
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Glycolysis, pyruvate metabolism, and gluconeogenesis are central metabolic pathways involved in cellular energy production and glucose homeostasis. These pathways are especially important in tissues with high energy demand such as the brain, skeletal muscle, liver, and red blood cells. Glycolysis occurs in the cytoplasm and provides rapid ATP production by breaking down glucose into pyruvate. Pyruvate metabolism links glycolysis with aerobic energy production through the pyruvate dehydrogenase (PDH) complex. Gluconeogenesis mainly occurs in the liver and helps maintain blood glucose levels during fasting and starvation. These pathways are clinically important because defects may lead to hypoglycemia, lactic acidosis, hemolytic anemia, and metabolic disorders. Understanding these pathways also explains important concepts in diabetes mellitus, exercise physiology, starvation, and cancer metabolism.
🔹 2️⃣ Foundation Concepts
🔹 3️⃣ Core Learning — Curriculum Coverage
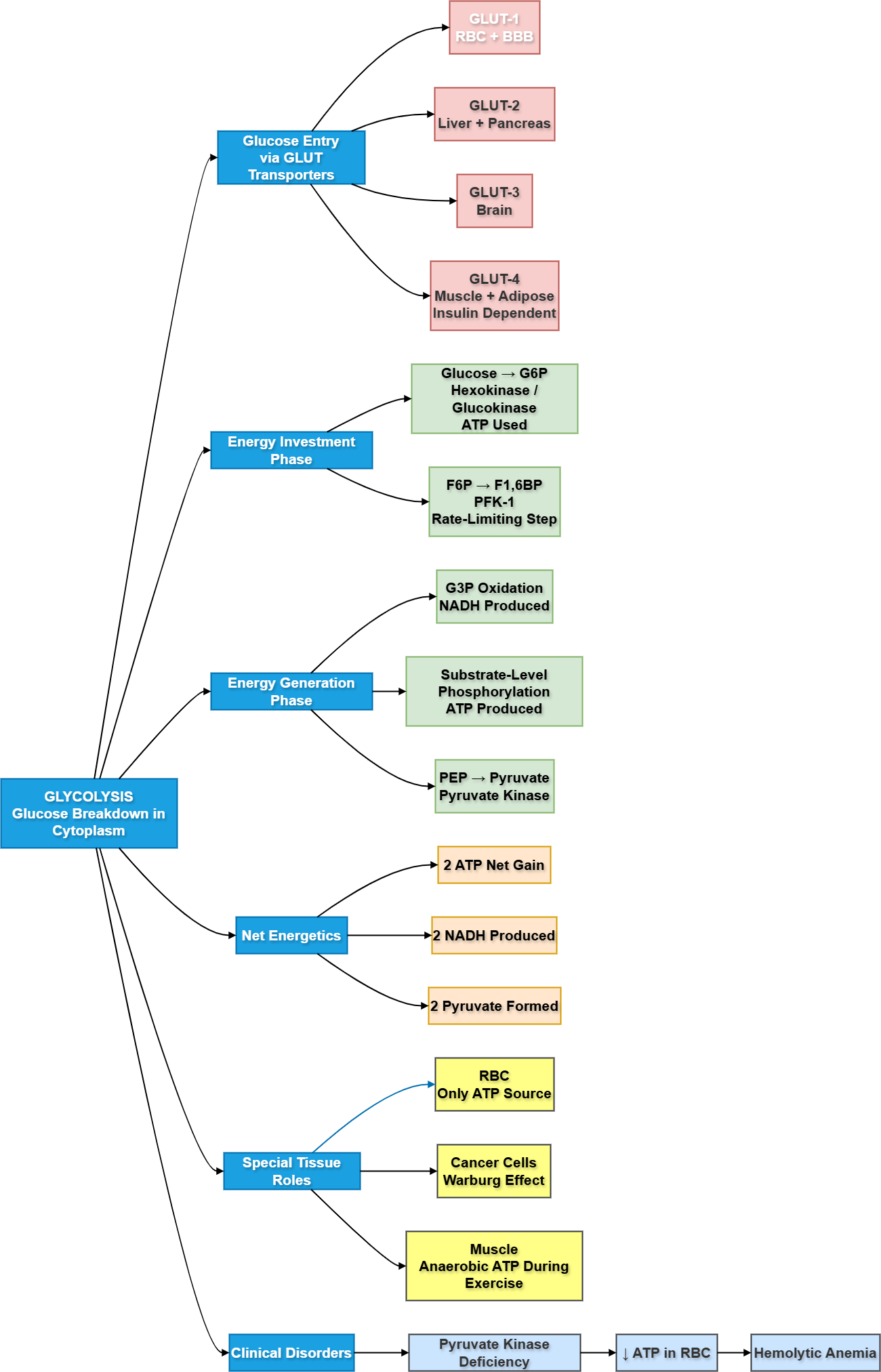
1️⃣ Glycolysis
Definition of Glycolysis
🧠 CORE
- Glycolysis means “splitting of glucose.”
- One glucose molecule is converted into two pyruvate molecules.
- It occurs in cytoplasm.
- It does not directly require oxygen.
- It produces ATP and NADH.
- It is the first step of glucose metabolism.
- It supplies pyruvate for TCA cycle.
- It supplies lactate during anaerobic conditions.
🔬 CONCEPT EXPLAINED
Glycolysis is a universal energy pathway. Glucose, a 6-carbon molecule, is gradually converted into two 3-carbon molecules of pyruvate. During this process, energy is trapped as ATP and NADH.
⚠️ IF DAMAGED
Defective glycolysis → reduced ATP production → cell dysfunction.
In RBCs, this causes membrane instability → hemolysis → anemia.
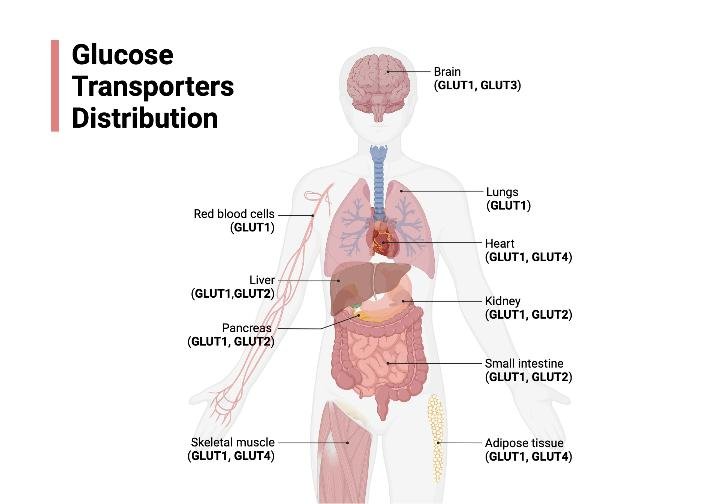
Glucose Transport via GLUT Transporters
🧠 CORE
- Glucose enters cells through GLUT transporters.
- GLUT transporters are facilitated diffusion channels.
- They do not require ATP.
- GLUT-1 is present in RBCs and blood-brain barrier.
- GLUT-2 is present in liver and pancreatic beta cells.
- GLUT-3 is important in neurons.
- GLUT-4 is insulin-dependent.
- GLUT-4 is present in skeletal muscle and adipose tissue.
🔬 CONCEPT EXPLAINED
Glucose is water-soluble and cannot freely cross the lipid cell membrane. GLUT transporters allow glucose entry according to concentration gradient. Insulin increases GLUT-4 movement to the cell membrane, increasing glucose uptake in muscle and fat.
⚠️ IF DAMAGED
Insulin resistance → reduced GLUT-4 activity → reduced glucose uptake → hyperglycemia, as seen in type 2 diabetes mellitus.
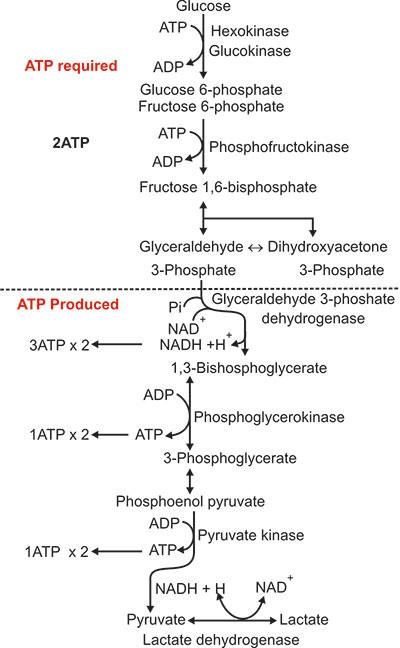
Reactions of Glycolysis
🧠 CORE
- Glycolysis has 10 reactions.
- It has an energy investment phase and energy generation phase.
- First phase uses 2 ATP.
- Second phase produces 4 ATP.
- Net gain is 2 ATP.
- Glucose is converted into glucose-6-phosphate.
- Fructose-6-phosphate is converted into fructose-1,6-bisphosphate.
- Pyruvate is the final aerobic product.
🔬 CONCEPT EXPLAINED
Glycolysis first traps glucose inside the cell by phosphorylation. Then glucose is split into two 3-carbon molecules. These are further oxidized to produce ATP and NADH.
⚠️ IF DAMAGED
Failure of glycolytic reactions → reduced ATP → muscle weakness, RBC hemolysis, and impaired tissue energy metabolism.
NADH Shuttle Systems
🧠 CORE
- Cytoplasmic NADH cannot directly enter mitochondria.
- Shuttle systems transfer reducing equivalents.
- Main shuttles are malate-aspartate shuttle and glycerol phosphate shuttle.
- Malate-aspartate shuttle gives more ATP.
- Glycerol phosphate shuttle gives less ATP.
- These shuttles support aerobic ATP production.
- They link glycolysis with oxidative phosphorylation.
🔬 CONCEPT EXPLAINED
NADH formed in cytoplasm carries high-energy electrons. Because inner mitochondrial membrane is impermeable to NADH, shuttle systems transfer these electrons into mitochondria for ATP generation.
⚠️ IF DAMAGED
Poor NADH transfer → reduced oxidative phosphorylation → reduced ATP production, especially in energy-demanding tissues.
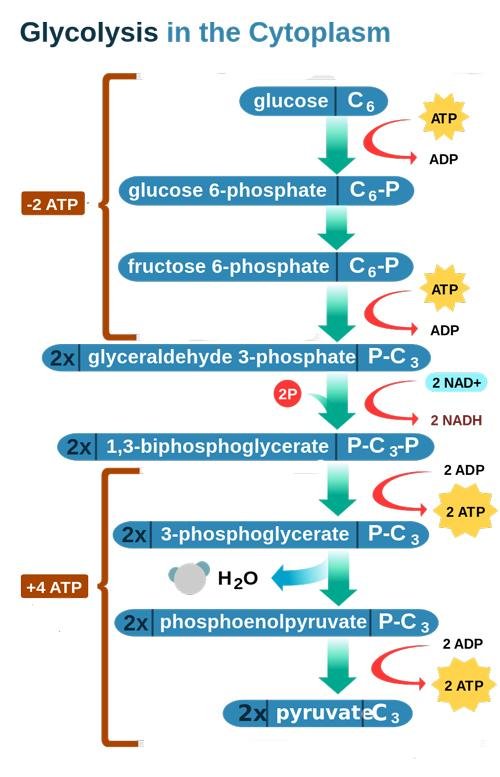
Energetics of Glycolysis
🧠 CORE
- ATP consumed: 2.
- ATP produced: 4.
- Net ATP: 2.
- NADH produced: 2.
- Aerobic glycolysis gives more ATP through NADH shuttles.
- Anaerobic glycolysis gives only 2 ATP.
- RBCs depend only on this 2 ATP.
- ATP is used for membrane pumps and cell survival.
🔬 CONCEPT EXPLAINED
Glycolysis is not highly efficient alone, but it is fast. In anaerobic conditions, it rapidly supplies ATP even without mitochondria.
⚠️ IF DAMAGED
Low ATP in RBCs → failure of ion pumps → cell swelling → hemolysis.
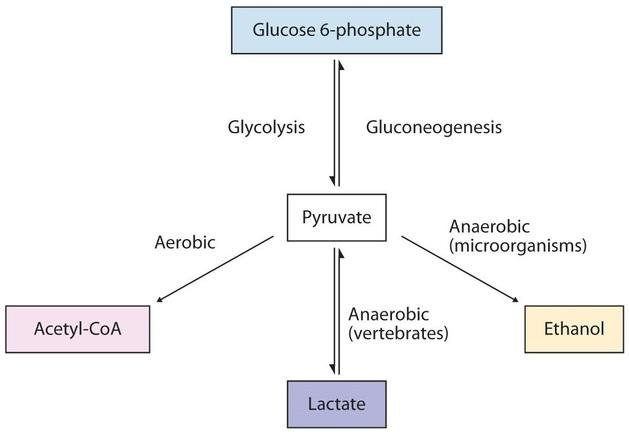
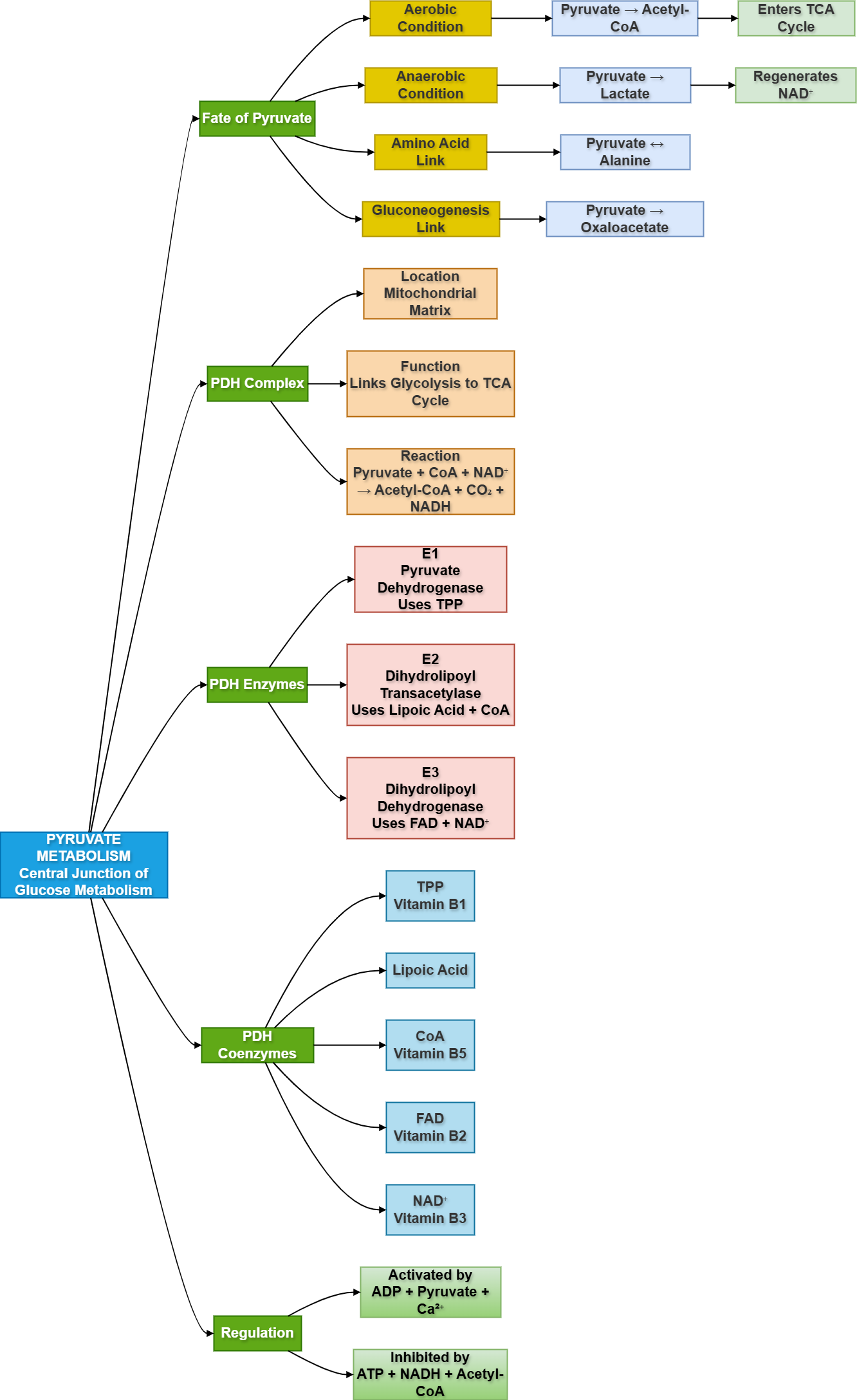
Fate of Pyruvate
🧠 CORE
- Pyruvate is the end product of aerobic glycolysis.
- It can convert to acetyl-CoA.
- It can convert to lactate.
- It can convert to oxaloacetate.
- It can convert to alanine.
- Fate depends on oxygen availability and tissue need.
- Acetyl-CoA enters TCA cycle.
- Lactate forms during anaerobic metabolism.
🔬 CONCEPT EXPLAINED
Pyruvate is a metabolic junction. In oxygen-rich conditions, it enters mitochondria and becomes acetyl-CoA. In low oxygen, it becomes lactate to regenerate NAD⁺.
⚠️ IF DAMAGED
Failure of pyruvate metabolism → lactate accumulation → lactic acidosis.
Glycolysis in RBCs
🧠 CORE
- RBCs have no mitochondria.
- They depend completely on anaerobic glycolysis.
- ATP maintains RBC membrane flexibility.
- NADH helps maintain hemoglobin function.
- 2,3-BPG is produced from glycolytic pathway.
- 2,3-BPG helps oxygen release from hemoglobin.
- Pyruvate kinase deficiency affects RBC survival.
🔬 CONCEPT EXPLAINED
RBCs cannot use TCA cycle or oxidative phosphorylation. Therefore, glycolysis is their only ATP source. ATP keeps membrane pumps active and maintains RBC shape.
⚠️ IF DAMAGED
Glycolytic enzyme deficiency → low ATP → rigid RBC membrane → hemolytic anemia.
Glycolysis in Cancer Cells
🧠 CORE
- Cancer cells show increased glycolysis.
- This occurs even in presence of oxygen.
- This is called Warburg effect.
- Cancer cells consume more glucose.
- Lactate production increases.
- PET scan uses high glucose uptake.
- Rapid glycolysis supports tumor growth.
- Glycolytic intermediates support biosynthesis.
🔬 CONCEPT EXPLAINED
Cancer cells prefer glycolysis because it provides both energy and building blocks for rapid cell division, even though it is less efficient than oxidative phosphorylation.
⚠️ IF DAMAGED
Uncontrolled glycolysis in cancer → increased lactate → acidic tumor environment → invasion and poor tissue function.
2️⃣ Pyruvate Dehydrogenase Complex
Introduction
Pyruvate dehydrogenase complex links glycolysis with the TCA cycle. It converts pyruvate into acetyl-CoA inside mitochondria. This step is irreversible and highly regulated. It is very important because acetyl-CoA enters the TCA cycle for further ATP production. Clinically, PDH deficiency causes lactic acidosis and neurological problems because pyruvate cannot enter aerobic metabolism.
Foundation Basics
- PDH complex: Converts pyruvate into acetyl-CoA.
- Location: Mitochondrial matrix.
- Nature: Irreversible reaction.
- Main function: Links glycolysis to TCA cycle.
- Main products: Acetyl-CoA, NADH, CO₂.
- Important coenzymes: TPP, lipoic acid, CoA, FAD, NAD⁺.
- Clinical deficiency: Lactic acidosis and neurological dysfunction.
Conversion of Pyruvate into Acetyl-CoA
🧠 CORE
- Pyruvate enters mitochondria.
- PDH complex converts pyruvate into acetyl-CoA.
- CO₂ is released.
- NADH is produced.
- Acetyl-CoA enters TCA cycle.
- Reaction is irreversible.
- It connects carbohydrate metabolism with energy production.
- It is inhibited when ATP and NADH are high.
🔬 CONCEPT EXPLAINED
After glycolysis, pyruvate must be converted into acetyl-CoA before entering the TCA cycle. This is done by PDH complex in mitochondria. This step allows glucose-derived carbon to enter aerobic energy metabolism.
⚠️ IF DAMAGED
PDH failure → pyruvate cannot become acetyl-CoA → pyruvate converts to lactate → lactic acidosis.
Enzymes of PDH Complex
🧠 CORE
- PDH complex has three main enzymes.
- E1: Pyruvate dehydrogenase.
- E2: Dihydrolipoyl transacetylase.
- E3: Dihydrolipoyl dehydrogenase.
- E1 requires thiamine pyrophosphate.
- E2 transfers acetyl group to CoA.
- E3 regenerates oxidized lipoamide.
- Enzymes work as a coordinated complex.
🔬 CONCEPT EXPLAINED
The PDH complex acts like an assembly line. Pyruvate enters, is decarboxylated, transferred, oxidized, and finally converted into acetyl-CoA.
⚠️ IF DAMAGED
Defect in any enzyme → reduced acetyl-CoA formation → reduced TCA cycle activity → energy failure.
Coenzymes of PDH Complex
🧠 CORE
- TPP comes from vitamin B1.
- Lipoic acid transfers acetyl groups.
- CoA comes from vitamin B5.
- FAD comes from vitamin B2.
- NAD⁺ comes from vitamin B3.
- These coenzymes support oxidation and transfer reactions.
- Vitamin deficiency can impair PDH function.
- Thiamine deficiency is especially important.
🔬 CONCEPT EXPLAINED
PDH requires multiple vitamin-derived coenzymes. These molecules help remove CO₂, transfer acetyl groups, and generate NADH.
⚠️ IF DAMAGED
Thiamine deficiency → poor PDH activity → pyruvate accumulation → lactic acidosis and neurological symptoms.
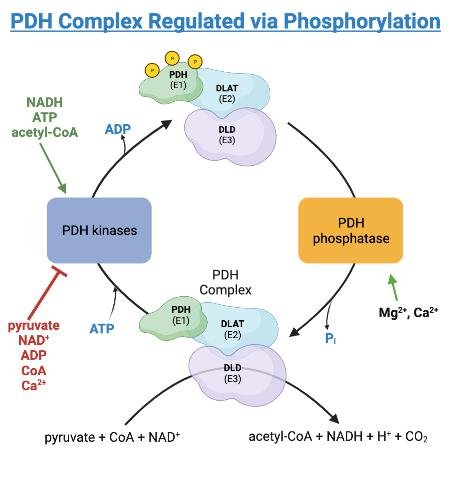
Regulation of PDH
🧠 CORE
- PDH is controlled by energy status.
- ATP inhibits PDH.
- NADH inhibits PDH.
- Acetyl-CoA inhibits PDH.
- ADP activates PDH.
- Pyruvate activates PDH.
- PDH kinase inhibits PDH.
- PDH phosphatase activates PDH.
🔬 CONCEPT EXPLAINED
When the cell has enough energy, PDH is switched off. When energy is low, PDH is activated to produce more acetyl-CoA for ATP generation.
⚠️ IF DAMAGED
Poor regulation → either energy waste or energy failure. PDH deficiency particularly affects brain because brain depends heavily on glucose oxidation.
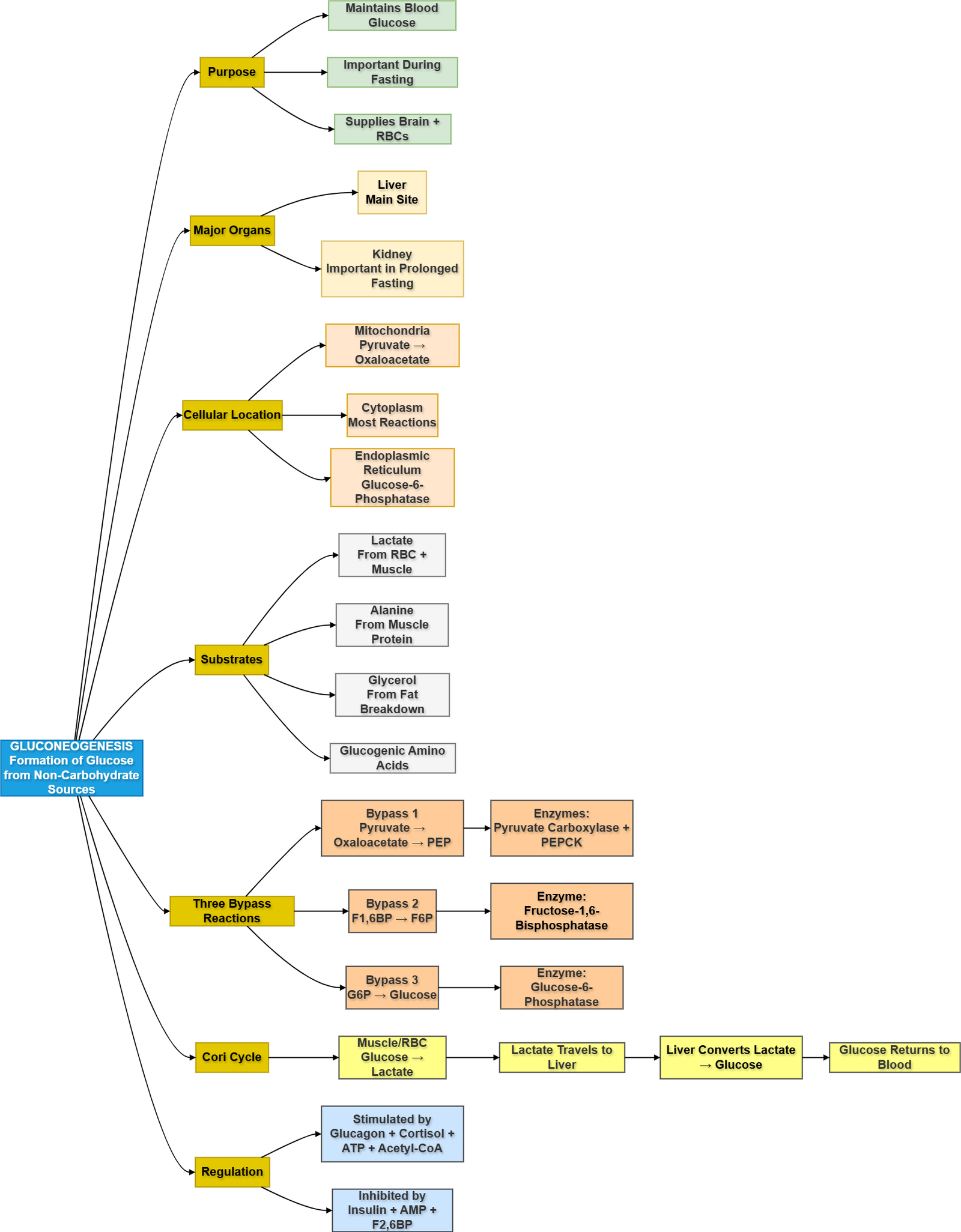
3️⃣ Gluconeogenesis
Definition and Organs of Gluconeogenesis
🧠 CORE
- Gluconeogenesis means synthesis of glucose from non-carbohydrate sources.
- It occurs mainly in liver.
- Kidney contributes during prolonged fasting.
- It maintains blood glucose.
- It is important between meals.
- It becomes more active during fasting.
- It protects brain and RBCs from glucose deficiency.
- It is opposite to glycolysis but not exact reverse.
🔬 CONCEPT EXPLAINED
Gluconeogenesis is needed because glycogen stores are limited. After glycogen is depleted, the body must make new glucose to maintain blood sugar.
⚠️ IF DAMAGED
Failure of gluconeogenesis → fasting hypoglycemia → sweating, confusion, seizures, coma.
Cellular Location
🧠 CORE
- Occurs in cytoplasm and mitochondria.
- Pyruvate carboxylase works in mitochondria.
- PEPCK may work in cytosol or mitochondria.
- Fructose-1,6-bisphosphatase works in cytosol.
- Glucose-6-phosphatase is in endoplasmic reticulum.
- Liver has glucose-6-phosphatase.
- Muscle lacks glucose-6-phosphatase.
- Muscle cannot release free glucose into blood.
🔬 CONCEPT EXPLAINED
Different steps occur in different cellular compartments. This allows controlled glucose production and prevents direct reversal of glycolysis.
⚠️ IF DAMAGED
Enzyme or compartment defect → impaired glucose release → fasting hypoglycemia.
Substrates of Gluconeogenesis
🧠 CORE
- Lactate is an important substrate.
- Alanine comes from muscle.
- Glycerol comes from fat breakdown.
- Glucogenic amino acids can form glucose.
- Propionate from odd-chain fatty acids may contribute.
- Even-chain fatty acids cannot produce net glucose.
- Substrates increase during fasting.
- Liver converts them into glucose.
🔬 CONCEPT EXPLAINED
During fasting, muscle protein and fat breakdown provide carbon skeletons. These enter gluconeogenesis to maintain blood glucose.
⚠️ IF DAMAGED
Substrate deficiency or enzyme failure → reduced glucose synthesis → hypoglycemia.
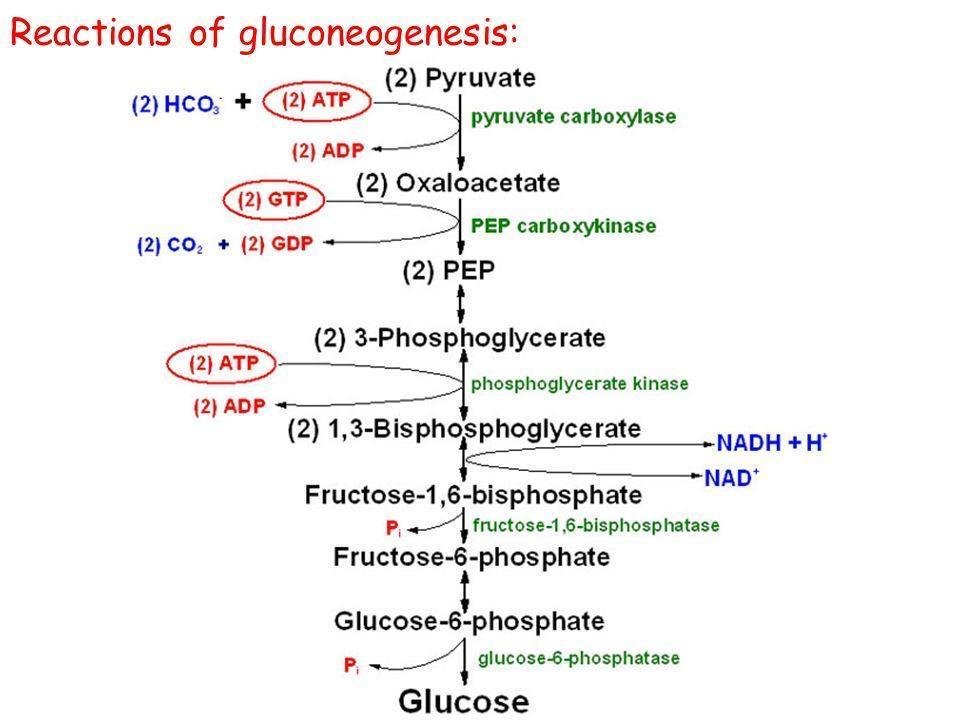
Three Bypass Reactions
🧠 CORE
- Gluconeogenesis bypasses irreversible glycolysis steps.
- Pyruvate kinase is bypassed.
- PFK-1 is bypassed.
- Hexokinase/glucokinase is bypassed.
- Pyruvate → oxaloacetate → PEP.
- Fructose-1,6-bisphosphate → fructose-6-phosphate.
- Glucose-6-phosphate → glucose.
- These steps require special enzymes.
🔬 CONCEPT EXPLAINED
Glycolysis has three irreversible steps. Gluconeogenesis cannot simply reverse them, so it uses bypass enzymes to move around these blocks.
⚠️ IF DAMAGED
Defective bypass enzymes → inability to make glucose → fasting hypoglycemia and lactic acidosis.
Cori Cycle
🧠 CORE
- Muscle and RBC produce lactate.
- Lactate travels to liver.
- Liver converts lactate into glucose.
- Glucose returns to blood.
- Muscle/RBC use glucose again.
- It prevents lactate accumulation.
- It supports anaerobic tissues.
- It costs energy in liver.
🔬 CONCEPT EXPLAINED
The Cori cycle connects anaerobic glycolysis in tissues with gluconeogenesis in liver. It allows lactate to be recycled into glucose.
⚠️ IF DAMAGED
Poor lactate recycling → lactate accumulation → lactic acidosis.
Regulation of Gluconeogenesis
🧠 CORE
- Glucagon stimulates gluconeogenesis.
- Cortisol supports gluconeogenesis.
- Insulin inhibits gluconeogenesis.
- ATP activates gluconeogenesis.
- AMP inhibits gluconeogenesis.
- Acetyl-CoA activates pyruvate carboxylase.
- Fructose-2,6-bisphosphate inhibits gluconeogenesis.
- It is active during fasting.
🔬 CONCEPT EXPLAINED
When blood glucose is low, glucagon activates gluconeogenesis. When blood glucose is high, insulin suppresses it. This maintains glucose homeostasis.
⚠️ IF DAMAGED
Excess gluconeogenesis → hyperglycemia.
Reduced gluconeogenesis → fasting hypoglycemia.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
- GLUT transporters → Glucose entry → Fuel availability
- Glycolysis in cytoplasm → Rapid ATP production → Cell survival
- RBC glycolysis → ATP without mitochondria → Maintains RBC membrane
- Pyruvate → Acetyl-CoA → TCA cycle entry
- PDH complex → Link between glycolysis and TCA → Aerobic ATP production
- Gluconeogenesis in liver → New glucose synthesis → Maintains blood glucose
- Cori cycle → Lactate recycling → Prevents lactate accumulation
🩺 5️⃣ Clinical Correlation
- Pyruvate kinase deficiency: Low ATP in RBCs → hemolytic anemia.
- PDH deficiency: Pyruvate accumulation → lactate formation → lactic acidosis, neurological signs.
- Thiamine deficiency: Reduced PDH activity → poor aerobic glucose metabolism.
- Cancer metabolism: Warburg effect → increased glucose uptake and lactate production.
- Fasting hypoglycemia: May occur when gluconeogenesis is defective.
- Diabetes mellitus: Increased hepatic gluconeogenesis contributes to hyperglycemia.
- Lactic acidosis: Can occur when pyruvate is diverted excessively to lactate
📌 6️⃣ Summary Points
- Glycolysis occurs in the cytoplasm of all cells.
- Net gain of glycolysis is 2 ATP and 2 NADH.
- Anaerobic glycolysis converts pyruvate into lactate.
- RBCs depend completely on glycolysis for ATP.
- Cancer cells show increased glycolysis called Warburg effect.
- PDH complex converts pyruvate into acetyl-CoA.
- PDH requires five coenzymes: TPP, lipoic acid, CoA, FAD, NAD⁺.
- PDH deficiency causes lactic acidosis.
- Gluconeogenesis mainly occurs in liver and kidney.
- Gluconeogenesis maintains blood glucose during fasting.
- Cori cycle recycles lactate into glucose.
- Insulin inhibits gluconeogenesis, while glucagon stimulates it.
🎥 7️⃣ Video Explanation