
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
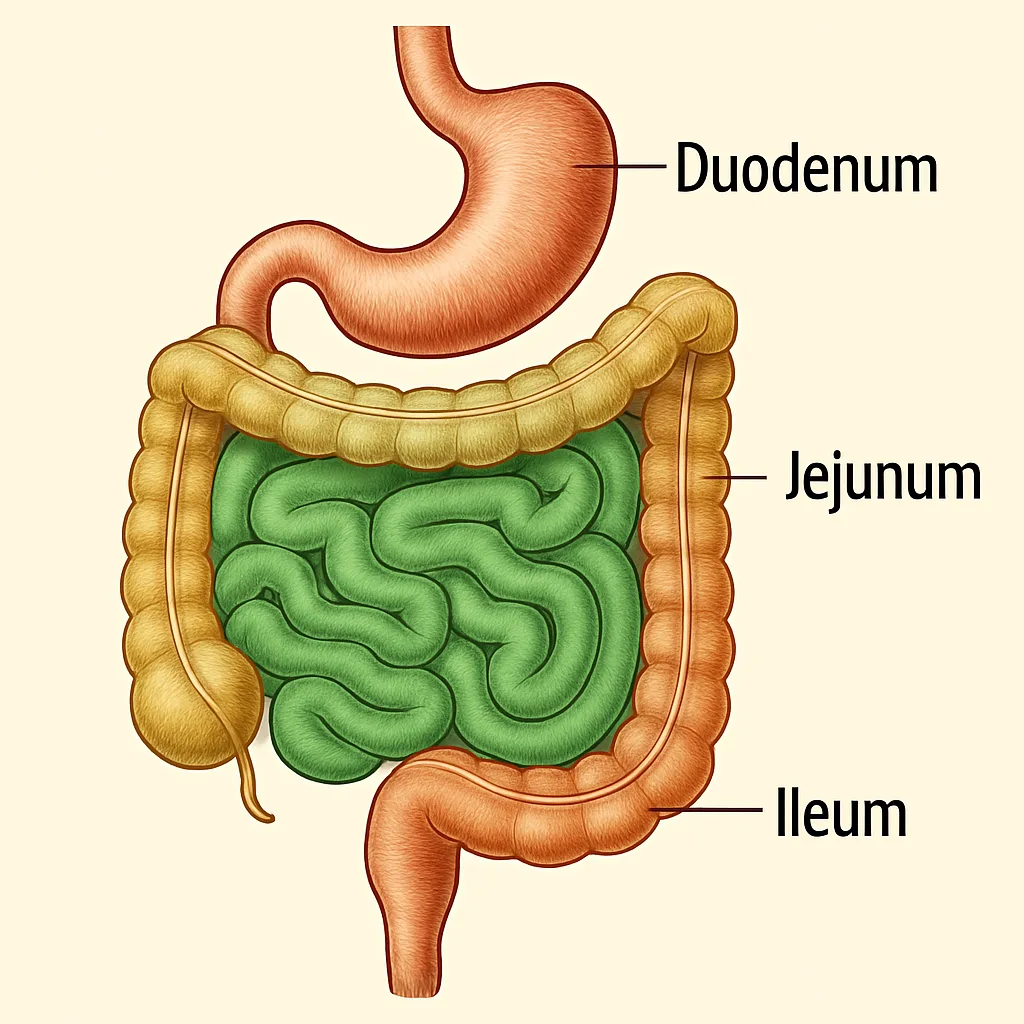
The jejunum and ileum form the major absorptive part of the small intestine. They extend from the duodenojejunal flexure to the ileocecal junction and occupy mainly the central and lower abdomen. The jejunum is mainly concerned with rapid absorption of nutrients, while the ileum is specialized for absorption of bile salts and vitamin B12. Both are suspended from the posterior abdominal wall by the mesentery, which carries blood vessels, lymphatics, and nerves. Clinically, knowledge of jejunum, ileum, and mesentery is important in intestinal obstruction, ischemia, Crohn disease, Meckel diverticulum, and volvulus.
🔹 2️⃣ Foundation Concepts
- Jejunum: Proximal two-fifths of the small intestine beyond the duodenum.
- Ileum: Distal three-fifths of the small intestine ending at the ileocecal junction.
- Mesentery: Double layer of peritoneum suspending jejunum and ileum from posterior abdominal wall.
- Root of mesentery: Oblique attachment from duodenojejunal flexure to ileocecal junction.
- Vasa recta: Straight terminal arterial branches supplying intestinal wall.
- Arterial arcades: Interconnected arterial loops formed by branches of superior mesenteric artery.
- Plicae circulares: Circular mucosal folds that increase surface area for absorption.
- Peyer’s patches: Aggregated lymphoid nodules, abundant in ileum.
- Ileocecal junction: Site where ileum opens into cecum
🔹 3️⃣ Core Learning — Curriculum Coverage
Objective 1: Gross Features of Jejunum
🧠 CORE
- Jejunum is the proximal two-fifths of the mobile small intestine.
- It begins at the duodenojejunal flexure.
- It lies mainly in the upper left part of the abdomen.
- It has a wider lumen than ileum.
- Its wall is thicker and more vascular.
- It appears redder because of richer blood supply.
- It has tall and numerous plicae circulares.
- It has fewer arterial arcades.
- It has long vasa recta.
- It has less mesenteric fat near the intestinal wall.
🔬 CONCEPT EXPLAINED
The jejunum is designed for active absorption of digested nutrients. Its thick wall and rich vascularity help rapid transfer of absorbed nutrients into blood.
The tall plicae circulares increase the surface area of mucosa. This increases contact between chyme and absorptive epithelium.
The long vasa recta supply blood directly to the jejunal wall. Since the jejunum performs intense absorption, it requires good perfusion.
Structure → Function:
Tall folds + rich blood supply + wide lumen → efficient mixing and absorption of nutrients.
⚠️ IF DAMAGED
- Jejunal ischemia → reduced blood supply → mucosal injury → malabsorption.
- Jejunal obstruction → food contents cannot pass → vomiting, abdominal distension, dehydration.
- Loss of jejunal surface area → reduced nutrient absorption → weight loss and nutritional deficiency.
2: Gross Features of Ileum
🧠 CORE
- Ileum is the distal three-fifths of the mobile small intestine.
- It ends at the ileocecal junction.
- It lies mainly in the lower right abdomen and pelvis.
- It has a narrower lumen than jejunum.
- Its wall is thinner.
- It is paler due to relatively less vascularity.
- Plicae circulares are fewer and lower.
- It has more arterial arcades.
- It has short vasa recta.
- It contains abundant Peyer’s patches.
🔬 CONCEPT EXPLAINED
The ileum receives intestinal contents after most digestion and absorption have already occurred. Therefore, its folds are less prominent than jejunum.
The ileum is important for absorption of bile salts and vitamin B12. It also has an immune role because it contains Peyer’s patches, which monitor intestinal antigens.
More arterial arcades provide collateral circulation, while short vasa recta reach the intestinal wall.
Structure → Function:
Peyer’s patches + distal location → immune surveillance before intestinal contents enter large intestine.
⚠️ IF DAMAGED
- Terminal ileal disease → reduced bile salt absorption → fat malabsorption and diarrhea.
- Ileal resection → vitamin B12 malabsorption → megaloblastic anemia.
- Inflammation of ileum → narrowing of lumen → intestinal obstruction.
3: Differences Between Jejunum and Ileum
🧠 CORE
| Feature | Jejunum | Ileum |
|---|---|---|
| Position | Upper left abdomen | Lower right abdomen and pelvis |
| Length | Proximal two-fifths | Distal three-fifths |
| Lumen | Wider | Narrower |
| Wall | Thick | Thin |
| Color | Redder | Paler |
| Plicae circulares | Tall and numerous | Few and low |
| Arterial arcades | Fewer | More |
| Vasa recta | Long | Short |
| Mesenteric fat | Less near wall | More, reaches near wall |
| Lymphoid tissue | Less | Peyer’s patches abundant |
🔬 CONCEPT EXPLAINED
The jejunum and ileum differ because they perform slightly different functions. The jejunum mainly absorbs nutrients, so it has a thick wall, wide lumen, and prominent folds.
The ileum has a stronger immune and selective absorption role. Therefore, it contains Peyer’s patches and is adapted for absorption of bile salts and vitamin B12.
Structure → Function:
Jejunum = absorption-focused design.
Ileum = immune + terminal absorption design.
⚠️ IF DAMAGED
- Jejunal damage → generalized nutrient malabsorption.
- Ileal damage → bile salt and vitamin B12 malabsorption.
- Ileal inflammation → may mimic appendicitis due to right lower abdominal pain.
4: Blood Supply of Jejunum and Ileum
🧠 CORE
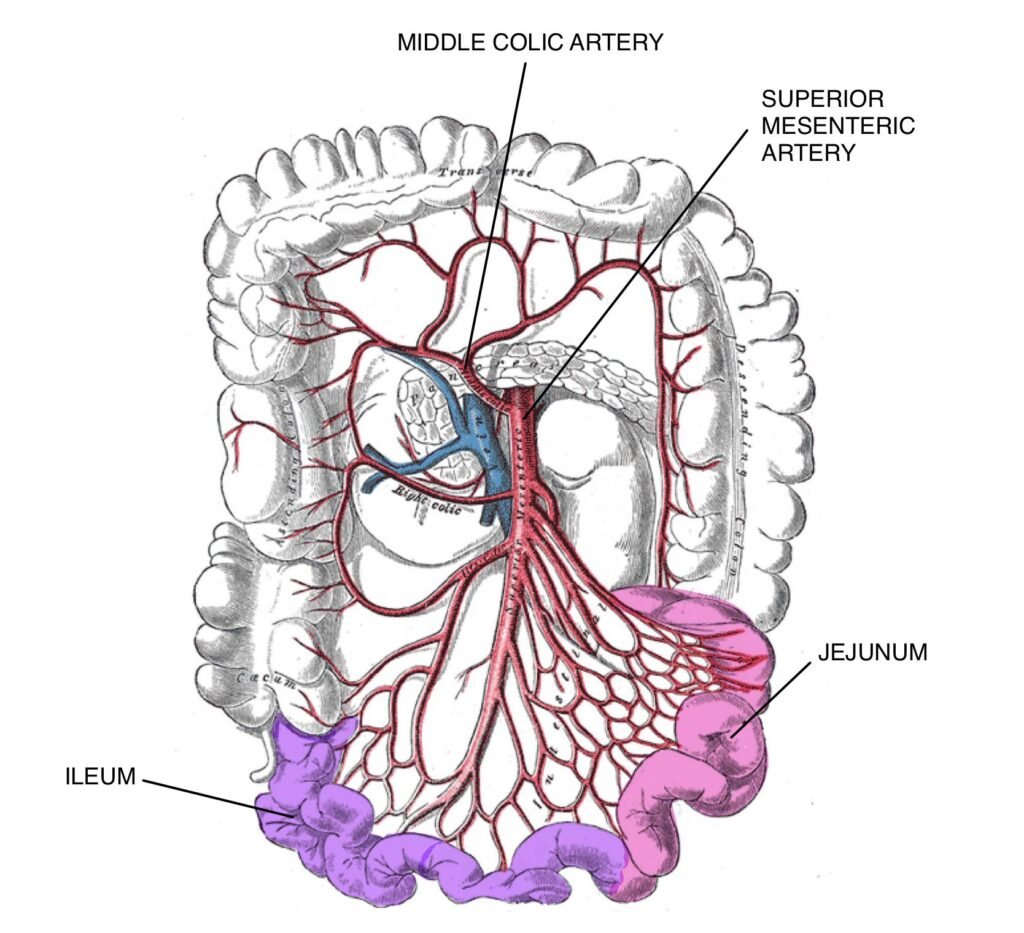
- Primary arterial supply comes from the superior mesenteric artery.
- Jejunal and ileal branches arise from the left side of the superior mesenteric artery.
- These branches form arterial arcades within the mesentery.
- Terminal straight branches are called vasa recta.
- Jejunum has fewer arcades and longer vasa recta.
- Ileum has more arcades and shorter vasa recta.
- Venous drainage follows arteries.
- Venous blood drains into the superior mesenteric vein.
- Superior mesenteric vein contributes to portal venous drainage.
- Lymph drains through mesenteric lymph nodes.
🔬 CONCEPT EXPLAINED
The superior mesenteric artery supplies the midgut. Since jejunum and ileum are midgut derivatives, they receive blood from jejunal and ileal branches of this artery.
Arterial arcades provide alternative pathways for blood flow. Vasa recta then carry blood directly to the intestinal wall.
Jejunum has long vasa recta because it needs strong direct blood supply for absorption. Ileum has more arcades, giving more collateral channels.
Structure → Function:
SMA branches → arcades → vasa recta → intestinal wall perfusion → absorption and motility.
⚠️ IF DAMAGED
- SMA obstruction → intestinal ischemia → severe abdominal pain and bowel necrosis.
- Mesenteric vessel injury → hemorrhage → reduced intestinal perfusion.
- Venous thrombosis → congestion → bowel edema and impaired absorption.
5: Mesentery of Small Intestine
🧠 CORE
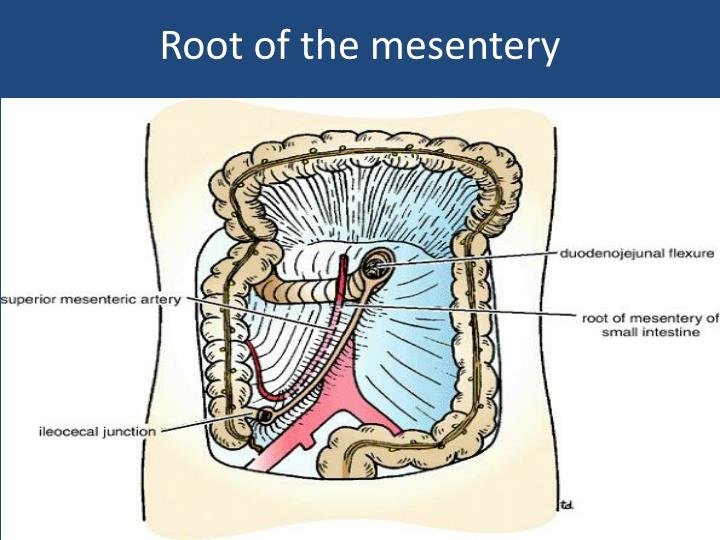
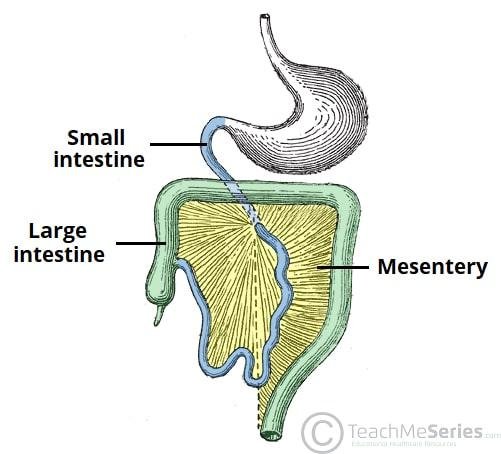
- Mesentery is a double layer of peritoneum.
- It suspends jejunum and ileum from posterior abdominal wall.
- Its root is attached obliquely.
- Root extends from duodenojejunal flexure to ileocecal junction.
- It carries arteries, veins, lymphatics, nerves, and fat.
- Superior mesenteric vessels pass within it.
- Mesenteric lymph nodes are present inside it.
- It allows mobility of jejunum and ileum.
- It maintains vascular connection with posterior abdominal wall.
- It prevents excessive twisting while allowing movement.
🔬 CONCEPT EXPLAINED
The jejunum and ileum are mobile parts of the small intestine. They need freedom of movement for peristalsis, but they also need a secure blood and nerve supply.
The mesentery solves both problems. It suspends the intestine and acts as a pathway for vessels, nerves, and lymphatics.
Its fan-shaped arrangement allows the long intestinal tube to be attached to a relatively short posterior abdominal wall root.
Structure → Function:
Double-layered peritoneal fold + vessels inside + mobile attachment → support, nutrition, drainage, and movement.
⚠️ IF DAMAGED
- Twisting of mesentery → volvulus → vascular compromise and obstruction.
- Mesenteric ischemia → reduced intestinal blood flow → bowel infarction.
- Mesenteric lymph node enlargement → abdominal pain, especially in infections.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
- Tall plicae circulares in jejunum → increased surface area → efficient nutrient absorption.
- Thick jejunal wall → strong motility and absorption → rapid processing of chyme.
- Rich jejunal vascularity → quick transport of absorbed nutrients → effective digestion support.
- Peyer’s patches in ileum → immune surveillance → protection against gut pathogens.
- Ileal specialization → bile salt and vitamin B12 absorption → normal fat digestion and RBC formation.
- Mesentery → suspends intestine and carries vessels → mobile but nourished bowel.
- Arterial arcades → collateral blood channels → protection against minor vascular compromise.
🩺 5️⃣ Clinical Correlation
1. Intestinal Obstruction
- Obstruction may occur due to adhesions, hernia, volvulus, or tumors.
- Jejunal obstruction usually causes early vomiting.
- Ileal obstruction causes abdominal distension and delayed vomiting.
2. Mesenteric Ischemia
- Caused by reduced blood flow through superior mesenteric vessels.
- Produces severe abdominal pain.
- If untreated, it may lead to bowel necrosis.
3. Crohn Disease
- Commonly affects terminal ileum.
- Can cause thickening, narrowing, pain, diarrhea, and malabsorption.
- May reduce bile salt and vitamin B12 absorption.
4. Meckel Diverticulum
- Congenital diverticulum usually found in ileum.
- It may cause bleeding, inflammation, or obstruction.
- Important exam point: usually located near the ileocecal junction.
5. Volvulus
- Twisting of bowel around mesentery.
- Causes obstruction and vascular compromise.
- If blood supply is blocked, bowel ischemia may occur.
📌 6️⃣ Summary Points
- Jejunum is proximal two-fifths; ileum is distal three-fifths of mobile small intestine.
- Jejunum lies mainly in the upper left abdomen.
- Ileum lies mainly in the lower right abdomen and pelvis.
- Jejunum has thick wall, wide lumen, tall folds, fewer arcades, and long vasa recta.
- Ileum has thin wall, narrow lumen, more arcades, short vasa recta, and Peyer’s patches.
- Jejunum is mainly for nutrient absorption.
- Ileum absorbs bile salts and vitamin B12.
- Blood supply is from jejunal and ileal branches of the superior mesenteric artery.
- Mesentery suspends jejunum and ileum and carries vessels, nerves, lymphatics, and fat.
- Terminal ileal disease may cause bile salt malabsorption and vitamin B12 deficiency.
- Mesenteric twisting can cause volvulus and intestinal ischemia.
- Peyer’s patches are a key identifying feature of ileum.