
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
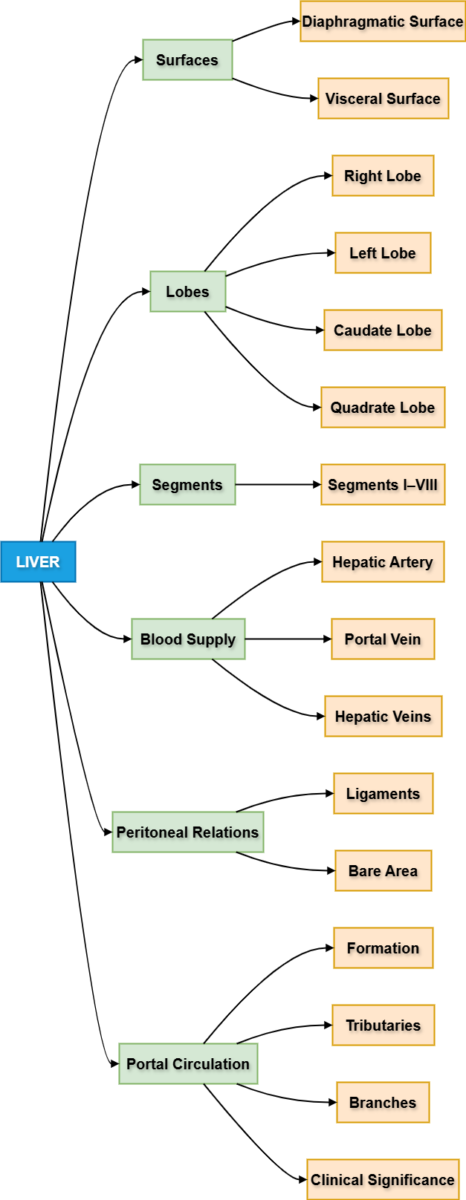
The liver is the largest gland in the human body and plays a central role in metabolism, detoxification, and digestion. It is located mainly in the right upper quadrant of the abdomen beneath the diaphragm. Understanding the liver’s gross anatomy and vascular connections is essential for interpreting imaging, diagnosing liver diseases, and performing surgical procedures. The hepatic portal circulation forms a vital pathway that transports nutrients from the gastrointestinal tract to the liver. Peritoneal reflections and ligaments help suspend the liver and define important clinical spaces such as Morrison’s pouch. Knowledge of these anatomical relationships is critical in trauma, ascites, portal hypertension, and liver diseases.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Liver — Largest gland in the body responsible for metabolism, detoxification, and bile production.
- Portal circulation — Venous system that carries blood from abdominal organs to the liver.
- Peritoneum — Serous membrane lining abdominal cavity and covering abdominal organs.
- Ligaments of liver — Peritoneal folds attaching liver to surrounding structures.
- Portal vein — Main vein carrying nutrient-rich blood to the liver.
- Hepatorenal pouch (Morrison’s pouch) — Space between liver and right kidney.
- Liver segments — Functional subdivisions based on vascular supply.
Essential Terminology
- Anterior surface
- Posterior surface
- Superior surface
- Inferior (visceral) surface
- Bare area
- Porta hepatis
- Falciform ligament
- Coronary ligament
- Ligamentum teres
- Ligamentum venosum
Basic Overview
- Liver lies beneath diaphragm.
- Mostly occupies right hypochondrium.
- Has dual blood supply.
- Connected to stomach, duodenum, and pancreas through vascular network.
- Covered mostly by peritoneum.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. Borders and Surfaces of Liver
🧠 CORE
- Liver has two main surfaces:
- Diaphragmatic surface
- Visceral surface
- Borders:
- Inferior border
- Posterior border
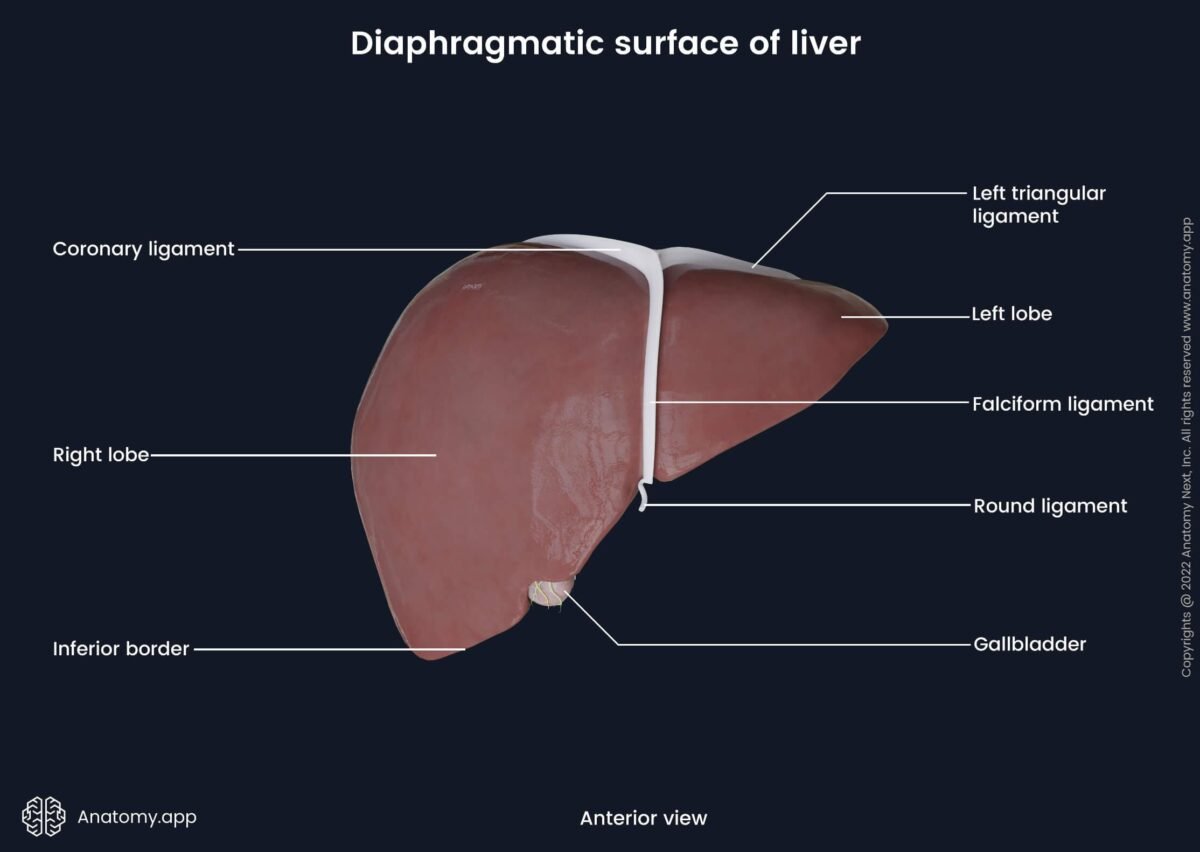
- Diaphragmatic surface:
- Smooth and convex
- Faces diaphragm
- Visceral surface:
- Irregular
- Contains impressions of organs
- Superior surface:
- Lies under diaphragm
- Anterior surface:
- Faces abdominal wall
- Posterior surface:
- Related to inferior vena cava (IVC)
🔬 CONCEPT EXPLAINED
The liver has a smooth diaphragmatic surface, shaped to match the dome of the diaphragm. This large convex surface allows tight contact with the diaphragm, aiding in respiratory movement synchronization.
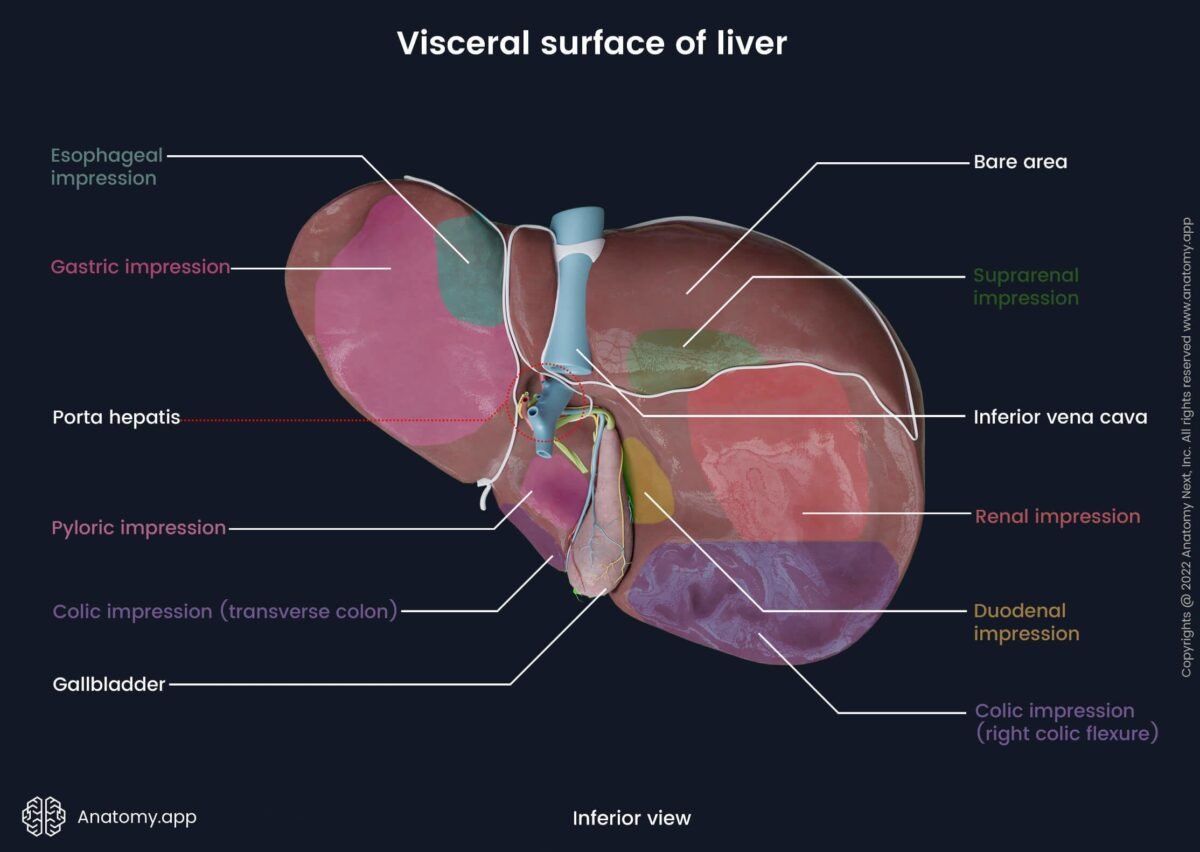
The visceral surface is irregular because it contacts several abdominal organs including stomach, duodenum, right kidney, and colon. These contacts form visceral impressions, which help identify anatomical orientation during surgery and imaging.
The inferior border is sharp and palpable during deep inspiration. Enlargement of liver (hepatomegaly) causes this border to descend below the costal margin.
Structure → Function:
Smooth convex diaphragm-facing surface allows respiratory movement and protection, while irregular visceral surface supports close contact with abdominal organs for vascular communication.
⚠️ IF DAMAGED
Cause → Effect:
Liver enlargement → Inferior border descends → Palpable below costal margin → Suggests hepatomegaly.
Trauma to posterior surface → Injury to IVC → Severe bleeding risk.
2. Visceral Surface of Liver
🧠 CORE
- Located inferiorly.
- Contains porta hepatis.
- Divided into lobes:
- Right lobe
- Left lobe
- Caudate lobe
- Quadrate lobe
- Shows impressions of:
- Stomach
- Right kidney
- Duodenum
- Colon
- Porta hepatis transmits:
- Portal vein
- Hepatic artery
- Bile duct
🔬 CONCEPT EXPLAINED
The visceral surface acts as the functional gateway of the liver. The porta hepatis lies centrally and serves as the entry and exit point for major vessels and ducts.
Organ impressions exist due to close anatomical relationships. For example:
- Gastric impression — contact with stomach
- Renal impression — contact with right kidney
- Colic impression — contact with colon
Structure → Function:
The arrangement of lobes around porta hepatis supports efficient vascular distribution.
⚠️ IF DAMAGED
Cause → Effect:
Blockage at porta hepatis → Impaired bile flow → Jaundice.
Tumor at visceral surface → Compression of portal vein → Portal hypertension.

3. Peritoneal Reflections of Liver
🧠 CORE
- Liver mostly covered by visceral peritoneum.
- Areas of reflection form ligaments.
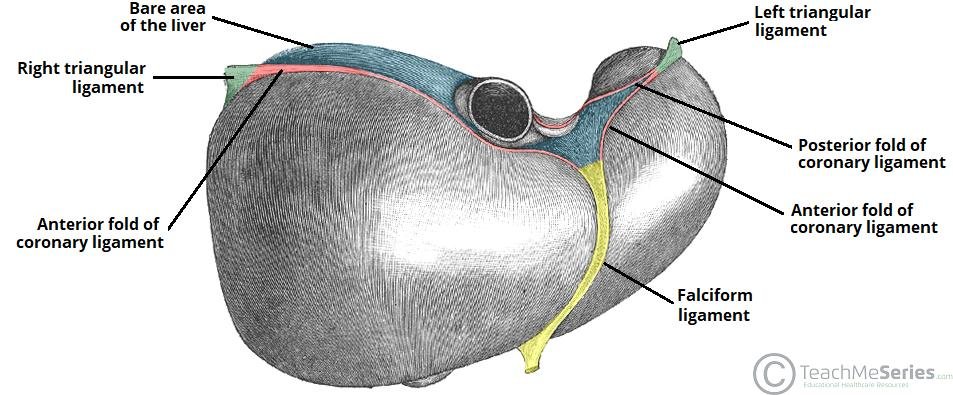
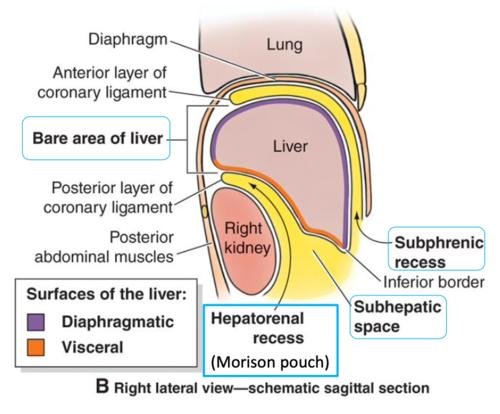
- Bare area lacks peritoneal covering.
- Peritoneal reflections attach liver to diaphragm.
- Defines subphrenic spaces.
🔬 CONCEPT EXPLAINED
Peritoneum folds around liver creating ligaments that stabilize the liver in position.
The bare area lies directly against diaphragm without peritoneal covering, allowing vascular and lymphatic communication.
Structure → Function:
Peritoneal reflections maintain position and reduce friction during movement.
⚠️ IF DAMAGED
Cause → Effect:
Fluid accumulation → Subphrenic abscess formation → Fever and abdominal pain.
4. Ligaments of Liver
🧠 CORE
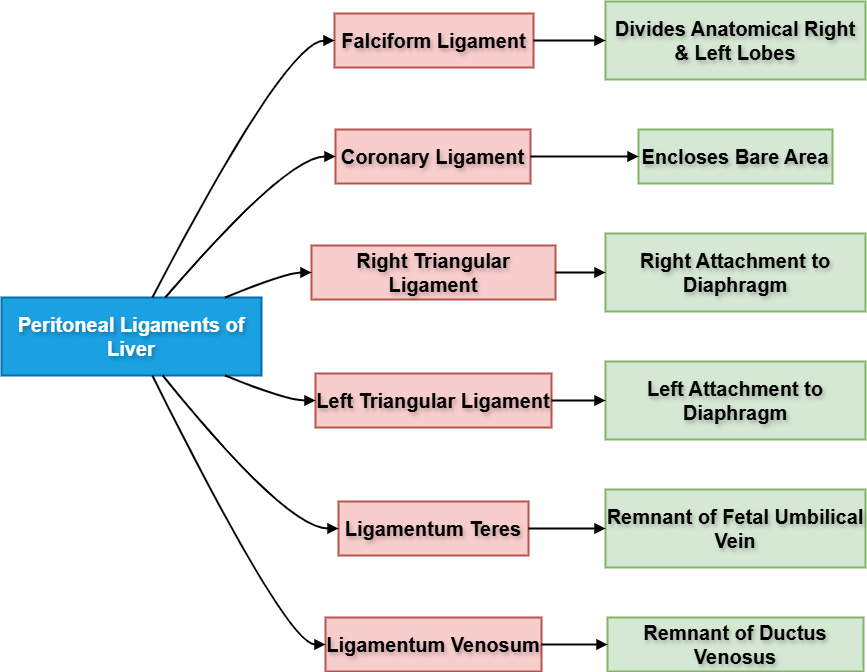
Main ligaments:
- Falciform ligament
- Coronary ligament
- Right triangular ligament
- Left triangular ligament
- Ligamentum teres
- Ligamentum venosum
Functions:
- Attach liver to diaphragm
- Support liver position
🔬 CONCEPT EXPLAINED
The falciform ligament divides liver into right and left anatomical lobes.
The ligamentum teres is a remnant of fetal umbilical vein.
The ligamentum venosum is a remnant of ductus venosus.
Structure → Function:
Ligaments stabilize liver during movement.
⚠️ IF DAMAGED
Cause → Effect:
Weak ligament support → Liver displacement → Altered anatomical relationships.
5. Lobes of Liver
🧠 CORE
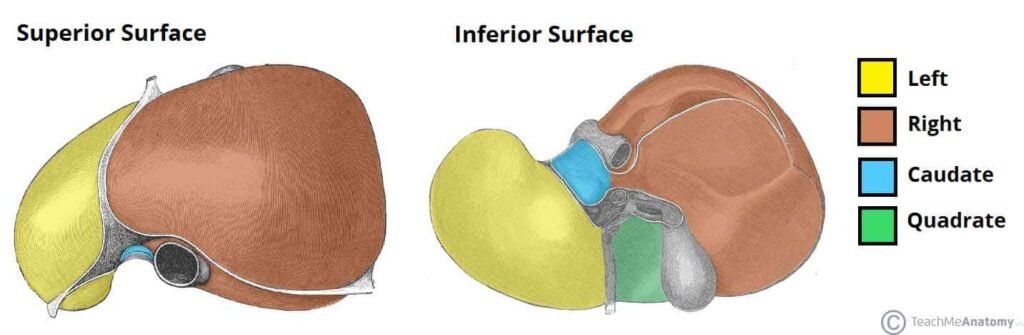
Four lobes:
- Right lobe
- Left lobe
- Caudate lobe
- Quadrate lobe
Functional division:
- Based on vascular supply.
🔬 CONCEPT EXPLAINED
Right lobe is largest.
Caudate and quadrate lobes are functionally part of left lobe.
Structure → Function:
Functional division supports segmental blood flow.
⚠️ IF DAMAGED
Cause → Effect:
Lobe disease → Segmental dysfunction → Localized liver failure.
6. Segments of Liver
🧠 CORE
- Liver divided into 8 functional segments.
- Based on portal vein branches.
- Each segment has:
- Portal vein branch
- Hepatic artery branch
- Bile duct
🔬 CONCEPT EXPLAINED
Segments act as independent functional units. This allows surgical removal of one segment without affecting others.
Structure → Function:
Segmental design allows targeted surgery.
⚠️ IF DAMAGED
Cause → Effect:
Segment obstruction → Local necrosis → Segmental liver dysfunction.
7. Blood Supply of Liver
🧠 CORE
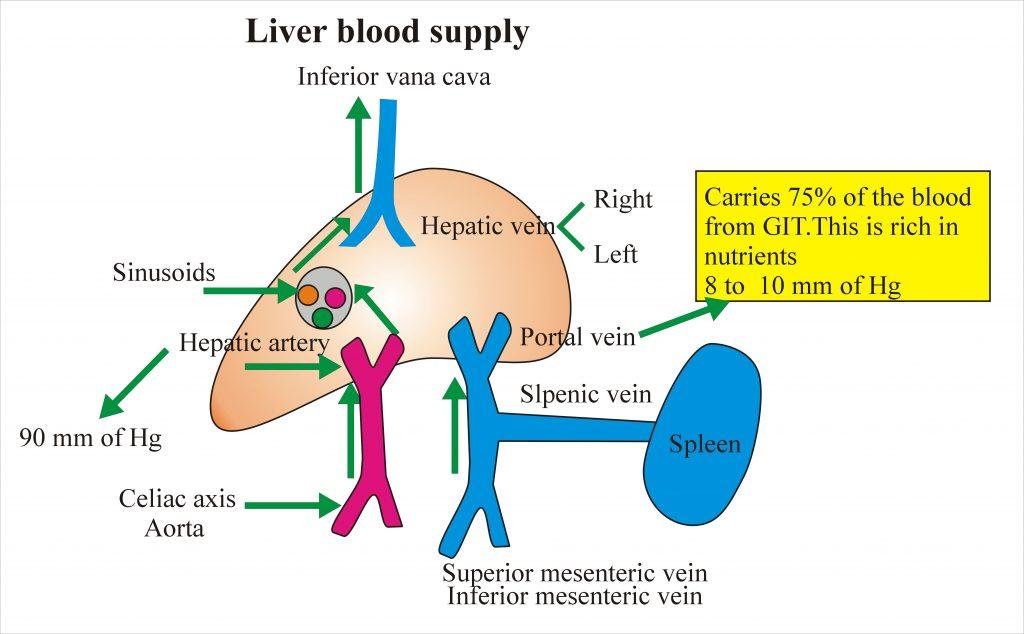
Dual blood supply:
- Hepatic artery (oxygenated blood)
- Portal vein (nutrient-rich blood)
Venous drainage:
- Hepatic veins → IVC
🔬 CONCEPT EXPLAINED
Portal vein supplies most liver blood (~75%).
Hepatic artery supplies oxygen.
Structure → Function:
Dual supply ensures continuous metabolic activity.
⚠️ IF DAMAGED
Cause → Effect:
Portal vein obstruction → Portal hypertension.
Hepatic artery injury → Liver ischemia.
8. Hepatorenal Pouch (Morrison’s Pouch)
🧠 CORE
- Located between:
- Liver
- Right kidney
- Deepest peritoneal space in supine position.
- First site of fluid collection.
🔬 CONCEPT EXPLAINED
Gravity directs fluid into this pouch during supine position.
Structure → Function:
Acts as fluid collection site.
⚠️ IF DAMAGED
Cause → Effect:
Fluid accumulation → Detectable on ultrasound.
9. Clinical Significance of Hepatorenal Pouch
🧠 CORE
Fluid accumulation seen in:
- Ascites
- Hemorrhage
- Peritonitis
🔬 CONCEPT EXPLAINED
FAST ultrasound detects fluid here first.
⚠️ IF DAMAGED
Cause → Effect:
Trauma → Blood collects → Early diagnostic sign.
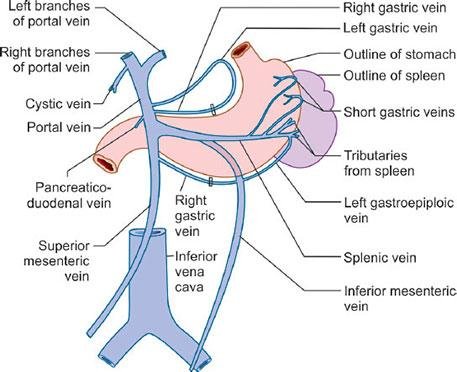
10. Formation of Hepatic Portal Vein
🧠 CORE
Formed by union of:
- Superior mesenteric vein
- Splenic vein
Location:
Behind pancreas neck.
🔬 CONCEPT EXPLAINED
Portal vein collects nutrient-rich blood from intestines.
Structure → Function:
Allows metabolic processing before systemic circulation.
⚠️ IF DAMAGED
Cause → Effect:
Portal vein blockage → Portal hypertension.
11. Tributaries of Portal Vein
🧠 CORE
Major tributaries:
- Splenic vein
- Superior mesenteric vein
- Left gastric vein
🔬 CONCEPT EXPLAINED
Tributaries drain digestive organs.
Structure → Function:
Ensures nutrient transport.
⚠️ IF DAMAGED
Cause → Effect:
Obstruction → Venous congestion.
12. Branches of Portal Venous System
🧠 CORE
Portal vein divides into:
- Right portal vein
- Left portal vein
🔬 CONCEPT EXPLAINED
These branches supply functional liver segments.
⚠️ IF DAMAGED
Cause → Effect:
Branch blockage → Segment necrosis.
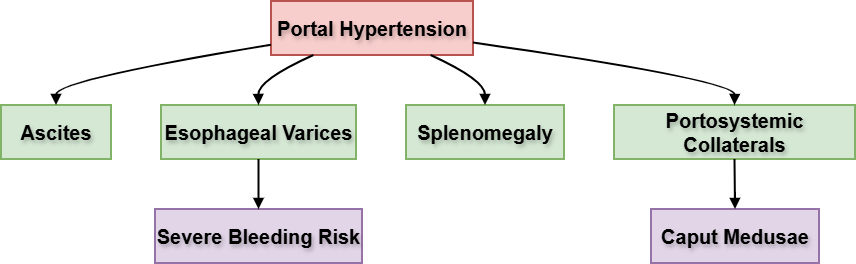
13. Clinical Significance of Portal System
🧠 CORE
Portal hypertension leads to:
- Ascites
- Varices
- Splenomegaly
🔬 CONCEPT EXPLAINED
Raised portal pressure forces blood through collateral pathways.
⚠️ IF DAMAGED
Cause → Effect:
Portal hypertension → Esophageal varices → Life-threatening bleeding.
⚙️ 4️⃣ Functional Flow
- Nutrients absorbed from intestine.
- Blood enters superior mesenteric vein.
- Splenic vein joins SMV.
- Portal vein formed.
- Portal vein enters liver.
- Blood distributed into segments.
- Processed blood exits via hepatic veins.
- Drains into inferior vena cava.
🩺 5️⃣ Clinical Correlation
Common Conditions:
- Hepatomegaly
- Portal hypertension
- Ascites
- Esophageal varices
- Subphrenic abscess
- Liver cirrhosis
- Portal vein thrombosis
📌 6️⃣ Summary Points
- Liver has dual blood supply.
- Porta hepatis is the gateway of liver.
- Morrison’s pouch is first site of fluid collection.
- Portal vein formed behind pancreas.
- Liver divided into 8 segments.
- Falciform ligament separates anatomical lobes.
- Bare area lacks peritoneum.
- Portal hypertension causes varices.
- Hepatic veins drain into IVC.
- Right lobe is largest.
- Caudate lobe lies posteriorly.