
📖 Learning Material
This section builds conceptual understanding of the oral cavity and tongue by integrating Anatomy, Embryology, Histology, ENT, and Clinical Medicine.
1️⃣ Introduction
The oral cavity and tongue form the beginning of the digestive tract and play a critical role in mastication, speech, taste, and swallowing. The tongue is a muscular organ located in the floor of the mouth, while the lips and teeth form the entrance and functional framework of the oral cavity.
Understanding this topic is essential because many clinical conditions such as oral ulcers, tongue paralysis, developmental anomalies, taste disturbances, and swallowing difficulty arise from defects in structure, development, histology, or nerve supply.
2️⃣ Foundation Basics
🔑 Key Definitions
- Oral cavity: First part of digestive tract bounded by lips, cheeks, palate, tongue, and teeth.
- Tongue: Muscular organ involved in taste, speech, swallowing, and food manipulation.
- Papillae: Surface projections on tongue responsible for taste and friction.
- Intrinsic muscles: Muscles that change the shape of tongue.
- Extrinsic muscles: Muscles that change the position of tongue.
- Lingual nerve: Nerve supplying general sensation to anterior two-thirds of tongue.
- Aphthous ulcer: Painful superficial ulcer of oral mucosa.
3️⃣ Core Learning
🔹 Anatomy
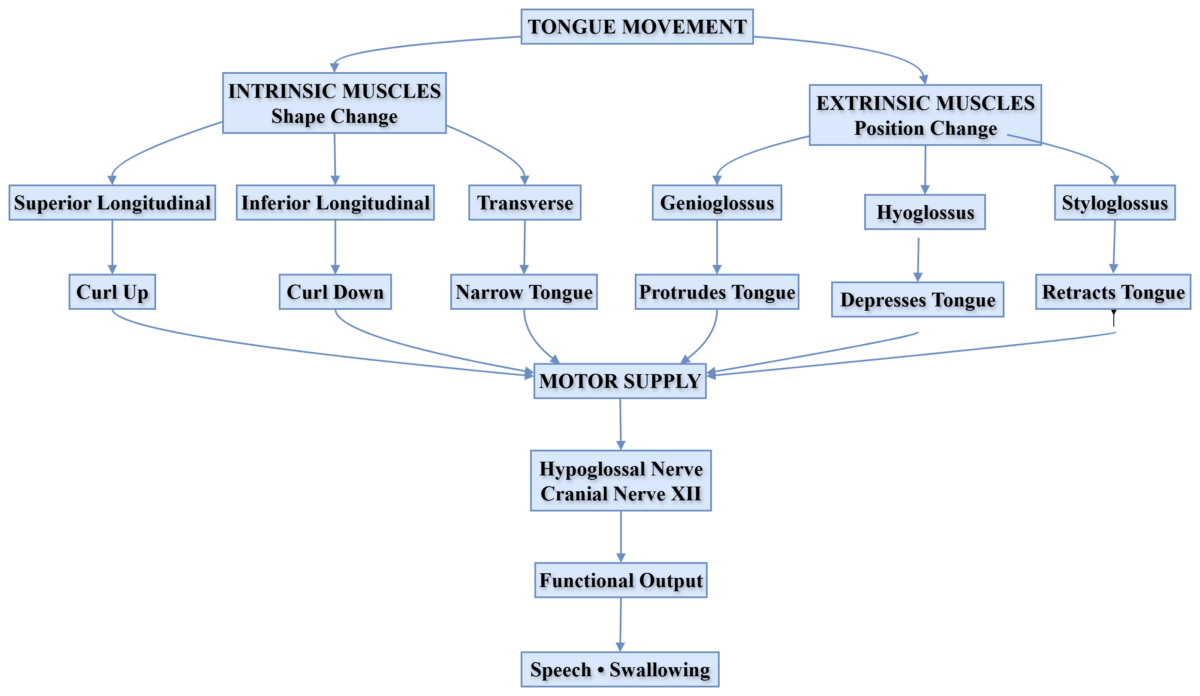
Musculature of Tongue
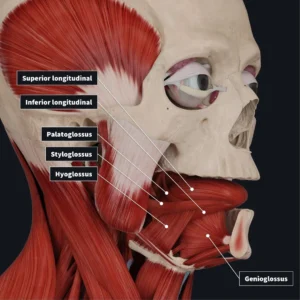
Muscles of the tongue are skeletal muscles responsible for movement and shape control.
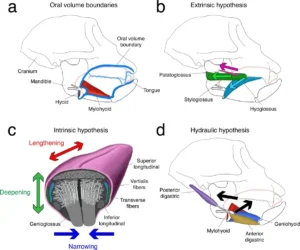
Intrinsic muscles — shape change:
- Superior longitudinal
- Inferior longitudinal
- Transverse
- Vertical
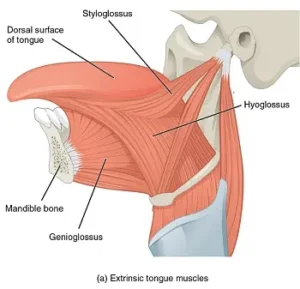
Extrinsic muscles — position change:
- Genioglossus
- Hyoglossus
- Styloglossus
- Palatoglossus
Intrinsic muscles change the shape of the tongue, allowing precise articulation and food manipulation. Extrinsic muscles move the tongue in different directions, helping in swallowing, speech, and maintaining airway patency.
Hypoglossal nerve injury can cause tongue paralysis. The tongue deviates toward the injured side, leading to speech difficulty and swallowing problems.
Nerve Supply of Tongue
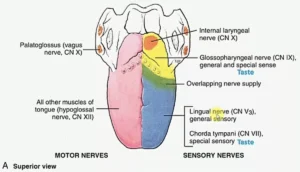
- Hypoglossal nerve CN XII → all tongue muscles except palatoglossus.
- Palatoglossus → vagus nerve CN X.
Sensory supply:
- Anterior 2/3 general sensation → lingual nerve CN V3.
- Anterior 2/3 taste → chorda tympani CN VII.
- Posterior 1/3 general sensation and taste → glossopharyngeal nerve CN IX.
- Posterior-most part → vagus nerve CN X.
Different parts of the tongue have different embryological origins. This explains why the anterior two-thirds and posterior one-third have different sensory and taste nerve supply.
- Lingual nerve injury: loss of general sensation from anterior tongue and risk of unnoticed tongue biting.
- Chorda tympani injury: loss of taste from anterior two-thirds of tongue.
- Glossopharyngeal nerve injury: impaired taste and sensation from posterior one-third; may also affect gag reflex.
- Hypoglossal nerve injury: tongue weakness, deviation, speech difficulty, and swallowing difficulty.
🧠 Concept Map
MAP 1: Tongue Muscles & Nerve Supply
Blood Supply of Tongue
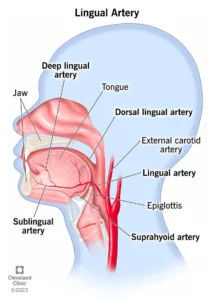
- Primary arterial supply → lingual artery.
- Parent artery → external carotid artery.
- Major branches → dorsal lingual, deep lingual, and sublingual arteries.
- Venous drainage → lingual vein to internal jugular vein.
🔹 Embryology
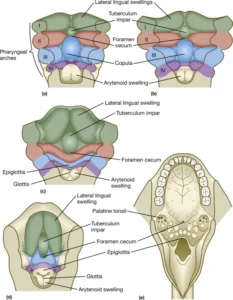
Development of Tongue
- Anterior 2/3 develops mainly from the first pharyngeal arch.
- Posterior 1/3 develops mainly from the third pharyngeal arch.
- Posterior-most part develops from the fourth arch.
- Tongue development begins around the 4th week and is completed by the 8th week.
- Tongue muscles migrate from occipital somites.
The different arch origins of the tongue explain the different cranial nerve supply of its anterior and posterior regions. This is a high-yield embryology-anatomy integration point.
🧠 MAP 2: Development of Tongue
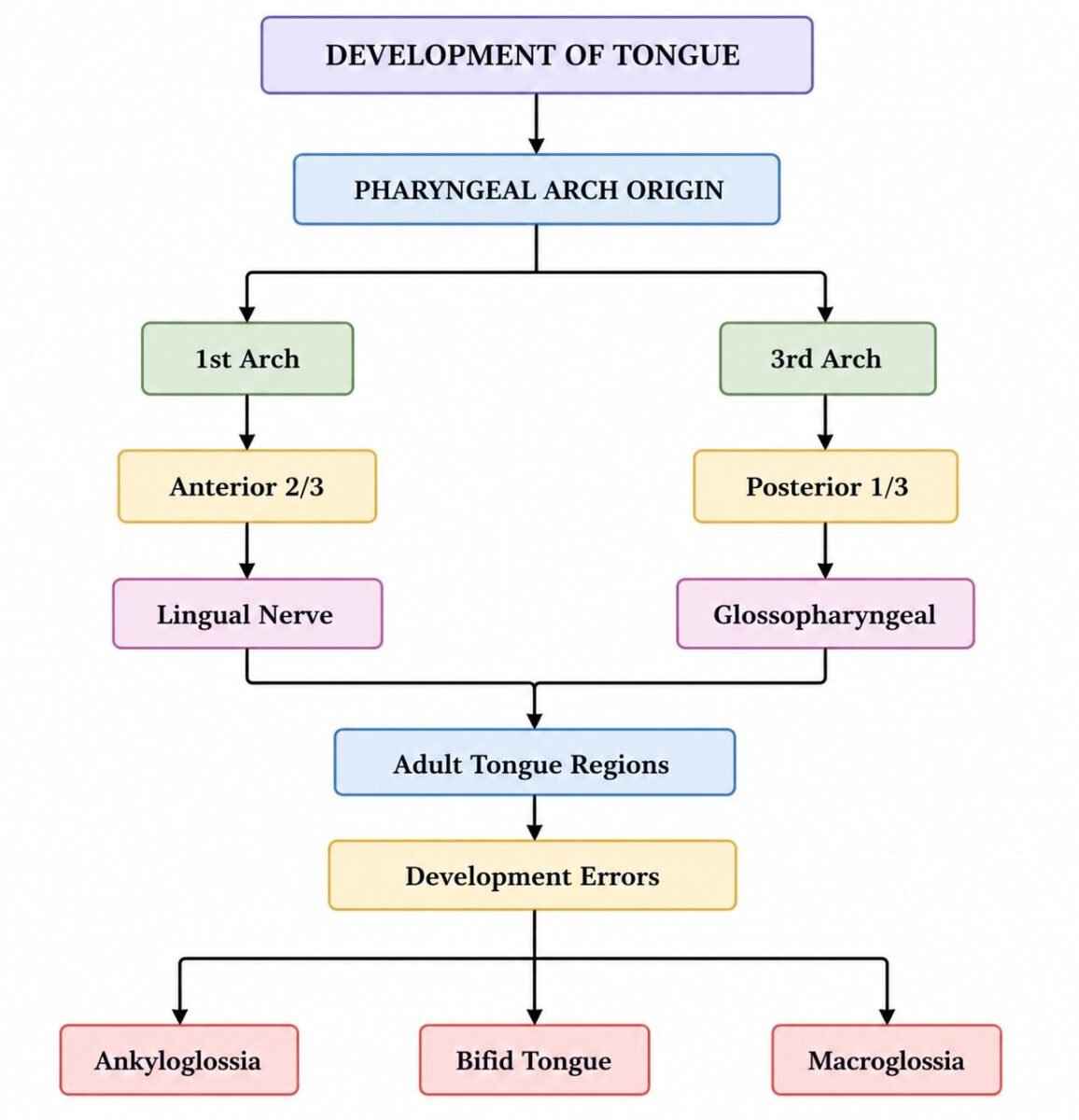
Anomalies of Tongue Development
- Ankyloglossia: short lingual frenulum causing restricted tongue movement.
- Macroglossia: enlarged tongue.
- Bifid tongue: failure of fusion.
- Microglossia: small tongue.
These anomalies may cause feeding difficulty, speech difficulty, and swallowing problems.
🔹 Histology
Microscopic Structure of Lips
- Skin layer
- Vermilion zone
- Oral mucosa
- Stratified squamous epithelium
- Skeletal muscle
- Sebaceous glands
The vermilion zone has rich blood supply, giving lips their red color. Thick epithelium protects the lips against mechanical stress.
Histological Structure of Tooth
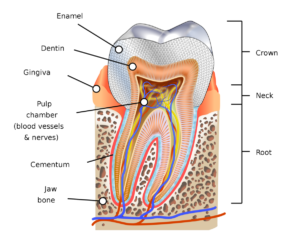
- Enamel: hard outer protective layer and hardest tissue in the body.
- Dentin: supportive layer containing tubules.
- Pulp: nutritive and sensory core containing vessels and nerves.
- Cementum: anchors tooth to periodontal ligament.
- Longitudinal section: helps identify crown, root, enamel, dentin, pulp cavity, cementum, and periodontal attachment.
- Transverse section: helps understand circular arrangement of enamel/dentin/pulp and relation of tooth layers.
- Clinical relevance: enamel loss exposes dentin and may lead to sensitivity or caries progression.
Loss of enamel exposes dentin and causes tooth sensitivity. Deep caries may involve pulp, producing pain and infection risk.
🧠 Concept Map Placeholder
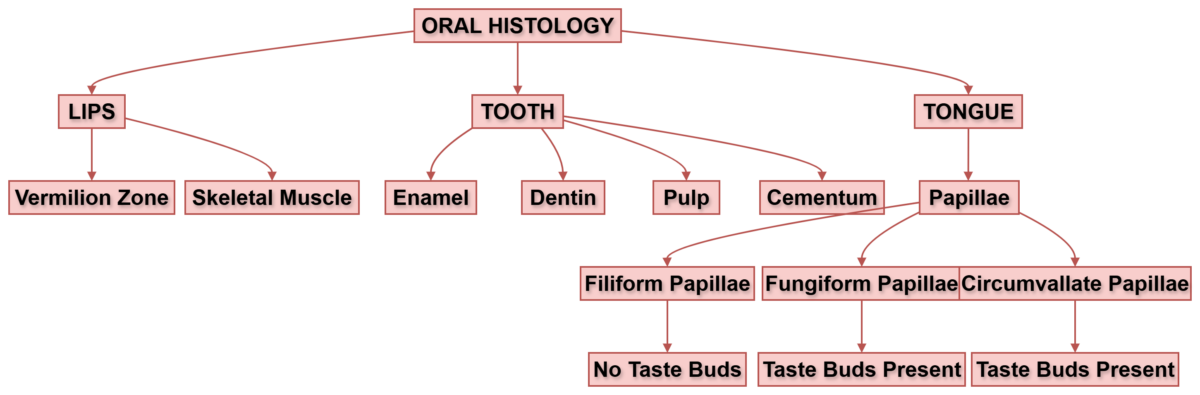
Histology of Tongue
- Filiform
- Fungiform
- Circumvallate
- Foliate
The tongue contains taste buds, stratified squamous epithelium, connective tissue, and skeletal muscle arranged in different planes.
Papillae increase surface area and help in taste sensation. Taste buds contain gustatory cells that detect taste stimuli. Filiform papillae are most numerous and mainly mechanical, while other papillae are more involved in taste.
Anterior 2/3 vs Posterior 1/3 of Tongue — Key Differences
| Feature | Anterior 2/3 | Posterior 1/3 |
|---|---|---|
| Embryological origin | 1st pharyngeal arch | 3rd pharyngeal arch |
| General sensation | Lingual nerve CN V3 | Glossopharyngeal nerve CN IX |
| Taste | Facial nerve CN VII via chorda tympani | Glossopharyngeal nerve CN IX |
| Clinical point | Lingual/chorda tympani injury affects anterior tongue sensation or taste | CN IX involvement may affect posterior taste and gag reflex |
🔹 ENT / Clinical Correlation
Causes of Oral Ulcerations
- Trauma
- Infection
- Vitamin deficiency
- Autoimmune disease
- Stress
Persistent oral ulceration should not be ignored because it may require evaluation for serious pathology, including malignancy.
Aphthous Ulcers and Treatment
Aphthous ulcers are small, painful ulcers of the oral mucosa.
Treatment options:
- Topical steroids
- Vitamin supplementation when deficiency is present
- Pain relief gels
- Maintenance of oral hygiene
4️⃣ Mechanism Flow
Taste Perception
- Food dissolves in saliva.
- Taste molecules bind to receptors on taste buds.
- Sensory impulse is generated.
- Signals travel through cranial nerves.
- Brain interprets taste.
Taste Pathway Summary
- Taste buds are stimulated by dissolved chemicals in saliva.
- Impulses are carried mainly through cranial nerves VII, IX, and X.
- Signals reach the nucleus tractus solitarius in the brainstem.
- Information is relayed to the thalamus.
- Signals project to the gustatory cortex for conscious taste perception.
5️⃣ Functional Integration
- Tongue muscles → movement → speech clarity.
- Papillae → taste detection → food selection.
- Teeth → mechanical breakdown → digestion efficiency.
- Nerve supply → sensation and motor control → coordinated swallowing.
- Embryological origin → nerve supply pattern → clinical examination findings.
6️⃣ Clinical Correlation
- Aphthous ulcers: painful but usually benign oral ulcers.
- Tongue paralysis: commonly linked with hypoglossal nerve injury.
- Ankyloglossia: restricted tongue movement due to short frenulum.
- Glossitis: inflammation of tongue, often associated with deficiency states or infection.
- Lingual nerve injury: loss of general sensation from anterior tongue.
- Chorda tympani injury: loss of taste from anterior two-thirds of tongue.
- Glossopharyngeal nerve injury: impaired posterior tongue sensation, taste, and gag reflex.
⭐ 7️⃣ Points to Remember
- Hypoglossal nerve supplies all tongue muscles except palatoglossus.
- Palatoglossus is supplied by vagus nerve.
- Anterior 2/3 taste is carried by facial nerve through chorda tympani.
- Posterior 1/3 sensation and taste are carried by glossopharyngeal nerve.
- Tongue develops from pharyngeal arches.
- Different embryological origins explain different nerve supply.
- Enamel is the hardest tissue in the body.
- Filiform papillae are the most numerous papillae.
- Ankyloglossia can cause speech difficulty.
- Aphthous ulcers are painful but usually benign.
- Tongue deviation suggests hypoglossal nerve injury.
- Persistent oral ulcer requires clinical evaluation.
Recommended Video