
📖 Step 2 — Learning Material
This section provides structured learning content for the topic. Follow each part in sequence to build clear conceptual understanding and maintain logical learning progression.
🔹 1️⃣ Introduction
Gastrointestinal motility and swallowing are essential physiological processes that ensure the proper movement of food from ingestion to digestion and absorption. These processes depend on coordinated electrical activity of smooth muscle, neural control through the enteric and autonomic nervous systems, and hormonal influences. The enteric nervous system functions as an independent regulatory network capable of controlling gastrointestinal movement and secretion. Swallowing is a precisely timed reflex involving voluntary and involuntary phases that protect the airway while directing food into the esophagus. Disturbances in motility or neural regulation can lead to clinical disorders such as dysphagia, achalasia, intestinal obstruction, and autonomic dysfunction affecting digestion.
🔹 2️⃣ Foundation Concepts
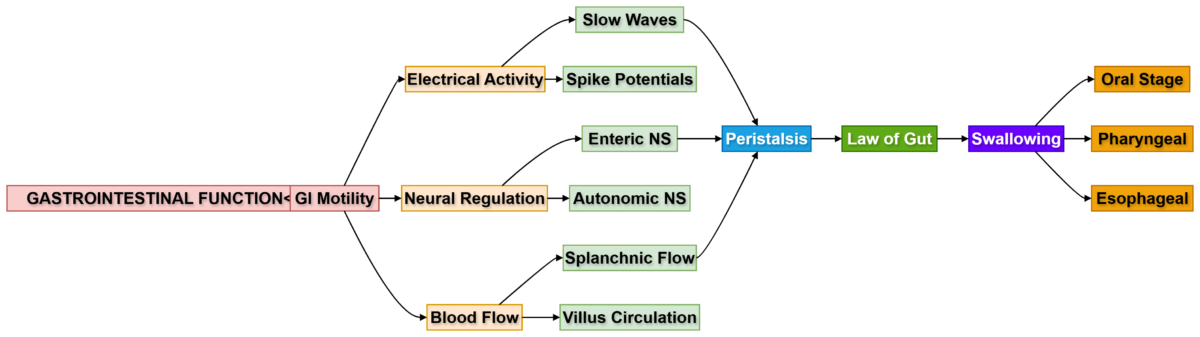
Gastrointestinal motility depends on coordinated contraction of smooth muscle layers that move food through the digestive tract. This movement is initiated by rhythmic electrical activity called slow waves, which set the basic rhythm of contractions but do not produce contraction alone. When slow waves reach threshold, spike potentials occur, allowing calcium entry into smooth muscle and producing contraction.
Control of gastrointestinal movement is mainly carried out by the enteric nervous system, which consists of the myenteric plexus controlling motility and the submucosal plexus regulating secretion and local blood flow. The autonomic nervous system further modifies gut activity, where parasympathetic stimulation increases motility and sympathetic stimulation reduces it.
Swallowing is a coordinated neuromuscular process that moves food from the mouth to the stomach through voluntary and involuntary phases while temporarily stopping respiration to protect the airway.
🔹 3️⃣ Core Learning — Curriculum Coverage
1. Electrical Activity of Gastrointestinal Smooth Muscle
Gastrointestinal (GI) smooth muscle shows spontaneous rhythmic electrical activity, which is essential for motility.
Types of Electrical Activity
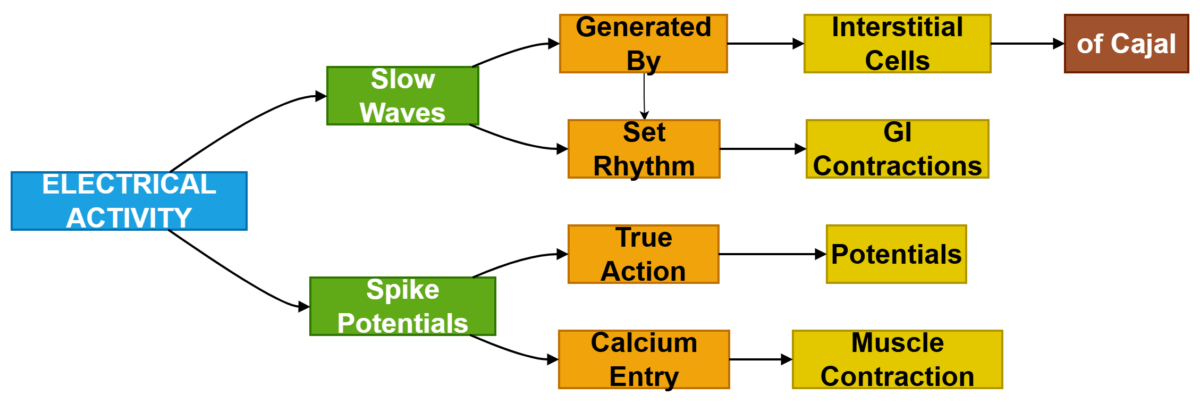
A. Slow Waves (Basic Electrical Rhythm — BER)
Definition:
Slow waves are rhythmic oscillations in membrane potential that determine the basic rhythm of GI motility.
Key Features
- Not true action potentials
- Generated by Interstitial Cells of Cajal (pacemaker cells)
- Determine frequency of contractions
- Do not cause contraction alone
Frequency of Slow Waves
Organ Frequency
Stomach 3/min
Duodenum 12/min
Ileum 8–9/min
Clinical Correlation
Damage to pacemaker cells results in: - Gastroparesis
- Motility disorders
- Functional dyspepsia
B. Spike Potentials
Spike potentials are true action potentials that occur when slow waves reach threshold.
Features
- Responsible for muscle contraction
- Associated with calcium entry
- Increased by stretch and parasympathetic activity
Clinical Correlation
Excess spike activity → - Diarrhea
- Intestinal spasm
Reduced spike activity → - Ileus
- Constipation
2. Mechanism of Excitation of Smooth Muscle
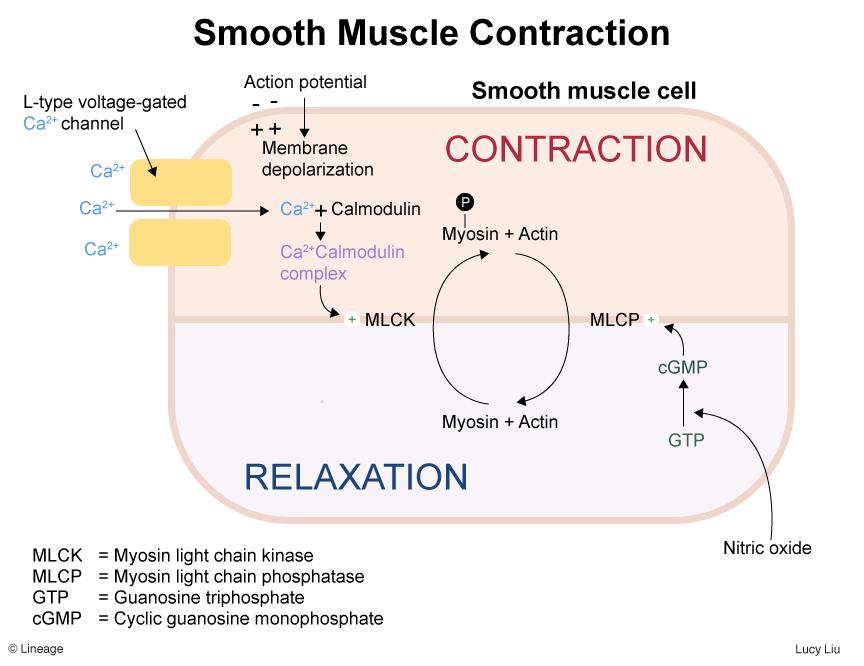
Smooth muscle contraction depends mainly on calcium ion entry.
Mechanism
- Membrane depolarization
- Calcium channels open
- Calcium enters cell
- Calcium binds calmodulin
- Activates myosin light chain kinase (MLCK)
- Contraction occurs
Clinical Correlation
Calcium channel blockers may reduce:
- GI motility
- Smooth muscle tone
3. Enteric Nervous System (ENS)
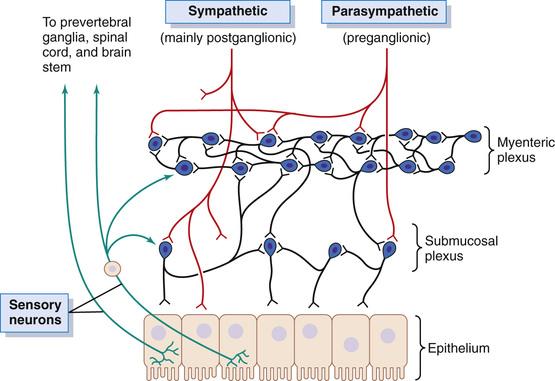
The ENS is known as the “brain of the gut.”
It operates independently but is modified by the autonomic nervous system.
Two Major Plexuses
A. Myenteric Plexus (Auerbach’s Plexus)
Location:
Between longitudinal and circular muscle layers.
Functions
- Controls motility
- Regulates tone
- Coordinates peristalsis
- Controls rate of contraction
Clinical Correlation
Damage leads to: - Achalasia
- Hirschsprung disease
B. Submucosal Plexus (Meissner’s Plexus)
Location:
Within submucosa.
Functions
- Controls secretion
- Regulates absorption
- Local blood flow control
4. Enteric Neurotransmitters
Important neurotransmitters regulate contraction and relaxation.
Excitatory Neurotransmitters
- Acetylcholine
- Substance P
Cause: - Muscle contraction
- Increased secretion
Inhibitory Neurotransmitters - Nitric oxide (NO)
- Vasoactive intestinal peptide (VIP)
Cause: - Muscle relaxation
- Reduced motility
Clinical Correlation
Loss of inhibitory neurons → - Achalasia
5. Autonomic Nervous System Regulation
Autonomic Nervous System Regulation
The ENS is influenced by sympathetic and parasympathetic systems.
Parasympathetic System
Origin
- Vagus nerve
- Pelvic nerves
Effects - Increases motility
- Increases secretion
- Relaxes sphincters
Sympathetic System
Origin
- Thoracolumbar spinal cord
Effects - Decreases motility
- Decreases secretion
- Contracts sphincters
6. Gastrointestinal Reflexes
GI reflexes regulate coordinated digestion.
Types of Reflexes
Short Reflexes
- Within enteric system
- Local control
Example: - Peristaltic reflex
Long Reflexes
- Involve CNS
Examples: - Gastrocolic reflex
- Enterogastric reflex
7. Gastrointestinal Hormones
Gastrointestinal hormones are chemical messengers released from specialized endocrine cells in the mucosa of the gastrointestinal tract. These hormones regulate digestive processes by controlling secretion, motility, absorption, and blood flow. They act locally through the bloodstream or nearby tissues to coordinate digestion according to the type and amount of food entering the gut.
Most gastrointestinal hormones are released in response to food in the lumen, particularly proteins, fats, and acids. Their effects ensure proper digestion, efficient absorption of nutrients, and regulation of gastrointestinal movement.
Major Gastrointestinal Hormones
The four principal gastrointestinal hormones include:
- Gastrin
- Cholecystokinin (CCK)
- Secretin
- Gastric Inhibitory Peptide (GIP)
These hormones are considered primary regulators of digestive activity.
1️⃣ Gastrin
Source
Gastrin is secreted by:
G cells located in the pyloric region of the stomach and upper duodenum.
Stimuli for Secretion
Gastrin secretion increases in response to:
- Presence of proteins in stomach
- Gastric distension
- Vagal stimulation
- Peptides and amino acids
Functions
Gastrin produces several important effects:
- Increases gastric acid secretion
- Stimulates growth of gastric mucosa
- Increases gastric motility
These actions help prepare the stomach for digestion of proteins.
Clinical Correlation
Excess gastrin secretion occurs in:
Zollinger–Ellison syndrome
This leads to:
- Excess gastric acid
- Peptic ulcer formation
- Severe gastric irritation
2️⃣ Cholecystokinin (CCK)
Source
CCK is secreted by:
I cells located in the duodenum and jejunum.
Stimuli for Secretion
CCK secretion occurs when:
- Fatty acids enter duodenum
- Partially digested proteins are present
Functions
CCK has multiple important digestive functions:
- Stimulates pancreatic enzyme secretion
- Causes gallbladder contraction
- Relaxes sphincter of Oddi
- Slows gastric emptying
These actions help digestion of fats and proteins.
Clinical Correlation
Failure of gallbladder contraction due to impaired CCK response may lead to:
- Gallstone formation
- Poor fat digestion
3️⃣ Secretin
Source
Secretin is released from:
S cells located in the duodenum.
Stimuli for Secretion
Secretin is released when:
- Acidic chyme enters duodenum
- Low duodenal pH occurs
Functions
Secretin produces:
- Increased bicarbonate secretion from pancreas
- Increased bile secretion from liver
- Decreased gastric acid secretion
These actions neutralize acid entering the small intestine.
Clinical Correlation
Deficiency of bicarbonate secretion can result in:
- Duodenal ulcer formation
- Mucosal injury due to acid exposure
4️⃣ Gastric Inhibitory Peptide (GIP)
(Also called Glucose-Dependent Insulinotropic Peptide)
Source
GIP is secreted by:
K cells located in the duodenum and jejunum.
Stimuli for Secretion
GIP secretion increases in response to:
- Glucose
- Fatty acids
- Amino acids
Functions
Major actions include:
- Stimulates insulin secretion
- Reduces gastric motility
- Slows gastric emptying
This hormone plays an important role in glucose metabolism.
Clinical Correlation
GIP contributes to:
Incretin effect
Which enhances insulin secretion after oral glucose intake.
This principle is used in:
Diabetes mellitus treatment (incretin-based therapy)
Minor Gastrointestinal Hormones (Important Overview)
In addition to major hormones, several minor hormones regulate digestive processes.
These include:
- Motilin — stimulates migrating motor complex
- Somatostatin — inhibits secretion and motility
- Histamine — stimulates gastric acid secretion
These hormones provide fine control of gastrointestinal activity.
8. Functional Types of Gastrointestinal Movements
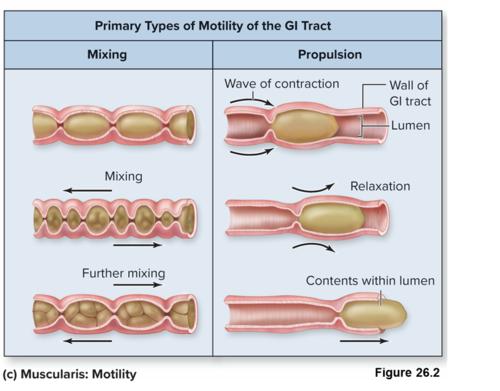
A. Propulsive Movements (Peristalsis)
Move contents forward.
Mechanism
- Contraction behind bolus
- Relaxation ahead of bolus
This mechanism follows:
Law of the Gut
Definition:
“Contraction above and relaxation below the bolus ensures forward movement.”
Clinical Correlation
Failure causes: - Intestinal obstruction symptoms
- Severe constipation
B. Mixing Movements
Help digestion and absorption.
Examples:
- Segmentation contractions
- Pendular movements
9. Gastrointestinal Blood Flow
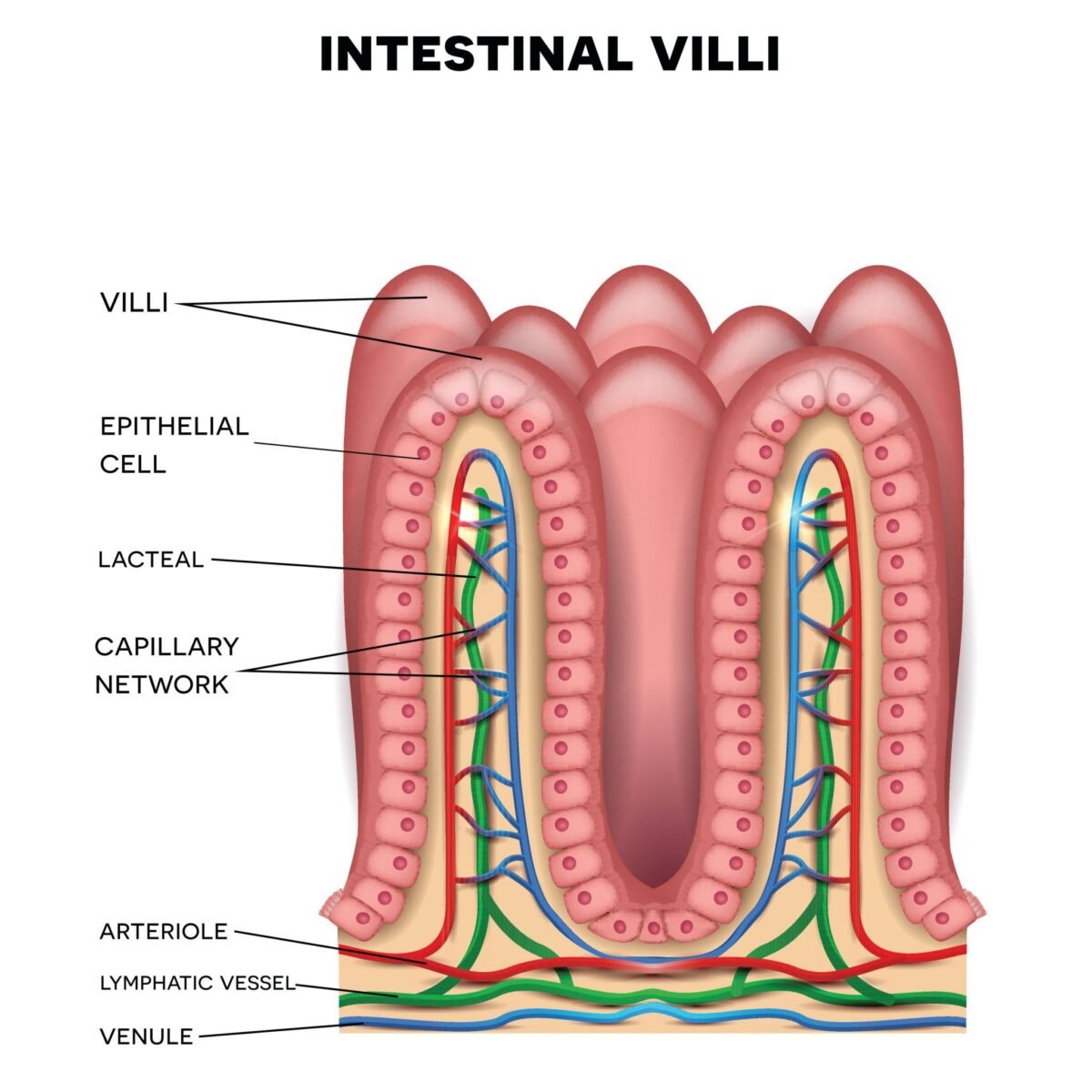
Blood Flow Through Villus
Villus contains:
- Arteriole
- Capillary network
- Venule
Special Feature
Countercurrent exchange occurs between arteriole and venule.
Clinical Correlation
Reduced blood flow → - Ischemic bowel
Splanchnic Circulation
Includes blood supply to:
- Stomach
- Intestines
- Liver
- Pancreas
- Spleen
Major Arteries - Celiac trunk
- Superior mesenteric artery
- Inferior mesenteric artery
Effect of Metabolic Activity on Blood Flow
Increased digestion →
- Increased metabolic activity
- Vasodilation
- Increased blood supply
Nervous Control of GI Blood Flow
Parasympathetic:
- Increases blood flow
Sympathetic: - Causes vasoconstriction
10. Swallowing Physiology
Swallowing is a coordinated reflex involving voluntary and involuntary phases.
Mechanics of Ingestion
Includes:
- Chewing
- Mastication
- Formation of bolus
Chewing and Mastication
Functions
- Break food into small particles
- Increase surface area
- Mix with saliva
Control - Controlled by reflex and voluntary action
Stages of Swallowing
There are three stages:
- Oral Stage (Voluntary)
Food is pushed to pharynx.
Muscles:
- Tongue
- Buccal muscles
- Pharyngeal Stage (Involuntary)
Important protective stage.
Events:
- Soft palate closes nasal cavity
- Epiglottis closes airway
- Vocal cords close
- Respiration temporarily stops
Clinical Correlation
Failure leads to: - Aspiration pneumonia
- Esophageal Stage (Involuntary)
Bolus moves to stomach by peristalsis.
Effect of Pharyngeal Stage on Respiration
During swallowing:
- Respiration stops briefly
- Known as deglutition apnea
Prevents: - Aspiration
11. Stimulation of Alimentary Gland Secretion
Secretion depends on:
- Neural stimulation
- Hormonal stimulation
- Mechanical stimulation
Dual Effect of Sympathetic Stimulation
Sympathetic stimulation:
Short-term:
- Slight secretion
Long-term: - Reduced secretion due to vasoconstriction
12. Anatomy of Gastrointestinal Blood Supply (Integration)
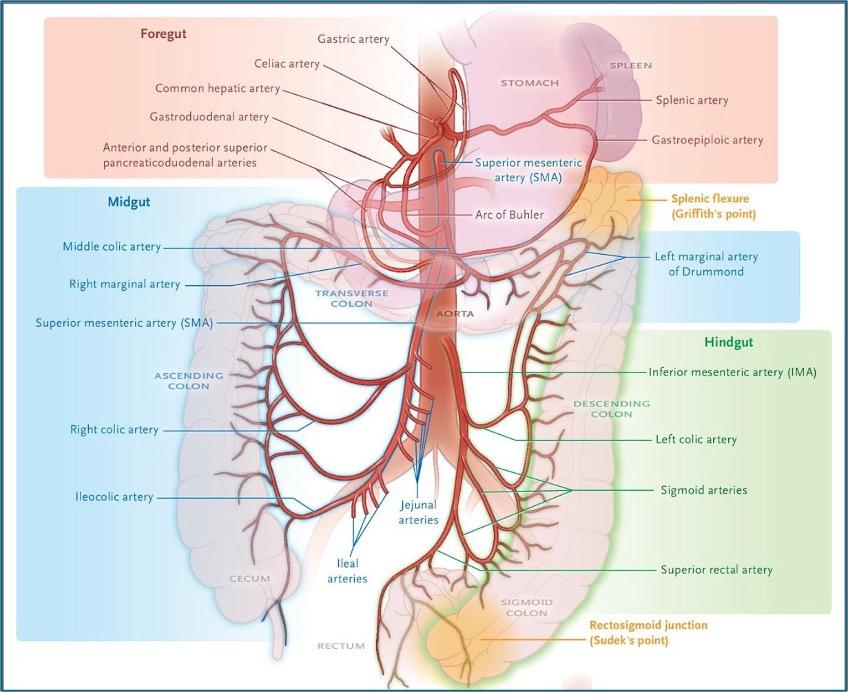
Foregut Blood Supply
Supplied by:
Celiac Trunk
Major Branches
- Left gastric artery
- Common hepatic artery
- Splenic artery
Foregut Organs - Lower esophagus
- Stomach
- Proximal duodenum
- Liver
- Pancreas
- Spleen
Midgut Blood Supply
Supplied by:
Superior Mesenteric Artery (SMA)
Midgut Organs
- Distal duodenum
- Jejunum
- Ileum
- Cecum
- Ascending colon
- Proximal two-thirds of transverse colon
Hindgut Blood Supply
Supplied by:
Inferior Mesenteric Artery (IMA)
Hindgut Organs
- Distal one-third of transverse colon
- Descending colon
- Sigmoid colon
- Rectum (upper part)
Clinical Correlation — Mesenteric Ischemia
Occurs due to:
- Reduced blood supply
- Arterial blockage
Common symptoms: - Severe abdominal pain
- Postprandial pain
- Weight loss
Integrated Clinical Correlations
Important clinical connections include:
- Achalasia → Loss of inhibitory neurons
- Hirschsprung disease → Absence of enteric ganglia
- Ileus → Reduced motility
- Dysphagia → Swallowing dysfunction
- Aspiration pneumonia → Failure of airway protection
- Mesenteric ischemia → Reduced splanchnic circulation
🧩 Master Concept Map
⚙️ Mechanism Flow
Food enters gastrointestinal tract
↓
Chemical components (protein, fat, acid) stimulate endocrine cells
↓
Gastrointestinal hormones released into bloodstream
↓
Target organs activated (stomach, pancreas, liver, intestine)
↓
Secretion and motility adjusted according to food type
↓
Efficient digestion and nutrient absorption occur
🔗 Functional Integration
Gastrointestinal hormones coordinate digestion by linking different organs of the digestive system.
- Gastrin increases gastric acid secretion to digest proteins.
- Secretin stimulates bicarbonate secretion to neutralize acidic chyme.
- Cholecystokinin (CCK) promotes pancreatic enzyme release and gallbladder contraction for fat digestion.
- GIP enhances insulin secretion and slows gastric emptying.
Together, these hormones ensure that digestion, neutralization, and absorption occur in a controlled sequence.
🩺 Clinical Correlation
Zollinger–Ellison Syndrome
Cause:
Excess secretion of gastrin due to gastrin-producing tumor.
Effect:
- Excess gastric acid secretion
- Recurrent peptic ulcers
- Severe mucosal irritation
Gallstone Formation
Cause:
Reduced gallbladder contraction due to impaired CCK response.
Effect:
- Poor bile release
- Difficulty in fat digestion
- Formation of gallstones
Duodenal Ulcer
Cause:
Failure of adequate bicarbonate secretion due to reduced secretin activity.
Effect:
- Acid injury to duodenal mucosa
- Ulcer formation
Effect: Paste effect here.
Clinical Importance: Paste clinical relevance here.
📌 Summary Points
- Gastrointestinal hormones regulate secretion, motility, and digestion.
- Gastrin increases gastric acid secretion and motility.
- CCK stimulates pancreatic enzymes and gallbladder contraction.
- Secretin promotes bicarbonate secretion to neutralize acid.
- GIP stimulates insulin secretion and reduces gastric motility.
- Hormones are released in response to food entering the gut.
- Proper hormonal coordination ensures efficient digestion and absorption.