
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
The hindgut forms the terminal part of the embryonic gut tube and gives rise to important structures of the distal gastrointestinal and urogenital systems. Proper partitioning of the cloaca is essential for separation of urinary and digestive pathways during fetal life. Histologically, the large intestine is specialized mainly for absorption of water and electrolytes and formation of feces rather than nutrient absorption. Understanding the microscopic organization of the colon and rectum helps students recognize normal tissue architecture and identify pathological changes in disease. Developmental defects of the hindgut can lead to serious congenital anomalies such as imperforate anus and fistulas. This topic integrates Embryology and Histology to explain how embryonic development produces the adult structure and function of the large intestine.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Hindgut: Caudal part of primitive gut tube extending from distal one-third of transverse colon to upper anal canal.
- Cloaca: Common embryonic chamber receiving intestinal and urinary tracts.
- Urorectal septum: Mesodermal partition dividing cloaca into urogenital sinus and anorectal canal.
- Large intestine: Portion of gastrointestinal tract involved mainly in water absorption and feces formation.
- Crypts of Lieberkühn: Straight tubular intestinal glands present in large intestine.
- Goblet cells: Mucus-secreting epithelial cells abundant in colon.
Essential Terminology
- Cloacal membrane
- Anal canal
- Rectum
- Cecum
- Colon
- Taeniae coli
- Haustra
- Mucosa
- Muscularis externa
- Enterocytes
Basic Overview
- Hindgut develops during embryonic folding of primitive gut.
- Cloaca initially acts as a common cavity for digestive and urinary systems.
- Urorectal septum divides the cloaca into separate systems.
- Hindgut derivatives form distal gastrointestinal tract.
- Colon histology is adapted for lubrication and water absorption.
- Rectum shows transition toward anal canal structure.
🔹 3️⃣ Core Learning — Curriculum Coverage
EMBRYOLOGY
A. Partitioning of Cloaca
🧠 CORE
- Cloaca is the terminal dilated part of hindgut.
- Present during early embryonic development.
- Endoderm lines the cloaca internally.
- Closed externally by cloacal membrane.
- Urorectal septum divides cloaca.
- Division occurs during 4th–7th week.
- Anterior part forms urogenital sinus.
- Posterior part forms anorectal canal.
- Cloacal membrane divides into anal and urogenital membranes.
🔬 CONCEPT EXPLAINED
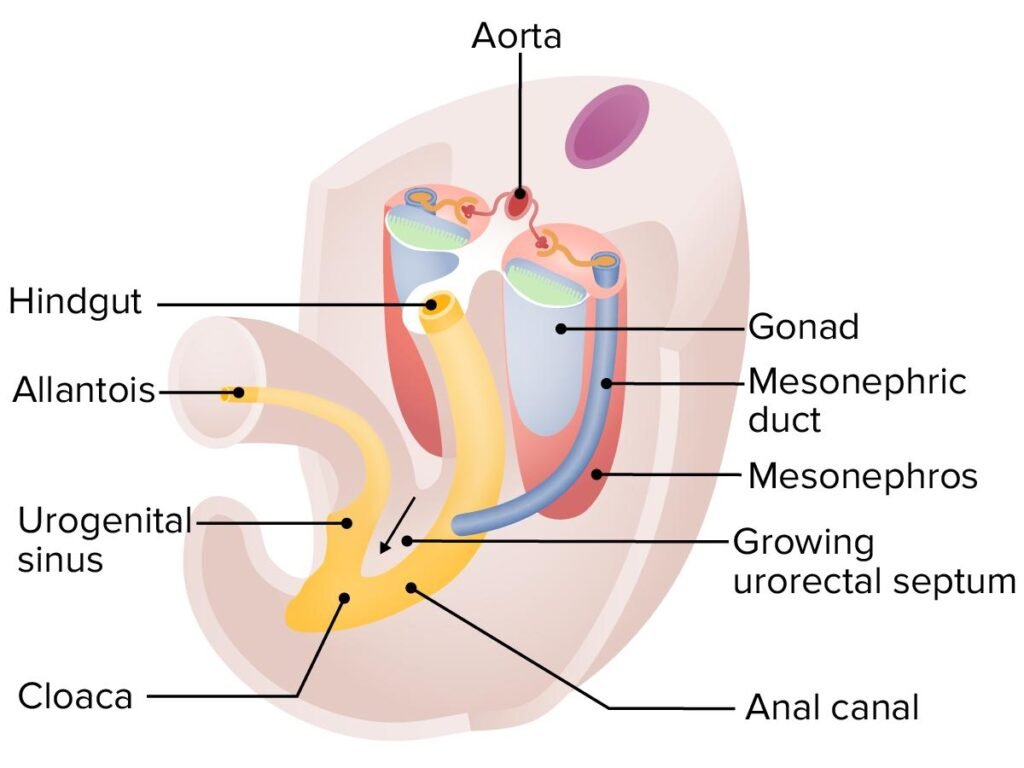
The cloaca is a common chamber where the intestinal, urinary, and genital tracts initially open during embryonic life. It is located at the caudal end of the embryo.
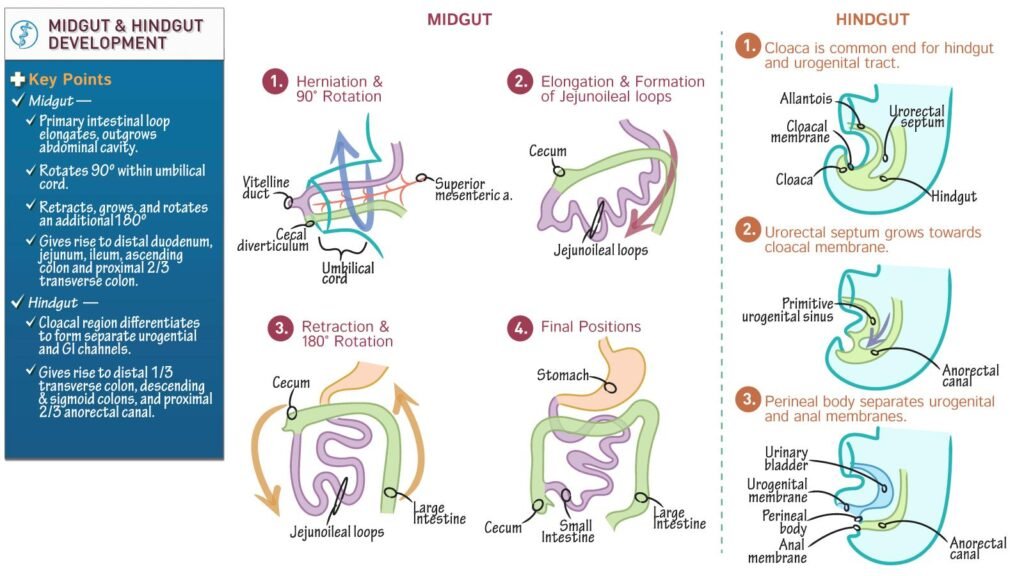
A wedge of mesoderm called the urorectal septum grows downward between the primitive hindgut and allantois. As the septum enlarges, it gradually divides the cloaca into two separate compartments:
- Anterior compartment → Urogenital sinus
- Posterior compartment → Anorectal canal
Eventually, the urorectal septum reaches the cloacal membrane and divides it into:
- Urogenital membrane anteriorly
- Anal membrane posteriorly
Later, the anal membrane ruptures to create the anal opening.
Structure → Function
- Separation of urinary and digestive tracts prevents mixing of urine and feces.
- Proper partitioning establishes normal pelvic anatomy.
⚠️ IF DAMAGED
Failure of urorectal septum development
Cause → Incomplete partitioning of cloaca
Effect → Rectourethral or rectovaginal fistulas
Cause → Failure of anal membrane rupture
Effect → Imperforate anus
Cause → Abnormal septum positioning
Effect → Anorectal malformations
B. Derivatives of Hindgut
🧠 CORE
- Hindgut forms distal one-third of transverse colon.
- Gives rise to descending colon.
- Forms sigmoid colon.
- Forms rectum.
- Forms upper anal canal.
- Epithelium derived from endoderm.
- Connective tissue and muscle derived from splanchnic mesoderm.
- Blood supply mainly from inferior mesenteric artery.
🔬 CONCEPT EXPLAINED
The hindgut extends from the distal third of the transverse colon to the upper anal canal.
Major derivatives include:
- Distal transverse colon
- Descending colon
- Sigmoid colon
- Rectum
- Upper two-thirds of anal canal
The epithelial lining develops from endoderm, while smooth muscle, connective tissue, and blood vessels develop from surrounding mesoderm.
Development → Adult Structure Link
- Embryonic hindgut rotation and elongation help position the adult colon.
- Mesenteric fixation determines mobility of bowel segments.
Structure → Function
- Large intestinal derivatives specialize in:
- Water absorption
- Fecal storage
- Lubrication by mucus secretion
⚠️ IF DAMAGED
Cause → Abnormal recanalization
Effect → Intestinal stenosis or atresia
Cause → Failure of migration/fixation
Effect → Malrotation or volvulus risk
Cause → Aganglionosis in distal bowel
Effect → Hirschsprung disease with severe constipation
C. Developmental Anomalies of Hindgut
🧠 CORE
- Imperforate anus is common anomaly.
- Rectourethral fistula may occur in males.
- Rectovaginal fistula may occur in females.
- Hirschsprung disease affects enteric ganglia.
- Congenital megacolon results from aganglionosis.
- Anal stenosis may develop due to incomplete canalization.
- Abnormal cloacal partitioning causes anorectal defects.
🔬 CONCEPT EXPLAINED
Developmental anomalies occur when normal embryological steps fail.
Hirschsprung Disease
Neural crest cells normally migrate into bowel wall to form enteric ganglia. Failure of migration leads to absence of ganglion cells in distal colon.
Without ganglia:
- Peristalsis fails
- Bowel remains contracted
- Feces accumulate proximally
This produces congenital megacolon.
Imperforate Anus
Occurs when anal membrane fails to rupture properly.
Fistulas
Incomplete separation of cloaca causes abnormal communication between rectum and urinary or genital tracts.
⚠️ IF DAMAGED
Cause → Absence of enteric ganglia
Effect → Severe constipation and abdominal distension
Cause → Persistent fistulous connection
Effect → Fecal contamination of urinary tract
Cause → Anal obstruction
Effect → Failure to pass meconium in newborn
HISTOLOGY
D. Histological Features of Colon
🧠 CORE
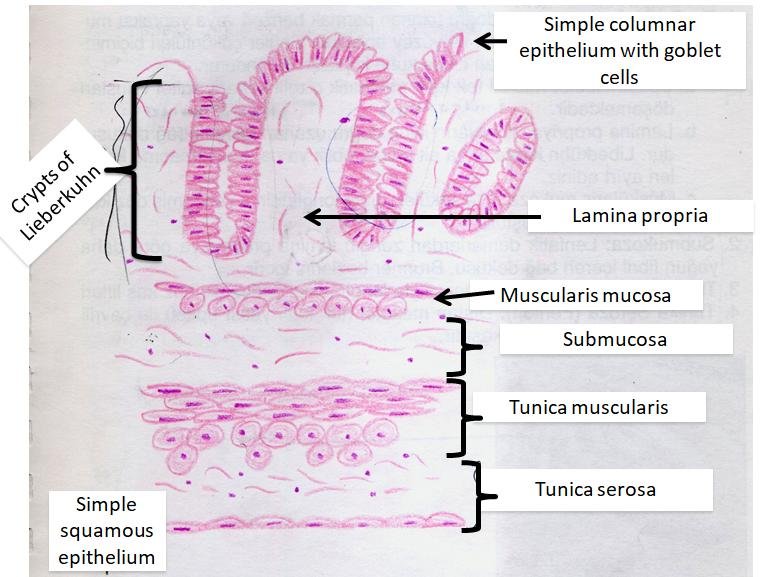
- Colon mucosa lacks villi.
- Surface lined by simple columnar epithelium.
- Numerous goblet cells present.
- Straight tubular glands are present.
- Crypts of Lieberkühn are deep and numerous.
- Lamina propria contains lymphoid tissue.
- Muscularis externa has taeniae coli.
- Main function is water absorption and lubrication.
🔬 CONCEPT EXPLAINED
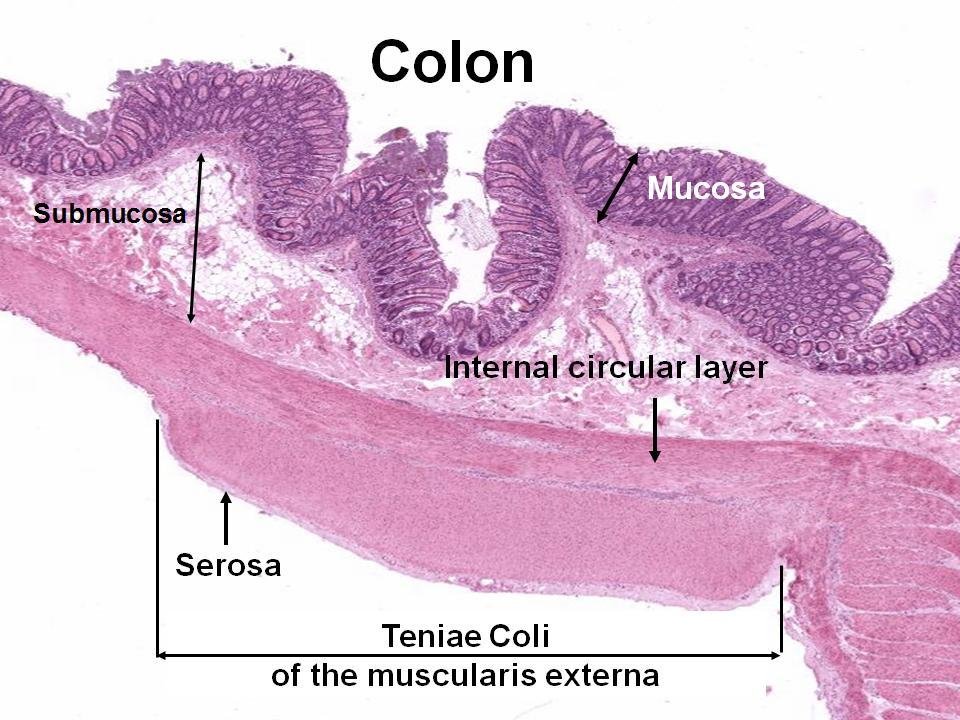
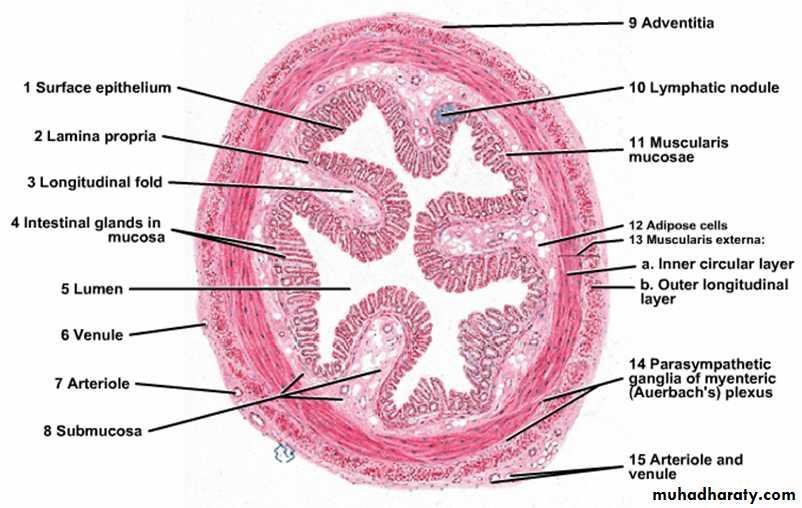
The colon wall has four layers:
- Mucosa
- Submucosa
- Muscularis externa
- Serosa/adventitia
Microscopic Appearance
- No villi are present.
- Surface epithelium contains absorptive cells and goblet cells.
- Goblet cells increase distally.
Intestinal Glands
The crypts are long, straight tubular glands extending toward muscularis mucosa.
Structure → Function
- Absorptive cells reclaim water and electrolytes.
- Goblet cells secrete mucus to lubricate feces.
- Lack of villi reflects reduced role in nutrient absorption.
Muscularis Externa
Outer longitudinal muscle forms three bands called taeniae coli, producing sacculations called haustra.
⚠️ IF DAMAGED
Cause → Goblet cell damage
Effect → Poor lubrication and mucosal injury
Cause → Inflammation of mucosa
Effect → Colitis with diarrhea and bleeding
Cause → Weak muscular wall
Effect → Diverticula formation
E. Characteristic Features of Intestinal Glands
🧠 CORE
- Called crypts of Lieberkühn.
- Straight tubular glands.
- Extend into lamina propria.
- Rich in goblet cells.
- Contain absorptive cells.
- Paneth cells usually absent in colon.
- Open onto luminal surface.
- Important for mucus secretion.
🔬 CONCEPT EXPLAINED
The intestinal glands of the large intestine are deeper and straighter than those of the small intestine.
Cell Arrangement
Main cell types include:
- Goblet cells
- Columnar absorptive cells
- Stem cells
- Enteroendocrine cells
Goblet cells become more numerous toward rectum.
Structure → Function
- Straight glands permit continuous mucus secretion.
- Stem cells maintain epithelial renewal.
- Mucus protects mucosa from friction caused by feces.
Recognition Features for Exams
- No villi
- Numerous goblet cells
- Straight parallel crypts
⚠️ IF DAMAGED
Cause → Crypt inflammation
Effect → Ulceration and diarrhea
Cause → Stem cell injury
Effect → Impaired mucosal regeneration
Cause → Reduced mucus secretion
Effect → Increased mucosal trauma
F. Histological Features of Rectum
🧠 CORE
- Rectum resembles colon histologically.
- Goblet cells are very abundant.
- Deep intestinal glands present.
- No villi are present.
- Muscular layer thicker than colon.
- Longitudinal muscle becomes continuous.
- Rectum stores feces temporarily.
🔬 CONCEPT EXPLAINED
The rectum has a thicker muscular wall because it must store and expel feces.
Microscopic Appearance
- Mucosa contains numerous goblet cells.
- Straight crypts extend deeply.
- Muscularis externa is well developed.
Transition Toward Anal Canal
Near the anal canal:
- Epithelium gradually changes
- Simple columnar epithelium transitions toward stratified squamous epithelium
Structure → Function
- Thick muscle assists defecation.
- Increased mucus reduces friction during fecal passage.
⚠️ IF DAMAGED
Cause → Venous dilation
Effect → Hemorrhoids
Cause → Mucosal inflammation
Effect → Proctitis
Cause → Muscular dysfunction
Effect → Defecation difficulty
⚙️ 4️⃣ Functional Flow
| Structure | Function | Outcome |
|---|---|---|
| Urorectal septum | Separates cloaca | Independent urinary and digestive tracts |
| Goblet cells | Secrete mucus | Lubrication of feces |
| Absorptive cells | Absorb water | Formation of solid stool |
| Crypts of Lieberkühn | Mucus secretion and renewal | Protection of mucosa |
| Thick rectal muscle | Fecal propulsion | Defecation |
| Taeniae coli | Segmental contractions | Haustra formation |
🩺 5️⃣ Clinical Correlation
Hirschsprung Disease
- Congenital absence of enteric ganglion cells
- Causes functional intestinal obstruction
- Presents with constipation and abdominal distension
Imperforate Anus
- Failure of anal membrane rupture
- Newborn cannot pass meconium
- Requires surgical correction
Ulcerative Colitis
- Chronic inflammation of colon mucosa
- Causes ulcers, bleeding, and diarrhea
Diverticulosis
- Outpouching of colonic wall
- Common in elderly
- Associated with weak muscular wall
Hemorrhoids
- Dilated rectal veins
- Internal or external types
- Common due to increased venous pressure
📌 6️⃣ Summary Points
- Hindgut forms distal one-third of transverse colon to upper anal canal.
- Cloaca is divided by urorectal septum.
- Colon mucosa lacks villi.
- Goblet cells are abundant in large intestine.
- Crypts of Lieberkühn are straight tubular glands.
- Taeniae coli are characteristic of colon.
- Hirschsprung disease results from absent enteric ganglia.
- Imperforate anus results from failure of anal membrane rupture.
- Rectum has thicker muscular wall for defecation.
- Upper anal canal is endoderm-derived.
- Large intestine mainly absorbs water and electrolytes.
- Rectal epithelium transitions near anal canal.