
📖 Step 2 — Learning Material
1️⃣ Introduction
Gastric secretion is a vital physiological process that enables digestion of food within the stomach. The stomach, located in the upper left quadrant of the abdomen, functions both as a reservoir and as a secretory organ producing acid, enzymes, and protective mucus. These secretions initiate protein digestion, kill ingested microorganisms, and prepare food for absorption in the intestine.
Understanding gastric secretion is clinically important because disturbances in acid production lead to common disorders such as peptic ulcer disease, gastritis, and vitamin B₁₂ deficiency. The coordinated action of gastric glands, hormones, nerves, and reflexes ensures proper digestion.
This topic integrates Physiology and Biochemistry, linking cellular mechanisms of secretion with functional digestive outcomes.
2️⃣ Foundation Basics
Key Definitions
• Gastric Secretion
Release of digestive fluids (acid, enzymes, mucus, intrinsic factor) from gastric glands.
• Gastric Glands
Specialized tubular glands located in gastric mucosa responsible for secretion.
• Hydrochloric Acid (HCl)
Strong acid secreted by parietal cells that creates an acidic environment.
• Intrinsic Factor (IF)
Glycoprotein secreted by parietal cells required for Vitamin B₁₂ absorption.
• Pepsinogen
Inactive enzyme precursor secreted by chief cells.
• Pepsin
Active proteolytic enzyme formed from pepsinogen.
• Mucus
Viscous protective secretion produced by mucous cells.
Essential Terminology
• Parietal cells — Secrete HCl and intrinsic factor
• Chief cells — Secrete pepsinogen
• Mucous cells — Secrete mucus
• Enteroendocrine cells — Secrete hormones (e.g., gastrin)
• Pylorus — Regulates gastric emptying
• Vagus nerve — Major parasympathetic supply
Basic Overview
Gastric secretion:
• Begins even before food enters stomach
• Continues during digestion
• Is controlled by nerves and hormones
• Produces acidic environment (pH 1–3)
• Protects stomach lining through mucus barrier
• Prepares nutrients for intestinal digestion
3️⃣ Core Learning — Curriculum Coverage
CHARACTERISTICS OF GASTRIC SECRETION
🧠 CORE
• Gastric secretion volume: 1500–2500 mL/day
• Highly acidic (pH 1–3)
• Contains HCl, enzymes, mucus, intrinsic factor
• Produced by gastric glands
• Secreted continuously but varies with food intake
• Plays role in digestion and protection
• Contains antibacterial components
• Secretion regulated by neural and hormonal control
🔬 CONCEPT EXPLAINED
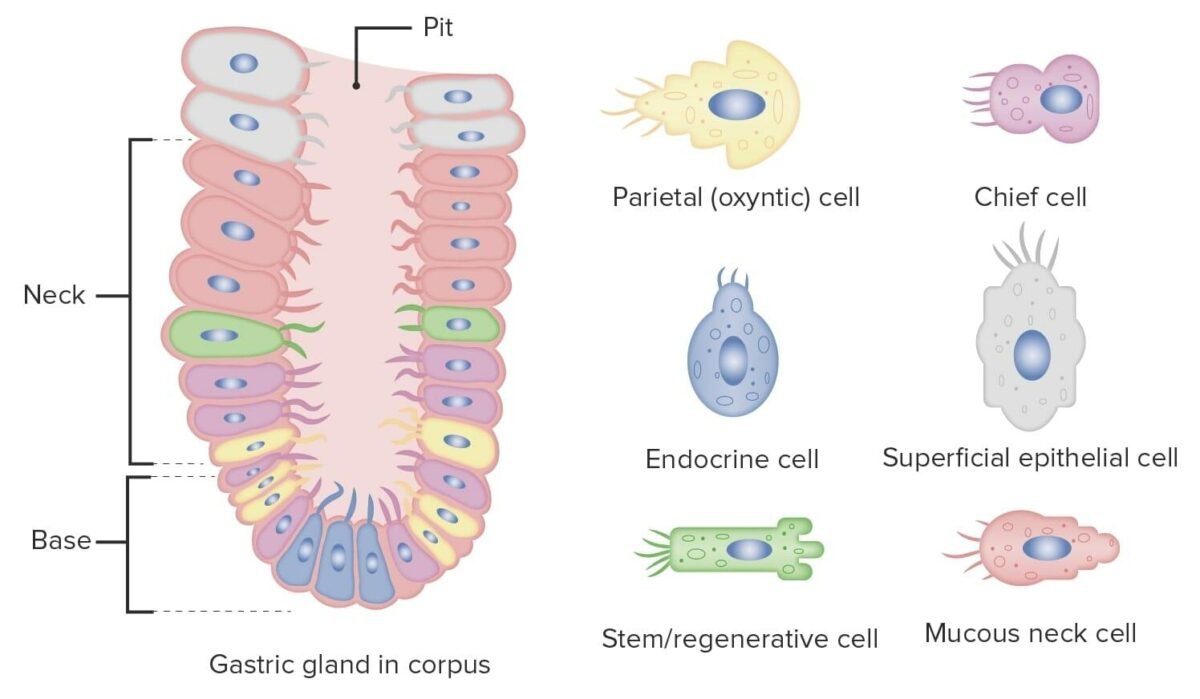
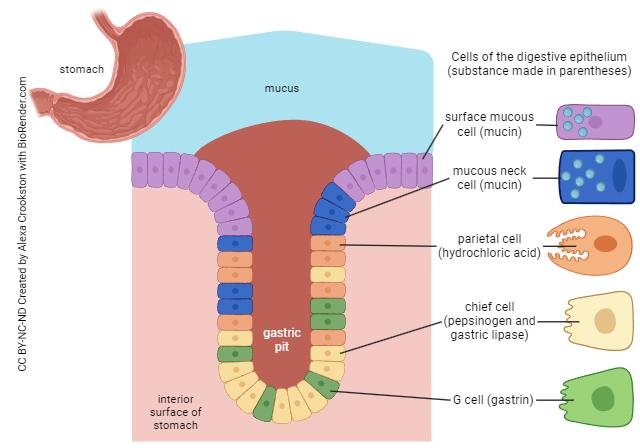
Gastric glands are embedded within the mucosa of the stomach. These glands consist of different specialized cells that produce distinct components of gastric juice.
Parietal cells produce hydrochloric acid, which maintains acidic pH necessary for digestion. Chief cells produce pepsinogen, which becomes active pepsin in acidic medium. Mucous cells secrete mucus forming a protective barrier that shields the stomach lining from acid damage.
This coordinated secretion ensures that digestion begins efficiently while protecting gastric tissue from self-digestion.
⚠️ IF DAMAGED
If gastric secretion is abnormal:
Cause → Effect
↓ Acid secretion → Poor digestion → Bacterial overgrowth
↓ Mucus barrier → Acid injury → Gastric ulcer
↓ Intrinsic factor → Vitamin B₁₂ deficiency → Pernicious anemia
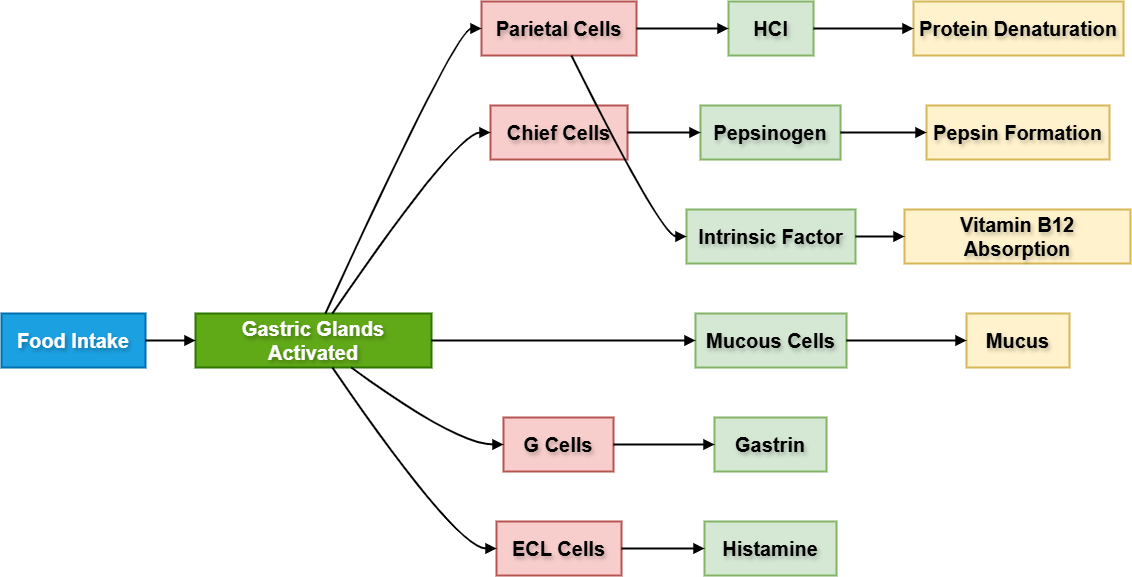
MECHANISM OF GASTRIC GLAND SECRETION
🧠 CORE
Major gastric gland cells:
• Parietal cells — HCl, intrinsic factor
• Chief cells — Pepsinogen
• Mucous cells — Mucus
• Enteroendocrine cells — Hormones
• Secretion stimulated by food intake
• Requires neural and hormonal signals
• Energy-dependent cellular process
• Occurs through membrane transport systems
🔬 CONCEPT EXPLAINED
Gastric gland secretion depends on coordinated activity of different cell types. When food enters stomach, vagal stimulation activates parietal and chief cells.
Parietal cells use proton pumps to actively transport hydrogen ions into gastric lumen. Chief cells release pepsinogen through exocytosis. Mucous cells continuously secrete protective mucus.
Hormones such as gastrin stimulate secretion by increasing activity of parietal cells.
⚠️ IF DAMAGED
Damage to gastric gland cells leads to:
Loss of parietal cells → No acid → Poor digestion
Chief cell damage → Reduced enzyme → Impaired protein digestion
Mucous cell damage → Ulcer formation
PHASES OF GASTRIC SECRETION
🧠 CORE
Three phases:
• Cephalic phase
• Gastric phase
• Intestinal phase
• Controlled by neural and hormonal mechanisms
• Begins before food ingestion
• Continues during digestion
• Declines after gastric emptying
🔬 CONCEPT EXPLAINED
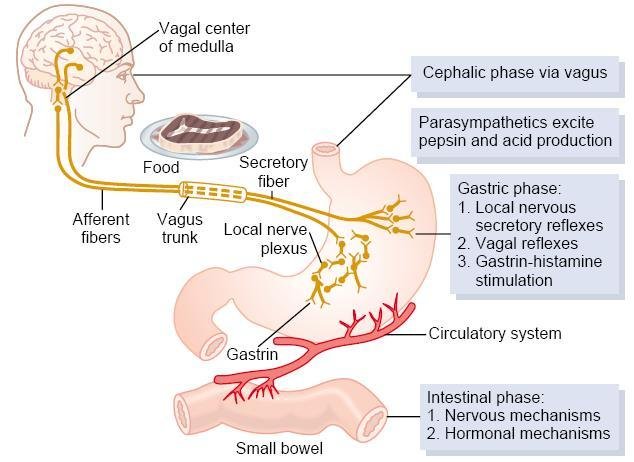
Cephalic Phase
Triggered by:
• Sight
• Smell
• Taste
• Thought of food
Mechanism:
Vagus nerve stimulates gastric glands → Secretion begins.
Accounts for ~30% of secretion.
Gastric Phase
Triggered by:
• Food entering stomach
• Gastric distension
• Presence of peptides
Mechanism:
Stretch receptors + gastrin release → Increased secretion.
Accounts for ~60% of secretion.
Intestinal Phase
Triggered by:
• Food entering intestine
Mechanism:
Initially stimulates secretion briefly, then inhibits gastric secretion.
Accounts for ~10% of secretion.
⚠️ IF DAMAGED
Failure of phase coordination leads to:
Excess secretion → Ulcers
Reduced secretion → Poor digestion
REGULATION OF GASTRIC SECRETION
🧠 CORE
Controlled by:
• Nervous system
• Hormonal system
• Local reflexes
• Vagus nerve stimulation
• Gastrin hormone
• Histamine release
• Negative feedback mechanisms
🔬 CONCEPT EXPLAINED
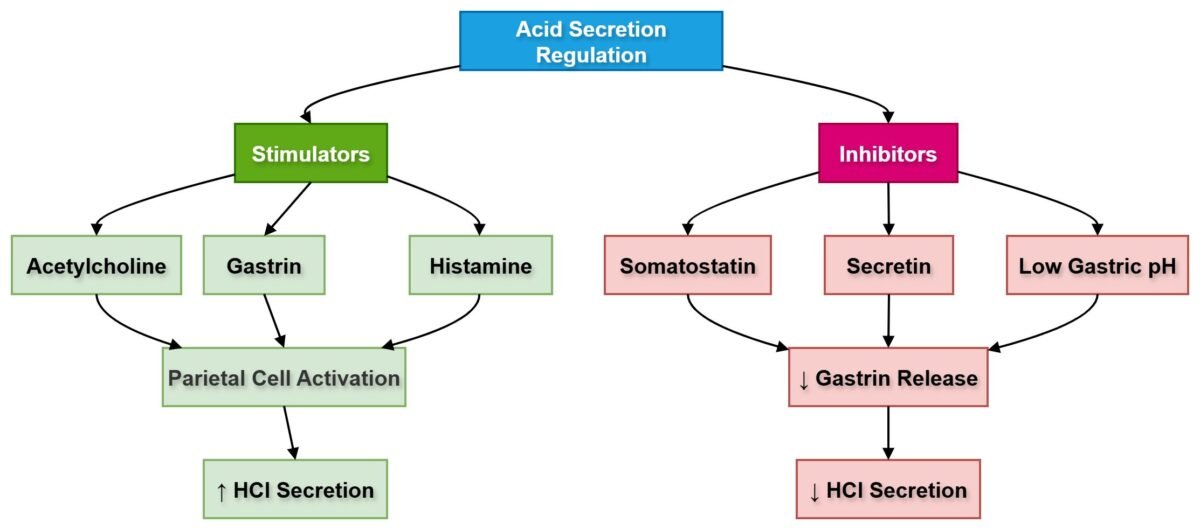
Gastric secretion regulation involves both neural and hormonal pathways. The vagus nerve releases acetylcholine, stimulating parietal cells. Gastrin released from G cells enhances acid production. Histamine released from ECL cells increases proton pump activity.
When gastric pH becomes very acidic, feedback mechanisms reduce secretion to prevent excessive acid accumulation.
⚠️ IF DAMAGED
Loss of regulation leads to:
Hypersecretion → Ulcer formation
Hyposecretion → Malabsorption
HORMONES REGULATING GASTRIC SECRETION
🧠 CORE
Major hormones:
• Gastrin — Stimulates acid secretion
• Histamine — Enhances acid production
• Somatostatin — Inhibits secretion
• Secretin — Reduces gastric secretion
• Cholecystokinin (CCK) — Inhibits gastric emptying
• Released from enteroendocrine cells
• Maintain digestive balance
🔬 CONCEPT EXPLAINED
Gastrin is released in response to proteins in stomach. It stimulates parietal cells directly and indirectly through histamine release. Somatostatin acts as inhibitory hormone preventing excessive secretion.
Secretin released from duodenum reduces acid production when acidic chyme enters intestine.
⚠️ IF DAMAGED
Hormonal imbalance causes:
↑ Gastrin → Hyperacidity → Ulcers
↓ Somatostatin → Uncontrolled secretion
REFLEX CONTROL OF GASTRIC SECRETION
🧠 CORE
Controlled through:
• Short reflexes
• Long reflexes
• Vagus nerve
• Enteric nervous system
• Stretch receptors
• Chemoreceptors
• Local reflex arcs
🔬 CONCEPT EXPLAINED
Reflexes regulate secretion depending on gastric contents. Stretch receptors detect stomach distension. Chemoreceptors detect food chemicals. Signals transmitted via enteric nervous system and vagus nerve stimulate secretion.
⚠️ IF DAMAGED
Loss of reflex control results in:
Poor secretion timing → Digestive disorders
CHEMICAL COMPOSITION OF GASTRIC SECRETION
🧠 CORE
Components:
• Hydrochloric acid
• Pepsinogen
• Mucus
• Intrinsic factor
• Water
• Electrolytes
• Lipase
• Bicarbonate
🔬 CONCEPT EXPLAINED
Each component serves specific function:
HCl maintains acidic pH. Pepsinogen converts into pepsin to digest proteins. Mucus protects mucosa. Intrinsic factor enables Vitamin B₁₂ absorption.
⚠️ IF DAMAGED
Loss of components leads to:
No mucus → Ulcers
No intrinsic factor → Pernicious anemia
FUNCTIONS OF HCl
🧠 CORE
HCl functions:
• Activates pepsinogen
• Provides acidic pH
• Kills bacteria
• Denatures proteins
• Facilitates mineral absorption
• Enhances digestion
• Supports enzyme function
🔬 CONCEPT EXPLAINED
HCl lowers gastric pH, creating environment optimal for enzyme activation. It denatures protein structures making them easier to digest. Acidic medium also destroys harmful microorganisms entering with food.
⚠️ IF DAMAGED
Low acid → Infection risk
High acid → Ulcers
MECHANISM OF HCl SECRETION
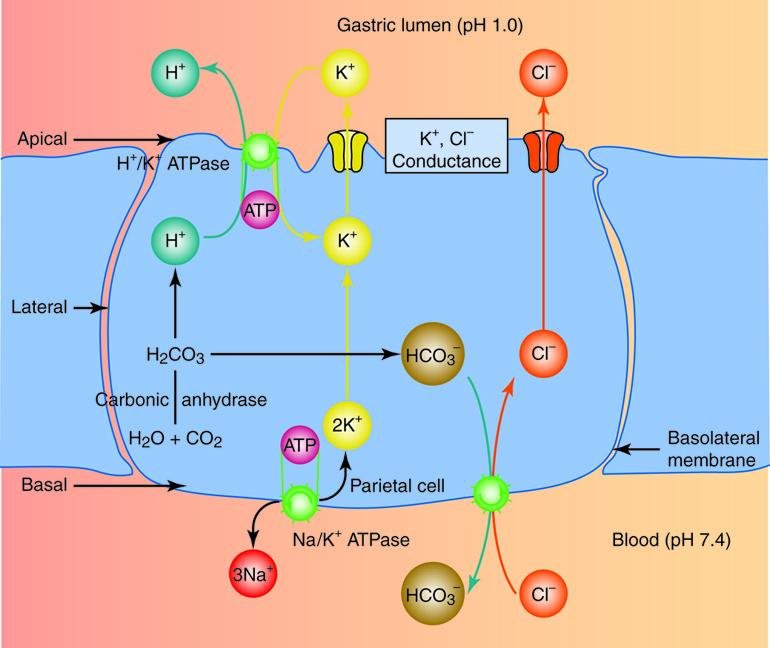
🧠 CORE
Occurs in:
• Parietal cells
• Involves proton pump
• Requires ATP
• Carbonic anhydrase enzyme
• Hydrogen ion transport
• Chloride ion movement
• Formation of hydrochloric acid
🔬 CONCEPT EXPLAINED
Hydrogen ions are generated inside parietal cells using carbonic anhydrase. Proton pumps transport hydrogen ions into gastric lumen. Chloride ions follow, forming hydrochloric acid.
⚠️ IF DAMAGED
Proton pump inhibition → Reduced acid
Carbonic anhydrase failure → Poor acid formation
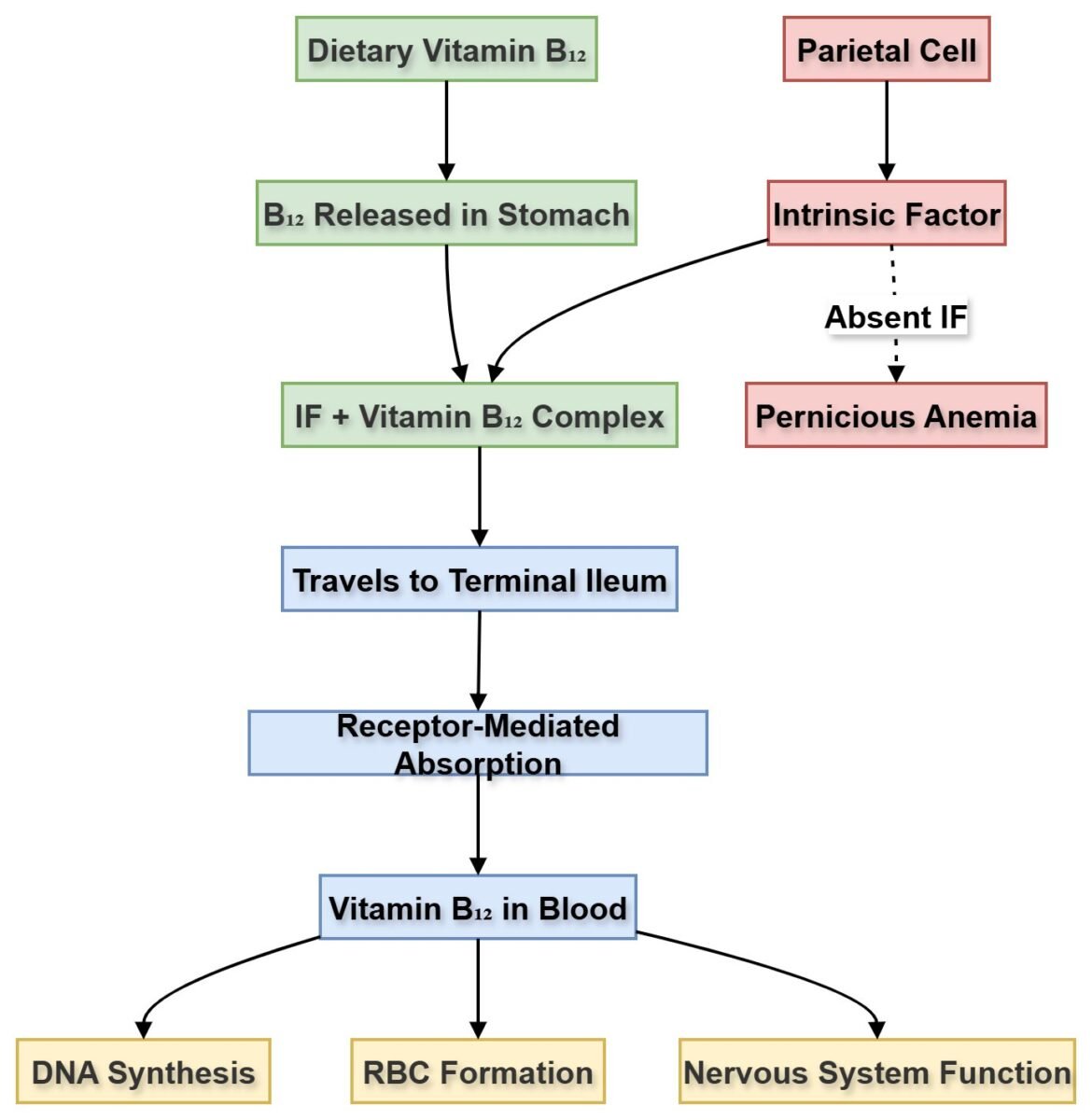
INTRINSIC FACTOR SECRETION
🧠 CORE
• Secreted by parietal cells
• Glycoprotein in nature
• Essential for Vitamin B₁₂ absorption
• Binds Vitamin B₁₂
• Protects Vitamin B₁₂
• Facilitates absorption in ileum
🔬 CONCEPT EXPLAINED
Intrinsic factor binds Vitamin B₁₂ forming stable complex. This complex travels to ileum where absorption occurs through receptor-mediated process.
⚠️ IF DAMAGED
Loss of intrinsic factor leads to:
Vitamin B₁₂ deficiency → Megaloblastic anemia
Topic 7 — Title
Write Topic 7 content here.
Topic 8 — Title
Write Topic 8 content here.
4️⃣ Mechanism Flow
Mechanism of HCl Secretion
- CO₂ enters parietal cell
- Carbonic anhydrase forms carbonic acid
- Carbonic acid splits into H⁺ and HCO₃⁻
- H⁺ pumped into lumen via proton pump
- Cl⁻ diffuses into lumen
- H⁺ + Cl⁻ → HCl formation
5️⃣ Functional Integration
Structure → Function → Outcome
Parietal cells → Acid secretion → Protein digestion
Chief cells → Pepsin secretion → Protein breakdown
Mucous cells → Mucus barrier → Protection
Intrinsic factor → Vitamin B₁₂ absorption → RBC production
6️⃣ Clinical Correlation
• Peptic Ulcer Disease (PUD)
Localized mucosal erosion of stomach or duodenum caused by excess acid–pepsin activity or reduced mucosal protection.
• Gastritis
Inflammation of gastric mucosa due to infection (commonly H. pylori), drugs, or alcohol.
• Pernicious Anemia
Megaloblastic anemia caused by deficiency of intrinsic factor leading to impaired Vitamin B₁₂ absorption.
• Zollinger–Ellison Syndrome
Condition caused by gastrin-secreting tumor (gastrinoma) leading to excessive gastric acid production.
• Achlorhydria
Complete absence of hydrochloric acid secretion from stomach.
⭐ 7️⃣ Points to Remember
• Gastric secretion volume: ~2 liters/day
• Three phases: Cephalic, Gastric, Intestinal
• Parietal cells produce HCl + intrinsic factor
• Chief cells produce pepsinogen
• Gastrin stimulates acid secretion
• Histamine enhances proton pump activity
• Mucus protects stomach lining
• HCl activates pepsin
• Intrinsic factor required for Vitamin B₁₂ absorption
• Excess acid causes ulcers
• Reduced intrinsic factor causes pernicious anemia