
📖 Step 2 — Learning Material
🔹 1️⃣ Introduction
Colorectal carcinoma is one of the most common gastrointestinal malignancies worldwide and is an important cause of cancer-related mortality. It mainly affects the colon and rectum, particularly the sigmoid colon and rectosigmoid junction. The disease develops gradually through genetic mutations and transformation of normal mucosa into adenomatous polyps and finally carcinoma. Understanding colorectal carcinoma is essential because early diagnosis significantly improves survival. Clinically, patients commonly present with altered bowel habits, rectal bleeding, weight loss, or intestinal obstruction. Pathology explains the cellular changes and staging of the tumor, while surgery focuses on diagnosis, investigation, and management. This topic integrates pathology and surgery to help students understand disease progression and clinical decision-making.
🔹 2️⃣ Foundation Concepts
Key Definitions
- Colorectal carcinoma (CRC): Malignant tumor arising from epithelial lining of colon or rectum.
- Adenocarcinoma: Most common histological type of colorectal cancer.
- Polyp: Abnormal mucosal growth projecting into intestinal lumen.
- Metastasis: Spread of malignant cells to distant organs.
- TNM staging: System used to classify tumor extent.
- Screening colonoscopy: Endoscopic examination used for early detection.
Essential Terminology
- Right-sided colon cancer: Involves cecum and ascending colon.
- Left-sided colon cancer: Involves descending and sigmoid colon.
- Rectal carcinoma: Malignancy involving rectum.
- Dysplasia: Premalignant epithelial atypia.
- Lymphatic spread: Tumor dissemination through lymph nodes.
- Occult bleeding: Hidden blood loss in stool.
Basic Overview
- Most colorectal cancers are adenocarcinomas.
- Usually develops from adenomatous polyps.
- Risk increases with age.
- Diet and genetics both contribute.
- Liver is the most common metastatic site.
- Early stages may be asymptomatic.
- Screening reduces mortality.
- Surgery is the main curative treatment.
🔹 3️⃣ Core Learning — Curriculum Coverage
PATHOLOGY
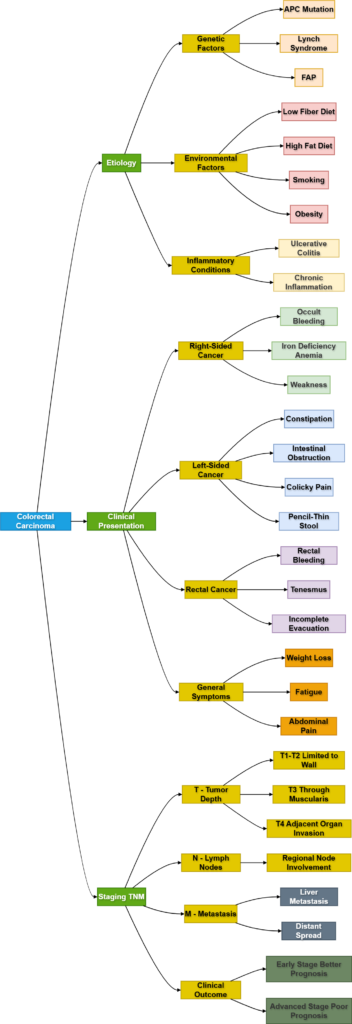
A. Etiology of Colorectal Carcinoma
🧠 CORE
- Colorectal carcinoma develops due to genetic and environmental factors.
- Most arise from adenomatous polyps.
- High-fat, low-fiber diet increases risk.
- Familial syndromes strongly predispose to CRC.
- Chronic inflammatory bowel disease increases risk.
- Age >50 years is a major risk factor.
- Smoking and obesity contribute to carcinogenesis.
- APC gene mutation is common in sporadic CRC.
- Lynch syndrome involves mismatch repair gene defects.
🔬 CONCEPT EXPLAINED
The colon normally undergoes continuous epithelial turnover. Controlled cell division maintains mucosal integrity. Mutations affecting growth-regulating genes cause uncontrolled proliferation.
Most colorectal cancers follow the adenoma-carcinoma sequence. Initially, mutation of the APC tumor suppressor gene leads to formation of adenomatous polyps. Additional mutations involving KRAS and p53 promote progression toward invasive carcinoma.
Diet rich in processed meat and low in fiber prolongs exposure of mucosa to carcinogens. Chronic inflammation in ulcerative colitis causes repeated mucosal injury and dysplasia.
Genetic syndromes accelerate malignant transformation:
- Familial adenomatous polyposis (FAP): Hundreds of polyps develop due to APC mutation.
- Lynch syndrome: DNA mismatch repair defects cause microsatellite instability.
⚠️ IF DAMAGED
- Mutation of tumor suppressor genes → uncontrolled cell division.
- Loss of DNA repair mechanisms → accumulation of mutations.
- Chronic inflammation → repeated epithelial injury → dysplasia.
- Progressive dysplasia → invasive carcinoma.
- Untreated carcinoma → metastasis and bowel obstruction.
B. Histological Findings of Colorectal Carcinoma
🧠 CORE
- Most tumors are adenocarcinomas.
- Tumor arises from glandular epithelium.
- Malignant glands invade bowel wall.
- Nuclear atypia and hyperchromasia are present.
- Increased mitotic activity occurs.
- Mucin production may be seen.
- Necrosis is common in advanced lesions.
- Tumor may invade lymphatics and blood vessels.
- Degree of differentiation affects prognosis.
🔬 CONCEPT EXPLAINED
Normal colonic mucosa contains orderly tubular glands lined by columnar epithelium. In carcinoma, gland architecture becomes distorted.
Microscopically:
- Glands become irregular and crowded.
- Cells show enlarged hyperchromatic nuclei.
- Loss of polarity occurs.
- Tumor invades through muscularis mucosa into deeper layers.
Some tumors produce abundant mucin forming mucinous adenocarcinoma. Poorly differentiated tumors lose gland formation and behave aggressively.
Tumor invasion into lymphatics allows spread to regional lymph nodes. Venous invasion facilitates liver metastasis through portal circulation.
⚠️ IF DAMAGED
- Loss of glandular organization → impaired absorption and secretion.
- Deep wall invasion → bowel wall thickening.
- Vascular invasion → distant metastasis.
- Lymphatic spread → nodal enlargement.
- Poor differentiation → rapid progression and poor prognosis.
C. Clinical Presentation of Colorectal Carcinoma
🧠 CORE
- Rectal bleeding is common.
- Altered bowel habits may occur.
- Weight loss occurs in advanced disease.
- Iron deficiency anemia suggests right-sided cancer.
- Left-sided tumors commonly cause obstruction.
- Tenesmus occurs in rectal carcinoma.
- Abdominal pain may develop.
- Fatigue may result from chronic blood loss.
- Liver metastasis may cause hepatomegaly.
🔬 CONCEPT EXPLAINED
Clinical features depend on tumor location.
Right-sided tumors
The right colon has a wider lumen and liquid fecal content. Tumors grow silently for longer periods. Chronic occult bleeding leads to iron deficiency anemia and weakness.
Left-sided tumors
The left colon has narrower lumen and solid feces. Circumferential tumors cause intestinal obstruction leading to constipation, abdominal distension, and colicky pain.
Rectal tumors
Rectal cancers commonly present with:
- Fresh blood per rectum
- Tenesmus
- Sensation of incomplete evacuation
Systemic symptoms such as cachexia and weight loss occur in advanced malignancy.
⚠️ IF DAMAGED
- Tumor ulceration → chronic bleeding → anemia.
- Luminal narrowing → bowel obstruction.
- Local invasion → pain and perforation.
- Liver metastasis → hepatomegaly and jaundice.
- Progressive disease → cachexia and weakness.
D. Staging of Colorectal Carcinoma
🧠 CORE
- Staging determines prognosis and treatment.
- TNM system is commonly used.
- T describes tumor invasion depth.
- N describes lymph node involvement.
- M describes distant metastasis.
- Stage I disease is localized.
- Stage IV disease has distant spread.
- Liver is common metastatic site.
- Early-stage cancers have better survival.
🔬 CONCEPT EXPLAINED
Tumor stage reflects anatomical spread.
T Stage
- T1/T2: Limited to bowel wall
- T3: Extends through muscularis propria
- T4: Invades adjacent structures
N Stage
Regional lymph node involvement worsens prognosis.
M Stage
Distant metastasis indicates advanced disease.
The liver is commonly affected because venous drainage of colon enters portal circulation.
Staging guides management:
- Early stages → surgical resection
- Advanced stages → surgery + chemotherapy
⚠️ IF DAMAGED
- Advanced invasion → perforation and local spread.
- Nodal involvement → higher recurrence risk.
- Metastasis → reduced survival.
- Late-stage diagnosis → limited curative options.
SURGERY
E. Clinical Features of Colorectal Cancers
🧠 CORE
- Symptoms vary with tumor site.
- Rectal bleeding is important warning sign.
- Change in bowel habit is common.
- Obstruction occurs mainly in left-sided lesions.
- Anemia suggests chronic occult bleeding.
- Weight loss suggests advanced disease.
- Rectal examination is essential.
- Palpable abdominal mass may occur.
🔬 CONCEPT EXPLAINED
Clinical assessment begins with detailed history and examination.
Right-sided cancers usually present late because stool is liquid and lumen is wide. Patients may only complain of fatigue due to anemia.
Left-sided lesions produce obstructive symptoms because of narrow lumen:
- Constipation
- Pencil-thin stools
- Colicky abdominal pain
Rectal examination can identify low rectal tumors. Examination also helps assess fixation and local spread.
⚠️ IF DAMAGED
- Delayed diagnosis → advanced-stage disease.
- Obstruction → bowel perforation.
- Chronic blood loss → severe anemia.
- Local invasion → pelvic pain and urinary symptoms.
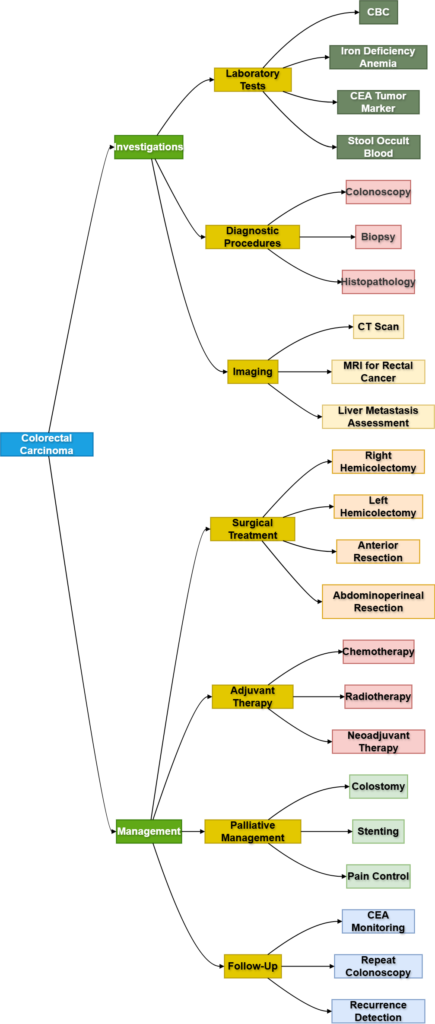
F. Investigations of Colorectal Cancers
🧠 CORE
- Colonoscopy is gold standard investigation.
- Biopsy confirms diagnosis.
- CT scan assesses spread.
- MRI is important for rectal cancer staging.
- CEA is used as tumor marker.
- CBC may show iron deficiency anemia.
- Stool occult blood test aids screening.
- Imaging detects metastasis.
🔬 CONCEPT EXPLAINED
Colonoscopy
Allows direct visualization and biopsy of lesions. Polyps may also be removed during procedure.
Biopsy
Histopathological examination confirms malignancy.
CT Scan
Evaluates:
- Local spread
- Lymph node involvement
- Liver metastasis
MRI
Provides detailed pelvic anatomy and rectal tumor staging.
CEA (Carcinoembryonic Antigen)
Used mainly for monitoring recurrence after treatment rather than diagnosis.
⚠️ IF DAMAGED
- Failure of screening → delayed diagnosis.
- Missed metastasis → inappropriate treatment planning.
- Incomplete staging → poor surgical outcomes.
G. Management of Colorectal Cancers
🧠 CORE
- Surgery is main curative treatment.
- Resection removes tumor and lymph nodes.
- Chemotherapy is used in advanced disease.
- Radiotherapy is important for rectal cancer.
- Early detection improves prognosis.
- Palliative care relieves symptoms in advanced cases.
- Stoma may be required in some patients.
- Follow-up is essential for recurrence detection.
🔬 CONCEPT EXPLAINED
Surgical Management
Treatment depends on location and stage.
- Right hemicolectomy → right-sided tumors
- Left hemicolectomy → left-sided tumors
- Anterior resection → upper rectal tumors
- Abdominoperineal resection → low rectal tumors
Adequate lymph node removal is essential for staging and recurrence reduction.
Chemotherapy
Used for:
- Node-positive disease
- Metastatic disease
- Adjuvant therapy
Radiotherapy
Especially useful in rectal carcinoma to reduce local recurrence.
Palliative Care
Advanced disease may require:
- Stenting
- Colostomy
- Pain control
⚠️ IF DAMAGED
- Incomplete resection → recurrence.
- Untreated obstruction → perforation and sepsis.
- Metastatic disease → organ failure.
- Delayed treatment → poor survival.
⚙️ 4️⃣ Functional Flow
Structure → Function → Outcome
Normal Colon
- Organized glandular epithelium
→ Absorption and mucus secretion
→ Smooth bowel function
Dysplastic Epithelium
- Abnormal cell proliferation
→ Loss of growth control
→ Polyp formation
Invasive Carcinoma
- Tumor invades bowel wall
→ Obstruction and bleeding
→ Metastasis and systemic illness
🩺 5️⃣ Clinical Correlation
Familial Adenomatous Polyposis (FAP)
- Autosomal dominant APC mutation
- Hundreds of adenomatous polyps develop
- Very high risk of colorectal carcinoma
Lynch Syndrome
- Defective DNA mismatch repair
- Early-onset colorectal cancer
- Associated with endometrial carcinoma
Obstructive Left-Sided Colon Cancer
- Narrow lumen predisposes obstruction
- Presents with constipation and abdominal distension
- Surgical emergency may occur
Liver Metastasis
- Common due to portal venous drainage
- Causes hepatomegaly and weight loss
- Advanced-stage disease indicator
📌 6️⃣ Summary Points
- Most colorectal cancers are adenocarcinomas.
- Adenoma-carcinoma sequence is central to pathogenesis.
- APC mutation is an early event in CRC development.
- Right-sided tumors commonly cause anemia.
- Left-sided tumors commonly cause obstruction.
- Rectal bleeding in elderly patients must be investigated.
- Colonoscopy with biopsy is gold standard diagnosis.
- TNM staging guides prognosis and treatment.
- Liver is the most common metastatic site.
- Surgery is the main curative treatment.
- Radiotherapy is especially important in rectal carcinoma.
- Early screening significantly reduces mortality.