
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The large intestine plays an essential role in water absorption, fecal storage, mucus secretion, and elimination of waste from the body. Unlike the small intestine, its major function is not digestion but movement and processing of fecal material. Coordinated colonic motility and defecation reflexes ensure proper bowel evacuation while maintaining continence. Reflexes such as the gastro-colic and duodeno-colic reflex help move colonic contents after meals. The large intestine also secretes mucus that protects the mucosa and facilitates passage of stool. Disturbance of these mechanisms can lead to important clinical disorders such as constipation, diarrhea, spinal cord-related bowel dysfunction, and megacolon. Understanding colonic physiology is important for explaining common gastrointestinal complaints encountered in clinical practice.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Colon: Major part of large intestine responsible for absorption of water and fecal storage.
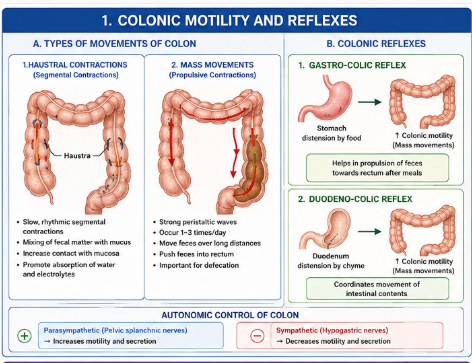
- Haustration: Segmental sac-like contractions of colon.
- Mass movement: Powerful peristaltic contraction moving feces long distances.
- Defecation reflex: Reflex mechanism responsible for expulsion of feces.
- Gastro-colic reflex: Increased colonic motility after stomach distension.
- Duodeno-colic reflex: Increased colonic movement after duodenal distension.
- Constipation: Difficult or infrequent passage of stool.
- Diarrhea: Increased frequency and liquidity of stool.
- Megacolon: Abnormal dilatation of colon due to impaired motility.
Essential Terminology
- Internal anal sphincter
- External anal sphincter
- Rectal distension
- Enteric nervous system
- Parasympathetic reflex
- Pelvic nerves
- Colonic propulsion
- Mucosal lubrication
Basic Overview
- Colon performs absorption of water and electrolytes.
- Colonic movements are slower than small intestine.
- Motility helps mixing and propulsion of feces.
- Defecation involves autonomic and voluntary control.
- Mucus secretion protects colonic mucosa.
- Failure of motility causes constipation or megacolon.
- Excess secretion and reduced absorption contribute to diarrhea.
🔹 3️⃣ Core Learning — Curriculum Coverage
Colonic Motility and Reflexes
Types of Movements of Colon
🧠 CORE
- Colon shows two major movement types:
- Haustral contractions
- Mass movements
- Haustrations are slow segmental contractions.
- Mass movements are strong propulsive contractions.
- Haustrations aid water absorption.
- Mass movements move feces toward rectum.
- Colonic motility is regulated by enteric and autonomic nerves.
- Parasympathetic stimulation increases motility.
- Sympathetic stimulation reduces motility.
🔬 CONCEPT EXPLAINED
Haustral Contractions
Haustrations are slow segmental contractions produced mainly by circular muscle of the colon. These contractions divide the colon into pouch-like sacculations called haustra.
Structure → Function
- Segmental contractions expose fecal matter to mucosa.
- Increased mucosal contact improves water and electrolyte absorption.
- Slow movement allows temporary storage of feces.
Mass Movements
Mass movements are powerful peristaltic contractions occurring a few times daily, especially after meals.
Stepwise Mechanism
- Strong contraction begins in transverse colon.
- Circular and longitudinal muscles contract together.
- Contraction wave travels toward sigmoid colon.
- Fecal material is rapidly propelled into rectum.
- Rectal distension initiates defecation reflex.
Why It Exists
Mass movements clear the colon and create space for incoming intestinal contents.
⚠️ IF DAMAGED
Reduced Colonic Motility
Cause:
- Low fiber diet
- Neurological disorders
- Reduced parasympathetic activity
Effect:
- Excess water absorption
- Hard stool formation
- Constipation
Excess Motility
Cause:
- Infection
- Irritation
- Hyperactive reflexes
Effect:
- Reduced absorption time
- Loose stools
- Diarrhea
Gastro-colic Reflex
🧠 CORE
- Reflex increases colonic motility after meals.
- Triggered by stomach distension.
- Mediated through autonomic and enteric pathways.
- Produces mass movements in colon.
- Helps move feces toward rectum.
- Stronger in infants and young children.
- Important physiological post-meal reflex.
🔬 CONCEPT EXPLAINED
The gastro-colic reflex is initiated when food enters the stomach and stretches the gastric wall.
Stepwise Mechanism
- Food distends stomach.
- Stretch receptors in gastric wall activated.
- Neural signals travel through autonomic pathways.
- Colonic motility increases.
- Mass movements propel feces toward rectum.
- Urge for defecation may occur after meals.
Structure → Function
- Stomach acts as sensory trigger.
- Colon responds by increasing propulsion.
- Coordination ensures efficient intestinal transit.
Why It Exists
The reflex helps empty the distal bowel to accommodate incoming intestinal contents.
⚠️ IF DAMAGED
Cause:
- Autonomic dysfunction
- Neurological disease
Effect:
- Reduced bowel propulsion
- Delayed bowel emptying
- Constipation
Duodeno-colic Reflex
🧠 CORE
- Reflex initiated by duodenal distension.
- Increases colonic motility.
- Helps propel fecal material.
- Coordinates movement throughout intestine.
- Works with gastro-colic reflex.
🔬 CONCEPT EXPLAINED
When chyme enters the duodenum, stretch receptors stimulate neural pathways that increase colonic activity.
Stepwise Mechanism
- Chyme enters duodenum.
- Duodenal wall stretches.
- Neural reflex pathways activated.
- Colonic motility increases.
- Fecal movement toward rectum accelerates.
Structure → Function
- Duodenum detects incoming intestinal contents.
- Colon prepares for movement and evacuation.
- Coordination maintains smooth digestive flow.
⚠️ IF DAMAGED
Effect:
- Sluggish bowel movement
- Delayed fecal propulsion
- Constipation
Defecation Physiology
Mechanism of Defecation Reflex
🧠 CORE
- Defecation begins with rectal distension.
- Reflex involves enteric and parasympathetic pathways.
- Internal anal sphincter relaxes involuntarily.
- External anal sphincter is under voluntary control.
- Pelvic nerves carry parasympathetic fibers.
- Reflex strengthened by abdominal muscle contraction.
- Defecation can be voluntarily delayed.
🔬 CONCEPT EXPLAINED
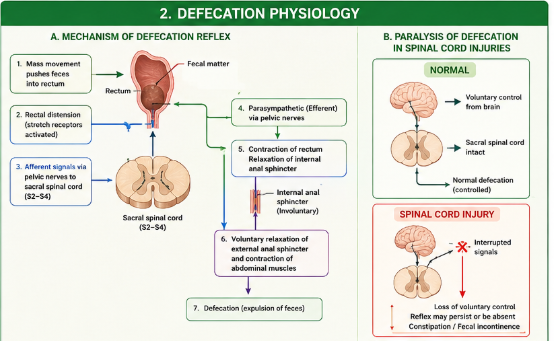
Defecation is a coordinated reflex involving rectum, anal sphincters, pelvic floor muscles, spinal cord, and autonomic nerves.
Stepwise Mechanism
- Mass movement pushes feces into rectum.
- Rectal wall stretches.
- Stretch receptors activated.
- Signals travel to sacral spinal cord.
- Parasympathetic fibers stimulate rectal contraction.
- Internal anal sphincter relaxes.
- External anal sphincter voluntarily relaxes.
- Abdominal muscles contract.
- Feces expelled through anal canal.
Structure → Function
- Internal sphincter maintains involuntary continence.
- External sphincter allows conscious control of defecation.
- Pelvic parasympathetic nerves coordinate reflex activity.
Why It Exists
The reflex allows controlled elimination of waste while maintaining continence between bowel movements.
⚠️ IF DAMAGED
Loss of Reflex Pathway
Cause:
- Sacral spinal cord damage
- Pelvic nerve injury
Effect:
- Loss of bowel control
- Constipation or fecal incontinence
Paralysis of Defecation in Spinal Cord Injuries
🧠 CORE
- Spinal cord injury disrupts defecation control.
- Sacral reflex pathways may be damaged.
- Voluntary control of external sphincter lost.
- Defecation may become reflex or absent.
- Severe constipation commonly occurs.
- Fecal incontinence may develop.
🔬 CONCEPT EXPLAINED
Normal defecation requires communication between rectum, spinal cord, and brain.
Stepwise Mechanism
- Rectal distension occurs normally.
- Signals cannot properly reach higher centers.
- Voluntary sphincter control lost.
- Defecation becomes impaired.
- Stool retention or incontinence develops.
Structure → Function
- Sacral spinal segments coordinate parasympathetic reflexes.
- Higher brain centers regulate voluntary continence.
Why Clinical Dysfunction Occurs
Interruption of neural pathways prevents coordinated bowel evacuation.
⚠️ IF DAMAGED
Effects:
- Chronic constipation
- Fecal impaction
- Reflex bowel emptying
- Fecal incontinence
Secretory Functions of Large Intestine
Secretion of Mucus by Large Intestine
🧠 CORE
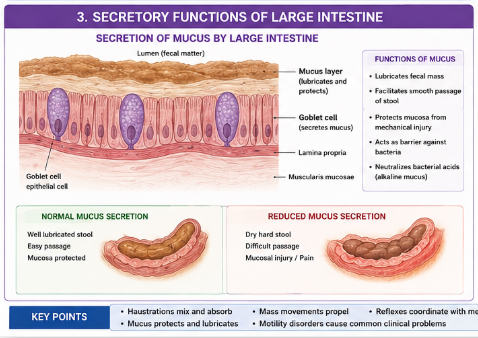
- Colon mainly secretes mucus.
- Goblet cells produce mucus.
- Large intestine does not secrete digestive enzymes.
- Mucus lubricates fecal matter.
- Mucus protects mucosa from injury.
- Alkaline mucus neutralizes bacterial acids.
- Secretion increases during irritation.
🔬 CONCEPT EXPLAINED
The mucosa of the large intestine contains numerous goblet cells specialized for mucus secretion.
Structure → Function
- Goblet cells synthesize mucin.
- Mucin absorbs water forming slippery mucus.
- Lubrication facilitates passage of stool.
- Protective mucus layer prevents mucosal trauma.
Stepwise Mechanism
- Goblet cells produce mucin granules.
- Mucin released onto mucosal surface.
- Water combines with mucin forming mucus.
- Mucus coats fecal material and mucosa.
- Stool passage becomes smooth and less traumatic.
Why It Exists
The colon handles dry fecal matter; lubrication is necessary to prevent injury during defecation.
⚠️ IF DAMAGED
Cause:
- Reduced mucus secretion
- Inflammation
Effect:
- Painful defecation
- Mucosal injury
- Ulceration
Disorders of Bowel Function
Constipation
🧠 CORE
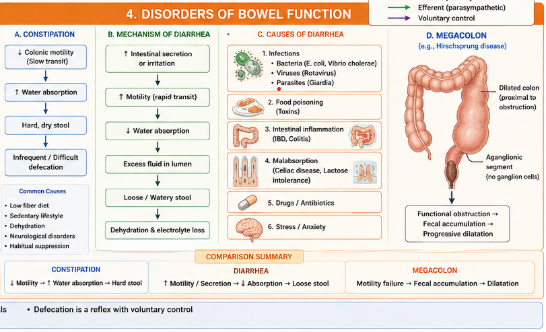
- Constipation means infrequent or difficult bowel evacuation.
- Often caused by slow colonic transit.
- Excess water absorption hardens stool.
- Low fiber intake is common cause.
- Neurological disorders may contribute.
- Chronic constipation may produce hemorrhoids.
🔬 CONCEPT EXPLAINED
Stepwise Mechanism
- Colonic motility decreases.
- Transit time increases.
- More water absorbed from feces.
- Stool becomes hard and dry.
- Defecation becomes painful and difficult.
Structure → Function
- Normal colonic motility prevents excessive water absorption.
- Reduced movement causes stool retention.
Why It Happens
Slow movement allows prolonged contact between stool and absorptive mucosa.
⚠️ IF DAMAGED
Effects:
- Fecal impaction
- Hemorrhoids
- Anal fissures
- Abdominal discomfort
Mechanism of Diarrhea
🧠 CORE
- Diarrhea is passage of frequent loose stool.
- Caused by reduced absorption or increased secretion.
- Rapid intestinal transit decreases water absorption.
- Infection commonly causes diarrhea.
- Severe diarrhea leads to dehydration.
- Electrolyte imbalance may occur.
🔬 CONCEPT EXPLAINED
Stepwise Mechanism
- Infection or irritation stimulates intestine.
- Intestinal secretion increases.
- Motility becomes excessive.
- Water absorption decreases.
- Excess fluid remains in lumen.
- Loose stool passed frequently.
Structure → Function
- Normal colon absorbs water efficiently.
- Excess motility shortens absorption time.
Why Dangerous
Large fluid and electrolyte loss can impair circulation and cellular function.
⚠️ IF DAMAGED
Effects:
- Dehydration
- Hypokalemia
- Weakness
- Circulatory collapse
Causes of Diarrhea
🧠 CORE
Common causes include:
- Bacterial infections
- Viral infections
- Food poisoning
- Intestinal inflammation
- Increased motility
- Malabsorption disorders
- Anxiety and stress
🔬 CONCEPT EXPLAINED
Infectious Causes
Microbial toxins stimulate intestinal secretion and motility.
Inflammatory Causes
Inflammation damages mucosa reducing absorption.
Functional Causes
Stress and anxiety increase autonomic stimulation causing rapid transit.
Structure → Function
- Healthy mucosa absorbs water efficiently.
- Damaged mucosa fails to absorb properly.
⚠️ IF DAMAGED
Persistent diarrhea may cause:
- Malnutrition
- Severe dehydration
- Electrolyte imbalance
Megacolon
🧠 CORE
- Megacolon is abnormal dilatation of colon.
- Usually caused by impaired colonic motility.
- Hirschsprung disease is common congenital cause.
- Affected segment lacks enteric ganglion cells.
- Feces accumulate proximal to obstruction.
- Severe constipation develops.
🔬 CONCEPT EXPLAINED
Structure
In Hirschsprung disease, enteric ganglion cells are absent in part of colon.
Stepwise Mechanism
- Aganglionic segment cannot relax.
- Functional obstruction develops.
- Fecal material accumulates proximally.
- Colon progressively dilates.
- Severe constipation and distension occur.
Structure → Function
- Enteric ganglia coordinate colonic relaxation and propulsion.
- Loss of ganglion cells causes motility failure.
Why It Happens
Failure of neural crest cell migration during development results in absent enteric ganglia.
⚠️ IF DAMAGED
Effects:
- Severe constipation
- Abdominal distension
- Intestinal obstruction
- Toxic megacolon in severe cases
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| Haustrations | Mixing and absorption | Water conservation |
| Mass movements | Fecal propulsion | Rectal filling |
| Goblet cells | Mucus secretion | Lubrication and protection |
| Internal anal sphincter | Involuntary continence | Stool retention |
| External anal sphincter | Voluntary continence | Controlled defecation |
| Enteric ganglia | Coordinate motility | Normal bowel movement |
🩺 5️⃣ Clinical Correlation
Hirschsprung Disease
- Congenital absence of enteric ganglion cells.
- Produces congenital megacolon and severe constipation.
Spinal Cord Injury
- Causes loss of voluntary bowel control.
- Reflex bowel emptying may persist.
Chronic Constipation
- Common with low-fiber diet and sedentary lifestyle.
Infectious Diarrhea
- Major cause of dehydration, especially in children.
Ulcerative Colitis
- Colonic inflammation causing diarrhea and bleeding.
📌 6️⃣ Summary Points
- Colon mainly absorbs water and electrolytes.
- Haustrations are mixing contractions.
- Mass movements propel feces long distances.
- Gastro-colic reflex increases motility after meals.
- Defecation begins with rectal distension.
- Internal anal sphincter is involuntary.
- External anal sphincter is voluntary.
- Goblet cells secrete protective mucus.
- Slow transit causes constipation.
- Excess motility contributes to diarrhea.
- Hirschsprung disease causes congenital megacolon.
- Severe diarrhea can cause life-threatening dehydration.