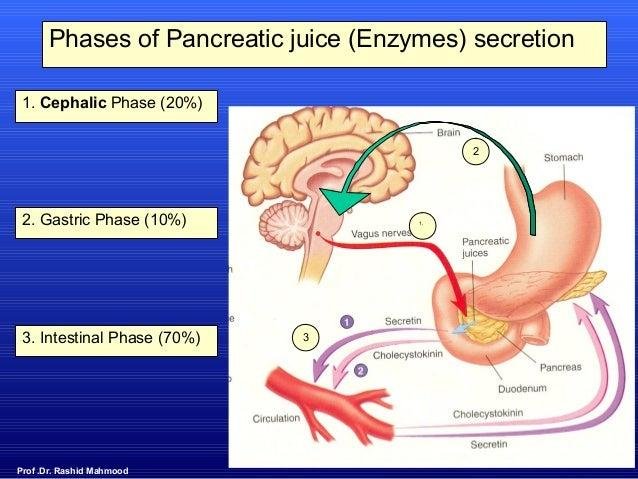
• Pancreatic secretion occurs in three phases.
• These are cephalic, gastric, and intestinal phases.
• Cephalic phase begins before food reaches the stomach.
• Gastric phase begins when food enters the stomach.
• Intestinal phase is the most important phase.
• Intestinal phase occurs when chyme enters the duodenum.
• Vagus nerve stimulates early pancreatic secretion.
• Secretin stimulates bicarbonate secretion.
• Cholecystokinin stimulates enzyme secretion.
• Acid and fat in duodenum are major stimulants.
🔬 CONCEPT EXPLAINED
In the cephalic phase, sight, smell, taste, and chewing of food activate the vagus nerve. This causes mild pancreatic enzyme secretion.
In the gastric phase, stomach distension continues vagal stimulation and produces further pancreatic secretion.
In the intestinal phase, acidic and fatty chyme enters the duodenum. This strongly stimulates secretin and CCK release, producing the major pancreatic response.
⚠️ IF DAMAGED
Cause → Effect:
• Vagal dysfunction → weak early pancreatic response
• Impaired secretin release → poor bicarbonate secretion
• Impaired CCK release → poor enzyme secretion
• Poor intestinal phase → incomplete digestion in duodenum
3. Regulation of Pancreatic Secretion
🧠 CORE
• Pancreatic secretion is regulated by nerves and hormones.
• Parasympathetic vagus nerve increases secretion.
• Sympathetic activity reduces pancreatic secretion indirectly by reducing blood flow.
• Secretin is released from duodenal S cells.
• Secretin mainly stimulates bicarbonate secretion.
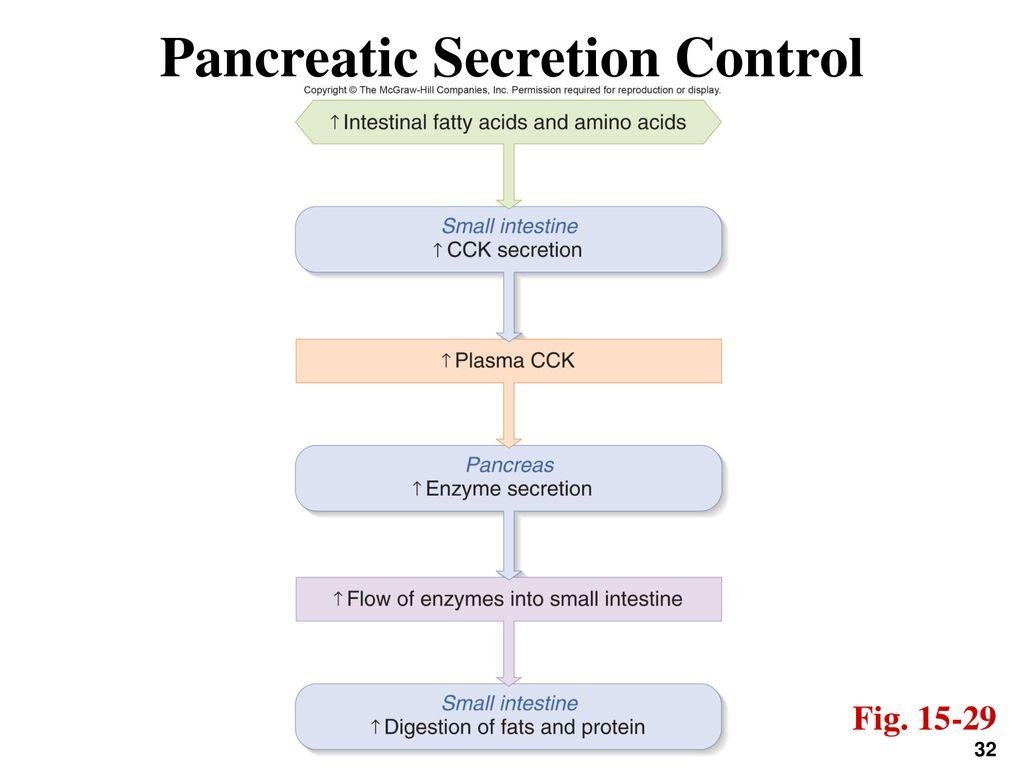
• CCK is released from duodenal I cells.
• CCK mainly stimulates enzyme secretion from acinar cells.
• Acid in duodenum stimulates secretin.
• Fat and amino acids stimulate CCK.
• Enterokinase activates trypsinogen into trypsin in the intestine.
🔬 CONCEPT EXPLAINED
Pancreatic secretion must match the type of food entering the duodenum. If acidic chyme enters, secretin stimulates duct cells to release bicarbonate. If fatty or protein-rich food enters, CCK stimulates acinar cells to release enzymes.
Trypsinogen is secreted in inactive form to protect the pancreas from self-digestion. It becomes active trypsin only in the intestinal lumen.
⚠️ IF DAMAGED
Cause → Effect:
• Premature activation of enzymes inside pancreas → autodigestion → acute pancreatitis
• Low bicarbonate secretion → duodenal acidity → enzyme inactivation
• Low enzyme secretion → malabsorption
• Poor regulation → ineffective digestion
4. Physiological Anatomy of Liver
🧠 CORE
• The liver is the largest gland in the body.
• It lies mainly in the right hypochondrium and epigastrium.
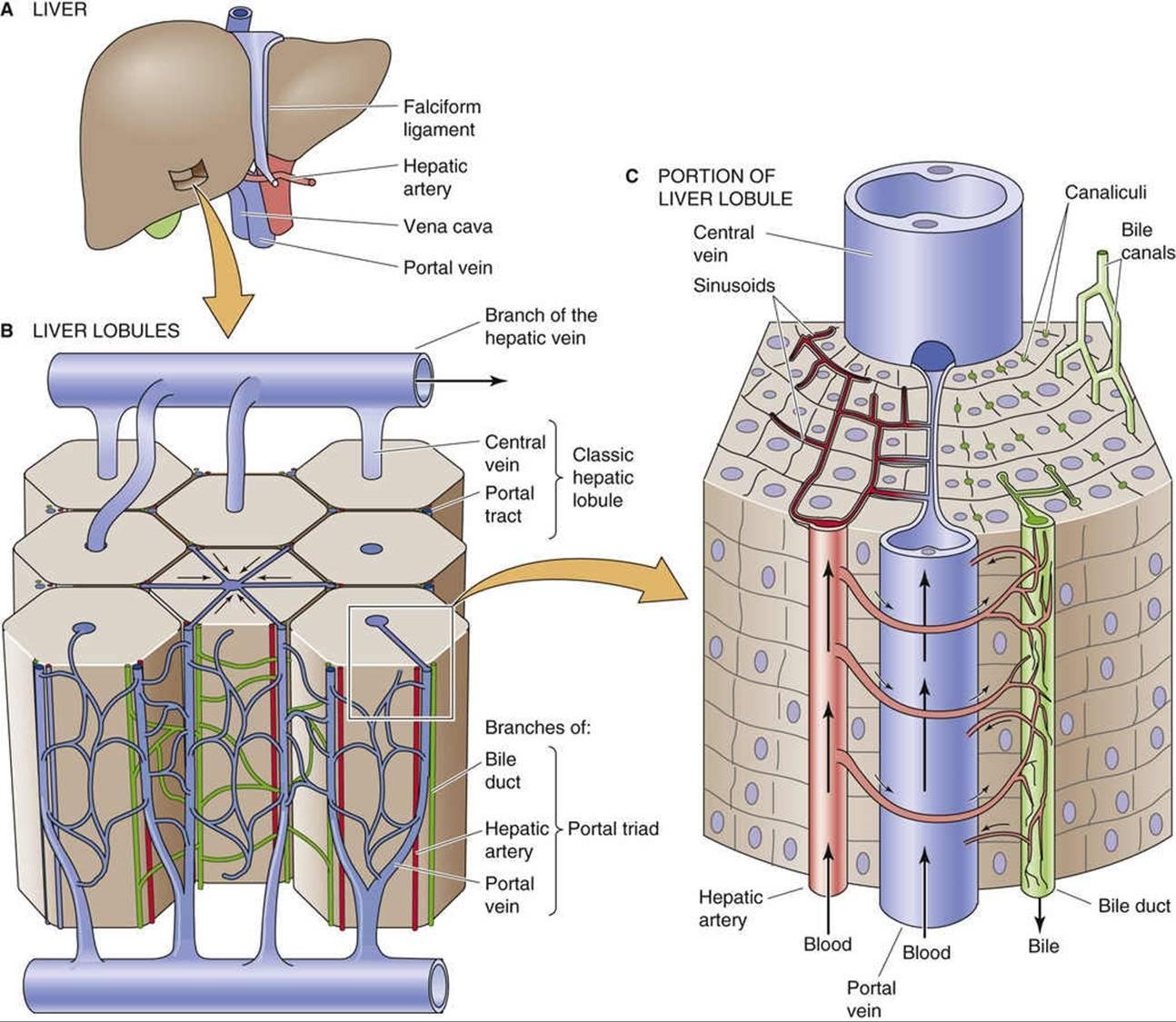
• Hepatocytes are the main functional cells.
• Liver lobules are functional microscopic units.
• Blood flows from portal areas toward the central vein.
• Bile flows in the opposite direction, from hepatocytes toward bile ducts.
• Portal triad contains portal vein branch, hepatic artery branch, and bile ductule.
• Sinusoids allow exchange between blood and hepatocytes.
• Kupffer cells are macrophages in liver sinusoids.
• The liver performs digestive, metabolic, storage, detoxification, and excretory functions.
🔬 CONCEPT EXPLAINED
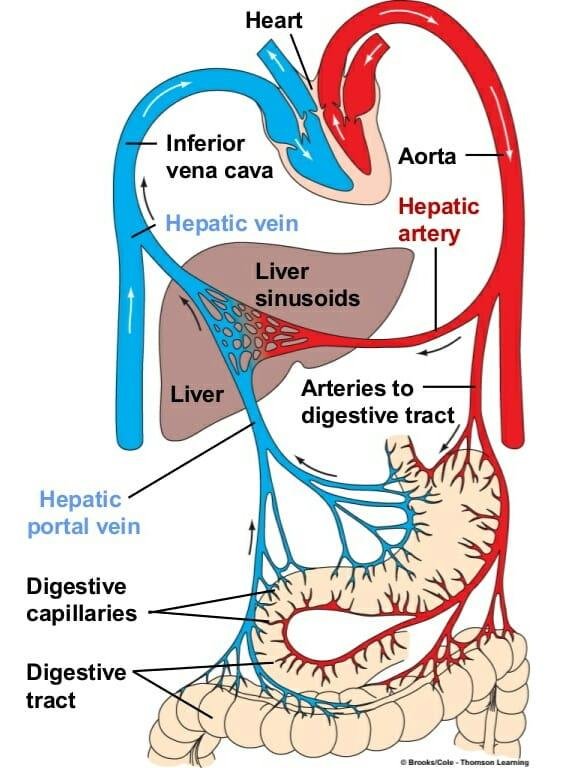
The liver is designed as a blood-processing organ. Blood from the intestine enters through the portal vein and mixes with oxygenated blood from the hepatic artery. This mixed blood passes through sinusoids where hepatocytes remove nutrients, toxins, and waste products.
Bile flows in the opposite direction to blood. This arrangement allows hepatocytes to secrete bile into canaliculi while processing incoming portal blood.
Structure → Function:
Sinusoids are wide vascular channels that allow close contact between blood and hepatocytes, making metabolism and detoxification efficient.
⚠️ IF DAMAGED
Cause → Effect:
• Hepatocyte injury → reduced metabolism and detoxification
• Sinusoidal fibrosis → impaired blood flow → portal hypertension
• Bile canaliculi obstruction → bile retention → jaundice
• Kupffer cell dysfunction → reduced clearance of bacteria and debris
5. Blood Flow Through Liver
🧠 CORE
• Liver has dual blood supply.
• Portal vein supplies about 75% of liver blood flow.
• Hepatic artery supplies about 25% of liver blood flow.
• Portal vein carries nutrient-rich venous blood from gut.
• Hepatic artery carries oxygenated blood.
• Blood enters through portal triads.
• Blood flows through sinusoids.
• Blood drains into central veins.
• Central veins join hepatic veins.
• Hepatic veins drain into inferior vena cava.
🔬 CONCEPT EXPLAINED
The liver receives blood from two sources. Portal venous blood brings absorbed nutrients, drugs, and toxins from the gastrointestinal tract. Hepatic arterial blood supplies oxygen.
Inside the liver lobule, these blood sources mix in sinusoids. Hepatocytes extract nutrients, metabolize substances, and detoxify harmful compounds. Blood then exits through central veins and hepatic veins.
⚠️ IF DAMAGED
Cause → Effect:
• Portal vein obstruction → portal hypertension
• Cirrhosis → increased resistance to portal flow → ascites and varices
• Reduced hepatic arterial flow → ischemic liver injury
• Hepatic vein obstruction → liver congestion
6. Metabolic Functions of Liver
🧠 CORE
• Liver regulates carbohydrate metabolism.
• It stores glucose as glycogen.
• It performs glycogenolysis during fasting.
• It performs gluconeogenesis from non-carbohydrate sources.
• It metabolizes amino acids and forms urea.
• It synthesizes plasma proteins such as albumin.
• It metabolizes fats and cholesterol.
• It produces bile salts from cholesterol.
• It stores vitamins A, D, B12, and iron.
• It detoxifies drugs, toxins, and hormones.
🔬 CONCEPT EXPLAINED
The liver maintains blood glucose levels by storing glucose after meals and releasing glucose during fasting. It also converts excess amino acids and fats into usable metabolic forms.
Ammonia produced from amino acid breakdown is toxic. The liver converts ammonia into urea, which is excreted by kidneys.
The liver also synthesizes albumin, clotting factors, and transport proteins. This supports oncotic pressure, blood clotting, and systemic metabolism.
⚠️ IF DAMAGED
Cause → Effect:
• Reduced albumin synthesis → edema and ascites
• Reduced clotting factor production → bleeding tendency
• Failure of ammonia detoxification → hepatic encephalopathy
• Poor glucose regulation → hypoglycemia during fasting
• Reduced bile salt production → fat malabsorption
7. Liver Regeneration
🧠 CORE
• Liver has strong regenerative ability.
• Hepatocytes can divide after injury or partial removal.
• Regeneration restores liver mass, not always perfect original architecture.
• Growth factors stimulate hepatocyte proliferation.
• Regeneration depends on intact blood supply and extracellular framework.
• Mild injury may recover completely.
• Repeated chronic injury causes fibrosis.
• Fibrosis can progress to cirrhosis.
• Cirrhosis reduces functional regeneration.
• Regeneration is clinically important after partial hepatectomy.
🔬 CONCEPT EXPLAINED
Unlike many organs, the liver can replace lost tissue by hepatocyte proliferation. After injury, surviving hepatocytes enter the cell cycle and multiply.
However, regeneration works best when the supporting framework remains intact. In chronic liver disease, repeated inflammation and fibrosis distort liver architecture. This produces nodules and cirrhosis rather than normal regeneration.
⚠️ IF DAMAGED
Cause → Effect:
• Acute limited injury → regeneration → recovery
• Chronic repeated injury → fibrosis → cirrhosis
• Cirrhosis → poor blood flow and poor liver function
• Failed regeneration → liver failure
8. Bilirubin Formation
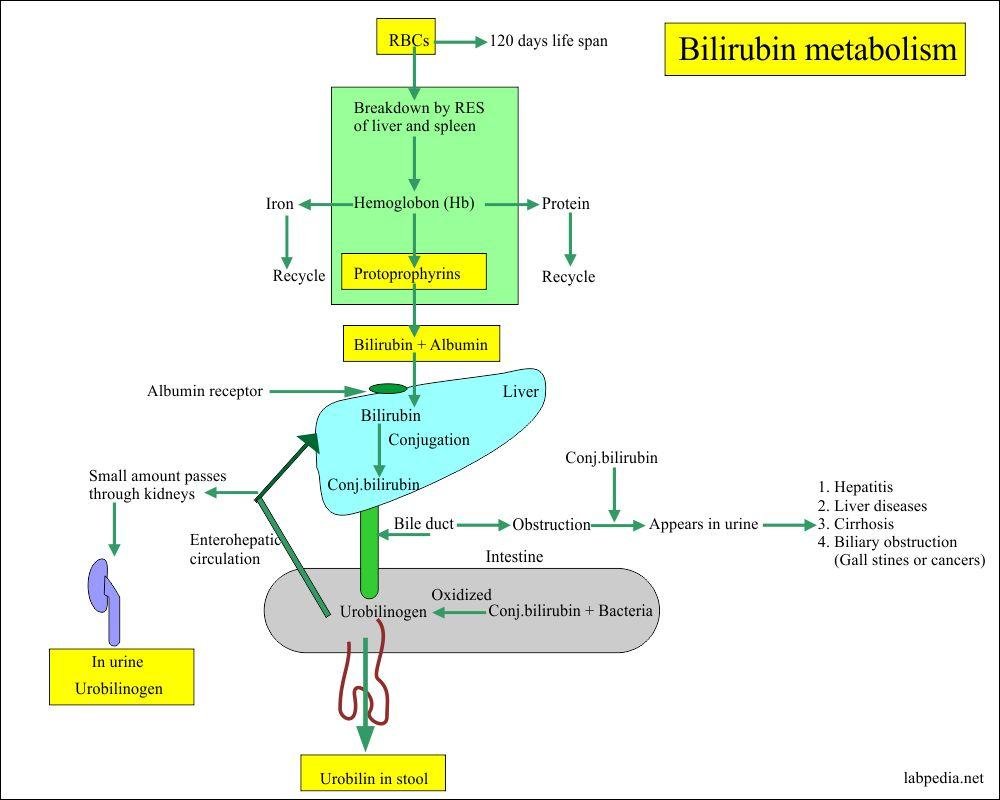
🧠 CORE
• Bilirubin is formed from breakdown of hemoglobin.
• Old red blood cells are destroyed mainly in spleen, liver, and bone marrow.
• Hemoglobin splits into globin and heme.
• Heme is converted into biliverdin.
• Biliverdin is converted into unconjugated bilirubin.
• Unconjugated bilirubin is lipid-soluble.
• It travels in blood bound to albumin.
• Liver takes up unconjugated bilirubin.
• Hepatocytes conjugate bilirubin with glucuronic acid.
• Conjugated bilirubin is water-soluble.
🔬 CONCEPT EXPLAINED
When red blood cells become old, macrophages break them down. The heme part of hemoglobin is converted into bilirubin. Initially, bilirubin is unconjugated and cannot dissolve in water, so it must bind to albumin for transport in blood.
The liver takes up unconjugated bilirubin and conjugates it. Conjugation makes bilirubin water-soluble, allowing it to be excreted in bile.
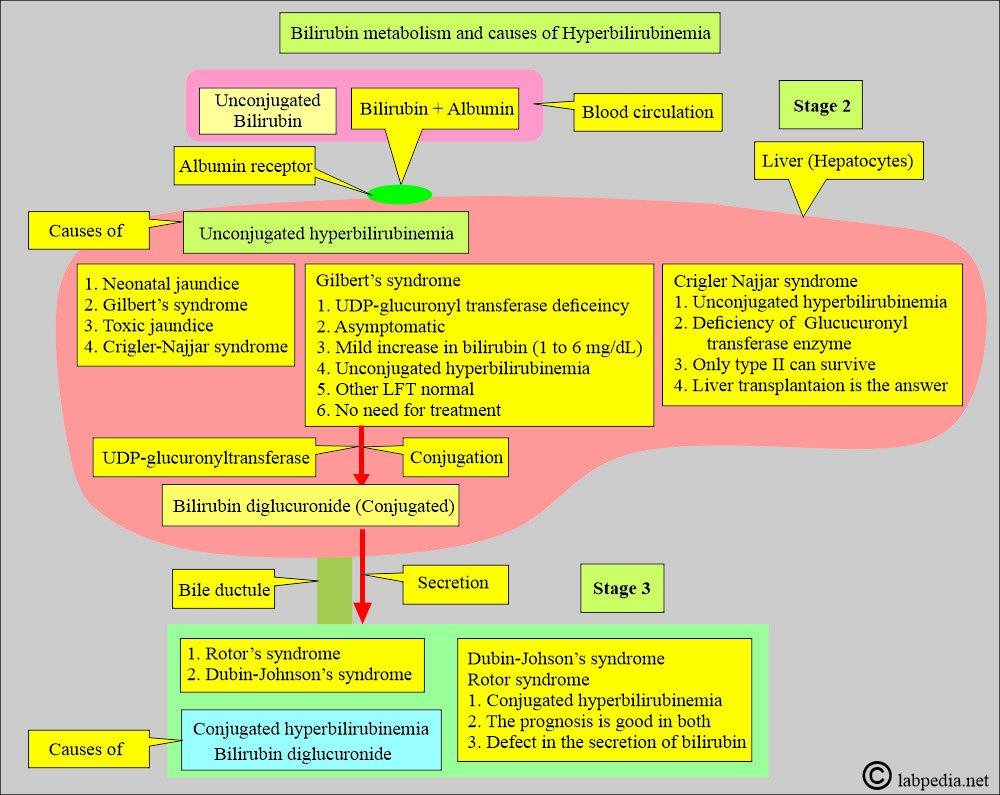
⚠️ IF DAMAGED
Cause → Effect:
• Excess RBC breakdown → increased unconjugated bilirubin → hemolytic jaundice
• Liver cell damage → impaired uptake/conjugation → hepatic jaundice
• Poor conjugation in newborns → neonatal jaundice
• Excess unconjugated bilirubin in newborns → risk of kernicterus
9. Bilirubin Excretion
🧠 CORE
• Conjugated bilirubin is secreted into bile canaliculi.
• It flows with bile into bile ducts.
• Bile reaches the duodenum.
• Intestinal bacteria convert bilirubin into urobilinogen.
• Some urobilinogen is reabsorbed into blood.
• Some is excreted in urine as urobilin.
• Most is converted into stercobilin.
• Stercobilin gives stool its brown color.
• Obstruction prevents bilirubin from reaching intestine.
• Obstructive jaundice causes pale stools and dark urine.
🔬 CONCEPT EXPLAINED
After conjugation, bilirubin is actively secreted into bile. Bile carries it through the biliary tract into the intestine. In the intestine, bacteria convert bilirubin into urobilinogen.
Some urobilinogen returns to the liver through enterohepatic circulation. Some is excreted in urine. The remaining pigment becomes stercobilin, which colors stool brown.
⚠️ IF DAMAGED
Cause → Effect:
• Bile duct obstruction → conjugated bilirubin backs up into blood
• No bilirubin reaches intestine → pale stools
• Conjugated bilirubin enters urine → dark urine
• Bile salt retention → itching
• Fat digestion decreases → steatorrhea
⚙️ 4️⃣ Functional Flow
A. Pancreatic Secretion Flow
- Food enters mouth.
- Vagus nerve is stimulated.
- Pancreatic acini begin enzyme secretion.
- Food enters stomach.
- Gastric distension continues vagal stimulation.
- Acidic chyme enters duodenum.
- Duodenal S cells release secretin.
- Secretin stimulates duct cells.
- Bicarbonate-rich fluid enters duodenum.
- Fat and amino acids stimulate CCK release.
- CCK stimulates acinar cells.
- Enzymes digest proteins, fats, and carbohydrates.
B. Liver Blood Flow
- Portal vein brings nutrient-rich blood from gut.
- Hepatic artery brings oxygenated blood.
- Both enter liver through portal triads.
- Blood flows into sinusoids.
- Hepatocytes process nutrients and toxins.
- Kupffer cells remove bacteria and debris.
- Blood drains into central veins.
- Central veins join hepatic veins.
- Hepatic veins drain into inferior vena cava.
C. Bilirubin Metabolism Flow
- Old RBCs are broken down by macrophages.
- Hemoglobin is split into heme and globin.
- Heme is converted into biliverdin.
- Biliverdin becomes unconjugated bilirubin.
- Unconjugated bilirubin binds albumin in blood.
- Liver takes up bilirubin.
- Hepatocytes conjugate bilirubin with glucuronic acid.
- Conjugated bilirubin enters bile.
- Bile carries bilirubin to intestine.
- Intestinal bacteria form urobilinogen.
- Stercobilin gives stool brown color.
- Urobilin gives urine yellow color.
🩺 5️⃣ Clinical Correlation
1. Acute Pancreatitis
Cause:
• Premature activation of pancreatic enzymes inside pancreas
Effect:
• Autodigestion of pancreatic tissue
• Severe epigastric pain
• Raised serum amylase and lipase
2. Exocrine Pancreatic Insufficiency
Cause:
• Reduced pancreatic enzyme secretion
Effect:
• Poor digestion
• Fat malabsorption
• Steatorrhea
• Weight loss
3. Obstructive Jaundice
Cause:
• Blockage of bile duct, commonly by gallstones
Effect:
• Conjugated bilirubin rises in blood
• Dark urine
• Pale stools
• Itching due to bile salt retention
4. Hemolytic Jaundice
Cause:
• Excessive breakdown of red blood cells
Effect:
• Increased unconjugated bilirubin
• Liver conjugation capacity may be exceeded
• Usually no pale stools
5. Hepatocellular Jaundice
Cause:
• Liver cell injury due to hepatitis, toxins, or cirrhosis
Effect:
• Impaired uptake, conjugation, and excretion of bilirubin
• Mixed increase of conjugated and unconjugated bilirubin
• Abnormal liver function tests
6. Cirrhosis
Cause:
• Chronic liver injury and fibrosis
Effect:
• Distorted liver architecture
• Portal hypertension
• Ascites
• Reduced albumin and clotting factors
• Risk of hepatic encephalopathy
7. Neonatal Jaundice
Cause:
• Immature bilirubin conjugating system in newborn
Effect:
• Increased unconjugated bilirubin
• Yellow discoloration
• Severe cases may affect brain tissue
📌 6️⃣ Summary Points
• Pancreatic acini secrete enzymes; duct cells secrete bicarbonate.
• Secretin mainly stimulates bicarbonate secretion.
• CCK mainly stimulates pancreatic enzyme secretion.
• Pancreatic enzymes work best in alkaline pH.
• Liver receives dual blood supply from portal vein and hepatic artery.
• Blood flows toward central vein; bile flows away from hepatocytes toward bile ducts.
• Hepatocytes perform metabolism, detoxification, storage, and bile formation.
• Liver converts ammonia into urea.
• Unconjugated bilirubin is lipid-soluble and albumin-bound.
• Conjugated bilirubin is water-soluble and excreted in bile.
• Obstructive jaundice causes dark urine and pale stools.
• Chronic liver injury may cause fibrosis and cirrhosis.