
📖 Learning Material
1️⃣ Introduction
The esophagus is a muscular tube that transports food from the pharynx to the stomach, forming an essential part of the gastrointestinal tract. It lies in the neck, thorax, and abdomen, passing through the posterior mediastinum before entering the stomach. Proper functioning of the esophagus ensures safe swallowing and prevents reflux of gastric contents. Understanding its structure, development, and histology helps explain swallowing disorders, congenital defects, and cancers. Clinically, the esophagus is important because it is involved in conditions such as dysphagia, gastroesophageal reflux disease (GERD), and esophageal carcinoma, which are frequently tested in exams and encountered in clinical practice.
2️⃣ Foundation Basics
🔑 Key Definitions
• Esophagus: A muscular tube connecting the pharynx to the stomach.
• Deglutition: The process of swallowing.
• Upper Esophageal Sphincter (UES): Muscular opening at the junction of pharynx and esophagus.
• Lower Esophageal Sphincter (LES): Functional sphincter preventing gastric reflux.
• Peristalsis: Wave-like muscular contraction moving food downward.
Essential Terminology
• Posterior mediastinum: Space in thoracic cavity where most of esophagus lies.
• Constrictions of esophagus: Narrow areas clinically important.
• Stratified squamous epithelium: Protective epithelial lining of esophagus.
• Adventitia: Outer connective tissue covering most of esophagus.
• Carcinoma: Malignant tumor arising from epithelial tissue.
Basic Overview
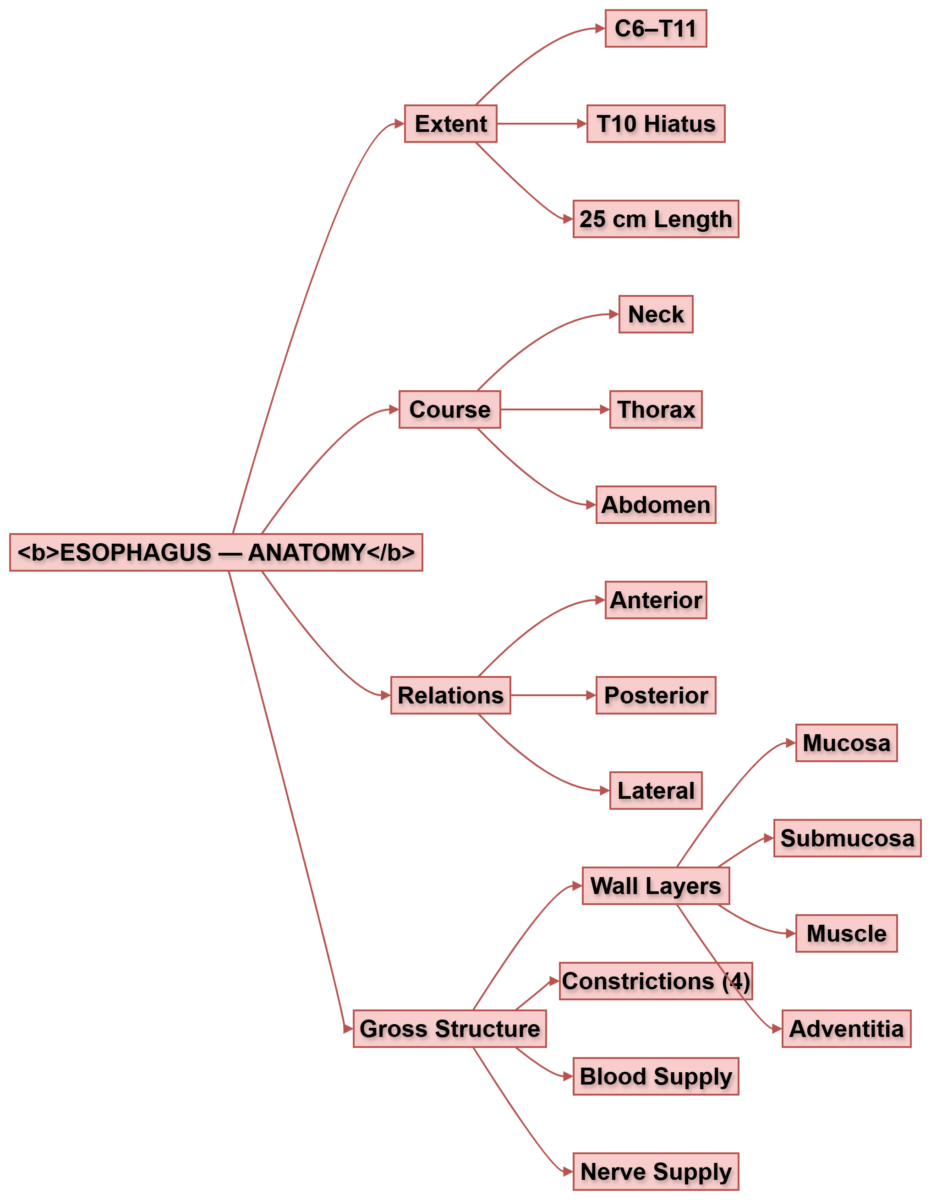
• Length: ~25 cm
• Extends from C6 vertebra to T11 vertebra
• Divided into:
o Cervical part
o Thoracic part
o Abdominal part
• Functions mainly in transport of food
• Lined by protective mucosa
• Supported by coordinated muscular contractions
3️⃣ Core Learning
🔹 Anatomy
 CORE
CORE• Begins at lower border of cricoid cartilage (C6)
• Ends at cardiac orifice of stomach (T11)
• Length: ~25 cm
• Lies posterior to trachea
• Passes through esophageal hiatus at T10
• Divided into:
o Cervical part (5 cm)
o Thoracic part (18 cm)
o Abdominal part (2 cm)
• Connects pharynx to stomach
• Crosses diaphragm before entering stomach
 CONCEPT EXPLAINED
CONCEPT EXPLAINED
Structure:
The esophagus begins at the level of C6 vertebra, where the pharynx ends. It descends vertically through the thorax and passes through the diaphragm at T10, ending at T11.
Mechanism:
This pathway allows swallowed food to travel from mouth to stomach efficiently.
Structure → Function:
Its vertical alignment ensures gravity assists swallowing.
🔬 CONCEPT EXPLAINED
Intrinsic muscles change the shape of the tongue, allowing precise articulation and food manipulation. Extrinsic muscles move the tongue in different directions, helping in swallowing, speech, and maintaining airway patency.
 IF DAMAGED
IF DAMAGED• Injury → disruption of swallowing
• Result → dysphagia
• Severe trauma → leakage of contents → mediastinitis
Course of Esophagus
CORE
• Begins at C6
• Passes behind trachea
• Enters thorax through superior thoracic aperture
• Lies in posterior mediastinum
• Deviates slightly to left near lower thorax
• Passes through diaphragm at T10
• Ends at T11
• Crossed anteriorly by left bronchus
• Lies anterior to vertebral column
CONCEPT EXPLAINED
Structure:
The esophagus descends behind the trachea and heart before entering the stomach.
Mechanism:
Its position allows smooth transition of food through thorax.
Structure → Function:
Posterior location protects it from compression during breathing.
IF DAMAGED
Compression → swallowing difficulty
Example:
• Enlarged left atrium → compresses esophagus
• Result → dysphagia
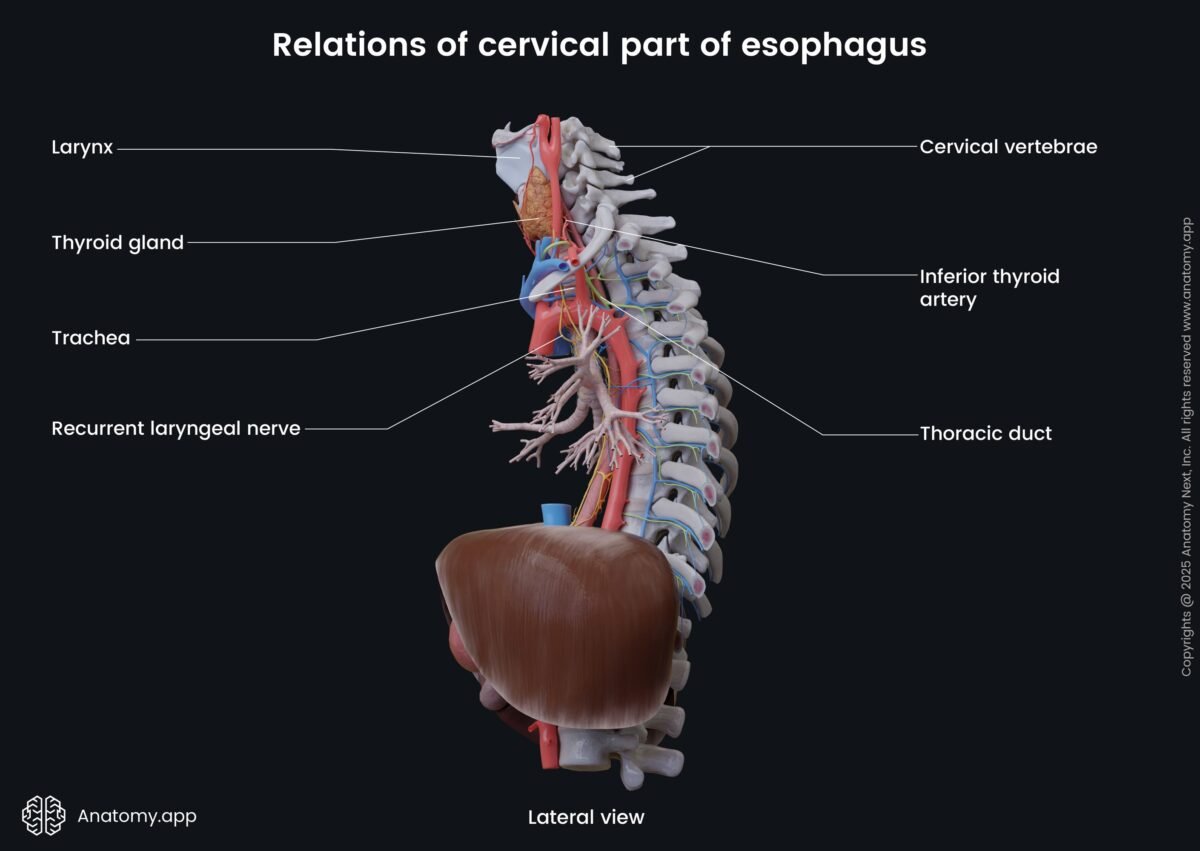
Relations of Esophagus
CORE
Cervical Part Relations
Anterior:
• Trachea
Posterior:
• Vertebral column
Lateral:
• Thyroid gland
• Carotid sheath
Thoracic Part Relations
Anterior:
• Trachea
• Left bronchus
• Left atrium
Posterior:
• Vertebral column
• Thoracic duct
Lateral:
• Lungs and pleura
Abdominal Part Relations
Anterior:
• Left lobe of liver
Posterior:
• Left crus of diaphragm
CONCEPT EXPLAINED
Structure:
Relations change as esophagus moves from neck to abdomen.
Mechanism:
These relations influence symptoms in diseases affecting nearby organs.
Structure → Function:
Close relation to heart explains cardiac effects on swallowing.
IF DAMAGED
• Tumor growth → compress adjacent structures
• Example:
Esophageal tumor → tracheal compression → breathing difficulty
Gross Structure of Esophagus
CORE
• Muscular tube
• Four layers:
- Mucosa
- Submucosa
- Muscularis externa
- Adventitia
• Contains four constrictions
• Upper and lower sphincters present
• Lumen normally collapsed
• Rich nerve supply from vagus nerve
• Blood supply from multiple arteries - CONCEPT EXPLAINED
Structure:
The esophagus wall consists of muscular layers allowing contraction.
Mechanism:
Muscle contraction produces peristalsis, pushing food downward.
Structure → Function:
Circular and longitudinal muscle layers enable directional movement. IF DAMAGED
Muscle damage → ineffective peristalsis
Result → food stagnation → dysphagia
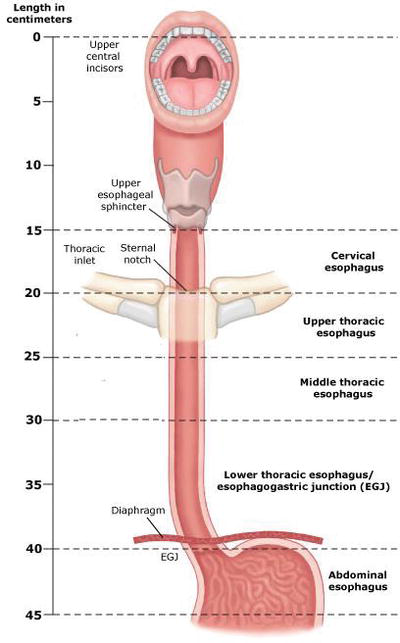
🔴 Esophageal Constrictions
🧠 CORE
The esophagus has four normal constrictions:
1️⃣ Cricopharyngeal Constriction
• Level: C6
• Cause: Cricopharyngeus muscle
• Distance from incisors: ~15 cm
2️⃣ Aortic Constriction
• Level: T4
• Cause: Arch of aorta
• Distance from incisors: ~25 cm
3️⃣ Bronchial Constriction
• Level: T5
• Cause: Left main bronchus
• Distance from incisors: ~27 cm
4️⃣ Diaphragmatic Constriction
• Level: T10
• Cause: Esophageal hiatus of diaphragm
• Distance from incisors: ~40 cm
🔬 CONCEPT EXPLAINED
Structure:
Constrictions occur where surrounding structures compress the esophagus.
Mechanism:
These narrow points regulate passage of food and are common sites of obstruction.
Structure → Function:
Natural narrowing ensures coordinated passage into stomach.
⚠️ IF DAMAGED / CLINICAL IMPORTANCE
- Most common sites for foreign body lodgement
• Important landmarks during endoscopy
• Common sites of esophageal carcinoma
• Risk of injury during nasogastric tube insertion
Blood Supply of Esophagus
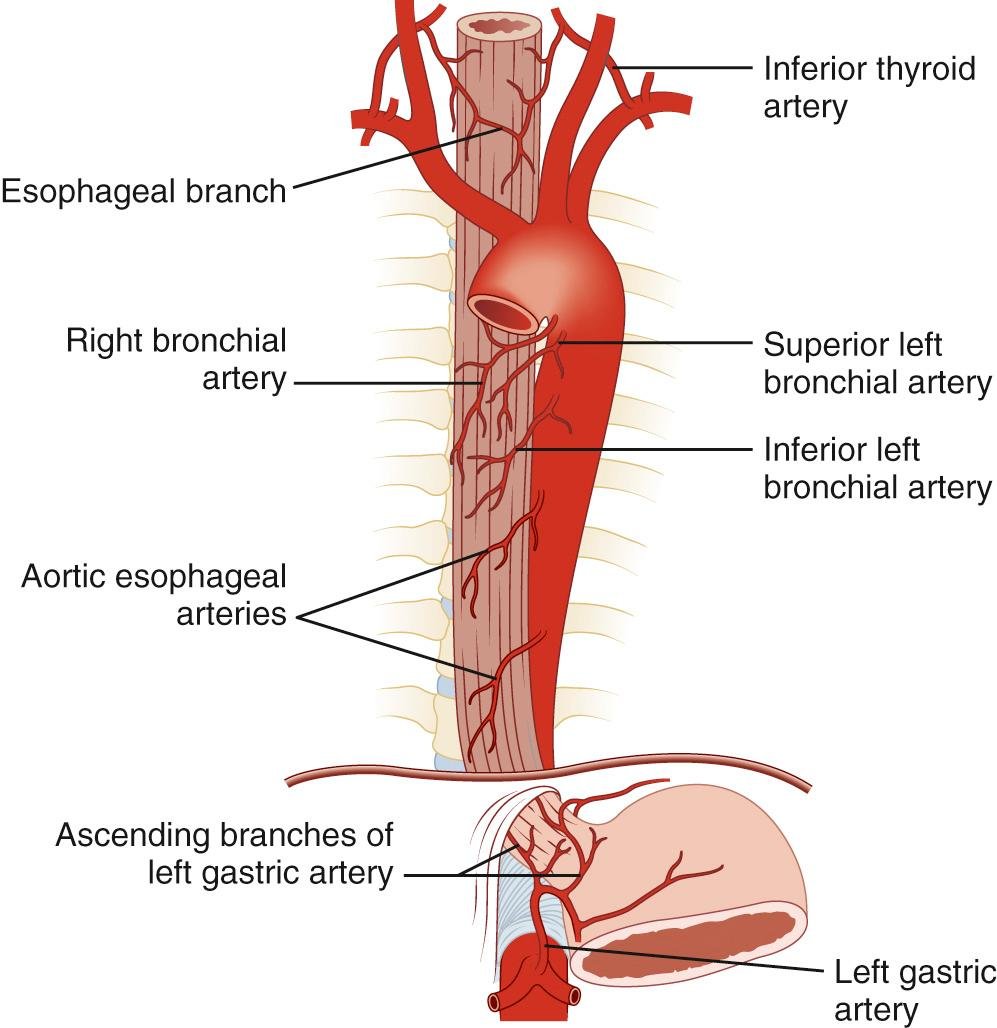
Arterial:
• Inferior thyroid artery
• Thoracic aorta
• Left gastric artery
Venous:
• Portal-systemic anastomosis
• Varices concept
Nerve Supply
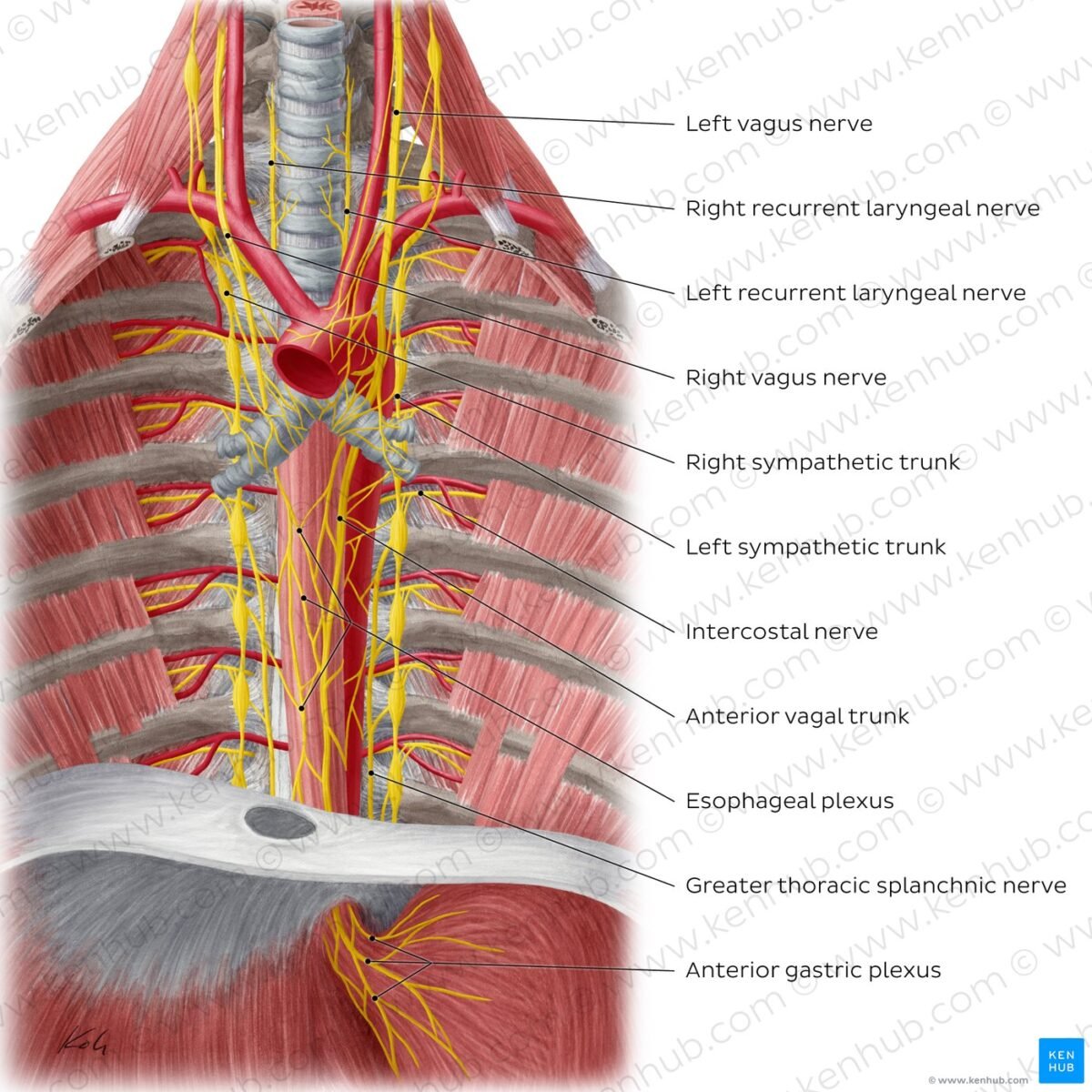
Include:
• Vagus nerve
• Sympathetic trunk
• Esophageal plexus
EMBRYOLOGY
Development of Esophagus
CORE
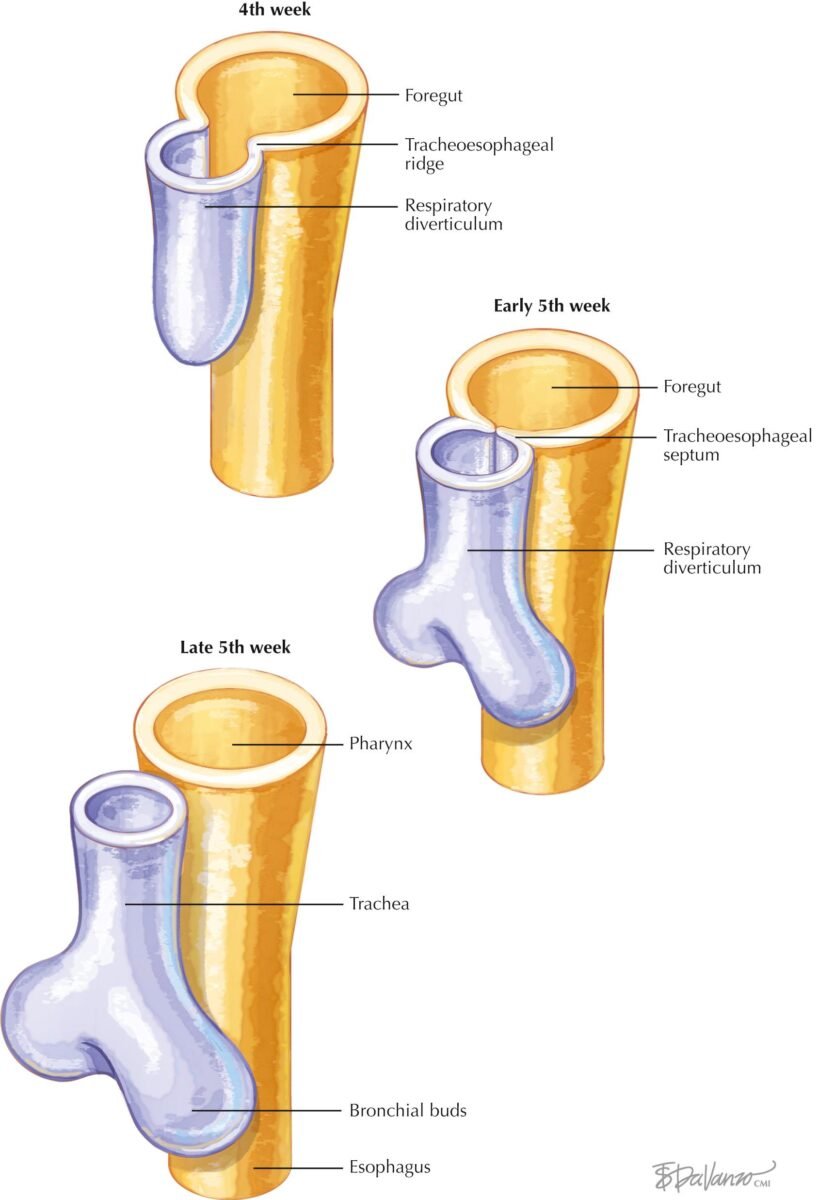
• Develops from foregut
• Begins in 4th week
• Tracheoesophageal septum divides foregut
• Upper part forms esophagus
• Lining initially stratified columnar
• Later becomes stratified squamous
• Muscles differentiate from mesenchyme
• Length increases as heart descends
CONCEPT EXPLAINED
Structure:
Foregut divides into respiratory and digestive tubes.
Mechanism:
Septum formation separates trachea and esophagus.
Structure → Function:
Separation prevents aspiration of food into lungs.
IF DAMAGED
Failure of separation →
→ Tracheoesophageal fistula
Effects:
• Choking during feeding
• Milk enters lungs
• Respiratory distress
HISTOLOGY
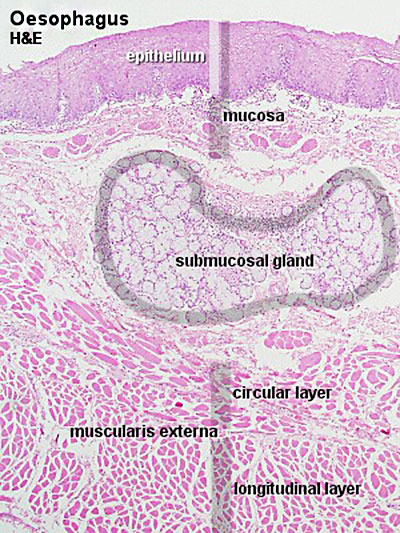
Epithelium of Esophagus CORE
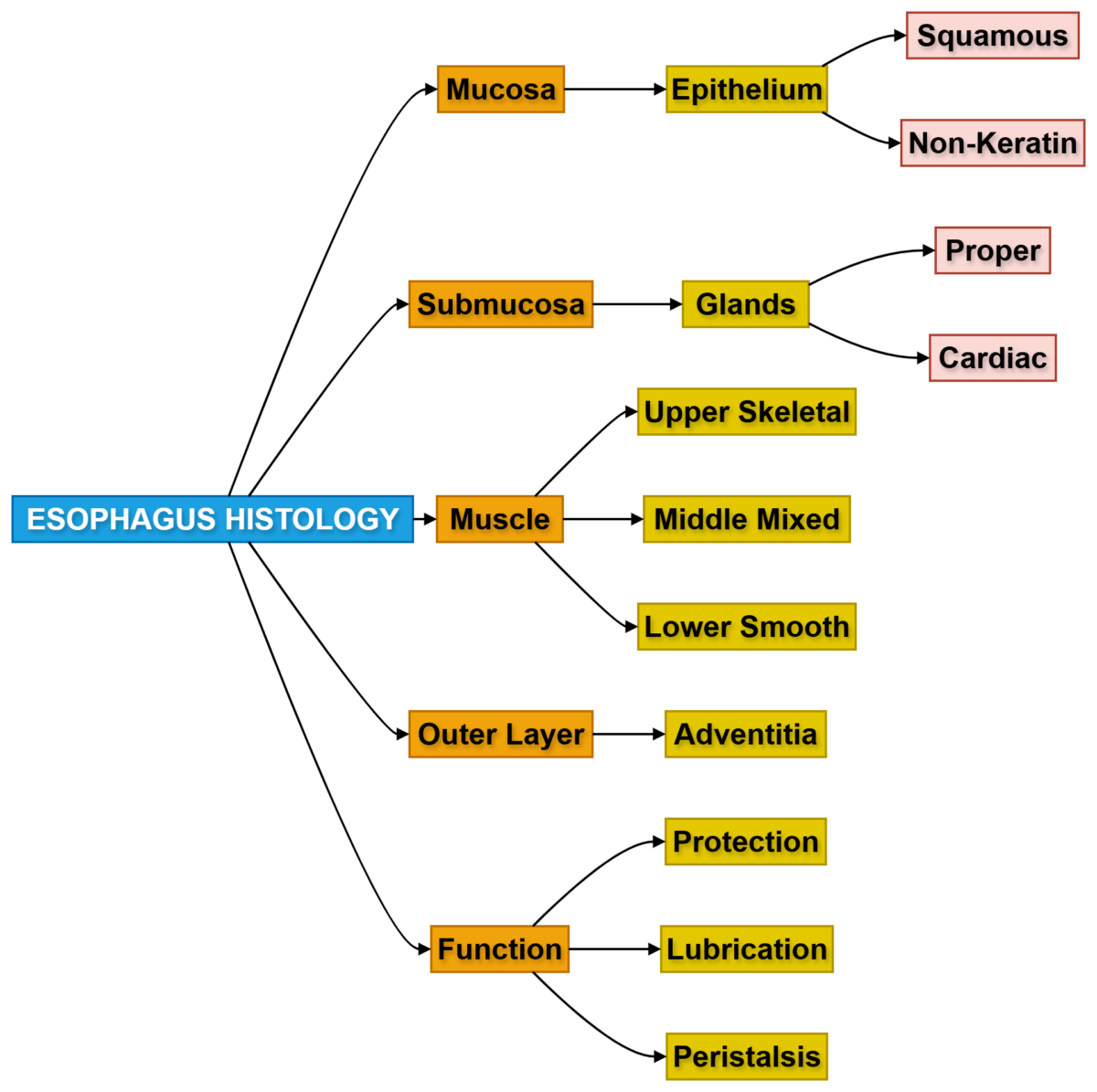
• Stratified squamous epithelium
• Non-keratinized
• Protective function
• Resists mechanical injury
• Thick mucosal lining
• Contains basal cells
• Rapid cell turnover
• Protects against friction
CONCEPT EXPLAINED
Structure:
Multiple layers of cells provide mechanical strength.
Mechanism:
Food bolus causes friction → epithelium resists damage.
Structure → Function:
Stratification prevents ulcer formation.
IF DAMAGED
Chronic irritation →
→ Metaplasia (Barrett esophagus)
Risk:
→ Esophageal carcinoma
Esophageal Glands
Types of Esophageal Glands
• Proper glands
• Cardiac glands
CORE
• Located in submucosa
• Mucus-secreting glands
• Lubricate lumen
• Facilitate swallowing
• Protect mucosa
• Numerous along length
• Produce alkaline mucus
Structure:
Glands open into esophageal lumen.
Mechanism:
Mucus reduces friction.
Structure → Function:
Smooth passage of food. IF DAMAGED
Reduced mucus →
→ Painful swallowing
Musculature Differences in Esophagus
CORE
Upper third:
• Skeletal muscle
Middle third:
• Mixed muscle
Lower third:
• Smooth muscle
Function:
• Produces peristalsis
Controlled by:
• Vagus nerve
CONCEPT EXPLAINED
Structure:
Gradual transition from voluntary to involuntary muscle.
Mechanism:
Allows voluntary swallowing initially and involuntary continuation.
Structure → Function:
Ensures coordinated movement.
IF DAMAGED
Nerve injury →
→ Loss of peristalsis
→ Dysphagia
PATHOLOGY
Histological Types of Esophageal Carcinoma
CORE
Two main types:
- Squamous cell carcinoma
- Adenocarcinoma
Locations:
• Squamous: upper and middle
• Adenocarcinoma: lower esophagus
Risk factors:
• Smoking
• Alcohol
• GERD
• Barrett esophagus CONCEPT EXPLAINED
Structure:
Carcinoma arises from epithelial lining.
Mechanism:
Chronic irritation causes mutation.
Structure → Function:
Tumor narrows lumen. IF DAMAGED
Tumor growth →
→ Obstruction → Dysphagia
Presentation of Esophageal Carcinoma
CORE
• Progressive dysphagia
• Weight loss
• Painful swallowing
• Regurgitation
• Hoarseness
• Chronic cough
• Hematemesis (late)
• Anemia
CONCEPT EXPLAINED
Structure:
Tumor compresses lumen.
Mechanism:
Food passage becomes difficult.
Structure → Function:
Swallowing failure leads to malnutrition.
IF DAMAGED
Late detection →
→ Poor prognosis
🧠 Concept Map
MAP 1 — Anatomy Overview Map
🧠 MAP 2 — Histology Map
4️⃣ Mechanism Flow
- Food enters pharynx
- Upper esophageal sphincter relaxes
- Food enters esophagus
- Circular muscles contract
- Longitudinal muscles shorten tube
- Peristaltic wave pushes food downward
- Lower sphincter relaxes
- Food enters stomach
Taste Pathway Summary
- Taste buds are stimulated by dissolved chemicals in saliva.
- Impulses are carried mainly through cranial nerves VII, IX, and X.
- Signals reach the nucleus tractus solitarius in the brainstem.
- Information is relayed to the thalamus.
- Signals project to the gustatory cortex for conscious taste perception.
5️⃣ Functional Integration
Structure → Function → Outcome
• Stratified epithelium → Protection → Safe food passage
• Muscular layers → Peristalsis → Food transport
• Submucosal glands → Lubrication → Smooth swallowing
• Sphincters → Direction control → Prevent reflux
6️⃣ Clinical Correlation
- Common exam-relevant conditions:
Dysphagia
Cause:
• Tumor
• Nerve damage
• Stricture
Effect:
• Difficulty swallowingGastroesophageal Reflux Disease (GERD)
Cause:
• Weak lower esophageal sphincter
Effect:
• Acid reflux
• HeartburnTracheoesophageal Fistula
Cause:
• Developmental defect
Effect:
• Food enters airwayEsophageal Carcinoma
Key signs:
• Progressive dysphagia
• Weight loss
⭐ 7️⃣ Points to Remember
- Esophagus extends from C6 to T11
- Passes through diaphragm at T10
- Length approximately 25 cm
- Lined by stratified squamous epithelium
- Upper third contains skeletal muscle
- Lower third contains smooth muscle
- Develops from foregut
- Failure of septum formation → tracheoesophageal fistula
- Two major carcinoma types exist
- Progressive dysphagia is key warning symptom
- Submucosal glands produce lubricating mucus
- Lower esophageal sphincter prevents reflux
Recommended Video