
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Cholesterol is an essential lipid molecule required for normal cell structure and function. It is present in all animal cells and is especially important in cell membranes, steroid hormone synthesis, bile acid formation, and vitamin D synthesis. Most cholesterol synthesis occurs in the liver, intestine, adrenal cortex, and reproductive organs. Although cholesterol is essential, excess cholesterol is clinically important because it contributes to atherosclerosis, gallstone formation, and cardiovascular disease. The liver plays the central role in cholesterol synthesis, degradation, conversion into bile acids, and excretion through bile. Bile acids are important for fat digestion because they help form micelles and allow absorption of dietary lipids and fat-soluble vitamins.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Cholesterol: A steroid lipid present in cell membranes and precursor of bile acids, steroid hormones, and vitamin D.
- HMG-CoA reductase: Rate-limiting enzyme of cholesterol synthesis.
- Statins: Drugs that inhibit HMG-CoA reductase and reduce cholesterol synthesis.
- Bile acids: Cholesterol-derived molecules synthesized in the liver.
- Bile salts: Conjugated bile acids present as sodium or potassium salts.
- Micelles: Small lipid-containing particles formed by bile salts to help fat absorption.
- Enterohepatic circulation: Recycling of bile salts from intestine back to liver.
- Bile acid sequestrants: Drugs that bind bile acids in intestine and increase their excretion.
- Dietary fiber: Plant-based material that can bind bile acids and reduce cholesterol reabsorption.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. Introduction & Sources of Cholesterol
Sites of Cholesterol Synthesis
🧠 CORE
- Cholesterol synthesis occurs in many tissues.
- The liver is the major site.
- Other sites include intestine, adrenal cortex, gonads, and skin.
- Synthesis occurs mainly in the cytosol and smooth endoplasmic reticulum.
- All nucleated cells can synthesize cholesterol to some extent.
- Red blood cells cannot synthesize cholesterol because they lack nucleus and organelles.
- Cholesterol synthesis is highest when dietary cholesterol intake is low.
- The liver controls blood cholesterol by synthesis, uptake, conversion, and excretion.
🔬 CONCEPT EXPLAINED
Cholesterol is required by almost all cells because it stabilizes cell membranes. The liver is the metabolic center because it not only synthesizes cholesterol but also converts it into bile acids and secretes it into bile.
Structure → Function:
Cholesterol has a rigid steroid ring structure. This allows it to fit between phospholipids in the cell membrane and regulate membrane fluidity.
⚠️ IF DAMAGED
Liver dysfunction → reduced cholesterol handling → abnormal lipid profile, impaired bile formation, fat malabsorption, and possible jaundice or cholestasis.
Source of Cholesterol
🧠 CORE
- Cholesterol comes from two main sources.
- Endogenous source: Synthesized inside the body.
- Exogenous source: Obtained from diet.
- Animal foods such as egg yolk, meat, dairy, and organ meat contain cholesterol.
- Plant foods do not contain cholesterol.
- Endogenous synthesis contributes the major portion.
- Dietary cholesterol can suppress liver cholesterol synthesis.
- Excess cholesterol may accumulate in blood and tissues.
🔬 CONCEPT EXPLAINED
The body does not depend only on diet for cholesterol. Even if dietary cholesterol is low, the liver can synthesize cholesterol from acetyl-CoA. This is important because cholesterol is needed for cell membranes, steroid hormones, bile acids, and vitamin D.
⚠️ IF DAMAGED
Excess intake + increased endogenous synthesis → hypercholesterolemia → LDL deposition in arteries → atherosclerosis → ischemic heart disease and stroke risk.
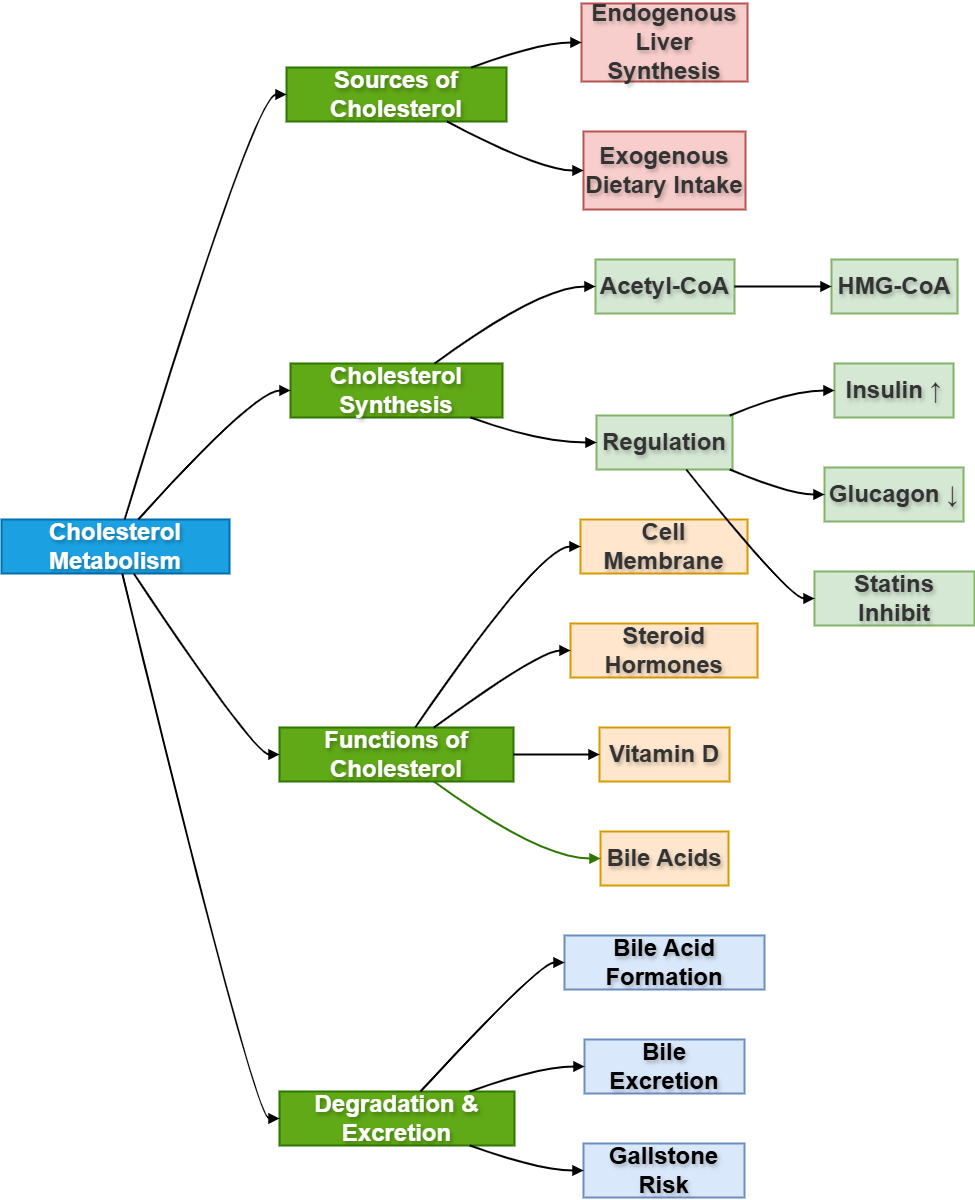
2. Cholesterol Biosynthesis
Steps of Cholesterol Synthesis
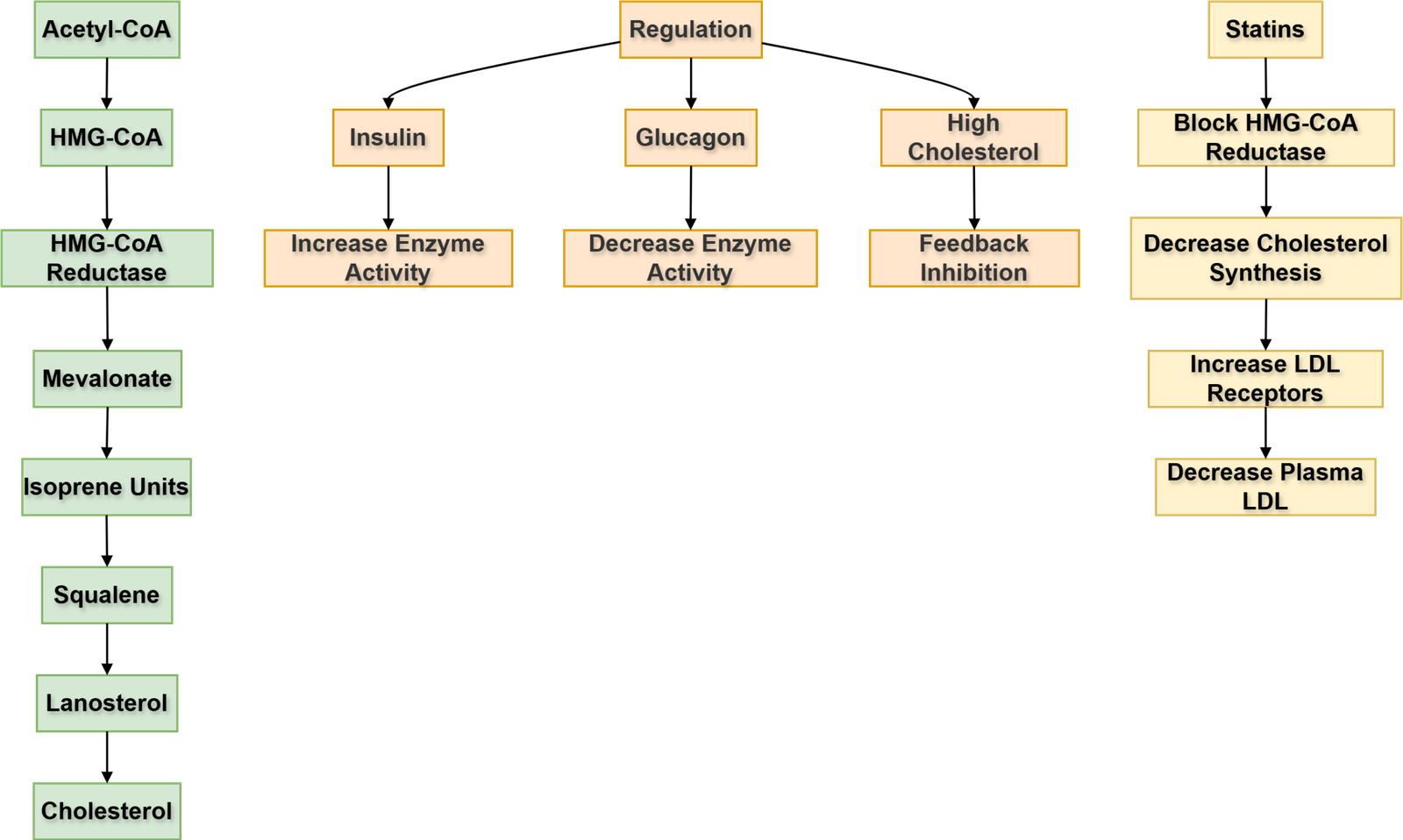
🧠 CORE
- Cholesterol synthesis begins from acetyl-CoA.
- It mainly occurs in cytosol and smooth ER.
- Acetyl-CoA forms HMG-CoA.
- HMG-CoA is converted into mevalonate.
- This step is catalyzed by HMG-CoA reductase.
- HMG-CoA reductase is the rate-limiting enzyme.
- Mevalonate forms activated isoprene units.
- Isoprene units form squalene.
- Squalene forms lanosterol.
- Lanosterol is converted into cholesterol.
🔬 CONCEPT EXPLAINED
Cholesterol synthesis is an anabolic pathway. It builds a large steroid molecule from small acetyl-CoA units. The most important control point is the conversion of HMG-CoA into mevalonate because this commits the cell to cholesterol synthesis.
⚠️ IF DAMAGED
Excess synthesis → raised plasma cholesterol.
Reduced synthesis → impaired steroid hormone, bile acid, vitamin D, and membrane cholesterol formation.
Regulation of Cholesterol Synthesis
🧠 CORE
- Main regulatory enzyme is HMG-CoA reductase.
- High intracellular cholesterol inhibits synthesis.
- Low cholesterol increases synthesis.
- Insulin increases HMG-CoA reductase activity.
- Glucagon decreases HMG-CoA reductase activity.
- Statins inhibit HMG-CoA reductase.
- Cholesterol also regulates LDL receptor expression.
- Liver cholesterol level controls bile acid synthesis.
🔬 CONCEPT EXPLAINED
The body regulates cholesterol synthesis according to need. When cholesterol is abundant, the liver reduces synthesis. When cholesterol is low, synthesis increases and LDL receptors may increase to take more cholesterol from blood.
⚠️ IF DAMAGED
Poor regulation → hypercholesterolemia → increased LDL → atherosclerotic plaque formation.
HMG-CoA Reductase Inhibitors
🧠 CORE
- HMG-CoA reductase inhibitors are called statins.
- They reduce endogenous cholesterol synthesis.
- They act mainly in the liver.
- They decrease hepatic cholesterol production.
- Liver increases LDL receptor expression.
- More LDL is removed from blood.
- Plasma LDL cholesterol decreases.
- Statins are important in prevention of cardiovascular disease.
🔬 CONCEPT EXPLAINED
Statins block the rate-limiting step of cholesterol synthesis. When liver cholesterol decreases, the liver compensates by increasing LDL receptors. These receptors remove LDL from blood, lowering plasma LDL cholesterol.
⚠️ IF DAMAGED
If LDL remains high despite regulation → cholesterol deposits in arterial walls → foam cells → fatty streaks → atherosclerosis.
3. Cholesterol Degradation & Bile Acid Formation
Degradation of Cholesterol
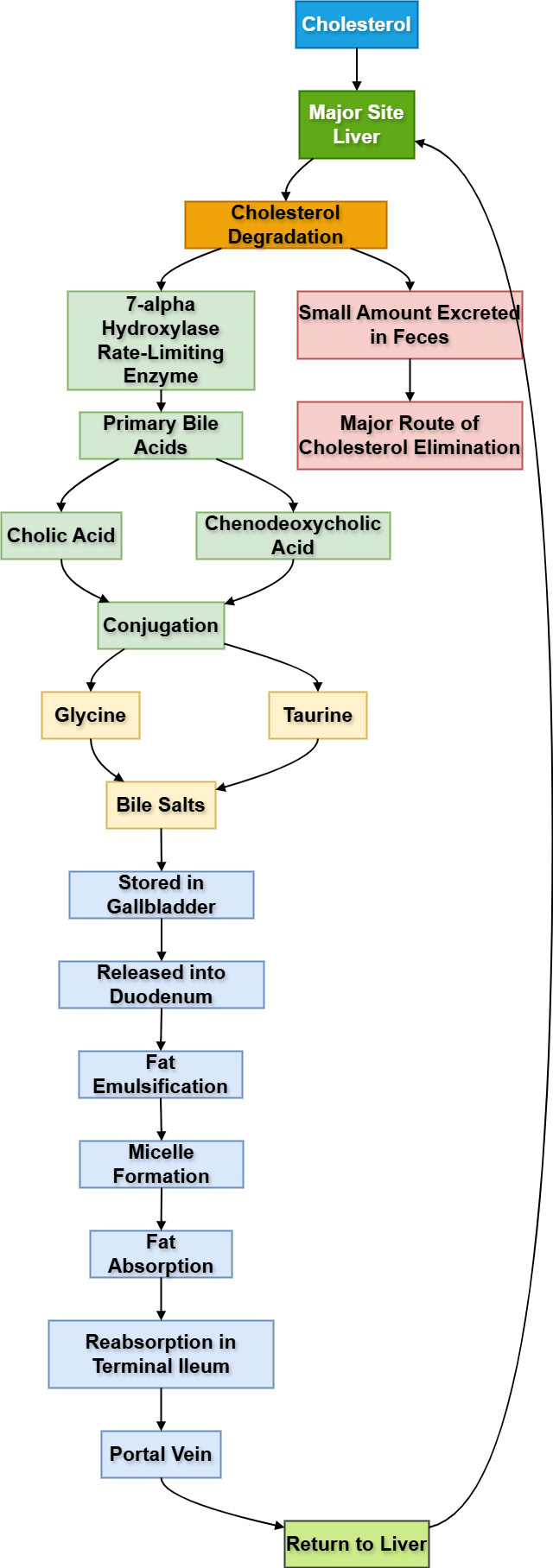
🧠 CORE
- Cholesterol ring cannot be completely degraded to CO₂ and water in humans.
- Major route of cholesterol disposal is conversion into bile acids.
- Some cholesterol is secreted directly into bile.
- Bile acids are excreted in feces.
- Liver is the major organ for cholesterol degradation.
- Bile acid synthesis maintains cholesterol balance.
- Excess cholesterol in bile may form gallstones.
- Cholesterol excretion depends on bile flow.
🔬 CONCEPT EXPLAINED
Unlike fatty acids, cholesterol cannot be broken down completely for energy. The body removes cholesterol mainly by converting it into bile acids and secreting it into bile. This is why bile acid metabolism is central to cholesterol homeostasis.
⚠️ IF DAMAGED
Reduced bile acid formation or bile flow → cholesterol accumulation → hypercholesterolemia, cholestasis, and gallstone risk.
Bile Acid Synthesis
🧠 CORE
- Bile acids are synthesized from cholesterol in the liver.
- Primary bile acids are cholic acid and chenodeoxycholic acid.
- The rate-limiting enzyme is cholesterol 7α-hydroxylase.
- Bile acids help in lipid digestion.
- They are secreted into bile.
- They are stored in the gallbladder.
- They are released into duodenum after meals.
- They emulsify fats and help micelle formation.
🔬 CONCEPT EXPLAINED
Bile acid synthesis converts a poorly water-soluble cholesterol molecule into amphipathic molecules. Amphipathic means they have both water-soluble and fat-soluble parts. This property allows bile acids to interact with both fat and intestinal fluid.
⚠️ IF DAMAGED
Reduced bile acid synthesis → poor fat digestion → steatorrhea, fat-soluble vitamin deficiency, and impaired cholesterol excretion.
Conjugation of Bile Acids
🧠 CORE
- Bile acids are conjugated in the liver.
- They combine with glycine or taurine.
- Conjugation increases water solubility.
- Conjugated bile acids are stronger detergents.
- They remain ionized in intestinal pH.
- This prevents passive reabsorption in upper intestine.
- Conjugation improves fat emulsification.
- Conjugated bile acids form bile salts.
🔬 CONCEPT EXPLAINED
Conjugation makes bile acids more effective in the intestine. By attaching glycine or taurine, bile acids become more polar and can remain active in the watery intestinal environment while still interacting with lipids.
⚠️ IF DAMAGED
Poor conjugation → reduced bile salt formation → impaired micelle formation → fat malabsorption.
Bile Salt Formation
🧠 CORE
- Bile salts are sodium or potassium salts of conjugated bile acids.
- They are present in bile.
- They are amphipathic molecules.
- They emulsify dietary fat.
- They help pancreatic lipase action.
- They form micelles.
- They help absorption of fatty acids, monoglycerides, cholesterol, and fat-soluble vitamins.
- They are mostly reabsorbed in terminal ileum.
🔬 CONCEPT EXPLAINED
Bile salts act like biological detergents. One side interacts with fat and the other side interacts with water. This allows large fat globules to break into smaller droplets, increasing surface area for pancreatic lipase.
⚠️ IF DAMAGED
Bile salt deficiency → large fat droplets remain undigested → decreased lipase action → steatorrhea and vitamin A, D, E, K deficiency.
4. Functions of Bile Salts in Digestion
Micelle Formation
🧠 CORE
- Micelles are small particles formed by bile salts and lipid digestion products.
- They contain fatty acids, monoglycerides, cholesterol, and fat-soluble vitamins.
- Bile salts surround lipid molecules.
- Micelles transport lipids to intestinal epithelial cells.
- They are essential for fat absorption.
- Micelles do not enter the enterocyte as a whole.
- Lipid contents diffuse into intestinal cells.
- Bile salts remain in intestinal lumen for recycling.
🔬 CONCEPT EXPLAINED
After pancreatic lipase digests triglycerides, the products are still poorly soluble in water. Bile salts form micelles around these lipid products and carry them through the watery intestinal contents toward the brush border of enterocytes.
⚠️ IF DAMAGED
Failure of micelle formation → fat malabsorption → bulky, greasy stools, weight loss, and fat-soluble vitamin deficiency.
Enterohepatic Circulation
🧠 CORE
- Enterohepatic circulation is recycling of bile salts.
- Bile salts are secreted by liver into bile.
- They enter the duodenum after meals.
- They help fat digestion and absorption.
- Most are reabsorbed in terminal ileum.
- They return to liver through portal blood.
- Liver re-secretes them into bile.
- This cycle conserves bile salts.
🔬 CONCEPT EXPLAINED
The body does not synthesize large amounts of bile salts every day. Instead, it efficiently recycles them. The terminal ileum is the major site where bile salts are actively reabsorbed and returned to the liver.
⚠️ IF DAMAGED
Ileal disease or resection → bile salt loss → reduced bile salt pool → fat malabsorption and diarrhea. Increased bile acids reaching colon can cause bile acid diarrhea.
5. Pharmacological & Dietary Regulation
Role of Bile Acid Sequestrants
🧠 CORE
- Bile acid sequestrants bind bile acids in intestine.
- They prevent bile acid reabsorption.
- More bile acids are lost in feces.
- Liver uses more cholesterol to synthesize new bile acids.
- Hepatic cholesterol decreases.
- LDL receptor expression increases.
- Plasma LDL decreases.
- Examples include cholestyramine and colestipol.
🔬 CONCEPT EXPLAINED
These drugs interrupt enterohepatic circulation. When bile acids are lost, the liver must convert more cholesterol into bile acids. This lowers liver cholesterol and increases LDL uptake from blood.
⚠️ IF DAMAGED
If bile acid loss is excessive → fat malabsorption may occur. These drugs may also interfere with absorption of fat-soluble vitamins and some medicines.
Dietary Fiber Effects
🧠 CORE
- Dietary fiber can bind bile acids in intestine.
- It increases fecal bile acid excretion.
- Liver uses cholesterol to replace lost bile acids.
- This may reduce plasma cholesterol.
- Soluble fiber is especially useful.
- Fiber also slows glucose absorption.
- It supports gut motility.
- It may reduce cardiovascular risk when combined with healthy diet.
🔬 CONCEPT EXPLAINED
Fiber acts partly like a natural bile acid binder. By increasing bile acid loss in stool, it encourages the liver to use cholesterol for new bile acid production. This helps reduce cholesterol burden.
⚠️ IF DAMAGED
Low fiber diet → reduced bile acid binding → increased cholesterol reabsorption tendency → higher risk of dyslipidemia and constipation.
Regulation of Bile Acid Synthesis
🧠 CORE
- Bile acid synthesis is controlled mainly in liver.
- Rate-limiting enzyme is cholesterol 7α-hydroxylase.
- Bile acids inhibit their own synthesis.
- Increased bile acid return suppresses synthesis.
- Reduced bile acid return increases synthesis.
- Cholesterol availability also affects synthesis.
- Bile acid synthesis is linked to cholesterol homeostasis.
- It is a major route of cholesterol elimination.
🔬 CONCEPT EXPLAINED
Bile acid synthesis is regulated by feedback inhibition. When enough bile acids return to liver through portal blood, the liver reduces new synthesis. When bile acids are lost in feces, synthesis increases and uses more cholesterol.
⚠️ IF DAMAGED
Defective regulation → abnormal bile acid pool → impaired fat digestion, cholesterol imbalance, and increased risk of gallstones or dyslipidemia.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
- Cholesterol steroid ring → stabilizes cell membranes → maintains membrane fluidity.
- Liver synthetic enzymes → produce cholesterol → support membrane, hormone, bile acid, and vitamin D formation.
- HMG-CoA reductase → controls cholesterol synthesis → major target of statins.
- Bile acids from cholesterol → convert insoluble cholesterol into useful digestive molecules → help lipid digestion.
- Conjugated bile acids → become more water-soluble → form effective bile salts.
- Bile salts amphipathic structure → emulsifies fat → increases surface area for pancreatic lipase.
- Micelles → transport lipid digestion products → allow intestinal fat absorption.
- Terminal ileum reabsorption → conserves bile salts → maintains bile salt pool.
- Bile acid excretion → removes cholesterol from body → helps cholesterol balance.
🩺 5️⃣ Clinical Correlation
1. Hypercholesterolemia
- Increased LDL cholesterol raises risk of atherosclerosis.
- Excess LDL enters arterial wall.
- Macrophages take up oxidized LDL and become foam cells.
- Fatty streaks progress to atherosclerotic plaques.
- Clinical outcomes include ischemic heart disease and stroke.
2. Statin Therapy
- Statins inhibit HMG-CoA reductase.
- Liver cholesterol synthesis decreases.
- LDL receptor expression increases.
- More LDL is cleared from blood.
- Plasma LDL level falls.
3. Gallstones
- Excess cholesterol in bile may precipitate.
- Cholesterol stones can form in gallbladder.
- Risk increases when bile has too much cholesterol or reduced bile salts.
- May cause biliary colic, cholecystitis, or obstructive jaundice.
4. Ileal Disease or Resection
- Terminal ileum normally reabsorbs bile salts.
- Ileal disease reduces bile salt reabsorption.
- Bile salt pool decreases.
- Fat digestion becomes impaired.
- Patient may develop steatorrhea and fat-soluble vitamin deficiency.
5. Bile Acid Sequestrants
- These drugs bind bile acids in intestine.
- Bile acids are lost in feces.
- Liver uses cholesterol to make new bile acids.
- LDL cholesterol decreases.
- They are useful in selected cases of hypercholesterolemia.
6. Fat-Soluble Vitamin Deficiency
- Bile salts are required for absorption of vitamins A, D, E, and K.
- Bile salt deficiency can cause:
- Vitamin A deficiency → night blindness
- Vitamin D deficiency → bone problems
- Vitamin E deficiency → neurological issues
- Vitamin K deficiency → bleeding tendency
📌 6️⃣ Summary Points
- Liver is the major site of cholesterol synthesis and cholesterol disposal.
- Cholesterol synthesis occurs mainly in cytosol and smooth ER.
- HMG-CoA reductase is the rate-limiting enzyme of cholesterol synthesis.
- Statins inhibit HMG-CoA reductase and reduce LDL cholesterol.
- Humans cannot completely degrade cholesterol to CO₂ and water.
- Main route of cholesterol elimination is conversion into bile acids.
- Primary bile acids are cholic acid and chenodeoxycholic acid.
- Bile acids are conjugated with glycine or taurine to form bile salts.
- Bile salts are essential for emulsification, micelle formation, and fat absorption.
- Terminal ileum is the main site of bile salt reabsorption.
- Enterohepatic circulation conserves the bile salt pool.
- Bile acid sequestrants and dietary fiber increase bile acid loss and help lower cholesterol.