
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Eicosanoids are powerful biochemical mediators derived from fatty acids that regulate inflammation, pain, fever, allergy, platelet function, and smooth muscle activity. They are produced in almost all tissues of the body, especially at sites of injury and inflammation. Although synthesized in very small amounts, they have potent local effects.
The major eicosanoids include prostaglandins, thromboxanes, leukotrienes, and prostacyclin. These mediators are formed mainly from arachidonic acid released from membrane phospholipids. Their synthesis occurs through cyclo-oxygenase (COX) and lipoxygenase pathways.
Clinically, eicosanoids are extremely important because many commonly used drugs such as aspirin, NSAIDs, corticosteroids, montelukast, and zileuton act by modifying their synthesis or action. Excess or deficiency of eicosanoid activity contributes to diseases like asthma, gastric ulcer, thrombosis, allergy, and chronic inflammation.
Understanding eicosanoid metabolism helps explain:
- Mechanism of inflammation
- Drug action of NSAIDs and steroids
- Bronchial asthma pathogenesis
- Fever and pain mechanisms
- Platelet aggregation and thrombosis
🔹 2️⃣ Foundation Concepts
Key Definitions
- Eicosanoids: Biologically active lipid mediators derived from 20-carbon polyunsaturated fatty acids mainly arachidonic acid.
- Arachidonic acid: A 20-carbon omega-6 fatty acid stored in membrane phospholipids.
- Cyclo-oxygenase (COX): Enzyme pathway producing prostaglandins and thromboxanes.
- Lipoxygenase (LOX): Enzyme pathway producing leukotrienes.
- Prostaglandins (PGs): Mediators involved in inflammation, pain, fever, and smooth muscle regulation.
- Thromboxane (TXA₂): Promotes platelet aggregation and vasoconstriction.
- Prostacyclin (PGI₂): Inhibits platelet aggregation and causes vasodilation.
- Leukotrienes: Mediators important in bronchoconstriction and allergic inflammation.
- NSAIDs: Non-steroidal anti-inflammatory drugs that inhibit COX enzymes.
Essential Terminology
- Local hormones
- Autocrine action
- Paracrine action
- Inflammatory mediators
- Platelet aggregation
- Bronchoconstriction
- Vasodilation
- Chemotaxis
Basic Overview
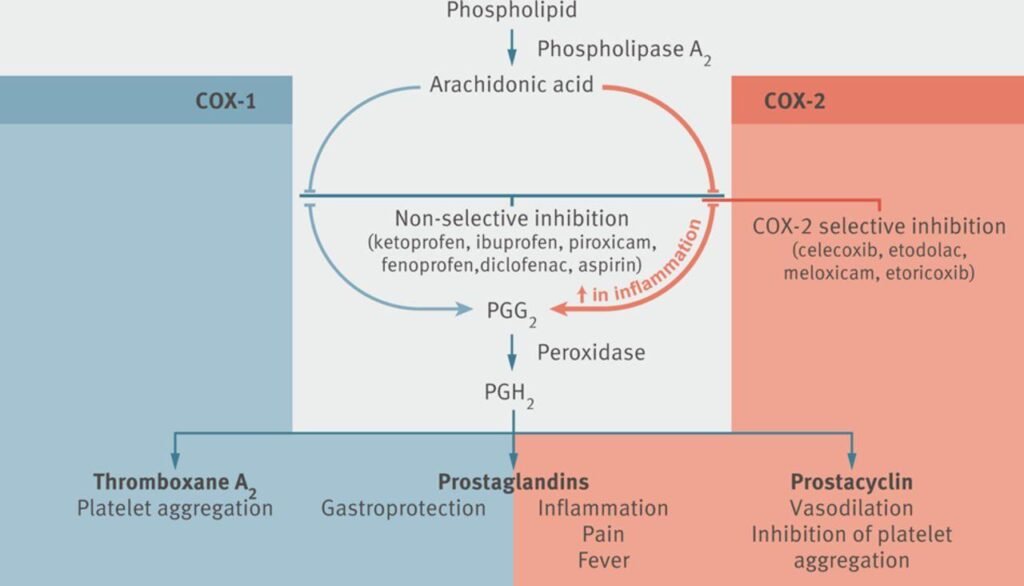
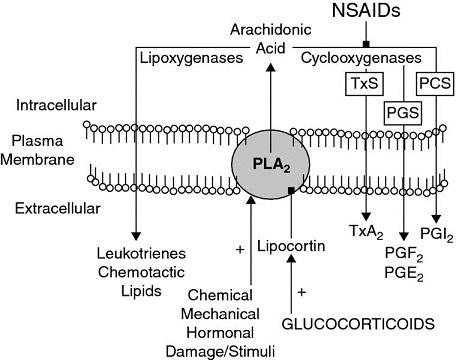
- Cell membrane phospholipids contain arachidonic acid.
- Injury or inflammation activates phospholipase A₂.
- Arachidonic acid is released.
- It enters:
- COX pathway → prostaglandins + thromboxanes
- LOX pathway → leukotrienes
- Drugs modify these pathways to reduce inflammation.
🔹 3️⃣ Core Learning — Curriculum Coverage
2️⃣ Cyclo-Oxygenase (COX) Pathway
🧠 CORE
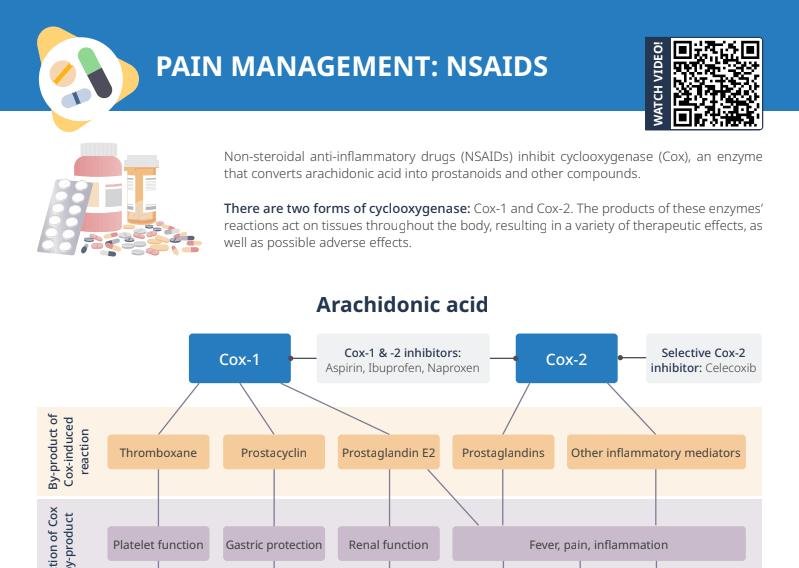
- Cyclo-oxygenase (COX) pathway converts arachidonic acid into prostaglandins and thromboxanes.
- It is the major inflammatory pathway of eicosanoid metabolism.
- COX enzymes act on arachidonic acid released from membrane phospholipids.
- Two major COX isomers:
- COX-1
- COX-2
- COX-1 is constitutive and protective.
- COX-2 is inducible and inflammatory.
- NSAIDs and aspirin inhibit COX enzymes.
- Prostaglandins mediate:
- Pain
- Fever
- Inflammation
- Thromboxane A₂ promotes platelet aggregation.
🔬 CONCEPT EXPLAINED
Cell membrane phospholipids contain arachidonic acid. During tissue injury or inflammation, phospholipase A₂ releases arachidonic acid from the membrane.
The released arachidonic acid enters the cyclo-oxygenase pathway.
Main Steps of COX Pathway
- Arachidonic acid enters COX enzyme.
- COX converts arachidonic acid into:
- PGG₂
- PGH₂
- PGH₂ is converted into different prostanoids depending on tissue type.
Important Prostanoids Produced
| Prostanoid | Major Function |
|---|---|
| PGE₂ | Pain, fever, vasodilation |
| PGI₂ (Prostacyclin) | Vasodilation, inhibits platelet aggregation |
| TXA₂ | Platelet aggregation, vasoconstriction |
| PGF₂α | Smooth muscle contraction |
The body uses this pathway because inflammation requires rapid local chemical signaling to protect tissues and recruit immune responses.
COX-1 vs COX-2
🧠 CORE
COX-1
- Physiological enzyme
- Present normally in tissues
- Protects gastric mucosa
- Maintains renal blood flow
- Produces platelet thromboxane
COX-2
- Inducible enzyme
- Activated during inflammation
- Produces inflammatory prostaglandins
- Responsible for pain and swelling
🔬 CONCEPT EXPLAINED
COX-1 — “Protective Housekeeping Enzyme”
COX-1 functions continuously in normal tissues.
Major functions:
- Gastric mucosal protection
- Platelet aggregation
- Maintenance of renal perfusion
In the stomach:
- Stimulates mucus secretion
- Stimulates bicarbonate secretion
- Reduces acid injury
In platelets:
- Produces TXA₂
- Helps hemostasis
COX-2 — “Inflammatory Enzyme”
COX-2 is induced by:
- Cytokines
- Trauma
- Infection
- Inflammation
Produces prostaglandins causing:
- Pain
- Fever
- Vasodilation
- Edema
This separation allows the body to preserve normal physiological protection while still mounting inflammatory responses when needed.
⚠️ IF DAMAGED
Excess COX-2 Activity
Cause:
- Increased inflammatory prostaglandins
Effect:
- Pain
- Fever
- Chronic inflammation
COX-1 Inhibition
Cause:
- Loss of protective prostaglandins
Effect:
- Gastric ulcer
- GI bleeding
- Reduced platelet function
COX Inhibition
🧠 CORE
- NSAIDs inhibit cyclo-oxygenase enzymes.
- This decreases prostaglandin synthesis.
- Reduces inflammation, pain, and fever.
- Most NSAIDs reversibly inhibit COX.
- Aspirin irreversibly inhibits COX.
- COX inhibition is the basis of anti-inflammatory drug therapy.
🔬 CONCEPT EXPLAINED
Inflammation produces prostaglandins that sensitize pain receptors and increase vascular permeability.
NSAIDs block conversion of arachidonic acid into prostaglandins.
Effects of COX Inhibition
| Reduced Mediator | Clinical Effect |
|---|---|
| ↓ PGE₂ | Reduced pain |
| ↓ PGE₂ in hypothalamus | Reduced fever |
| ↓ inflammatory PGs | Reduced swelling |
| ↓ TXA₂ | Reduced platelet aggregation |
This mechanism explains why NSAIDs are widely used in:
- Fever
- Headache
- Arthritis
- Musculoskeletal pain
⚠️ IF DAMAGED
Excessive COX Inhibition
Cause:
- Reduced protective prostaglandins
Effect:
- Gastric mucosal injury
- Peptic ulcer
- Renal ischemia
- Bleeding tendency
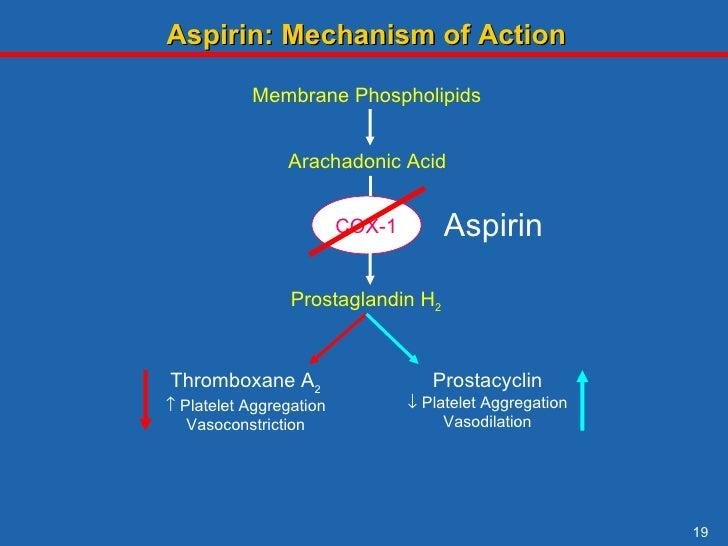
Aspirin Mechanism
🧠 CORE
- Aspirin irreversibly inhibits COX enzyme.
- Acetylates COX active site.
- Prevents thromboxane synthesis.
- Reduces platelet aggregation.
- Used in cardiovascular disease prevention.
- Has analgesic, antipyretic, and anti-inflammatory actions.
🔬 CONCEPT EXPLAINED
Aspirin transfers an acetyl group to the COX enzyme, permanently inactivating it.
In Platelets
Platelets lack nuclei and cannot synthesize new COX enzyme.
Result:
- Persistent reduction in TXA₂
- Reduced platelet aggregation
- Reduced thrombosis risk
In Endothelial Cells
Endothelial cells can synthesize new COX enzyme.
Therefore:
- PGI₂ production recovers
- Vasodilatory protection continues
This selective balance explains why low-dose aspirin is used for prevention of:
- Myocardial infarction
- Stroke
⚠️ IF DAMAGED
Excess Aspirin Use
Cause:
- Excessive COX inhibition
Effect:
- Gastric bleeding
- Peptic ulceration
- Hemorrhage
- Tinnitus
- Salicylate toxicity
Aspirin in Children
Cause:
- Viral illness + aspirin use
Effect:
- Reye syndrome
- Hepatic dysfunction
- Encephalopathy
3️⃣ Clinical Pharmacology of COX Inhibition
NSAIDs Adverse Effects
🧠 CORE
Major adverse effects:
- Gastritis
- Peptic ulcer
- GI bleeding
- Renal impairment
- Sodium retention
- Hypersensitivity
- Bronchospasm
🔬 CONCEPT EXPLAINED
NSAIDs inhibit protective prostaglandins produced by COX-1.
In Stomach
Normally prostaglandins:
- Increase mucus
- Increase bicarbonate
- Maintain blood flow
NSAID inhibition causes:
- Acid injury
- Mucosal erosion
- Ulcer formation
In Kidney
Prostaglandins maintain renal perfusion.
NSAID inhibition causes:
- Renal vasoconstriction
- Reduced GFR
- Fluid retention
In Airways
COX inhibition shifts arachidonic acid metabolism toward leukotriene pathway.
Result:
- Bronchospasm in susceptible patients
⚠️ IF DAMAGED
Cause → Effect
- Loss of gastric protection → ulcer
- Reduced renal blood flow → renal injury
- Increased leukotrienes → asthma exacerbation
Steroid Adverse Effects
🧠 CORE
- Steroids inhibit phospholipase A₂.
- Block both COX and LOX pathways.
- Powerful anti-inflammatory drugs.
- Cause immunosuppression.
Major adverse effects:
- Hyperglycemia
- Hypertension
- Osteoporosis
- Infection risk
- Muscle wasting
🔬 CONCEPT EXPLAINED
Steroids act earlier than NSAIDs in the inflammatory pathway.
They prevent release of arachidonic acid from membrane phospholipids.
Therefore:
- Prostaglandin synthesis decreases
- Leukotriene synthesis decreases
This produces strong anti-inflammatory action.
However, long-term suppression of inflammatory and immune pathways causes systemic adverse effects.
⚠️ IF DAMAGED
Long-term steroid therapy may cause:
- Diabetes mellitus
- Osteoporosis
- Cushingoid appearance
- Delayed wound healing
- Increased infection susceptibility
Prostanoid Catabolism
🧠 CORE
- Prostanoids have very short half-life.
- Rapidly metabolized in lungs, liver, and kidneys.
- Inactivated by enzymatic oxidation.
- Prevents excessive inflammation.
🔬 CONCEPT EXPLAINED
Prostaglandins and thromboxanes act locally near their site of synthesis.
Rapid degradation is necessary because prolonged prostanoid action could cause:
- Excess vasodilation
- Persistent pain
- Chronic inflammation
- Hemodynamic instability
This allows tight regulation of inflammatory responses.
⚠️ IF DAMAGED
Reduced prostanoid breakdown may cause:
- Persistent inflammatory response
- Chronic pain
- Excess vascular effects
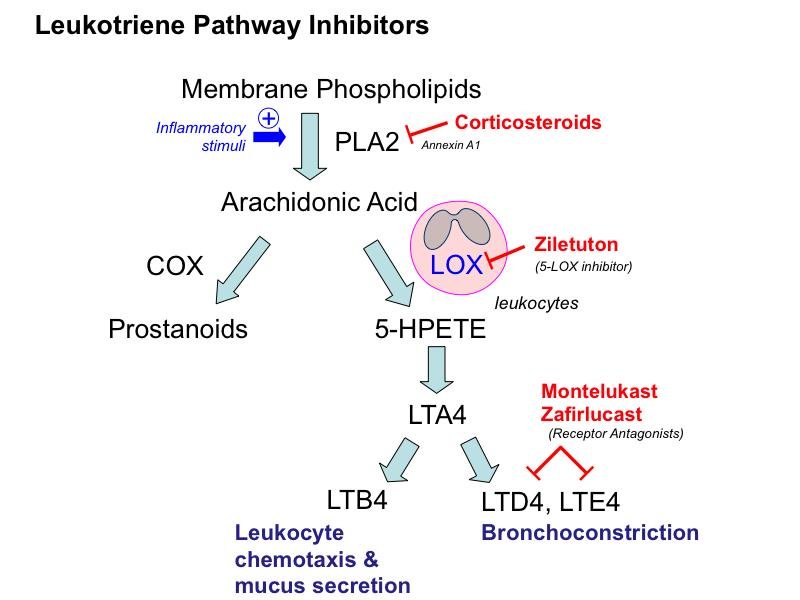
4️⃣ Lipoxygenase (LOX) Pathway and Leukotrienes
🧠 CORE
- Lipoxygenase pathway converts arachidonic acid into leukotrienes.
- Mediated mainly by 5-lipoxygenase enzyme.
- Leukotrienes are important inflammatory mediators.
- Major role in asthma and allergy.
- Cause bronchoconstriction and chemotaxis.
- Leukotriene inhibitors are used in asthma therapy.
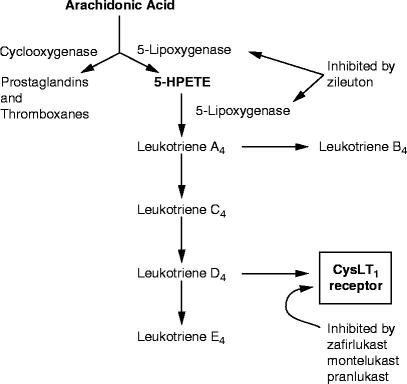
🔬 CONCEPT EXPLAINED
When arachidonic acid enters the lipoxygenase pathway, it is converted into leukotrienes.
Leukotriene Synthesis
- Arachidonic acid released from membrane
- 5-lipoxygenase activated
- Formation of LTA₄
- LTA₄ converted into:
- LTB₄
- LTC₄
- LTD₄
- LTE₄
Functions of Leukotrienes
| Leukotriene | Major Action |
|---|---|
| LTB₄ | Neutrophil chemotaxis |
| LTC₄ | Bronchoconstriction |
| LTD₄ | Increased vascular permeability |
| LTE₄ | Mucus secretion |
Leukotrienes exist because inflammatory cells require chemical mediators to recruit immune cells and regulate airway responses.
Leukotriene Inhibitors
🧠 CORE
- Zileuton inhibits 5-lipoxygenase.
- Prevents leukotriene synthesis.
- Reduces bronchoconstriction.
- Used in bronchial asthma.
🔬 CONCEPT EXPLAINED
Zileuton blocks conversion of arachidonic acid into leukotrienes.
Result:
- Reduced airway inflammation
- Reduced edema
- Reduced bronchospasm
This improves airflow in asthmatic patients.
⚠️ IF DAMAGED
Adverse effect:
- Hepatotoxicity
- Elevated liver enzymes
Leukotriene Receptor Antagonists
🧠 CORE
Examples:
- Montelukast
- Zafirlukast
Functions:
- Block leukotriene receptors
- Reduce bronchoconstriction
- Improve asthma symptoms
🔬 CONCEPT EXPLAINED
These drugs do not stop leukotriene formation.
Instead, they block leukotriene receptors on bronchial smooth muscle and inflammatory cells.
Effects:
- Bronchodilation
- Reduced mucus secretion
- Reduced airway edema
Especially useful in:
- Allergic asthma
- Exercise-induced asthma
⚠️ IF DAMAGED
Failure of therapy may cause:
- Persistent wheezing
- Airway inflammation
- Recurrent asthma attacks
Rare adverse effects:
- Headache
- Neuropsychiatric symptoms
⚙️ 4️⃣ Functional Flow
Eicosanoid Metabolism Flow
- Cell membrane phospholipids contain arachidonic acid
- Phospholipase A₂ releases arachidonic acid
- Arachidonic acid enters two pathways:
COX Pathway
- COX converts arachidonic acid → prostaglandins + thromboxanes
- Prostaglandins produce:
- Pain
- Fever
- Vasodilation
- TXA₂ promotes platelet aggregation
LOX Pathway
- 5-lipoxygenase converts arachidonic acid → leukotrienes
- Leukotrienes cause:
- Bronchoconstriction
- Chemotaxis
- Allergy
Drug Actions
- Steroids inhibit phospholipase A₂
- NSAIDs inhibit COX enzymes
- Aspirin irreversibly inhibits COX
- Zileuton inhibits 5-LOX
- Montelukast blocks leukotriene receptors
🩺 5️⃣ Clinical Correlation
Bronchial Asthma
- Leukotrienes are major mediators of bronchospasm.
- Montelukast and zileuton are used therapeutically.
Peptic Ulcer Disease
- NSAIDs reduce protective gastric prostaglandins.
- Causes gastric erosion and bleeding.
Cardiovascular Disease Prevention
- Low-dose aspirin reduces platelet aggregation.
- Prevents thrombosis and myocardial infarction.
Aspirin-Induced Asthma
- COX inhibition increases leukotriene pathway activity.
- Produces bronchospasm.
Long-Term Steroid Therapy
May cause:
- Hyperglycemia
- Osteoporosis
- Infection susceptibility
📌 6️⃣ Summary Points
- Eicosanoids are derived from arachidonic acid.
- COX pathway forms prostaglandins and thromboxanes.
- LOX pathway forms leukotrienes.
- COX-1 is protective; COX-2 is inflammatory.
- Aspirin irreversibly inhibits COX.
- NSAIDs commonly cause gastric ulceration.
- Steroids inhibit phospholipase A₂.
- Leukotrienes are major mediators in asthma.
- Montelukast blocks leukotriene receptors.
- Zileuton inhibits 5-lipoxygenase.
- TXA₂ promotes platelet aggregation.
- PGI₂ inhibits platelet aggregation.