
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The midgut is the embryological part of the gut tube that gives rise to most of the small intestine and part of the large intestine.
It extends from the distal duodenum to the proximal two-thirds of the transverse colon.
Its development is important because the midgut undergoes rapid growth, physiological herniation, and rotation before returning to the abdominal cavity.
These events explain the adult arrangement of the intestines, mesentery, and blood supply.
Failure of normal midgut development can produce clinically important anomalies such as malrotation, volvulus, omphalocele, Meckel’s diverticulum, and persistent vitelline duct.
Understanding midgut development helps students connect embryology with adult abdominal anatomy.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Midgut: Embryonic gut region supplied by the superior mesenteric artery.
- Midgut loop: U-shaped intestinal loop formed due to rapid elongation of the midgut.
- Physiological herniation: Temporary herniation of midgut into the umbilical cord during development.
- Rotation of midgut: Counterclockwise movement of midgut around the superior mesenteric artery.
- Vitelline duct: Embryonic connection between midgut and yolk sac.
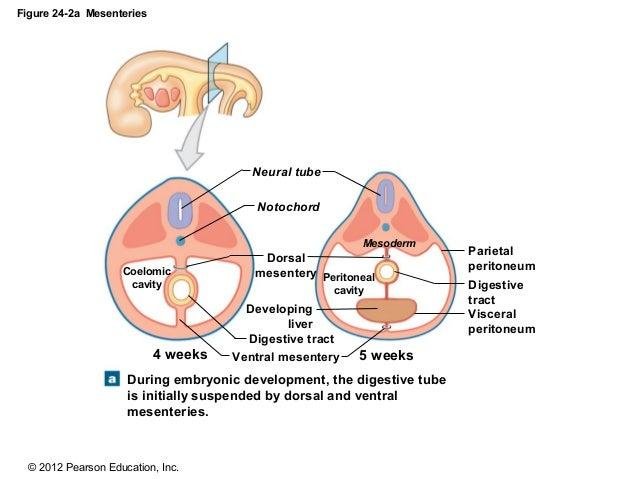
- Mesentery: Double layer of peritoneum that suspends gut and carries vessels, nerves, and lymphatics.
- Dorsal mesentery: Mesentery attached to the posterior abdominal wall.
- Ventral mesentery: Present only in foregut region, not midgut.
- Midgut derivatives: Structures developing from distal duodenum to proximal two-thirds of transverse colon.
🔹 3️⃣ Core Learning — Curriculum Coverage
1: Formation of Midgut Loop
🧠 CORE
- The midgut develops from the endoderm-lined embryonic gut tube.
- It remains temporarily connected to the yolk sac through the vitelline duct.
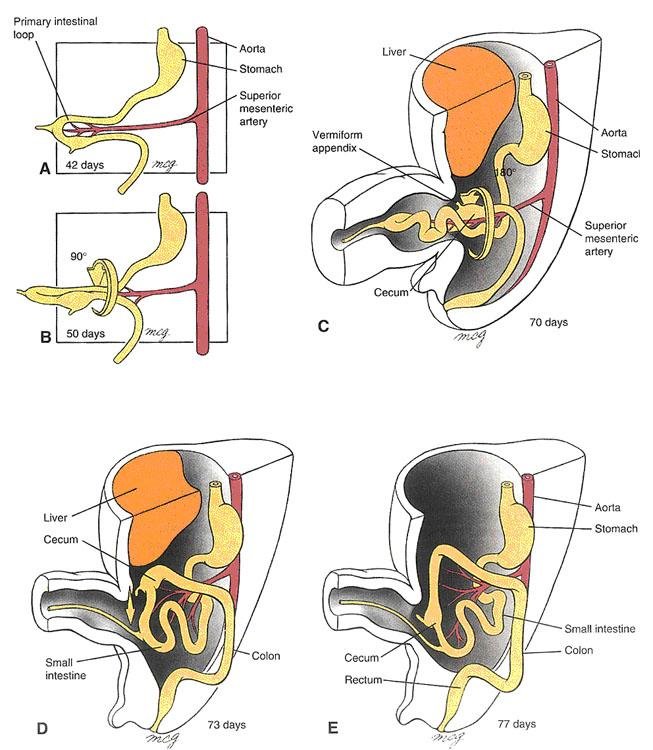
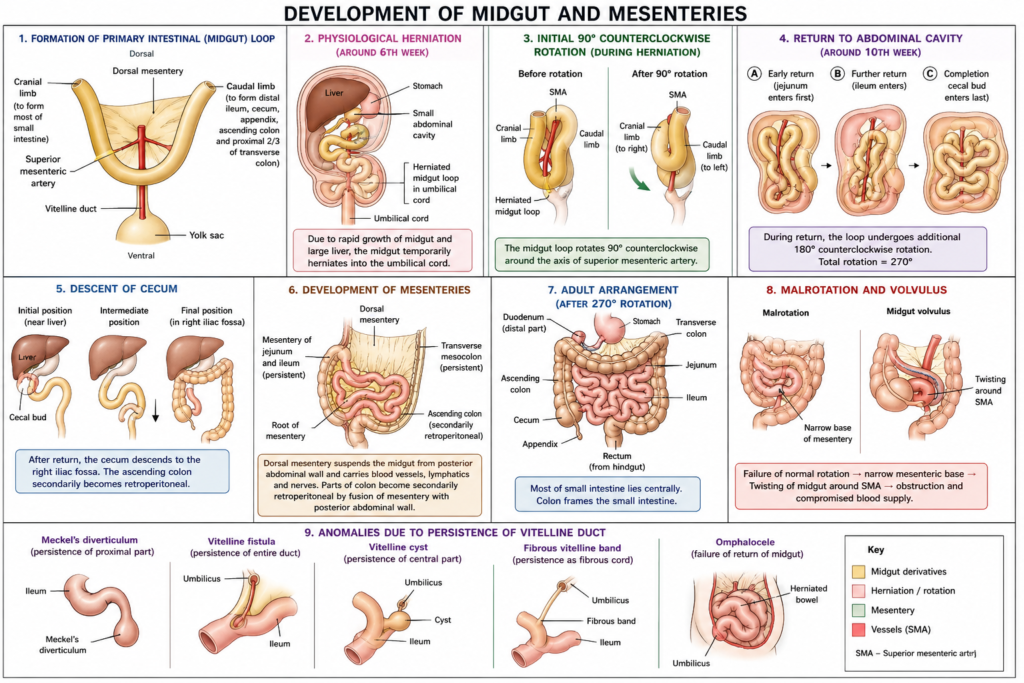
- Rapid growth of the midgut forms a U-shaped primary intestinal loop.
- The loop develops around the axis of the superior mesenteric artery.
- It has two limbs:
- Cranial limb
- Caudal limb
- The cranial limb mainly forms most of the small intestine.
- The caudal limb mainly forms distal ileum and part of large intestine.
- The midgut loop is essential for proper intestinal length and arrangement.
🔬 CONCEPT EXPLAINED
During early development, the midgut grows faster than the abdominal cavity.
Because the embryo is still small, the abdominal cavity cannot contain the rapidly elongating intestinal loop.
The midgut therefore forms a U-shaped loop around the superior mesenteric artery.
This artery acts as the central axis of development and later becomes the main arterial supply of adult midgut derivatives.
The loop is divided into:
- Cranial limb: Forms distal duodenum, jejunum, and most of ileum.
- Caudal limb: Forms distal ileum, cecum, appendix, ascending colon, and proximal two-thirds of transverse colon.
Structure → Function
- Rapid elongation → increases intestinal length.
- Loop formation → allows intestine to arrange properly.
- SMA axis → organizes blood supply and rotation.
⚠️ IF DAMAGED
- Abnormal loop formation can disturb intestinal positioning.
- Failure of normal development may contribute to malrotation.
- Abnormal relation with SMA can predispose to twisting of intestine.
Cause → Effect:
Abnormal midgut loop formation → abnormal intestinal rotation → abnormal adult gut position.
2: Rotation of Midgut Loop
🧠 CORE
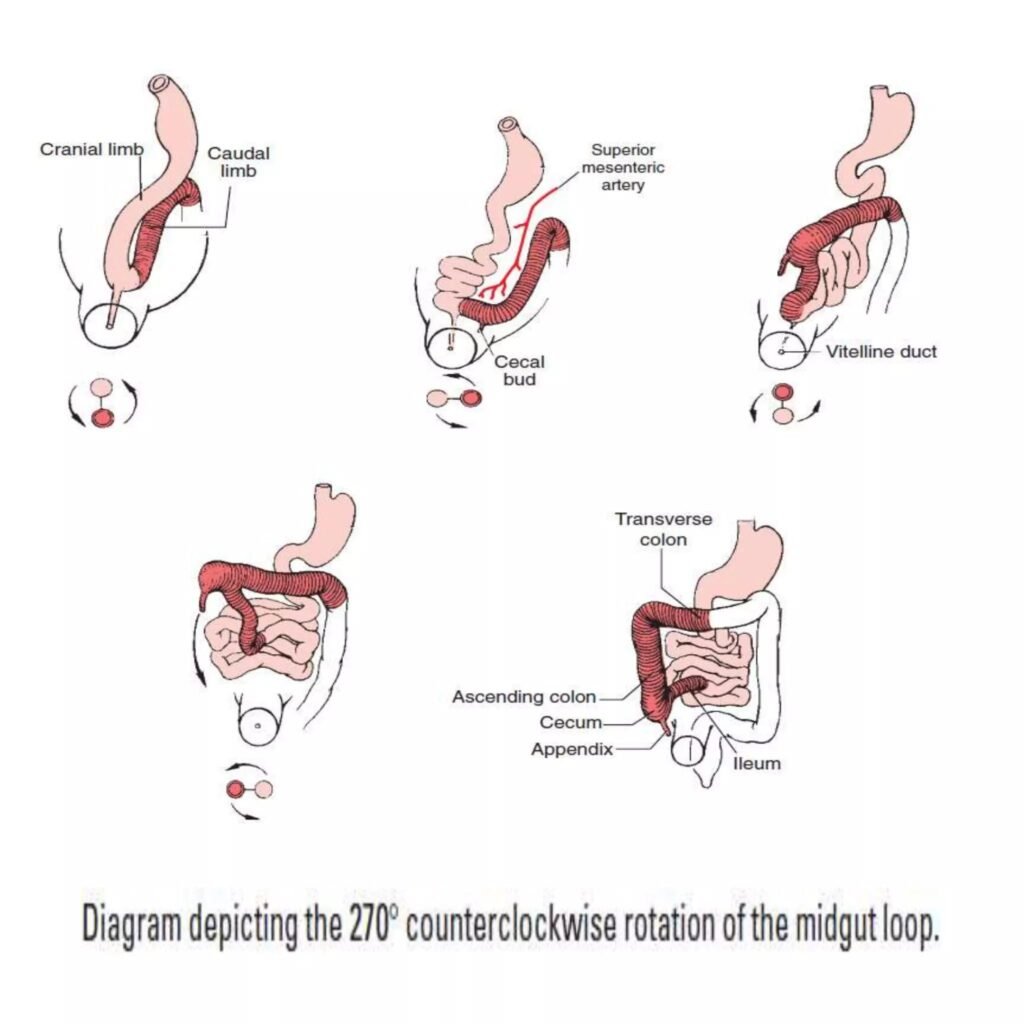
- The midgut rotates around the superior mesenteric artery.
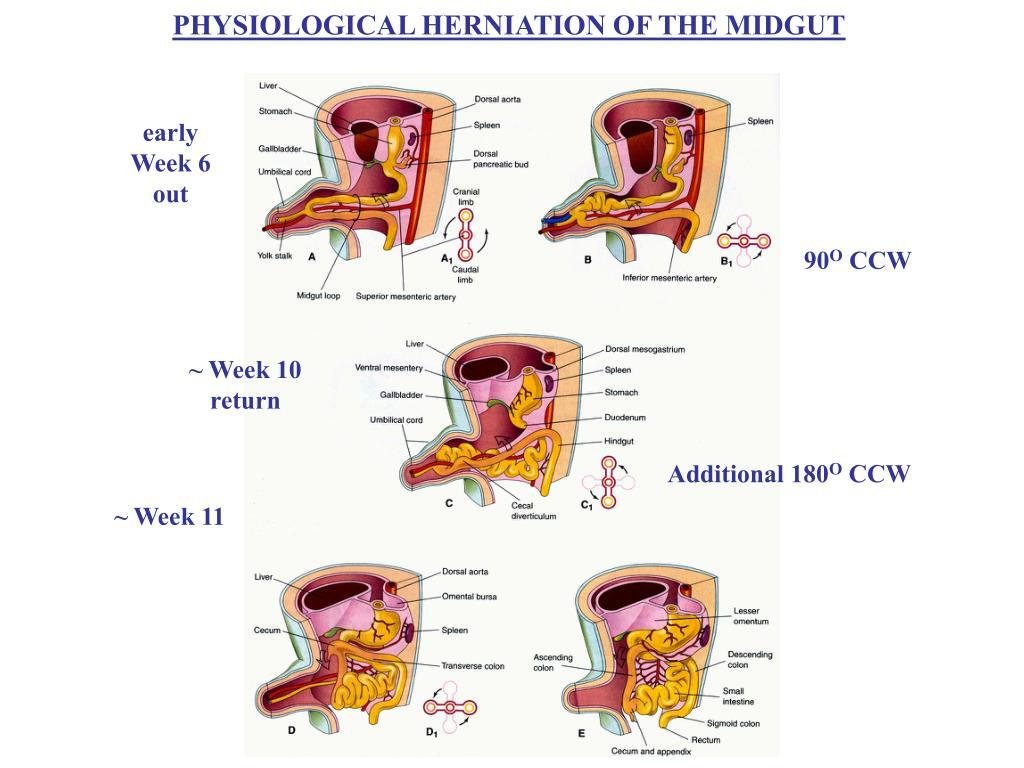
- Rotation occurs in a counterclockwise direction.
- Total rotation is approximately 270 degrees counterclockwise.
- The first 90 degrees occur during physiological herniation.
- The remaining 180 degrees occur during return to the abdomen.
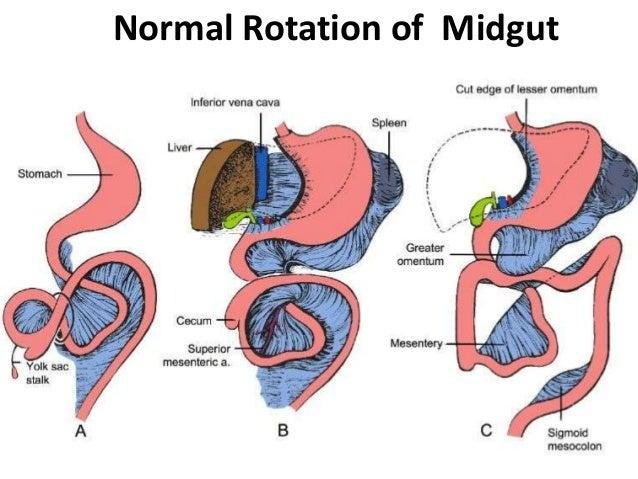
- Rotation places small intestine mainly centrally.
- Large intestine becomes arranged around the small intestine.
- Cecum initially lies near the liver, then descends to the right iliac fossa.
- Rotation is essential for normal adult intestinal anatomy.
🔬 CONCEPT EXPLAINED
The midgut loop rotates because the intestine must fit into the abdominal cavity in an organized way.
Rotation occurs around the superior mesenteric artery, which remains fixed as the central vascular axis.
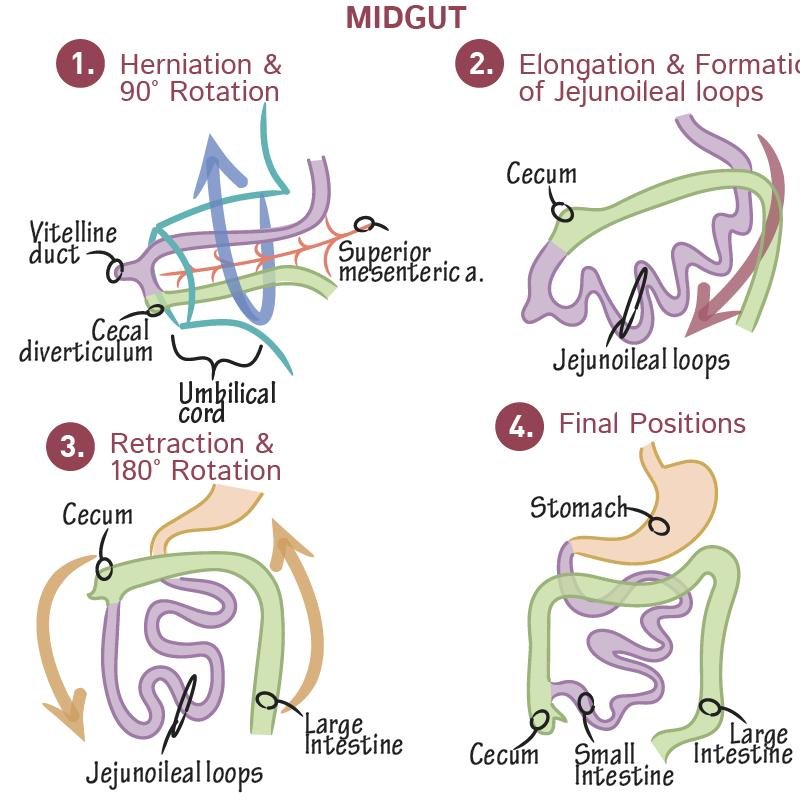
Stepwise Concept
- The primary intestinal loop forms.
- It herniates into the umbilical cord.
- It rotates 90 degrees counterclockwise.
- The cranial limb elongates rapidly.
- The loop returns to the abdomen.
- During return, it rotates another 180 degrees counterclockwise.
- Total rotation becomes 270 degrees.
This rotation explains why:
- Jejunum and ileum lie mostly in the central abdomen.
- Cecum and ascending colon lie on the right side.
- Transverse colon crosses the abdomen.
- The superior mesenteric artery supplies all midgut derivatives.
⚠️ IF DAMAGED
Failure of normal rotation causes intestinal malrotation.
Cause → Effect:
Incomplete rotation → abnormal gut fixation → narrow mesenteric base → risk of volvulus.
Volvulus can twist the intestine around SMA, causing intestinal obstruction and ischemia.
3: Physiological Herniation
🧠 CORE
- Physiological herniation is a normal developmental event.
- It occurs because the midgut grows faster than the abdominal cavity.
- It usually occurs around the 6th week of development.
- The midgut temporarily enters the extraembryonic cavity of the umbilical cord.
- The cranial limb grows rapidly during this period.
- Return to the abdominal cavity occurs around the 10th week.
- The midgut returns in a specific order.
- Failure of return may cause congenital abdominal wall defects.
🔬 CONCEPT EXPLAINED
During early fetal life, the liver and intestines grow rapidly.
The abdominal cavity is temporarily too small to contain all developing organs.
Therefore, the midgut loop herniates into the umbilical cord.
This is not abnormal. It is called physiological herniation because it normally occurs during development.
By the 10th week, the abdominal cavity enlarges enough to receive the intestines back.
Why It Exists
- Allows rapid intestinal elongation.
- Provides temporary space for developing gut.
- Permits midgut rotation outside the tight abdominal cavity.
⚠️ IF DAMAGED
If the herniated intestine fails to return, congenital defects may occur.
Cause → Effect:
Failure of return of midgut → persistent herniation at umbilicus → omphalocele.
In omphalocele, abdominal contents remain outside the abdominal cavity covered by a membrane.
4: Derivatives of Midgut Loop
🧠 CORE
The midgut gives rise to:
- Distal part of duodenum
- Jejunum
- Ileum
- Cecum
- Appendix
- Ascending colon
- Proximal two-thirds of transverse colon
Key features:
- All midgut derivatives are supplied by the superior mesenteric artery.
- They receive parasympathetic supply mainly from the vagus nerve.
- Pain from midgut structures is commonly referred around the umbilicus.
- The cranial limb forms most of small intestine.
- The caudal limb forms distal ileum and large intestinal derivatives.
🔬 CONCEPT EXPLAINED
The adult gut can be understood by embryological origin.
The midgut extends from the region distal to the opening of the bile duct in the duodenum up to the proximal two-thirds of the transverse colon.
Because all these structures develop from the same embryological region, they share:
- Common arterial supply
- Common lymphatic drainage pattern
- Similar visceral pain referral pattern
Development → Adult Structure Link
- Cranial limb → distal duodenum, jejunum, major part of ileum.
- Caudal limb → terminal ileum, cecum, appendix, ascending colon, proximal transverse colon.
Structure → Function
- Small intestine derivatives → digestion and absorption.
- Cecum and colon derivatives → water absorption and fecal movement.
- Appendix → lymphoid tissue contribution.
⚠️ IF DAMAGED
Developmental disturbance can lead to:
- Abnormal position of cecum
- Malrotation
- Congenital bands causing obstruction
- Abnormal persistence of vitelline duct
Cause → Effect:
Faulty derivative positioning → abnormal adult anatomy → intestinal obstruction or volvulus.
5: Development of Mesenteries
🧠 CORE
- Mesenteries are double layers of peritoneum.
- They suspend the gut from the body wall.
- They carry blood vessels, lymphatics, and nerves.
- The midgut is suspended by the dorsal mesentery.
- Ventral mesentery is not present in the midgut region.
- Rotation of the gut changes the position of mesenteries.
- Some parts retain mesentery and remain mobile.
- Some parts lose mesentery and become secondarily retroperitoneal.
- Proper mesenteric fixation prevents twisting of bowel.
🔬 CONCEPT EXPLAINED
The developing gut tube is suspended in the abdominal cavity by mesenteries.
The midgut has a dorsal mesentery that attaches it to the posterior abdominal wall.
As the midgut rotates and returns to the abdominal cavity, the mesentery also changes position.
This helps produce the final arrangement of small and large intestine.
Adult Result
Structures retaining mesentery:
- Jejunum
- Ileum
- Transverse colon
Structures becoming secondarily retroperitoneal:
- Ascending colon
- Descending colon
The mesentery is important because it carries:
- Superior mesenteric artery branches
- Veins
- Lymphatics
- Autonomic nerves
⚠️ IF DAMAGED
Improper mesenteric fixation may cause excessive mobility of intestine.
Cause → Effect:
Narrow mesenteric attachment → bowel twists around its vascular pedicle → volvulus → obstruction and ischemia.
6: Developmental Anomalies of Midgut
🧠 CORE
Common developmental anomalies include:
- Meckel’s diverticulum
- Vitelline fistula
- Vitelline cyst
- Fibrous vitelline band
- Omphalocele
- Malrotation
- Midgut volvulus
- Non-rotation
These occur due to failure of:
- Normal vitelline duct obliteration
- Normal return of herniated midgut
- Normal rotation
- Normal fixation of mesentery
🔬 CONCEPT EXPLAINED
Midgut anomalies are clinically important because they can present with intestinal obstruction, bleeding, abdominal pain, or umbilical discharge.
Meckel’s Diverticulum
- Caused by persistence of proximal vitelline duct.
- Present on the ileum.
- May contain ectopic gastric or pancreatic tissue.
- Can cause painless bleeding or inflammation.
Vitelline Fistula
- Complete persistence of vitelline duct.
- Connects ileum to umbilicus.
- May cause fecal discharge from umbilicus.
Vitelline Cyst
- Central part of vitelline duct persists.
- Forms a cyst between ileum and umbilicus.
Fibrous Band
- Vitelline duct becomes a fibrous cord.
- May cause intestinal obstruction.
Omphalocele
- Failure of physiological herniated midgut to return.
- Abdominal contents remain outside but covered by membrane.
Malrotation
- Failure of normal 270-degree counterclockwise rotation.
- May cause abnormal intestinal position and volvulus.
⚠️ IF DAMAGED
Cause → Effect examples:
- Persistent vitelline duct → abnormal ileum-umbilicus connection → umbilical discharge.
- Incomplete rotation → narrow mesenteric base → volvulus.
- Failure of return → omphalocele.
- Fibrous vitelline band → trapping of bowel loop → intestinal obstruction.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
- Midgut loop formation → increases intestinal length → allows development of absorptive surface.
- Physiological herniation → provides temporary space → permits rapid gut growth.
- Rotation around SMA → organizes gut position → produces normal adult intestinal arrangement.
- Cranial limb growth → forms jejunum and ileum → supports digestion and absorption.
- Caudal limb development → forms cecum and colon → supports water absorption and fecal movement.
- Dorsal mesentery → carries vessels and nerves → maintains blood supply and gut mobility.
- Mesenteric fixation → prevents abnormal twisting → protects against volvulus.
🩺 5️⃣ Clinical Correlation
1. Meckel’s Diverticulum
- Most common congenital anomaly of gastrointestinal tract.
- Due to persistence of proximal vitelline duct.
- Present on ileum.
- May cause bleeding, inflammation, or mimic appendicitis.
2. Vitelline Fistula
- Complete persistence of vitelline duct.
- Connects ileum with umbilicus.
- May present with fecal discharge from umbilicus.
3. Omphalocele
- Failure of midgut to return to abdominal cavity.
- Abdominal organs remain outside the abdomen.
- Covered by a membranous sac.
4. Malrotation
- Incomplete or abnormal rotation of midgut.
- Intestines occupy abnormal positions.
- May cause intestinal obstruction.
5. Midgut Volvulus
- Twisting of bowel around SMA.
- Can cause obstruction and ischemia.
- Clinically important emergency in infants.
6. Fibrous Vitelline Band
- Remnant of vitelline duct becomes a fibrous band.
- Can trap intestinal loops.
- May cause intestinal obstruction.
📌 6️⃣ Summary Points
- Midgut derivatives are supplied by the superior mesenteric artery.
- Midgut extends from distal duodenum to proximal two-thirds of transverse colon.
- Primary intestinal loop forms due to rapid elongation of midgut.
- Midgut rotation is 270 degrees counterclockwise around SMA.
- Physiological herniation occurs around the 6th week.
- Return of midgut to abdomen occurs around the 10th week.
- Cranial limb mainly forms jejunum and ileum.
- Caudal limb forms distal ileum, cecum, appendix, ascending colon, and proximal transverse colon.
- Meckel’s diverticulum is due to persistence of proximal vitelline duct.
- Failure of return of midgut causes omphalocele.
- Malrotation predisposes to volvulus.
- Dorsal mesentery carries vessels, nerves, and lymphatics to the midgut.